Interactive Cases. Victor Tseng, MD
|
|
|
- Jasmin Atkinson
- 6 years ago
- Views:
Transcription


1 Interactive Cases Victor Tseng, MD
2
3 WHO HAS A NEUTROPENIC FEVER? 61 M ANC T 38.9 being treated for stage IIIA CRC 22 F ANC T 37.0 getting consolidation for ALL 53 F ANC 580 (710 yesterday) + T 38.4 who completed first induction cycle for dose for DLBCL 3 days ago 40 M ANC T 39.0 being treated with ATG/CSA for aplastic anemia 36 F ANC 360 (200 yesterday) + T new RML infiltrate on CXR, having count recovery after second induction cycle for T-cell ALL 83 M with dementia residing in NH who developed dysuria and rigors 2 days prior. Found in ED to have ANC T 39.1 None of the above All of the above
4 WHO HAS A NEUTROPENIC FEVER? 61 M ANC T 38.9 being treated for stage IIIA CRC 22 F ANC T 37.0 getting consolidation for ALL 53 F ANC 580 (710 yesterday) + T 38.4 who completed first induction cycle for dose for DLBCL 3 days ago 40 M ANC T 39.0 being treated with ATG/CSA for aplastic anemia 36 F ANC 360 (200 yesterday) + T new RML infiltrate on CXR, having count recovery after second induction cycle for T-cell ALL 83 M with dementia residing in NH who developed dysuria and rigors 2 days prior. Found in ED to have ANC T 39.1 None of the above All of the above
5 WHO HAS A NEUTROPENIC FEVER? Neutropenia Fever ANC 500 T 38.3 single reading ANC anticipated to nadir 500 in next 48h T 38.0 over 1h
6 BEWARE OF NF MIMICKERS Neutropenia secondary to Sepsis Myeloid Reconstitution (Inflammatory) Syndrome ( MyRIS )
7 Incidence of NF in Solid Tumor and Hematologic malignancies? 5% and 10% 25% and 10% 15% and 50% 25% and > 80% Incidence of a microbiologically provable infection during NF? 10% 25% 50% > 75%

8 Marchetti and Calandra (2002)
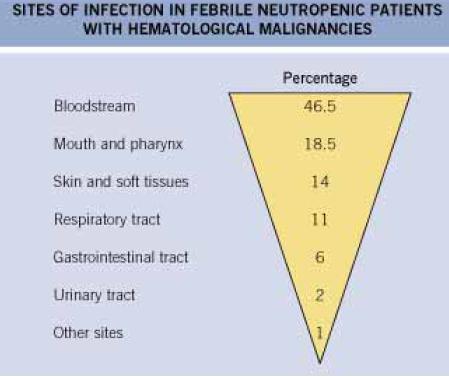
9 What are the most common pathogens isolated during NF? Yeast Mold GPC GNR GPR Anareobes Virus What is the most common source/site of infection? HCAP SSTI Unexplained (Sterile) Genitourinary Catheter-Related Infection Endocarditis Enterocolitis (GI)
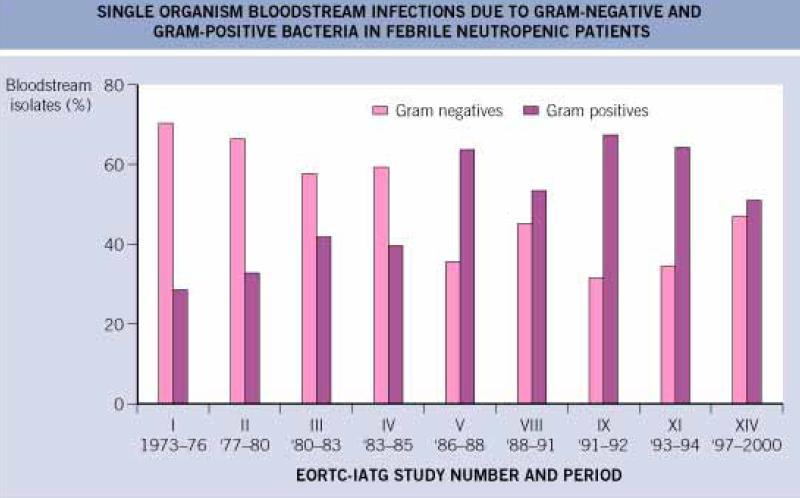
10 MICROBIOLOGY OF NF
11 MICROBIOLOGY OF NF
12 WHAT FACTOR(S) ARE INVOLVED IN THE PATHOGENESIS OF NF? Decreased Quantity of Neutrophils Decreased Chemotaxis and Phagocytic Activity of Neutrophils Disruption of Mucosal Barrier Direct Bacterial Invasion of Gut Mucosal Layers LPS Endotoxemia Hypothalamic Dysfunction due to Neutropenia
13 WHICH ITEM(S) ARE NOT A PART OF THE VA NEUTROPENIC PRECAUTIONS? Single-Bed Room Neutropenic Diet Flowers Prohibited No PR Medications No Foley Patient wears N-95 outside Reverse Isolation (Full PPE for HCW) HEPA Filter Dedicated Reusable Equipment
14 o You are the hematology fellow taking home call. o Mr. B is a 51 year old AAM with a locally destructive gluteal myxosarcoma, stage IIB. He is has just completed the first cycle of AIM. He has CKD stage 2, COPD stage 3, and obstructive CAD s/p stent placement. o One week after reciecing G-CSF, he calls you at 2 am complaining of rigors, fevers (102 F) and diarrhea.
15 HOW DO YOU RESPOND ON THE TELEPHONE? Take up to four APAP and we ll see you in clinic next week I ll mail you some antibiotics and more G-CSF right away Please come to the ER immediately. You will be admitted to the hospital, and I will see you in the morning Come to the ER now. I will see you there Um Let me call my attending
16 o In the ED, temperature is 38.8, pulse 112, BP 124/48, RR 24 and SpOx 91% on room air. He looks flushed but otherwise is in no distress. He is mentating clearly. o Scattered oral ulcers are noted. R arm port entry is free of erythema. Lungs are clear throghout. He has no murmurs. Abdomen is mildy tender in the RUQ. There are no signs of skin infection. o Stat CBC shows WBC 0.8 with 30% PMN. Creatinine is 1.7. AST and ALT at 310 and 270 respectively. Bicarbonate is 17 with normal anion gap. CXR and cultures are pending.
