Implementation and execution of civilian RDCR programs Minnesota RDCR
|
|
|
- Brian Parsons
- 5 years ago
- Views:
Transcription

1 Implementation and execution of civilian RDCR programs Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General Surgery Saint Marys Hospital, Rochester MN June 2013

2 Remote Damage Control: Civilian Experience in the Pre-Hospital Setting No Disclosures
3 Objectives Indications for treatment with blood products for traumatic hemorrhagic shock in the pre-hospital setting Monitoring devices used for coagulopathy and shock Therapeutics utilized in these patients for pre-hospital treatment of casualties Evacuations of long durations compared to rapid ones Methods of implementation to improve rapid incorporation of recently initiated changes in practice

4 Remote Damage Control Resusc Austere/rural environment patients Modified transfusion strategy Different than those with scene/pre-hospital time < 30 minutes Limited resources available Lack of plasma availability 40% of the population, 60% of the trauma mortality Current treatment options for uncontrolled hemorrhage in this environment are very limited >75% of combat fatalities occur in the field
5 Hartford Consensus February 2013 Leaders in law enforcement, EMS, military and the American College of Surgeons Recommendations for civilian organizations to improve survival during active shooter scenarios Stress the importance of early and definitive hemorrhage control to maximize survival in the victims.
6 Hartford Consensus THREAT T - Threat suppression H - Hemorrhage Control RE - Rapid Extraction to safety, A - Assessment by medical providers T - Transport to definitive care




7
8 Coagulopathy on Presentation An initial INR 1.5 reliably predicts those military casualties who will require MT. Pts who have a significant injury present with a coagulopathy. Severity of injury and mortality is linearly associated with the degree of the initial coagulopathy. - Schreiber MA, Perkins JP, Kiraly L, Underwood SJ, Wade CE, Holcomb JB. Early Predictors of Massive Transfusion in Combat Casualties. Submitted, J Trauma. - Brohi K, et al. Acute traumatic coagulopathy. J Trauma
9 Background MacLeod JBA et al. Early Coagulopathy Predicts Mortality in Trauma J Trauma 2003 Brohi K et al. Acute Traumatic Coagulopathy J Trauma 2003 By the time of arrival at the ED, 28% (2,994 of 10,790) of trauma patients had a detectable coagulopathy that was associated with poor outcome

10 Background Mortality was associated with worse Plasma Deficit & The efficacy of the Plasma Repletion occurs within hours de Biasi et al. Early Coagulopathy Predicts Mortality in Trauma Transfusion (Epub, Accepted 2010)


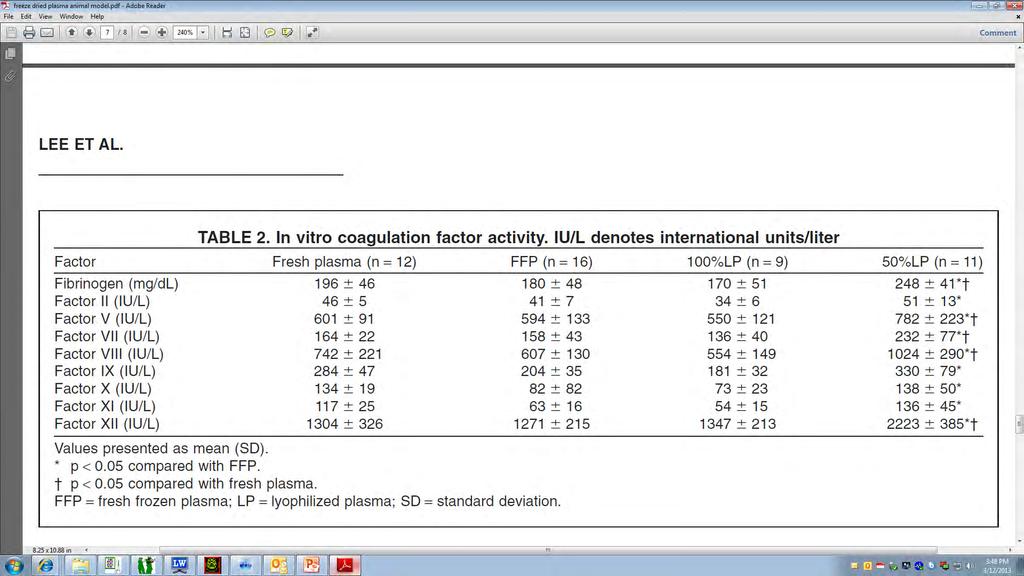
11 DoD Learned About Thawed Plasma Thawed plasma is FFP that is kept for up to 5 days at 4 C This product should be present upon arrival of the casualty in the ED should be used as a primary resuscitative fluid started in the ED This approach not only addresses the metabolic abnormality of shock, but initiates reversal of the coagulopathy present in the ED. Thawed plasma is used in theater The DoD Level 1 trauma center uses this product Decreases waste by 60-70% - Malone DL, Hess JR, Fingerhut A. Comparison of practices around the globe and suggestion for a massive transfusion protocol. J Trauma, Armand R, Hess JR. Treating coagulopathy in trauma patients. Transfus Med Rev 2003.


12 Early Use of Blood in the Prehospital Setting Mayo Clinic Experience retrospective review Criteria: Hgb<10, shock, hypotension after resuscitation ~2100 helicopter flights, 94 patients received PRBC s (4%, 91% interfacility transfer) 48% trauma patients, 25% GI bleed, 38% AAA Hgb increased from 8.9 to 10.2 after 2 PRBC No transfusion reactions or complications Average 12 u PRBC after admision Age of RBC is < 14 days Air Med J 1998 Zietlow and Berns

13 Age of Blood and Procoagulant Microparticles Historically, PCMP increases with age of blood 52 trauma patients vs 22 volunteers Higher PCMP with injury; no difference between transfused (n=19)/not transfused 24 hour PCMP decreased with transfusion No decrease if no transfusion Difference widened with increasing transfusion Spinella Crit Care 2009 Jy Transfusion 2011 Rubin Transfusion

14 Catchment Area

15 Rationale Coagulopathy & the Golden Hour Trauma Induced Coagulopathy (TIC) predicts mortality Plasma and RBC resuscitation should occur early in the hemorrhagic / coagulopathic pt Catchment area / Rural location provides geographic obstacles Regional plasma deficiency
16 Protocol ED Phase Thawed Plasma Program Developed in Feb 2008 with input from: - Blood Bank Team - Transfusion Medicine - Medical Transport - Trauma, Critical Care and General Surgery Initial 9 months were restricted to in-hospital Emergency Department use Medical and Surgical emergencies - Safety concerns - Utilization of resources
17 Product immediately available in the Trauma Resuscitation Area: - 4 units thawed plasma (A+) - 4 units PRBCs (0 negative) Order of transfusion for trauma patients was: 2 units PRBC 2 units thawed Plasma 2 units PRBC 2 units thawed Plasma

