Objectives 2/13/2013. Figuring out the dose. Sub Optimal Glycemic Control: Moving to the Appropriate Treatment
|
|
|
- Kenneth Pierce
- 5 years ago
- Views:
Transcription
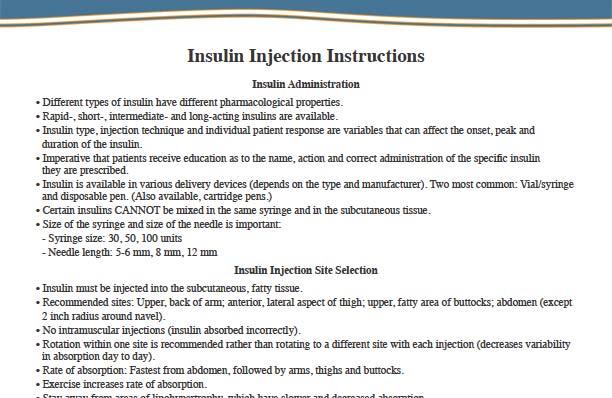
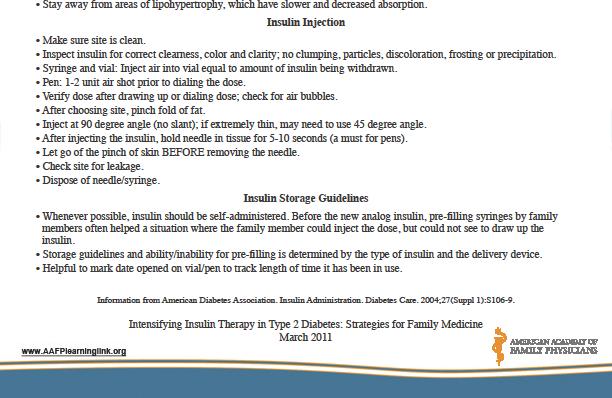
1 Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better able to: 1. Describe the various oral agents available for the management of type 2 diabetes and describe strategies for adjusting therapy to optimize patient outcomes. 2. Apply patient specific criteria for ongoing adjustments of the most effective treatment option for type 2 diabetes. 3. Select appropriate insulin formulations and regimens based on pharmacodynamic properties and patients lifestyle. 4. Intensify insulin therapy appropriately in patients with type 2 diabetes. 5. Communicate effectively with patients regarding their needs for insulin therapy, the appropriate use of insulin and blood glucose self-monitoring techniques. Figuring out the dose Depends on level of insulin resistance. Basal insulin should be approximately 40 to 50% of total daily dose, but this may vary from patient to patient How do you know that it is the right dose? No hypoglycemia occurs when patient is fasting 1

2 The Art Of Insulins Type Onset Peak Duration Timing with Meal Rapid Acting Insulins Humalog (Insulin lispro) Novolog (Insulin aspart) Short Acting Insulins (Regular) Humulin R Novolin R Intermediate Acting Insulins 5-15 minutes minutes minutes minutes 3-5 hours Administer 5-15 minutes before a meal 1-3 hours 3-5 hours Administer 5-10 minutes before a meal 1-5 hours 6-10 hours Administer 30 minutes prior to a meal Lente (Novolin L and Humulin L) 1-3 hours 6-14 hours hours Administer 15 minutes prior to meal if mixed with rapid acting insulin Administer 30 minutes prior to meal if mixed with RPH NPH (Novolin N and Humulin N) 1-2 hours 6-14 hours hours Administer 15 minutes prior to meal if mixed with rapid acting insulin Administer 30 minutes prior to meal if mixed with RPH Long-acting Insulins Lantus and Levemir 1 to 2 hrs 24 hrs Does not need to be given in regards to meals Insulin Secretion Adult human pancreas secretes units of insulin per day. Basal concentration in fasting state ~10 µu/ml 8-10 minutes after food ingestion, peripheral insulin begins to increase. At minutes after food ingestion, insulin concentration peaks. Plasma glucose returns to baseline by minutes. Plasma glucose levels below mg/dl do not stimulate insulin release. 2
3 Basal insulin Insulin Onset Peak Duration NPH 1-4 hrs 8-12 hrs hrs Ultralente 3-5 hrs hrs hrs Glargine(Lantus) and Levemir (Detemir) 1-4 hrs None In some pts, mild peak 24 hrs In some pts, may last only hrs Patients with renal insufficiency may have longer durations The Basal/Bolus Insulin Concept Basal Insulin Suppresses glucose production between meals and overnight Nearly constant levels 50 % of daily needs Bolus Insulin (mealtime or prandial) Limits hyperglycemia after meals Immediate rise and sharp peak at one hour 10% to 20% of total daily insulin requirement at each meal Physiologic Insulin Secretion: Basal/Bolus Concept Insulin (µu/ml) 50 Nutritional (Prandial) Insulin 25 0 Basal Insulin Breakfast Lunch Supper Suppresses Glucose Production Between Meals & Overnight Glucose (mg/dl) Nutritional Glucose 50 Basal Glucose A.M. P.M. Time of Day The 50/50 Rule 3
 Glargine (Lantus) Regular Lispro (Humalog) Aspart (Novolog) Glulisine (Apidra) 0 6 12 18 24 Time (hours) Self-Monitoring of Blood Glucose (SMBG) THERAPEUTIC")

4 Which Insulins are Best for Nutritional Coverage? n Effect Insulin NPH Detemir (Levemir) Glargine (Lantus) Regular Lispro (Humalog) Aspart (Novolog) Glulisine (Apidra) Time (hours) Self-Monitoring of Blood Glucose (SMBG) THERAPEUTIC REGIMEN FREQUENCY Diet... periodically Oral agents x/day QD insulin injections x/day BID insulin injections x/day TID QID insulin or insulin pump x/day Can decrease to 2 3x per week if stable. Notes Results should be recorded in a log (with each column containing glucose values during the same time of day [e.g., fasting, pre supper, etc.]), so that trends can be tracked and acted upon at each visit. Most glucose meters have download capabilities that facilitate recording and displaying glucose values, usually both in log format as well as graphically 2011; Diabetes Facts and Guidelines: Silvio E. Inzucchi, M.D. Benefits are classified according to major effects on fasting glucose, postprandial glucose, and nonalcoholic fatty liver disease (NAFLD). Eight broad categories of risks are summarized. The intensity of the background shading of the cells reflects relative importance of the benefit or risk.* * The abbreviations used here correspond to those used on the algorithm (Fig. 1). ** The term glinide includes both repaglinide and nateglinide. Available at AACE December 2009 Update. May not be reproduced in any form without express written permission from AACE 4