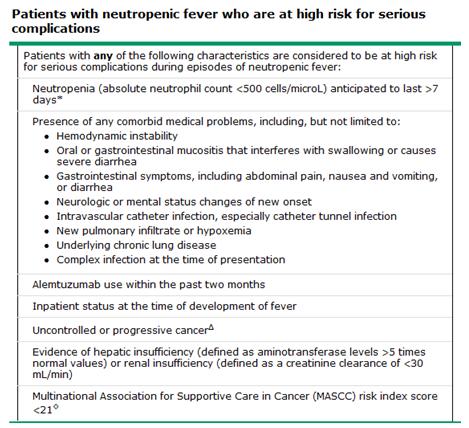
17 WHERE SHOULD THE PATIENT BE TREATED? Observation (CDU) area of ER Home General Medicine Ward MICU
18
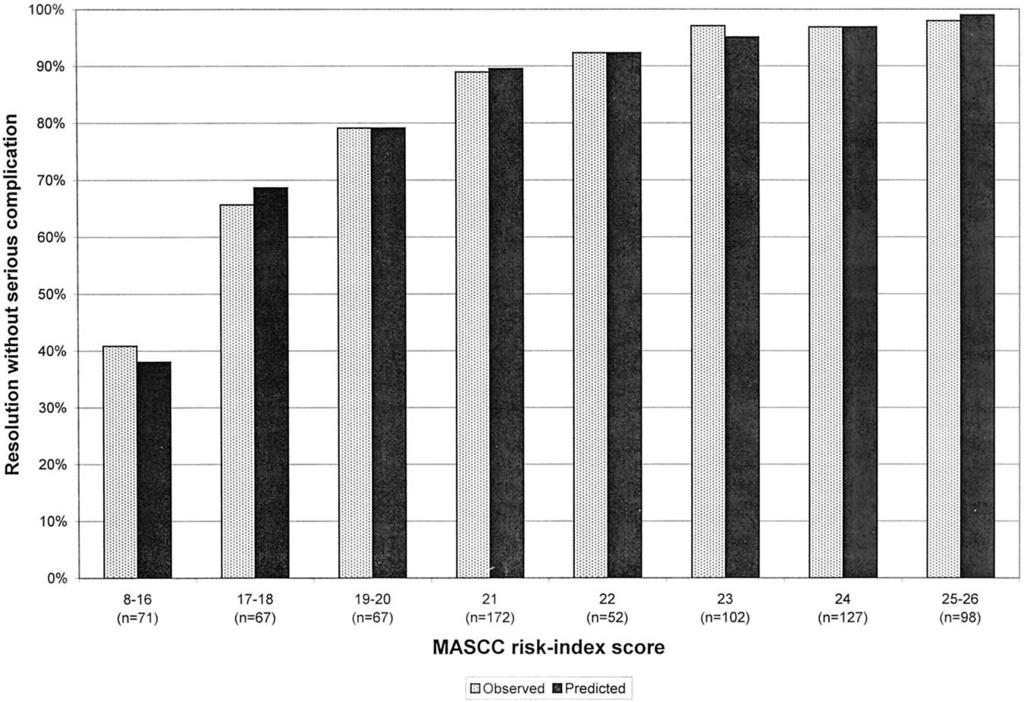
19 PPV 98.3% NPV 86.4 % SENS 95% SPEC 95% Uys et al. 2004
20
21
22 WHICH OF THE FOLLOWING ARE ACCEPTABLE REGIMEN(S) FOR OUTPATIENT THERAPY? Levofloxacin 750 mg PO qd + Augmentin 500/125 mg PO q8h Ciprofloxacin 500 mg PO q12h + Clindamycin 300 mg PO q6h Ceftriaxone 1.5 g IV qd Zosyn 2 g IV q8h Azithromycin 500 mg PO qd + Ampicillin 500 mg q6h Levofoxacin 750 mg PO qd + Vancomycin 1.5 g IV q12h
23 WHICH OF THE FOLLOWING ARE ACCEPTABLE REGIMEN(S) FOR OUTPATIENT THERAPY? Levofloxacin 750 mg PO qd + Augmentin 500/125 mg PO q8h Ciprofloxacin 500 mg PO q12h + Clindamycin 300 mg PO q6h Ceftriaxone 1.5 g IV qd Zosyn 2 g IV q8h Azithromycin 500 mg PO qd + Ampicillin 500 mg q6h Levofoxacin 750 mg PO qd + Vancomycin 1.5 g IV q12h
24 Teuffel et al. Ann Oncol 2011;22:
25 WHAT DIAGNOSTIC TESTS SHOULD BE PERFORMED? BCx from CVC BCx from peripheral vein UA + reflex UCx LP Stool Cx C. difficile toxin assay Nasal Respiratory Virus Swab CXR Mini-BAL



26 o CXR shows clear airspaces and normal terminus of catheter tip. Gram stain of BCx reveals numerous GPC in clusters. UA is positive for nitrate and bacteria, negative for LE or WBC. o He is admitted to the floor by the night float medicine intern. M3 PGY-1 PGY-3
27
28 WHICH OF THE FOLLOWING ARE ACCEPTABLE REGIMEN(S) FOR INITIAL EMPIRIC INPATIENT THERAPY? Zosyn 2 g IV q8h Cefepime 2 g IV q8h Ceftazidime 1.5 g IV q12h + Levofloxacin 750 mg IV qd Vancomycin 1 g IV q8h + Zosyn 2 g IV q8h Vancomycin 1 g IV q8h + Zosyn 2 g IV q8h + Tobramycin 100 mg IV q8h Zosyn 2 g IV q8h + Levofloxacin 750 mg IV qd Cefepime 2 g IV q8h + Voriconazole 250 mg IV q12h Zosyn 2 g IV q8h + Micafungin 100 mg IV qd + Acyclovir 400 mg IV q8h
29 WHICH OF THE FOLLOWING ARE ACCEPTABLE REGIMEN(S) FOR INITIAL EMPIRIC INPATIENT THERAPY? Zosyn 2 g IV q8h Cefepime 2 g IV q8h Ceftazidime 1.5 g IV q12h + Levofloxacin 750 mg IV qd Vancomycin 1 g IV q8h + Zosyn 2 g IV q8h Vancomycin 1 g IV q8h + Zosyn 2 g IV q8h + Tobramycin 100 mg IV q8h Zosyn 2 g IV q8h + Levofloxacin 750 mg IV qd Cefepime 2 g IV q8h + Voriconazole 250 mg IV q12h Zosyn 2 g IV q8h + Micafungin 100 mg IV qd + Acyclovir 400 mg IV q8h
30
31 WHICH OF THE FOLLOWING IS NOT AN INDICATION FOR EMPIRIC VANCOMYCIN? Clusters of GPC NOS in 1 BCx Pulmonary Infiltrate Hypotension Rigors or Fever during CVC Infusion New Cardiac Murmur NF Occuring During Inpatient Stay Altered Mental Status Suspected SSTI
32 WHICH OF THE FOLLOWING IS NOT AN INDICATION FOR EMPIRIC VANCOMYCIN? Clusters of GPC NOS in 1 BCx Pulmonary Infiltrate Hypotension Rigors or Fever during CVC Infusion New Cardiac Murmur NF Occuring During Inpatient Stay Altered Mental Status Suspected SSTI
33 o Mr. B is started on Vancomycin + Cefepime IV and given a generous IVF resuscitation. o Unfortunately, he continues to spike intermittent fevers, up to 39.2, even after four days of ABx therapy. He has some mild facial congestion but no other localizing symptoms. His ANC remains in a nadir of He remains hemodynamically stable without any evidenceof new end-organ dysfunction from sepsis. o Repeat BCx are growing broadly susceptible CNSA x 1/4
34 WHAT IS YOUR NEXT MOVE? Continue Current ABx Discontinue ABx due to drug fever Broaden to Meropenem IV + Levaquin IV Remove R arm Port and CVC TTE CT Sinus and Chest Start Empiric Antifunal Therapy CT Abdomen MRI Pelvis to assess of Osteomyelitis
35 WHAT IS YOUR NEXT MOVE? Continue Current ABx Discontinue ABx due to drug fever Broaden to Meropenem IV + Levaquin IV Remove R arm Port and CVC TTE CT Sinus and Chest Start Empiric Antifungal Therapy CT Abdomen MRI Pelvis to assess of Osteomyelitis
36
37
38 WHEN SHOULD THE CATHETER STAY IN PLACE (i.e. TREAT THROUGH)? BCx grow S. aureus BCx grow P. auruginosa BCx grow MDR E. coli BCx grow ESBL enterobactericiae spp BCx grow Candida spp. Patient develops hypotension Bacteremia 72 hr after taylored ABx therapy Port or Pocket Site Infection
39 WHEN SHOULD THE CATHETER STAY IN PLACE (i.e. TREAT THROUGH)? BCx grow S. aureus BCx grow P. auruginosa BCx grow MDR E. coli BCx grow ESBL enterobactericiae spp BCx grow Candida spp. Patient develops hypotension Bacteremia 72 hr after taylored ABx therapy Port or Pocket Site Infection

40 BONUS QUESTION o A 48 y/o F with late relapsed HL is getting slavage chemotherapy with Stanford V. She had completed her last cycle 8 days ago and develops NF with ANC < 100 and T She has intense R flank and epigastric pain. CT of the abdomen is shown below.
