A Fork in the Road: Navigating Through New Terrain
|
|
|
- Edmund Quinn
- 6 years ago
- Views:
Transcription
1 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for Diabetes and Endocrinology Spokane, Washington Chairperson, Professional Practice Committee American Diabetes Association
2 Disclosure - Duality of Interest Consultant, Advisory Board Amylin Pharmaceuticals, Boehringer Ingelheim, Eli Lilly Speakers Bureau Amylin, Eli Lilly, Merck, Novo Nordisk, sanofi-aventis
:243-54. DCCT Study Group. N Engl J Med 329:977, 1993. UKPDS 35. Stratton IM.")
3 Relative Risk of Complications Complications Risk in Diabetes The Impact of Intensive Glycemic Control Hemoglobin A1c eag Glucose DM Kendall. International Diabetes Center Adapted from: Skyler JS. Endocrinol Metab Clin North Am Jun;25(2): DCCT Study Group. N Engl J Med 329:977, UKPDS 35. Stratton IM. BMJ 321: , 2000.
4 Cardiovascular Disease and Diabetes ~65% of deaths are due to CV disease Coronary heart disease deaths 2- to 4-fold Cardiovascular complications of T2DM Stroke risk 2- to 4-fold Bell DSH. Diabetes Care. 2003;26: Centers for Disease Control (CDC). Heart failure 2- to 5-fold T2DM = type 2 diabetes mellitus
5 Glycemic Control for Vascular Complications: Is Late Too Late? ADVANCE VADT ACCORD Kumamoto UGDP VA UKPDS UKPDS + DCCT EDIC SDIS At Risk Years of Diabetes Diagnosis
6 Glycemic Control for Vascular Complications: Is Late Too Late? Type 1 Diabetes N Duration of Diabetes Baseline A1C Follow Up (Yrs) Publication DCCT 1441 <5 9.0% Stockholm (SDIS) 102 ~18 9.4% EDIC 1394 ~ % Type 2 Diabetes UGDP 823 <1 ~7% (145 mg/dl) ~ Kumamoto VACSDM ½ 1995 UKPDS 5102 <1 ~9% /2008 ACCORD ½ 2008 ADVANCE VADT
7 Early Intensive Diabetes Therapy: Reduction in Microvascular Complications DCCT Kumamoto UKPDS HbA1c 9 7.1% % 7.9 7% Retinopathy 63% 69% 17-29% Nephropathy 54% 70% 24-33% Neuropathy 60% Improved - CV disease NS - 16% (NS) DCCT Research Group. N Engl J Med. 1993;329: Ohkubo Y, et al. Diabetes Res Clin Pract. 1995;28: UKPDS 33: Lancet 1998; 352,
8 Rate of Retinopathy (per 100 patient-years) Complication Rate (%) per 1,000 Person-years DCCT and UKPDS Glycemic Control and Microvascular Risk DCCT UKPDS A1C (%) Updated Mean HbA 1c (%) DCCT Study Group. N Engl J Med 329:977, 1993 UKPDS 35. Stratton IM. BMJ. 2000;321:
9 Early Intervention Is It Truly Early? Benefit in Primary and Secondary Prevention Reduction in microvascular disease risk Occurred with both primary and secondary prevention Effect observed in DCCT, UKPDS and Kumamoto Primary Prevention Secondary Intervention DCCT Research Group. N Engl J Med. 1993;329:
10 Stockholm Diabetes Intervention Study Is Late Intervention for Glycemic Control of Benefit? SDIS Study Design Intensive insulin therapy A1C Mean duration of diabetes at study entry = ~18 years Significant (but modest) reduction in rates of microvascular disease Reichard P. N Engl J Med 1993;329;
11 The Durable Effect of Early Intervention Long Term Follow up from EDIC and UKPDS Follow up cohort with similar glycemic control for years A1C achieved = ~8.0% Retinopathy Incidence (%) Conventional Intensive (SU/Ins) vs. Conventional control 4 Intensive EDIC YEAR EDIC Research Group. N Engl J Med 2000;342:381-9 Holman RR. N Engl J Med. 2008;359:
12 Glycemic Control for Prevention of Macrovascular Complications: ADVANCE VADT ACCORD Kumamoto UGDP VA UKPDS UKPDS + DCCT EDIC SDIS At Risk Diabetes Years of Diabetes Diagnosis