5 LIFESTYLE MODIFICATION A1C > 9.0% AACE/ACE DIABETES ALGORITHM FOR GLYCEMIC CONTROL Drug Naive Under Treatment Symptoms No Symptoms MET + GLP-1 or DPP4 1 ± SU 7 TZD 2 GLP-1 or DPP4 1 ± TZD 2 1 DPP4 if PPG and FPG or GLP 1 if PPG 2 TZD if metabolic syndrome and/or nonalcoholic fatty liver disease (NAFLD) 6 a) Discontinue insulin secretagogue with multidose insulin b) Can use pramlintide with prandial insulin 7 Decrease secretagogue by 50% when added to GLP 1 or DPP 4 Available at AACE December 2009 Update. May not be reproduced in any form without express written permission from AACE LIFESTYLE MODIFICATION A1C % AACE/ACE DIABETES ALGORITHM FOR GLYCEMIC CONTROL Dual Therapy 8 MET + GLP-1 or DPP4 1 or TZD 2 SU or Glinide 4,5 2-3 Mos. *** Triple Therapy 9 *** If A1C goal not achieved safely GLP-1 + TZD 2 or DPP4 1 MET + GLP-1 or DPP4 1 + SU 7 TZD Mos. *** Preferred dinitial iti agent 1 DPP4 if PPG and FPG or GLP 1 if PPG 2 TZD if metabolic syndrome and/or nonalcoholic fatty liver disease (NAFLD) 4 Glinide if PPG or SU if FPG 5 Low dose secretagogue recommended 6 a) Discontinue insulin secretagogue with multidose insulin b) Can use pramlintide with prandial insulin 7 Decrease secretagogue by 50% when added to GLP 1 or DPP 4 8 If A1C <8.5%, combination Rx with agents that cause hypoglycemia should be used with caution 9 If A1C >8.5%, in patients on Dual Therapy, insulin should be considered Available at AACE December 2009 Update. May not be reproduced in any form without express written permission from AACE A1C % ** A1C % A1C > 9.0% Drug Naive Under Treatment Symptoms No Symptoms Monotherapy MET DPP4 1 GLP-1 TZD 2 AGI Mos. *** Dual Therapy GLP-1 ordpp4 1 MET + TZD 2 Glinide or SU 5 TZD + GLP-1 or DPP4 1 Colesevelam MET + AGI Mos. *** Triple Therapy TZD 2 MET + DPP4 1 GLP-1 or + Glinide or SU 4,7 2-3 Mos. *** Dual Therapy 8 GLP-1 or DPP4 1 MET or TZD + 2 SU or Glinide 4,5 2-3M Mos. *** Triple Therapy 9 GLP-1 or DPP4 1 + TZD 2 MET + GLP-1 or DPP4 1 + SU 7 TZD Mos. *** GLP-1 or DPP4 1 ± SU 7 MET + TZD 2 GLP-1 or DPP4 1 ± TZD 2 * May not be appropriate for all patients ** For patients with diabetes and A1C < 6.5%, pharmacologic Rx may be considered *** AACE/ACE Algorithm for Glycemic Control If A1C goal not achieved safely Committee Preferred initial agent Cochairpersons: 1 DPP4 if PPG and FPG or GLP 1 if PPG Helena W. Rodbard, MD, FACP, MACE 2 TZD if metabolic syndrome and/or Paul S. Jellinger, MD, MACE nonalcoholic fatty liver disease (NAFLD) Zachary T. Bloomgarden, MD, FACE 3 AGI if PPG Jaime A. Davidson, MD, FACP, MACE 4 Glinide if PPG or SU if FPG Daniel Einhorn, MD, FACP, FACE 5 Low dose secretagogue recommended Alan J. Garber, MD, PhD, FACE James R. Gavin III, MD, PhD 6 a) Discontinue insulin secretagogue George Grunberger, MD, FACP, FACE with multidose insulin Yehuda Handelsman, MD, FACP, FACE b) Can use pramlintide with prandial insulin Edward S. Horton, MD, FACE 7 Decrease secretagogue by 50% when added to GLP Harold Lebovitz, MD, FACE 1 or DPP 4 Philip Levy, MD, MACE 8 If A1C < 8.5%, combination Rx with agents that Etie S. Moghissi, MD, FACP, FACE cause hypoglycemia should be used with caution Stanley S. Schwartz, MD, FACE 9 If A1C > 8.5%, in patients on Dual Therapy, insulin should be considered Available at AACE December 2009 Update. May not be reproduced in any form without express written permission from AACE 5

 and")


6 Basal insulin Insulin Onset Peak Duration NPH 1-4 hrs 8-12 hrs hrs Ultralente 3-5 hrs hrs hrs Glargine(Lantus) and Levemir (Detemir) 1-4 hrs None In some pts, mild peak 24 hrs In some pts, may last only hrs Patients with renal insufficiency may have longer durations 6



7 7

8 8
9 Maximum Oral Agents When combination therapy of 2-3 agents are used and patients has poor glycemic control may need insulin. Oral Agent Failure 1. Primary Failure: the patient is prescribed oral agents and their blood glucose not indicate lowered blood glucose after being on the medication for at least 3 months. 2. Secondary Failure: in type 2 patients, we frequently find that that a patient has a therapeutic response to the oral agents for years before secondary failure occurs. Summary of Oral Agents 1. No oral agents are used during pregnancy or breast feeding. 2. Children year old may use metformin. 3. Oral agents which cause weight gain; sulfonylureas, thiozolidiones and meglitinides. 4. Oral agents that may cause hypoglycemia; sulfonylureas, meglitinides. 5. Oral agents which do cause hypoglycemia if used as monotherapy; biguanide, thiozolidiones, alpha glucosidase inhibitors. 6. Previous surgeries may effect how medications are asborbed. 9
