Tips and Tricks for Starting and Adjusting Insulin. MC MacSween The Moncton Hospital
|
|
|
- Reginald Stafford
- 6 years ago
- Views:
Transcription
1 Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital
2 Progression of type 2 diabetes Beta cell apoptosis

3 Natural History of Type 2 Diabetes
4 The Burden of Treatment Failure in Type 2 Diabetes Brown JB. Diabetes Care July % 8% 7% Patients spend on average of 59 months on dual oral agents with A1C > 7.0% before insulin is initiated

5 Physiologic Insulin Secretion

6 Bottom Line It s Definitely Time to Start Insulin If : Decompensated diabetes i.e. if symptomatic hyperglycemia and losing weight. A1C > 9.5%, FBG > 14 mmol/l, insulin is required. Preconception Type 2 Diabetes.



7 Decompensated Diabetes +/- Metformin May be short term insulin; 4-6 weeks if turns out to be new T2D. Send GAD Antibodies if age < 40 or lean.
8 Bottom Line Consider Insulin if : If A1C >8.5% on pharmacologic therapy. Ideally initiate insulin when A1C < 8.5% on oral agents so able to start with fewer injections and simplified regime. If contraindication or intolerances to multiple oral agents limits therapy (i.e. renal insufficiency).
9 Oral Agents and Insulin Initiation What to Keep and What to Stop Unless contraindicated, Metformin is usually continued to decrease variability of morning glucose and to mitigate weight gain on insulin. May wean other oral agents if doing well on moderate doses of insulin. Secretagogues (i.e. SU s) should be stopped once on meal insulin.
10 Choices of Insulin Regimes Basal intermediate or basal analog at hs. Basal Plus 1-2 meal doses of rapid insulin. Premix rapid. Basal bolus (MDI).
11 Basal Insulins: Intermediate Acting Humulin N, Novolin NPH: cloudy due to preservatives that allow prolonged action so half life is hours. Less than half the price of basal analogues and no difference in A1C but some increase in nocturnal hypoglycemia. Must mix properly before injection by rolling and rotating pen 20 x or will risk hypoglycemia. 20% coefficient of variation in effect so try to avoid in type 1 diabetes. Vial (1000 units) is $20 or 5 cartridges (1500 units) $8.50 each and $42 for pack of 5. is
12 Basal Analogues Basalglar (biosimilar glargine, $15 per cartridge), Lantus (glargine, $18.50 per cartridge), Levemir (detemir $20). Smoother 24 hour profile with somewhat less nocturnal hypoglyemia vs. intermediate acting insulin. Clear, so no mixing required and can be given AM or HS. Levemir has a shorter half life so may need BID. More weight favorable but most expensive basal analog.
13 Rapid Acting Insulins Apidra (glulisine $10 per cartridge), Humalog (lispro, $11 per cartridge), NovoRapid (aspart $12 per cartridge). Often helpful to give minutes ac unless glucose <5. Health Canada recent approval of faster insulin aspart, Fiasp. Concentrated insulins



14 Injection Technique: 4 mm Pen Needles and Site Rotation Leave needle in seconds after injection

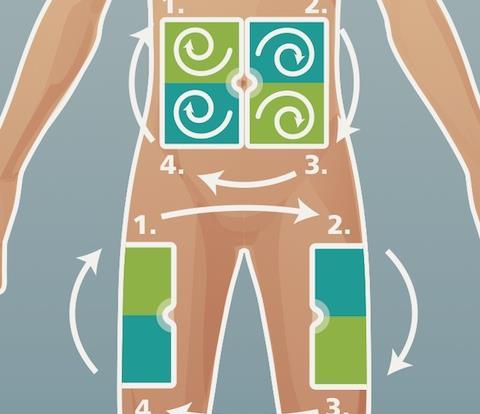

15 Injection Technique: Site Rotation
16 Starting Basal Insulin Not very useful if the AM glucose is the best of the day lean elderly more insulin deficient than resistant). Least weight gain and hypoglycemia vs. other regimes. Usual starting dose is 10 units NPH, N, Lantus, Levemir or Basalglar. Titrate up by 1 unit every night until fasting glucose is 5-6 mmol/l. No further dose increase if 1 nocturnal low or 2 morning lows. Average hs NPH dose (+ daytime Metformin) is 42 units. Average Lantus dose 47 units but 30% require > 60 units. (i.e.
17 Pitfalls Very high dose glargine (Lantus) units and persistent daytime hyperglycemia (? max 0.5 u/kg). Likely needs 1-3 meal doses if glucose falls significantly overnight (BeAM factor > 3 mmol/l). Beware the catecholamine effect of untreated OSA causing increasing overnight glucose. Often can reduce very high Lantus dose 20% -30% and use this amount of insulin for divided meal doses.

18 Predicting Success of Daytime Oral Agents and Bedtime Insulin Baseline A1C < 8.5% Baseline A1C > 8.5% 75% get to goal 45% get to goal Consider Basal plus One
19 Insulin Initiation: Multiple Injections Premix Analogs MDI Humalog Mix 25 and Mix 50 and NovaMix 30. Start 6-10 units BID (ac bkft and ac supper) and titrate morning dose based on before supper readings and evening dose based on AM readings. Must have stable meals and activity. No adjustment scale possible units/kg total daily dose. Use lower range if elderly, lean or renal insufficiency. 40% basal and 20% each meal. Most flexible regime but 4 injections per day. Preferred regime for Type 1 diabetes where starting dose should be 0.5 u/kg.
