Chronic deep venous occlusions: Case planning, recanalization and stent technique
|
|
|
- Gabriel Blake
- 5 years ago
- Views:
Transcription

1 Chronic deep venous occlusions: Case planning, recanalization and stent technique Michael K. W. Lichtenberg, FESC German Venous Center Arnsberg, Germany

2 Conflict of Interest - Disclosure Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below. Affiliation/Financial Relationship Company 1. Honoraria for lectures: CR Bard, Veniti, AB Medica, Volcano, Optimed GmbH, Straub Medical, Terumo, Biotronik, Veryan 2. Honoraria for advisory board activities: Veniti, Optimed GmbH, Straub Medical, Biotronik, Veryan, Boston Scientific 3. Participation in clinical trials: Biotronik, CR Bard, Veryan, Straub Medical, Veniti, TVA Medical, Boston Scientific, LimFlow 4. Research funding: Biotronik, Boston Scientific, Veryan, Veniti, AB Medica

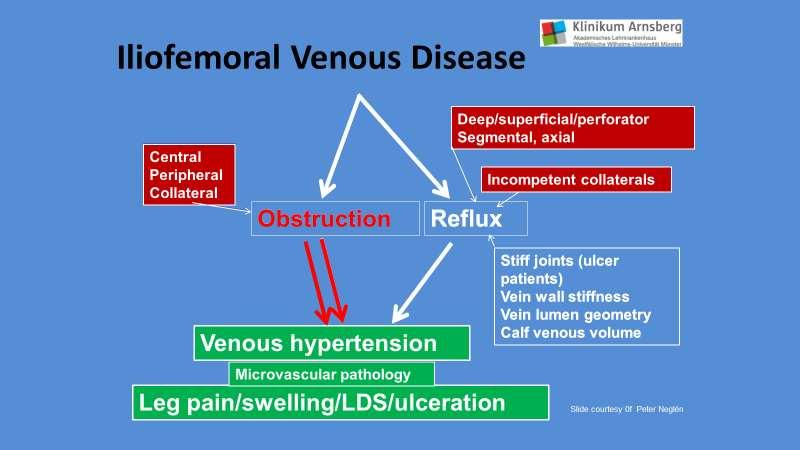
3 Complexity of Venous Hemodynamics Artery High-pressure High-velocity Small-volume High-resistance diverging pipe system Pulsatile flow Stiffer vessel walls Vein Low-pressure Low-velocity Large-volume Low-resistance converging pipe system Phasic flow High compliance Valves
4


5 C6, 58 year female, postthrombotic syndrome

6
 4 x")

7 Sinus XL Stent (22 x 80 mm) 4 x Veniti Stents (16 x 120 mm + 14 x 60 mm)
8 What has ilio-caval vein stenting shown us? Venous outflow obstruction plays an important role in clinical expression of CVD, particularly pain 1,3-4 Ulcerated limbs have a high rate of obstruction (37-52%) 5-6 In limbs with obstruction, ulcers occur rarely with isolated obstruction (4%), more often in association with reflux (30%) 1 Treatment results in impressive clinical relief of pain, swelling, VCSS, VDS and QoL, even when associated reflux is left untreated 1-3 Treatment results in healing of ulcers, despite untreated reflux, in 55-58% of the patients 1,3,6 1 Neglén et al, J Vasc Surg 2003;38: Hartung et al, J Vasc Surg 2005;42: Neglén et al, J Vasc Surg 2007;46: Delis KT et al. Ann Surg 2007, 245: Marston et al, J Vasc Surg 2011, 53: Alhalbouni S et al, Ann Vasc Surg. 2012, 26:185-9
9 How do I find patients with ilio-femoral venous obstruction? Awareness Think obstruction! Specific clinical signs and symptoms severe C 3, C 4-6 abdominal collaterals, atypical vv, early vv recurrence typical venous claudication venous visceral type of pain/discomfort postthrombotic disease pain out of proportion to lesion no detectable lesion explaining symptoms
10 Morphological Studies Duplex Doppler scanning (including pelvic outflow) Ascending venogram Transfemoral antegrade venogram CT-V, MR-V or IVUS Morphological diameter/ area stenosis >50% is considered significant.

11 Intravascular Ultrasound Evaluation of lumen diameter and stenosis Evaluation of thrombus, fibrotic tissue and scare tissue Evaluation of compression Intervention without contrast dye Peter Neglen 2002 Journal of Vascular Surgery: In comparison to standard venography IVUS appears to be superior for identify morphologic changes of iliac venous outflow obstruction


12 Visions PV.035 Digital IVUS Catheter Visions PV.035 IVUS Catheter * Product Overview 60 mm field of view, free of wire artifact - 10 MHz 90 cm working length Over-the-wire design guide wire compatible Min. Sheath 8.5 F New radiopaque and inked centimeter markers Radiopaque Markers 12





13 Venous obstruction
14 Can the patient be stented? Assess the Landing Zones Attempt to assess the central and peripheral extent of the disease before the intervention is scheduled using DUS, venogram, CTV, MRV etc. 1. Central landing zone a. Is the IVC patent? b. Does the disease involve the IVC? c. Is the potential outflow of the stent system appropriate? d. Is the contralateral venous outflow compromised? 2. Peripheral landing zone a. Is the CFV involved? b. Is there a potential landing zone in the CFV above the profundafemoral vein confluence? c. Is there a sufficient inflow from the periphery to sustain patency of a stent placed in the pelvic outflow?
15 Tips and trick for access Ipsilateral femoral vein Ultrasound guided access Vein is usually post-thrombotic scarred Orientation can be difficult Stiff hydrophilic guidewire (Terumo) Dilators 6,8,10 F Extra support, long sheaths Different projections

16
17 Recanalization Exchange for superstiff guidewire Advance PTA ballons (10,12,14,16,18 mm) Predilatation is eminent Standard inflation pressure is 6 12 atm (PAINFULL!!!!) No rupture risk!
18 Stenting Double barrel Apposition Fenestration Bifurcation
19 Venous Stenting is Not New Significant body of clinical work Existing stents Wallstent Good success treating obstructive component of many venous disorders Current generation of stents being studied VIVO Trial Zilver Vena (Cook Medical) VIRTUS Trial VICI VENOUS STENT (VENITI, Inc.) 19








20 Venous Stent Attributes Self-expandable Crush resistant across length of stent Sufficient chronic outward force Sufficient wall coverage Flexibility sufficient to resist kink at physiological angles Durability allowing repeated shortening, twisting, and bending at the groin Minimal foreshortening on deployment and balloon dilation Predictable, consistent deployment Strength Flexibility Lumen quality




21 Stent options! Boston Wallstent Optimed Cook Zilver Vena VIVO (EU) Trial Veniti Vici VIRTUS Trial Optimed Sinus obliquus Sinus Obliquus-01-NIS Bard Venovo VERNACULAR Trial Upcoming: Medtronic, Gore, ab Medica, INTACT, Abbott Vascular

22

23


24 Venovo Stent 14 x 120 mm and 14 x 80 mm on both CIV and EIV



25 Performance Characteristics Closed Cell Open Cell Design Attributes All struts interconnected Not all struts interconnected Performance Crush Resistance ++ + Flexibility + ++ Coverage ++ +
26 Radial Resistive Force at 1mm oversize (N/mm) Local Compression Force (N) Radial Force and Crush Resistance Radial Resistive Force Crush Resistance BARD VENOVO 14X160 N=20 OPTIMED SINUS VENOUS 14X80 N=3 COOK ZILVER VENA 14X100 N=2 BARD VENOVO 14X160 N=20 OPTIMED SINUS VENOUS 14X80 N=3 COOK ZILVER VENA 14X100 N=3 Bench testing may not be indicative of clinical performance. Different test methods may yield different results. Competitive testing samples represent commercially available venous stents with CE mark as of June This product is not available for sale in the US



27 3 Point Bending Stiffness (N) Stent Flexibility BARD VENOVO 14X160 OPTIMED SINUS VENOUS 14X80 COOK ZILVER VENA 14X100 Bard Bard N=20 Optimed Sinus Venous N=3 Cook Zilver Vena N=3 Bench testing may not be indicative of clinical performance. Different test methods may yield different results. Competitive testing samples represent commercially available venous stents with CE mark as of June Optimed Cook This product is not available for sale in the US

28 Results from VIVO-EU, a Prospective Study of the Zilver Vena TM Venous Stent in the Treatment of Symptomatic Iliofemoral Outflow Obstruction Michael Lichtenberg, M.D. and Jennifer McCann-Brown, Ph.D., RAC 1 Klinikum Arnsberg, Germany; 2 Cook Research Incorporated On behalf of the Investigators: Christoph Binkert, M.D. Narayan Karunanithy, M.D. Gerard O`Sullivan, M.D. Marta Ramirez Ortega, M.D. 28
29 Real World Patient Population Medical History Reported (N=35) Clotting disorder (family history) 14.3% (5) Bleeding diathesis/coagulopathy 14.3% (5) Pulmonary embolism (history or current) 20.0% (7) Deep vein thrombosis (DVT) 62.9% (22) Acute DVT Acute DVT on Chronic DVT Acute DVT Acute DVT Chronic Chronic DVT DVT Chronic DVT 40.9% (9/22) 9.1% (2/22) 50.0% (11/22) 40.9% (9/22) 9.1% (2/22) 50.0% (11/22) DVT (family history) 28.6% (10) History of cancer 8.6% (3) Currently undergoing treatment 33.3% (1/3) 29
30 Side treated Lesion Location Vessel location(s) Baseline Lesion Data Left Right Site Reported (n=35) 94.3% (33) 5.7% (2) Core Lab (n=34) 94.1% (32) 5.9% (2) Common iliac vein 57.1% (20) 55.9% (19) External iliac, common iliac veins 22.9% (8) 14.7% (5) Common femoral, external iliac, common iliac veins 20.0% (7) 20.6% (7) Common femoral vein 0% (0) 5.9% (2) Femoral, common femoral, external iliac, common iliac veins Lesion Characteristics 0% (0) 2.9% (1) Lesion Length (mm; Mean ± SD) 106 ± 69 (n=35) (range: mm) 89.3 ±58.6 mm (n=31) (range: ) Total Occlusion 12.9% (4/31) % (7/31) 1 A determination of total occlusion could not be made in four patients.. Lesion data are consistent with previous reports for this population. 30
31 Major Adverse Events Major Adverse Event Frequency (n=35) Procedural bleeding requiring transfusion 0 Procedure- or device-related death 0 Clinically-driven target lesion reintervention for occlusion 1 1 Stent migration requiring intervention 0 Procedure- or device-related symptomatic pulmonary embolism 2 1 Procedure-related uncorrectable perforation 0 Procedure-related flow-limiting dissection of the target vessel 0 Total 2 1 A clinically-driven reintervention for occlusion at 155 days post-procedure. Edema and a prereintervention INR of 1.1; the occlusion was treated by thrombolysis, balloon angioplasty, and additional stent placement. 2 A symptomatic pulmonary embolism one day post-procedure, categorized as possibly related to the study procedure and managed by a change in medication. No additional clinical sequelae reported. 31
32 Venous Clinical Severity Score Improved Following Treatment Four patients did not complete 12-month follow-up due to unrelated death (n=1), withdrawal (n=1), or lost-tofollow-up (n=2). Patients with any reintervention (n=5) in the stented vessel were excluded from subsequent assessment of venous clinical symptoms. 32
. Patients with any reintervention (n=5) in the stented vessel were excluded from subsequent assessment of venous clinical symptoms.")
33 Venous Disability Score Improved Following Treatment Four patients did not complete 12-month follow-up due to unrelated death (n=1), withdrawal (n=1), or lost-tofollow-up (n=2). Patients with any reintervention (n=5) in the stented vessel were excluded from subsequent assessment of venous clinical symptoms. 33



34 VICI 14 x 120 mm

; Non Thrombotic (25%) Core Labs Venography: Syntactx IVUS: St.")
35 VIRTUS Feasibility Trial Design Objective Safety Assess safety & effectiveness in achieving patency of target venous lesion through 12-M post stent placement 30 days Post-thrombotic Effectiveness Primary 12-M Principal Investigators Study Design Patient Population Dr. William Marston Dr. Mahmood Razavi Prospective, multicenter, single arm nonrandomized, up to 45 sites worldwide 200 subjects with clinically significant chronic nonmalignant obstruction of the iliofemoral venous segment first 30 were feasibility. Image Courtesy of Mr. Stephen Black Non-thrombotic Etiologies: Post Thrombotic (75%); Non Thrombotic (25%) Core Labs Venography: Syntactx IVUS: St. Lukes DUS: VasCore/MGH X-Ray: Syntactx Image Courtesy of Mr. Mahmood Razavi

")


 1")

36 Demographics & Medical History Female 24 (80%) Male 6 (20%) Age CEAP* 44.4 ±14.1 years Baseline 0 3% (pain by VCSS Score of 2) 1 0% 2 0% 3 47% 4 40% 5 7% 6 3% Etiology PTS 63% NIVL 37%
 11.9 ±6.7 cm 1. Some patients have more than 1 lesion or lesion extends in multiple vein segments 2.")
37 Target Lesion Location Lesion 1 Location Patients N = 30 Left N = 25 (83%) CIV lesions 26/30 (87%) EIV lesions 18/30 (60%) CIV & EIV lesions 15/30 (50%) Right N = 5 (17%) Lesions that extended into CFV 2 Average Target Lesion Length 9/30 (30%) 11.9 ±6.7 cm 1. Some patients have more than 1 lesion or lesion extends in multiple vein segments 2. No lesions were isolated to the CFV alone

38 Patency by Duplex Ultrasound (Corelab Analysis) Patency Results of Feasibility Cohort (N=30) Primary Patency 1 Secondary Patency 1- M 93% 100% 6 M 90% 100% 12 M 93% 97% Courtesy of Dr. Ediberto Soto-Cora
 NIVL 37% 100% (11/11) 100% (11/11) PTS 63% 79% (15/19) 95% (18/19) Courtesy by Dr Michael Sadek All patients enrolled in the study will be followed until study")
39 Patency by Lesion Etiology (Site Reported) Patency Results at 12-Months (Site Reported) Full Cohort Etiology (N=30) Primary Patency 1 87% (26/30) Secondary Patency 97% (29/30) NIVL 37% 100% (11/11) 100% (11/11) PTS 63% 79% (15/19) 95% (18/19) Courtesy by Dr Michael Sadek All patients enrolled in the study will be followed until study completion
")
40 VCSS Pain Scale 45% had substantial symptomatic improvement (VCSS 2


41 CIVIQ-20
42 Arnsberg Venous Registry VENITI VICI VENOUS STENT System Objective Assess safety & effectiveness in achieving patency of target venous lesion through 36 months post stent placement (VENITI VICI Stent) Effectiveness Primary 12-M Principle Investigators Dr. Michael Lichtenberg Dr. Rick de Graaf Study Design Ongoing prospective, single arm, single center non-randomized registry FU 1 (4 weeks), FU 2 (6 months), FU 3 (12 months), FU 4 (24 months), FU 5 (36 months) Patient Population Subjects with clinically significant chronic non-malignant obstruction of the iliofemoral venous segment
43 Demographics N=90 Age in years (mean ± SD [range]) 57.4 ± 16.4 [19-84] Gender Male Female 47.8% (N=43) 52.2% (N=47) Ethnicity Caucasian 100% (N=90) Medical history N=90 Coagulation disorder 4.4% (N=4) Pulmonary embolism 24.4% (N=22) Deep vein thrombosis 47.8% (N=43) History of cancer 14.4% (N=13)
44 Lesion analysis N=90 Sides treated Both Left Right Lesion location(s) Left: Common iliac vein External iliac vein Common femoral vein Common iliac vein, external iliac vein Common iliac vein, external iliac vein, common femoral vein External iliac vein, common femoral vein Right: Common femoral vein Common iliac vein External iliac vein Common iliac vein, external iliac vein Common iliac vein, external iliac vein, common femoral vein External iliac vein, common femoral vein Both: 64 / 90 (71%) patients: Postthrombotic 26 / 90 (29%) patients: NIVL External iliac (R), common iliac (L) vein External iliac (R), common iliac (L), external iliac (L) vein Common iliac (R+L), external iliac (L) vein Common iliac (R+L), external iliac (R+L), common femoral (L) vein Common iliac (R+L), external iliac (R+L), common femoral (R+L) vein 7.8% (N=7) 74.4% (N=67) 17.8% (N=16) 37.8% (N=34) 4.4% (N=4) 2.2% (N=2) 17.8% (N=16) 8.9% (N=8) 3.3% (N=3) 2.2% (N=2) 3.3% (N=3) 6.7% (N=6) 1.1% (N=1) 1.1% (N=1) 3.3% (N=3) 1.1% (N=1) 2.2% (N=2) 2.2% (N=2) 1.1% (N=1) 1.1% (N=1)

45 Effectiveness analysis % Patentcy analysis % 100 % 100 % 97% 90 % 87 % 10 0 N=82 N=50 N=21 FU 4 w FU 6 mo FU 12 mo NIVL PTS
46 Mean VCSS score (±SD) Claudication, Pain, Swelling, Ulceration improvemnt N=90 N=82 N=50 N=21 0 Baseline FU1 FU2 FU3

47 Mean CEAP score (±SD) N=90 N=82 N=50 N=21 0 Baseline FU1 FU2 FU3

48 The BARD VENOVO Venous Stent Study A Prospective, Non-Randomized, Multi-Center, Single-Arm Study of the Treatment of Iliofemoral Occlusive Disease an Assessment for Effectiveness and Safety (VERNACULAR)
49 Study Design Type of Study Prospective, multi-center, global, singlearm, non-randomized study Number of Sites Up to 35 Number of Subjects 170 Primary Endpoint Follow Up Follow-Up Intervals 12-Months Post-Procedure 30-Days and 6-, 12-, 24-, & 36-Months Post-Procedure.









50 8 European Sites Dr. Gerard O Sullivan University College Hospital Galway Dr. Rick de Graaf Maastricht Universitair Medisch Centrum+ Maastricht Dr. Stephen Black St. Thomas, London Dr. Houman Jalaie Uniklinik RWTH, Aachen Prof. Salah Dine Qanadli Centre Hospitalier Universitaire Vaudois. Lausanne Dr. Michael Lichtenberg Klinikum Arnsberg Prof. Luis Miguel Izquierdo Lamoca, Hospitales Universitarios Montepríncipe, Madrid Prof. Thomas Zeller Universitäts- Herzzentrum Freiburg Bad Krozingen
51 Efficacy: Primary Endpoint Primary Patency rate at 12 months defined as Freedom from TVR Freedom from thrombus occlusion and stenosis > 50% as measured by DUS.


52

53
54 THANK YOU FOR YOUR ATTENTION

55

56 21 y, female, descending DVT in May Thurner syndrome.
57 KAHN et al. Determinants of health-related quality of life during the 2 years following deep vein thrombosis. Journal of Thrombosis and Haemostasis 2009, 6:

58 Standard Treatment vs. CDT Enden T, et al: CaVenT Study Follow-Up 24 months: Number needed to treat: 7 Lancet Jan 7;379(9810):31-8.


59 Long-Term Results using Catheter-directed Thrombolysis in 103 Lower Limbs with Acute Iliofemoral Venous Thrombosis N. Bækgaard, R. Broholm, S. Just, M. Jørgensen, L.P. Jensen European Journal of Vascular and Endovascular Surgery, Volume 39, Issue 1, Pages (January 2010) All patients with patent veins and normal valve function showed no sign of dermal pigmentation, ulceration or venous claudication at follow-up 1 major bleeding complication

60
61
62 2. Indications for early thrombus removal 2.1. We suggest a strategy of early thrombus removal in selected patients meeting the following criteria: (a) a first episode of acute iliofemoral deep venous thrombosis (b) symptoms <14 days in duration (c) a low risk of bleeding (d) ambulatory with good functional capacity and an acceptable life expectancy (Grade 2C)


63



64






, C. Tiefenbacher,")


65 Early Clot Removal Many Choices None Perfect! EKOS Peripheral Infusion System Trellis System AngioJet Aspirex (Rotational thrombectomy) Indigo System (Penumbra) 6 10 French M. Lichtenberg (Hrsg.), C. Tiefenbacher, M. Katoh, P. Minko, E. Minar, C. Wissgott, A. Storck, B. Hailer: Thrombektomie: medikamentös, mechnisch, operativ. Uni-med Verlag, 2013
66

67
68 The difference in PTS severity was almost entirely seen in the iliofemoral DVT patients with moderate/severe PTS seen in 18.4% of PCDT patients versus 28.2% in the no-pcdt group 2-Year ATTRACT Data Overall, the 2-year data supported the use of standard therapy/anticoagulation alone in most DVT patients PCDT was not shown to prevent postthrombotic syndrome (PTS) and was associated with increased bleeding. Leg pain and leg swelling were significantly improved in patients who received PCDT vs no-pcdt: (leg pain, 10 days: vs -1.29; P =.019; 30 days: vs -1.83; P =.026) (leg swelling, 10 days: vs +0.27; P =.024; 30 days: vs -0.28; P =.051). However, PCDT was shown to reduce early DVT symptoms as well as PTS severity The PCDT arm saw a statistically significant higher rate of major bleeding within 10 days (1.7% vs 0.3%; P =.049),
69 THANK YOU FOR YOUR ATTENTION
70 Chronic deep venous occlusions: Case planning, recanalization and stent technique Michael K. W. Lichtenberg, FESC German Venous Center Arnsberg, Germany
REKANALISATION CHRONISCH VENÖSER VERSCHLÜSSE. Michael K. W. Lichtenberg, FESC
 REKANALISATION CHRONISCH VENÖSER VERSCHLÜSSE Michael K. W. Lichtenberg, FESC Conflict of Interest - Disclosure Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
REKANALISATION CHRONISCH VENÖSER VERSCHLÜSSE Michael K. W. Lichtenberg, FESC Conflict of Interest - Disclosure Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Clinical results of venous stents. Michael K. W. Lichtenberg MD, FESC
 Clinical results of venous stents Michael K. W. Lichtenberg MD, FESC Conflict of Interest - Disclosure Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation
Clinical results of venous stents Michael K. W. Lichtenberg MD, FESC Conflict of Interest - Disclosure Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation
Patency rates and clinical results of the Veniti VICI Stent for treatment of iliac vein lesion Data from the Arnsberg Venous Registry
 Patency rates and clinical results of the Veniti VICI Stent for treatment of iliac vein lesion Data from the Arnsberg Venous Registry Michael K. W. Lichtenberg MD, FESC Conflict of Interest - Disclosure
Patency rates and clinical results of the Veniti VICI Stent for treatment of iliac vein lesion Data from the Arnsberg Venous Registry Michael K. W. Lichtenberg MD, FESC Conflict of Interest - Disclosure
Venous stent experience in Arnsberg Michael K. W. Lichtenberg MD, FESC
 Venous stent experience in Arnsberg Michael K. W. Lichtenberg MD, FESC IMPORTANT INFORMATION: These materials are intended to describe common clinical considerations and procedural steps for the on-label
Venous stent experience in Arnsberg Michael K. W. Lichtenberg MD, FESC IMPORTANT INFORMATION: These materials are intended to describe common clinical considerations and procedural steps for the on-label
VIVO-EU Results: Prospective European Study of the Zilver Vena TM Venous Stent in the Treatment of Symptomatic Iliofemoral Venous Outflow Obstruction
 VIVO-EU Results: Prospective European Study of the Zilver Vena TM Venous Stent in the Treatment of Symptomatic Iliofemoral Venous Outflow Obstruction Gerard J O Sullivan, M.D. and Jennifer McCann-Brown,
VIVO-EU Results: Prospective European Study of the Zilver Vena TM Venous Stent in the Treatment of Symptomatic Iliofemoral Venous Outflow Obstruction Gerard J O Sullivan, M.D. and Jennifer McCann-Brown,
Techniques for thrombus removal in acute DVT Benefits of an Endovascular Approach for Rapid Flow Restoration in DVT
 Techniques for thrombus removal in acute DVT Benefits of an Endovascular Approach for Rapid Flow Restoration in DVT Michael K. W. Lichtenberg, MD, FESC Vascular Centre Arnsberg, Germany Disclosure Speaker
Techniques for thrombus removal in acute DVT Benefits of an Endovascular Approach for Rapid Flow Restoration in DVT Michael K. W. Lichtenberg, MD, FESC Vascular Centre Arnsberg, Germany Disclosure Speaker
- Our patients with iliofemoral DVT - Effective thrombus removal with purely mechanical thrombectomy can lead to better outcomes
 - Our patients with iliofemoral DVT - Effective thrombus removal with purely mechanical thrombectomy can lead to better outcomes Michael K. W. Lichtenberg, FESC Conflict of Interest - Disclosure Within
- Our patients with iliofemoral DVT - Effective thrombus removal with purely mechanical thrombectomy can lead to better outcomes Michael K. W. Lichtenberg, FESC Conflict of Interest - Disclosure Within
VIRTUS: Trial Design and Primary Endpoint Results
 VIRTUS: Trial Design and Primary Endpoint Results Mahmood K. Razavi, MD St. Joseph Cardiac and Vascular Center Orange, CA, USA IMPORTANT INFORMATION: These materials are intended to describe common clinical
VIRTUS: Trial Design and Primary Endpoint Results Mahmood K. Razavi, MD St. Joseph Cardiac and Vascular Center Orange, CA, USA IMPORTANT INFORMATION: These materials are intended to describe common clinical
Improved clinical outcomes Evidence on venous mechanical thrombectomy followed by stenting
 Improved clinical outcomes Evidence on venous mechanical thrombectomy followed by stenting Michael K. W. Lichtenberg, MD, FESC Vascular Centre Arnsberg, Germany German Venous Centre Arnsberg, Germany Disclosure
Improved clinical outcomes Evidence on venous mechanical thrombectomy followed by stenting Michael K. W. Lichtenberg, MD, FESC Vascular Centre Arnsberg, Germany German Venous Centre Arnsberg, Germany Disclosure
Improved clinical outcomes Evidence on venous thrombectomy followed by stenting
 Improved clinical outcomes Evidence on venous thrombectomy followed by stenting Michael K. W. Lichtenberg, MD, FESC Vascular Centre Arnsberg, Germany Venous Centre Arnsberg, Germany Disclosure Speaker
Improved clinical outcomes Evidence on venous thrombectomy followed by stenting Michael K. W. Lichtenberg, MD, FESC Vascular Centre Arnsberg, Germany Venous Centre Arnsberg, Germany Disclosure Speaker
Complex ilio-caval revascularization in chronic venous obstruction with the Venovo Stent. Michael K. W. Lichtenberg MD, FESC
 Complex ilio-caval revascularization in chronic venous obstruction with the Venovo Stent Michael K. W. Lichtenberg MD, FESC German Venous Center Arnsberg, Germany Not available for sale or distribution
Complex ilio-caval revascularization in chronic venous obstruction with the Venovo Stent Michael K. W. Lichtenberg MD, FESC German Venous Center Arnsberg, Germany Not available for sale or distribution
The Ideal Venous Stent and Early Results from Venous Stent Trials PNEC, Seattle
 The Ideal Venous Stent and Early Results from Venous Stent Trials 2017 PNEC, Seattle Bill Marston MD Professor, Div of Vascular Surgery University of N. Carolina DISCLOSURES William Marston, MD Consultant/Advisory
The Ideal Venous Stent and Early Results from Venous Stent Trials 2017 PNEC, Seattle Bill Marston MD Professor, Div of Vascular Surgery University of N. Carolina DISCLOSURES William Marston, MD Consultant/Advisory
VIRTUS Trial: Pivotal Cohort 12-Month Primary Safety and Efficacy Results of the VICI Venous Stent System
 VIRTUS Trial: Pivotal Cohort 12-Month Primary Safety and Efficacy Results of the VICI Venous Stent System Mahmood K. Razavi, MD St. Joseph Cardiac and Vascular Center Orange, CA, USA Disclosure Speaker
VIRTUS Trial: Pivotal Cohort 12-Month Primary Safety and Efficacy Results of the VICI Venous Stent System Mahmood K. Razavi, MD St. Joseph Cardiac and Vascular Center Orange, CA, USA Disclosure Speaker
The evidence for venous interventions is evolving- many patients do actually benefit. Nils Kucher University Hospital Bern Switzerland
 The evidence for venous interventions is evolving- many patients do actually benefit Nils Kucher University Hospital Bern Switzerland Disclosure Speaker name: Nils Kucher X X I have the following potential
The evidence for venous interventions is evolving- many patients do actually benefit Nils Kucher University Hospital Bern Switzerland Disclosure Speaker name: Nils Kucher X X I have the following potential
Aspirex for Upper and Lower Extremity DVT
 Aspirex for Upper and Lower Extremity DVT Steven Kum MD Vascular & Endovascular Surgeon Director of Vascular Service Changi General Hospital Singapore Disclosure Speaker name:... I have the following potential
Aspirex for Upper and Lower Extremity DVT Steven Kum MD Vascular & Endovascular Surgeon Director of Vascular Service Changi General Hospital Singapore Disclosure Speaker name:... I have the following potential
On Which Criteria Do You Select Your Stent for Ilio-femoral Venous Obstruction? North American Point of View
 On Which Criteria Do You Select Your Stent for Ilio-femoral Venous Obstruction? North American Point of View Peter Gloviczki, MD Ying Huang, MD, PhD Division of Vascular and Endovascular Surgery, Mayo
On Which Criteria Do You Select Your Stent for Ilio-femoral Venous Obstruction? North American Point of View Peter Gloviczki, MD Ying Huang, MD, PhD Division of Vascular and Endovascular Surgery, Mayo
Case Study of Implantation of a VICI VENOUS STENT - Combined NIVL and PTS Stenting
 Case Study of Implantation of a VICI VENOUS STENT - Combined NIVL and PTS Stenting Courtesy of Mr. Stephen Black United kingdom Patient History 25 y/o female 2011: Conservatively treated ilio-femoral DVT
Case Study of Implantation of a VICI VENOUS STENT - Combined NIVL and PTS Stenting Courtesy of Mr. Stephen Black United kingdom Patient History 25 y/o female 2011: Conservatively treated ilio-femoral DVT
Successful recanalisation of venous thrombotic occlusions with Aspirex mechanical thrombectomy. Michael K. W. Lichtenberg
 Successful recanalisation of venous thrombotic occlusions with Aspirex mechanical thrombectomy Michael K. W. Lichtenberg Disclosure Speaker name: Michael Lichtenberg... I have the following potential conflicts
Successful recanalisation of venous thrombotic occlusions with Aspirex mechanical thrombectomy Michael K. W. Lichtenberg Disclosure Speaker name: Michael Lichtenberg... I have the following potential conflicts
Michael K. W. Lichtenberg MD, FESC on behalf of KANSHAS 1 investigators; Tepe G, Müller-Hülsbeck S, Deloose K, Verbist J, Goverde P, Zeller T
 Interim 30-day analysis from the KANSHAS 1 study of the novel KANSHAS drug coated balloon for treatment of femoropopliteal occlusive disease; a latest first-in-human study Michael K. W. Lichtenberg MD,
Interim 30-day analysis from the KANSHAS 1 study of the novel KANSHAS drug coated balloon for treatment of femoropopliteal occlusive disease; a latest first-in-human study Michael K. W. Lichtenberg MD,
Future Devices of Venous Interventions
 Future Devices of Venous Interventions Director of Peripheral Vascular Medicine Department of Shin Kong Wu Ho-Su Memorial Hospital, Taiwan Interventional Cardiologist Tien-Yu Wu MD Disclosure Speaker name:...
Future Devices of Venous Interventions Director of Peripheral Vascular Medicine Department of Shin Kong Wu Ho-Su Memorial Hospital, Taiwan Interventional Cardiologist Tien-Yu Wu MD Disclosure Speaker name:...
Chronic Iliocaval Venous Occlusive Disease
 none Chronic Iliocaval Venous Occlusive Disease David Rigberg, M.D. Clinical Professor of Surgery Division of Vascular Surgery University of California Los Angeles Chronic Venous Occlusive Disease Chronic
none Chronic Iliocaval Venous Occlusive Disease David Rigberg, M.D. Clinical Professor of Surgery Division of Vascular Surgery University of California Los Angeles Chronic Venous Occlusive Disease Chronic
Should We Be More Aggressive in the Treatment of Acute DVT?
 DISCLOSURES Consultant Penumbra, Inc. UCSF Vascular Surgery Symposium April 6, 2017 K. Pallav Kolli, MD Assistant Professor of Clinical Radiology University of California, San Francisco 17 yo male, DVT
DISCLOSURES Consultant Penumbra, Inc. UCSF Vascular Surgery Symposium April 6, 2017 K. Pallav Kolli, MD Assistant Professor of Clinical Radiology University of California, San Francisco 17 yo male, DVT
Pharmaco-mechanical techniques stand alone procedures? Peter Neglén, MD, PhD SP Vascular Center Limassol Cyprus
 Pharmaco-mechanical techniques stand alone procedures? Peter Neglén, MD, PhD SP Vascular Center Limassol Cyprus Faculty Disclosure Peter Neglén, M.D., Ph.D Stockholder/Founder of Veniti, Inc. Member, Medical
Pharmaco-mechanical techniques stand alone procedures? Peter Neglén, MD, PhD SP Vascular Center Limassol Cyprus Faculty Disclosure Peter Neglén, M.D., Ph.D Stockholder/Founder of Veniti, Inc. Member, Medical
VENOVO Venous Stent Update on the Vernacular Trial
 VENOVO Venous Stent Update on the Vernacular Trial Dr. Sunder Narasimhan, MBBS, MS Senior Consultant Vascular and Endovascular Surgeon Apollo Hospital, Bangalore, India VENOVO is a registered trademark
VENOVO Venous Stent Update on the Vernacular Trial Dr. Sunder Narasimhan, MBBS, MS Senior Consultant Vascular and Endovascular Surgeon Apollo Hospital, Bangalore, India VENOVO is a registered trademark
Venous Stents Placed Below the Inguinal Ligament: No Worries
 Venous Stents Placed Below the Inguinal Ligament: No Worries Disclosure Speaker name: Lowell S. Kabnick, MD, FACS, FACPh, RPhS... I have the following potential conflicts of interest to report: Consulting:
Venous Stents Placed Below the Inguinal Ligament: No Worries Disclosure Speaker name: Lowell S. Kabnick, MD, FACS, FACPh, RPhS... I have the following potential conflicts of interest to report: Consulting:
Understanding of the importance of venous
 The Critical Need for an Iliofemoral Venous Obstruction Classification System An overview of a potential classification system to better identify and treat iliofemoral venous outflow obstruction. BY WILLIAM
The Critical Need for an Iliofemoral Venous Obstruction Classification System An overview of a potential classification system to better identify and treat iliofemoral venous outflow obstruction. BY WILLIAM
Imaging, it s central role in planning and guiding intervention. Prof. Luis Izquierdo. MD, PhD, FEBVS
 Imaging, it s central role in planning and guiding intervention Prof. Luis Izquierdo. MD, PhD, FEBVS IMPORTANT INFORMATION: These materials are intended to describe common clinical considerations and procedural
Imaging, it s central role in planning and guiding intervention Prof. Luis Izquierdo. MD, PhD, FEBVS IMPORTANT INFORMATION: These materials are intended to describe common clinical considerations and procedural
Straub Endovascular System &
 Straub Endovascular System & S t r a u b E n d o v a s c u l a r To o l s Straub Endovascular System Effective debulking in occluded arteries and veins Effective debulking in many indications Rotarex
Straub Endovascular System & S t r a u b E n d o v a s c u l a r To o l s Straub Endovascular System Effective debulking in occluded arteries and veins Effective debulking in many indications Rotarex
Complex Iliocaval Reconstruction PNEC. Seattle WA. Bill Marston MD Professor, Div of Vascular Surgery University of N.
 Complex Iliocaval Reconstruction 2017 PNEC. Seattle WA Bill Marston MD Professor, Div of Vascular Surgery University of N. Carolina DISCLOSURES William Marston, MD Consultant/Advisory Board: Veniti, Cardinal
Complex Iliocaval Reconstruction 2017 PNEC. Seattle WA Bill Marston MD Professor, Div of Vascular Surgery University of N. Carolina DISCLOSURES William Marston, MD Consultant/Advisory Board: Veniti, Cardinal
Treatment of Chronic DVT with EKOS: Reproducing ACCESS PTS Data in Every Day Clinical Practice
 Treatment of Chronic DVT with EKOS: Reproducing ACCESS PTS Data in Every Day Clinical Practice Mert Dumantepe, MD Acibadem Altunizade Hospital, Istanbul, Turkey Department of Cardiovascular Surgery Disclosure
Treatment of Chronic DVT with EKOS: Reproducing ACCESS PTS Data in Every Day Clinical Practice Mert Dumantepe, MD Acibadem Altunizade Hospital, Istanbul, Turkey Department of Cardiovascular Surgery Disclosure
Venous stenting in Marseille
 Venous stenting in Marseille Olivier HARTUNG, MD, MSc CHU Nord, Marseille, FRANCE Disclosure Speaker name: Olivier HARTUNG I have the following potential conflicts of interest to report: x Consulting :
Venous stenting in Marseille Olivier HARTUNG, MD, MSc CHU Nord, Marseille, FRANCE Disclosure Speaker name: Olivier HARTUNG I have the following potential conflicts of interest to report: x Consulting :
How to best approach chronic venous occlusions?
 How to best approach chronic venous occlusions? Prof. Nils Kucher Director Venous Thromboembolism Reseach Group University Hospital Bern nilskucher.com Disclosure Speaker name: Nils Kucher X X I have the
How to best approach chronic venous occlusions? Prof. Nils Kucher Director Venous Thromboembolism Reseach Group University Hospital Bern nilskucher.com Disclosure Speaker name: Nils Kucher X X I have the
Percutaneous Mechanical Thrombectomy for Acute Iliofemoral DVT with the Aspirex Catheter: The Dijon Experience
 JFICV 2018, Beaune Percutaneous Mechanical Thrombectomy for Acute Iliofemoral DVT with the Aspirex Catheter: The Dijon Experience Prof. Romaric LOFFROY, MD, PhD, FCIRSE Chief, Department of Vascular and
JFICV 2018, Beaune Percutaneous Mechanical Thrombectomy for Acute Iliofemoral DVT with the Aspirex Catheter: The Dijon Experience Prof. Romaric LOFFROY, MD, PhD, FCIRSE Chief, Department of Vascular and
The Conservative and Active Management of Post Thrombotic Syndrome
 The Conservative and Active Management of Post Thrombotic Syndrome Stephen Black Consultant Vascular Surgeon Clinical Lead for Venous and Lymphoedema Surgery Guys and St Thomas Hospital London How important
The Conservative and Active Management of Post Thrombotic Syndrome Stephen Black Consultant Vascular Surgeon Clinical Lead for Venous and Lymphoedema Surgery Guys and St Thomas Hospital London How important
What Really Matters to Patient is QOL: Veniti Virtus Venous Feasibility Trial
 DISCLOSURES Speaker name: Lowell S. Kabnick, MD, FACS... I have the following potential conflicts of interest: Consultant and shareholder, VENITI, Inc. Consultant to BARD What Really Matters to Patient
DISCLOSURES Speaker name: Lowell S. Kabnick, MD, FACS... I have the following potential conflicts of interest: Consultant and shareholder, VENITI, Inc. Consultant to BARD What Really Matters to Patient
Michael K.W. Lichtenberg, MD
 Ranger All-Comer Registry Treatment of femoropopliteal atherosclerotic lesions using the Drug eluting Balloon Ranger: An All Comers Registry Michael K.W. Lichtenberg, MD Klinikum Arnsberg Arnsberg, Germany
Ranger All-Comer Registry Treatment of femoropopliteal atherosclerotic lesions using the Drug eluting Balloon Ranger: An All Comers Registry Michael K.W. Lichtenberg, MD Klinikum Arnsberg Arnsberg, Germany
Not all Leg DVT s are the Same: Which Patients Benefit from Interventional Therapy? Case 1:
 12/16/2015 Not all Leg DVT s are the Same: Which Patients Benefit from Interventional Therapy? Constantino S.Peña, FSIR, FSCCT, FAHA Interventional Radiologist Medical Director, Vascular Imaging Miami
12/16/2015 Not all Leg DVT s are the Same: Which Patients Benefit from Interventional Therapy? Constantino S.Peña, FSIR, FSCCT, FAHA Interventional Radiologist Medical Director, Vascular Imaging Miami
RANGER SFA REGISTRY Interim Analysis. Bernd Gehringhoff, MD On behalf the Ranger SFA Registry Investigators
 RANGER SFA REGISTRY Interim Analysis Bernd Gehringhoff, MD On behalf the Ranger SFA Registry Investigators Conflict of Interest - Disclosure Within the past 12 months, I or my spouse/partner have had a
RANGER SFA REGISTRY Interim Analysis Bernd Gehringhoff, MD On behalf the Ranger SFA Registry Investigators Conflict of Interest - Disclosure Within the past 12 months, I or my spouse/partner have had a
Iliofemoral DVT: Miminizing Post-Thrombotic Syndrome
 Iliofemoral DVT: Miminizing Post-Thrombotic Syndrome Catherine K. Chang, MD FACS Vascular Surgery San Diego Southern California Permanente Medical Group Acute Deep Venous Thrombosis Incidence & Outcomes
Iliofemoral DVT: Miminizing Post-Thrombotic Syndrome Catherine K. Chang, MD FACS Vascular Surgery San Diego Southern California Permanente Medical Group Acute Deep Venous Thrombosis Incidence & Outcomes
A Dedicated Venous Self-expanding Oblique Hybrid Nitinol Stent (Sinus-Obliquus Stent)
") A Dedicated Venous Self-expanding Oblique Hybrid Nitinol Stent (Sinus-Obliquus Stent) Anna Stuck, Rolf P. Engelberger, Nils Kucher Division of Angiology Cantonal Hospital Fribourg & Bern University Hospital
A Dedicated Venous Self-expanding Oblique Hybrid Nitinol Stent (Sinus-Obliquus Stent) Anna Stuck, Rolf P. Engelberger, Nils Kucher Division of Angiology Cantonal Hospital Fribourg & Bern University Hospital
Complete Evaluation of the Chronic Venous Patient: Recognizing deep venous obstruction. Erin H. Murphy, MD Rane Center
 Complete Evaluation of the Chronic Venous Patient: Recognizing deep venous obstruction Erin H. Murphy, MD Rane Center Disclosure Speaker name: Erin H. Murphy... I have the following potential conflicts
Complete Evaluation of the Chronic Venous Patient: Recognizing deep venous obstruction Erin H. Murphy, MD Rane Center Disclosure Speaker name: Erin H. Murphy... I have the following potential conflicts
BC Vascular Day. Contents. November 3, Abdominal Aortic Aneurysm 2 3. Peripheral Arterial Disease 4 6. Deep Venous Thrombosis 7 8
 BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
Venous interventions in DVT
 Venous interventions in DVT Sriram Narayanan Chief of Vascular and Endovascular Surgery, Tan Tock Seng Hospital A/Prof of Surgery, National University of Singapore ANTI-COAGULATION LMWH Warfarin x 6m Acute
Venous interventions in DVT Sriram Narayanan Chief of Vascular and Endovascular Surgery, Tan Tock Seng Hospital A/Prof of Surgery, National University of Singapore ANTI-COAGULATION LMWH Warfarin x 6m Acute
Aggressive endovascular management of ilio-femoral DVT. thrombotic syndrome. is the key in preventing post
 CACVS 2017 Aggressive endovascular management of ilio-femoral DVT is the key in preventing post thrombotic syndrome ALI AMIN MD, FACS,FACC, RVT CHIEF OF ENDOVASCULAR INTERVENTIONS READING HEALTH SYSTEM
CACVS 2017 Aggressive endovascular management of ilio-femoral DVT is the key in preventing post thrombotic syndrome ALI AMIN MD, FACS,FACC, RVT CHIEF OF ENDOVASCULAR INTERVENTIONS READING HEALTH SYSTEM
VERNACULAR Trial & Clinical Experience with the VENOVO Venous Stent
 Stephen Black, MD VERNACULAR Trial & Clinical Experience with the VENOVO Venous Stent 1 Speaker Disclaimers The speakers presentation today is on behalf of Bard Peripheral Vascular, Inc. Any discussion
Stephen Black, MD VERNACULAR Trial & Clinical Experience with the VENOVO Venous Stent 1 Speaker Disclaimers The speakers presentation today is on behalf of Bard Peripheral Vascular, Inc. Any discussion
2017 Florida Vascular Society
 Current Management of Venous Leg Ulcers: How to Identify Patients with Correctable Venous Disease and Interventional Procedures to Heal and Prevent Recurrence 2017 Florida Vascular Society Bill Marston
Current Management of Venous Leg Ulcers: How to Identify Patients with Correctable Venous Disease and Interventional Procedures to Heal and Prevent Recurrence 2017 Florida Vascular Society Bill Marston
Iliofemoral outflow obstruction. - Acute and chronic DVT - Michael K.W. Lichtenberg, MD. Venous Center Arnsberg
 Iliofemoral outflow obstruction - Acute and chronic DVT - Awareness, Diagnostic approach, Treatment strategies Michael K.W. Lichtenberg, MD Venous Center Arnsberg EVIDENCE / GUIDELINES General Antithrombotic
Iliofemoral outflow obstruction - Acute and chronic DVT - Awareness, Diagnostic approach, Treatment strategies Michael K.W. Lichtenberg, MD Venous Center Arnsberg EVIDENCE / GUIDELINES General Antithrombotic
Image-Guided Approach to Treatment of Patients with Nonthrombotic
 Image-Guided Approach to Treatment of Patients with Nonthrombotic May Thurner Syndrome Brian DeRubertis, MD, FACS Associate Professor of Surgery Division of Vascular Surgery UCLA School of Medicine Los
Image-Guided Approach to Treatment of Patients with Nonthrombotic May Thurner Syndrome Brian DeRubertis, MD, FACS Associate Professor of Surgery Division of Vascular Surgery UCLA School of Medicine Los
Technique de recanalisation: mon expérience avec Aspirex
 JFICV 2017, Deauville Thrombose veineuse profonde aiguë en 2017 Technique de recanalisation: mon expérience avec Aspirex Romaric LOFFROY Département de Radiologie Diagnostique et Thérapeutique CHU Hôpital
JFICV 2017, Deauville Thrombose veineuse profonde aiguë en 2017 Technique de recanalisation: mon expérience avec Aspirex Romaric LOFFROY Département de Radiologie Diagnostique et Thérapeutique CHU Hôpital
Endovascular Therapy vs. Open Femoral Endarterectomy Rationale and Design of the Randomized PESTO Trial
 Endovascular Therapy vs. Open Femoral Endarterectomy Rationale and Design of the Randomized PESTO Trial Prof. Thomas Zeller, MD Department Angiology Clinic for Cardiology and Angiology II University Heart-Center
Endovascular Therapy vs. Open Femoral Endarterectomy Rationale and Design of the Randomized PESTO Trial Prof. Thomas Zeller, MD Department Angiology Clinic for Cardiology and Angiology II University Heart-Center
Venogram Versus Intravascular Ultrasound for Diagnosing and Treating Iliofemoral Vein Obstruction (VIDIO)
") Venogram Versus Intravascular Ultrasound for Diagnosing and Treating Iliofemoral Vein Obstruction (VIDIO) Report From a Multicenter, Prospective Study of Iliofemoral Vein Interventions Paul J. Gagne, MD,
Venogram Versus Intravascular Ultrasound for Diagnosing and Treating Iliofemoral Vein Obstruction (VIDIO) Report From a Multicenter, Prospective Study of Iliofemoral Vein Interventions Paul J. Gagne, MD,
Interventional Treatment VTE: Radiologic Approach
 Interventional Treatment VTE: Radiologic Approach Hae Giu Lee, MD Professor, Dept of Radiology Seoul St. Mary s Hospital The Catholic University of Korea Introduction Incidence High incidence: 250,000-1,000,000/year
Interventional Treatment VTE: Radiologic Approach Hae Giu Lee, MD Professor, Dept of Radiology Seoul St. Mary s Hospital The Catholic University of Korea Introduction Incidence High incidence: 250,000-1,000,000/year
THERE IS NO ROLE FOR SURGICAL THERAPY FOR DVT
 THERE IS NO ROLE FOR SURGICAL THERAPY FOR DVT Tara D. Balint, MD FACS Sentara RMH Thursday, June 14, 2018 1 Objectives of treatment for DVT Prevent death from PE Prevent recurrent VTE Prevent post-thrombotic
THERE IS NO ROLE FOR SURGICAL THERAPY FOR DVT Tara D. Balint, MD FACS Sentara RMH Thursday, June 14, 2018 1 Objectives of treatment for DVT Prevent death from PE Prevent recurrent VTE Prevent post-thrombotic
Intervention for Deep Venous Thrombosis and Pulmonary Embolus
 Intervention for Deep Venous Thrombosis and Pulmonary Embolus Michael R. Jaff, DO Paul and Phyllis Fireman Endowed Chair in Vascular Medicine Massachusetts General Hospital Professor of Medicine Harvard
Intervention for Deep Venous Thrombosis and Pulmonary Embolus Michael R. Jaff, DO Paul and Phyllis Fireman Endowed Chair in Vascular Medicine Massachusetts General Hospital Professor of Medicine Harvard
Michael Meuse, M.D. Vascular and Interventional Radiology
 Michael Meuse, M.D. Vascular and Interventional Radiology Iliac Vein Compression Syndrome Left CIV compressed by right CIA Virchow 1851: DVT L>R May and Thurner 1954: venous spurs Cockett and Thomas 1965:
Michael Meuse, M.D. Vascular and Interventional Radiology Iliac Vein Compression Syndrome Left CIV compressed by right CIA Virchow 1851: DVT L>R May and Thurner 1954: venous spurs Cockett and Thomas 1965:
Update on the Ranger clinical trial programme
 Update on the Ranger clinical trial programme Dierk Scheinert, MD Universitätsklinikum Leipzig, Leipzig, Germany on behalf of the RANGER SFA investigators Disclosure Speaker s name: Dierk Scheinert I have
Update on the Ranger clinical trial programme Dierk Scheinert, MD Universitätsklinikum Leipzig, Leipzig, Germany on behalf of the RANGER SFA investigators Disclosure Speaker s name: Dierk Scheinert I have
Starting with deep venous treatment
 Starting with deep venous treatment Carsten Arnoldussen, MD Interventional Radiologist Maastricht University Medical Centre, Maastricht VieCuri Medical Centre, Venlo The Netherlands Background Maastricht
Starting with deep venous treatment Carsten Arnoldussen, MD Interventional Radiologist Maastricht University Medical Centre, Maastricht VieCuri Medical Centre, Venlo The Netherlands Background Maastricht
When Outcomes Matter, Design Matters
 to receive our latest news and key activities. Cordis S.M.A.R.T. Self-Expanding Nitinol Lower Extremity Solutions When Outcomes Matter, Design Matters For superficial femoral artery (SFA) and iliac lesions.
to receive our latest news and key activities. Cordis S.M.A.R.T. Self-Expanding Nitinol Lower Extremity Solutions When Outcomes Matter, Design Matters For superficial femoral artery (SFA) and iliac lesions.
Emerging Tools for Lytic-Free, Single-Session Treatment of Venous Thromboembolic Disease
 FEATURED TECHNOLOGY THE CLOTTRIEVER AND FLOWTRIEVER SYSTEMS Emerging Tools for Lytic-Free, Single-Session Treatment of Venous Thromboembolic Disease The ClotTriever Outcomes (CLOUT) registry principal
FEATURED TECHNOLOGY THE CLOTTRIEVER AND FLOWTRIEVER SYSTEMS Emerging Tools for Lytic-Free, Single-Session Treatment of Venous Thromboembolic Disease The ClotTriever Outcomes (CLOUT) registry principal
IVUS is strongly recommanded before treating a venous femoro-iliac obstruction CONS. F Thony CHU Grenoble
 IVUS is strongly recommanded before treating a venous femoro-iliac obstruction CONS F Thony CHU Grenoble Disclosure Speaker name: Frédéric THONY I do not have any potential conflict of interest Introduction
IVUS is strongly recommanded before treating a venous femoro-iliac obstruction CONS F Thony CHU Grenoble Disclosure Speaker name: Frédéric THONY I do not have any potential conflict of interest Introduction
CHALLENGING ILIAC ACCESSES AND THROMBOSIS PREVENTION
 CHALLENGING ILIAC ACCESSES AND THROMBOSIS PREVENTION ARMANDO MANSILHA MD, PhD, FEBVS UNIVERSITY HOSPITAL - PORTO Disclosure of Interest Speaker name: ARMANDO MANSILHA I have the following potential conflicts
CHALLENGING ILIAC ACCESSES AND THROMBOSIS PREVENTION ARMANDO MANSILHA MD, PhD, FEBVS UNIVERSITY HOSPITAL - PORTO Disclosure of Interest Speaker name: ARMANDO MANSILHA I have the following potential conflicts
Copy Here. The Easy One.. What is the Role of Thrombus Removal in Acute Proximal DVT after ATTRACT? Deep Venous Thrombosis Spectrum
 What is the Role of Thrombus Removal in Acute Proximal DVT after ATTRACT? Mitchell J. Silver DO FACC FSVM RPVI Director, Center for Critical Limb Care Riverside Methodist Hospital Ohio Health Heart and
What is the Role of Thrombus Removal in Acute Proximal DVT after ATTRACT? Mitchell J. Silver DO FACC FSVM RPVI Director, Center for Critical Limb Care Riverside Methodist Hospital Ohio Health Heart and
Re-intervention for occluded iliac vein stents
 Review Article Re-intervention for occluded iliac vein stents Stacey Black 1, Amy Janicek 2, M. Grace Knuttinen 3 1 University of Arizona, Tucson, Arizona, USA; 2 Arizona State Radiology, Tucson, Arizona,
Review Article Re-intervention for occluded iliac vein stents Stacey Black 1, Amy Janicek 2, M. Grace Knuttinen 3 1 University of Arizona, Tucson, Arizona, USA; 2 Arizona State Radiology, Tucson, Arizona,
Selection and work up for the right patients suspected of deep venous disease
 Selection and work up for the right patients suspected of deep venous disease R A G H U K O L L U R I, M S, M D, R V T S Y S T E M M E D I C A L D I R E C T O R V A S C U L A R M E D I C I N E / V A S
Selection and work up for the right patients suspected of deep venous disease R A G H U K O L L U R I, M S, M D, R V T S Y S T E M M E D I C A L D I R E C T O R V A S C U L A R M E D I C I N E / V A S
Canadian Society of Internal Medicine Annual Meeting 2017 Toronto, ON
 Canadian Society of Internal Medicine Annual Meeting 2017 Toronto, ON How to Prevent and Manage the Post-Thrombotic Syndrome? Jean-Philippe Galanaud Clinical Thromboembolism & Division of GIM Sunnybrook,
Canadian Society of Internal Medicine Annual Meeting 2017 Toronto, ON How to Prevent and Manage the Post-Thrombotic Syndrome? Jean-Philippe Galanaud Clinical Thromboembolism & Division of GIM Sunnybrook,
Ovation. Sean Lyden, MD Department Chair, Vascular Surgery Cleveland Clinic
 Ovation Sean Lyden, MD Department Chair, Vascular Surgery Cleveland Clinic Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Ovation Sean Lyden, MD Department Chair, Vascular Surgery Cleveland Clinic Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Complications of endovascular treatment of May-Thurner syndrome George Geroulakos
 Complications of endovascular treatment of May-Thurner syndrome George Geroulakos Professor of Vascular Surgery, National and Kapodistrian University of Athens Director, Department of Vascular Surgery,
Complications of endovascular treatment of May-Thurner syndrome George Geroulakos Professor of Vascular Surgery, National and Kapodistrian University of Athens Director, Department of Vascular Surgery,
Current Best Practices, Trial Experiences, and Device Designs
 ROUNDTABLE DISCUSSION VENOUS Venous Stenting Perspectives: Current Best Practices, Trial Experiences, and Device Designs WITH STEVEN D. ABRAMOWITZ, MD; STEPHEN A. BLACK, MD, FRCS(Ed), FEBVS; MICHAEL D.
ROUNDTABLE DISCUSSION VENOUS Venous Stenting Perspectives: Current Best Practices, Trial Experiences, and Device Designs WITH STEVEN D. ABRAMOWITZ, MD; STEPHEN A. BLACK, MD, FRCS(Ed), FEBVS; MICHAEL D.
Duplex ultrasound is first-line imaging for all
 Our Protocol for Transabdominal Pelvic Vein Duplex Ultrasound A summary of s protocol for pelvic vein duplex ultrasonography, including equipment, patient positioning, ultrasound settings, and technique.
Our Protocol for Transabdominal Pelvic Vein Duplex Ultrasound A summary of s protocol for pelvic vein duplex ultrasonography, including equipment, patient positioning, ultrasound settings, and technique.
IN.PACT AV Access IDE Study Full Baseline Data. Robert Lookstein, MD MHCDL New York, NY On Behalf of the IN.PACT AV ACCESS Investigators
 IN.PACT AV Access IDE Study Full Baseline Data Robert Lookstein, MD MHCDL New York, NY On Behalf of the IN.PACT AV ACCESS Investigators Disclosures Speaker name: Robert Lookstein, MD... I have the following
IN.PACT AV Access IDE Study Full Baseline Data Robert Lookstein, MD MHCDL New York, NY On Behalf of the IN.PACT AV ACCESS Investigators Disclosures Speaker name: Robert Lookstein, MD... I have the following
Acoustic Pulse Thrombolysis Treatment
 Acoustic Pulse Thrombolysis Treatment BTGVascular.com SETTING THE STANDARD FOR VASCULAR THERAPIES Quickly & safely dissolve thrombus with the EKOS System. The Acoustic Pulse Difference Acoustic Pulse Thrombolysis
Acoustic Pulse Thrombolysis Treatment BTGVascular.com SETTING THE STANDARD FOR VASCULAR THERAPIES Quickly & safely dissolve thrombus with the EKOS System. The Acoustic Pulse Difference Acoustic Pulse Thrombolysis
COMPARE-Pilot RCT: 1-year results of a randomised comparison of RANGER DCB vs. IN.PACT DCB in complex SFA lesions. Dierk Scheinert
 COMPARE-Pilot RCT: 1-year results of a randomised comparison of RANGER DCB vs. IN.PACT DCB in complex SFA lesions Dierk Scheinert Department of Angiology University Hospital Leipzig, Germany Disclosure
COMPARE-Pilot RCT: 1-year results of a randomised comparison of RANGER DCB vs. IN.PACT DCB in complex SFA lesions Dierk Scheinert Department of Angiology University Hospital Leipzig, Germany Disclosure
Shockwave Medical Lithoplasty. Thomas Zeller MD Universitäts-Herzzentrum Freiburg & Bad Krozingen, Germany
 Shockwave Medical Lithoplasty Thomas Zeller MD Universitäts-Herzzentrum Freiburg & Bad Krozingen, Germany Disclosure Speaker name: Thomas Zeller, MD I have the following potential conflicts of interest
Shockwave Medical Lithoplasty Thomas Zeller MD Universitäts-Herzzentrum Freiburg & Bad Krozingen, Germany Disclosure Speaker name: Thomas Zeller, MD I have the following potential conflicts of interest
14F OD Ovation Abdominal Stent Graft System
 14F OD Ovation Abdominal Stent Graft System 2 Year Results from the European Study Dierk Scheinert, MD Center for Vascular Medicine Angiology and Vascular Surgery Park Hospital Leipzig, Germany Disclosure
14F OD Ovation Abdominal Stent Graft System 2 Year Results from the European Study Dierk Scheinert, MD Center for Vascular Medicine Angiology and Vascular Surgery Park Hospital Leipzig, Germany Disclosure
Which Stent Is Best for Various Femoropopliteal Anatomy? 2018 Pacific Northwest Endovascular Conference June 15-26, 2018 Seattle, WA
 Which Stent Is Best for Various Femoropopliteal Anatomy? 2018 Pacific Northwest Endovascular Conference June 15-26, 2018 Seattle, WA Brian DeRubertis, MD, FACS Associate Professor of Surgery UCLA Division
Which Stent Is Best for Various Femoropopliteal Anatomy? 2018 Pacific Northwest Endovascular Conference June 15-26, 2018 Seattle, WA Brian DeRubertis, MD, FACS Associate Professor of Surgery UCLA Division
Accurate Vessel Sizing Drives Clinical Results. IVUS In the Periphery
 Accurate Vessel Sizing Drives Clinical Results IVUS In the Periphery Discussion Iida O, et. al. Study Efficacy of Intravascular Ultrasound in Femoropopliteal Stenting for Peripheral Artery Disease With
Accurate Vessel Sizing Drives Clinical Results IVUS In the Periphery Discussion Iida O, et. al. Study Efficacy of Intravascular Ultrasound in Femoropopliteal Stenting for Peripheral Artery Disease With
Iliocaval Confluence Stenting for Chronic Venous Obstructions
 Cardiovasc Intervent Radiol (2015) 38:1198 1204 DOI 10.1007/s00270-015-1068-5 CLINICAL INVESTIGATION VENOUS INTERVENTIONS Iliocaval Confluence Stenting for Chronic Venous Obstructions Rick de Graaf Mark
Cardiovasc Intervent Radiol (2015) 38:1198 1204 DOI 10.1007/s00270-015-1068-5 CLINICAL INVESTIGATION VENOUS INTERVENTIONS Iliocaval Confluence Stenting for Chronic Venous Obstructions Rick de Graaf Mark
Deep Venous Pathology. Eberhard Rabe Department of Dermatology University of Bonn Germany
 Deep Venous Pathology Eberhard Rabe Department of Dermatology University of Bonn Germany Disclosures None for this presentation Consultant: Sigvaris, EUROCOM Speakers bureau: Bayer Vital, Aspen, Boehringer,
Deep Venous Pathology Eberhard Rabe Department of Dermatology University of Bonn Germany Disclosures None for this presentation Consultant: Sigvaris, EUROCOM Speakers bureau: Bayer Vital, Aspen, Boehringer,
Ultrasound-assisted catheter-directed thrombolysis: Does it really work? The BERNUTIFUL trial
 Ultrasound-assisted catheter-directed thrombolysis: Does it really work? The BERNUTIFUL trial Rolf P. Engelberger Division of Angiology CHUV, Lausanne & Inselspital, Bern Switzerland Disclosure Speaker
Ultrasound-assisted catheter-directed thrombolysis: Does it really work? The BERNUTIFUL trial Rolf P. Engelberger Division of Angiology CHUV, Lausanne & Inselspital, Bern Switzerland Disclosure Speaker
Surgical approach for DVT. Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine
 Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach
 Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach Prof. I. Baumgartner Head Clinical and Interventional Angiology About the ACCP guidelines Widely
Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach Prof. I. Baumgartner Head Clinical and Interventional Angiology About the ACCP guidelines Widely
Device Evolution. Atherectomy: Where Do We Stand After 12 Years Since FDA Clearance. Where Do We Stand? 4/18/2015
 Disclosure Statement of Financial Interest Atherectomy: Where Do We Stand After 12 Years Since FDA Clearance Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Disclosure Statement of Financial Interest Atherectomy: Where Do We Stand After 12 Years Since FDA Clearance Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
The Role of Lithotripsy in Solving the Challenges of Vascular Calcium. Thomas Zeller, MD
 The Role of Lithotripsy in Solving the Challenges of Vascular Calcium Thomas Zeller, MD 1 1 Disclosure Speaker name: Thomas Zeller... I have the following potential conflicts of interest to report: X X
The Role of Lithotripsy in Solving the Challenges of Vascular Calcium Thomas Zeller, MD 1 1 Disclosure Speaker name: Thomas Zeller... I have the following potential conflicts of interest to report: X X
Final Results of the Feasibility Study for the Drug-coated Chocolate Touch PTA balloon. (The ENDURE Trial)
") Final results of the feasibility study for the drug-coated Chocolate Touch PTA balloon of of femoropopliteal Femoropopliteal lesions lesions: (The ENDURE Trial) Final Results of the Feasibility Study for
Final results of the feasibility study for the drug-coated Chocolate Touch PTA balloon of of femoropopliteal Femoropopliteal lesions lesions: (The ENDURE Trial) Final Results of the Feasibility Study for
Chronic Venous Disease: A Complex Disorder. A N Nicolaides
 Chronic Venous Disease: A Complex Disorder A N Nicolaides Emeritus Professor of Vascular Surgery, Imperial College, London. Hon. Professor of Surgery, University of Nicosia Medical School, Cyprus Disclosures
Chronic Venous Disease: A Complex Disorder A N Nicolaides Emeritus Professor of Vascular Surgery, Imperial College, London. Hon. Professor of Surgery, University of Nicosia Medical School, Cyprus Disclosures
Long Lesions: Primary stenting or DCB first? John Laird MD Adventist Heart and Vascular Institute, St. Helena, CA
 Long Lesions: Primary stenting or DCB first? John Laird MD Adventist Heart and Vascular Institute, St. Helena, CA Disclosures John R. Laird Within the past 12 months, I or my spouse/partner have had a
Long Lesions: Primary stenting or DCB first? John Laird MD Adventist Heart and Vascular Institute, St. Helena, CA Disclosures John R. Laird Within the past 12 months, I or my spouse/partner have had a
Patency and Clinical Outcomes of a Dedicated, Self-Expanding, Hybrid Oblique Stent Used in the Treatment of Common Iliac Vein Compression
 676803JETXXX10.1177/1526602816676803Journal of Endovascular TherapyStuck et al research-article2016 Clinical Investigation Patency and Clinical Outcomes of a Dedicated, Self-Expanding, Hybrid Oblique Stent
676803JETXXX10.1177/1526602816676803Journal of Endovascular TherapyStuck et al research-article2016 Clinical Investigation Patency and Clinical Outcomes of a Dedicated, Self-Expanding, Hybrid Oblique Stent
Clinical use and safety of the Lutonix DCB for the treatment of BTK: interim data from a prospective registry
 Clinical use and safety of the Lutonix DCB for the treatment of BTK: interim data from a prospective registry Alexander Zimmermann Department of Vascular and Endovascular Surgery Klinikum rechts der Isar
Clinical use and safety of the Lutonix DCB for the treatment of BTK: interim data from a prospective registry Alexander Zimmermann Department of Vascular and Endovascular Surgery Klinikum rechts der Isar
Christian Wissgott MD, PhD Assistant Director, Radiology Westküstenkliniken Heide
 2-Year Results Of The Tack Optimized Balloon Angioplasty (TOBA) Trial For Fem- Pop Lesions Demonstrates Safety and Efficacy Of The Tack Endovascular System In Repairing Focal Post-PTA Dissections Christian
2-Year Results Of The Tack Optimized Balloon Angioplasty (TOBA) Trial For Fem- Pop Lesions Demonstrates Safety and Efficacy Of The Tack Endovascular System In Repairing Focal Post-PTA Dissections Christian
Evidence for endovascular therapy of iliofemoral DVT: CAVENT, ATTRACT, CAVA and more to come
 Evidence for endovascular therapy of iliofemoral DVT: CAVENT, ATTRACT, CAVA and more to come Stephen Black Consultant Vascular Surgeon Reader in Venous Surgery Or rephrased To lyse or not to lyse: that
Evidence for endovascular therapy of iliofemoral DVT: CAVENT, ATTRACT, CAVA and more to come Stephen Black Consultant Vascular Surgeon Reader in Venous Surgery Or rephrased To lyse or not to lyse: that
PEARL Registry Update Overview Venous Arterial AV Access
 PEARL Registry Update Overview Venous Arterial AV Access PEARL Registry Overview (as of 10 Sep12*) Overview Venous Arterial AV Access HOME Topic Data Support Comments Study Design Prospective, non-randomized,
PEARL Registry Update Overview Venous Arterial AV Access PEARL Registry Overview (as of 10 Sep12*) Overview Venous Arterial AV Access HOME Topic Data Support Comments Study Design Prospective, non-randomized,
Ileo Femoral DVT Review and Update
 Ileo Femoral DVT Review and Update Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Deep Vein Thrombosis Venous thromboembolism is a major national health problem,
Ileo Femoral DVT Review and Update Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Deep Vein Thrombosis Venous thromboembolism is a major national health problem,
Koen Keirse, MD RZ Tienen, Belgium
 Clinical Benefits of the Vanguard IEP Peripheral Balloon Angioplasty System with Integrated Embolic Protection from the ENTRAP Study Koen Keirse, MD RZ Tienen, Belgium Disclosure Speaker name: Koen Keirse...
Clinical Benefits of the Vanguard IEP Peripheral Balloon Angioplasty System with Integrated Embolic Protection from the ENTRAP Study Koen Keirse, MD RZ Tienen, Belgium Disclosure Speaker name: Koen Keirse...
What is the optimal time window for treating deep venous thrombosis? Acute vs subacute vs chronic
 What is the optimal time window for treating deep venous thrombosis? Acute vs subacute vs chronic Peter A. Schneider, MD Chief of Vascular Therapy Kaiser Foundation Hospital Honolulu, Hawaii Disclosure
What is the optimal time window for treating deep venous thrombosis? Acute vs subacute vs chronic Peter A. Schneider, MD Chief of Vascular Therapy Kaiser Foundation Hospital Honolulu, Hawaii Disclosure
Dierk Scheinert, MD. Department of Angiology University Hospital Leipzig, Germany
 The RANGER clinical trial programme: 12-month results from the RANGER RCT and first look at the COMARE I study of RANGER vs. IN.PACT for femoropopliteal lesions Dierk Scheinert, MD Department of Angiology
The RANGER clinical trial programme: 12-month results from the RANGER RCT and first look at the COMARE I study of RANGER vs. IN.PACT for femoropopliteal lesions Dierk Scheinert, MD Department of Angiology
Post-thrombotic syndrome (PTS), often the
, often the") Revascularization of Chronic Venous Occlusion in the Setting of Post-Thrombotic Syndrome Jon George, MD; Deepakraj Gajanana; Sean Janzer; Vincent Figueredo; Dennis Morris From the Einstein Heart and Vascular
Revascularization of Chronic Venous Occlusion in the Setting of Post-Thrombotic Syndrome Jon George, MD; Deepakraj Gajanana; Sean Janzer; Vincent Figueredo; Dennis Morris From the Einstein Heart and Vascular
Bilateral stenting at the iliocaval confluence
 From the American Venous Forum Bilateral stenting at the iliocaval confluence Peter Neglén, MD, PhD, a Rikki Darcey, BS, a Jake Olivier, PhD, b and Seshadri Raju, MD, a Flowood, Miss; and Sydney, New South
From the American Venous Forum Bilateral stenting at the iliocaval confluence Peter Neglén, MD, PhD, a Rikki Darcey, BS, a Jake Olivier, PhD, b and Seshadri Raju, MD, a Flowood, Miss; and Sydney, New South
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of Interventional procedure overview of ultrasound-enhanced, catheterdirected thrombolysis
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of Interventional procedure overview of ultrasound-enhanced, catheterdirected thrombolysis
Final Results of the Feasibility Study for the Drug-coated Chocolate Touch PTA balloon. (The ENDURE Trial)
") Final results of the feasibility study for the drug-coated Chocolate Touch PTA balloon of of femoropopliteal Femoropopliteal lesions lesions: (The ENDURE Trial) Final Results of the Feasibility Study for
Final results of the feasibility study for the drug-coated Chocolate Touch PTA balloon of of femoropopliteal Femoropopliteal lesions lesions: (The ENDURE Trial) Final Results of the Feasibility Study for
Chronic Swelling, Pain, and Ulceration in the Left Lower Extremity
 WHAT WOULD YOU DO? Chronic Swelling, Pain, and Ulceration in the Left Lower Extremity MODERATOR: BROOKE SPENCER, MD, FSIR PANEL: LAWRENCE RUSTY HOFMANN, MD; MARK J. GARCIA, MD, FSIR, FACR; AND BRENT T.
WHAT WOULD YOU DO? Chronic Swelling, Pain, and Ulceration in the Left Lower Extremity MODERATOR: BROOKE SPENCER, MD, FSIR PANEL: LAWRENCE RUSTY HOFMANN, MD; MARK J. GARCIA, MD, FSIR, FACR; AND BRENT T.