Disclosure 1/16/2017. Michael R. Brennan D.O., M.S., F.A.C.E Director Beaumont Endocrine Center Chief of Endocrine Beaumont Grosse Pointe 1/16/2017 2
|
|
|
- Luke Walsh
- 5 years ago
- Views:
Transcription

, determir (levemir), 70/30 mix insulin (NovoLog and Novolin 70/30), degludec (Tresiba), repaglinide (Prandin), glucagon (GlucaGen HypoKit), estradiol vaginal tablets (Vagifem),")
1 Therapy For Diabetes Michigan Association of Osteopathic Family Physicians Mid-Winter Family Medicine Update Shanty Creek Resort, MI January 19-22nd 2017 Michael R. Brennan D.O., M.S., F.A.C.E Director Beaumont Endocrine Center Chief of Endocrine Beaumont Grosse Pointe Disclosure I m married to a drug representative and she works for Novo Nordisk Makers of liraglutide (Victoza/Saxsenda), aspart (NovoLog), determir (levemir), 70/30 mix insulin (NovoLog and Novolin 70/30), degludec (Tresiba), repaglinide (Prandin), glucagon (GlucaGen HypoKit), estradiol vaginal tablets (Vagifem), estradiol/norethindrone (Activella), somatropin (Norditropin), coagulation factor VIIIa (NovoSeven) I m a consultant on insulin pumps and lead groups for the Insulet Corporation They make an insulin delivery system (pod/pump) called the Omni Pod 1/16/ /16/


2 1/16/ /16/ Resources 1/16/

 Understand the device")
3 Resources 2017 ADA 1/16/ Resources - 1/16/ Objectives To understand the general types of insulin Be able to start and dose a patient on a reasonable amount of insulin therapy in a physiologic replacement pattern Be aware of all continuous insulin infusion devices (insulin pumps, pods and patches) Understand the device settings of a continuous insulin infusion device (pump) 9 3
4 Background/Physiology The physiologic range of insulin produced by the body in a normal individual 0.3 to 0.5 units/kg per day Half a person s daily pancreatic insulin secretion is basal (chronic relatively constant secretion) and half is bolus (secreted in bursts with hyperglycemia) Most people you see have insulin resistance and will be slightly beyond the physiologic range 10 All Diabetes Classes of Medication Bigunides Alpha-Glucosidase Inhibitors Amylin Mimetic Bile Acid Sequestrants Dipeptidyl Peptidase-4 inhibitor Dopamine-2 Agonist Glucagon-Like Peptide-1 Inhaled insulin Meglitinides Thiazolidinedione Sodium-glucose transporter 2 Sulfonylurea Subcutaneous/IV 11 Four Generalized Classes: Basal Rapid Acting Regular Mix 12 4
5 Basal insulin: administered to cover endogenous glucose production (glucose made by the liver/body). Doses can be administered subcutaneously one, two, or three shots per day Glargine (Lantus/Toujeo/Basaglar) Detemir (Levemir) Degludec U-100 and U-200 (Tresiba) Neutral Protamine Hagedorn (NPH, Humulin N or Novolin N) 13 Rapid acting insulin Covers the glucose created by stress, consumption of glucose or infusion of glucose. It is used in subcutaneous bolus method to correct or prevent hyperglycemia Lispro and Lispro U-200 (Humalog) Glulisine (Apidra) Aspart (Novolog) 14 Regular insulin Conceptually can be considered the first insulin (just the human insulin molecule). No substitutions in molecule configurations, amino acids. Now relatively slow compared to rapid insulin, and not long acting compared to basal for subcutaneous use. Great for IV use as it is inexpensive and extremely effective. Regular insulin has a short IV half-life, which can be a problem in a patient that requires insulin. Regular insulin (Humulin R, Novolin R) 15 5
6 Mix insulin An attempt to cover both meal and endogenous glucose in one shot. This is not an ideal insulin with fluctuating PO intake (e.g. the hospital). Dosed generally before breakfast and dinner or before all meals: 30% Aspart, 70% Prot-aspart (NovoLog 70/30) 30% Novolin-R, 70% NPH (Novolin 70/30) 25% Lispro, 75% Prot-Lispro (Humalog 75/25) 30% Humulin-R, 70% NPH (Humulin 70/30) 50% Lispro, 50% Prot-Lispro (Humalog 50/50) 16 Concentrated resistance can be so severe that the volume of the insulin injection can be overwhelming. Therefore, the units of insulin can be manufactured in a smaller volume. U-500 Regular U-300 Glargine (Toujeo) U-200 Lispro (U-200 Humalog) U-200 Degludec (U-200 Tresiba) 17 Normal secretion of insulin Basic Slide Header Theoretical insulin secretion (always normal glucose levels) secretion duration over 24 hours 18 6
7 Starting Basal Basal insulin covers endogenous glucose production (glucose made by body) Basal insulin Dose can be one or two shots per day: Start patient on 0.25 units per kg/d Glargine (Lantus/Toujeo/Basaglar) Indicated for once a day dosing Detemir (Levemir) Indicated for once or twice a day dosing Degludec (Tresiba) Indicated for once a day 1/16/ Basic Basal Slide Header Theoretical insulin secretion and duration with one basal shot secretion duration over 24 hours 1/16/ Basic Basal Slide Header Theoretical insulin secretion and duration with two basal shot regimen secretion duration over 24 hours 1/16/
8 Basic Rapid Slide acting Header insulin Theoretical insulin secretion and duration with three rapid acting shots secretion duration over 24 hours 1/16/ Basic Mixed Slide Header An attempt to cover both meal and endogenous glucose in one shot Mix insulin Dose generally before breakfast and dinner or before all meals: Start patient on 0.5 units per kilogram per day and divide the dose by 2-3 to determine the doses for the day 30% Aspart, 70% Prot-Aspart (NovoLog Mix 70/30) 30% Novolin-R, 70% NPH (Novolin 70/30) 25% Lispro, 75% Prot-Lispro (Humalog 75/25) 30% Humalin-R, 70% NPH (Humulin 70/30) 50% Lispro, 50% Prot-Lispro (Humalog 50/50) 1/16/ Basic Mixed Slide Header Theoretical insulin secretion and duration with two mix injections secretion duration over 24 hours 1/16/
9 Basic Basal Slide Plus Header Bolus Theoretical insulin secretion and duration with one basal shot and three bolus shots secretion duration over 24 hours 1/16/ Basic Basal Plus Slide Two Header Bolus Theoretical insulin secretion and duration with two basal shot and three bolus shots secretion duration over 24 hours 1/16/ Normal Basic secretion Slide Header of insulin Theoretical insulin secretion (always normal glucose levels) secretion duration over 24 hours 1/16/
10 Basal-Bolus Versus Mix To Simplify: Hypoglycemia is less, and meal flexibility is greater in a four to five shot a day regimen using rapid acting and long acting insulin On the other hand, frequency of injection is less using a two to three shots per day mixed insulin regimen. In this scenario, hypoglycemia is greater and flexibility is less 1/16/ The physiologic range of insulin produced by the body in a normal individual 0.3 to 0.5 units/kg per day 1/16/ Basic Slide Case #1 Header Example #1: a 72kg T1DM admitted and treated for DKA, is now ready to transition to sub Q insulin using basal bolus (4 shots): 0.5units/kg/day * 72 kg = 36 units per day Choose 18 units of basal The (18/3) 6 units of rapid acting with meals Patient is 72 kg and the total daily dose of insulin is 36 units 1/16/
11 Basic Slide Case #2 Header Example #2: A 100kg T2DM admitted and treated for DKA, is now ready to go home (hates shots, but needs them) on sub Q insulin using mix insulin (2 shots): 0.5units/kg/day * 100 kg = 50 units per day 25 units of mix insulin for breakfast 25 units of mix insulin for dinner Total daily dose is 50 units of insulin and the patient weighs 100kg 1/16/ Transition Out of the Hospital Talk to care management and write scripts before discharge (maybe 2 days before) Try to fill the insulin to determine what is available via their insurance (basal, rapid, and mix insulin) within the same class (basal, rapid acting, and mix) can be used similarly KEY: Instruct the nurse to give the insulin used at the bedside in the hospital to the patient at discharge 1/16/ Outpatient Basic Slide Transition Header How do you transition the basal only patient to basal bolus? Remember goal of basal is to titrate the fasting am glucose to mg/dlNOT to hemoglobin A1C of 7% Once goal a.m. glucose (70-120mg/dl) is attained, then you can consider taking that basal dose, dividing it by 3, and administering that number of units 3 times a day with meals 1/16/


12 Basic Slide Case #3 Header Example #3: a 120kg T2DM takes 30 units of basal insulin every evening. The a.m. fasting glucoses are mg/dl but the HbA1c is 8.9%. Starting dose of meal time insulin could be? 1/16/ Basic Transition Slide Case Header #3 Example #3 a 120kg T2DM takes 30 units of basal insulin every evening. a.m. glucoses are mg/dl but the HbA1c is 8.9% Starting dose of meal time could be: 30 units/3 = 10 units rapid acting insulin before meals three times a day That s a total daily dose of 60 units, which in this individual equals 0.5 units/kg/day 1/16/ Delivery delivery can generally be done via three methods of subcutaneous delivery: Vial and syringe Pens Pump/Pods/Patch 36 12






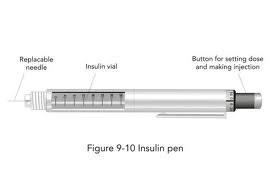
13 Vial and Syringe 37 Pens and Pen Needles 38 Pens and Pen Needles 39 13




14 Continuous Delivery Systems Pumps Company/Pump 1/16/ Continuous Delivery Systems Pumps 1/16/ Continuous Delivery Systems Pods Company/Pod 1/16/




15 Continuous Delivery Systems Patch Company/Patch 1/16/ Continuous Delivery Systems Pods and a patch 1/16/ Delivery with Syringe/Pen Vial and syringe or insulin pens: Mealtime dose/carbohydrate Ratio Basal dose Sliding Scale/Correction Factor and Target 1/16/
16 Delivery with Syringe/Pen Mealtime Dose: Usually aspart (NovoLog), lispro (Humalog), or glulisine (Apidra) Example: I take 10 units before breakfast, lunch and dinner, and like 5 units with snacks. 1/16/ Delivery with Syringe/Pen Basal Dose - Covers endogenous glucose production (glucose made by body). It will be either glargine (Lantus/Toujeo/Basaglar), detemir (Levemir), or degludec (Tresiba) Example: I give myself 24 units of Lantus every night 1/16/ Delivery with Syringe/Pen Sliding Scale: Usually aspart (NovoLog), lispro (Humalog), or glulisine (Apidra) Patient uses this scale to correct high glucoses (generally Q 4 or AC TID and QHS) Example: Glucose (mg/dl) (units) > /16/
17 Delivery with a Pump/Pod Background: Based on informal observations by Paul Davidson in 1982, he attempted to calculate a correction factor (sliding scale) and a carbohydrate to insulin ratio (meal time insulin) for patients with type 1 diabetes (but it applies to anyone with insulin requiring diabetes) 1/16/ Delivery with a Pump/Pod for Pump/Pod: Any insulin can be placed in a pump/pod 99% of the time it is a rapid acting analog insulin: Aspart (NovoLog) Lispro (Humalog) Glulisine (Apidra) Other pump insulin includes: Regular (Humulin R and Novolin R) Used for years prior to rapid acting insulin analogs U-500 Regular U-200 Lispro 1/16/ Delivery with a Pump/Pod Pump/Pod: to carbohydrate ratio (Mealtime dose) Basal Rate (Basal dose) Target glucose and correction factor (Sliding scale) 1/16/
18 Delivery with a Pump/Pod Background: The carbohydrate to insulin ratio is the insulin required to maintain a static blood sugar per the amount of carbohydrates (in grams) consumed Basal Rate is a continuous amount of insulin being infused subcutaneously to keep the patient euglycemic The correction factor is the estimated change in blood glucose from one unit of insulin 1/16/ Delivery with a Pump/Pod Carbohydrate Ratio: The carbohydrate ratio is the insulin required to maintain a static blood sugar per the amount of carbohydrates (in grams) consumed Example: 1 unit of insulin for every 10 grams of carbohydrate If patient is about to eat 80 grams of carbohydrates, then they get 8 units of insulin at meal time Carbs in grams are entered in the pump 1/16/ Delivery with a Pump/Pod Carbohydrate Ratio: Advantage: Patient can change the amount and the types of food per meals as long as carbohydrates are counted Patient can eat at whatever time they like, or however frequently they like Both within reason Disadvantage If the Pump/pod fails or gets removed, then there would be no more insulin on board (set up for DKA) 1/16/
19 Delivery with a Pump/Pod Basal Rate: Instead of Degludec (Tresiba), glargine (Lantus/Toujeo/Basaglar) or detemir (Levemir), a continuous subcutaneous infusion is given with rapid acting insulin (either aspart(novolog), lispro(humalog), or glulisine(apidra) 1/16/ Delivery with a Pump/Pod Basal Rate: Advantage: Rates can be given at various amounts (1/100 th of a unit per hour) Varying times the basal rate can be adjusted in half hour increments based on various levels of need Disadvantage If the Pump/pod fails or gets removed, then there would be no more insulin on board (set up for DKA) 1/16/ Delivery with a Pump/Pod Basal Rate: Example: Basal Rate Midnight 5a.m. = 1.2 units/hr (5 hours, 6 units) 5a.m. 2p.m. = 1 units/hr (9 hours, 9 units) 2p.m. 7p.m. = 1.75 units/hr (5 hours, 10.5 units) 7p.m. Midnight = 0.9 unit/hr (5 hours, 4.5 units) Total basal in this case is 30 units of insulin over 24 hours ( = 30) 1/16/
20 Delivery with a Pump/Pod Basal Rate: EXTEREMLY helpful BASAL RATE for 24 hours is a great approximation of the basal dose! In the previous slide, the patient s basal rate - Indicates the patient s basal insulin dose is approximately 30 units of detemir (Levemir), glargine (Lantus/Toujeo/Basaglar) or degludec (Tresiba) 1/16/ Delivery with a Pump/Pod Target glucose and correction factor: Target is chosen by the practitioner It is ideally where we would like the individual s glucose to always be People generally choose between mg/dl I generally choose 90 or 100 mg/dl Correction Factor: the estimated amount of blood glucose (mg/dl) that will change with one unit of insulin 1/16/ Delivery with a Pump/Pod Correction Factor: The correction factor in mg/dl can be estimated using 1500 divided by the total daily dose of insulin: Example: Our 100kg gentleman takes 30 units of long acting and 10 units 3 times a day before meals Therefore he generally takes 60 units total daily dose (or 0.6units/kg/day) 1500 divided by 60 = 25 Correction factor is 1 unit for every 25mg/dl greater than the target 1/16/
21 Pump/Pod vs Sub Q Correction Factor (CF): If the CF is 1 unit for 25mg/dL, and If the target is 150 mg/dl Then every 25 mg/dl greater than the target, the patient gets one unit from the pump Example: The patient s glucose is 225mg/dL, then when the patient tells this info to the pump, the pump suggests 3 units of insulin be administered Sliding Scale: Glucose (mg/dl) (units) > IN THIS CASE: SAME EXACT THING!!! (Just sliding scale has less precision with delivery) 1/16/ Delivery with a Pump/Pod Correction Factor Advantage Correction intervals can be in 1mg/dL units (doesn t have to be every 50 mg/dl) The correction insulin dose can be less than 1 unit increments The pump can use the known ½ life of the insulin in the pump to prevent insulin stacking Disadvantage If the Pump/pod fails or gets removed, then there would be no more insulin on board (set up for DKA) 1/16/ Delivery with a Pump/Pod Correction Factor: Extremely useful Use this to determine how much insulin it takes to lower a patient s glucose This is helpful if you want to try to lower a person s glucose by 50mg/dl 1/16/
22 Delivery with a Pump/Pod Correction Factor: Example #1: Patient reports My correction factor is 1 unit for 25 mg/dl above my target Then you have a clue that in order to lower the blood glucose by 50 mg/dl, it would take approximately 2 units of insulin subcutaneously 1/16/ Delivery with a Pump/Pod Correction Factor: Example #2: Patient reports My correction factor is 1 unit for 40 mg/dl above my target Then you have a clue that in order to lower the blood glucose by 50 mg/dl, it would take approximately 1.25 units of insulin subcutaneously 1/16/ Delivery with a Pump/Pod Correction Factor: Example #3: Patient reports My correction factor is 1 unit for 10 mg/dl above my target Then you have a clue that in order to lower the blood glucose by 50 mg/dl, it would take approximately 5 units of insulin subcutaneously 1/16/
23 Delivery with a Pump/Pod For an insulin pump patient try to know the following: The sum of the basal rate, because then you know the basal dose if needed The correction factor, to help estimate how much rapid acting insulin is required to correct the glucose Extremely useful if the pump delivery is stopped 1/16/ Delivery with a Pump/Pod What should a doctor do when the pump fails or is removed? Give a basal dose of insulin!!! With basal insulin, give at least 0.25 units/kg or the summation of the basal rates In Hospital setting: Make sure the attending, team or consultant is aware, takes responsibility, and has an immediate plan of insulin management now that the pump failed 1/16/ /16/

24 1/16/ /16/ /16/

25 1/16/ /16/ /16/


26 1/16/ Conclusion is a great medication and frequently required to manage diabetes Classify different insulin as either basal, rapid, mix, or regular The use of pumps/patches/pods and subcutaneous insulin pens is now common Be familiar with knowing: Basal dose or rate Meal time/carb ratio doses Sliding scales/correction factors and targets The physiologic range of insulin produced by the body in a normal individual 0.3 to 0.5 Units/kg per day When in doubt poke the finger and check the blood glucose, then give insulin when the glucose is too high and glucose if the glucose is too low 1/16/ Thanks 1/16/
27 Questions? 1/16/ Thank you! Questions? To Contact Dr. Michael R. Brennan Contact the Beaumont Endocrine Center Little Mack, Suite 204 St. Clair Shores, MI Phone: Fax: Call Beaumont Health system and ask to have him paged /16/
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols. Askiel Bruno, MD, MS Protocol PI
 Trial Treatment Protocols. Askiel Bruno, MD, MS Protocol PI") Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI SHINE Synopsis Acute ischemic stroke
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI SHINE Synopsis Acute ischemic stroke
Insulin Prior Authorization with optional Quantity Limit Program Summary
 Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Tips and Tricks for Starting and Adjusting Insulin. MC MacSween The Moncton Hospital
 Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Insulin Regimens: Hitting Glycemia Targets
 Insulin Regimens: Hitting Glycemia Targets Grant Kelley MD March 1 st, 2018 Faculty Disclosure: Financial relationships with commercial interests None Overview Mortality and Morbidity Insulin and Insulin
Insulin Regimens: Hitting Glycemia Targets Grant Kelley MD March 1 st, 2018 Faculty Disclosure: Financial relationships with commercial interests None Overview Mortality and Morbidity Insulin and Insulin
Faculty. Concentrated Insulin: Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management. Disclosures. Learning Objectives
 Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management Faculty Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Professor of Pharmacy Practice Associate Director of Experiential
Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management Faculty Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Professor of Pharmacy Practice Associate Director of Experiential
Type I Type II Insulin Resistance
 Insulin An aqueous hormonal solution made in the pancreas. Affects metabolism by allowing glucose to leave the blood and enter the body cells, preventing hyperglycemia. It is measured in units, e.g. 100
Insulin An aqueous hormonal solution made in the pancreas. Affects metabolism by allowing glucose to leave the blood and enter the body cells, preventing hyperglycemia. It is measured in units, e.g. 100
Inpatient Glycemic Management:
 Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
Type 2 Diabetes Mellitus Insulin Therapy 2012
 Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Mixed Insulins Pick Me
 Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
Learning Objectives. Are you ready for more insulin formulations?
 Are you ready for more insulin formulations? Shara Elrod, PharmD, BCACP, BCGP Learning Objectives Review pharmacology and dosing of new insulin formulations Compare and contrast new insulin formulations
Are you ready for more insulin formulations? Shara Elrod, PharmD, BCACP, BCGP Learning Objectives Review pharmacology and dosing of new insulin formulations Compare and contrast new insulin formulations
Adjusting Insulin Doses
 Adjusting Insulin Doses Everyone with diabetes, including you, will need to adjust your insulin doses at some time. There are several reasons why a person may need an insulin adjustment. These reasons
Adjusting Insulin Doses Everyone with diabetes, including you, will need to adjust your insulin doses at some time. There are several reasons why a person may need an insulin adjustment. These reasons
Newer Insulins. Boca Raton Regional Hospital 15th Annual Internal Medicine Conference
 Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Nph insulin conversion to lantus
 Nph insulin conversion to lantus Search 26-2-2003 RESPONSE FROM AVENTIS. We appreciate the opportunity to respond to Dr. Grajower s request for information regarding Lantus ( insulin glargine [rdna origin.
Nph insulin conversion to lantus Search 26-2-2003 RESPONSE FROM AVENTIS. We appreciate the opportunity to respond to Dr. Grajower s request for information regarding Lantus ( insulin glargine [rdna origin.
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Converting lantus to humalog 75 25
 P ford residence southampton, ny Converting lantus to humalog 75 25 This page includes the following topics and synonyms: Insulin Dosing in Type 2 Diabetes, Insulin Dosing in Type II Diabetes. Thiazide
P ford residence southampton, ny Converting lantus to humalog 75 25 This page includes the following topics and synonyms: Insulin Dosing in Type 2 Diabetes, Insulin Dosing in Type II Diabetes. Thiazide
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Insulin Basics. Bryan Primary Care Conference May 21, 2016 Shannon Wakeley MD Complete Endocrinology
 Insulin Basics Bryan Primary Care Conference May 21, 2016 Shannon Wakeley MD Complete Endocrinology Disclosures Speakers Bureau for Sanofi, Astra Zeneca, Janssen, Boehringer-Ingelheim Objectives Discuss
Insulin Basics Bryan Primary Care Conference May 21, 2016 Shannon Wakeley MD Complete Endocrinology Disclosures Speakers Bureau for Sanofi, Astra Zeneca, Janssen, Boehringer-Ingelheim Objectives Discuss
Objectives. How Medicine Works to Control Blood Sugar Levels. What Happens When We Eat? What is diabetes? High Blood Glucose (Hyperglycemia)
") How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
Short-acting insulins. Biphasic insulins. Intermediate- and long-acting insulins
 Recommended Insulin Products This guideline states the Gloucestershire Joint Formulary recommended, first choice insulin products. The intention is to support the choice of treatment for new patients,
Recommended Insulin Products This guideline states the Gloucestershire Joint Formulary recommended, first choice insulin products. The intention is to support the choice of treatment for new patients,
Learning Objectives. Perioperative SWEET Success
 Perioperative SWEET Success PERIOPERATIVE SWEET SUCCESS PRESENTED BY: KENDRA MARTIN, RN, BSN, CDE JENNIFER SIMPSON, RN, BC-ADM, MSN, CNS Disclosure to Participants Notice of Requirements For Successful
Perioperative SWEET Success PERIOPERATIVE SWEET SUCCESS PRESENTED BY: KENDRA MARTIN, RN, BSN, CDE JENNIFER SIMPSON, RN, BC-ADM, MSN, CNS Disclosure to Participants Notice of Requirements For Successful
CANDY Camp Application
 CANDY Camp Application Please complete the following form and submit it by June 15, 2016. Please mail form to Bonnie Kruse, Diabetes Program Coordinator, HSHS St. Anthony s Memorial Hospital, 503 North
CANDY Camp Application Please complete the following form and submit it by June 15, 2016. Please mail form to Bonnie Kruse, Diabetes Program Coordinator, HSHS St. Anthony s Memorial Hospital, 503 North
INSULIN 101: When, How and What
 INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Pharmacy Plan Guidance
 Pharmacy Plan Guidance The pharmacy plan is a tool used during the site readiness process to develop and document the site-specific procedures for study drug ordering, labeling and dispensing for the SHINE
Pharmacy Plan Guidance The pharmacy plan is a tool used during the site readiness process to develop and document the site-specific procedures for study drug ordering, labeling and dispensing for the SHINE
8/13/2016. Insulin Basics. Rapid-Acting Insulin Analogs. Current Insulin Products and Pens. Basal Insulin Analogs. History of Insulin Therapy
 Insulin Basics Anabolic hormone involved in metabolism Following carbohydrate ingestion insulin release is stimulated Suppresses hepatic glucose production Stimulates peripheral glucose uptake Commercially-available
Insulin Basics Anabolic hormone involved in metabolism Following carbohydrate ingestion insulin release is stimulated Suppresses hepatic glucose production Stimulates peripheral glucose uptake Commercially-available
What the Pill Looks Like. How it Works. Slows carbohydrate absorption. Reduces amount of sugar made by the liver. Increases release of insulin
 Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Initiation and Adjustment of Insulin Regimens for Type 2 Diabetes
 Types of Insulin Rapid-acting insulin: lispro (Humalog), aspart (NovoRapid), glulisine (Apidra) Regular short-acting insulin: Humulin R, Novolin ge Toronto, Hypurin Regular Basal insulin: NPH (Humulin
Types of Insulin Rapid-acting insulin: lispro (Humalog), aspart (NovoRapid), glulisine (Apidra) Regular short-acting insulin: Humulin R, Novolin ge Toronto, Hypurin Regular Basal insulin: NPH (Humulin
Premixed Insulin for Type 2 Diabetes. a gu i d e f o r a d u lt s
 Premixed Insulin for Type 2 Diabetes a gu i d e f o r a d u lt s March 2009 What This Guide Covers / 2 Type 2 Diabetes / 3 Learning About Blood Sugar / 4 Learning About Insulin / 5 Comparing Medicines
Premixed Insulin for Type 2 Diabetes a gu i d e f o r a d u lt s March 2009 What This Guide Covers / 2 Type 2 Diabetes / 3 Learning About Blood Sugar / 4 Learning About Insulin / 5 Comparing Medicines
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Insulin Prior Authorization Criteria For Individuals who Purchased BlueCare / KS Solutions products
 Insulin Prior Authorization Criteria For Individuals who Purchased BlueCare / KS Solutions products FDA LABELED INDICATIONS 1-13,16-20 Rapid-Acting Indication Onset Peak Duration Insulins Fiasp (insulin
Insulin Prior Authorization Criteria For Individuals who Purchased BlueCare / KS Solutions products FDA LABELED INDICATIONS 1-13,16-20 Rapid-Acting Indication Onset Peak Duration Insulins Fiasp (insulin
Objectives. Navigating New Insulins. Disclosures. Diabetes: The Stats. Normal Insulin Release Individuals without diabetes. History of Insulin 5/23/17
 Objectives Compare and contrast currently available products. Navigating New s Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Diabetes Center Determine the factors
Objectives Compare and contrast currently available products. Navigating New s Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Diabetes Center Determine the factors
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE
 INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION
 INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
Implementing Hospital Policies & Protocols
 Implementing Hospital Policies & Protocols Jane Jeffrie Seley DNP MPH GNP BC-ADM CDE CDTC FAADE FAAN Division of Endocrinology, Diabetes & Metabolism NewYork-Presbyterian Hospital Weill Cornell Medicine
Implementing Hospital Policies & Protocols Jane Jeffrie Seley DNP MPH GNP BC-ADM CDE CDTC FAADE FAAN Division of Endocrinology, Diabetes & Metabolism NewYork-Presbyterian Hospital Weill Cornell Medicine
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
Insulin Prior Authorization Criteria For Individuals Who Purchased BlueCare/KS Solutions/EPO Products
 Insulin Prior Authorization Criteria For Individuals Who Purchased BlueCare/KS Solutions/EPO Products FDA LABELED INDICATIONS 1-13,16-21 Rapid-Acting Indication Onset Peak Duration Insulins Admelog (insulin
Insulin Prior Authorization Criteria For Individuals Who Purchased BlueCare/KS Solutions/EPO Products FDA LABELED INDICATIONS 1-13,16-21 Rapid-Acting Indication Onset Peak Duration Insulins Admelog (insulin
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Basal-Bolus Insulin Therapy. Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January
 Basal-Bolus Insulin Therapy Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January 18 2018 Terminology No longer using the term diabetic. Diabetes does not define people. People with diabetes are individuals
Basal-Bolus Insulin Therapy Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January 18 2018 Terminology No longer using the term diabetic. Diabetes does not define people. People with diabetes are individuals
The ABCs of MDI: Gaining a working knowledge of Multiple Daily Injection insulin therapy. Today s Presenter
 FD Title Slide The ABCs of MDI: Gaining a working knowledge of Multiple Daily Injection insulin therapy learn.extension.org/events/3369 3 This material is based upon work supported by the National Institute
FD Title Slide The ABCs of MDI: Gaining a working knowledge of Multiple Daily Injection insulin therapy learn.extension.org/events/3369 3 This material is based upon work supported by the National Institute
Lantus to levemir conversion
 Lantus to levemir conversion The Borg System is 100 % Lantus to levemir conversion 16-6-2005 Ask the Expert on... Lantus Conversion. Karen Shapiro, PharmD, BCPS. Disclosures. June 16, 2005. Question. Would
Lantus to levemir conversion The Borg System is 100 % Lantus to levemir conversion 16-6-2005 Ask the Expert on... Lantus Conversion. Karen Shapiro, PharmD, BCPS. Disclosures. June 16, 2005. Question. Would
Collaborative Practice Agreement
 Collaborative Practice Agreement [community pharmacy name] [address] [phone number] [physician practice] [address] [phone number] Effective: [date] Expiration: [date] 1 Table of Contents 1.0 Introduction...4
Collaborative Practice Agreement [community pharmacy name] [address] [phone number] [physician practice] [address] [phone number] Effective: [date] Expiration: [date] 1 Table of Contents 1.0 Introduction...4
In-Hospital Management of Diabetes. Dr Benjamin Schiff Assistant Professor McGill University
 In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
Initiation and Titration of Insulin in Diabetes Mellitus Type 2
 Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
4/16/2018. Flexible Intensive Insulin Therapy (FIIT) in People with Type 2 Diabetes: A Viable Option. Disclosures. Outline. No financial disclosures
 in People with Type 2 Diabetes: A Viable Option. Disclosures. Outline. No financial disclosures") Flexible Intensive Insulin Therapy (FIIT) in People with Type Diabetes: A Viable Option Kim Bisanz, MFCS, RDN, LDN, CDE Minnesota Academy of Nutrition & Dietetics Annual Meeting April 19, 18 18 MFMER slide-1
Flexible Intensive Insulin Therapy (FIIT) in People with Type Diabetes: A Viable Option Kim Bisanz, MFCS, RDN, LDN, CDE Minnesota Academy of Nutrition & Dietetics Annual Meeting April 19, 18 18 MFMER slide-1
Rebecca Newberry APRN MS CDE
 Current Diabetes Medications Nursing Implications and Applications Rebecca Newberry APRN MS CDE Methodist Center for Diabetes and Nutritional Health Disclosures Objectives Speakers Bureaus/Consulting Board
Current Diabetes Medications Nursing Implications and Applications Rebecca Newberry APRN MS CDE Methodist Center for Diabetes and Nutritional Health Disclosures Objectives Speakers Bureaus/Consulting Board
Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy
 Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy Jerry Meece, BPharm, CDE, FACA, FAADE Director of Clinical Services Plaza Pharmacy and Wellness Center Gainesville,
Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy Jerry Meece, BPharm, CDE, FACA, FAADE Director of Clinical Services Plaza Pharmacy and Wellness Center Gainesville,
Diabetes: What You Need to Know
 UW MEDICINE PATIENT EDUCATION Diabetes: What You Need to Know Discharge review before you leave the hospital We want to be sure that we explained your diabetes instructions well, so that you know how to
UW MEDICINE PATIENT EDUCATION Diabetes: What You Need to Know Discharge review before you leave the hospital We want to be sure that we explained your diabetes instructions well, so that you know how to
Lantus levemir conversion
 Lantus levemir conversion Search Learn about starting insulin-naïve patients with type 2 diabetes on Levemir. Read Important Safety & Prescribing Info on the HCP Website. Lantus and Levemir have a variety
Lantus levemir conversion Search Learn about starting insulin-naïve patients with type 2 diabetes on Levemir. Read Important Safety & Prescribing Info on the HCP Website. Lantus and Levemir have a variety
Objectives 2/13/2013. Figuring out the dose. Sub Optimal Glycemic Control: Moving to the Appropriate Treatment
 Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Technology for Diabetes: 101 Basic Rules of the Road. Karen Hamon RN, BSN, CDE Stephen Stone MD, FAAP Neil H. White, MD, CDE
 Technology for Diabetes: 101 Basic Rules of the Road Karen Hamon RN, BSN, CDE Stephen Stone MD, FAAP Neil H. White, MD, CDE Quick Pump Facts! o Constant insulin supply o Pager-sized mini-computer worn
Technology for Diabetes: 101 Basic Rules of the Road Karen Hamon RN, BSN, CDE Stephen Stone MD, FAAP Neil H. White, MD, CDE Quick Pump Facts! o Constant insulin supply o Pager-sized mini-computer worn
Diabetes Head to Toe May 31, 2017
 Innovations in Insulin Joanne Reid RN CDE jmreid@gbhs.on.ca Danielle Benedict RPh Outline Setting the stage Insulin as pancreas replacement therapy Commonly used insulins New insulins Case Studies Dosing
Innovations in Insulin Joanne Reid RN CDE jmreid@gbhs.on.ca Danielle Benedict RPh Outline Setting the stage Insulin as pancreas replacement therapy Commonly used insulins New insulins Case Studies Dosing
In-hospital management of diabetes
 Dr. Tom Elliott MBBS, FRCPC Medical Director 400-210 W Broadway phone: 604.683.3734 Vancouver, BC fax: 604.628.3821 V5Y 3W2 Canada email: moa@bcdiabetes.ca In-hospital management of diabetes General Management
Dr. Tom Elliott MBBS, FRCPC Medical Director 400-210 W Broadway phone: 604.683.3734 Vancouver, BC fax: 604.628.3821 V5Y 3W2 Canada email: moa@bcdiabetes.ca In-hospital management of diabetes General Management
Drug Effectiveness Review Project Summary Report Long acting Insulins
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
These Aren t Your Average Rookies: A Primer on New and Emerging Insulins. Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP
 These Aren t Your Average Rookies: A Primer on New and Emerging Insulins Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP Disclosures Eli Lilly & Company: Advisory board member Boehringer Ingelheim: Advisory
These Aren t Your Average Rookies: A Primer on New and Emerging Insulins Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP Disclosures Eli Lilly & Company: Advisory board member Boehringer Ingelheim: Advisory
Degludec lantus conversion
 Degludec lantus conversion Search embarazadas con elevado riesgo de enfermedad tiroidea usando la. There are various possible causes of a high blood sugar level in the morning: The Dawn Phenomenon which
Degludec lantus conversion Search embarazadas con elevado riesgo de enfermedad tiroidea usando la. There are various possible causes of a high blood sugar level in the morning: The Dawn Phenomenon which
Management of Diabetes New Concepts New Devices New Medications. Richard J. Comi, MD Professor of Medicine Geisel School of Medicine at Dartmouth
 Management of Diabetes New Concepts New Devices New Medications Richard J. Comi, MD Professor of Medicine Geisel School of Medicine at Dartmouth Objectives: At the end of this lecture, the learner will
Management of Diabetes New Concepts New Devices New Medications Richard J. Comi, MD Professor of Medicine Geisel School of Medicine at Dartmouth Objectives: At the end of this lecture, the learner will
Pediatric Diabetes Update Fran R. Cogen, MD, CDE Professor of Pediatrics Director, Diabetes Services
 1.19.18 Pediatric Diabetes Update Fran R. Cogen, MD, CDE Professor of Pediatrics Director, Diabetes Services DISCLOSURES 1. No financial incentives 2. Volunteer Positions 1. National Certification Board
1.19.18 Pediatric Diabetes Update Fran R. Cogen, MD, CDE Professor of Pediatrics Director, Diabetes Services DISCLOSURES 1. No financial incentives 2. Volunteer Positions 1. National Certification Board
8/21/2017 UNRAVELING THE CROWED INSULIN SCENE. A Practical Overview of Insulin Focusing on New Insulin Preparations
 UNRAVELING THE CROWED INSULIN SCENE A Practical Overview of Insulin Focusing on New Insulin Preparations Patricia Garnica MS, ANP-BC, CDE, CDTC North Shore University Hospital, Manhasset, N.Y. October
UNRAVELING THE CROWED INSULIN SCENE A Practical Overview of Insulin Focusing on New Insulin Preparations Patricia Garnica MS, ANP-BC, CDE, CDTC North Shore University Hospital, Manhasset, N.Y. October
The Diabetes Guidelines Trek: The Next Generation. Inpatient Diabetes Guidelines. Learning Objectives. Current Inpatient Guidelines
 The Diabetes Guidelines Trek: The Next Generation J. Christopher Lynch, PharmD, BCACP Southern Illinois University Edwardsville School of Pharmacy Susan Cornell BS, PharmD, CDE, FAPhA, FAADE Midwestern
The Diabetes Guidelines Trek: The Next Generation J. Christopher Lynch, PharmD, BCACP Southern Illinois University Edwardsville School of Pharmacy Susan Cornell BS, PharmD, CDE, FAPhA, FAADE Midwestern
Module 5. Understanding Insulin Therapy
 Module 5. Understanding Insulin Therapy EDUCATIONAL OBJECTIVES Upon completion of this activity, participants will be better able to: 1. Define the basic physiologic concept of basal-bolus insulin; 2.
Module 5. Understanding Insulin Therapy EDUCATIONAL OBJECTIVES Upon completion of this activity, participants will be better able to: 1. Define the basic physiologic concept of basal-bolus insulin; 2.
DRUG ALLERGIES WT: KG
 DRUG AND TREATMENT Acute Diabetic Ketoacidosis Condition/Status ***(NOTE)*** For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS
DRUG AND TREATMENT Acute Diabetic Ketoacidosis Condition/Status ***(NOTE)*** For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
DIABETES. overview of pharmacologic agents used in the management of. Overview 4/3/2014 OBJECTIVES. Injectable Agents
 overview of pharmacologic agents used in the management of DIABETES Kyle Roberts, Pharm.D. PGY-1 Pharmacy Resident Saint Alphonsus RMC 1. List the different classes of diabetes medications, including the
overview of pharmacologic agents used in the management of DIABETES Kyle Roberts, Pharm.D. PGY-1 Pharmacy Resident Saint Alphonsus RMC 1. List the different classes of diabetes medications, including the
Pharmacology. Kacy Aderhold, MSN, APRN-CNS, CMSRN
 Pharmacology Kacy Aderhold, MSN, APRN-CNS, CMSRN Biguanides Decreases hepatic glucose production and improves insulin sensitivity (increases number of insulin receptors) Common Adverse Reaction: diarrhea
Pharmacology Kacy Aderhold, MSN, APRN-CNS, CMSRN Biguanides Decreases hepatic glucose production and improves insulin sensitivity (increases number of insulin receptors) Common Adverse Reaction: diarrhea
Poll Question 2. Special Boot Camp Workshop Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services.
 Special Boot Camp Workshop Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Poll Question 1 Mary takes 6 units lispro (Humalog) before dinner. Which BG result reflects
Special Boot Camp Workshop Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Poll Question 1 Mary takes 6 units lispro (Humalog) before dinner. Which BG result reflects
Starting and Helping People with Type 2 Diabetes on Insulin
 Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
ANNUAL MEETING 2 #FSHP2017
 FSHP Disclosure Strategies for Glycemic Management in the Inpatient Setting: Guidelines vs. Reality Melissa Marshall, PharmD, BCPS Jeffrey Ruff, PharmD We do not have (nor does any immediate family member
FSHP Disclosure Strategies for Glycemic Management in the Inpatient Setting: Guidelines vs. Reality Melissa Marshall, PharmD, BCPS Jeffrey Ruff, PharmD We do not have (nor does any immediate family member
Insulin 10/11/17. Disclosures. Objectives. Speaker and Consultant for Jansen and Healthscripts Speaker and Consultant for Boehringer Ingelheim (BI)
") Insulin The What, When, Where, Who and Why Disclosures Speaker and Consultant for Jansen and Healthscripts Speaker and Consultant for Boehringer Ingelheim (BI) Objectives Define background and history
Insulin The What, When, Where, Who and Why Disclosures Speaker and Consultant for Jansen and Healthscripts Speaker and Consultant for Boehringer Ingelheim (BI) Objectives Define background and history
Update on Insulin-based Agents for T2D
 Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Insulin Pump Therapy. WakeMed Children s Endocrinology & Diabetes WakeMed Health & Hospitals Version 1.3, rev 5/21/13 MP
 Insulin Pump Therapy WakeMed Children s Endocrinology & Diabetes Overview What is an insulin pump? What are the advantages and disadvantages of an insulin pump? Lifestyle Changes Food Management Exercise
Insulin Pump Therapy WakeMed Children s Endocrinology & Diabetes Overview What is an insulin pump? What are the advantages and disadvantages of an insulin pump? Lifestyle Changes Food Management Exercise
Drug Use Criteria: Exogenous Insulin Products
 Texas Vendor Program Use Criteria: Exogenous Products Publication History 1. Developed June 2017. Notes: Information on indications for use or diagnosis is assumed to be unavailable. All criteria may be
Texas Vendor Program Use Criteria: Exogenous Products Publication History 1. Developed June 2017. Notes: Information on indications for use or diagnosis is assumed to be unavailable. All criteria may be
Insulin Pump Therapy
 Patient and Family Education Insulin Pump Therapy The insulin pump is a device that gives insulin to the body at a steady rate. With the pump you won t need daily shots. This handout describes how insulin
Patient and Family Education Insulin Pump Therapy The insulin pump is a device that gives insulin to the body at a steady rate. With the pump you won t need daily shots. This handout describes how insulin
INSULIN OVERVIEW. Type Brand Name Onset Peak Duration Role in glucose management Page Rapid-Acting lispro min. 3-5 hrs min.
 INSULIN OVERVIEW Type Brand Name Onset Peak Duration Role in glucose management Page Rapid-Acting lispro Humalog 15-30 min 30-90 min 3-5 hrs aspart glulisine Short-Acting Regular insulin NovoLog Apidra
INSULIN OVERVIEW Type Brand Name Onset Peak Duration Role in glucose management Page Rapid-Acting lispro Humalog 15-30 min 30-90 min 3-5 hrs aspart glulisine Short-Acting Regular insulin NovoLog Apidra
Insulin Management. By Susan Henry Diabetes Specialist Nurse
 Insulin Management By Susan Henry Diabetes Specialist Nurse The Discovery of Insulin - 1921 - Banting & Best University Of Toronto Discovered hormone insulin in pancreatic extract of dog - Marjorie the
Insulin Management By Susan Henry Diabetes Specialist Nurse The Discovery of Insulin - 1921 - Banting & Best University Of Toronto Discovered hormone insulin in pancreatic extract of dog - Marjorie the
Conversion from lantus to tresiba
 Conversion from lantus to tresiba Search dosages for Diabetes Type 2 and Diabetes Type 1; plus renal, liver and. Forecast your health care. Every time you have a symptom or are diagnosed of a condition,
Conversion from lantus to tresiba Search dosages for Diabetes Type 2 and Diabetes Type 1; plus renal, liver and. Forecast your health care. Every time you have a symptom or are diagnosed of a condition,
Basal Insulin Drug Class Prior Authorization Protocol
 Basal Insulin Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
Basal Insulin Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
New Therapies for Diabetes Management: Hope or Headache?
 New Therapies for Diabetes Management: Hope or Headache? Elizabeth Stephens, MD, FACP PMG- Endocrinology Elizabeth.Stephens@providence.org November 2018 Disclosures None 1 Objectives Discussion of 3 rd
New Therapies for Diabetes Management: Hope or Headache? Elizabeth Stephens, MD, FACP PMG- Endocrinology Elizabeth.Stephens@providence.org November 2018 Disclosures None 1 Objectives Discussion of 3 rd
For patients uncontrolled on multiple daily injections of insulin. A quick-start guide for your practice ALL-DAY CONTROL WITH
 For patients uncontrolled on multiple daily injections of insulin A quick-start guide for your practice Dosing guidance 1,* V-Go: 3 options 1 For initiating V-Go in patients switching from MDI The majority
For patients uncontrolled on multiple daily injections of insulin A quick-start guide for your practice Dosing guidance 1,* V-Go: 3 options 1 For initiating V-Go in patients switching from MDI The majority
DIABETES. Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes. November 2013
 DIABETES Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes November 2013 mbruskewitz@outlook.com Objectives Part 1 Overview of Endocrine Physiology Pathophysiology of Diabetes Diabetes
DIABETES Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes November 2013 mbruskewitz@outlook.com Objectives Part 1 Overview of Endocrine Physiology Pathophysiology of Diabetes Diabetes
Information for Patients
 Information for Patients Guidance for Diabetic Persons having an OGD or Bronchoscopy This guidance is provided to assist with your preparation for your endoscopic procedure. If you feel unclear about how
Information for Patients Guidance for Diabetic Persons having an OGD or Bronchoscopy This guidance is provided to assist with your preparation for your endoscopic procedure. If you feel unclear about how
Insulin Basic facts. Patient Education Patient Care Services. What is insulin? What types of insulin are there? Basal Insulin
 Patient Education Insulin Basic facts Insulin is a protein made by the pancreas that allows your cells to use glucose for energy. There are different types of insulin: Basal long-acting insulin that controls
Patient Education Insulin Basic facts Insulin is a protein made by the pancreas that allows your cells to use glucose for energy. There are different types of insulin: Basal long-acting insulin that controls
Supplemental Health Record and Authorization for Care of Child with Insulin Dependent Diabetes
 477 Beaverkill Road Olivebridge, New York 12461 (845) 657-8333 Ext. 15 Fax (845) 657-8489 martin.bernstein@ashokancenter.org www.ashokancenter.org 2012-13 Supplemental Health Record and Authorization for
477 Beaverkill Road Olivebridge, New York 12461 (845) 657-8333 Ext. 15 Fax (845) 657-8489 martin.bernstein@ashokancenter.org www.ashokancenter.org 2012-13 Supplemental Health Record and Authorization for
SCHOOL HEALTH PLAN: DIABETES
 BRANDON FLORENCE MCLAURIN NORTHWEST PELAHATCHIE RANKIN COUNTY SCHOOL DISTRICT GREAT TO BEST PISGAH PUCKETT RICHLAND RANKIN COUNTY SCHOOL DISTRICT SCHOOL HEALTH PLAN: DIABETES of Plan: Effective s: This
BRANDON FLORENCE MCLAURIN NORTHWEST PELAHATCHIE RANKIN COUNTY SCHOOL DISTRICT GREAT TO BEST PISGAH PUCKETT RICHLAND RANKIN COUNTY SCHOOL DISTRICT SCHOOL HEALTH PLAN: DIABETES of Plan: Effective s: This
January 7, 5:00 p.m. EST
 Study 3-151 Phase 2 Trial: Preliminary Results BIOD-531, a Concentrated Ultra-Rapid-Acting Prandial/Basal Insulin, Demonstrates Superior Post-Meal Glucose Control Compared to Marketed Prandial/Basal Insulins
Study 3-151 Phase 2 Trial: Preliminary Results BIOD-531, a Concentrated Ultra-Rapid-Acting Prandial/Basal Insulin, Demonstrates Superior Post-Meal Glucose Control Compared to Marketed Prandial/Basal Insulins
Pumping Insulin is it for your patients?
 Pumping Insulin is it for your patients? YOU CAN make managing diabetes easier. Fred Porcase D.O. Disclosures to Participants Conflicts Of Interest and Financial Relationships Disclosures: No professional
Pumping Insulin is it for your patients? YOU CAN make managing diabetes easier. Fred Porcase D.O. Disclosures to Participants Conflicts Of Interest and Financial Relationships Disclosures: No professional
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions. Insulins. Rapid Short Intermediate Long Mix
 Diabetes Medications Diabetes Medications Type 1 Insulin is needed Type 2 Oral Diabetes Medications Or Oral Diabetes Medications plus Insulin Or Insulin Alone Diabetes Medications Secretagogues Glipizide
Diabetes Medications Diabetes Medications Type 1 Insulin is needed Type 2 Oral Diabetes Medications Or Oral Diabetes Medications plus Insulin Or Insulin Alone Diabetes Medications Secretagogues Glipizide
How they work and when to take them. Diabetes Medications
 How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
Important Stuff. Basal Bolus What Adjustments? Pt weighs 80kg
 Diabetes Boot Camp Class 4 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Special Insulin and Pattern Management Diabetes Education Services 1998-2015. All rights
Diabetes Boot Camp Class 4 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Special Insulin and Pattern Management Diabetes Education Services 1998-2015. All rights
Exogenous Insulin in type 2 DM
 Exogenous Insulin in type 2 DM Russell Scott 2015 Part 1: Some basic biochemistry for Insulin absorption and action MY CHECK LIST Factors influencing insulin action: Forgets to inject Amount given Timing
Exogenous Insulin in type 2 DM Russell Scott 2015 Part 1: Some basic biochemistry for Insulin absorption and action MY CHECK LIST Factors influencing insulin action: Forgets to inject Amount given Timing
Understanding Diabetes and Insulin Delivery Systems
 Page 1 This program has been supported by an educational grant from Sanofi Aventis Scott K. Stolte, Pharm.D. Associate Dean, Academic Affairs Bernard J. Dunn School of Pharmacy Shenandoah University Winchester,
Page 1 This program has been supported by an educational grant from Sanofi Aventis Scott K. Stolte, Pharm.D. Associate Dean, Academic Affairs Bernard J. Dunn School of Pharmacy Shenandoah University Winchester,
HAP PA-HEN Achieving More Together
 HAP PA-HEN Achieving More Together Managing Hyperglycemia in the Hospital: Strategies for Safe and Effective Care Pennsylvania Patient Safety Authority Managing Hyperglycemia in the Hospital: Strategies
HAP PA-HEN Achieving More Together Managing Hyperglycemia in the Hospital: Strategies for Safe and Effective Care Pennsylvania Patient Safety Authority Managing Hyperglycemia in the Hospital: Strategies
How to Fight Diabetes and Win. Diabetes. Medications
 How to Fight Diabetes and Win Diabetes Medications MEDICATIONS FOR DIABETES According to the American Diabetes Association, 85% of adults diagnosed with diabetes take insulin and/or oral medication to
How to Fight Diabetes and Win Diabetes Medications MEDICATIONS FOR DIABETES According to the American Diabetes Association, 85% of adults diagnosed with diabetes take insulin and/or oral medication to
Managing Diabetes when you are having a colonoscopy
 Managing Diabetes when you are having a colonoscopy Disclaimer This is general information developed by The Ottawa Hospital. It is not intended to replace the advice of a qualified health-care provider.
Managing Diabetes when you are having a colonoscopy Disclaimer This is general information developed by The Ottawa Hospital. It is not intended to replace the advice of a qualified health-care provider.
Spending on Individuals with Type 1 Diabetes and the Role of Rapidly Increasing Insulin Prices
 Spending on Individuals with Type 1 Diabetes and the Role of Rapidly Increasing Insulin Prices Authors: Jean Fuglesten Biniek William Johnson January 2019 Insulin Prices Were the Primary Driver of Rapid
Spending on Individuals with Type 1 Diabetes and the Role of Rapidly Increasing Insulin Prices Authors: Jean Fuglesten Biniek William Johnson January 2019 Insulin Prices Were the Primary Driver of Rapid
Timely!Insulinization In!Type!2! Diabetes,!When!and!How
 Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Diabetes Technology Continuous Subcutaneous Insulin Infusion Therapy And Continuous Glucose Monitoring In Adults: An Endocrine Society Clinical
 Diabetes Technology Continuous Subcutaneous Insulin Infusion Therapy And Continuous Glucose Monitoring In Adults: An Endocrine Society Clinical Practice Guideline Task Force Members Anne Peters, MD (Chair)
Diabetes Technology Continuous Subcutaneous Insulin Infusion Therapy And Continuous Glucose Monitoring In Adults: An Endocrine Society Clinical Practice Guideline Task Force Members Anne Peters, MD (Chair)