20 Meal Insulin Type 2 Diabetes: usually don t need carb counting can often give a range i.e. 10 units for a small meal and 15 units for a large meal. In insulin resistance often helpful to give rapid acting meal dose minutes before the meal rather than progressively increase the dose and provoke further weight gain.
.")
21 Coming Soon: Basal GLP-1 Agonist Combinations Lantus Lixisenatide (LixiLan). Degludec Liraglutide (ideglira). GLP-1 mitigates the weight gain of insulin with excellent A1C lowering effect.
22 Monday 45 year old woman came to Sackville ER with blurry vision. Polyuria, nocturia and some weight loss over past 3 weeks. Weight 60 kg. Blood glucose 37 mmol/l. What s your management? Start MDI with 0.5 units/kg (30 units/d) with 40% basal i.e. 12 units and remainder divided for meals i.e. 6 units per meal
23 Wednesday 66 year old male with T2DM on Metformin, Diamicron MR and A1C 9.0%. Weight 102 kg and BMI 39. Doesn t want to gain more weight. Doesn t want low blood sugars. Mild gastroparesis.

24
25
26 Correct Treatment HYPOGLYCEMIA
:102-2013 Elderly on Insulin Mini Cog Clock drawing test can be used to predict who is likely to have problems")
27 Trimble LA et al. Can J Diabetes 2005;29(2): Elderly on Insulin Mini Cog Clock drawing test can be used to predict who is likely to have problems with insulin therapy Write numbers on the blank clock face and draw hands on the clock to show 10 minutes past 11 o clock
28 Diabetes in the Elderly 2013 Checklist INDIVIDUALIZE glycemic targets based on the above (A1C 8.5% for frail elderly) but if otherwise healthy, use the same targets as younger people AVOID hypoglycemia in cognitive impairment SELECT antihyperglycemic therapy carefully caution with sulfonylureas or thiazolidinediones Basal analogues instead of NPH or human 30/70 insulin Premixed insulins instead of mixing insulins separately in syringe. GIVE regular diets instead of diabetic diets or nutritional formulas in nursing homes


29 Diabetes in the frail and not so frail elderly Lean elderly are usually insulin deficient not insulin resistant so basal insulin alone often not very useful. Caution in stopping longstanding insulin C-peptide.


30 Blood Glucose Meter with Rapid Acting Insulin Calculator (InsuLinx)

31 Memory Pens for NovoRapid

32 Libre Glucose Monitor
33 Summary: Insulin ADVANTAGES Long-term experience No maximal dose Multiple formulations and regimens No contraindications DISADVANTAGES Injection Hypoglycemia risk Weight gain Increased cost of SMBG No increased CV or cancer risk SMBG= Self-monitoring of blood glucose Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Can J Diabetes 2013;37(suppl 1):S1-S212. Origin Trial Investigators. NEJM 2012.;367(4):
34 Bottom Line It s Definitely Time to Start Insulin if : Decompensated diabetes i.e. if symptomatic hyperglycemia and losing weight. A1C > 9.5%, FBG > 14 mmol/l, insulin is required. Preconception Type 2 Diabetes.
35 Starting Basal Insulin Not very useful if the AM glucose is the best of the day (i.e. lean elderly more insulin deficient than resistant). Least weight gain and hypoglycemia vs. other regimes. Usual starting dose is 10 units NPH/N, Lantus, Levemir or Basalglar. Titrate up by 1 unit every night until fasting glucose is 5-6 mmol/l. No further dose increase if 1 nocturnal low or 2 morning lows. Average hs NPH dose (+ daytime Metformin) is 42 units. Average Lantus dose 47 units but 30% require > 60 units.
36 Pitfalls Very high dose glargine (Lantus) units and persistent daytime hyperglycemia (? max effect 0.5 u/kg). Likely needs 1-3 meal doses if glucose falls significantly overnight (BeAM factor > 3 mmol/l). Basal Plus 1. Beware the catecholamine effect of untreated OSA causing increasing overnight glucose. Often can reduce Lantus dose 20% -30% and use this amount of insulin for divided meal doses.
37 Insulin Initiation: Multiple Injections Premix Analogs MDI Humalog Mix 25 and Mix 50 and NovaMix 30. Start 6-10 units BID (ac bkft and ac supper) and titrate morning dose based on before supper readings and evening dose based on AM readings. Must have stable meals and activity. No adjustment scale possible. Highest rate of weight gain hypoglycemia and least efficacious at A1C lowering units/kg total daily dose. Use lower range if elderly, lean or renal insufficiency. 40% basal and 20% each meal. Most flexible regime but 4 injections per day. Preferred regime for Type 1 diabetes where starting dose should be 0.5 u/kg.
 and may reduce basal dose.")
38 Meal Insulin Type 2 Diabetes: usually don t need carb counting can often give a range i.e. 10 units for a small meal and 15 units for a large meal. Can start at 6 units per meal but if already on a large dose of basal can often start 0.1 unit/kg/meal (i.e. 90 kg start 9 units per meal) and may reduce basal dose. In insulin resistance often helpful to give rapid acting meal dose minutes before the meal rather than progressively increase the dose and provoke further weight gain (unless insulin Fiasp).