 2. Tachycardia (single reading of heart rate 120) 3.")

18 Protocol Helicopter Phase Indications for PRBC and Plasma administration in adult trauma patients prbc + Plasma 1. Hypotension (single reading of systolic blood pressure < 90mmHg) 2. Tachycardia (single reading of heart rate 120) 3. Penetrating mechanism 4. Point of care lactate 5.0 mg/dl 5. Point of care INR 1.5 Plasma Alone 1. Point of care INR Stable Hemodynamics


19


20 Waste Prevention Division of Transfusion Medicine monitors usage - Thawed plasma is removed from the satellite blood refrigerator on Day #3 and sent to the Operating Theater for immediate use.
21 Mayo Helicopter Transfusion Criteria

22 5 for hemorrhage RESULTS 10 TRAUMA PATIENTS TRANSFUSED IN FLIGHT 2/2009 9/ required massive transfusion (> 10 units/24 hours) 5 pts transfused for history of trauma and coumadin use All 4 deaths were in this group All pts entered into protocol required ongoing blood product transfusion after arrival to the hospital.



")




23 Trauma Patients (n=10) Age (years) Male ISS LOS (days) Mortality 71.5 [ ] 8/ [ ] 4.5 [ ] 4/10
24 Admission Laboratory Values Coumadin 5/10 (50%) Lactate 2.8 [ ] Base -4.1 [ ] PLT 149 [ ] PTT 30 [28-42] HgB 10.8 [ ] Post-Flight INR 1.6 [ ] Pre-Flight INR 2.7 [ ]

25 Feasibility Excellent utilization No discarded units of plasma to date No transfusion reactions documented to date; use of product parallels massive transfusion in the standard setting

26 Protocol Evolution During the study period, total of 771 flights Only two pts received all 4 units of PRBC during transport Product Order and Ratio 2009: 2 PRBC, 2 Plasma, 2 PRBC 2010: 2 Plasma, 2 PRBC, 2 PRBC 2011: 3 Plasma, 3 PRBC
27 Hemostatic Resuscitation in Our Trauma Center Pre-hospital plasma and POC testing INR/Lactate pre-hospital Early Diagnosis in ED StO2/i-Stat 1:1 ratio (thawed plasma to RBC) Plasma-first transfusion sequence ED use of PCC? Frequent TEG and early platelet use Minimal crystalloid Repeated doses of PCC and/or transfusion in OR and ICU as required by TEG Young red cells (<14 days)
28 Ratios / Plasma Balance PTP (n=9) Control (n=50) p En Route P:RBC 1.3 : 1.0 N/A < min P:RBC 1.3 : : 1.0 < hr P:RBC 1.0 : : 1.0 < hr P:RBC 1.0 : : 1.0 <0.001 En Route Plasma Deficit min Plasma Deficit hr Plasma Deficit hr Plasma Deficit
29 Time & the Geographic Plasma Deficit PTP (n=9) Control (n=50) p Facility Transfer 100% 54% Transport à Trauma Ctr (min) Injury à First Plasma (min) Trauma Ctr arrivalà Plasma (min)

30 Inaba K et al. Arch Surg 2010 Group A Plasma Transfusion Introduction ABO-identical preferred Universal plasma donor Group AB Lacks anti-a/anti-b Pan-ABO compatible Rarest blood group

31 Isaak EJ et al. Immunohematology 2011 Josephson CD et al. Transfus Apher Sci 2010 Group A Plasma Transfusion Group AB supply Recent safety data ABO incompatible platelets 1 2 plasma units 1 in 9000 hemolysis Group O Immunosuppression
32 Group A Plasma Transfusion Results 10,206 patients over study period Trauma patient July 2008 June unit emergency release plasma (group A plasma) 258 emergency release plasma (2.5%) 4 died prior to blood grouping



")
33 Group A Plasma Transfusion Results 254 patients 35 ABO Incompatible (14%) 25 group B 10 group AB 219 ABO Compatible (86%) 116 group A 103 group O
34 Group A Plasma Transfusion Results Feature ABO Incompatible n = 35 ABO compatible n = 219 P Age (years) 56 (39-79) 59 (32-79) Male sex 63% 63% ISS 25 (16-37) 22 (12-30) TRISS 0.86 ( ) 0.93 ( ) Scene transfer 34% 38% Time from injury to trauma bay admission (mins) 145 (54-185) 172 (92-230) Time in trauma bay (mins) 24 (20-35) 26.5 (20-36) Time at referring hospital 119 (96-144) 121 (70-172) 0.920
35 Group A Plasma Transfusion Results ABO Incompatible n = 35 ABO compatible N = 219 P Ventilator days 6 (2-12) 3 (2-8) ICU LOS (days) 4 (1-11) 3 (1-7) Hospital LOS (days) 9 (3-24) 7 (3-17) Complications 43% 35% ALI 3.7% 2.5% Possible TRALI 2.9% 3.0% ARDS 2.9% 1.8% Pneumonia 17% 9% DVT 2.9% 4.1% 1.00 PE 5.8% 7.3% 1.00 Acute renal failure 0% 1.8% Mortality Sepsis 0% 0.5% % 22% 0.798
36 Group A Plasma Transfusion Results ABO Incompatible n = 35 ABO compatible N = 219 P Ventilator days 6 (2-12) 3 (2-8) ICU LOS (days) 4 (1-11) 3 (1-7) Hospital LOS (days) 9 (3-24) 7 (3-17) Complications 43% 35% ALI 3.7% 2.5% Possible TRALI 2.9% 3.0% ARDS 2.9% 1.8% Pneumonia 17% 9% DVT 2.9% 4.1% 1.00 PE 5.8% 7.3% 1.00 Acute renal failure 0% 1.8% Mortality Sepsis 0% 0.5% % 22% 0.798
37 Group A Plasma Transfusion Results ABO Incompatible n = 35 ABO compatible N = 219 P Ventilator days 6 (2-12) 3 (2-8) ICU LOS (days) 4 (1-11) 3 (1-7) Hospital LOS (days) 9 (3-24) 7 (3-17) Complications 43% 35% ALI 3.7% 2.5% Possible TRALI 2.9% 3.0% ARDS 2.9% 1.8% Pneumonia 17% 9% DVT 2.9% 4.1% 1.00 PE 5.8% 7.3% 1.00 Acute renal failure 0% 1.8% Mortality Sepsis 0% 0.5% % 22% 0.798
38 Group A Plasma Transfusion Results Product ABO Incompatible N = 35 ABO compatible N = 219 P Emergency release plasma (units) 2 (1-4) 2 (1-4) Total Incompatible Units 3 (2-4) 0 (0-0) <0.001 Total compatible 24 hours Total 24 hours (units) 2 (0-6) 3 (2-6) (3-10) 4 (2-7) Total 24 hours (units) 5 (0-12) 4 (0-8) hours 1.3:1 1.1: Plasma 24 hours 2 (0-3) 1 ( - 1-3) Total Platelet 24 hours 0 (0-2) 0 (0-1) 0.801
39 Group A Plasma Transfusion Results Product ABO Incompatible N = 35 ABO compatible N = 219 P Emergency release plasma (units) 2 (1-4) 2 (1-4) Total Incompatible Units 3 (2-4) 0 (0-0) <0.001 Total compatible 24 hours Total 24 hours (units) 2 (0-6) 3 (2-6) (3-10) 4 (2-7) Total 24 hours (units) 5 (0-12) 4 (0-8) hours 1.3:1 1.1: Plasma 24 hours 2 (0-3) 1 ( - 1-3) Total Platelet 24 hours 0 (0-2) 0 (0-1) 0.801
40 Group A Plasma Transfusion Results Product ABO Incompatible N = 35 ABO compatible N = 219 P Emergency release plasma (units) 2 (1-4) 2 (1-4) Total Incompatible Units 3 (2-4) 0 (0-0) <0.001 Total compatible 24 hours Total 24 hours (units) 2 (0-6) 3 (2-6) (3-10) 4 (2-7) Total 24 hours (units) 5 (0-12) 4 (0-8) hours 1.3:1 1.1: Plasma 24 hours 2 (0-3) 1 ( - 1-3) Total Platelet 24 hours 0 (0-2) 0 (0-1) 0.801