41 WHAT IS THIS? Acute Neutropenic Hepatitis Septic Mesenteric Embolization Abdominal Abscess Neutropenic Necrotizing Enterocolitis Lymphoma
Neutropenic Fever. CID 2011; 52 (4):e56-e93
:e56-e93") Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
December 3, 2015 Severe Sepsis and Septic Shock Antibiotic Guide
 Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
Pneumonia Community-Acquired Healthcare-Associated
 Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Urinary Tract Infections in Hospitalized Patients
 Urinary Tract Infections in Hospitalized Patients Puerto Rico Chapter Annual Meeting Daniel C. DeSimone, MD March 9, 2019 2017 MFMER slide-1 Disclosures for speaker: Date of presentation: 3/9/2019 No relevant
Urinary Tract Infections in Hospitalized Patients Puerto Rico Chapter Annual Meeting Daniel C. DeSimone, MD March 9, 2019 2017 MFMER slide-1 Disclosures for speaker: Date of presentation: 3/9/2019 No relevant
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
PAEDIATRIC FEBRILE NEUTROPENIA CARE PATHWAY
 PAEDIATRIC FEBRILE NEUTROPENIA CARE PATHWAY Purpose: This document is intended as a guide to the investigation and management of children presenting in Salisbury District Hospital with suspected neutropenic
PAEDIATRIC FEBRILE NEUTROPENIA CARE PATHWAY Purpose: This document is intended as a guide to the investigation and management of children presenting in Salisbury District Hospital with suspected neutropenic
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Shannon Carty, PGY-2 ICCR IRB Project Proposal April 9, 2008
 Shannon Carty, PGY-2 ICCR IRB Project Proposal April 9, 2008 Study Title: Observational Study to Determine the Effect of an Emergency Department Adult Oncology Stat Antibiotic Protocol on Clinical Outcomes
Shannon Carty, PGY-2 ICCR IRB Project Proposal April 9, 2008 Study Title: Observational Study to Determine the Effect of an Emergency Department Adult Oncology Stat Antibiotic Protocol on Clinical Outcomes
Acute Cholangitis. Kelsey Knotts PharmD Candidate Class of 2016
 Acute Cholangitis Kelsey Knotts PharmD Candidate Class of 2016 Learning Objectives 1. Describe the mechanism of the development of acute cholangitis 2. Identify common causative organisms in acute cholangitis
Acute Cholangitis Kelsey Knotts PharmD Candidate Class of 2016 Learning Objectives 1. Describe the mechanism of the development of acute cholangitis 2. Identify common causative organisms in acute cholangitis
Infected cardiac-implantable electronic devices: diagnosis, and treatment
 Infected cardiac-implantable electronic devices: diagnosis, and treatment The incidence of infection following implantation of cardiac implantable electronic devices (CIEDs) is increasing at a faster rate
Infected cardiac-implantable electronic devices: diagnosis, and treatment The incidence of infection following implantation of cardiac implantable electronic devices (CIEDs) is increasing at a faster rate
Septic Shock. Kathryn Sims, PGY I
 Septic Shock Kathryn Sims, PGY I A 6 y.o. previously healthy boy presents to the ED with 7 days of fever accompanied by chills. Further history reveals the patient has also been experiencing dysuria for
Septic Shock Kathryn Sims, PGY I A 6 y.o. previously healthy boy presents to the ED with 7 days of fever accompanied by chills. Further history reveals the patient has also been experiencing dysuria for
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Febrile neutropenia. Febrile neutropenia. Febrile neutropenia. Febrile neutropenia 1/30/2019. Infection in patients with cancer
 Manit Sae-teaw B.Pharm, BCP, BCOP Glad dip in pharmacotherapy Faculty of pharmaceutical sciences Ubon Ratchathani University Fever Oral temperature measurement of 38.3 C (101.0 F) single 38.0 C (100.4
Manit Sae-teaw B.Pharm, BCP, BCOP Glad dip in pharmacotherapy Faculty of pharmaceutical sciences Ubon Ratchathani University Fever Oral temperature measurement of 38.3 C (101.0 F) single 38.0 C (100.4
MICHIGAN MEDICINE GUIDELINES FOR TREATMENT OF URINARY TRACT INFECTIONS IN ADULTS
 When to Order a Urine Culture: Asymptomatic bacteriuria is often treated unnecessarily, and accounts for a substantial burden of unnecessary antimicrobial use. National guidelines recommend against testing
When to Order a Urine Culture: Asymptomatic bacteriuria is often treated unnecessarily, and accounts for a substantial burden of unnecessary antimicrobial use. National guidelines recommend against testing
Ready to answer the questions?