39 Bottom Line Consider Insulin if : If A1C >8.5% on pharmacologic therapy. Ideally initiate insulin when A1C < 8.5% on oral agents so able to start with fewer injections and simplified regime. If contraindications or intolerances to multiple oral agents limits therapy (i.e. renal insufficiency).
40 Basal Analogues Basalglar (biosimilar glargine, $15 per cartridge), Lantus (glargine, $18.50 per cartridge), Levemir (detemir $20). Smoother 24 hour profile with somewhat less nocturnal hypoglyemia vs. intermediate acting insulin. Clear, so no mixing required and can be given AM or HS. Levemir has a shorter half life so may need BID. More weight favorable but most expensive basal analog. Concentrated U300 glargine (Toujeo) need 14% higher dose.
41 Rapid Acting Insulins Apidra (glulisine $10 per cartridge), Humalog (lispro, $11 per cartridge), NovoRapid (aspart $12 per cartridge). Often helpful to give minutes ac unless glucose <5. Health Canada recent approval of faster insulin aspart, Fiasp. Targeted for type 1 diabetes on MDI. Advantage of faster onset so can give immediately ac or even pc meals. Concentrated insulin Humalog U200 in unique pen.
INSULIN 101: When, How and What
 INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Diabetes Head to Toe May 31, 2017
 Innovations in Insulin Joanne Reid RN CDE jmreid@gbhs.on.ca Danielle Benedict RPh Outline Setting the stage Insulin as pancreas replacement therapy Commonly used insulins New insulins Case Studies Dosing
Innovations in Insulin Joanne Reid RN CDE jmreid@gbhs.on.ca Danielle Benedict RPh Outline Setting the stage Insulin as pancreas replacement therapy Commonly used insulins New insulins Case Studies Dosing
Newer Insulins. Boca Raton Regional Hospital 15th Annual Internal Medicine Conference
 Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Guide to Starting and Adjusting Insulin for Type 2 Diabetes*
 Guide to Starting and Adjusting Insulin for Type 2 Diabetes* www.cadth.ca * Adapted from Guide to Starting and Adjusting Insulin for Type 2 Diabetes, 2008 International Diabetes Center, Minneapolis, MN.
Guide to Starting and Adjusting Insulin for Type 2 Diabetes* www.cadth.ca * Adapted from Guide to Starting and Adjusting Insulin for Type 2 Diabetes, 2008 International Diabetes Center, Minneapolis, MN.
Objectives. Navigating New Insulins. Disclosures. Diabetes: The Stats. Normal Insulin Release Individuals without diabetes. History of Insulin 5/23/17
 Objectives Compare and contrast currently available products. Navigating New s Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Diabetes Center Determine the factors
Objectives Compare and contrast currently available products. Navigating New s Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Diabetes Center Determine the factors
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES
 PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
Learning Objectives. Are you ready for more insulin formulations?
 Are you ready for more insulin formulations? Shara Elrod, PharmD, BCACP, BCGP Learning Objectives Review pharmacology and dosing of new insulin formulations Compare and contrast new insulin formulations
Are you ready for more insulin formulations? Shara Elrod, PharmD, BCACP, BCGP Learning Objectives Review pharmacology and dosing of new insulin formulations Compare and contrast new insulin formulations
Update on Insulin-based Agents for T2D
 Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Mixed Insulins Pick Me
 Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
In-Hospital Management of Diabetes. Dr Benjamin Schiff Assistant Professor McGill University
 In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
Initiation and Titration of Insulin in Diabetes Mellitus Type 2
 Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES
 PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
Insulin Prior Authorization with optional Quantity Limit Program Summary
 Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Short-acting insulins. Biphasic insulins. Intermediate- and long-acting insulins
 Recommended Insulin Products This guideline states the Gloucestershire Joint Formulary recommended, first choice insulin products. The intention is to support the choice of treatment for new patients,
Recommended Insulin Products This guideline states the Gloucestershire Joint Formulary recommended, first choice insulin products. The intention is to support the choice of treatment for new patients,
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Disclosure 1/16/2017. Michael R. Brennan D.O., M.S., F.A.C.E Director Beaumont Endocrine Center Chief of Endocrine Beaumont Grosse Pointe 1/16/2017 2
 Therapy For Diabetes Michigan Association of Osteopathic Family Physicians Mid-Winter Family Medicine Update Shanty Creek Resort, MI January 19-22nd 2017 Michael R. Brennan D.O., M.S., F.A.C.E Director