10 When A1C Doesn t Correlate to Blood Glucose Readings:Things to Remember About an A1C 1. A1C is not accurate in anemia of chronic disease such as ESRD. Or sample is hemolysed. 2. Consider when an A1C result is within the normal range and reading doesn t correlate, causes such as frequent low blood glucose readings or alcoholism with poor food intake could be the reason for the discrepency of the A1C and BG reading. 3. Consider when is the patient testing e.g. testing only fast or post prandially or immediately after exercising. 4. Consider if testing was done only post prandially. 5. Exam insulin injection technique, needle to short may be giving self injections intradermally, redness or bruising at site of injection indicates need to rotate injections within the site. Consider using use a fructosamine test (glycosylated serum albumin over 2-3 weeks) for more accurate correlation of long term control. 10
AACE/ACE Consensus Statement
 AACE/ACE Consensus Statement Statement by an American Association of Clinical Endocrinologists/ American College of Endocrinology Consensus Panel on Type 2 Diabetes Mellitus: An Algorithm for Glycemic
AACE/ACE Consensus Statement Statement by an American Association of Clinical Endocrinologists/ American College of Endocrinology Consensus Panel on Type 2 Diabetes Mellitus: An Algorithm for Glycemic
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
The Diabetes Guidelines Trek: The Next Generation. Inpatient Diabetes Guidelines. Learning Objectives. Current Inpatient Guidelines
 The Diabetes Guidelines Trek: The Next Generation J. Christopher Lynch, PharmD, BCACP Southern Illinois University Edwardsville School of Pharmacy Susan Cornell BS, PharmD, CDE, FAPhA, FAADE Midwestern
The Diabetes Guidelines Trek: The Next Generation J. Christopher Lynch, PharmD, BCACP Southern Illinois University Edwardsville School of Pharmacy Susan Cornell BS, PharmD, CDE, FAPhA, FAADE Midwestern
Current Trends in Management of Blood Glucose in Type 2 Diabetes Mellitus (T2DM)
") Current Trends in Management of Blood Glucose in Type 2 Diabetes Mellitus (T2DM) Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Assistant Professor, of Pharmacy Practice Midwestern University Chicago College
Current Trends in Management of Blood Glucose in Type 2 Diabetes Mellitus (T2DM) Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Assistant Professor, of Pharmacy Practice Midwestern University Chicago College
Timely!Insulinization In!Type!2! Diabetes,!When!and!How
 Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Julie White, MS Administrative Director Boston University School of Medicine Continuing Medical Education
 MENTOR QI Diabetes Performance Improvement Initiative, Getting Patients to Goal in Glycemic Control: Current Data Julie White, MS Administrative Director Boston University School of Medicine Continuing
MENTOR QI Diabetes Performance Improvement Initiative, Getting Patients to Goal in Glycemic Control: Current Data Julie White, MS Administrative Director Boston University School of Medicine Continuing
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Type 2 Diabetes Mellitus Insulin Therapy 2012
 Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
5/18/2011. Diabetes: Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Diabetes: 2011 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Pre Test Questions 1. There is evidence that lowering A1c reduces the risk of both micro- and macrovascular disease. A. True
Diabetes: 2011 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Pre Test Questions 1. There is evidence that lowering A1c reduces the risk of both micro- and macrovascular disease. A. True
Role of Insulin Analogs in
 Role of Insulin Analogs in Type 2 Diabetes Supported by an educational grant from Novo Nordisk Inc. This program is supported by an educational grant from Novo Nordisk Inc. It has been accredited by the
Role of Insulin Analogs in Type 2 Diabetes Supported by an educational grant from Novo Nordisk Inc. This program is supported by an educational grant from Novo Nordisk Inc. It has been accredited by the
第十五章. Diabetes Mellitus
 Diabetes-1/9 第十五章 Diabetes Mellitus 陳曉蓮醫師 2/9 - Diabetes 羅東博愛醫院 Management of Diabetes mellitus A. DEFINITION OF DIABETES MELLITUS Diabetes Mellitus is characterized by chronic hyperglycemia with disturbances
Diabetes-1/9 第十五章 Diabetes Mellitus 陳曉蓮醫師 2/9 - Diabetes 羅東博愛醫院 Management of Diabetes mellitus A. DEFINITION OF DIABETES MELLITUS Diabetes Mellitus is characterized by chronic hyperglycemia with disturbances
Insulin Prior Authorization with optional Quantity Limit Program Summary
 Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Self-Monitoring Blood Glucose (SMBG) Frequency & Pattern Tool
 Frequency & Pattern Tool") Self-Monitoring Blood Glucose () Pattern Recommendation: Basal Insulin Only (To Target) NPH or long-acting analogue, typically given at. at least as often as is being given. Optional, less frequent can
Self-Monitoring Blood Glucose () Pattern Recommendation: Basal Insulin Only (To Target) NPH or long-acting analogue, typically given at. at least as often as is being given. Optional, less frequent can