41 Group A Plasma Transfusion Discussion Emergency plasma use is increasing Limited access New universal donor resulted in 97.6% reduction in AB plasma use


42 Group A Plasma Transfusion Discussion Group A plasma has equivalent outcomes to group AB Incompatible transfusions occurred No hemolytic reactions Similar mortality Similar immunogenic complications Limitations Small comparison group Type II error potential




43 CRASH-2 Study Lancet, Online Article, 2010 Prospective, randomized controlled trial 20,211 patients TXA significantly reduced all cause mortality from 16.0% to 14.5% TXA significantly reduced death due to bleeding from 5.7% to 4.9% 43
44 44
45 45
46

47 StO2

48 Beilman Study Over a 15-month period, seven Level I trauma centers in the USA enrolled 383 patients, 50 of whom developed MODS StO2 below 75% indicates serious hypoperfusion in trauma patients 78% of patients who developed MODS, and 91% of patients who died, had StO2 below 75% in the first hour Trauma patients who maintained StO2 above 75% within the first hour had an 88% chance of MODS-free survival J Trauma 2006
49 Can early StO2 predict the need of blood product requirement in trauma population? Total 632 level 1 trauma 325 patients with recorded StO2


 Heart rate,")
50 Scene Assessment Variable StO2< 65 n=23 StO2>65 n=302 p Systolic blood pressure, (SD) Heart rate, (SD) NS NS
 0.23 Heart rate, (SD) 0.")
 36.1 (1.2) 36.6 (0.")
51 Emergency Department Assessment Variable StO2< 65 n=23 StO2>65 n=302 Systolic blood pressure, (SD) 0.23 Heart rate, (SD) 0.39 Respiratory rate, (SD) 0.06 O2 saturation, (SD) 0.2 Temperature, (SD) 36.1 (1.2) 36.6 (0.7) Trauma score, (SD) 9 (2) 10 (2) Glasgow coma score, (SD) 7.7 (6) 10 (6) p
52 Laboratory Results and FAST Variable StO2< 65 n=23 StO2>65 n=302 p Hemoglobin, (SD) Hematocrit, (SD) ph, (SD) Base deficit, (SD) Lactate, (SD) 3.9 (3.2) 2.4 (2.1) FAST done Positive FAST NS NS NS NS NS NS
53 Outcomes Variable StO2< 65 N=23 StO2>65 N=302 p ICU days, (SD) Hospital length of stay, (SD) Mortality Surgical interven.on 18 (78%) 152 (50%) Morbidity 11 (48%) 68 (23%) NS NS NS
54 Multivariate analysis Variable StO2 < 65% 0.01 Systolic BP 0.11 Heart rate 0.97 O2 satura.on 0.91 Lactate level 0.25 Age 0.32 ISS 0.33 GCS 0.74 Posi.ve FAST 0.19 p
55 Current Status All 3 Mayo helicopter bases carrying 3 PRBC and 3 thawed plasma All 3 use same transfusion triggers All 3 use i-stat INR and ABG cartridges All 3 carry TXA; uses similar triggers but has some limitations for use Just added StO2 as a trigger Limited waste at all 3 sites No crystalloid for those with hemorrhage Tourniquets and Combat Gauze on all 3 ships
56 The Future Freeze dried plasma? Whole blood? Platelets? Prothrombin complex concentrates?


57 Why Freeze Dried Plasma? Remote Damage Control Resuscitation!
58

59 Implementation of Change Consensus Review of the literature and our own data Practicality and safety are first order of business with best interest of patient in mind Continuous monitoring of program Education of all health care providers Willingness of blood bank and transfusion medicine to consider novel use of products
 Observed decline open abdomen (under study) Observed decline in massive tx (under study) Arrival TEG improved?")
60 Overall System Results Current era (2011) compared to the era before pre-hospital plasma Referrals up (838 vs 998*) ISS up (9 vs 12*) Mortality same (2.5% vs 2.2%) Observed decline open abdomen (under study) Observed decline in massive tx (under study) Arrival TEG improved? (under study)

61 Summary Trauma patients die from shock Our job is to limit preventable trauma death First, identify the patient in shock Pre-hospital resuscitation with plasma can prevent the trauma induced coagulopathy and limit the risk of death due to hemorrhage Making dried plasma available in the rural and pre-hospital/austere environment will save lives