Therapy For Diabetes Michigan Association of Osteopathic Family Physicians Mid-Winter Family Medicine Update Shanty Creek Resort, MI January 19-22nd 2017 Michael R. Brennan D.O., M.S., F.A.C.E Director
Position Statement of ADA / EASD 2012
 Management of Hyperglycemia in Type2 Diabetes: A Patient- Centered Approach Position Statement of ADA / EASD 2012 Cause of : Type 2 diabetes Cardiovascular disorders Blindness End-stage renal failure Amputations
Management of Hyperglycemia in Type2 Diabetes: A Patient- Centered Approach Position Statement of ADA / EASD 2012 Cause of : Type 2 diabetes Cardiovascular disorders Blindness End-stage renal failure Amputations
Basal Bolus Insulin Therapy Frequently Asked Questions
 1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
What the Pill Looks Like. How it Works. Slows carbohydrate absorption. Reduces amount of sugar made by the liver. Increases release of insulin
 Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Initiation and Adjustment of Insulin Regimens for Type 2 Diabetes
 Types of Insulin Rapid-acting insulin: lispro (Humalog), aspart (NovoRapid), glulisine (Apidra) Regular short-acting insulin: Humulin R, Novolin ge Toronto, Hypurin Regular Basal insulin: NPH (Humulin
Types of Insulin Rapid-acting insulin: lispro (Humalog), aspart (NovoRapid), glulisine (Apidra) Regular short-acting insulin: Humulin R, Novolin ge Toronto, Hypurin Regular Basal insulin: NPH (Humulin
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
UKPDS: Over Time, Need for Exogenous Insulin Increases
 UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
Objectives 2/13/2013. Figuring out the dose. Sub Optimal Glycemic Control: Moving to the Appropriate Treatment
 Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
LET S TALK INSULIN THE BASICS
 LET S TALK INSULIN THE BASICS AUTHOR S DISCLOSURES Contracted for program development for Lifescan Canada Speaker for Lifescan, Lilly, BI, Consultant for Lilly, Janssen, Novo Nordisk, Lifescan Canada OBJECTIVES
LET S TALK INSULIN THE BASICS AUTHOR S DISCLOSURES Contracted for program development for Lifescan Canada Speaker for Lifescan, Lilly, BI, Consultant for Lilly, Janssen, Novo Nordisk, Lifescan Canada OBJECTIVES
Timely!Insulinization In!Type!2! Diabetes,!When!and!How
 Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
New Therapies for Diabetes Management: Hope or Headache?
 New Therapies for Diabetes Management: Hope or Headache? Elizabeth Stephens, MD, FACP PMG- Endocrinology Elizabeth.Stephens@providence.org November 2018 Disclosures None 1 Objectives Discussion of 3 rd
New Therapies for Diabetes Management: Hope or Headache? Elizabeth Stephens, MD, FACP PMG- Endocrinology Elizabeth.Stephens@providence.org November 2018 Disclosures None 1 Objectives Discussion of 3 rd
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE
 INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Basal-Bolus Insulin Therapy. Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January
 Basal-Bolus Insulin Therapy Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January 18 2018 Terminology No longer using the term diabetic. Diabetes does not define people. People with diabetes are individuals
Basal-Bolus Insulin Therapy Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January 18 2018 Terminology No longer using the term diabetic. Diabetes does not define people. People with diabetes are individuals
Converting lantus to humalog 75 25
 P ford residence southampton, ny Converting lantus to humalog 75 25 This page includes the following topics and synonyms: Insulin Dosing in Type 2 Diabetes, Insulin Dosing in Type II Diabetes. Thiazide
P ford residence southampton, ny Converting lantus to humalog 75 25 This page includes the following topics and synonyms: Insulin Dosing in Type 2 Diabetes, Insulin Dosing in Type II Diabetes. Thiazide
Starting and Helping People with Type 2 Diabetes on Insulin
 Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy
 Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy Jerry Meece, BPharm, CDE, FACA, FAADE Director of Clinical Services Plaza Pharmacy and Wellness Center Gainesville,
Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy Jerry Meece, BPharm, CDE, FACA, FAADE Director of Clinical Services Plaza Pharmacy and Wellness Center Gainesville,
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
Nph insulin conversion to lantus
 Nph insulin conversion to lantus Search 26-2-2003 RESPONSE FROM AVENTIS. We appreciate the opportunity to respond to Dr. Grajower s request for information regarding Lantus ( insulin glargine [rdna origin.
Nph insulin conversion to lantus Search 26-2-2003 RESPONSE FROM AVENTIS. We appreciate the opportunity to respond to Dr. Grajower s request for information regarding Lantus ( insulin glargine [rdna origin.