Tips and Tricks for Starting and Adjusting Insulin. MC MacSween The Moncton Hospital
 Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
AACE COMPREHENSIVE DIABETES MANAGEMENT ALGORITHM
 AACE COMPREHENSIVE DIABETES MANAGEMENT ALGORITHM 2013 TASK FORCE Alan J. Garber, MD, PhD, FACE, Chair Martin J. Abrahamson, MD Joshua I. Barzilay, MD, FACE Lawrence Blonde, MD, FACP, FACE Zachary T. Bloomgarden,
AACE COMPREHENSIVE DIABETES MANAGEMENT ALGORITHM 2013 TASK FORCE Alan J. Garber, MD, PhD, FACE, Chair Martin J. Abrahamson, MD Joshua I. Barzilay, MD, FACE Lawrence Blonde, MD, FACP, FACE Zachary T. Bloomgarden,
Inpatient Glycemic Management:
 Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
Application of the Diabetes Algorithm to a Patient
 Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
In-Hospital Management of Diabetes. Dr Benjamin Schiff Assistant Professor McGill University
 In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
Nph insulin conversion to lantus
 Nph insulin conversion to lantus Search 26-2-2003 RESPONSE FROM AVENTIS. We appreciate the opportunity to respond to Dr. Grajower s request for information regarding Lantus ( insulin glargine [rdna origin.
Nph insulin conversion to lantus Search 26-2-2003 RESPONSE FROM AVENTIS. We appreciate the opportunity to respond to Dr. Grajower s request for information regarding Lantus ( insulin glargine [rdna origin.
Session 3: Insulin Strategies for Primary Care Providers: Addressing a Core Defect in Diabetes Learning Objectives
 Session 3: Insulin Strategies for Primary Care Providers: Addressing a Core Defect in Diabetes Learning Objectives 1. Design strategies to help patients overcome cultural barriers to using insulin, and
Session 3: Insulin Strategies for Primary Care Providers: Addressing a Core Defect in Diabetes Learning Objectives 1. Design strategies to help patients overcome cultural barriers to using insulin, and
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville
 Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE
 INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols. Askiel Bruno, MD, MS Protocol PI
 Trial Treatment Protocols. Askiel Bruno, MD, MS Protocol PI") Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI SHINE Synopsis Acute ischemic stroke
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI SHINE Synopsis Acute ischemic stroke
Newer Insulins. Boca Raton Regional Hospital 15th Annual Internal Medicine Conference
 Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Starting and Helping People with Type 2 Diabetes on Insulin
 Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
SHARP-SHOOTING MANAGING INSULIN LIKE A PRO
 SHARP-SHOOTING MANAGING INSULIN LIKE A PRO Christine Kessler RN MN CNS ANP BC-ADM The Diabetes Institute Dept of Endocrinology & Metabolic Medicine Fort Belvoir Community Hospital, Fort Belvoir, VA Walter
SHARP-SHOOTING MANAGING INSULIN LIKE A PRO Christine Kessler RN MN CNS ANP BC-ADM The Diabetes Institute Dept of Endocrinology & Metabolic Medicine Fort Belvoir Community Hospital, Fort Belvoir, VA Walter
9/16/2013. Sherwin D Souza, M.D.
 Sherwin D Souza, M.D. Burden of disease in 2013 Type 2 DM Glucose Management Goals-understand the new guidelines by ADA/ AACE Drugs available for management of diabetes in 2013 (non insulin and insulin
Sherwin D Souza, M.D. Burden of disease in 2013 Type 2 DM Glucose Management Goals-understand the new guidelines by ADA/ AACE Drugs available for management of diabetes in 2013 (non insulin and insulin
Mixed Insulins Pick Me
 Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes
 Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Diabetes in Pregnancy
 Diabetes in Pregnancy Ebony Boyce Carter, MD, MPH Division of Maternal Fetal Medicine Washington University School of Medicine Disclosures I have no financial disclosures to report. Objectives Review the
Diabetes in Pregnancy Ebony Boyce Carter, MD, MPH Division of Maternal Fetal Medicine Washington University School of Medicine Disclosures I have no financial disclosures to report. Objectives Review the
Your Chart Review Data. Lara Zisblatt, MA Assistant Director Continuing Medical Education Boston University School of Medicine
 Your Chart Review Data Lara Zisblatt, MA Assistant Director Continuing Medical Education Boston University School of Medicine Participation 243 registered for the program 98 have completed the Practice
Your Chart Review Data Lara Zisblatt, MA Assistant Director Continuing Medical Education Boston University School of Medicine Participation 243 registered for the program 98 have completed the Practice
UKPDS: Over Time, Need for Exogenous Insulin Increases
 UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
New Therapies for Diabetes Management: Hope or Headache?