62 Thank You!



63 Questions?
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out?
 and Tranexamic acid (TXA): Is the Jury Still Out?") Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Coagulopathy: Measuring and Management. Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine
 Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors. THOR Collaboration
 Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
3/16/15. Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation. Obligatory Traumatologist Slide
 Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Hemostatic Resuscitation in Trauma. Joanna Davidson, MD 6/6/2012
 Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
Kay Barrera MD. Surgery Grand Rounds June 19, 2014 SUNY Downstate
 Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Outline Why are we talking about this SCORE expectations When do we use
Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Outline Why are we talking about this SCORE expectations When do we use
TXA. Things Change. Tranexamic Acid TXA. Resuscitation 2017 TXA In The ED March 31, MAST Trousers. High Flow IV Fluids.
 Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department
 Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure
Transfusion Pitfalls. Objectives. Packed Red Blood Cells. TRICC trial (subgroups): Is transfusion always good? Components
: Is transfusion always good? Components") Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Strategies to Enhance Plasma Availability
 Strategies to Enhance Plasma Availability Andrew Bernard, MD Professor of Surgery Medical Director, Acute Care Surgery and Trauma Chief, Section on Trauma and Acute Care Surgery Paul A. Kearney, MD Endowed
Strategies to Enhance Plasma Availability Andrew Bernard, MD Professor of Surgery Medical Director, Acute Care Surgery and Trauma Chief, Section on Trauma and Acute Care Surgery Paul A. Kearney, MD Endowed
Transfusion 2004: Current Practice Standards. Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service
 SBB SWMC Transfusion Service") Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
High Risk + Challenging Trauma Cases. Hawaii. Topics 1/27/2014. David Thompson, MD, MPH. Head injury in the anticoagulated patient.
 High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
1/16/2014 NONE WILL BE TALKING ABOUT NON FDA APPROVED DRUGS WILL LET YOU KNOW WHEN NOT ENDORSING ANY PARTICULAR PIECE OF EQUIPMENT
 CUTTING EDGE TACTICAL MEDICINE SECRETS FROM THE BATTLEFIELD Brendan Anzalone, DO, Maj, USAF, MC Emergency Physician Special Tactics Medicine USAF Special Operations Surgical/Critical Care Evacuation Team
CUTTING EDGE TACTICAL MEDICINE SECRETS FROM THE BATTLEFIELD Brendan Anzalone, DO, Maj, USAF, MC Emergency Physician Special Tactics Medicine USAF Special Operations Surgical/Critical Care Evacuation Team
No Disclosures OBJECTIVES. Damage Control Resuscitation Lessons Learned and the Way Forward After More Than a Decade of War
 Damage Control Resuscitation Lessons Learned and the Way Forward After More Than a Decade of War No Disclosures COL(ret) Michael M. Woll, MD, FACS Surgical Det. A, 249 th General Hospital 28 th Combat
Damage Control Resuscitation Lessons Learned and the Way Forward After More Than a Decade of War No Disclosures COL(ret) Michael M. Woll, MD, FACS Surgical Det. A, 249 th General Hospital 28 th Combat
Epidemiology. Case. Pre-Hospital SI and Massive Transfusion
 Epidemiology Preston Maxim, MD Assoc. Professor of Emergency Medicine San Francisco General Hospital ~180,000 deaths 2007 due to trauma 25% trauma patients require 1 unit of PRBC and only 25% of those
Epidemiology Preston Maxim, MD Assoc. Professor of Emergency Medicine San Francisco General Hospital ~180,000 deaths 2007 due to trauma 25% trauma patients require 1 unit of PRBC and only 25% of those
HYPOTHERMIA IN TRAUMA. Kevin Palmer EMT-P, DiMM
 HYPOTHERMIA IN TRAUMA Kevin Palmer EMT-P, DiMM DISCLOSURE No Financial conflicts of interest Member of the Wilderness Medical Society Diploma in Mountain Medicine Fellowship in the Academy of Wilderness
HYPOTHERMIA IN TRAUMA Kevin Palmer EMT-P, DiMM DISCLOSURE No Financial conflicts of interest Member of the Wilderness Medical Society Diploma in Mountain Medicine Fellowship in the Academy of Wilderness
WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA?
 WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA? Bryce Robinson MD, MS, FACS, FCCM Associate Professor of Surgery Associate Medical Director, Critical Care Harborview Medical Center Department of Surgery
WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA? Bryce Robinson MD, MS, FACS, FCCM Associate Professor of Surgery Associate Medical Director, Critical Care Harborview Medical Center Department of Surgery
Hemostatic Resuscitation
 Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Surgical Resuscitation Management in Poly-Trauma Patients
 Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference
 Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference John A. Aucar, MD, MSHI, FACS, CPE EmCare Acute Care Surgery Del Sol Medical Center Associate Professor, University
Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference John A. Aucar, MD, MSHI, FACS, CPE EmCare Acute Care Surgery Del Sol Medical Center Associate Professor, University
Damage Control Resuscitation
 Damage Control Resuscitation H M Cassimjee Critical Care Specialist Department of Critical Care & Level 1 Trauma Unit Inkosi Albert Luthuli Central Hospital Damage Control Resuscitation only for DAMAGED
Damage Control Resuscitation H M Cassimjee Critical Care Specialist Department of Critical Care & Level 1 Trauma Unit Inkosi Albert Luthuli Central Hospital Damage Control Resuscitation only for DAMAGED
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY
 MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
10/4/2018. Nothing to Disclose. Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO
 Nothing to Disclose Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO History of IV Resuscitation Review of Data for Fluid Strategies Historical Examples of IV
Nothing to Disclose Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO History of IV Resuscitation Review of Data for Fluid Strategies Historical Examples of IV
Recombinant Activated Factor VII: Useful. Department of Surgery Grand Rounds 11/8/10 David Mauchley MD
 Recombinant Activated Factor VII: Useful Department of Surgery Grand Rounds 11/8/10 David Mauchley MD Hemostasis and Coagulation Traditional cascade model Two convergent pathways Series of proteolytic