Insulin Management. By Susan Henry Diabetes Specialist Nurse
 Insulin Management By Susan Henry Diabetes Specialist Nurse The Discovery of Insulin - 1921 - Banting & Best University Of Toronto Discovered hormone insulin in pancreatic extract of dog - Marjorie the
Insulin Management By Susan Henry Diabetes Specialist Nurse The Discovery of Insulin - 1921 - Banting & Best University Of Toronto Discovered hormone insulin in pancreatic extract of dog - Marjorie the
Management of Diabetes New Concepts New Devices New Medications. Richard J. Comi, MD Professor of Medicine Geisel School of Medicine at Dartmouth
 Management of Diabetes New Concepts New Devices New Medications Richard J. Comi, MD Professor of Medicine Geisel School of Medicine at Dartmouth Objectives: At the end of this lecture, the learner will
Management of Diabetes New Concepts New Devices New Medications Richard J. Comi, MD Professor of Medicine Geisel School of Medicine at Dartmouth Objectives: At the end of this lecture, the learner will
What s New in Type 1 and Type 2 Diabetes? Updates from 2013 CDA CPGs and Advancements in Insulin Therapy
 What s New in Type 1 and Type 2 Diabetes? Updates from 2013 CDA CPGs and Advancements in Insulin Therapy 2013 Rocky Mountain/ACP Internal Medicine Conference November 15, 2013 David C.W. Lau, MD, PhD,
What s New in Type 1 and Type 2 Diabetes? Updates from 2013 CDA CPGs and Advancements in Insulin Therapy 2013 Rocky Mountain/ACP Internal Medicine Conference November 15, 2013 David C.W. Lau, MD, PhD,
Inpatient Glycemic Management:
 Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations
 177 TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary Coverage Indication for use with: INSULIN THERAPY NS NB NL PE ADULTS PEDIATRICS PREGNANCY BOLUS
177 TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary Coverage Indication for use with: INSULIN THERAPY NS NB NL PE ADULTS PEDIATRICS PREGNANCY BOLUS
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations
 177 TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary
177 TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary
Insulin 301: Case, after case, after case
 Insulin 301: Case, after case, after case Learning objectives By the end of this session, you will be able to : 1. List the 3 types of insulin, 3 insulin regimens and pros/cons of each 2. Select the regimen
Insulin 301: Case, after case, after case Learning objectives By the end of this session, you will be able to : 1. List the 3 types of insulin, 3 insulin regimens and pros/cons of each 2. Select the regimen
Individualizing Care for Patients with Type 2 Diabetes
 Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Table 1. Antihyperglycemic agents for use in type 2 diabetes
 Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
BRIAN MOSES, MD, FRCPC (INTERNAL MEDICINE) CHIEF OF MEDICINE, SOUTH WEST HEALTH
 CHIEF OF MEDICINE, SOUTH WEST HEALTH") Insulin Initiation BRIAN MOSES, MD, FRCPC (INTERNAL MEDICINE) CHIEF OF MEDICINE, SOUTH WEST HEALTH Disclosures In the past 12 months, I have received speakers honoraria from AstraZeneca, Boehringer Ingelheim,
Insulin Initiation BRIAN MOSES, MD, FRCPC (INTERNAL MEDICINE) CHIEF OF MEDICINE, SOUTH WEST HEALTH Disclosures In the past 12 months, I have received speakers honoraria from AstraZeneca, Boehringer Ingelheim,
Sponsor / Company: Sanofi Drug substance(s): insulin glargine (HOE901) According to template: QSD VERSION N 4.0 (07-JUN-2012) Page 1
: insulin glargine (HOE901) According to template: QSD VERSION N 4.0 (07-JUN-2012) Page 1") These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
8/21/2017 UNRAVELING THE CROWED INSULIN SCENE. A Practical Overview of Insulin Focusing on New Insulin Preparations
 UNRAVELING THE CROWED INSULIN SCENE A Practical Overview of Insulin Focusing on New Insulin Preparations Patricia Garnica MS, ANP-BC, CDE, CDTC North Shore University Hospital, Manhasset, N.Y. October
UNRAVELING THE CROWED INSULIN SCENE A Practical Overview of Insulin Focusing on New Insulin Preparations Patricia Garnica MS, ANP-BC, CDE, CDTC North Shore University Hospital, Manhasset, N.Y. October
Injecting Insulin into Out Patient Practice
 Injecting Insulin into Out Patient Practice Kathleen Colleran, MD Associate Professor UNMHSC 4/22/10 Overview Natural history of Type 2 diabetes Reasons clinicians are reluctant to start insulin therapy
Injecting Insulin into Out Patient Practice Kathleen Colleran, MD Associate Professor UNMHSC 4/22/10 Overview Natural history of Type 2 diabetes Reasons clinicians are reluctant to start insulin therapy
Type I Type II Insulin Resistance
 Insulin An aqueous hormonal solution made in the pancreas. Affects metabolism by allowing glucose to leave the blood and enter the body cells, preventing hyperglycemia. It is measured in units, e.g. 100
Insulin An aqueous hormonal solution made in the pancreas. Affects metabolism by allowing glucose to leave the blood and enter the body cells, preventing hyperglycemia. It is measured in units, e.g. 100
MANAGEMENT OF TYPE 1 DIABETES MELLITUS
 MANAGEMENT OF TYPE 1 DIABETES MELLITUS INVESTIGATIONS AND TREATMENT MANSI NAIK VII SEMESTER INVESTIGATIONS FASTING BLOOD SUGAR PLASMA GLUCOSE HEMOGLOBIN A 1c SYMPTOMS OF TYPE 1 DIABETES MELLITUS Polyuria
MANAGEMENT OF TYPE 1 DIABETES MELLITUS INVESTIGATIONS AND TREATMENT MANSI NAIK VII SEMESTER INVESTIGATIONS FASTING BLOOD SUGAR PLASMA GLUCOSE HEMOGLOBIN A 1c SYMPTOMS OF TYPE 1 DIABETES MELLITUS Polyuria
