HYPOTHERMIA IN TRAUMA. Kevin Palmer EMT-P, DiMM
|
|
|
- Grace Robertson
- 6 years ago
- Views:
Transcription
1 HYPOTHERMIA IN TRAUMA Kevin Palmer EMT-P, DiMM
2 DISCLOSURE No Financial conflicts of interest Member of the Wilderness Medical Society Diploma in Mountain Medicine Fellowship in the Academy of Wilderness Medicine
3 Typically when we think hypothermia we imagine

4

5

6

7 ANNA BAGENHOLM
8 HISTORY HYPOTHERMIA IN MEDICINE Hippocrates advocated the packing of wounded solders in Ice and snow Napoleonic war surgeons noted warm officers had worse outcomes than the cold infantryman 1950 s first application in modern medicine during brain surgeries Wikipedia
9 In the 80 s more extensive research into mild hypothermia 32-34C Dog models demonstrated hypothermia had positive effects after brain ischemia. In studies published positive effects of mild hypothermia following cardiac arrest. This has lead to the ILCOR and AHA recommendations of hypothermia after cardiac arrest. Since then numerous studies have demonstrated positive effects of hypothermia following brain injury.
10 PRIMARY VS. SECONDARY HYPOTHERMIA Primary Hypothermia Due to environmental exposure, no underlying medical condition causing disruption of t emperature regulation. Secondary Hypothermia Low body temperature resulting from a medical illness, e.g., trauma. Paramedic Practice Today vol_2-546
11 PRIMARY HYPOTHERMIA DEFINITIONS Cold Stress = >35C Mild hypothermia = 35C 32C Moderate Hypothermia = 32C 28C Severe / Profound hypothermia = <28C (WMS Practice Guidelines for Hypothermia - Wilderness and Environmental Medicine 2015)

12 DiMM Mt. Rainer June 2015
13 INJURY SEVERITY SCORE The Injury Severity Score (ISS) is an anatomical scoring system that provides an overall score for patients with multiple injuries Takes values from 0 75 Severe injury 15+ Trauma.org
14 VALERI ET AL HYPOTHERMIA INDUCED REVERSIBLE PLATELET DYSFUNCTION 1986 Hypothermia played a roll in altering clotting factors (thromboxane b2) Local warming and cooling of the bleeding site changed bleeding times. Cold skin (27C) had significantly increased bleeding times Warming the skin reversed the effects.
15 cold arm / warm arm / normothermic normothermic Cold arm / hypothermic warm arm / hypothermic bleeding time
16 Prior to transfusions attempts should be made to normalize skin and wound temperatures Do not cool wounds with ice/snow to cause vasoconstriction in an attempt to control bleeding.

17 DiMM Mt. Rainer June 2015
18 IF HYPOTHERMIA WORSENS BLEEDING, THEN: Does hypothermia worsen outcome in trauma?
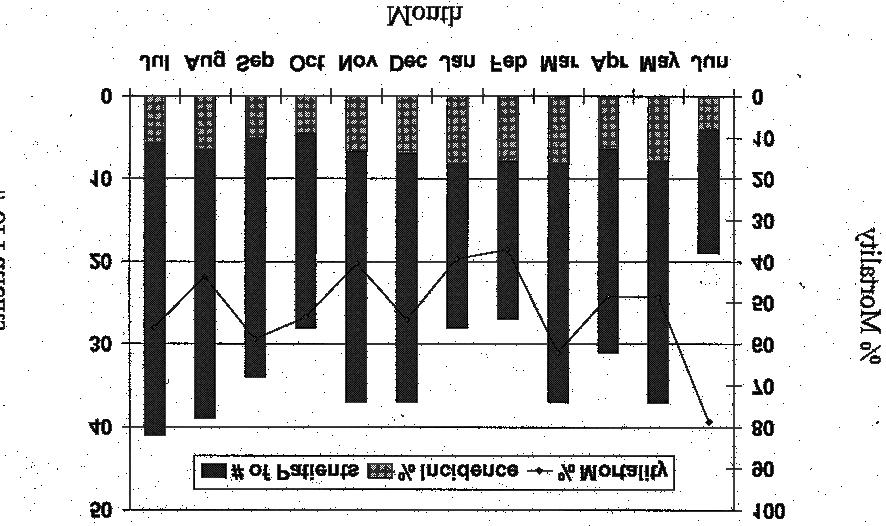
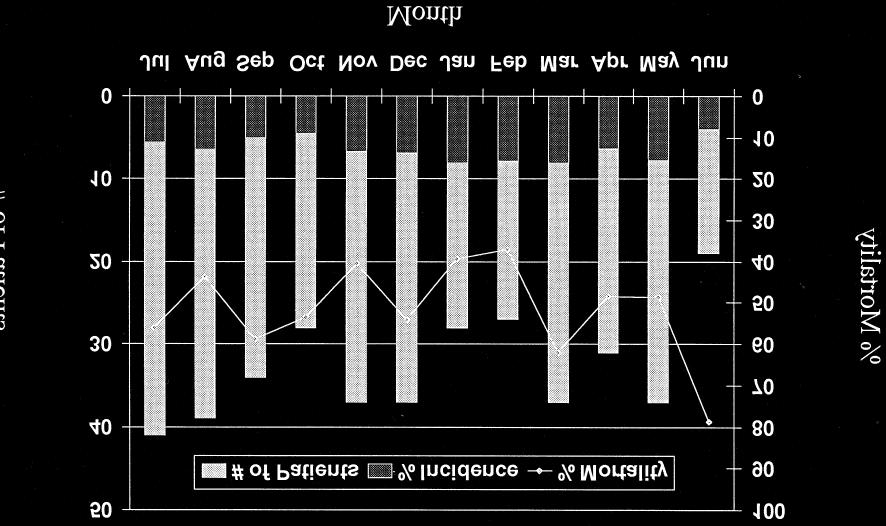
19 JURKOVITCH ET AL HYPOTHERMIA IN TRAUMA VICTIMS: AN OMINOUS PREDICTOR OF SURVIVAL 1987 Study of 71 severely traumatized patients (ISS >24) Increased mortality if temperature <34C 100% mortality temperature <32C regardless of ISS Decrease in core temperature correlated with increase in blood or crystalloid administration (>5 liters)
20 LUNA ET AL INCIDENTS AND EFFECTS OF HYPOTHERMIA IN SERIOUSLY INJURED PATIENTS 1987 Study included intubated patients in ICU 66% (63/94) patients enrolled were hypothermic (<36C) 43% mild and 23% severe
21 Higher trauma scores (ISS) Required more blood Majority of severely injured patients are hypothermic Hypothermia is detrimental to physiology except conditions causing cerebral edema. Severely injured patients are unable to thermoregulate
22 Severely hypothermic patients become hypothermic in the following ways: Alcohol may cause blunting of the vasoconstriction response Immobility trauma causes increases heat loss and decreases heat production Injuries may impair thermoregulation Evaluation, resuscitation, treatments may aggravate heat loss (paralytics / fluids)


23 Courtesy Dr. Brad Bennett PhD NREMT-P

24 DiMM Mt. Rainer June 2015
25 DANZI D, POZOS R. ACCIDENTAL HYPOTHERMIA THE NEW ENGLAND JOURNAL OF MEDICINE Risk factors that can threaten thermostablity : Impaired shivering Inactivity Acute spinal cord transection CNS failure or neurologic abnormalities Pharmacological causes

26 DANZI D, POZOS R. ACCIDENTAL HYPOTHERMIA THE NEW ENGLAND JOURNAL OF MEDICINE CNS trauma Exposure (assessment) Cold infusions Environmental causes Multisystem trauma Shock systemic acidosis
27 WE CAN CAUSE HYPOTHERMIA Exposure of patient during examination Spinal precautions, Analgesia Sedation Kirkpatrick et al 1999

28 DiMM Mt. Rainer June 2015
29 ALL ABOUT NUMBERS Rutherford et al hypothermia in critically ill trauma patients patients ICU admissions 661 were hypothermic (9.1%) Martin et al injury-associated hypothermia: an analysis of the 2004 national trauma databank ,491 National trauma registries cases reviewed. 11,026 were hypothermic (<35C) - 1.5% Shari et al Is hypothermia simply a marker of shock and injury severity or an independent risk factor for mortality in trauma patients? Analysis of a large national trauma registry ,550 patients enrolled 3267 (9.1%) presented with hypothermia (<35C) Wang et al Admission hypothermia and outcome after major trauma ,520 patients enrolled of which 1921 were hypothermic (5%)
30 (Rutherford) Mean temperature of survivors was 34C versus those that died was 33.1C No correlation of seasons. ICU length of stay increased (doubled) Length of ICU stay for survivors was double that of normothermic patients Increase mortality, acidosis, severity of injury, ICU admissions and ventilator days. Morbidity plateaus at 32C
31 Hypothermia is an independent predictor of mortality No apparent protective effect of hypothermia in trauma patients Hypothermia is independently associated with increase mortality and severity of injuries As injury severity increases so does occurrence of hypothermia Aggressive attempts to prevent and treat hypothermia are warranted
32
33
34
35 DEFINITION OF TRAUMATIC HYPOTHERMIA (secondary) Traumatic Hypothermia Normal >36C Mild = 35.9C 34C Moderate = 34C 32C Severe = <32C (primary) Accidental Hypothermia Cold Stress = >35C Mild hypothermia = 35C 32C Moderate Hypothermia = 32C 28C Severe / Profound hypothermia = <28C Arthurs et al WMS Guidelines

36 DiMM Mt. Rainer June 2015
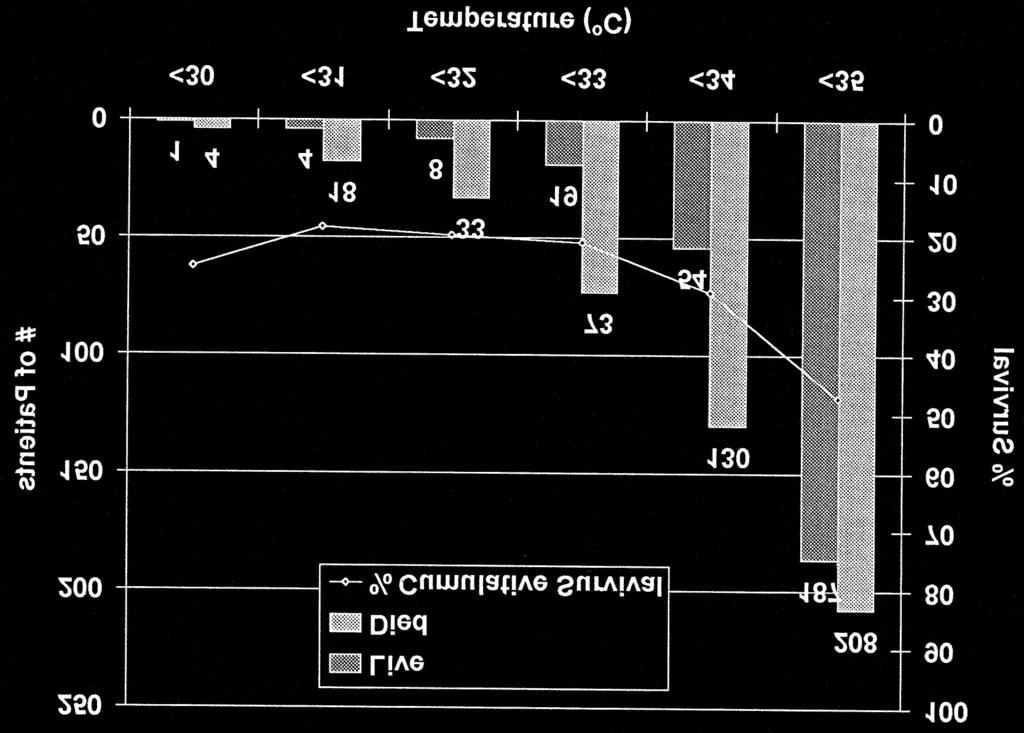
37 ARTHURS ET AL IMPACT OF HYPOTHERMIA ON TRAUMA CARE AT THE 31 ST COMBAT SUPPORT HOSPITAL Demonstrated that 18% of patients were hypothermic Hypothermic patients presented with: lower BP s Tachycardia, hypotension, lower GCS, hemocrits, ph, and high base deficits
38 higher bleeding control surgery, Blood and factor VIIa administration Spent more time in the ICU significantly higher mortality rates Independently, penetrating trauma, GCS <8 or shock (BP<90mmHg) were all predictive of patients arriving hypothermic.
39 89% of hypothermic patients presented with temperatures between 34C 36C Although only 18% of presentations accounted for: 50% of packed blood, 56% of fresh frozen plasma, 60% of whole blood and 63% of factor VIIa use.
40 100% mortality with a temp <33 (similar to Jurkovitch et al) 40% mortality if temperatures were above 33C Using rapid rewarming techniques mortality, fluid requirements and morbidity can be altered.

41 Courtesy Dr. Brad Bennett PhD NREMT-P
42 Application of these (measures) has made it (hypothermia) an uncommon finding. Holcomb J et al The Journal of Trauma Feb 2007
43 WADE ET AL ADMISSION HYPO OR HYPERTHERMIA AND SURVIVAL AFTER TRAUMA IN CIVILIAN AND MILITARY ENVIRONMENTS civilians 382 hypothermic (9.3%) 92 hyperthermic (2.2%) 4394 military 263 hypothermic (6.0%) 327 hyperthermic (7.3%) hypothermia is detrimental in trauma patients hyperthermia (>38C) could also be detrimental to outcome.
44
45 Hypothermia: May occur from many different reasons Mild traumatic hypothermia is as high as 36C Severe traumatic hypothermia is <32C. Effects coagulopathy preventing clot formation Increases ICU stay
46 Hypothermia: Increases blood, blood product and crystalloid administration No correlation to seasons and hypothermia An independent predictor of negative outcome Increases mortality, morbidity in trauma patients Effects may be reversed with warming

47 DiMM Mt. Rainer June 2015
48 HYPOTHERMIA AND ACIDOSIS Metabolic causes of acidosis includes: Lactate generation from shivering and hypoperfusion Impaired hepatic metabolism Impaired acid excretion
49 MARTINI COAGULOPATHY BY HYPOTHERMIA AND ACIDOSIS: MECHANISMS OF THROMBIN GENERATION AND FIBRINOGEN AVAILABILITY 2009 Hypothermia inhibits fibrin generation at the initiation phase Acid imbalance further effects thrombin and increases fibrinogen breakdown. Thrombin generation is thermally regulated Coagulopathy resulting from hypothermia and acidosis is a major contributor to mortality and morbidity in trauma
50 TRIAD OF DEATH Pillars Hypothermia (<35C) Acidosis (<7.1) Coagulopathy (INR > 1.5) In the most severely injured casualties, when the lethal triad are present, death is imminent Bleeding patients with these findings have up to 90% mortality rate. Kirkpatrick A et al Canadian Journal of Surgery 1999 Holcomb J et al The Journal of Trauma 2007 Sayad M et al Emergency medicine International 2013

51 DiMM Mt. Rainer June 2015
52 ACUTE TRAUMATIC COAGULOPATHY Holcomb J. Et al Damage Control Resuscitation: Directly addressing the early coagulopathy of trauma 2007 Firth D. et al Acute Traumatic coagulopathy 2012 Davenport Pathogenesis of acute traumatic coagulopathy
53 Acute Traumatic coagulopathy (ATC) driven by tissue injury and shock (hypoperfusion) Associated with increased mortality and worse outcomes ATC causes Protein C activation which leads to rapid anticoagulation and fibrinolysis Clotting dysfunction begins at the moment of traumatic impact Physiological responses are initiated producing acute traumatic coagulopathy (ATC)
54 Blood samples within 25min of injury found 56% had coagulopathy >3L of crystalloid administration pre-hospital are independently associated with a worse ED coagulation profile ATC is an impairment of all components of haemostasis It is exacerbated by hypothermia, acidosis and fluid resuscitation.
55 ATC is most commonly evident in the presence of tissue hypoperfusion Remoteness may prolong shock, hypothermia and increase volume depletion. This may potentiate ATC or functions independent mechanisms of coagulopathy.
56 My question. In the austere environments is hypothermia treatment as effective as fluid and blood product therapy in severely injured patients?

57 DiMM Mt. Rainer June 2015



58 DETERMINING HYPOTHERMIA
59 KIRKPATRICK ET AL HYPOTHERMIA IN THE TRAUMA PATIENT CANADIAN JOURNAL OF SURGERY It is crucial to accurately measure the body temperature.
60 SAYAD M. ET AL RECENT ADVANCES OF HEMORRHAGE MANAGEMENT IN SEVERE TRAUMA Whilst massive hemorrhage continues to be a major cause of mortality, it is often reversible. It can be managed by early identification and prevention of the lethal triad

61 CLINICAL PRACTICE GUIDELINE: NON-INVASIVE TEMPERATURE MEASUREMENT IN THE EMERGENCY DEPARTMENT Emergency Nurses Association December 2011
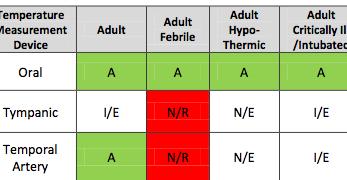
62


63 SHOULD OUT OF HOSPITAL TRAUMA CARE INCLUDE MORE DIAGNOSTIC INSTRUMENTS? I-Stat EG8+ cartridge (or similar) Profound acidosis (<ph 7.1) appears necessary for coagulation dysfunction Davenport 2013

64 DiMM Mt. Rainer June 2015
65 RECOMMENDED TREATMENTS FOR SECONDARY HYPOTHERMIA ATLS guidelines stress temperature control with aggressive efforts to avoid and treat hypothermia - Kirkpatrick et al 1999 Reverse acidosis and prevent hypothermia Holcomb J et al 2007
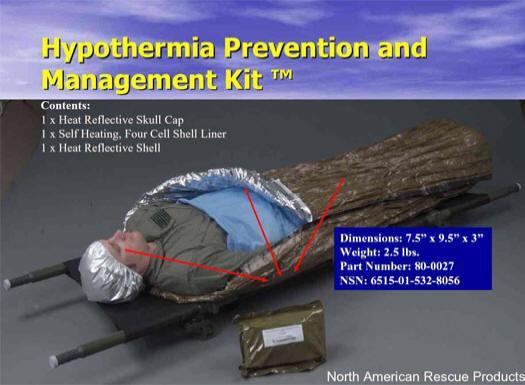
66 HENDRIKSSON ET AL PROTECTION AGAINST COLD IN PREHOSPITAL CARE: WET CLOTHING REMOVAL OR ADDITION OF A VAPOUR BARRIER 2015 in addition to treating life threatening conditions, early application of adequate insulation to prevent cooling is an important part of pre-hospital trauma care. It compares using a single wool blanket to a blanket plus: clothing removal, vapour barrier or second blanket.
67 A wool blanket plus a vapour barrier or 2 nd blanket will: Improve metabolic rate, skin temp, heart rate and cold discomfort. Clothing removal and single warm blanket has similar results except for cold discomfort The extra steps has 15% reduction in metabolic rate which could be significant in trauma/shock

68 DiMM Mt. Rainer June 2015
69 Sayad M. et al ACTIVE VS. PASSIVE Passive warming prevents further heat loss: Covering patients Warming the resuscitation room Active warming involves: Covering with warming blankets Administering warm intravenous fluid
70
71 AHS PROTOCOL
72
73 THE PROBLEM FOR SYMPTOM BASED DETERMINATION OF HYPOTHERMIA IN A TRAUMATIZED PATIENT: Alcohol and TBI may cause hypothalamic dysfunction Which blunts protective vasoconstrictive and shivering responses. Hypotension may also reset hypothalmic set-point for shivering. Paralytics, sedation, spinal injury, ATP depletion Kirkpatrick et al hypothermia in the trauma patient Canadian journal of surgery
74 28C is the ambient temperature in which and unclothed normothermic human will neither gain nor lose heat A severely injured patient should be treated early and aggressively with active rewarming prevent hypothermia (<35C) In this patient population (trauma) external warming methods are only capable of reducing further heat loss. Taylor E. et al 2008 WMS consensus guidelines for the treatment of hypothermia
75 KIRKPATRICK ET AL HYPOTHERMIA IN THE TRAUMA PATIENT CANADIAN JOURNAL OF SURGERY Passive warming should be applied at the scene. Rapid extrication and transport times minimized Best therapy is active rewarming Avoid cold fluids All trauma patients should be treated for hypothermia (passively) Patients who are moderately or severely hypothermic must get actively rewarmed



76

77 Courtesy Dr. Brad Bennett PhD NREMT-P

78 Courtesy Dr. Brad Bennett PhD NREMT-P
79

80 Courtesy Dr. Brad Bennett PhD NREMT-P
81 Courtesy Dr. Brad Bennett PhD NREMT-P

82 DiMM Mt. Rainer June 2015
83 THANK YOU Questions?
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY
 MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
INDUCED HYPOTHERMIA. F. Ben Housel, M.D.
 INDUCED HYPOTHERMIA F. Ben Housel, M.D. Historical Use of Induced Hypothermia 1950 s - Moderate hypothermia (30-32º C) in open heart surgery to protect brain against global ischemia 1960-1980 s - Use of
INDUCED HYPOTHERMIA F. Ben Housel, M.D. Historical Use of Induced Hypothermia 1950 s - Moderate hypothermia (30-32º C) in open heart surgery to protect brain against global ischemia 1960-1980 s - Use of
Coagulopathy: Measuring and Management. Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine
 Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
TRAUMA RESUSCITATION. Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital
 TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
Cold Water Shock, Hypothermia and Cardiac Arrest
 Cold Water Shock, Hypothermia and Cardiac Arrest In spring the warm air temperatures lure hibernating humans out of the house. and the waters beckon. While the air temperature may be 60-80 F, the water
Cold Water Shock, Hypothermia and Cardiac Arrest In spring the warm air temperatures lure hibernating humans out of the house. and the waters beckon. While the air temperature may be 60-80 F, the water
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Massive Transfusion in Pediatric Trauma: Analysis of the National Trauma Databank
 Massive Transfusion in Pediatric Trauma: Analysis of the National Trauma Databank Michelle Shroyer, MPH, Russell Griffin, PhD, Vincent Mortellaro, MD, and Rob Russell MD, MPH Introduction Hemorrhage is
Massive Transfusion in Pediatric Trauma: Analysis of the National Trauma Databank Michelle Shroyer, MPH, Russell Griffin, PhD, Vincent Mortellaro, MD, and Rob Russell MD, MPH Introduction Hemorrhage is
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out?
 and Tranexamic acid (TXA): Is the Jury Still Out?") Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Emergency Preservation and Resuscitation
 Emergency Preservation and Resuscitation Samuel A. Tisherman, MD, FACS, FCCM Director, Center for Critical Care and Trauma Education Director, SICU RA Cowley Shock Trauma Center Disclosures Co-author of
Emergency Preservation and Resuscitation Samuel A. Tisherman, MD, FACS, FCCM Director, Center for Critical Care and Trauma Education Director, SICU RA Cowley Shock Trauma Center Disclosures Co-author of
-Blood Warming- A Hot topic?
 -Blood Warming- A Hot topic? Blaine Kent, MD, FRCPC Associate Professor of Anesthesia Director, Peri-Operative Blood Management Chief, Cardiac Anesthesia Objectives To learn / review the deleterious systemic
-Blood Warming- A Hot topic? Blaine Kent, MD, FRCPC Associate Professor of Anesthesia Director, Peri-Operative Blood Management Chief, Cardiac Anesthesia Objectives To learn / review the deleterious systemic
Adult Trauma Advances in Pediatrics. (sometimes they are little adults) FAST examination. Who is bleeding? How much and what kind of TXA volume?
 FAST examination. Who is bleeding? How much and what kind of TXA volume?") Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Toxins and Environmental: HEAT- and COLD-RELATED EMERGENCIES. Accidental Hypothermia/Cold Exposure
 Toxins and Environmental: HEAT- and COLD-RELATED EMERGENCIES Accidental Hypothermia/Cold Exposure Goal: To aid EMS Providers in: the recognition and treatment of systemic effects of accidental hypothermia
Toxins and Environmental: HEAT- and COLD-RELATED EMERGENCIES Accidental Hypothermia/Cold Exposure Goal: To aid EMS Providers in: the recognition and treatment of systemic effects of accidental hypothermia
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Neurotrauma: The Place for Cooling
 Neurotrauma: The Place for Cooling Cooling: to achieve hypothermia History, evidence, open questions Cooling: to achieve normothermia Evidence, open questions Cooling: Practical Aspects Hypothermia: History
Neurotrauma: The Place for Cooling Cooling: to achieve hypothermia History, evidence, open questions Cooling: to achieve normothermia Evidence, open questions Cooling: Practical Aspects Hypothermia: History
UTSW/BioTel EMS TRAINING BULLETIN January EMS TB Accidental Hypothermia
 UTSW/BioTel EMS TRAINING BULLETIN January 2015 EMS TB 15-001 Accidental Hypothermia Purpose: 1. To provide patient assessment and management guidance to UTSW/BioTel EMS Providers about Accidental Hypothermia
UTSW/BioTel EMS TRAINING BULLETIN January 2015 EMS TB 15-001 Accidental Hypothermia Purpose: 1. To provide patient assessment and management guidance to UTSW/BioTel EMS Providers about Accidental Hypothermia
Ac#ve, ECMO or locally available alterna#ves. invasive warming. Ini#ally: Ac#ve noninvasive or minimally
 Suspected Hypothermia Temp
Suspected Hypothermia Temp
Thicker than Water. Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago
 Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Implementation and execution of civilian RDCR programs Minnesota RDCR
 Implementation and execution of civilian RDCR programs Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General
Implementation and execution of civilian RDCR programs Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors. THOR Collaboration
 Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Massive transfusion: Recent advances, guidelines & strategies. Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad
 Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
*Corresponding author: Key words: neurotrauma, coagulopathy
 COAGULOPATHY IN NEURO TRAUMA A PROSPECTIVE ANALYSIS OF THE INCIDENCE AND CAUSES OF COAGULOPATHY IN PATIENTS WITH PURE NEURO TRAUMA AND MIXED TRAUMA ADMITTED TO THE NATIONAL HOSPITAL SRI LANKA *Jayawickrama
COAGULOPATHY IN NEURO TRAUMA A PROSPECTIVE ANALYSIS OF THE INCIDENCE AND CAUSES OF COAGULOPATHY IN PATIENTS WITH PURE NEURO TRAUMA AND MIXED TRAUMA ADMITTED TO THE NATIONAL HOSPITAL SRI LANKA *Jayawickrama
DAMAGE CONTROL RESUSCITATION
 DAMAGE CONTROL RESUSCITATION Chapter 4 Contributing Authors Jeremy G. Perkins, MD, FACP, LTC, MC, US Army Alec C. Beekley, MD, FACS, LTC, MC, US Army All figures and tables included in this chapter have
DAMAGE CONTROL RESUSCITATION Chapter 4 Contributing Authors Jeremy G. Perkins, MD, FACP, LTC, MC, US Army Alec C. Beekley, MD, FACS, LTC, MC, US Army All figures and tables included in this chapter have
Damage Control Resuscitation
 Damage Control Resuscitation H M Cassimjee Critical Care Specialist Department of Critical Care & Level 1 Trauma Unit Inkosi Albert Luthuli Central Hospital Damage Control Resuscitation only for DAMAGED
Damage Control Resuscitation H M Cassimjee Critical Care Specialist Department of Critical Care & Level 1 Trauma Unit Inkosi Albert Luthuli Central Hospital Damage Control Resuscitation only for DAMAGED
CrackCast Episode 8 Brain Resuscitation
 CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CHILL OUT! Induced Hypothermia: Challenges & Successes in the
 CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
Epidemiology. Case. Pre-Hospital SI and Massive Transfusion
 Epidemiology Preston Maxim, MD Assoc. Professor of Emergency Medicine San Francisco General Hospital ~180,000 deaths 2007 due to trauma 25% trauma patients require 1 unit of PRBC and only 25% of those
Epidemiology Preston Maxim, MD Assoc. Professor of Emergency Medicine San Francisco General Hospital ~180,000 deaths 2007 due to trauma 25% trauma patients require 1 unit of PRBC and only 25% of those
Just like Adults? Evaluating the Impact of Fluid Resuscitation in Pediatric Trauma
 Just like Adults? Evaluating the Impact of Fluid Resuscitation in Pediatric Trauma Abbas PI 1,2, Carpenter K 2, Sheikh F 1,2, Peterson ML 1,2, Kljajic M 1, Naik-Mathuria B 1,2 1 Texas Children s Hospital
Just like Adults? Evaluating the Impact of Fluid Resuscitation in Pediatric Trauma Abbas PI 1,2, Carpenter K 2, Sheikh F 1,2, Peterson ML 1,2, Kljajic M 1, Naik-Mathuria B 1,2 1 Texas Children s Hospital
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient
 Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Mild. Moderate. Severe. 32 to to and below
 Mohamud Daya MD, MS Mild 32 to 34 Moderate 28 to 32 Severe 28 and below Jon Rittenberger Shervin Ayati Protocol Development Committee Hypothermia Working Group Lynn Wittwer Jon Jui John Stouffer Scott
Mohamud Daya MD, MS Mild 32 to 34 Moderate 28 to 32 Severe 28 and below Jon Rittenberger Shervin Ayati Protocol Development Committee Hypothermia Working Group Lynn Wittwer Jon Jui John Stouffer Scott
Mechanisms of Trauma Coagulopathy. Dr B M Schyma Changi General Hospital Singapore
 Mechanisms of Trauma Coagulopathy Dr B M Schyma Changi General Hospital Singapore HAEMORRHAGE A continued cause of PREVENTABLE death. 24% of trauma patients are coagulopathic on arrival 1 56% of severe
Mechanisms of Trauma Coagulopathy Dr B M Schyma Changi General Hospital Singapore HAEMORRHAGE A continued cause of PREVENTABLE death. 24% of trauma patients are coagulopathic on arrival 1 56% of severe
FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
 Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
INDUCED HYPOTHERMIA A Hot Topic. R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences
 INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
Review Article Hypotensive Resuscitation among Trauma Patients
 BioMed Research International Volume 2016, Article ID 8901938, 8 pages http://dx.doi.org/10.1155/2016/8901938 Review Article Hypotensive Resuscitation among Trauma Patients Matthew M. Carrick, 1 Jan Leonard,
BioMed Research International Volume 2016, Article ID 8901938, 8 pages http://dx.doi.org/10.1155/2016/8901938 Review Article Hypotensive Resuscitation among Trauma Patients Matthew M. Carrick, 1 Jan Leonard,
Case Presentation. Cooling. Case Presentation. New Developments in Cardiopulmonary Arrest: Therapeutic Hypothermia in Resuscitation
 New Developments in Cardiopulmonary Arrest: Therapeutic Hypothermia in Resuscitation Michael Sayre, MD Emergency Medicine and LeRoy Essig, MD Pulmonary/Critical Care Medicine Case Presentation 3:40 (+
New Developments in Cardiopulmonary Arrest: Therapeutic Hypothermia in Resuscitation Michael Sayre, MD Emergency Medicine and LeRoy Essig, MD Pulmonary/Critical Care Medicine Case Presentation 3:40 (+
Hemostatic Resuscitation in Trauma. Joanna Davidson, MD 6/6/2012
 Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Cold Injuries: Frostbite and Hypothermia. Michael White MD,FACS Director Detroit Receiving Hospital Wayne State University
 Cold Injuries: Frostbite and Hypothermia Michael White MD,FACS Director Detroit Receiving Hospital Wayne State University Objectives of Talk Describe the incidence and characteristics of Frostbite injury
Cold Injuries: Frostbite and Hypothermia Michael White MD,FACS Director Detroit Receiving Hospital Wayne State University Objectives of Talk Describe the incidence and characteristics of Frostbite injury
TXA. Things Change. Tranexamic Acid TXA. Resuscitation 2017 TXA In The ED March 31, MAST Trousers. High Flow IV Fluids.
 Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Pediatric massive transfusion protocols
 University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
ICU treatment of the trauma patient. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
Emergency Blood and Massive Transfusion: The Surgeon s Perspective. Transfusion Medicine Update September 16 17, 2009
 Transfusion Medicine Update September 16 17, 2009 Mandip S. Atwal, D.O. FACOS Carl M. Pesta, D.O. FACOS Agenda History Hemorrhagic shock Transfusion is Bad Transfusion Prevention Transfusion The Red Chest
Transfusion Medicine Update September 16 17, 2009 Mandip S. Atwal, D.O. FACOS Carl M. Pesta, D.O. FACOS Agenda History Hemorrhagic shock Transfusion is Bad Transfusion Prevention Transfusion The Red Chest
CUTTING EDGE DECOMPRESSION. A new approach to thoracostomy, p. 26. DRUG WAR Medics p. 38 NECK Trauma p. 50 TRAUMA S Lethal Triad p.
 NITROUS Oxide p. 34 DRUG WAR Medics p. 38 NECK Trauma p. 50 TRAUMA S Lethal Triad p. 56 APRIL 2014 CUTTING EDGE DECOMPRESSION A new approach to thoracostomy, p. 26 Always En Route At Hypothermia, acidosis
NITROUS Oxide p. 34 DRUG WAR Medics p. 38 NECK Trauma p. 50 TRAUMA S Lethal Triad p. 56 APRIL 2014 CUTTING EDGE DECOMPRESSION A new approach to thoracostomy, p. 26 Always En Route At Hypothermia, acidosis
Induced Hypothermia for Cardiac Arrest. Heather Hand RN,CCRN,CNRN,ATCN,LNC
 Induced Hypothermia for Cardiac Arrest Heather Hand RN,CCRN,CNRN,ATCN,LNC Cardiac Arrest Epidemiology 400,000 arrests / year in U.S.A 3 / 4 Out-of-hospital 1 / 4 In-hospital survival to hospital 1-5% discharge
Induced Hypothermia for Cardiac Arrest Heather Hand RN,CCRN,CNRN,ATCN,LNC Cardiac Arrest Epidemiology 400,000 arrests / year in U.S.A 3 / 4 Out-of-hospital 1 / 4 In-hospital survival to hospital 1-5% discharge
Instituting preventive warming measures for patients who are normothermic. A variety of measures may be used, unless contraindicated.
 Patient Warmer Perioperative Hypothermia specifies that a preoperative patient management assessment should include: Identification of a patient s risk factors for unplanned perioperative hypothermia Measurement
Patient Warmer Perioperative Hypothermia specifies that a preoperative patient management assessment should include: Identification of a patient s risk factors for unplanned perioperative hypothermia Measurement
Prehospital Care Bundles
 Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Thermoregulation 2015 WMA
 1 Structure: Temperature sensors Endocrine system Muscles Skin Function: Maintain body core at 37 C Problem: Too little heat Too much heat 2 Normal Body Compensation Heat Response: Vasodilation Sweat Cold
1 Structure: Temperature sensors Endocrine system Muscles Skin Function: Maintain body core at 37 C Problem: Too little heat Too much heat 2 Normal Body Compensation Heat Response: Vasodilation Sweat Cold
Hemostatic Resuscitation
 Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Damage control resuscitation from major haemorrhage in polytrauma
 Eur J Orthop Surg Traumatol (2014) 24:137 141 DOI 10.1007/s00590-013-1172-7 GENERAL REVIEW Damage control resuscitation from major haemorrhage in polytrauma William Carlino Received: 27 November 2012 /
Eur J Orthop Surg Traumatol (2014) 24:137 141 DOI 10.1007/s00590-013-1172-7 GENERAL REVIEW Damage control resuscitation from major haemorrhage in polytrauma William Carlino Received: 27 November 2012 /
VanderbiltEM.com. Prehospital STEMIs. EMS Today 2018 Research That Should Be On Your Radar Screen 3/1/2018
 EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
Where Have we Come From, and Where are we Going
 Where Have we Come From, and Where are we Going James Augustine, MD, FACEP Emergency Physician and Fire/EMS Medical Director Naples, Atlanta, and Dayton Clinical Professor, Wright State Univ. Dept of Emergency
Where Have we Come From, and Where are we Going James Augustine, MD, FACEP Emergency Physician and Fire/EMS Medical Director Naples, Atlanta, and Dayton Clinical Professor, Wright State Univ. Dept of Emergency
Pre-hospital Trauma Life Support. Rattiya Banjungam Emergency Physician, Khon Kaen Hospital
 Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Hypothermia in Trauma What happens? Hypothermia in the Trauma Patient. Hypothermia in Trauma 10/6/2010
 Hypothermia in the Trauma Patient Friend or Foe? Clark Hayward EMTP, AWLS 10/2/10 Hypothermia in Trauma What happens? From the time of injury, trauma itself alters the normal central thermoregulation and
Hypothermia in the Trauma Patient Friend or Foe? Clark Hayward EMTP, AWLS 10/2/10 Hypothermia in Trauma What happens? From the time of injury, trauma itself alters the normal central thermoregulation and
High Risk + Challenging Trauma Cases. Hawaii. Topics 1/27/2014. David Thompson, MD, MPH. Head injury in the anticoagulated patient.
 High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
PEDIATRIC MASSIVE TRANSFUSION
 PEDIATRIC MASSIVE TRANSFUSION CHELSEA RUNKLE RN, BSN, CCRN, SRNA CROZER-CHESTER MEDICAL CENTER/VILLANOVA UNIVERSITY NURSE ANESTHESIA PROGRAM LEADING CAUSE OF DEATH Trauma Motor vehicle accidents, nonaccidental
PEDIATRIC MASSIVE TRANSFUSION CHELSEA RUNKLE RN, BSN, CCRN, SRNA CROZER-CHESTER MEDICAL CENTER/VILLANOVA UNIVERSITY NURSE ANESTHESIA PROGRAM LEADING CAUSE OF DEATH Trauma Motor vehicle accidents, nonaccidental
Therapeutic hypothermia
 INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
Patient Case. Post cardiac arrest pathophysiology 10/19/2017. Disclosure. Objectives. Patient Case-TM
 Disclosure TARGETED TEMPERATURE MANAGEMENT POST CARDIAC ARREST I have nothing to disclose concerning possible financial or personal relationships with commercial entities that may have a direct or indirect
Disclosure TARGETED TEMPERATURE MANAGEMENT POST CARDIAC ARREST I have nothing to disclose concerning possible financial or personal relationships with commercial entities that may have a direct or indirect
Factors Contributing to Fatal Outcome of Traumatic Brain Injury: A Pilot Case Control Study
 Factors Contributing to Fatal Outcome of Traumatic Brain Injury: A Pilot Case Control Study D. HENZLER, D. J. COOPER, K. MASON Intensive Care Department, The Alfred Hospital, Melbourne, VICTORIA ABSTRACT
Factors Contributing to Fatal Outcome of Traumatic Brain Injury: A Pilot Case Control Study D. HENZLER, D. J. COOPER, K. MASON Intensive Care Department, The Alfred Hospital, Melbourne, VICTORIA ABSTRACT
Accidental Hypothermia
 Accidental Hypothermia Gordon G. Giesbrecht, Ph.D., Professor Health Leisure and Human Performance Research Institute University of Manitoba, Winnipeg, Manitoba, Canada, R3T 2N2 Learning Objectives: 1)
Accidental Hypothermia Gordon G. Giesbrecht, Ph.D., Professor Health Leisure and Human Performance Research Institute University of Manitoba, Winnipeg, Manitoba, Canada, R3T 2N2 Learning Objectives: 1)
Blood Reviews 23 (2009) Contents lists available at ScienceDirect. Blood Reviews. journal homepage:
 Contents lists available at ScienceDirect. Blood Reviews. journal homepage:") Blood Reviews 23 (2009) 231 240 Contents lists available at ScienceDirect Blood Reviews journal homepage: www.elsevier.com/locate/blre REVIEW Resuscitation and transfusion principles for traumatic hemorrhagic
Blood Reviews 23 (2009) 231 240 Contents lists available at ScienceDirect Blood Reviews journal homepage: www.elsevier.com/locate/blre REVIEW Resuscitation and transfusion principles for traumatic hemorrhagic
Shock. William Schecter, MD
 Shock William Schecter, MD The Cell as a furnace O 2 1 mole Glucose Cell C0 2 ATP 38 moles H 2 0 Shock = Inadequate Delivery of 02 and Glucose to the Cell 0 2 Cell ATP 2 moles Lactic Acid Treatment of
Shock William Schecter, MD The Cell as a furnace O 2 1 mole Glucose Cell C0 2 ATP 38 moles H 2 0 Shock = Inadequate Delivery of 02 and Glucose to the Cell 0 2 Cell ATP 2 moles Lactic Acid Treatment of
Surgical Resuscitation Management in Poly-Trauma Patients
 Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Kristan Staudenmayer, MD Stanford University, Stanford, CA
 Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
NIH Public Access Author Manuscript Blood Rev. Author manuscript; available in PMC 2011 August 22.
 NIH Public Access Author Manuscript Published in final edited form as: Blood Rev. 2009 November ; 23(6): 231 240. doi:10.1016/j.blre.2009.07.003. Resuscitation and transfusion principles for traumatic
NIH Public Access Author Manuscript Published in final edited form as: Blood Rev. 2009 November ; 23(6): 231 240. doi:10.1016/j.blre.2009.07.003. Resuscitation and transfusion principles for traumatic
3/16/15. Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation. Obligatory Traumatologist Slide
 Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Transfusion in major bleeding: new insights. Gert Poortmans
 Transfusion in major bleeding: new insights Gert Poortmans Trauma Cardiac Surgery Major Surgery with ongoing blood loss Burn Surgery Lethal Triad Polytransfusion: definitions Coagulation Coagulopathy of
Transfusion in major bleeding: new insights Gert Poortmans Trauma Cardiac Surgery Major Surgery with ongoing blood loss Burn Surgery Lethal Triad Polytransfusion: definitions Coagulation Coagulopathy of
HYPOTHALAMIC SET POINT HYPOTHALAMIC SET
 Some like it HOT! Revelations in Managing Fever in the ICU. By Vini Bains, RN, BSN, CNCC(C) Vininder.Bains@vch.ca Fever in Critical Illness 1. Normal Thermoregulation 2. Physiology of Fever 3. Costs and
Some like it HOT! Revelations in Managing Fever in the ICU. By Vini Bains, RN, BSN, CNCC(C) Vininder.Bains@vch.ca Fever in Critical Illness 1. Normal Thermoregulation 2. Physiology of Fever 3. Costs and
Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest
 Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest By Meagan Dunn, BScN, MSc,, RN, CNE NP Forum April 8, 2016 Objectives To understand: What Therapeutic Temperature Management (TTM)
Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest By Meagan Dunn, BScN, MSc,, RN, CNE NP Forum April 8, 2016 Objectives To understand: What Therapeutic Temperature Management (TTM)
Hypothermia Presentation
 Hypothermia Presentation Thermoregulation Thermal regulation is a balance between heat production and heat loss. Despite marked changes in skin temperature, the body s homeostatic mechanisms are able to
Hypothermia Presentation Thermoregulation Thermal regulation is a balance between heat production and heat loss. Despite marked changes in skin temperature, the body s homeostatic mechanisms are able to
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
Intraoperative haemorrhage and haemostasis. Dr. med. Christian Quadri Capoclinica Anestesia, ORL
 Intraoperative haemorrhage and haemostasis Dr. med. Christian Quadri Capoclinica Anestesia, ORL Haemostasis is like love. Everybody talks about it, nobody understands it. JH Levy 2000 Intraoperative Haemorrhage
Intraoperative haemorrhage and haemostasis Dr. med. Christian Quadri Capoclinica Anestesia, ORL Haemostasis is like love. Everybody talks about it, nobody understands it. JH Levy 2000 Intraoperative Haemorrhage
PUZZLE. EARLY IMPACT ALS Jamie Syrett, MD Director of Prehospital Care Rochester General Health System PUZZLE THINKING OUTSIDE THE BOX! EARLY IMPACT?
 PUZZLE EARLY IMPACT ALS Jamie Syrett, MD Director of Prehospital Care Rochester General Health System PUZZLE THINKING OUTSIDE THE BOX! EARLY IMPACT? IV ACCESS? What things do we do that make a difference?
PUZZLE EARLY IMPACT ALS Jamie Syrett, MD Director of Prehospital Care Rochester General Health System PUZZLE THINKING OUTSIDE THE BOX! EARLY IMPACT? IV ACCESS? What things do we do that make a difference?
Post-Resuscitation Care: Optimizing & Improving Outcomes after Cardiac Arrest. Objectives: U.S. stats
 Post-Resuscitation Care: Optimizing & Improving Outcomes after Cardiac Arrest Nicole L. Kupchik RN, MN, CCNS CCRN-CMC Clinical Nurse Specialist Harborview Medical Center Seattle, WA Objectives: At the
Post-Resuscitation Care: Optimizing & Improving Outcomes after Cardiac Arrest Nicole L. Kupchik RN, MN, CCNS CCRN-CMC Clinical Nurse Specialist Harborview Medical Center Seattle, WA Objectives: At the
Hypothermia: The Science and Recommendations (In-hospital and Out)
") Hypothermia: The Science and Recommendations (In-hospital and Out) L. Kristin Newby, MD, MHS Professor of Medicine Duke University Medical Center Chair, Council on Clinical Cardiology, AHA President, Society
Hypothermia: The Science and Recommendations (In-hospital and Out) L. Kristin Newby, MD, MHS Professor of Medicine Duke University Medical Center Chair, Council on Clinical Cardiology, AHA President, Society
8/20/12. Discuss the importance of thermoregulation in the neonate.
 Sharon Rush MSN NNP-BC Discuss the importance of thermoregulation in the neonate. To maintain correct body temperature range in order to: Reduce oxygen consumption Reduce calorie expenditure Maximize metabolic
Sharon Rush MSN NNP-BC Discuss the importance of thermoregulation in the neonate. To maintain correct body temperature range in order to: Reduce oxygen consumption Reduce calorie expenditure Maximize metabolic
12/29/2014. IV/IO Therapy & Fluid Administration. Objectives. Cleansing of the soul
 IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
CEDR 2018 QCDR Measures for CMS 2018 MIPS Performance Year Reporting
 ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
Clinical Overview of Coagulation Testing Issues
 Clinical Overview of Coagulation Testing Issues Adam M. Vogel, MD Assistant Professor, Division of Pediatric Surgery Washington University in St. Louis School of Medicine September 19, 2014 Disclosure
Clinical Overview of Coagulation Testing Issues Adam M. Vogel, MD Assistant Professor, Division of Pediatric Surgery Washington University in St. Louis School of Medicine September 19, 2014 Disclosure
EMSS17: Bleeding patients course material
 EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
State of Florida Hypothermia Protocol. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
Accidental Hypothermia
 Accidental Hypothermia Doug Brown, MD, FRCPC Emergency Physician Royal Columbian & Eagle Ridge Hospital October, 2013 Objectives 45min lecture, 15min discussion & questions: Inspirational case & overview
Accidental Hypothermia Doug Brown, MD, FRCPC Emergency Physician Royal Columbian & Eagle Ridge Hospital October, 2013 Objectives 45min lecture, 15min discussion & questions: Inspirational case & overview
WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA?
 WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA? Bryce Robinson MD, MS, FACS, FCCM Associate Professor of Surgery Associate Medical Director, Critical Care Harborview Medical Center Department of Surgery
WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA? Bryce Robinson MD, MS, FACS, FCCM Associate Professor of Surgery Associate Medical Director, Critical Care Harborview Medical Center Department of Surgery
Damage Control Resuscitation:
 American Journal of Clinical Medicine Fall 2011 Volume Eight, Number Three 129 Damage Control Resuscitation: The Case For Early Use of Blood Products and Hypertonic Saline in Exsanguinating Trauma Victims
American Journal of Clinical Medicine Fall 2011 Volume Eight, Number Three 129 Damage Control Resuscitation: The Case For Early Use of Blood Products and Hypertonic Saline in Exsanguinating Trauma Victims
The principle of 1:1:1 blood product use in the resuscitation of trauma victims. K. D. Boffard
 The principle of 1:1:1 blood product use in the resuscitation of trauma victims K. D. Boffard Milpark Hospital Department of Surgery University of the Witwatersrand Johannesburg, South Africa Annual Controversies
The principle of 1:1:1 blood product use in the resuscitation of trauma victims K. D. Boffard Milpark Hospital Department of Surgery University of the Witwatersrand Johannesburg, South Africa Annual Controversies
ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD
 ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD Trauma represents a leading cause of disability and preventable death and is mainly affecting people between 15 and 40 years of age, accounting
ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD Trauma represents a leading cause of disability and preventable death and is mainly affecting people between 15 and 40 years of age, accounting
Hypotensive Resuscitation
 Curr Anesthesiol Rep (2014) 4:209 215 DOI 10.1007/s40140-014-0064-7 ANESTHESIA FOR TRAUMA (J-F PITTET, SECTION EDITOR) Hypotensive Resuscitation Jeremy B. Smith Jean-Francois Pittet Albert Pierce Published
Curr Anesthesiol Rep (2014) 4:209 215 DOI 10.1007/s40140-014-0064-7 ANESTHESIA FOR TRAUMA (J-F PITTET, SECTION EDITOR) Hypotensive Resuscitation Jeremy B. Smith Jean-Francois Pittet Albert Pierce Published
1) According to ILCOR guidelines, to what temperature should patients be cooled? a ºC b ºC c ºC d ºC
 According to ILCOR guidelines, to what temperature should patients be cooled? a ºC b ºC c ºC d ºC") MANAGEMENT OF OUT-OF-HOSPITAL CARDIAC ARRESTS WITH INDUCED HYPOTHERMIA ANAESTHESIA TUTORIAL OF THE WEEK 206 22 ND NOVEMBER 2010 Dr Clare Attwood, Specialist Trainee in Anaesthesia Royal Devon and Exeter
MANAGEMENT OF OUT-OF-HOSPITAL CARDIAC ARRESTS WITH INDUCED HYPOTHERMIA ANAESTHESIA TUTORIAL OF THE WEEK 206 22 ND NOVEMBER 2010 Dr Clare Attwood, Specialist Trainee in Anaesthesia Royal Devon and Exeter
Massive Transfusion in Trauma
 Page 1 Massive Transfusion in Trauma Robert S. Harris, M.D. Atlanta, Georgia Definitions and Demographics Hemorrhage is the second most common cause of death following injury and trauma, and is responsible
Page 1 Massive Transfusion in Trauma Robert S. Harris, M.D. Atlanta, Georgia Definitions and Demographics Hemorrhage is the second most common cause of death following injury and trauma, and is responsible
10/4/2018. Nothing to Disclose. Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO
 Nothing to Disclose Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO History of IV Resuscitation Review of Data for Fluid Strategies Historical Examples of IV
Nothing to Disclose Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO History of IV Resuscitation Review of Data for Fluid Strategies Historical Examples of IV
Geriatric Trauma Resuscitation: Lessons from a Geriatric Trauma Surgeon
 Geriatric Trauma Resuscitation: Lessons from a Geriatric Trauma Surgeon Aurelio Rodriguez, M.D., FACS Conemaugh Memorial Medical Center Trauma Center Johnstown, PA Demographics The fastest growing age
Geriatric Trauma Resuscitation: Lessons from a Geriatric Trauma Surgeon Aurelio Rodriguez, M.D., FACS Conemaugh Memorial Medical Center Trauma Center Johnstown, PA Demographics The fastest growing age
DOCTORS AMPUTATE FROSTBITTEN FEET OFALL-AMERICAN RUNNER
 DOCTORS AMPUTATE FROSTBITTEN FEET OFALL-AMERICAN RUNNER This tragic recent headline involving Marco Cheseto serves as a grim reminder of the potential devastation inflicted by frostbite and hypothermia
DOCTORS AMPUTATE FROSTBITTEN FEET OFALL-AMERICAN RUNNER This tragic recent headline involving Marco Cheseto serves as a grim reminder of the potential devastation inflicted by frostbite and hypothermia
Therapeutic Hypothermia ANZCA 2013
 Therapeutic Hypothermia ANZCA 2013 Stephen Bernard MD Therapeutic Hypothermia-Indications Anoxic brain injury (cardiac arrest) Severe traumatic brain injury Spinal cord injury Why not Therapeutic Hypothermia?
Therapeutic Hypothermia ANZCA 2013 Stephen Bernard MD Therapeutic Hypothermia-Indications Anoxic brain injury (cardiac arrest) Severe traumatic brain injury Spinal cord injury Why not Therapeutic Hypothermia?
The cold never bother me anymore. R2 Wariya Vongchaiudomchoke & R2 Pichchaporn Praserdvigai Supervisor: Aj. Aphichat Suphathamwit
 The cold never bother me anymore R2 Wariya Vongchaiudomchoke & R2 Pichchaporn Praserdvigai Supervisor: Aj. Aphichat Suphathamwit Is that really true? Frozen by Walt Disney Animation Studios, 2013 Definition
The cold never bother me anymore R2 Wariya Vongchaiudomchoke & R2 Pichchaporn Praserdvigai Supervisor: Aj. Aphichat Suphathamwit Is that really true? Frozen by Walt Disney Animation Studios, 2013 Definition
THERAPEUTIC HYPOTHERMIA POST CARDIAC ARREST
 THERAPEUTIC HYPOTHERMIA POST CARDIAC ARREST Heather Harrington RN, BScN, CNCC(c) Clinical Nurse Educator Sunnybrook Health Sciences Centre Objectives Define Therapeutic Hypothermia (TH) Describe current
THERAPEUTIC HYPOTHERMIA POST CARDIAC ARREST Heather Harrington RN, BScN, CNCC(c) Clinical Nurse Educator Sunnybrook Health Sciences Centre Objectives Define Therapeutic Hypothermia (TH) Describe current
HEAT STROKE. Lindsay VaughLindsay Vaughn, DVM, DACVECCDVM, DACVECC
 HEAT STROKE Lindsay VaughLindsay Vaughn, DVM, DACVECCDVM, DACVECC Heat Stroke More Preventable Than Treatable Heat Stroke A form of hyperthermia associated with a systemic inflammatory response leading
HEAT STROKE Lindsay VaughLindsay Vaughn, DVM, DACVECCDVM, DACVECC Heat Stroke More Preventable Than Treatable Heat Stroke A form of hyperthermia associated with a systemic inflammatory response leading
Effect of post-intubation hypotension on outcomes in major trauma patients
 Effect of post-intubation hypotension on outcomes in major trauma patients Dr. Robert S. Green Professor, Emergency Medicine and Critical Care Dalhousie University Medical Director, Trauma Nova Scotia
Effect of post-intubation hypotension on outcomes in major trauma patients Dr. Robert S. Green Professor, Emergency Medicine and Critical Care Dalhousie University Medical Director, Trauma Nova Scotia
Does a Controlled Fluid Resuscitation Strategy Decrease Mortality in Trauma Patients?
 Does a Controlled Fluid Resuscitation Strategy Decrease Mortality in Trauma Patients? death Haemorrhage remains the biggest killer of major trauma patients Expected deaths will increase to 8 million/year
Does a Controlled Fluid Resuscitation Strategy Decrease Mortality in Trauma Patients? death Haemorrhage remains the biggest killer of major trauma patients Expected deaths will increase to 8 million/year