Recombinant Activated Factor VII: Useful Department of Surgery Grand Rounds 11/8/10 David Mauchley MD Hemostasis and Coagulation Traditional cascade model Two convergent pathways Series of proteolytic
Massive Transfusion Initiation & Implication
 Massive Transfusion Initiation & Implication Katayoun Fayaz MD Blood Bank Medical Director Northwell Health April 2017 Trauma Statistics/Facts Each year trauma accounts for 41 million emergency department
Massive Transfusion Initiation & Implication Katayoun Fayaz MD Blood Bank Medical Director Northwell Health April 2017 Trauma Statistics/Facts Each year trauma accounts for 41 million emergency department
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
2/2/2011. Blood Components and Transfusions. Why Blood Transfusion?
 Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
 Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Massive transfusion: Recent advances, guidelines & strategies. Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad
 Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
2 Liters. Goal: Basic Algorithm Volume Resuscitation in Trauma. Initial Fluids. Blood. Where do Blood Products Come From?
 Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
Novel Resuscitation Strategies
 Novel Resuscitation Strategies Hasan B Alam, MD Norman Thompson Professor of Surgery Head of General Surgery University of Michigan Case 2005 27 yrs old male. GSW x3, 10 min transport time SBP 70, HR 130,
Novel Resuscitation Strategies Hasan B Alam, MD Norman Thompson Professor of Surgery Head of General Surgery University of Michigan Case 2005 27 yrs old male. GSW x3, 10 min transport time SBP 70, HR 130,
Heme (Bleeding and Coagulopathies) in the ICU
 in the ICU") Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
EVIDENCE BASED RED CELL TRANSFUSION. Rana Samuel, MD DIRECTOR, PATHOLOGY AND LABORATORY MEDICINE VA WNY Health Care System
 EVIDENCE BASED RED CELL TRANSFUSION Rana Samuel, MD DIRECTOR, PATHOLOGY AND LABORATORY MEDICINE VA WNY Health Care System HISTORY Blood transfusion works (ie: red cell transfusion saves lives). based on
EVIDENCE BASED RED CELL TRANSFUSION Rana Samuel, MD DIRECTOR, PATHOLOGY AND LABORATORY MEDICINE VA WNY Health Care System HISTORY Blood transfusion works (ie: red cell transfusion saves lives). based on
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
NIH Public Access Author Manuscript Blood Rev. Author manuscript; available in PMC 2011 August 22.
 NIH Public Access Author Manuscript Published in final edited form as: Blood Rev. 2009 November ; 23(6): 231 240. doi:10.1016/j.blre.2009.07.003. Resuscitation and transfusion principles for traumatic
NIH Public Access Author Manuscript Published in final edited form as: Blood Rev. 2009 November ; 23(6): 231 240. doi:10.1016/j.blre.2009.07.003. Resuscitation and transfusion principles for traumatic
BLOOD IN THE AIR: THE STARS EXPERIENCE Dr. Ryan Deedo MD DipAeroRT FRCPC Transport Physician STARS Medical Communications Lead (Calgary)
") BLOOD IN THE AIR: THE STARS EXPERIENCE Dr. Ryan Deedo MD DipAeroRT FRCPC Transport Physician STARS Medical Communications Lead (Calgary) What s new at STARS? STARS bases and response areas Operations
BLOOD IN THE AIR: THE STARS EXPERIENCE Dr. Ryan Deedo MD DipAeroRT FRCPC Transport Physician STARS Medical Communications Lead (Calgary) What s new at STARS? STARS bases and response areas Operations
Damage control resuscitation using blood component therapy in standard doses has a limited effect on coagulopathy during trauma hemorrhage
 Intensive Care Med (2015) 41:239 247 DOI 10.1007/s00134-014-3584-1 ORIGINAL Sirat Khan Ross Davenport Imran Raza Simon Glasgow Henry D. De Ath Pär I. Johansson Nicola Curry Simon Stanworth Christine Gaarder
Intensive Care Med (2015) 41:239 247 DOI 10.1007/s00134-014-3584-1 ORIGINAL Sirat Khan Ross Davenport Imran Raza Simon Glasgow Henry D. De Ath Pär I. Johansson Nicola Curry Simon Stanworth Christine Gaarder
Resuscitation Update
 Resuscitation Update? Dr. Edward Pyun Jr., M.D. FACS Trauma Medical Director/Surgical ICU Director OSF St. Anthony Medical Center Trauma Services Perryville Surgical Associates November 10, 2012 2009 Recommendations
Resuscitation Update? Dr. Edward Pyun Jr., M.D. FACS Trauma Medical Director/Surgical ICU Director OSF St. Anthony Medical Center Trauma Services Perryville Surgical Associates November 10, 2012 2009 Recommendations
VanderbiltEM.com. Prehospital STEMIs. EMS Today 2018 Research That Should Be On Your Radar Screen 3/1/2018
 EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
Analysis of Trauma Patients with Massive Transfusion in the Emergency Department
 대한수혈학회지 : 제 27 권제 2 호, 2016 The Korean Journal of Blood Transfusion Vol. 27, No. 2, 130-136, August 2016 http://dx.doi.org/10.17945/kjbt.2016.27.2.130 pissn 1226-9336 eissn 2383-6881 Original Article 응급실에서대량수혈을받은외상환자분석
대한수혈학회지 : 제 27 권제 2 호, 2016 The Korean Journal of Blood Transfusion Vol. 27, No. 2, 130-136, August 2016 http://dx.doi.org/10.17945/kjbt.2016.27.2.130 pissn 1226-9336 eissn 2383-6881 Original Article 응급실에서대량수혈을받은외상환자분석
Massive transfusion (MT) occurs in 3% to 5% of all
 occurs in 3% to 5% of all") Early Prediction of Massive Transfusion in Trauma: Simple as ABC (Assessment of Blood Consumption)? Timothy C. Nunez, MD, Igor V. Voskresensky, MD, Lesly A. Dossett, MD, MPH, Ricky Shinall, BS, William
Early Prediction of Massive Transfusion in Trauma: Simple as ABC (Assessment of Blood Consumption)? Timothy C. Nunez, MD, Igor V. Voskresensky, MD, Lesly A. Dossett, MD, MPH, Ricky Shinall, BS, William
Effect of post-intubation hypotension on outcomes in major trauma patients
 Effect of post-intubation hypotension on outcomes in major trauma patients Dr. Robert S. Green Professor, Emergency Medicine and Critical Care Dalhousie University Medical Director, Trauma Nova Scotia
Effect of post-intubation hypotension on outcomes in major trauma patients Dr. Robert S. Green Professor, Emergency Medicine and Critical Care Dalhousie University Medical Director, Trauma Nova Scotia
The Effect of Evolving Fluid Resuscitation on the Outcome of Severely Injured Patients
 https://helda.helsinki.fi The Effect of Evolving Fluid Resuscitation on the Outcome of Severely Injured Patients Brinck, Tuomas 2016-06 Brinck, T, Handolin, L & Lefering, R 2016, ' The Effect of Evolving
https://helda.helsinki.fi The Effect of Evolving Fluid Resuscitation on the Outcome of Severely Injured Patients Brinck, Tuomas 2016-06 Brinck, T, Handolin, L & Lefering, R 2016, ' The Effect of Evolving
Major Haemorrhage in the Remote and Retrieval Environment. Stuart Gillon Royal Flying Doctor Service (Western Operations)