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION
 INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
Type 2 Diabetes Mellitus Insulin Therapy 2012
 Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
DEMYSTIFYING INSULIN THERAPY
 DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
Diana McNeill MD, FACP Professor of Medicine Duke University Medical Center. Disclosures
 Insulin Therapy in Diabetes So Many Choices Diana McNeill MD, FACP Professor of Medicine Duke University Medical Center Disclosures Mytonomy-consultant Quantia webinars Acknowledgements: Dr. Sue Kirkman-UNC-
Insulin Therapy in Diabetes So Many Choices Diana McNeill MD, FACP Professor of Medicine Duke University Medical Center Disclosures Mytonomy-consultant Quantia webinars Acknowledgements: Dr. Sue Kirkman-UNC-
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC)
") BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC) June 2017 Review: June 2020 (earlier if required see recommendations) Bulletin 255: Insulin aspart New Formulation - Fiasp JPC Recommendations:
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC) June 2017 Review: June 2020 (earlier if required see recommendations) Bulletin 255: Insulin aspart New Formulation - Fiasp JPC Recommendations:
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Premixed Insulin for Type 2 Diabetes. a gu i d e f o r a d u lt s
 Premixed Insulin for Type 2 Diabetes a gu i d e f o r a d u lt s March 2009 What This Guide Covers / 2 Type 2 Diabetes / 3 Learning About Blood Sugar / 4 Learning About Insulin / 5 Comparing Medicines
Premixed Insulin for Type 2 Diabetes a gu i d e f o r a d u lt s March 2009 What This Guide Covers / 2 Type 2 Diabetes / 3 Learning About Blood Sugar / 4 Learning About Insulin / 5 Comparing Medicines
These Aren t Your Average Rookies: A Primer on New and Emerging Insulins. Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP
 These Aren t Your Average Rookies: A Primer on New and Emerging Insulins Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP Disclosures Eli Lilly & Company: Advisory board member Boehringer Ingelheim: Advisory
These Aren t Your Average Rookies: A Primer on New and Emerging Insulins Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP Disclosures Eli Lilly & Company: Advisory board member Boehringer Ingelheim: Advisory
5/16/2018. Insulin Update: New and Emerging Insulins. Disclosures to Participants. Learning Objectives
 Insulin Update: New and Emerging Insulins Joshua J. Neumiller, PharmD, CDE, FASCP Vice Chair & Associate Professor, Department of Pharmacotherapy Washington State University Spokane, WA Disclosures to
Insulin Update: New and Emerging Insulins Joshua J. Neumiller, PharmD, CDE, FASCP Vice Chair & Associate Professor, Department of Pharmacotherapy Washington State University Spokane, WA Disclosures to
4/16/2018. Flexible Intensive Insulin Therapy (FIIT) in People with Type 2 Diabetes: A Viable Option. Disclosures. Outline. No financial disclosures
 in People with Type 2 Diabetes: A Viable Option. Disclosures. Outline. No financial disclosures") Flexible Intensive Insulin Therapy (FIIT) in People with Type Diabetes: A Viable Option Kim Bisanz, MFCS, RDN, LDN, CDE Minnesota Academy of Nutrition & Dietetics Annual Meeting April 19, 18 18 MFMER slide-1
Flexible Intensive Insulin Therapy (FIIT) in People with Type Diabetes: A Viable Option Kim Bisanz, MFCS, RDN, LDN, CDE Minnesota Academy of Nutrition & Dietetics Annual Meeting April 19, 18 18 MFMER slide-1
3. Cardiovascular Disease?
 Swiss recommendations 2016 Swiss Society of Endocrinology and Diabetology 1. Deficiency? Basal Premixed- Basal + GLP-1 RA (Xultophy ) or Basal Bolus 2. egfr < 30 ml/min? 3. Cardiovascular Disease? 4. Heart
Swiss recommendations 2016 Swiss Society of Endocrinology and Diabetology 1. Deficiency? Basal Premixed- Basal + GLP-1 RA (Xultophy ) or Basal Bolus 2. egfr < 30 ml/min? 3. Cardiovascular Disease? 4. Heart
New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection
 New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection Date of Review: March 2016 End Date of Literature Search: November 11, 2015 Generic Name: Insulin degludec and insulin aspart Brand
New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection Date of Review: March 2016 End Date of Literature Search: November 11, 2015 Generic Name: Insulin degludec and insulin aspart Brand
Intensification of Diabetic Therapy. Case studies
 Intensification of Diabetic Therapy Case studies Patient #1 1 st visit: 64 year old male, H/O prediabetes, lost weight 280 lbs. to 240 lbs. ER for dental abscess, glucose >300 A1C 11.4%, no diabetic medication,
Intensification of Diabetic Therapy Case studies Patient #1 1 st visit: 64 year old male, H/O prediabetes, lost weight 280 lbs. to 240 lbs. ER for dental abscess, glucose >300 A1C 11.4%, no diabetic medication,
Insulin Basics. Bryan Primary Care Conference May 21, 2016 Shannon Wakeley MD Complete Endocrinology
 Insulin Basics Bryan Primary Care Conference May 21, 2016 Shannon Wakeley MD Complete Endocrinology Disclosures Speakers Bureau for Sanofi, Astra Zeneca, Janssen, Boehringer-Ingelheim Objectives Discuss
Insulin Basics Bryan Primary Care Conference May 21, 2016 Shannon Wakeley MD Complete Endocrinology Disclosures Speakers Bureau for Sanofi, Astra Zeneca, Janssen, Boehringer-Ingelheim Objectives Discuss
Injectable Therapies in Diabetes
 Injectable Therapies in Diabetes Diabetes Specialist Nurse Joyce Robson Learning Outcomes Think about the place of injectible therapies in diabetes Insulin therapy GLP1 antagonists Consider commonly used
Injectable Therapies in Diabetes Diabetes Specialist Nurse Joyce Robson Learning Outcomes Think about the place of injectible therapies in diabetes Insulin therapy GLP1 antagonists Consider commonly used
第十五章. Diabetes Mellitus
 Diabetes-1/9 第十五章 Diabetes Mellitus 陳曉蓮醫師 2/9 - Diabetes 羅東博愛醫院 Management of Diabetes mellitus A. DEFINITION OF DIABETES MELLITUS Diabetes Mellitus is characterized by chronic hyperglycemia with disturbances
Diabetes-1/9 第十五章 Diabetes Mellitus 陳曉蓮醫師 2/9 - Diabetes 羅東博愛醫院 Management of Diabetes mellitus A. DEFINITION OF DIABETES MELLITUS Diabetes Mellitus is characterized by chronic hyperglycemia with disturbances
Important Stuff. Basal Bolus What Adjustments? Pt weighs 80kg
 Diabetes Boot Camp Class 4 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Special Insulin and Pattern Management Diabetes Education Services 1998-2015. All rights
Diabetes Boot Camp Class 4 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Special Insulin and Pattern Management Diabetes Education Services 1998-2015. All rights
Self-Monitoring Blood Glucose (SMBG) Frequency & Pattern Tool
 Frequency & Pattern Tool") Self-Monitoring Blood Glucose () Pattern Recommendation: Basal Insulin Only (To Target) NPH or long-acting analogue, typically given at. at least as often as is being given. Optional, less frequent can
Self-Monitoring Blood Glucose () Pattern Recommendation: Basal Insulin Only (To Target) NPH or long-acting analogue, typically given at. at least as often as is being given. Optional, less frequent can
The York Diabetes Care Model
 This Session The York Diabetes Care Model The annual review what s it for and how to do it How to make the diagnosis of diabetes and who to test Categorisation of diabetes at diagnosis Basics of Insulin
This Session The York Diabetes Care Model The annual review what s it for and how to do it How to make the diagnosis of diabetes and who to test Categorisation of diabetes at diagnosis Basics of Insulin
BEST 4 Diabetes. Optimisation of insulin module
 BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Module 5. Understanding Insulin Therapy
 Module 5. Understanding Insulin Therapy EDUCATIONAL OBJECTIVES Upon completion of this activity, participants will be better able to: 1. Define the basic physiologic concept of basal-bolus insulin; 2.
Module 5. Understanding Insulin Therapy EDUCATIONAL OBJECTIVES Upon completion of this activity, participants will be better able to: 1. Define the basic physiologic concept of basal-bolus insulin; 2.
APPENDIX American Diabetes Association. Published online at
 APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
Update on Insulin-based Agents for T2D. Harry Jiménez MD, FACE
 Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
BEST 4 Diabetes. Optimisation of insulin module
 BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
Insulin Therapies: An Educational Toolkit
 University Hospitals of Leicester, Department of Diabetes and Leicester Diabetes Centre: Insulin Therapies: An Educational Toolkit This document is designed for use by those trained and competent in insulin
University Hospitals of Leicester, Department of Diabetes and Leicester Diabetes Centre: Insulin Therapies: An Educational Toolkit This document is designed for use by those trained and competent in insulin
ClinicalTrials.gov Identifier: sanofi-aventis. Sponsor/company:
 These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: sanofi-aventis ClinicalTrials.gov
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: sanofi-aventis ClinicalTrials.gov
Insulin Bootcamp: Dosing, Monitoring, Titrating, and Care Coordination. Stuart T. Haines, Pharm.D., BCPS, BCACP, BC ADM
 Insulin Bootcamp: Dosing, Monitoring, Titrating, and Care Coordination Stuart T. Haines, Pharm.D., BCPS, BCACP, BC ADM University of Mississippi School of Pharmacy Joshua J. Neumiller, Pharm.D., CDE, FAADE,
Insulin Bootcamp: Dosing, Monitoring, Titrating, and Care Coordination Stuart T. Haines, Pharm.D., BCPS, BCACP, BC ADM University of Mississippi School of Pharmacy Joshua J. Neumiller, Pharm.D., CDE, FAADE,
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Injectable Therapies in Diabetes
 Injectable Therapies in Diabetes Diabetes Specialist Nurse Linda Burns Learning Outcomes Understand the place of injectible therapies in diabetes Understand when patients may require insulin therapy Consider
Injectable Therapies in Diabetes Diabetes Specialist Nurse Linda Burns Learning Outcomes Understand the place of injectible therapies in diabetes Understand when patients may require insulin therapy Consider
Medications for Diabetes
 Medications for Diabetes Sweet, but not too sweet Colette Raymond, Pharm D June 15, 2011 Learning Objectives At the end of this presentation you should be able to: Understand the prevalence and types of
Medications for Diabetes Sweet, but not too sweet Colette Raymond, Pharm D June 15, 2011 Learning Objectives At the end of this presentation you should be able to: Understand the prevalence and types of
2018 Diabetes Summit Managing Diabetes: An Art and a Science