 New Therapies for Diabetes Management: Hope or Headache? Elizabeth Stephens, MD, FACP PMG- Endocrinology Elizabeth.Stephens@providence.org November 2018 Disclosures None 1 Objectives Discussion of 3 rd
New Therapies for Diabetes Management: Hope or Headache? Elizabeth Stephens, MD, FACP PMG- Endocrinology Elizabeth.Stephens@providence.org November 2018 Disclosures None 1 Objectives Discussion of 3 rd
7/8/2016. Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine
 Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
INSULIN 101: When, How and What
 INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control
 Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control can prevent many of early type 1 DM(in DCCT trail ). UK
Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control can prevent many of early type 1 DM(in DCCT trail ). UK
Pharmacology. Kacy Aderhold, MSN, APRN-CNS, CMSRN
 Pharmacology Kacy Aderhold, MSN, APRN-CNS, CMSRN Biguanides Decreases hepatic glucose production and improves insulin sensitivity (increases number of insulin receptors) Common Adverse Reaction: diarrhea
Pharmacology Kacy Aderhold, MSN, APRN-CNS, CMSRN Biguanides Decreases hepatic glucose production and improves insulin sensitivity (increases number of insulin receptors) Common Adverse Reaction: diarrhea
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
Type. Diabetes Drugs. A Review
 Type Diabetes is a common diagnosis for home care patients. Diabetes drugs are now available that target the multiple defects of metabolism that characterize Type 2 diabetes. Understanding the wide variety
Type Diabetes is a common diagnosis for home care patients. Diabetes drugs are now available that target the multiple defects of metabolism that characterize Type 2 diabetes. Understanding the wide variety
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
Management of Diabetes New Concepts New Devices New Medications. Richard J. Comi, MD Professor of Medicine Geisel School of Medicine at Dartmouth
 Management of Diabetes New Concepts New Devices New Medications Richard J. Comi, MD Professor of Medicine Geisel School of Medicine at Dartmouth Objectives: At the end of this lecture, the learner will
Management of Diabetes New Concepts New Devices New Medications Richard J. Comi, MD Professor of Medicine Geisel School of Medicine at Dartmouth Objectives: At the end of this lecture, the learner will
Insulin Therapy Management. Insulin Therapy
 Insulin Therapy Management Insulin Therapy Contents Insulin and its effect on glycemic control Physiology of insulin secretion Insulin pharmacokinetics and regimens Insulin dose adjustment for pregnancy
Insulin Therapy Management Insulin Therapy Contents Insulin and its effect on glycemic control Physiology of insulin secretion Insulin pharmacokinetics and regimens Insulin dose adjustment for pregnancy
Pancreatic b-cell Dysfunction in Type 2 Diabetes ZIAD KAHWASH, M.D. Insulin resistance: Defects in Insulin Signaling
 Plasma insulin (mu/ml) ZIAD KAHWASH, M.D. resistance: Defects in Signaling Increased glucose production Glucose Insufficient glucose disposal X Liver glucagon insulin Pancreas Peripheral tissues (skeletal
Plasma insulin (mu/ml) ZIAD KAHWASH, M.D. resistance: Defects in Signaling Increased glucose production Glucose Insufficient glucose disposal X Liver glucagon insulin Pancreas Peripheral tissues (skeletal
Pharmacy Drug Class Review
 April 25, 2009 Pharmacy Drug Class Review Insulin in Type II DM 2009 Disclaimer: Specific agents may have variations Focus On Dosing, When to Initiate, Fate of Oral Agents, etc. 1. Where do the American
April 25, 2009 Pharmacy Drug Class Review Insulin in Type II DM 2009 Disclaimer: Specific agents may have variations Focus On Dosing, When to Initiate, Fate of Oral Agents, etc. 1. Where do the American
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care
 Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
Update on Insulin-based Agents for T2D
 Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
9/16/2013. No Conflict of Interest to Disclose
 Catie Prinzing MSN, APRN, Clinical Nurse Specialist September 27, 2013 No Conflict of Interest to Disclose List key concepts to determining patient insulin doses during transitions in care Identify 5 points
Catie Prinzing MSN, APRN, Clinical Nurse Specialist September 27, 2013 No Conflict of Interest to Disclose List key concepts to determining patient insulin doses during transitions in care Identify 5 points
Diabetes Head to Toe May 31, 2017
 Innovations in Insulin Joanne Reid RN CDE jmreid@gbhs.on.ca Danielle Benedict RPh Outline Setting the stage Insulin as pancreas replacement therapy Commonly used insulins New insulins Case Studies Dosing
Innovations in Insulin Joanne Reid RN CDE jmreid@gbhs.on.ca Danielle Benedict RPh Outline Setting the stage Insulin as pancreas replacement therapy Commonly used insulins New insulins Case Studies Dosing