") Major Haemorrhage in the Remote and Retrieval Environment Stuart Gillon Royal Flying Doctor Service (Western Operations) Aims Audit approach to major haemorrhage within RFDS (WO) Ascertain current major
Major Haemorrhage in the Remote and Retrieval Environment Stuart Gillon Royal Flying Doctor Service (Western Operations) Aims Audit approach to major haemorrhage within RFDS (WO) Ascertain current major
Tactical Combat Casualty Care Guideline Change Fluid Resuscitation for Hemorrhagic Shock in TCCC
 Tactical Combat Casualty Care Guideline Change 14-01 Fluid Resuscitation for Hemorrhagic Shock in TCCC 2 June 2014 Why a change was needed: The last update to the fluid resuscitation recommendations in
Tactical Combat Casualty Care Guideline Change 14-01 Fluid Resuscitation for Hemorrhagic Shock in TCCC 2 June 2014 Why a change was needed: The last update to the fluid resuscitation recommendations in
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
Immediate screening method for predicting the necessity of massive transfusions in trauma patients: a retrospective single-center study
 Yumoto et al. Journal of Intensive Care 2014, 2:54 RESEARCH Open Access Immediate screening method for predicting the necessity of massive transfusions in trauma patients: a retrospective single-center
Yumoto et al. Journal of Intensive Care 2014, 2:54 RESEARCH Open Access Immediate screening method for predicting the necessity of massive transfusions in trauma patients: a retrospective single-center
Where Have we Come From, and Where are we Going
 Where Have we Come From, and Where are we Going James Augustine, MD, FACEP Emergency Physician and Fire/EMS Medical Director Naples, Atlanta, and Dayton Clinical Professor, Wright State Univ. Dept of Emergency
Where Have we Come From, and Where are we Going James Augustine, MD, FACEP Emergency Physician and Fire/EMS Medical Director Naples, Atlanta, and Dayton Clinical Professor, Wright State Univ. Dept of Emergency
Exsanguinating hemorrhage continues to be one of the
 ORIGINAL ARTICLE All Massive Transfusion Criteria Are Not Created Equal: Defining the Predictive Value of Individual Transfusion Triggers to Better Determine Who Benefits From Blood Rachael A. Callcut,
ORIGINAL ARTICLE All Massive Transfusion Criteria Are Not Created Equal: Defining the Predictive Value of Individual Transfusion Triggers to Better Determine Who Benefits From Blood Rachael A. Callcut,
Disclosures. Lessons Learned in the War on Terror. The only victor in war is medicine The Mayo Brothers - WWII
 Lessons Learned in the War on Terror Martin Schreiber, COL, MC, USAR Professor of Surgery Chief of Trauma, Critical Care & Acute Care Surgery The Oregon Health & Science University Disclosures I have no
Lessons Learned in the War on Terror Martin Schreiber, COL, MC, USAR Professor of Surgery Chief of Trauma, Critical Care & Acute Care Surgery The Oregon Health & Science University Disclosures I have no
Clinical Overview of Coagulation Testing Issues
 Clinical Overview of Coagulation Testing Issues Adam M. Vogel, MD Assistant Professor, Division of Pediatric Surgery Washington University in St. Louis School of Medicine September 19, 2014 Disclosure
Clinical Overview of Coagulation Testing Issues Adam M. Vogel, MD Assistant Professor, Division of Pediatric Surgery Washington University in St. Louis School of Medicine September 19, 2014 Disclosure
Coagulopathy and shock on admission is associated with mortality for children with traumatic injuries at combat support hospitals*
 Coagulopathy and shock on admission is associated with mortality for children with traumatic injuries at combat support hospitals* Jason T. Patregnani, MD; Matthew A. Borgman, MD; Marc Maegele, MD; Charles
Coagulopathy and shock on admission is associated with mortality for children with traumatic injuries at combat support hospitals* Jason T. Patregnani, MD; Matthew A. Borgman, MD; Marc Maegele, MD; Charles
Communications. Multicenter Comparison of Emergency Release Group A versus AB Plasma in Blunt-Injured Trauma Patients
 Communications Multicenter Comparison of Emergency Release Group A versus AB Plasma in Blunt-Injured Trauma Patients Martin D. Zielinski, M.D. 1, Jason J. Schrager, M.D. 2, Pamela Johnson, B.S. 1, James
Communications Multicenter Comparison of Emergency Release Group A versus AB Plasma in Blunt-Injured Trauma Patients Martin D. Zielinski, M.D. 1, Jason J. Schrager, M.D. 2, Pamela Johnson, B.S. 1, James
Disclosure Chair of ACS COT EMS Committee Authored Evidence Based Prehospital Guideline for External Hemorrhage Control
 Eileen M. Bulger, MD Professor of Surgery, Chief of Trauma Harborview Medical Center University of Washington Disclosure Chair of ACS COT EMS Committee Authored Evidence Based Prehospital Guideline for
Eileen M. Bulger, MD Professor of Surgery, Chief of Trauma Harborview Medical Center University of Washington Disclosure Chair of ACS COT EMS Committee Authored Evidence Based Prehospital Guideline for
What is. InSpectra StO 2?
 What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
Just like Adults? Evaluating the Impact of Fluid Resuscitation in Pediatric Trauma
 Just like Adults? Evaluating the Impact of Fluid Resuscitation in Pediatric Trauma Abbas PI 1,2, Carpenter K 2, Sheikh F 1,2, Peterson ML 1,2, Kljajic M 1, Naik-Mathuria B 1,2 1 Texas Children s Hospital
Just like Adults? Evaluating the Impact of Fluid Resuscitation in Pediatric Trauma Abbas PI 1,2, Carpenter K 2, Sheikh F 1,2, Peterson ML 1,2, Kljajic M 1, Naik-Mathuria B 1,2 1 Texas Children s Hospital
The principle of 1:1:1 blood product use in the resuscitation of trauma victims. K. D. Boffard
 The principle of 1:1:1 blood product use in the resuscitation of trauma victims K. D. Boffard Milpark Hospital Department of Surgery University of the Witwatersrand Johannesburg, South Africa Annual Controversies
The principle of 1:1:1 blood product use in the resuscitation of trauma victims K. D. Boffard Milpark Hospital Department of Surgery University of the Witwatersrand Johannesburg, South Africa Annual Controversies
2012, Görlinger Klaus
 Gerinnungsmanagement der Gegenwart - wie gehen wir heute vor? 25. Allander Gerinnungsrunde am 15. März 2012 Klaus Görlinger Universitätsklinikum Essen klaus@goerlinger.net CSL Behring GmbH Octapharma AG
Gerinnungsmanagement der Gegenwart - wie gehen wir heute vor? 25. Allander Gerinnungsrunde am 15. März 2012 Klaus Görlinger Universitätsklinikum Essen klaus@goerlinger.net CSL Behring GmbH Octapharma AG
Mechanisms of Trauma Coagulopathy. Dr B M Schyma Changi General Hospital Singapore