 2018 Diabetes Summit Managing Diabetes: An Art and a Science Natasha Petry, PharmD, BCACP NDSU College of Health Professions, School of Pharmacy, Department of Pharmacy Practice Patient-Centered Medical
2018 Diabetes Summit Managing Diabetes: An Art and a Science Natasha Petry, PharmD, BCACP NDSU College of Health Professions, School of Pharmacy, Department of Pharmacy Practice Patient-Centered Medical
Insulin Therapy Management. Insulin Therapy
 Insulin Therapy Management Insulin Therapy Contents Insulin and its effect on glycemic control Physiology of insulin secretion Insulin pharmacokinetics and regimens Insulin dose adjustment for pregnancy
Insulin Therapy Management Insulin Therapy Contents Insulin and its effect on glycemic control Physiology of insulin secretion Insulin pharmacokinetics and regimens Insulin dose adjustment for pregnancy
Case Study: Competitive exercise
 Case Study: Competitive exercise 32 year-old cyclist Type 1 diabetes since age 15 Last HbA1 54 No complications and hypo aware On Humalog 8/8/8 and Levemir 15 Complains about significant hypoglycaemia
Case Study: Competitive exercise 32 year-old cyclist Type 1 diabetes since age 15 Last HbA1 54 No complications and hypo aware On Humalog 8/8/8 and Levemir 15 Complains about significant hypoglycaemia
Pediatric Diabetes Update Fran R. Cogen, MD, CDE Professor of Pediatrics Director, Diabetes Services
 1.19.18 Pediatric Diabetes Update Fran R. Cogen, MD, CDE Professor of Pediatrics Director, Diabetes Services DISCLOSURES 1. No financial incentives 2. Volunteer Positions 1. National Certification Board
1.19.18 Pediatric Diabetes Update Fran R. Cogen, MD, CDE Professor of Pediatrics Director, Diabetes Services DISCLOSURES 1. No financial incentives 2. Volunteer Positions 1. National Certification Board
Evolving insulin therapy: Insulin replacement methods and the impact on cardiometabolic risk
 Evolving insulin therapy: Insulin replacement methods and the impact on cardiometabolic risk Harvard/Joslin Primary Care Congress for Cardiometabolic Health 2013 Richard S. Beaser, MD Medical Executive
Evolving insulin therapy: Insulin replacement methods and the impact on cardiometabolic risk Harvard/Joslin Primary Care Congress for Cardiometabolic Health 2013 Richard S. Beaser, MD Medical Executive
The New Age of Insulin: Exploring the Latest Trends in Insulin Therapy. The New Age of Insulin: Exploring the Latest Trends in Insulin Therapy
 The New Age of Insulin: Exploring the Latest Trends in Insulin Therapy Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Director of Experiential Education Associate Professor of Pharmacy Practice Midwestern
The New Age of Insulin: Exploring the Latest Trends in Insulin Therapy Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Director of Experiential Education Associate Professor of Pharmacy Practice Midwestern
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES
 INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
DIABETES INDICATIONS FOR INSULIN
 DIABETES INDICATIONS FOR INSULIN 1 Introduce the likely need for insulin in the future early on as part of patient education Emphasise that it is the pancreas that fails not the patient Assess if greater
DIABETES INDICATIONS FOR INSULIN 1 Introduce the likely need for insulin in the future early on as part of patient education Emphasise that it is the pancreas that fails not the patient Assess if greater
Insulin for Adults with Type 2 Diabetes
 rth Central London Joint Formulary Committee Insulin for Adults with Type 2 Diabetes Disclaimer This guideline is registered at rth Central London (NCL) Joint Formulary Committee (JFC) and is intended
rth Central London Joint Formulary Committee Insulin for Adults with Type 2 Diabetes Disclaimer This guideline is registered at rth Central London (NCL) Joint Formulary Committee (JFC) and is intended
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
Diabetes, Type 2 Management
 CLINICAL GUIDELINE Diabetes, Type 2 Management A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised on the applicability
CLINICAL GUIDELINE Diabetes, Type 2 Management A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised on the applicability
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
INSULIN OVERVIEW. Type Brand Name Onset Peak Duration Role in glucose management Page Rapid-Acting lispro min. 3-5 hrs min.
 INSULIN OVERVIEW Type Brand Name Onset Peak Duration Role in glucose management Page Rapid-Acting lispro Humalog 15-30 min 30-90 min 3-5 hrs aspart glulisine Short-Acting Regular insulin NovoLog Apidra
INSULIN OVERVIEW Type Brand Name Onset Peak Duration Role in glucose management Page Rapid-Acting lispro Humalog 15-30 min 30-90 min 3-5 hrs aspart glulisine Short-Acting Regular insulin NovoLog Apidra
Objectives. How Medicine Works to Control Blood Sugar Levels. What Happens When We Eat? What is diabetes? High Blood Glucose (Hyperglycemia)
") How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
Subjects are requested to perform self-monitoring of blood glucose (SMBG) 4 times per
 4 times per") APPENDIX 1 Insulin Titration Algorithm Subjects are requested to perform self-monitoring of blood glucose (SMBG) 4 times per day. All subjects will be contacted weekly to review hypoglycemia and adverse
APPENDIX 1 Insulin Titration Algorithm Subjects are requested to perform self-monitoring of blood glucose (SMBG) 4 times per day. All subjects will be contacted weekly to review hypoglycemia and adverse