13 Comparison of Recent Glycemia Trials ACCORD, ADVANCE and VADT Characteristic ACCORD N 10,251 Mean Age 62 Duration of T2DM 10 yr History of CVD 35% BMI 32 Baseline A1C 8.3% A1C Achieved 6.4% vs. 7.5% RRR CVD Events 0.90 ( ) RRR Mortality 1.22 ( )* ACCORD Study Group. N Engl J Med. 2008;358: ADVANCE Collaborative Group. N Engl J Med 358: , Duckworth W for VADT. N Engl J Med 2009;360:129-39
14 Comparison of Recent Glycemia Trials ACCORD, ADVANCE and VADT Characteristic ACCORD ADVANCE VADT N 10,251 11,140 1,791 Mean Age Duration of T2DM 10 yr 8 yr 11.5 yr History of CVD 35% 32% 40% BMI Baseline A1C 8.3% 7.5% 9.4% A1C Achieved 6.4% vs. 7.5% 6.5% vs. 7.3% 6.9% vs. 8.4% RRR CVD Events 0.90 ( ) 0.94 ( ) 0.88 ( ) RRR Mortality 1.22 ( )* 0.93 ( ) 1.07 ( ) ACCORD Study Group. N Engl J Med. 2008;358: ADVANCE Collaborative Group. N Engl J Med 358: , Duckworth W for VADT. N Engl J Med 2009;360:129-39
15 A Broader View of Complications and Diabetes Implications of ACCORD, ADVANCE and VADT Study A1C Microvascular UKPDS DCCT/EDIC ACCORD / ADVANCE VADT Adapted from Bergenstal RM, Bailey C and Kendall DM. Am J Med 123:374e9-e18, 2010 UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352: Holman RR. N Engl J Med Oct 9;359(15): DCCT Research Group. N Engl J Med 329; , 1993 Nathan DM, et al. N Engl J Med. 2005;353: Gerstein HC, et al. N Engl J Med. 2008;358: Patel A, et al. N Engl J Med. 2008;358: Duckworth W et al N Engl J Med 2009;360: EY Chew for ACCORD. N Engl J Med ( /NEJMoa ) was published on June 29, 2010, at NEJM.org. Initial Trial Long Term Follow-up
16 A Broader View of Complications and Diabetes Implications of ACCORD, ADVANCE and VADT Study A1C Microvascular CVD Mortality UKPDS DCCT/EDIC ACCORD / ADVANCE VADT Adapted from Bergenstal RM, Bailey C and Kendall DM. Am J Med 123:374e9-e18, 2010 UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352: Holman RR. N Engl J Med Oct 9;359(15): DCCT Research Group. N Engl J Med 329; , 1993 Nathan DM, et al. N Engl J Med. 2005;353: Gerstein HC, et al. N Engl J Med. 2008;358: Patel A, et al. N Engl J Med. 2008;358: Duckworth W et al N Engl J Med 2009;360: EY Chew for ACCORD. N Engl J Med ( /NEJMoa ) was published on June 29, 2010, at NEJM.org. Initial Trial Long Term Follow-up
17 Epidemiologic Relationships Between A1c and All-cause Mortality in the ACCORD Trial Does A1C achieved predict a risk for all-cause mortality? Riddle M et al. Diabetes Care May;33(5):983-90
18 Epidemiologic Relationships Between A1c & All- Cause Mortality Effects of Intensive Glucose Lowering in the Management of Patients with Type 2 Diabetes Mellitus in ACCORD Baseline A1c >8.5% predicted 64% higher risk of death? Legacy from prior poor control? More B cell destruction? adherence Also history of taking aspirin Self-report of having neuropathy Riddle M et al. Diabetes Care May;33(5):983-90
19 ACCORD Glycemia Trial: Cause of Cardiovascular Deaths Intensive N (%) Standard N (%) Unexpected/Presumed CVD 86 (1.7) 67 (1.3) MI 19 (0.4) 13 (0.3) CHF 23 (0.5) 16 (0.3) CV Procedure 10 (0.2) 3 (0.1) Arrhythmia 4 (0.1) 10 (0.2) Non-CV Procedure 1 (0.02) 3 (0.1) Stroke 9 (0.2) 11 (0.2) Other CVD 8 (0.2) 10 (0.2) Total CV
20 Severe Hypoglycemia Requiring Medical Assistance Intensive Group Annual Incidence Rate = 3.3% Standard Group Annual Incidence Rate = 1.0%

21 ADVANCE: Severe Hypoglycemia and Adverse Clinical Outcomes Zoungas S et al. N Engl J Med 2010;363:
22 A Reasonable Hypothesis Intensive glycemic therapy increased all-cause and cardiovascular mortality because there was more overall hypoglycemia with intensive therapy. Duckworth W, Abraira C, Moritz T, Reda D et al NEJM 360: , 2009 ACCORD Study Group. NEJM 358: , 2008.
23 Hypoglycemia and CV Disease Hemodynamic Hypoglycemia Thrombotic Ischemia Arrhythmia Inflammatory Wright R et al Diabetes/ Metabolism Research and Reviews, 2008

24
25
26
27
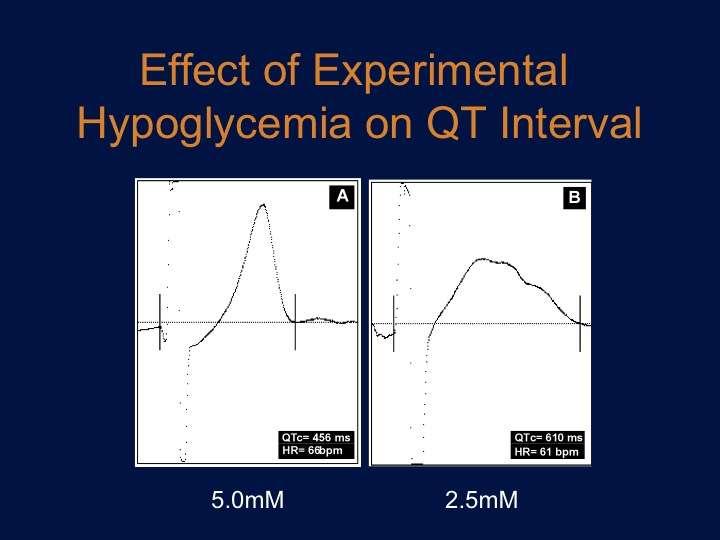
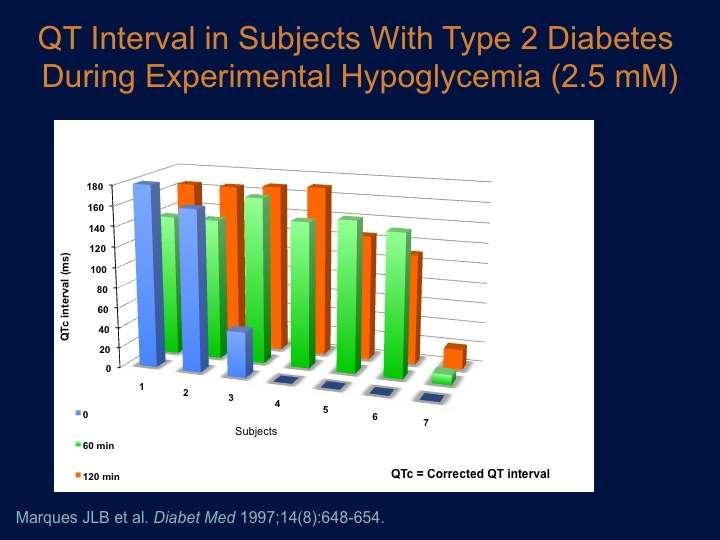
28 Hematologic and Inflammatory Responses to Acute Hypoglycemia
29 Intensive Glycemic Control in Diabetes: Implications of ACCORD, ADVANCE and VADT Intensive Glycemic Control in Diabetes Lowering A1C to < 7% significantly reduces the risk of microvascular complications in both type 1 and type 2 diabetes (DCCT, UKPDS, ACCORD) Does not reduce the risk of CVD events in short term studies Does not significantly increase mortality risk across studies (meta-analyses) Adverse effects of more intensive therapies 3-fold greater rates of severe hypoglycemia and risk of significant weight gain Increase in mortality risk in selected populations For some patients lower or higher A1C targets may be appropriate Skyler JS. Diabetes Care. 2009;32(1):187-92
30 Identifying Higher Risk Patients Intensive Glycemic Control in Type 2 Diabetes Conventional Wisdom: Older individuals with established CVD Those who achieved lower A1C values Use of insulin therapy Individuals with long duration diabetes Who May Be at Risk with more intensive Rx Longstanding poor control History of severe hypoglycemia Those less responsive to intensive Rx NO NO MAYBE MAYBE YES YES MAYBE
31 Diabetes and Glycemic Control A Rational Approach to A1C Targets As low as possible As early as possible For as long as possible As safely as possible And as rationally as possible And in the setting of multi-risk factor management
32 Glycemic Recommendations for Nonpregnant Adults with Diabetes 2011 Standards of Medical Care. Diabetes Care. 34: Suppl 1
33 Managing Hypertension in Diabetes Treatment Targets Treatment Approaches Implications of Recent Trials
34 Blood Pressure Goal in Diabetes < 130 extrapolated from benefits in nephropathy Bakris G. AJKD 2004;43(Suppl 1):S120
35 Complication Rate per 1000 person-years Type 2 Diabetes and Blood Pressure: BP Control and Risk in the ACCORD and ADVANCE Era 40 Microvascular Myocardial Infarction 30??? -10% -30% ~ 15% reduction in risk for each 10 mm Hg decrease in SBP ACCORD ADVANCE UKPDS Modified from Adler A. BMJ 321; , 2000 Mean SBP (mm Hg)
 Reduced all cause mortality Patel A for the ADVANCE Investigators.")
36 ADVANCE Trial Blood Pressure Intervention 11,140 subjects Type 2 diabetes and HTN Treated with fixed dose combo (ACEI-diuretic) vs usual care Blood pressure differential ~5 mm Hg (140.3 vs 134.7) Reduced all cause mortality Patel A for the ADVANCE Investigators. Lancet 370: , 2008
37 Multi-Risk Factor Intervention in Diabetes: The ACCORD Trial Intensive (SBP<120) BP Trial Standard (SBP<140) Group A Statin only Lipid Trial Group B Statin+Fibrate Intensive Glycemic Control (HbA1c<6%) Target SBP < 120 vs < * Standard Glycemic Control (HbA1c 7-7.9%) Multi-drug therapy Systematic titration Target driven approach * 2362* 2371* 2753* 2765* 10,251 *Primary analysis compares marginals for main effects ACCORD Study Group. Am J Cardiol 99(12A):21i-33i, 2007.
38 Effects of Intensive Blood Pressure Control The ACCORD Trial DBP=70.5 DBP=64.4 ACCORD Study Group. N Engl J Med Apr 29;362(17): Epub 2010 Mar 14.
39 Effects of Intensive Blood Pressure Control The ACCORD Trial More intensive control of SBP did not further reduce CVD risk in type 2 diabetes ACCORD Study Group. N Engl J Med Apr 29;362(17): Epub 2010 Mar 14.
40 The ACCORD Trial Effects of Intensive Blood Pressure Control in Type 2 Diabetes Intensive Events (%/yr) Standard Events (%/yr) HR (95% CI) P Primary 208 (1.87) 237 (2.09) 0.88 ( ) 0.20 Reduced rate of CVA and of progression of macroalbuminuria with more intensive blood pressure lowering Total Mortality 150 (1.28) 144 (1.19) 1.07 ( ) 0.55 CV Death 60 (0.52) 58 (0.49) 1.06 ( ) 0.74 The ACCORD Study Group. N Engl J Med Nonfatal Published MI at March (1.13) 14, 2010 ( /NEJMoa ) 146 (1.28) 0.87 ( ) 0.25 Nonfatal Stroke 34 (0.30) 55 (0.47) 0.63 ( ) 0.03 Total Stroke 36 (0.32) 62 (0.53) 0.59 ( ) 0.01 ACCORD Study Group. N Engl J Med Apr 29;362(17): Epub 2010 Mar 14.


41 Adverse Effects of Intensive Blood Pressure Lowering in ACCORD

42 SO WHAT BP SHOULD WE TARGET?
43 Systolic BP Targets in Diabetes Does the Evidence Support SBP Targets < 130? Trial N Mean SBP less intense Mean SBP more intense CVD Risk Reduction SHEP * 143* 22-56% Syst-Eur % HOT 1, ** 140** 30-67% UKPDS 1, % ABCD No CVD reduction ADVANCE 11, % * Communication - Sara Pressel: mean BP at 3 yrs of F/U ** BP in diabetes + non-diabetes population
44 Hypertension: 2011 Standards of Medical Care Goals A goal Whysystolic weren t blood the pressure BP targets < 130 mmhg changed? is appropriate for most patients with diabetes. No evidence of harm < 130. Based Definite on patient evidence characteristics of and benefit response < 140 to therapy, higher or lower systolic blood pressure targets ADVANCE may be appropriate. suggested benefit < 135 If you target 140, then most people will be satisfied with close enough and not get < 140 Patients with diabetes should be treated to a diastolic blood pressure <80 mmhg.
45 Individualizing Goals: Decision Points # Drugs Little evidence above three Orthostatic hypotension Side effects from medications Dizziness Bradycardia Drug interactions How low is too low for diastolic blood pressure?


46 J-Shaped cureve with Blood Pressure: INVEST I S Systolic BP Diastolic BP I S Bangalore S et al. Circulation 122:2142, 2010

47 Proper Measurement of Blood Pressure

48 Assure Proper Fit of Blood Pressure Cuff
49 Ambulatory BP Monitoring ABPM is warranted for evaluation of white-coat HTN in the absence of target organ injury. Ambulatory BP values are usually lower than clinic readings. Awake, individuals with hypertension have an average BP of <135/85 mmhg and during sleep <120/75 mmhg. BP drops by 10 to 20% during the night; if not, signals possible increased risk for cardiovascular events.
50 Managing Lipids in Diabetes Treatment Targets Treatment Approaches Implications of ACCORD

51 The ACCORD Trial Lipid Study Protocol BP Trial Lipid Trial Intensive (SBP<120) Standard (SBP<140) Group A Statin only Group B Statin+Fibrate Intensive Glycemic Control (HbA1c<6%) Fenofibrate or Placebo * Standard Glycemic Control (HbA1c 7-7.9%) Background statin 1370 LDL HDL < 50 and TG < * 2362* 2371* 2753* 2765* 10,251 *Primary analysis compares marginals for main effects ACCORD Study Group. Am J Cardiol 99(12A):21i-33i, 2007.
52 The ACCORD Trial Lipid Study Effect on Plasma Lipids The ACCORD Study Group. N Engl J Med Apr 29;362(17): Published at March 14, 2010 ( /NEJMoa )
53 The ACCORD Trial Lipid Study Effect on Major CVD Events No significant added benefit (in reducing MI, stroke or CVD death) with addition of fibrate to statin therapy Post-hoc analyses suggesting potential benefit in those with lowest HDL-c (< 34 mg/dl) and higher TG (> 204 mg/dl) The ACCORD Study Group. N Engl J Med Apr 29;362(17): Published at March 14, 2010 ( /NEJMoa )
54 Primary Outcome By Treatment Group and Baseline Subgroups
 59 (2.2%) 0.43 CK ever > 10X ULN 10 (0.4%) 9 (0.3%) 0.83 Serum creatinine elevation Women ever > 1.3 mg/dl Men ever > 1.5 mg/dl 235 (27.9%) 157 (18.7%) <0.001 698 (36.")
55 Lab Measures During Follow-up Fenofibrate Placebo Laboratory Measures (no. (%)) (N=2765) (N=2753) P value ALT ever > 3X ULN 52 (1.9%) 40 (1.5%) 0.21 ALT ever > 5X ULN 16 (0.6%) 6 (0.2%) 0.03 CK ever > 5X ULN 51 (1.9%) 59 (2.2%) 0.43 CK ever > 10X ULN 10 (0.4%) 9 (0.3%) 0.83 Serum creatinine elevation Women ever > 1.3 mg/dl Men ever > 1.5 mg/dl 235 (27.9%) 157 (18.7%) < (36.7%) 350 (18.5%) <0.001 Post-randomization incidence of microalbuminuria ( > 30 to < 300 mg/g*) 1050 (38.2%) 1137 (41.6%) 0.01 Post-randomization incidence of macroalbuminuria ( > 300 mg/g*) 289 (10.5%) 337 (12.3%) 0.03

56 ACCORD Eye Study: Fenofibrate decreased risk of progression of retinopathy The ACCORD Study Group. NEJM 2010;363:
57 Standards of Medical Care in Diabetes Lipid Management for CVD Risk Lowering LDL Cholesterol Primary goal = LDL cholesterol <100 mg/dl (LDL-C < 70 an option) Statin (+MNT) added in those with known CVD or at higher risk Alternative = 30-40% reduction in LDL-c Targeting Triglycerides and HDL-c Low HDL-C + high TG = most common pattern of dyslipidemia Managing TG and HDL-C Limited evidence that intervention with fibrate on top of statin further reduces CV risk (may be benefit for retinopathy and nephropathy) Data of addition of niacin to statin remains under study Standards of Medical Care in Diabetes 2011 Diabetes Care 34 (Suppl 1), 2011
58 Antiplatelet Agents in Diabetes, 2011 Primary Prevention ( mg/day): Type 1 or type 2 diabetes at increased CV risk (10 yr risk > 10%), including most men > 50 yr or women >60 yr who have at least one additional major risk factor (family history of CVD, hypertension, smoking, dyslipidemia, or albuminuria) (C) Aspirin should not be recommended for CVD prevention for adults with diabetes at low CVD risk (10-year CVD risk <5%) (C) In patients in these age-groups with multiple other risk factors (e.g. 10-year risk 5 10%), clinical judgment is required. (E) Secondary prevention ( mg/day): Use aspirin therapy as a secondary prevention strategy in those with diabetes with a history of CVD (A) For patients with CVD and documented aspirin allergy, clopidogrel (75 mg/day) should be used. (B) ADA Clinical Practice Recommendations, Diabetes Care, January 2011
59 Basis for Change in Recommendation Reference N Relative risk Confiendece Interval Belch (2008) ( ) NS Ogawa (2008) ( ) NS Belch J et al. BMJ 2008; 357:a1840 Ogawa H et al. JAMA
60 ADA Summary of Recommendations for Adults with Diabetes Measures A1C Treatment targets for diabetes as recommended remain Pre-meal glucose mg/dl unchanged as evidence Peak post-meal glucose < supports: 180 mg/dl 1. Targeting A1C < 7% (for reduction in risk of Blood Pressure: LDL-c 3. LDL lowering with statin (LDL<100 or 30-40%) Triglycerides < 150 mg/dl HDL-c Targets 2011 Standards of Care microvascular disease) < 7% < 130/80 mm Hg 2. SBP target < 130 supported by evidence of reduction in risk of stroke and microvascular disease progression < 100 mg/dl Further reduction in CVD risk (with added fibrate) of potential benefit if low HDL-c and high TG > 40 mg/dl American Diabetes Association. Diabetes Care 33 (Suppl 1), 2010
61 Cardiovascular Events: Steno-2 vs ACCORD Steno-2: Cardiovascular Events ACCORD: 1 outcome (composite nonfatal MI, nonfatal CVA, CVD death) standard intensive Gaede P, et al. N Engl J Med. 2008;358:

62 Should treatment and goals be standardized or individualized?
63 Heterogeneity of Type 2 Diabetes Obese versus Lean Slowly progressive versus rapidly progressive Abnormal Fasting Glucose Abnormal Postprandial Glucose High Insulin Secretion or Low Insulin Secretion Insulin Resistance or High Insulin Sensitivity High CVD Risk or low CVD Risk CVD present or CVD absent CKD present or CKD absent Age of the patient } Combination of both

64
, nephropathy and cardiovascular events (type 2) Lipid lowering")
65 Remember, the Vasculature is Like a Tree Does it make sense to separapte out complications between microvascular and macrovascular? Field Study: Showed benefit of fenofibrate on retinopathy and neuropathy ACE-I Therapy: benefits retinopathy, (in type 1), nephropathy and cardiovascular events (type 2) Lipid lowering therapy: alters progression of neuropathy (in epidemiologic studies)

66 Thank You
Slide 1. Slide 2. Slide 3. A Fork in the Road: Navigating Through New Terrain. Diabetes Standards of Care Then and Now
 Slide 1 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for
Slide 1 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for
Microvascular Complications in Diabetes:
 Microvascular Complications in Diabetes: Perspectives on Glycemic Control to Prevent Microvascular Complications Discussion Outline: Glycemia and Microvascular Compliations Clinical Trials - A Brief History
Microvascular Complications in Diabetes: Perspectives on Glycemic Control to Prevent Microvascular Complications Discussion Outline: Glycemia and Microvascular Compliations Clinical Trials - A Brief History
ACCORD, ADVANCE & VADT. Now what do I do in my practice?
 ACCORD, ADVANCE & VADT Now what do I do in my practice? Richard M. Bergenstal, MD International Diabetes Center Park Nicollet Health Services University of Minnesota Minneapolis, MN richard.bergenstal@parknicollet.com
ACCORD, ADVANCE & VADT Now what do I do in my practice? Richard M. Bergenstal, MD International Diabetes Center Park Nicollet Health Services University of Minnesota Minneapolis, MN richard.bergenstal@parknicollet.com
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Update on CVD and Microvascular Complications in T2D
 Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Glucose Control and Prevention of Cardiovascular Disease
 Glucose Control and Prevention of Cardiovascular Disease Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Diabetes Update+, March
Glucose Control and Prevention of Cardiovascular Disease Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Diabetes Update+, March
The target blood pressure in patients with diabetes is <130 mm Hg
 Controversies in hypertension, About Diabetes diabetes and and metabolic Cardiovascular syndrome Risk ESC annual congress August 29, 2011 The target blood pressure in patients with diabetes is
Controversies in hypertension, About Diabetes diabetes and and metabolic Cardiovascular syndrome Risk ESC annual congress August 29, 2011 The target blood pressure in patients with diabetes is
Diabetes Day for Primary Care Clinicians Advances in Diabetes Care
 Diabetes Day for Primary Care Clinicians Advances in Diabetes Care Elliot Sternthal, MD, FACP, FACE Chair New England AACE Diabetes Day Planning Committee Welcome and Introduction This presentation will:
Diabetes Day for Primary Care Clinicians Advances in Diabetes Care Elliot Sternthal, MD, FACP, FACE Chair New England AACE Diabetes Day Planning Committee Welcome and Introduction This presentation will:
Glucose and CV disease
 Glucose and CV disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Glucose and CV disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
ADVANCE post trial ObservatioNal Study
 Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
What s the Goal? Individualizing Glycemic Targets. Matthew Freeby M.D. December 3 rd, 2016
 What s the Goal? Individualizing Glycemic Targets Matthew Freeby M.D. December 3 rd, 2016 Diabetes Mellitus: Complications and Co-Morbid Conditions Retinopathy Between 2005-2008, 28.5% of patients with
What s the Goal? Individualizing Glycemic Targets Matthew Freeby M.D. December 3 rd, 2016 Diabetes Mellitus: Complications and Co-Morbid Conditions Retinopathy Between 2005-2008, 28.5% of patients with
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Prevention of complications: are we winning or losing the battle. Naveed Sattar Professor of Metabolic Medicine
 Prevention of complications: are we winning or losing the battle Naveed Sattar Professor of Metabolic Medicine Duality of Interest Declaration Consultant or speaker for: Amgen, AstraZeneca, Boehringer
Prevention of complications: are we winning or losing the battle Naveed Sattar Professor of Metabolic Medicine Duality of Interest Declaration Consultant or speaker for: Amgen, AstraZeneca, Boehringer
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Blood Pressure Treatment Goals
 Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Complications of Diabetes: Screening and Prevention
 Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Hypertension Management in Diabetic Patients
 Hypertension Management in Diabetic Patients Park, Chang G, MD, PhD Cardiovascular Center, Guro Hospital, Korea University Medical School Contents (Treatment of 2 Cases) Type 2 Diabetes Mellitus Hypertension
Hypertension Management in Diabetic Patients Park, Chang G, MD, PhD Cardiovascular Center, Guro Hospital, Korea University Medical School Contents (Treatment of 2 Cases) Type 2 Diabetes Mellitus Hypertension
Preventive Cardiology Scientific evidence
 Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Hypertension and the SPRINT Trial: Is Lower Better
 Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
CV Risk Management in Diabetes Mellitus
 CV Risk Management in Diabetes Mellitus J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine University of California, San Francisco Mr. B 40 y/o Latino male c/o fatigue,
CV Risk Management in Diabetes Mellitus J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine University of California, San Francisco Mr. B 40 y/o Latino male c/o fatigue,
Update on Diabetes. Ketan Dhatariya. Why it s Not Just About Glucose Lowering Any More. Consultant in Diabetes NNUH
 Update on Diabetes Why it s Not Just About Glucose Lowering Any More Ketan Dhatariya Consultant in Diabetes NNUH The Story So Far.. DCCT Retinopathy Neuropathy Nephropathy Intensive glucose control in
Update on Diabetes Why it s Not Just About Glucose Lowering Any More Ketan Dhatariya Consultant in Diabetes NNUH The Story So Far.. DCCT Retinopathy Neuropathy Nephropathy Intensive glucose control in
Evidence-Based Glucose Management in Type 2 Diabetes
 Evidence-Based Glucose Management in Type 2 Diabetes James R. Gavin III, MD, PhD CEO and Chief Medical Officer Healing Our Village, Inc. Clinical Professor of Medicine Emory University School of Medicine
Evidence-Based Glucose Management in Type 2 Diabetes James R. Gavin III, MD, PhD CEO and Chief Medical Officer Healing Our Village, Inc. Clinical Professor of Medicine Emory University School of Medicine
Management of Cardiovascular Disease in Diabetes
 Management of Cardiovascular Disease in Diabetes Radha J. Sarma, MBBS, FACP. FACC. FAHA. FASE Professor of Internal Medicine Western University of Health Sciences. Director, Heart and Vascular Center Western
Management of Cardiovascular Disease in Diabetes Radha J. Sarma, MBBS, FACP. FACC. FAHA. FASE Professor of Internal Medicine Western University of Health Sciences. Director, Heart and Vascular Center Western
T2 Diabetes in Sep-16. Stephen Leow Disclosures. Why do we treat diabetes? Agenda. Targets
 Stephen Leow Disclosures I have received honoraria, sat on the advisory boards or received grants from Novo Nordisk, Sanofi Aventis, Eli Lilly, Boehringer Ingleheim, Jansenn Cilag, Mundipharma, BioCSL,
Stephen Leow Disclosures I have received honoraria, sat on the advisory boards or received grants from Novo Nordisk, Sanofi Aventis, Eli Lilly, Boehringer Ingleheim, Jansenn Cilag, Mundipharma, BioCSL,
The ABCs (A1C, BP and Cholesterol) of Diabetes
 of Diabetes") The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
Microvascular Disease in Type 1 Diabetes
 Microvascular Disease in Type 1 Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine The Course
Microvascular Disease in Type 1 Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine The Course
Standards of Medical Care in Diabetes 2016
 Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes
 Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Diabetes new challenges, new agents, new order
 Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
American Academy of Insurance Medicine
 American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus. Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre
 Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Macrovascular Disease in Diabetes
 Macrovascular Disease in Diabetes William R. Hiatt, MD Professor of Medicine/Cardiology University of Colorado School of Medicine President, CPC Clinical Research Conflicts CPC Clinical Research (University-based
Macrovascular Disease in Diabetes William R. Hiatt, MD Professor of Medicine/Cardiology University of Colorado School of Medicine President, CPC Clinical Research Conflicts CPC Clinical Research (University-based
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
Glycemic control a matter of life and death
 Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
Cardiovascular outcomes in type 2 diabetes: the impact of preventative therapies
 Ann. N.Y. Acad. Sci. ISSN 0077-8923 ANNALS OF THE NEW YORK ACADEMY OF SCIENCES Issue: The Year in Diabetes and Obesity Cardiovascular outcomes in type 2 diabetes: the impact of preventative therapies Sophia
Ann. N.Y. Acad. Sci. ISSN 0077-8923 ANNALS OF THE NEW YORK ACADEMY OF SCIENCES Issue: The Year in Diabetes and Obesity Cardiovascular outcomes in type 2 diabetes: the impact of preventative therapies Sophia
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Individualized Treatment Goals for Optimal Long-Term Health Outcomes among Patients with Type 2 Diabetes Mellitus
 1 Dissertation Title Page: Individualized Treatment Goals for Optimal Long-Term Health Outcomes among Patients with Type 2 Diabetes Mellitus Qian Shi, MPH, PhD candidate Department of Global Health Management
1 Dissertation Title Page: Individualized Treatment Goals for Optimal Long-Term Health Outcomes among Patients with Type 2 Diabetes Mellitus Qian Shi, MPH, PhD candidate Department of Global Health Management
Diabetes Treatment Update
 Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Diabetes Mellitus: Evaluation and Care Management
 Diabetes Mellitus: Evaluation and Care Management Michael King, MD Assistant Professor Residency Program Director University of Kentucky Dept. of Family & Community Medicine Learning Objectives 1. Review
Diabetes Mellitus: Evaluation and Care Management Michael King, MD Assistant Professor Residency Program Director University of Kentucky Dept. of Family & Community Medicine Learning Objectives 1. Review
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Aggressive Lipid Management for Diabetes
 Aggressive Lipid Management for Diabetes Practical Ways to Achieve Targets in Diabetes Care Keystone, CO July 16, 2011 Robert H. Eckel, M.D. Professor of Medicine Professor of Physiology and Biophysics
Aggressive Lipid Management for Diabetes Practical Ways to Achieve Targets in Diabetes Care Keystone, CO July 16, 2011 Robert H. Eckel, M.D. Professor of Medicine Professor of Physiology and Biophysics
The Burden of the Diabetic Heart
 The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
Ischemic Heart and Cerebrovascular Disease. Harold E. Lebovitz, MD, FACE Kathmandu November 2010
 Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Glucose Control: Does it lower CV risk?
 Glucose Control: Does it lower CV risk? Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Glucose Control: Does it lower CV risk? Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
9/29/2015. Primary Prevention of Heart Disease: Objectives. Objectives. What works? What doesn t?
 Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes
 Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
The Metabolic Syndrome: Is It A Valid Concept? YES
 The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
Kidney and heart: dangerous liaisons. Luis M. RUILOPE (Madrid, Spain)
") Kidney and heart: dangerous liaisons Luis M. RUILOPE (Madrid, Spain) Type 2 diabetes and renal disease: impact on cardiovascular outcomes The "heavyweights" of modifiable CVD risk factors Hypertension
Kidney and heart: dangerous liaisons Luis M. RUILOPE (Madrid, Spain) Type 2 diabetes and renal disease: impact on cardiovascular outcomes The "heavyweights" of modifiable CVD risk factors Hypertension
Treatment to reduce cardiovascular risk: multifactorial management
 Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
The earlier BP control the better cardiovascular outcome. Jin Oh Na Cardiovascular center Korea University Medical College
 The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes
 Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
New Clinical Trends in Geriatric Medicine. April 8, 2016 Amanda Lathia, MD, MPhil Staff, Center for Geriatric Medicine
 New Clinical Trends in Geriatric Medicine April 8, 2016 Amanda Lathia, MD, MPhil Staff, Center for Geriatric Medicine Objectives Review current guidelines for blood pressure (BP) control in older adults
New Clinical Trends in Geriatric Medicine April 8, 2016 Amanda Lathia, MD, MPhil Staff, Center for Geriatric Medicine Objectives Review current guidelines for blood pressure (BP) control in older adults
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Diabetes and the Heart
 Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center
 Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Blood pressure treatment target in diabetes. Should it be <130 mmhg?
 Blood pressure treatment target in diabetes Should it be
Blood pressure treatment target in diabetes Should it be
Prevention And Treatment of Diabetic Nephropathy. MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
 Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
SESSION 3 11 AM 12:30 PM
 SESSION 3 11 AM 12:30 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
SESSION 3 11 AM 12:30 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden
 Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Review. Hyperglycemia, dyslipidemia and hypertension in older people with diabetes: the benefits of cardiovascular risk reduction
 Review Hyperglycemia, dyslipidemia and hypertension in older people with diabetes: the benefits of cardiovascular risk reduction Diabetes mellitus is increasingly recognized as an essentially vascular
Review Hyperglycemia, dyslipidemia and hypertension in older people with diabetes: the benefits of cardiovascular risk reduction Diabetes mellitus is increasingly recognized as an essentially vascular
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Clinical Therapeutics/Volume 33, Number 1, 2011
 Clinical Therapeutics/Volume 33, Number 1, 2011 Concurrent Control of Blood Glucose, Body Mass, and Blood Pressure in Patients With Type 2 Diabetes: An Analysis of Data From Electronic Medical Records
Clinical Therapeutics/Volume 33, Number 1, 2011 Concurrent Control of Blood Glucose, Body Mass, and Blood Pressure in Patients With Type 2 Diabetes: An Analysis of Data From Electronic Medical Records
Updates in Cardiovascular Recommendations for Diabetic Patients
 Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Diabetic Nephropathy. Objectives:
 There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Diabetes and Hypertension
 Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
The promise of the thiazolidinediones in the management of type 2 diabetes-associated cardiovascular disease
 The promise of the thiazolidinediones in the management of type 2 diabetes-associated cardiovascular disease Steve Smith, Group Director Scientific Affairs, Diabetes & Metabolism GlaxoSmithKline R & D
The promise of the thiazolidinediones in the management of type 2 diabetes-associated cardiovascular disease Steve Smith, Group Director Scientific Affairs, Diabetes & Metabolism GlaxoSmithKline R & D
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
2014/10/20. Management of Lipid Disorders Eric Klug Sunninghill, Sunward Park and CM JHB Academic Hospitals
 Management of Lipid Disorders Eric Klug Sunninghill, Sunward Park and CM JHB Academic Hospitals Sudden and unexpected deaths in an adult population, Cape Town, South Africa, 2001-2005 1 Sudden and unexpected
Management of Lipid Disorders Eric Klug Sunninghill, Sunward Park and CM JHB Academic Hospitals Sudden and unexpected deaths in an adult population, Cape Town, South Africa, 2001-2005 1 Sudden and unexpected