 Mechanisms of Trauma Coagulopathy Dr B M Schyma Changi General Hospital Singapore HAEMORRHAGE A continued cause of PREVENTABLE death. 24% of trauma patients are coagulopathic on arrival 1 56% of severe
Mechanisms of Trauma Coagulopathy Dr B M Schyma Changi General Hospital Singapore HAEMORRHAGE A continued cause of PREVENTABLE death. 24% of trauma patients are coagulopathic on arrival 1 56% of severe
NIH Public Access Author Manuscript Vox Sang. Author manuscript; available in PMC 2011 August 12.
 NIH Public Access Author Manuscript Published in final edited form as: Vox Sang. 2011 July ; 101(1): 44 54. doi:10.1111/j.1423-0410.2011.01466.x. The effect of FFP:RBC ratio on morbidity and mortality
NIH Public Access Author Manuscript Published in final edited form as: Vox Sang. 2011 July ; 101(1): 44 54. doi:10.1111/j.1423-0410.2011.01466.x. The effect of FFP:RBC ratio on morbidity and mortality
Kristan Staudenmayer, MD Stanford University, Stanford, CA
 Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
Overview of massive transfusion practice
 ORIGINAL RESEARCH Overview of massive transfusion practice Irena Seferi 1, Erind Cafi 1 1 National Blood Transfusion Centre (NBTC), Tirana, Albania. Corresponding Author: Irena Seferi, MD, PhD; Address:
ORIGINAL RESEARCH Overview of massive transfusion practice Irena Seferi 1, Erind Cafi 1 1 National Blood Transfusion Centre (NBTC), Tirana, Albania. Corresponding Author: Irena Seferi, MD, PhD; Address:
Geriatric Trauma Resuscitation: Lessons from a Geriatric Trauma Surgeon
 Geriatric Trauma Resuscitation: Lessons from a Geriatric Trauma Surgeon Aurelio Rodriguez, M.D., FACS Conemaugh Memorial Medical Center Trauma Center Johnstown, PA Demographics The fastest growing age
Geriatric Trauma Resuscitation: Lessons from a Geriatric Trauma Surgeon Aurelio Rodriguez, M.D., FACS Conemaugh Memorial Medical Center Trauma Center Johnstown, PA Demographics The fastest growing age
Massive Transfusion in Pediatric Trauma: Analysis of the National Trauma Databank
 Massive Transfusion in Pediatric Trauma: Analysis of the National Trauma Databank Michelle Shroyer, MPH, Russell Griffin, PhD, Vincent Mortellaro, MD, and Rob Russell MD, MPH Introduction Hemorrhage is
Massive Transfusion in Pediatric Trauma: Analysis of the National Trauma Databank Michelle Shroyer, MPH, Russell Griffin, PhD, Vincent Mortellaro, MD, and Rob Russell MD, MPH Introduction Hemorrhage is
Blood Reviews 23 (2009) Contents lists available at ScienceDirect. Blood Reviews. journal homepage:
 Contents lists available at ScienceDirect. Blood Reviews. journal homepage:") Blood Reviews 23 (2009) 231 240 Contents lists available at ScienceDirect Blood Reviews journal homepage: www.elsevier.com/locate/blre REVIEW Resuscitation and transfusion principles for traumatic hemorrhagic
Blood Reviews 23 (2009) 231 240 Contents lists available at ScienceDirect Blood Reviews journal homepage: www.elsevier.com/locate/blre REVIEW Resuscitation and transfusion principles for traumatic hemorrhagic
Intraoperative haemorrhage and haemostasis. Dr. med. Christian Quadri Capoclinica Anestesia, ORL
 Intraoperative haemorrhage and haemostasis Dr. med. Christian Quadri Capoclinica Anestesia, ORL Haemostasis is like love. Everybody talks about it, nobody understands it. JH Levy 2000 Intraoperative Haemorrhage
Intraoperative haemorrhage and haemostasis Dr. med. Christian Quadri Capoclinica Anestesia, ORL Haemostasis is like love. Everybody talks about it, nobody understands it. JH Levy 2000 Intraoperative Haemorrhage
Prehospital Plasma / TXA experience - FDP in Norwegian HEMS
 Prehospital Plasma / TXA experience - FDP in Norwegian HEMS Geir Arne Sunde COI: None Text of the day The Wiser Guys > scientific rationale behind FDP use in HEMS Point of care and competence to the scene?
Prehospital Plasma / TXA experience - FDP in Norwegian HEMS Geir Arne Sunde COI: None Text of the day The Wiser Guys > scientific rationale behind FDP use in HEMS Point of care and competence to the scene?
How can ROTEM testing help you in trauma?
 How can ROTEM testing help you in trauma? Complicated bleeding situations can appear intra and post operatively. They can be life-threatening and always require immediate action. A fast differential diagnosis
How can ROTEM testing help you in trauma? Complicated bleeding situations can appear intra and post operatively. They can be life-threatening and always require immediate action. A fast differential diagnosis
Armed Services Blood Program
 Armed Services Blood Program Defense Health Board Concerns Regarding the Collection and Transfusion of Non-FDA Compliant Blood Products in Theater Information Brief Defense Health Board 17 August 2009
Armed Services Blood Program Defense Health Board Concerns Regarding the Collection and Transfusion of Non-FDA Compliant Blood Products in Theater Information Brief Defense Health Board 17 August 2009
Update on pre-hospital blood transfusions. Dr Anne Weaver Consultant in Emergency Medicine & Pre-hospital Care RDCR 2016
 Update on pre-hospital blood transfusions Dr Anne Weaver Consultant in Emergency Medicine & Pre-hospital Care RDCR 2016 ObjecGves How and why Blood on board was launched Share our results Next steps And
Update on pre-hospital blood transfusions Dr Anne Weaver Consultant in Emergency Medicine & Pre-hospital Care RDCR 2016 ObjecGves How and why Blood on board was launched Share our results Next steps And
Emergency Blood and Massive Transfusion: The Surgeon s Perspective. Transfusion Medicine Update September 16 17, 2009
 Transfusion Medicine Update September 16 17, 2009 Mandip S. Atwal, D.O. FACOS Carl M. Pesta, D.O. FACOS Agenda History Hemorrhagic shock Transfusion is Bad Transfusion Prevention Transfusion The Red Chest
Transfusion Medicine Update September 16 17, 2009 Mandip S. Atwal, D.O. FACOS Carl M. Pesta, D.O. FACOS Agenda History Hemorrhagic shock Transfusion is Bad Transfusion Prevention Transfusion The Red Chest
Chest diseases Hospital Laboratory Hematology Practice guidelines
 Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury
 TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury Megan Brenner MD MS RPVI FACS Associate Professor of Surgery Division of Trauma/Surgical Critical Care, RA Cowley
TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury Megan Brenner MD MS RPVI FACS Associate Professor of Surgery Division of Trauma/Surgical Critical Care, RA Cowley
Massive Transfusion. MPQC Spring Summit April 29, Roger Belizaire MD PhD
 Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Fluid resuscitation in haemorrhagic shock in combat casualties