 파워포인트문서의제목 Reference 1. IDSA GUIDELINES. Clinical Practice Guidelines for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer: 2010 Update by the Infectious Disease Society of America.
파워포인트문서의제목 Reference 1. IDSA GUIDELINES. Clinical Practice Guidelines for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer: 2010 Update by the Infectious Disease Society of America.
Things your mother never told you about antibiotics, UTI s, and Pneumonia. Rob Kaplan, MD July 12 and 14, 2017
 Things your mother never told you about antibiotics, UTI s, and Pneumonia Rob Kaplan, MD July 12 and 14, 2017 Objectives After this talk participants will: Be able to articulate some of the principles
Things your mother never told you about antibiotics, UTI s, and Pneumonia Rob Kaplan, MD July 12 and 14, 2017 Objectives After this talk participants will: Be able to articulate some of the principles
UPDATE ON FEBRILE NEUTROPENIA
 UPDATE ON FEBRILE NEUTROPENIA Clinical approach and management Dr.Shafiq A. Alimad Head of medical department at university of science and technology hospital YICID 15-December-2014 INTRODUCTION Cancer
UPDATE ON FEBRILE NEUTROPENIA Clinical approach and management Dr.Shafiq A. Alimad Head of medical department at university of science and technology hospital YICID 15-December-2014 INTRODUCTION Cancer
Treatment of febrile neutropenia in patients with neoplasia
 Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment
 Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Dilemmas in Septic Shock
 Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Clinical Pearls Infectious Diseases. Pritish K. Tosh, MD MN ACP Nov 7, [Answers and discussion slides will be posted after the meeting]
![Clinical Pearls Infectious Diseases. Pritish K. Tosh, MD MN ACP Nov 7, [Answers and discussion slides will be posted after the meeting]](/thumbs/83/87318178.jpg "Clinical Pearls Infectious Diseases. Pritish K. Tosh, MD MN ACP Nov 7, [Answers and discussion slides will be posted after the meeting]") Clinical Pearls Infectious Diseases Pritish K. Tosh, MD MN ACP Nov 7, 2014 [Answers and discussion slides will be posted after the meeting] Case 1 A 33-year-old male with diffuse large B-cell lymphoma
Clinical Pearls Infectious Diseases Pritish K. Tosh, MD MN ACP Nov 7, 2014 [Answers and discussion slides will be posted after the meeting] Case 1 A 33-year-old male with diffuse large B-cell lymphoma
The Febrile Infant. SJRH ED Rounds Dec By: Robin Clouston
 1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
Prospective audit and feedback of piperacillin-tazobactam use in a 1115 bed acute care hospital
 Prospective audit and feedback of piperacillin-tazobactam use in a 1115 bed acute care hospital Final Results Nathan Beahm, BSP, PharmD(student) September 10, 2016 Objectives Review background information
Prospective audit and feedback of piperacillin-tazobactam use in a 1115 bed acute care hospital Final Results Nathan Beahm, BSP, PharmD(student) September 10, 2016 Objectives Review background information
Fever. National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital
 Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Febrile Neutropenia. These podcasts are designed to give medical students an overview of key topics in pediatrics. The
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Febrile Neutropenia. These podcasts are designed to give medical students an overview of key topics in pediatrics. The
Fever Without a Source Age: 0-28 Day Pathway - Emergency Department Evidence Based Outcome Center
 Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Neutropenic Sepsis Guideline
 Neutropenic Sepsis Guideline Neutropenic Sepsis Guideline - definitions Suspected or proven infection in a neutropenic patient is a MEDICAL EMERGENCY and is an indication for immediate assessment and prompt
Neutropenic Sepsis Guideline Neutropenic Sepsis Guideline - definitions Suspected or proven infection in a neutropenic patient is a MEDICAL EMERGENCY and is an indication for immediate assessment and prompt
Cystic Fibrosis: Pulmonary Exacerbations Management Guidelines
 Cystic Fibrosis: Pulmonary Exacerbations Management Guidelines Inclusion Criteria: Age 1 year with cystic fibrosis admitted for a pulmonary exacerbation. Exclusion Criteria: ICU Admission Newborn with
Cystic Fibrosis: Pulmonary Exacerbations Management Guidelines Inclusion Criteria: Age 1 year with cystic fibrosis admitted for a pulmonary exacerbation. Exclusion Criteria: ICU Admission Newborn with
CARE PATHWAY FOR CHILDREN AND YOUNG PERSONS WITH FEBRILE NEUTROPENIA, NEUTROPENIC SEPSIS OR SUSPECTED CENTRAL VENOUS LINE INFECTIONS
 CARE PATHWAY FOR CHILDREN AND YOUNG PERSONS WITH FEBRILE NEUTROPENIA, NEUTROPENIC SEPSIS OR SUSPECTED CENTRAL VENOUS LINE INFECTIONS This Care Pathway has been developed by a multidisciplinary team. It
CARE PATHWAY FOR CHILDREN AND YOUNG PERSONS WITH FEBRILE NEUTROPENIA, NEUTROPENIC SEPSIS OR SUSPECTED CENTRAL VENOUS LINE INFECTIONS This Care Pathway has been developed by a multidisciplinary team. It
Lanny Hsieh, M.D. Infectious Diseases Hospitalist Program
 Lanny Hsieh, M.D. Infectious Diseases Hospitalist Program Definition of Fever Arbitrary 38.0-38.4 (low grade may be significant in immunocompromised patients) > 38.5 (nurse will call you) Be aware of
Lanny Hsieh, M.D. Infectious Diseases Hospitalist Program Definition of Fever Arbitrary 38.0-38.4 (low grade may be significant in immunocompromised patients) > 38.5 (nurse will call you) Be aware of
Mortality Rate was unsightly!!! 4/24/2013. Sepsis Quality Improvement Project
 Libby, MT Sepsis Quality Improvement Project Barb Dumont RN, Director of Quality and Risk Management Mike Julius RN, ED Manager Cathy Wolfe RN, Chief Nursing Officer. Mortality Rate was unsightly!!! percent
Libby, MT Sepsis Quality Improvement Project Barb Dumont RN, Director of Quality and Risk Management Mike Julius RN, ED Manager Cathy Wolfe RN, Chief Nursing Officer. Mortality Rate was unsightly!!! percent
Choc septique. Frédéric Pène
 Choc septique Frédéric Pène Réanimation Médicale, Hôpital Cochin, AP-HP Université Paris Descartes Institut Cochin, Inserm U1016, CNRS UMR-8104, Département 3i No conflict of interest A 54 y.o. male patient
Choc septique Frédéric Pène Réanimation Médicale, Hôpital Cochin, AP-HP Université Paris Descartes Institut Cochin, Inserm U1016, CNRS UMR-8104, Département 3i No conflict of interest A 54 y.o. male patient
Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center
 Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center Kathy Peters is a 63 y.o. patient that presents to your urgent care office today with a history
Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center Kathy Peters is a 63 y.o. patient that presents to your urgent care office today with a history
+ Objectives. n Define who is at risk for SBI. n Clarify risk stratification. n Provide treatment guidelines. n Bust some myths
 Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
ESCMID Online Lecture Library. by author. CASE PRESENTATION ECCMID clinical grand round May Anat Stern, MD Rambam medical center Haifa, Israel
 CASE PRESENTATION ECCMID clinical grand round May 2014 Anat Stern, MD Rambam medical center Haifa, Israel An 18 years old Female, from Ukraine, diagnosed with acute lymphoblastic leukemia (ALL) in 2003.
CASE PRESENTATION ECCMID clinical grand round May 2014 Anat Stern, MD Rambam medical center Haifa, Israel An 18 years old Female, from Ukraine, diagnosed with acute lymphoblastic leukemia (ALL) in 2003.
Dr. Arghya Samanta PG-3 Department of Pediatrics
 Dr. Arghya Samanta PG-3 Department of Pediatrics A 3 year old male K/C/O B-cell Acute lymphoblastic leukemia Undergoing induction phase of chemotherapy On day 23 of induction Presented with - high grade
Dr. Arghya Samanta PG-3 Department of Pediatrics A 3 year old male K/C/O B-cell Acute lymphoblastic leukemia Undergoing induction phase of chemotherapy On day 23 of induction Presented with - high grade
Neutropenic Sepsis Acute General Management and Support. Ernie Marshall Macmillan Consultant in Medical Oncology Clatterbridge Centre for Oncology
 Neutropenic Sepsis Acute General Management and Support Ernie Marshall Macmillan Consultant in Medical Oncology Clatterbridge Centre for Oncology Who Am I? I am A Medical Oncologist (MCCN) Site specialist
Neutropenic Sepsis Acute General Management and Support Ernie Marshall Macmillan Consultant in Medical Oncology Clatterbridge Centre for Oncology Who Am I? I am A Medical Oncologist (MCCN) Site specialist
Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections
 Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections Objectives How do you to diagnose, classify and manage DFI? How do you diagnose
Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections Objectives How do you to diagnose, classify and manage DFI? How do you diagnose
CAP, HCAP, HAP, VAP. 1. In 1898, William Osler described community-acquired pneumonia as:
 1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
IDSA GUIDELINES EXECUTIVE SUMMARY
 IDSA GUIDELINES Clinical Practice Guideline for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer: 2010 Update by the Infectious Diseases Society of America Alison G. Freifeld, 1 Eric
IDSA GUIDELINES Clinical Practice Guideline for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer: 2010 Update by the Infectious Diseases Society of America Alison G. Freifeld, 1 Eric
Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT
 Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: All MHS employed providers within Primary Care, Urgent Care, and In-Hospital Care. The secondary audience
Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: All MHS employed providers within Primary Care, Urgent Care, and In-Hospital Care. The secondary audience
How did I decide on the topics?
 Disclosures None How did I decide on the topics? Important papers within 1 year vs topics of importance or innovation/aha moments Sepsis Atrial Fibrillation Pneumonia Procalcitonin Objectives By the end
Disclosures None How did I decide on the topics? Important papers within 1 year vs topics of importance or innovation/aha moments Sepsis Atrial Fibrillation Pneumonia Procalcitonin Objectives By the end
CANCER RELATED INFECTION AND USE OF COLONY STIMULATING FACTORS
 CANCER RELATED INFECTION AND USE OF COLONY STIMULATING FACTORS Suphat Subongkot, Pharm.D, BCPS, BCOP Clinical Pharmacy, Khon Kaen University, Thailand Learning Objectives Summarize national guidelines
CANCER RELATED INFECTION AND USE OF COLONY STIMULATING FACTORS Suphat Subongkot, Pharm.D, BCPS, BCOP Clinical Pharmacy, Khon Kaen University, Thailand Learning Objectives Summarize national guidelines
Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine
 Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine Discuss advances in predicting prognosis Understand dwhat we know (and don t know) about the Microbiology Recognize important
Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine Discuss advances in predicting prognosis Understand dwhat we know (and don t know) about the Microbiology Recognize important
Management of Catheter Related Bloodstream Infection (CRBSI), including Antibiotic Lock Therapy.
, including Antibiotic Lock Therapy.") Management of Catheter Related Bloodstream Infection (CRBSI), including Antibiotic Lock Therapy. Written by: Dr K Gajee, Consultant Microbiologist Date: June 2017 Approved by: Drugs & Therapeutics Committee
Management of Catheter Related Bloodstream Infection (CRBSI), including Antibiotic Lock Therapy. Written by: Dr K Gajee, Consultant Microbiologist Date: June 2017 Approved by: Drugs & Therapeutics Committee
Infectious Diseases in Clinical Practice February 2011 Lisa G. Winston, MD
 Infectious Diseases in Clinical Practice February 2011 Lisa G. Winston, MD A 60 year old man was hospitalized 2 months ago for CABG. His course was uncomplicated, and he was discharged after 5 days. He
Infectious Diseases in Clinical Practice February 2011 Lisa G. Winston, MD A 60 year old man was hospitalized 2 months ago for CABG. His course was uncomplicated, and he was discharged after 5 days. He
Guidelines/Guidance/CAP/ Hospitalized Child. PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014
 Guidelines/Guidance/CAP/ Hospitalized Child PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014 CAP in Children: Epi Greatest cause of death in children worldwide Estimated > 2 M deaths in children In developed
Guidelines/Guidance/CAP/ Hospitalized Child PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014 CAP in Children: Epi Greatest cause of death in children worldwide Estimated > 2 M deaths in children In developed
Sepsis and Hemodynamic Support in September 15, 2017 Carleen Risaliti
 Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
Guidebook for ED and Inpatient Sepsis Order Set Initiatives 2018
 Background The leadership of the Surviving Sepsis Campaign (SSC) believes, since its inception, that both the SSC Guidelines and the SSC performance improvement indicators (1) will evolve as new evidence
Background The leadership of the Surviving Sepsis Campaign (SSC) believes, since its inception, that both the SSC Guidelines and the SSC performance improvement indicators (1) will evolve as new evidence
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Think Globally: Strategies to Improve the Culture of Antibiotic Prescribing
 Think Globally: Strategies to Improve the Culture of Antibiotic Prescribing October 11, 2017 Paul Lewis, PharmD, BCPS (AQ-ID) Johnson City Medical Center Johnson City, TN 1 Outline Introduction to stewardship
Think Globally: Strategies to Improve the Culture of Antibiotic Prescribing October 11, 2017 Paul Lewis, PharmD, BCPS (AQ-ID) Johnson City Medical Center Johnson City, TN 1 Outline Introduction to stewardship
ID Emergencies. BGSMC Internal Medicine Edwin Yu
 ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
Disclosures. Background. Definitions. Why Worry about these Infants? Goals. Bacterial infection in the neonate and young infant: a review
 Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
Septic shock. Babak Tamizi Far M.D Isfahan university of medical sciences
 Septic shock Babak Tamizi Far M.D Isfahan university of medical sciences Definitions Used to Describe the Condition of Septic Patients Approximately 750,000 cases of severe sepsis or septic shock occur
Septic shock Babak Tamizi Far M.D Isfahan university of medical sciences Definitions Used to Describe the Condition of Septic Patients Approximately 750,000 cases of severe sepsis or septic shock occur
A Care Pathway exists for the management of neutropenic fever. Copies of the care pathway document are available in EAU, A&E, Deanesly and CHU.
 Subject: Neutropenic Fever Guideline for Junior Doctors Date of Implementation: January 2010 Date of Review: January 2012 Director Responsible for Implementation and Review: Policy location: Consultant
Subject: Neutropenic Fever Guideline for Junior Doctors Date of Implementation: January 2010 Date of Review: January 2012 Director Responsible for Implementation and Review: Policy location: Consultant
Aspiration pneumonia in older people
 Aspiration pneumonia in older people Ayman Morish, M.D. Internal medicine, Critical care Medicine and Geriatrics Fellow. Contents Epidemiology Causes of aspiration pneumonia Issues of older age Management
Aspiration pneumonia in older people Ayman Morish, M.D. Internal medicine, Critical care Medicine and Geriatrics Fellow. Contents Epidemiology Causes of aspiration pneumonia Issues of older age Management
CARE OF THE ADULT PNEUMONIA PATIENT
 Care Guideline CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: The target audience for this Care Guideline is all MultiCare providers and staff, including those associated with our clinically integrated
Care Guideline CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: The target audience for this Care Guideline is all MultiCare providers and staff, including those associated with our clinically integrated
Hot Hot Tot:! The Hot Tot. Fever in KIds <90 Days 5/26/10
 Hot Hot Tot:! Fever in KIds
Hot Hot Tot:! Fever in KIds
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A AAP. See American Academy of Pediatrics (AAP) Acyclovir dosing in infants, 185 187 American Academy of Pediatrics (AAP) COFN of, 199 204 Amphotericin
Note: Page numbers of article titles are in boldface type. A AAP. See American Academy of Pediatrics (AAP) Acyclovir dosing in infants, 185 187 American Academy of Pediatrics (AAP) COFN of, 199 204 Amphotericin
Upper...and Lower Respiratory Tract Infections
 Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
Antimicrobial Management of Febrile Neutropenic Sepsis
 Antimicrobial Management of Febrile Neutropenic Sepsis Written by: Dr J Joseph, Consultant Haematologist Dr K Gajee, Consultant Microbiologist Amended by: Larissa Claybourn, Antimicrobial Pharmacist Date:
Antimicrobial Management of Febrile Neutropenic Sepsis Written by: Dr J Joseph, Consultant Haematologist Dr K Gajee, Consultant Microbiologist Amended by: Larissa Claybourn, Antimicrobial Pharmacist Date:
Fever and Infections in Pediatrics
 Fever and Infections in Pediatrics Dr. Todd Twogood 2019 update Big Sky Conference Pediatric Fever and illness The most common reason for children to be taken to the doctor for acute illness Major concern
Fever and Infections in Pediatrics Dr. Todd Twogood 2019 update Big Sky Conference Pediatric Fever and illness The most common reason for children to be taken to the doctor for acute illness Major concern
The Challenge of Managing Staphylococcus aureus Bacteremia
 The Challenge of Managing Staphylococcus aureus Bacteremia M A R G A R E T G R A Y B S P F C S H P C L I N I C A L P R A C T I C E M A N A G E R N O R T H / I D P H A R M A C I S T A L B E R T A H E A
The Challenge of Managing Staphylococcus aureus Bacteremia M A R G A R E T G R A Y B S P F C S H P C L I N I C A L P R A C T I C E M A N A G E R N O R T H / I D P H A R M A C I S T A L B E R T A H E A
Central Venous Access Devices and Infection
 Central Venous Access Devices and Infection Dr Andrew Daley Microbiology & Infectious Diseases Women s & Children s Health Melbourne Background Types of infection! Local site infection! Blood stream infection!
Central Venous Access Devices and Infection Dr Andrew Daley Microbiology & Infectious Diseases Women s & Children s Health Melbourne Background Types of infection! Local site infection! Blood stream infection!
PILOT STUDY PROPOSAL FOR EARLY DISCHARGE OF LOW-RISK NEUTROPENIC PATIENTS
 PILOT STUDY PROPOSAL FOR EARLY DISCHARGE OF LOW-RISK NEUTROPENIC PATIENTS RATIONALE: It is increasingly being recognised that not all neutropenic patients have the same risk of complications during episodes
PILOT STUDY PROPOSAL FOR EARLY DISCHARGE OF LOW-RISK NEUTROPENIC PATIENTS RATIONALE: It is increasingly being recognised that not all neutropenic patients have the same risk of complications during episodes
Fraser Health pandemic preparedness
 Fraser Health pandemic preparedness DRAFT Last revised: April 2006 General Management of Patients in Acute Care Facilities During an Influenza Pandemic 1. OVERVIEW GENERAL MANAGEMENT OF PATIENTS IN ACUTE
Fraser Health pandemic preparedness DRAFT Last revised: April 2006 General Management of Patients in Acute Care Facilities During an Influenza Pandemic 1. OVERVIEW GENERAL MANAGEMENT OF PATIENTS IN ACUTE
Prevention of Important HAIs: Principle & Case Scenario in VAP/CAUTI. CPT. Pasri Maharom MD, MPH Dec 15, 2015
 Prevention of Important HAIs: Principle & Case Scenario in VAP/CAUTI CPT. Pasri Maharom MD, MPH Dec 15, 2015 Catheter Associated Urinary Tract Infection CAUTI CAUTI Epidemiology Key Principles of Preventing
Prevention of Important HAIs: Principle & Case Scenario in VAP/CAUTI CPT. Pasri Maharom MD, MPH Dec 15, 2015 Catheter Associated Urinary Tract Infection CAUTI CAUTI Epidemiology Key Principles of Preventing
Community Acquired & Nosocomial Pneumonias
 Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Osteomyelitis Samir S. Shah, MD, MSCE
 Osteomyelitis Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending Physician in Infectious Diseases
Osteomyelitis Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending Physician in Infectious Diseases
Infections In Cirrhotic patients. Dr Abid Suddle Institute of Liver Studies King s College Hospital
 Infections In Cirrhotic patients Dr Abid Suddle Institute of Liver Studies King s College Hospital Infection in cirrhotic patients Leading cause morbidity/mortality Common: 30-40% of hospitalised cirrhotic
Infections In Cirrhotic patients Dr Abid Suddle Institute of Liver Studies King s College Hospital Infection in cirrhotic patients Leading cause morbidity/mortality Common: 30-40% of hospitalised cirrhotic
Use of Antifungal Drugs in the Year 2006"
 Use of Antifungal Drugs in the Year 2006" Jose G. Montoya, MD Associate Professor of Medicine Associate Chief for Clinical Affairs Division of Infectious Diseases Stanford University School of Medicine
Use of Antifungal Drugs in the Year 2006" Jose G. Montoya, MD Associate Professor of Medicine Associate Chief for Clinical Affairs Division of Infectious Diseases Stanford University School of Medicine
Comparison of Meropenem with Ceftazidime as Monotherapy of Cancer Patients with Chemotherapy induced Febrile Neutropenia
 Comparison of Meropenem with Ceftazidime as Monotherapy of Cancer Patients with Chemotherapy induced Febrile Neutropenia I. Malik ( National Cancer lnsititute, Karachi ) Shaharyar (, Department of Radiotherapy
Comparison of Meropenem with Ceftazidime as Monotherapy of Cancer Patients with Chemotherapy induced Febrile Neutropenia I. Malik ( National Cancer lnsititute, Karachi ) Shaharyar (, Department of Radiotherapy
URINARY TRACT INFECTIONS 3 rd Y Med Students. Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan
 URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile.. It contains fluids, salts, and waste products,
URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile.. It contains fluids, salts, and waste products,
Changes in Etiologic Microorganisms in Thai Patients with Chemotherapy-Induced Neutropenia and Fever
 Original Article Changes in Etiologic Microorganisms in Thai Patients with Chemotherapy-Induced Neutropenia and Fever Chonticha Auesomwang MD 1, Bundarika Suwannawiboon MD 2, Methee Chayakulkeeree MD,
Original Article Changes in Etiologic Microorganisms in Thai Patients with Chemotherapy-Induced Neutropenia and Fever Chonticha Auesomwang MD 1, Bundarika Suwannawiboon MD 2, Methee Chayakulkeeree MD,
Neutropenic Fever 1 InpatientPediatric Treatment
 Neutropenic Fever InpatientPediatric Treatment (Hematologic Cancers and Stem Cell Patients) te: This algorithm should not be used for patients receiving CAR cell therapy. Page of 8 Patient presents with
Neutropenic Fever InpatientPediatric Treatment (Hematologic Cancers and Stem Cell Patients) te: This algorithm should not be used for patients receiving CAR cell therapy. Page of 8 Patient presents with
Fever in Lupus. 21 st April 2014
 Fever in Lupus 21 st April 2014 Fever in lupus Cause of fever N= 487 % SLE fever 206 42 Infection in SLE 265 54.5 Active SLE and infection 8 1.6 Tumor fever 4 0.8 Miscellaneous 4 0.8 Crucial Question Infection
Fever in Lupus 21 st April 2014 Fever in lupus Cause of fever N= 487 % SLE fever 206 42 Infection in SLE 265 54.5 Active SLE and infection 8 1.6 Tumor fever 4 0.8 Miscellaneous 4 0.8 Crucial Question Infection
Fever in neonates (age 0 to 28 days)
") Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Infections Amenable to OPAT. (Nabin Shrestha + Ajay Mathur)
") 3 Infections Amenable to OPAT (Nabin Shrestha + Ajay Mathur) Decisions regarding outpatient treatment of infections vary with the institution, the prescribing physician, the individual patient s condition
3 Infections Amenable to OPAT (Nabin Shrestha + Ajay Mathur) Decisions regarding outpatient treatment of infections vary with the institution, the prescribing physician, the individual patient s condition
Evidence-based Management of Fever in Infants and Young Children
 Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants
 Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
Objec&ves. Clinical Presenta&on
 Michelle A. Barron, MD Associate Professor of Medicine Division of Infectious Diseases University of Colorado Denver Objec&ves Determine who is at risk for invasive candidiasis. Understand whether prophylaxis
Michelle A. Barron, MD Associate Professor of Medicine Division of Infectious Diseases University of Colorado Denver Objec&ves Determine who is at risk for invasive candidiasis. Understand whether prophylaxis
FEBRILE NEUTROPENIA CURRENT GUIDELINES FOR CHILDREN Alia Zaidi, MD. St. Jude International Outreach Program
 SIOP PODC Supportive Care Education (ICON 2016) Presentation Date: 23 rd January 2016 Recording Link at www.cure4kids.org: https://www.cure4kids.org/ums/home/conference_rooms/enter.php?room=p25oti35nt7
SIOP PODC Supportive Care Education (ICON 2016) Presentation Date: 23 rd January 2016 Recording Link at www.cure4kids.org: https://www.cure4kids.org/ums/home/conference_rooms/enter.php?room=p25oti35nt7
Abdominal Pain. Luke Donnelly, MD Emergency Medicine
 Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
8/11/2015. Febrile neutropenia Bone marrow transplant Immunosuppressant medications
 Dean Van Loo Pharm.D. Febrile neutropenia Bone marrow transplant Immunosuppressant medications Steroids Biologics Antineoplastic Most data from cancer chemotherapy Bone marrow suppression Fever is the
Dean Van Loo Pharm.D. Febrile neutropenia Bone marrow transplant Immunosuppressant medications Steroids Biologics Antineoplastic Most data from cancer chemotherapy Bone marrow suppression Fever is the
Urinary Tract Infections
 Urinary Tract Infections Michelle Eslami, M.D., FACP Professor of Medicine Division of Geriatrics David Geffen SOM at UCLA Urinary Tract Infection (UTI) One of most common infections in outpatient and
Urinary Tract Infections Michelle Eslami, M.D., FACP Professor of Medicine Division of Geriatrics David Geffen SOM at UCLA Urinary Tract Infection (UTI) One of most common infections in outpatient and
Urinary tract infection. Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine
 Urinary tract infection Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine Objectives To differentiate between types of urinary tract infections To recognize the epidemiology of UTI in
Urinary tract infection Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine Objectives To differentiate between types of urinary tract infections To recognize the epidemiology of UTI in
CARDIOVASCULAR CASE-BASED SMALL GROUP DISCUSSION
 MHD I Session VIII Student Copy Page 1 CARDIOVASCULAR CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION VIII OCTOBER 22, 2014 STUDENT COPY MHD I Session VIII Student Copy Page 2 Case 1 Chief Complaint I
MHD I Session VIII Student Copy Page 1 CARDIOVASCULAR CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION VIII OCTOBER 22, 2014 STUDENT COPY MHD I Session VIII Student Copy Page 2 Case 1 Chief Complaint I
An Intriguing Case of Meningitis. Tiffany Mylius MLS (ASCP)
") An Intriguing Case of Meningitis { Tiffany Mylius MLS (ASCP) A 4yo male presents with 2wk history of URI symptoms. On the day of admission, the patient woke up with a HA in the morning, took a nap later
An Intriguing Case of Meningitis { Tiffany Mylius MLS (ASCP) A 4yo male presents with 2wk history of URI symptoms. On the day of admission, the patient woke up with a HA in the morning, took a nap later
DRUG ALLERGIES WT: KG
 DRUG AND TREATMENT Available ONLY at: BMC-B BMC-D BMC-N BMC-S Non Categorized Quality Measure Sepsis Bundle Admit to Inpatient Patient Status: Inpatient, Level of Care: Intensive Care (8), Diagnosis: Please
DRUG AND TREATMENT Available ONLY at: BMC-B BMC-D BMC-N BMC-S Non Categorized Quality Measure Sepsis Bundle Admit to Inpatient Patient Status: Inpatient, Level of Care: Intensive Care (8), Diagnosis: Please
Renal Unit. Catheter Related Bacteraemia Guidelines
 Renal Unit Policy Manager Drew Henderson Policy Group Renal Unit Policy Established 21/01/2014 Policy Review Period/Expiry 21/01/2015 Last Updated 21/01/2014 This policy does apply to Medical/Dental Staff
Renal Unit Policy Manager Drew Henderson Policy Group Renal Unit Policy Established 21/01/2014 Policy Review Period/Expiry 21/01/2015 Last Updated 21/01/2014 This policy does apply to Medical/Dental Staff
Provincial Clinical Knowledge Topic Fever and Neutropenia, Pediatric Acute Care V 1.0
 Provincial Clinical Knowledge Topic Fever and Neutropenia, Pediatric Acute Care V 1.0 2017, Alberta Health Services. This work is licensed under the Creative Commons Attribution-Non-Commercial-No Derivatives
Provincial Clinical Knowledge Topic Fever and Neutropenia, Pediatric Acute Care V 1.0 2017, Alberta Health Services. This work is licensed under the Creative Commons Attribution-Non-Commercial-No Derivatives
Clostridium difficile Infection: Diagnosis and Management
 Clostridium difficile Infection: Diagnosis and Management Brian Viviano D.O. Case study 42 year old female with history of essential hypertension and COPD presents to ED complaining of 24 hours of intractable,
Clostridium difficile Infection: Diagnosis and Management Brian Viviano D.O. Case study 42 year old female with history of essential hypertension and COPD presents to ED complaining of 24 hours of intractable,
 Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Cornely OA, Maertens J, Winston DJ, et al. Posaconazole vs.
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Cornely OA, Maertens J, Winston DJ, et al. Posaconazole vs.
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal catastrophes in ICU, 1017 1044. See also specific types, e.g., Abdominal compartment syndrome treatment of, 1032 1037 antimicrobial,
Index Note: Page numbers of article titles are in boldface type. A Abdominal catastrophes in ICU, 1017 1044. See also specific types, e.g., Abdominal compartment syndrome treatment of, 1032 1037 antimicrobial,
MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
 MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSP There are no translations available. MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSP There are no translations available. MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
Objectives. Pneumonia. Pneumonia. Epidemiology. Prevalence 1/7/2012. Community-Acquired Pneumonia in infants and children
 Objectives Community-Acquired in infants and children Review of Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America - 2011 Sabah Charania,
Objectives Community-Acquired in infants and children Review of Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America - 2011 Sabah Charania,
MDR AGENTS: RISK FACTORS AND THERAPEUTIC STRATEGIES
 MDR AGENTS: RISK FACTORS AND THERAPEUTIC STRATEGIES 1 Marin H. Kollef, MD Professor of Medicine Virginia E. and Sam J. Golman Chair in Respiratory Intensive Care Medicine Washington University School of
MDR AGENTS: RISK FACTORS AND THERAPEUTIC STRATEGIES 1 Marin H. Kollef, MD Professor of Medicine Virginia E. and Sam J. Golman Chair in Respiratory Intensive Care Medicine Washington University School of
BC Cancer Protocol Summary for the Maintenance Therapy of Multiple Myeloma Using Bortezomib for Patients with the High-Risk Chromosome Abnormality
 BC Cancer Protocol Summary for the Maintenance Therapy of Multiple Myeloma Using Bortezomib for Patients with the High-Risk Chromosome Abnormality Protocol Code Tumour Group Contact Physician MYBORMTN
BC Cancer Protocol Summary for the Maintenance Therapy of Multiple Myeloma Using Bortezomib for Patients with the High-Risk Chromosome Abnormality Protocol Code Tumour Group Contact Physician MYBORMTN