T2DM and Need for Insulin. Insulin Pharmacokinetics. When To Start Insulin in T2DM. FDA-approved Insulins for Subcutaneous Injection
 Plasma Insulin Levels Patients Requiring Insulin (%) Effective Use of Insulin in the Primary Care Practice: Insulin Therapy Initiation, Intensification, and the Insulinizing Complex Patients with T2DM:
Plasma Insulin Levels Patients Requiring Insulin (%) Effective Use of Insulin in the Primary Care Practice: Insulin Therapy Initiation, Intensification, and the Insulinizing Complex Patients with T2DM:
Drugs used in Diabetes. Dr Andrew Smith
 Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Faculty. Concentrated Insulin: Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management. Disclosures. Learning Objectives
 Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management Faculty Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Professor of Pharmacy Practice Associate Director of Experiential
Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management Faculty Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Professor of Pharmacy Practice Associate Director of Experiential
Redefining the Treatment Algorithm for Type 2 Diabetes Redefining the Treatment Algorithm for Type 2 Diabetes 2008 The June Addition 6/16/2008
 Redefining the Treatment Algorithm for Type 2 Diabetes 2008 Robert J. Rushakoff, MD Clinical Professor of Medicine University of California, San Francisco robert.rushakoff@ucsf.edu Redefining the Treatment
Redefining the Treatment Algorithm for Type 2 Diabetes 2008 Robert J. Rushakoff, MD Clinical Professor of Medicine University of California, San Francisco robert.rushakoff@ucsf.edu Redefining the Treatment
Injecting Insulin into Out Patient Practice
 Injecting Insulin into Out Patient Practice Kathleen Colleran, MD Associate Professor UNMHSC 4/22/10 Overview Natural history of Type 2 diabetes Reasons clinicians are reluctant to start insulin therapy
Injecting Insulin into Out Patient Practice Kathleen Colleran, MD Associate Professor UNMHSC 4/22/10 Overview Natural history of Type 2 diabetes Reasons clinicians are reluctant to start insulin therapy
Diabetes Management: A diagnostic perspective
 Diabetes Management: A diagnostic perspective Images: http://www.engadget.com/2009/09/23/bayer-introduces-countour-usb-glucose-meter/ http://www.medtronicdiabetes.com/treatment-and-products/minimed-530g-diabetes-system-with-enlite
Diabetes Management: A diagnostic perspective Images: http://www.engadget.com/2009/09/23/bayer-introduces-countour-usb-glucose-meter/ http://www.medtronicdiabetes.com/treatment-and-products/minimed-530g-diabetes-system-with-enlite
Drug List. Drug List (cont.) Objectives. Case 1 Bruce. Presenter Disclosure Information
 Objectives. Case 1 Bruce. Presenter Disclosure Information") 1:15 :3 PM GLP-1 Receptor Agonists and Basal Insulin Combination: A Complementary Strategy for Type Diabetes Treatment Intensification SPEAKERS Vivian Fonseca, MD Dace Trence, MD, FACE Presenter Disclosure
1:15 :3 PM GLP-1 Receptor Agonists and Basal Insulin Combination: A Complementary Strategy for Type Diabetes Treatment Intensification SPEAKERS Vivian Fonseca, MD Dace Trence, MD, FACE Presenter Disclosure
DEMYSTIFYING INSULIN THERAPY
 DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
Understanding Diabetes and Insulin Delivery Systems
 Page 1 This program has been supported by an educational grant from Sanofi Aventis Scott K. Stolte, Pharm.D. Associate Dean, Academic Affairs Bernard J. Dunn School of Pharmacy Shenandoah University Winchester,
Page 1 This program has been supported by an educational grant from Sanofi Aventis Scott K. Stolte, Pharm.D. Associate Dean, Academic Affairs Bernard J. Dunn School of Pharmacy Shenandoah University Winchester,
Insulin Prior Authorization Criteria For Individuals Who Purchased BlueCare/KS Solutions/EPO Products
 Insulin Prior Authorization Criteria For Individuals Who Purchased BlueCare/KS Solutions/EPO Products FDA LABELED INDICATIONS 1-13,16-21 Rapid-Acting Indication Onset Peak Duration Insulins Admelog (insulin
Insulin Prior Authorization Criteria For Individuals Who Purchased BlueCare/KS Solutions/EPO Products FDA LABELED INDICATIONS 1-13,16-21 Rapid-Acting Indication Onset Peak Duration Insulins Admelog (insulin
Guide to Starting and Adjusting Insulin for Type 2 Diabetes*
 Guide to Starting and Adjusting Insulin for Type 2 Diabetes* www.cadth.ca * Adapted from Guide to Starting and Adjusting Insulin for Type 2 Diabetes, 2008 International Diabetes Center, Minneapolis, MN.
Guide to Starting and Adjusting Insulin for Type 2 Diabetes* www.cadth.ca * Adapted from Guide to Starting and Adjusting Insulin for Type 2 Diabetes, 2008 International Diabetes Center, Minneapolis, MN.
Basal Bolus Insulin Therapy Frequently Asked Questions
 1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
Preventing Heart Attacks and Strokes Every Day (PHASE) RCHC Medication Titration Algorithm
 RCHC Medication Titration Algorithm") Preventing Heart Attacks and Strokes Every Day (PHASE) RCHC Medication Algorithm Updated 9/13/2017 PHASE Populations DM: type 2 ASCVD: hx heart attack/cad, CVA, TIA, AAA, Sx PAD Lifestyle Modifications
Preventing Heart Attacks and Strokes Every Day (PHASE) RCHC Medication Algorithm Updated 9/13/2017 PHASE Populations DM: type 2 ASCVD: hx heart attack/cad, CVA, TIA, AAA, Sx PAD Lifestyle Modifications
Comparative Effectiveness, Safety, and Indications of Insulin Analogues in Premixed Formulations for Adults With Type 2 Diabetes Executive Summary
 Number 14 Effective Health Care Comparative Effectiveness, Safety, and Indications of Insulin Analogues in Premixed Formulations for Adults With Type 2 Diabetes Executive Summary Background and Key Questions
Number 14 Effective Health Care Comparative Effectiveness, Safety, and Indications of Insulin Analogues in Premixed Formulations for Adults With Type 2 Diabetes Executive Summary Background and Key Questions
Changing Diabetes: The time is now!
 Midwest Cardiovascular Research Foundation Welcomes DANITA HARRISON, ARNP Ms. Harrison discloses speaking relationships with Lilly, Novo Nordisk and Pfizer. Changing Diabetes: The time is now! Danita Harrison
Midwest Cardiovascular Research Foundation Welcomes DANITA HARRISON, ARNP Ms. Harrison discloses speaking relationships with Lilly, Novo Nordisk and Pfizer. Changing Diabetes: The time is now! Danita Harrison
Basal-Bolus Insulin Therapy. Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January
 Basal-Bolus Insulin Therapy Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January 18 2018 Terminology No longer using the term diabetic. Diabetes does not define people. People with diabetes are individuals
Basal-Bolus Insulin Therapy Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January 18 2018 Terminology No longer using the term diabetic. Diabetes does not define people. People with diabetes are individuals
Position Statement of ADA / EASD 2012
 Management of Hyperglycemia in Type2 Diabetes: A Patient- Centered Approach Position Statement of ADA / EASD 2012 Cause of : Type 2 diabetes Cardiovascular disorders Blindness End-stage renal failure Amputations
Management of Hyperglycemia in Type2 Diabetes: A Patient- Centered Approach Position Statement of ADA / EASD 2012 Cause of : Type 2 diabetes Cardiovascular disorders Blindness End-stage renal failure Amputations
Disclosure 1/16/2017. Michael R. Brennan D.O., M.S., F.A.C.E Director Beaumont Endocrine Center Chief of Endocrine Beaumont Grosse Pointe 1/16/2017 2
 Therapy For Diabetes Michigan Association of Osteopathic Family Physicians Mid-Winter Family Medicine Update Shanty Creek Resort, MI January 19-22nd 2017 Michael R. Brennan D.O., M.S., F.A.C.E Director
Therapy For Diabetes Michigan Association of Osteopathic Family Physicians Mid-Winter Family Medicine Update Shanty Creek Resort, MI January 19-22nd 2017 Michael R. Brennan D.O., M.S., F.A.C.E Director
Objectives. How Medicine Works to Control Blood Sugar Levels. What Happens When We Eat? What is diabetes? High Blood Glucose (Hyperglycemia)
") How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
Medications for Diabetes
 Medications for Diabetes Sweet, but not too sweet Colette Raymond, Pharm D June 15, 2011 Learning Objectives At the end of this presentation you should be able to: Understand the prevalence and types of
Medications for Diabetes Sweet, but not too sweet Colette Raymond, Pharm D June 15, 2011 Learning Objectives At the end of this presentation you should be able to: Understand the prevalence and types of
Rhonda Eustice, PharmD, CDE. Will Power lasts about two weeks and is soluble in alcohol. Mark Twain
 Rhonda Eustice, PharmD, CDE Will Power lasts about two weeks and is soluble in alcohol. Mark Twain Diabetes Management: The Three Legged Stool Diet Medication Exercise Objectives Know the treatment goals
Rhonda Eustice, PharmD, CDE Will Power lasts about two weeks and is soluble in alcohol. Mark Twain Diabetes Management: The Three Legged Stool Diet Medication Exercise Objectives Know the treatment goals
INSULIN THERAY دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد
 INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
Adjusting Insulin Doses
 Adjusting Insulin Doses Everyone with diabetes, including you, will need to adjust your insulin doses at some time. There are several reasons why a person may need an insulin adjustment. These reasons
Adjusting Insulin Doses Everyone with diabetes, including you, will need to adjust your insulin doses at some time. There are several reasons why a person may need an insulin adjustment. These reasons
INSULIN THERAPY. Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital
 INSULIN THERAPY Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital 3 Sep. 2013 Case Somsak is a 64-year-old man was diagnosed with T2DM, HT, and dyslipidemia 9 years ago. No history of hypoglycemia
INSULIN THERAPY Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital 3 Sep. 2013 Case Somsak is a 64-year-old man was diagnosed with T2DM, HT, and dyslipidemia 9 years ago. No history of hypoglycemia
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
Initiation and Titration of Insulin in Diabetes Mellitus Type 2
 Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
CE on SUNDAY Miami, FL May 31, 2009
 CE on SUNDAY Miami, FL May 31, 2009 Date: Sunday, May 31, 2009 Time: 1:15 PM 2:15 PM Location: Doubletree Miami Mart/Airport Hotel Title: Speaker(s): Understanding Diabetes and Insulin Delivery Systems
CE on SUNDAY Miami, FL May 31, 2009 Date: Sunday, May 31, 2009 Time: 1:15 PM 2:15 PM Location: Doubletree Miami Mart/Airport Hotel Title: Speaker(s): Understanding Diabetes and Insulin Delivery Systems
Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy
 Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy Jerry Meece, BPharm, CDE, FACA, FAADE Director of Clinical Services Plaza Pharmacy and Wellness Center Gainesville,
Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy Jerry Meece, BPharm, CDE, FACA, FAADE Director of Clinical Services Plaza Pharmacy and Wellness Center Gainesville,
Update on Insulin-based Agents for T2D. Harry Jiménez MD, FACE
 Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
What s New in Type 1 and Type 2 Diabetes? Updates from 2013 CDA CPGs and Advancements in Insulin Therapy
 What s New in Type 1 and Type 2 Diabetes? Updates from 2013 CDA CPGs and Advancements in Insulin Therapy 2013 Rocky Mountain/ACP Internal Medicine Conference November 15, 2013 David C.W. Lau, MD, PhD,
What s New in Type 1 and Type 2 Diabetes? Updates from 2013 CDA CPGs and Advancements in Insulin Therapy 2013 Rocky Mountain/ACP Internal Medicine Conference November 15, 2013 David C.W. Lau, MD, PhD,
APPENDIX American Diabetes Association. Published online at
 APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
Diabetes: Inpatient Glucose control
 Diabetes: Inpatient Glucose control Leanne Current, PharmD, BCPS This activity is funded through the Medicaid section 1115(a) Demonstration Texas Healthcare Transformation and Quality Improvement Program
Diabetes: Inpatient Glucose control Leanne Current, PharmD, BCPS This activity is funded through the Medicaid section 1115(a) Demonstration Texas Healthcare Transformation and Quality Improvement Program
Current Clinical Practice Guideline for Diabetes Management
 Current Clinical Practice Guideline for Diabetes Management Chaicharn Deerochanawong M.D. Professor of Medicine, i Rangsit Medical University it Diabetes and Endocrinology Unit Department of Medicine Rajavithi
Current Clinical Practice Guideline for Diabetes Management Chaicharn Deerochanawong M.D. Professor of Medicine, i Rangsit Medical University it Diabetes and Endocrinology Unit Department of Medicine Rajavithi
Glycemic Control Insulin In The Hospital Setting
 Glycemic Control Insulin In The Hospital Setting Glycemic Control The Evidence For Insulin s s Benefit The Mechanism of Insulin s s Benefit The Achievement of Insulin s s Benefit A Few Cases Hyperglycemia
Glycemic Control Insulin In The Hospital Setting Glycemic Control The Evidence For Insulin s s Benefit The Mechanism of Insulin s s Benefit The Achievement of Insulin s s Benefit A Few Cases Hyperglycemia
Diabetes Update 2018: Challenging Transitions. Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley Health System
 Diabetes Update 2018: Challenging Transitions Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley Health System 1 Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley
Diabetes Update 2018: Challenging Transitions Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley Health System 1 Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley
Initiation and Adjustment of Insulin Regimens for Type 2 Diabetes
 Types of Insulin Rapid-acting insulin: lispro (Humalog), aspart (NovoRapid), glulisine (Apidra) Regular short-acting insulin: Humulin R, Novolin ge Toronto, Hypurin Regular Basal insulin: NPH (Humulin
Types of Insulin Rapid-acting insulin: lispro (Humalog), aspart (NovoRapid), glulisine (Apidra) Regular short-acting insulin: Humulin R, Novolin ge Toronto, Hypurin Regular Basal insulin: NPH (Humulin
Type I Type II Insulin Resistance
 Insulin An aqueous hormonal solution made in the pancreas. Affects metabolism by allowing glucose to leave the blood and enter the body cells, preventing hyperglycemia. It is measured in units, e.g. 100
Insulin An aqueous hormonal solution made in the pancreas. Affects metabolism by allowing glucose to leave the blood and enter the body cells, preventing hyperglycemia. It is measured in units, e.g. 100
Application of the Diabetes Algorithm to Patients
 Application of the Diabetes Algorithm to Patients Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Application of the Diabetes Algorithm to Patients Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Current Trends in Diagnosis and Management of Gestational Diabetes
 Current Trends in Diagnosis and Management of Gestational Diabetes Shreela Mishra, MD Assistant Clinical Professor UCSF Fresno Medical Education Program 2/2/2019 Disclosures No disclosures 2/2/19 Objectives
Current Trends in Diagnosis and Management of Gestational Diabetes Shreela Mishra, MD Assistant Clinical Professor UCSF Fresno Medical Education Program 2/2/2019 Disclosures No disclosures 2/2/19 Objectives
Insulin Prior Authorization Criteria For Individuals who Purchased BlueCare / KS Solutions products
 Insulin Prior Authorization Criteria For Individuals who Purchased BlueCare / KS Solutions products FDA LABELED INDICATIONS 1-13,16-20 Rapid-Acting Indication Onset Peak Duration Insulins Fiasp (insulin
Insulin Prior Authorization Criteria For Individuals who Purchased BlueCare / KS Solutions products FDA LABELED INDICATIONS 1-13,16-20 Rapid-Acting Indication Onset Peak Duration Insulins Fiasp (insulin