 DOI 10.1186/s40696-017-0030-2 Disaster and Military Medicine REVIEW Open Access Fluid resuscitation in haemorrhagic shock in combat casualties Parli R. Ravi 1* and Bipin Puri 2 Abstract This brief update
DOI 10.1186/s40696-017-0030-2 Disaster and Military Medicine REVIEW Open Access Fluid resuscitation in haemorrhagic shock in combat casualties Parli R. Ravi 1* and Bipin Puri 2 Abstract This brief update
Groupe d Intérêt en Hémostase Périopératoire
 How do I treat massive bleeding? Red blood cell / plasma / platelet ratio and massive transfusion protocols Anne GODIER Service d Anesthésie-Réanimation Hopital Cochin Paris Groupe d Intérêt en Hémostase
How do I treat massive bleeding? Red blood cell / plasma / platelet ratio and massive transfusion protocols Anne GODIER Service d Anesthésie-Réanimation Hopital Cochin Paris Groupe d Intérêt en Hémostase
Implementation of massive transfusion protocol (MTP) for trauma
 for trauma") LEADING ARTICLE Implementation of massive transfusion protocol (MTP) for trauma 1,2 2 2 R.N. Ellawala, K. Gonsalkorala, I.S. Wijesiriwardena 1 Department of Surgery, Faculty of Medicine, General Sir John
LEADING ARTICLE Implementation of massive transfusion protocol (MTP) for trauma 1,2 2 2 R.N. Ellawala, K. Gonsalkorala, I.S. Wijesiriwardena 1 Department of Surgery, Faculty of Medicine, General Sir John
Transfusion in major bleeding: new insights. Gert Poortmans
 Transfusion in major bleeding: new insights Gert Poortmans Trauma Cardiac Surgery Major Surgery with ongoing blood loss Burn Surgery Lethal Triad Polytransfusion: definitions Coagulation Coagulopathy of
Transfusion in major bleeding: new insights Gert Poortmans Trauma Cardiac Surgery Major Surgery with ongoing blood loss Burn Surgery Lethal Triad Polytransfusion: definitions Coagulation Coagulopathy of
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient
 Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Efficacy of Uncross-Matched Type O Packed Red Blood Cell Transfusion to Traumatic Shock Patients: a Propensity Score Match Study
 ORIGINAL ARTICLE Emergency & Critical Care Medicine https://doi.org/10.3346/jkms.2017.32.12.2058 J Korean Med Sci 2017; 32: 2058-2063 Efficacy of Uncross-Matched Type O Packed Red Blood Cell Transfusion
ORIGINAL ARTICLE Emergency & Critical Care Medicine https://doi.org/10.3346/jkms.2017.32.12.2058 J Korean Med Sci 2017; 32: 2058-2063 Efficacy of Uncross-Matched Type O Packed Red Blood Cell Transfusion
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
My Bloody Talk. Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne
 My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
Kevin Schulz, MD, FAEMS, FACEP
 Blood Therapy for EMS Kevin Schulz, MD, FAEMS, FACEP - Clinical Assistant Professor of Emergency Medicine, EMS Fellowship Program Director - McGovern School of Medicine at UTHealth - Assistant Medical
Blood Therapy for EMS Kevin Schulz, MD, FAEMS, FACEP - Clinical Assistant Professor of Emergency Medicine, EMS Fellowship Program Director - McGovern School of Medicine at UTHealth - Assistant Medical
EAST MULTICENTER STUDY DATA DICTIONARY
 EAST MULTICENTER STUDY DATA DICTIONARY Does the Addition of Daily Aspirin to Standard Deep Venous Thrombosis Prophylaxis Reduce the Rate of Venous Thromboembolic Events? Data Entry Points and appropriate
EAST MULTICENTER STUDY DATA DICTIONARY Does the Addition of Daily Aspirin to Standard Deep Venous Thrombosis Prophylaxis Reduce the Rate of Venous Thromboembolic Events? Data Entry Points and appropriate
5/30/2013. I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow. Trauma = #1 cause of death persons <40 yo 1
 I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow Trauma = #1 cause of death persons
I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow Trauma = #1 cause of death persons
PREPARED FOR: U.S. Army Medical Research and Materiel Command Fort Detrick, Maryland
 AD Award Number: W81XWH-11-2-0084 TITLE: Optimization of Lyophilized Plasma for Use in Combat Casualties PRINCIPAL INVESTIGATOR: Martin A. Schreiber, MD CONTRACTING ORGANIZATION: Oregon Health & Science
AD Award Number: W81XWH-11-2-0084 TITLE: Optimization of Lyophilized Plasma for Use in Combat Casualties PRINCIPAL INVESTIGATOR: Martin A. Schreiber, MD CONTRACTING ORGANIZATION: Oregon Health & Science
Balanced ratio of plasma to packed red blood cells improves outcomes in massive transfusion: A large multicenter study
 EXPERIMENTAL AND THERAPEUTIC MEDICINE 10: 37-42, 2015 Balanced ratio of plasma to packed red blood cells improves outcomes in massive transfusion: A large multicenter study JIANG CUN YANG 1*, CUI XIANG
EXPERIMENTAL AND THERAPEUTIC MEDICINE 10: 37-42, 2015 Balanced ratio of plasma to packed red blood cells improves outcomes in massive transfusion: A large multicenter study JIANG CUN YANG 1*, CUI XIANG
CRASH ing Trauma Patients: The CRASH trials. Tim Coats Professor of Emergency Medicine University of Leicester, UK
 CRASH ing Trauma Patients: The CRASH trials Tim Coats Professor of Emergency Medicine University of Leicester, UK www.le.ac.uk/emag I DO NOT have an affiliation (financial or otherwise) with a pharmaceutical,
CRASH ing Trauma Patients: The CRASH trials Tim Coats Professor of Emergency Medicine University of Leicester, UK www.le.ac.uk/emag I DO NOT have an affiliation (financial or otherwise) with a pharmaceutical,
ICU treatment of the trauma patient. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Does a Controlled Fluid Resuscitation Strategy Decrease Mortality in Trauma Patients?
 Does a Controlled Fluid Resuscitation Strategy Decrease Mortality in Trauma Patients? death Haemorrhage remains the biggest killer of major trauma patients Expected deaths will increase to 8 million/year
Does a Controlled Fluid Resuscitation Strategy Decrease Mortality in Trauma Patients? death Haemorrhage remains the biggest killer of major trauma patients Expected deaths will increase to 8 million/year
Learning Objectives: At the end of this exercise, the student will be able to:
 Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
GUIDANCE DOCUMENT FOR MASSIVE HEMORRHAGE MANAGEMENT IN ADULTS
 GUIDANCE DOCUMENT FOR MASSIVE HEMORRHAGE MANAGEMENT IN ADULTS 1.0 Definitions & Acronyms 1.1 Massive Hemorrhage Event (MHE): Transfusion of a volume of blood components equivalent to a patient s estimated
GUIDANCE DOCUMENT FOR MASSIVE HEMORRHAGE MANAGEMENT IN ADULTS 1.0 Definitions & Acronyms 1.1 Massive Hemorrhage Event (MHE): Transfusion of a volume of blood components equivalent to a patient s estimated
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions