A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
|
|
|
- Linda Boone
- 5 years ago
- Views:
Transcription



1 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
2 OBJECTIVES Discuss current trends and changing concepts in our understanding of atypical melanocytic proliferations. Suggest a practical approach to the management of atypical melanocytic lesions including Spitzoid melanocytic lesions and dysplastic nevi.
3 TRADITIONAL / SYMPLISTIC VIEW BENIGN MELANOMA


4 BENIGN NEVUS
5 MELANOMA

6 BENIGN OR MALIGNANT?
7 PROBLEMS WITH TRADITIONAL VIEWPOINT Unlike many other malignant neoplasms, the diagnosis of malignant melanoma is based on a constellation of many different features (any of which by themselves may be seen in benign lesions, some of which may not be seen in a given case). Even though indeterminate lesions do exist, because of medicolegal pressure many atypical cases are placed in the malignant category and are therefore overdiagnosed.
8 Implications of Overdiagnosis Cosmetic disfigurement Psychological implications Negative impact on insurance
9 Traditional view Regional lymph node metastasis is proof of malignancy! Problem: emerging data suggests that some atypical lesions (i.e atypical Spitz tumors in children) may show regional lymph node involvement without further progression.



10 BENIGN ATYPICAL MALIGNANT
11 BENIGN MELANOMA TRADITIONAL/ SYMPLISTIC VIEW BENIGN MELANOMA CONTEMPORARY/ PRACTICAL VIEW ATYPICAL/INTERMEDIATE
12 BENIGN No further treatment is necessary (given biopsy is representative) Increasing Atypia Or Uncertainty Excise if residual pigmentation remains Complete yet conservative re-excision with free microscopic margins MELANOMA In situ = 5mm Invasive = 1cm or greater +/- sentinel nodes *Note: Management should take into consideration other clinical risk factors (i.e family or personal history of melanoma, etc.)
13 MELANOCYTIC LESION BENIGN Clinical/ +/- ancillary studies/ expert consultation ATYPICAL MELANOMA Clinical/ +/- ancillarystudies/ expert consultation Morphologic simulator (i.e nevi of special site) No PROBABLY BENIGN WITH FEW ATYPICAL FEATURES (i.e low grade dysplastic nevi,?spitz nevi INDETERMINATE (i.e Atypical Spitz Nevi) BORDERLINE (i.e severely dysplastic Nevi)
14 Approach to Atypical Melanocytic Lesions: General Principles Diagnostic uncertainty should be expressed in the report and/or directly discussed with treating clinician. Treatment may be tailored to the differential diagnosis. If melanoma cannot be confidently ruled out (i.e borderline lesion), consider treating as melanoma of similar thickness (consider rendering a descriptive diagnosis, but report melanoma prognostic factors, i.e Breslow depth, mitotic activity, ulceration)
15 Practical Approach to Spitzoid Tumors

16 SPITZ NEVUS Melanocytic lesion with characteristic epithelioid morphology, First described by Sophie Spitz in 1948 as juvenile melanoma because of its propensity to occur in childhood, morphologically mimic melanoma but exhibit relatively indolent behaviour. 12 of 13 patients diagnosed as melanoma were alive following long term follow-up

17 SOPHIE SPITZ Differentiation histologically between the juvenile and adult melanomas could not be made with certainty in most cases.

18 There is no single feature that distinguishes a Spitz nevus from a melanoma


19 CYTOLOGIC ATYPIA Spitz Nevus Melanoma The individual cell that defines a Spitz nevus is by definition atypical

20 UPWARD PAGETOID SCATTER MELANOMA SPITZ NEVUS
21 MITOTIC ACTIVITY SPITZ NEVUS MELANOMA
22 SPITZOID MELANOCYTIC LESIONS SPITZ NEVUS/ TUMOR ATYPICAL SPITZ TUMOR SPITZOID MELANOMA
23 SPITZ NEVUS: Clinical features Great majority of lesions occur in childhood or in young adults Recent onset and rapid growth Usually less than 1 cm Pink-tan to reddish nodule Clinically symmetric with even borders
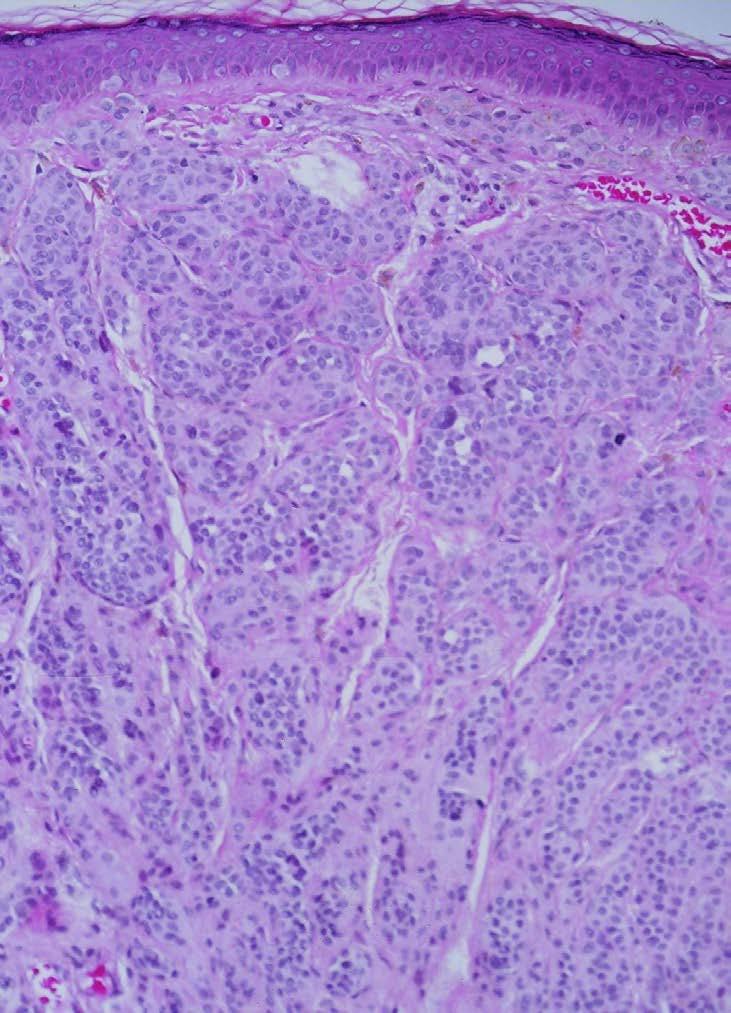
24 SPITZ NEVUS: Histology
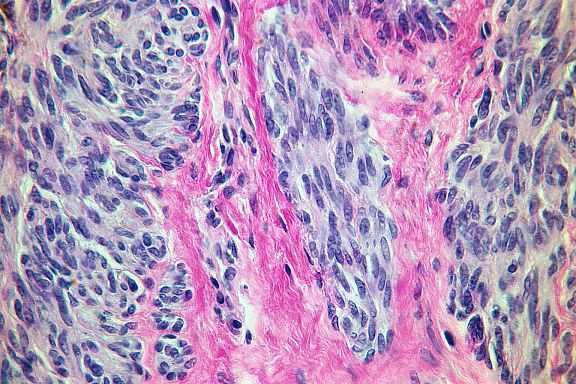
25


26 SPITZ NEVUS
27 Rationale for Complete Excision of All Spitzoid Tumors Morphologic overlap with melanoma Recurrence of Spitz nevi may demonstrate features which may be very difficult to differentiate from melanoma Very rarely Spitz nevi with classic morphologic features have been known to metastasize.
28 SPITZ NEVUS CYTOLOGY AND ARCHITECTURE + APPROPRIATE CLINICAL SETTING SPITZ NEVUS + LESION COMPLETELY EXCISED
29 ATYPICAL SPITZ TUMOR Subset of Spitzoid neoplasms with clinically and pathologically disturbing features in which a melanoma cannot be excluded with absolute certainty. Lesions are more likely to behave more indolently, particularly in childhood, although regional lymph node involvement can occur. The significance of nodal deposits is unclear and does not necessarily indicate aggressive behavior (especially in children).
30 ATYPICAL SPITZOID TUMORS (cont.) Features with significant risk of nodal metastasis (esp. in children): Age greater than 10 years old Lesional diameter greater than 1 cm Ulceration Involvement of subcutaneous fat Mitotic activity of at least 6/mm 2

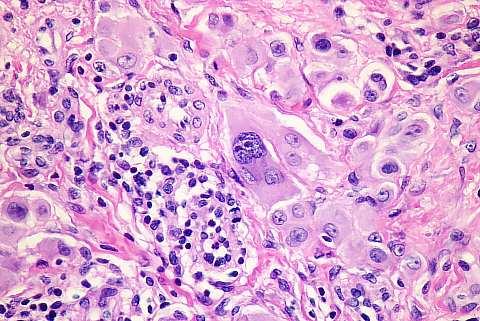
31 ATYPICAL SPITZ TUMOR: Histology
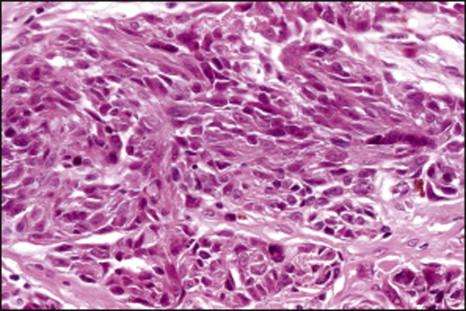
32
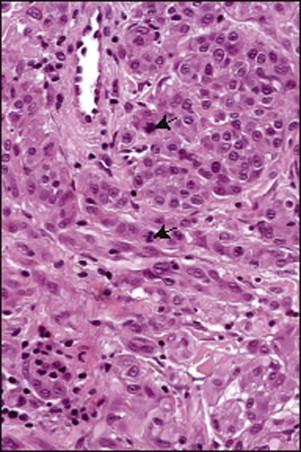
33
34 SPITZOID NEOPLASMS BENIGN INDETERMINATE MALIGNANT SPITZ NEVUS/TUMOR ATYPICAL SPITZ TUMOR SPITZOID MELANOMA TX: Excise TX: Excision +/- consider treating as melanoma Generally without systemic therapy TX: Wide excision +/- Sentinel node biopsy +/- Systemic therapy
35 Spitzoid melanomas are rare under the age of 20. The clinical diagnosis of a benign lesion in a child should be overruled only with very strong histologic evidence to the contrary. After age 50, a lesion with features resembling a Spitz nevus is more likely a melanoma than a nevus. In an older adult, a junctional Spitzoid tumor is most likely a melanoma. Beware of diagnosis of Spitz nevus on severely sun damaged skin (it is probably a melanoma).
36 How To Stay Out Of Court Spitz nevus is a high risk/low frequency diagnosis (like soft tissue or bone tumors. If pathologist does not see Spitz nevi on a regular basis and the patient is more than 20 years old, strongly consider sending to an expert. If Spitz nevi are seen on a regular basis but patient is more than 20 years old (unless typical diagnostic criteria are all present), strongly consider sending case to an expert. All Spitz nevi should be completely excised (although exceedingly rare, cases of classical Spitz nevi have been known to metastasize) Even experts disagree on Spitz tumors
37 CASE PRESENTATION
38
 MALIGNANT MELANOMA d) PIGMENTED SUPERFICIAL")
39 a) JUNCTIONAL MELANOCYTIC NEVUS b) MILDLY DYSPLASTIC JMN c) MALIGNANT MELANOMA d) PIGMENTED SUPERFICIAL BCC
40
41 a) Re-excise b) No further treatment necessary c) Additional clinical information necessary
42 Additional clinical information reveals that the biopsy was taken from a significantly larger clinical lesion. Re-excision recommended by pathologist ( reexcision should be considered, as clinically indicated, particularly if residual pigmentation remains ).
43
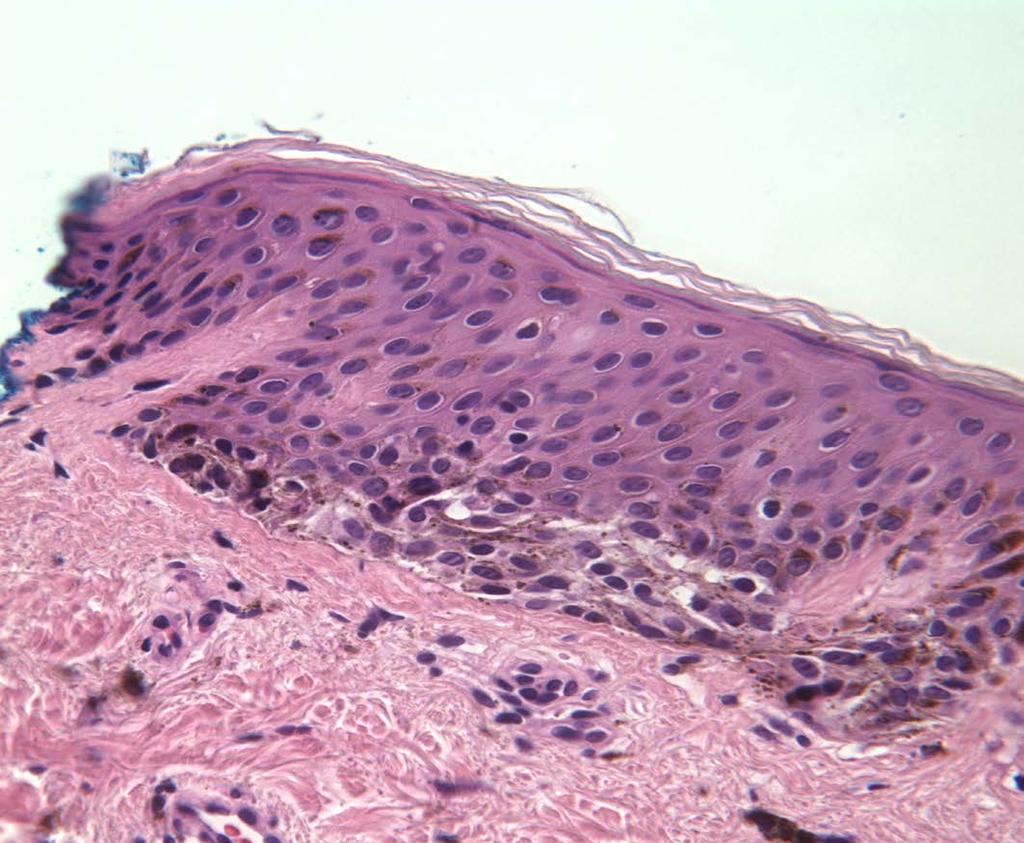
44 FINAL DIAGNOSIS Initial biopsy: Mildly dysplastic junctional melanocytic nevus, involving biopsy margins. Re-excision specimen: Malignant melanoma in-situ, superficial spreading type, arising in the background of dysplastic nevus..
45 SKIN MALIGNANT AREA BENIGN OR DYSPLASTIC AREA
46 Practical Approach to Dysplastic Nevi

47 Considerations prior to treatment Diagnostic pitfall (morphologic overlap with malignant melanoma) Association of dysplastic nevi and melanoma in the same lesion. dysplastic nevus melanoma Interobservor variability in diagnosis
48 Significance of Dysplastic Nevi Morphologic overlap with melanoma Marker of individuals at increased risk of developing melanoma Potential actual precursor of melanoma
49 Grading of Dysplastic Nevi BENIGN NEVUS DYSPLASTIC NEVUS MILD MODERATE SEVERE MELANOMA
50 Rationale For Grading of Dysplastic Nevi Separate slightly atypical but essentially benign nevi from those that: 1) might be confused with melanoma 2) possibly more likely to progress to melanoma 3) may be associated with a higher risk of melanoma
51 Practical Rationale for Grading of Dysplastic Nevi Conveys to the dermatologist Some information about the pathologist s concern about the lesion. The possible need for obtaining a second opinion. The decision to perform a complete excision or not (and possible extent of excision).
52 Problems With Grading of Dysplastic Nevi Not highly reproducible from one pathologist to another and therefore highly controversial. Some pathologists and dermatologists use the term dysplastic and atypical nevi interchangeably.
53 BENIGN NEVUS DYSPLASTIC NEVUS MILD MODERATE SEVERE MELANOMA Controversial: Clinicopathologic correlation Conservative re-excision Excise with at least 5mm margins
54 Lessons Learned from Medicolegal Cases. The diagnosis pertains only to the tissue submitted and assumes that the biopsy is representative. Claims involving dysplastic or atypical nevi appear to result in part from miscommunication between pathologist and dermatologist/clinician and most involve partial biopsies. Pathologist may use dysplastic or atypical nevus in a generic sense (i.e cytologically disturbing cells are present in lesion but lack diagnostic criteria for melanoma) and requests reexcision but the dermatologist may be reluctant to do so since to them these terms have a more specific meaning and connote a clinical syndrome or benign clinical entity.
55 NOTE: Optimal width of re-excision for atypical melanocytic lesions/indeterminate lesions are controversial, not based on hard data and are based largely on standard of care practices.
56 TAKE HOME MESSAGE! If there is disparity between the clinical and pathologic diagnosis, ask for a second read. Know your pathologist and his/her diagnostic tendencies in signing out melanocytic lesions.
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Vernon K. Sondak. Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida
 Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
Dermatopathology. Dr. Rafael Botella Estrada. Hospital La Fe de Valencia
 Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Conflict of Interest 9/2/2014. Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma
 Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is:
 Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
There is NO single Melanoma Stain. > 6000 Mutations in Melanoma. What else can be done to discriminate atypical nevi from melanoma?
 Las Vegas Fall Clinical 2016: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of
Las Vegas Fall Clinical 2016: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of
The Enigmatic Spitz Lesion
 The Enigmatic Spitz Lesion The Dawn of Spitz S Spitz Sophie Spitz Melanomas of Childhood ; Am J Pathol 1948 1910-1956 13 children (18 mo - 12 yrs) 12/13 had a benign clinical course Sophie Spitz Born 1910
The Enigmatic Spitz Lesion The Dawn of Spitz S Spitz Sophie Spitz Melanomas of Childhood ; Am J Pathol 1948 1910-1956 13 children (18 mo - 12 yrs) 12/13 had a benign clinical course Sophie Spitz Born 1910
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy
 Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology,
Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology,
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Clinical characteristics
 Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Associate Clinical Professor of Dermatology MUSC
 Re-excision of Moderately Dysplastic Nevi: Should we or shouldn t we? John C. Maize, Jr, M.D. Dermatologist and Dermatopathologist Trident Dermatology, Charleston SC Associate Clinical Professor of Dermatology
Re-excision of Moderately Dysplastic Nevi: Should we or shouldn t we? John C. Maize, Jr, M.D. Dermatologist and Dermatopathologist Trident Dermatology, Charleston SC Associate Clinical Professor of Dermatology
Pathology of Sarcoma ELEANOR CHEN, MD, PHD, ASSISTANT PROFESSOR DEPARTMENT OF PATHOLOGY UNIVERSITY OF WASHINGTON
 Pathology of Sarcoma ELEANOR CHEN, MD, PHD, ASSISTANT PROFESSOR DEPARTMENT OF PATHOLOGY UNIVERSITY OF WASHINGTON Presentation outline Background and epidemiology of sarcomas Sarcoma classification Sarcoma
Pathology of Sarcoma ELEANOR CHEN, MD, PHD, ASSISTANT PROFESSOR DEPARTMENT OF PATHOLOGY UNIVERSITY OF WASHINGTON Presentation outline Background and epidemiology of sarcomas Sarcoma classification Sarcoma
Management of Atypical Pigmented Lesions
 Management of Atypical Pigmented Lesions Jennifer A. Stein MD, PhD Associate Director, Pigmented Lesion Section Ronald O. Perelman Department of Dermatology NYU Langone Medical Center July 29, 2017 1-4
Management of Atypical Pigmented Lesions Jennifer A. Stein MD, PhD Associate Director, Pigmented Lesion Section Ronald O. Perelman Department of Dermatology NYU Langone Medical Center July 29, 2017 1-4
Management of pediatric melanocytic lesions
 Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
Primary Cutaneous Melanoma Pathology Reporting Proforma DD MM YYYY. *Tumour site. *Specimen laterality. *Specimen type
 Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology
 Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Malignant tumors of melanocytes: Part 1. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Melanoma Update: 8th Edition of AJCC Staging System
 Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018
 Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
Michael T. Tetzlaff MD, PhD
 Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department of Translational and
Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department of Translational and
Glenn D. Goldman, MD. University of Vermont Medical Center. University of Vermont College of Medicine
 Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
6/22/2015. Original Paradigm. Correlating Histology and Molecular Findings in Melanocytic Neoplasms
 6 Correlating Histology and Molecular Findings in Melanocytic Neoplasms Pedram Gerami MD, Associate Professor of Dermatology and Pediatrics at Northwestern University Disclosures: I have been a consultant
6 Correlating Histology and Molecular Findings in Melanocytic Neoplasms Pedram Gerami MD, Associate Professor of Dermatology and Pediatrics at Northwestern University Disclosures: I have been a consultant
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY
 IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors
 Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department
Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment. Justin Rivard MD, MSc, FRCSC September 21, 2018
 You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
WHAT DOES THE PATHOLOGY REPORT MEAN?
 Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Regression 2/3/18. Histologically regression is characterized: melanosis fibrosis combination of both. Distribution: partial or focal!
 Regression Margaret Oliviero MSN, ARNP Harold S. Rabinovitz MD Histologically regression is characterized: melanosis fibrosis combination of both Distribution: partial or focal! Dermatoscopic terminology
Regression Margaret Oliviero MSN, ARNP Harold S. Rabinovitz MD Histologically regression is characterized: melanosis fibrosis combination of both Distribution: partial or focal! Dermatoscopic terminology
Ways to get into trouble, ideas on avoiding trouble, and diagnostic approaches to keep trouble at bay
 Pitfalls in the diagnosis of melanocytic tumors Timothy McCalmont, MD University of California, San Francisco Ways to get into trouble, ideas on avoiding trouble, and diagnostic approaches to keep trouble
Pitfalls in the diagnosis of melanocytic tumors Timothy McCalmont, MD University of California, San Francisco Ways to get into trouble, ideas on avoiding trouble, and diagnostic approaches to keep trouble
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 12, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Melanoma. Consultation on draft guideline - stakeholder comments. Comments to be submitted before 5pm on Friday 13 March 2015
 Please note: Please fill in both the stakeholder organisation and name of commentator fields. We cannot accept forms with attachments such as research articles, letters or leaflets. Stakeholder organisation(s)
Please note: Please fill in both the stakeholder organisation and name of commentator fields. We cannot accept forms with attachments such as research articles, letters or leaflets. Stakeholder organisation(s)
Michael T. Tetzlaff MD, PhD
 American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
Malignant tumors of melanocytes : Part 3. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
The Pathology of Neoplasia Part II
 The Pathology of Neoplasia Part II February 2018 PAUL BOGNER, MD A S S O C I A T E P R O F E S S O R O F O N C O L O G Y P A T H O L O G Y A N D D E R M A T O L O G Y Clinical goals of cancer pathology
The Pathology of Neoplasia Part II February 2018 PAUL BOGNER, MD A S S O C I A T E P R O F E S S O R O F O N C O L O G Y P A T H O L O G Y A N D D E R M A T O L O G Y Clinical goals of cancer pathology
Glenn D. Goldman, MD. Fletcher Allen Health Care. University of Vermont College of Medicine
 Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Melanocytic proliferations in sundamaged
 Atypical Spitzoid Tumor: What Does It Mean And How Should It Be Managed? Melanocytic proliferations in sundamaged skin Jane L. Messina, Jane L. Messina MD International Melanoma Pathology Working Group
Atypical Spitzoid Tumor: What Does It Mean And How Should It Be Managed? Melanocytic proliferations in sundamaged skin Jane L. Messina, Jane L. Messina MD International Melanoma Pathology Working Group
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma. Michael T. Tetzlaff MD, PhD
 Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is:
 Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is: A. Desmoplastic Spitz naevus B. Atypical Spitz Tumour C. Spitzoid melanoma D. Deep penetrating naevus E. Spitz naevus Case 26: M
Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is: A. Desmoplastic Spitz naevus B. Atypical Spitz Tumour C. Spitzoid melanoma D. Deep penetrating naevus E. Spitz naevus Case 26: M
Springer Healthcare. Staging and Diagnosing Cutaneous Melanoma. Concise Reference. Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone
 Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Melanoma Underwriting Presented at 2018 AHOU Conference. Hank George FALU
 Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Impact of Prognostic Factors
 Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Case study 1. Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research
 NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
An Overview of Melanoma. Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center
 An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG
 Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Multispectral Digital Skin Lesion Analysis. Summary
 Subject: Multispectral Digital Skin Lesion Analysis Page: 1 of 8 Last Review Status/Date: March 2016 Multispectral Digital Skin Lesion Analysis Summary There is interest in noninvasive devices that will
Subject: Multispectral Digital Skin Lesion Analysis Page: 1 of 8 Last Review Status/Date: March 2016 Multispectral Digital Skin Lesion Analysis Summary There is interest in noninvasive devices that will
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012
 Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies. Agenda
 Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Melanoma: The Basics. What is a melanocyte?
 Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
Epithelial Cancer- NMSC & Melanoma
 Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 13, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Histotechnological problems in dermatopathology and their possible consequences
 Histotechnological problems in dermatopathology and their possible consequences Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology University of Washington, Seattle,
Histotechnological problems in dermatopathology and their possible consequences Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology University of Washington, Seattle,
Melanoma. Kaushik Mukherjee MD A. Scott Pearson MD
 Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Mole mapping and monitoring. Dr Stephen Hayes. Associate Specialist in Dermatology, University Hospital Southampton
 Mole mapping and monitoring Dr Stephen Hayes Associate Specialist in Dermatology, University Hospital Southampton Outline of presentation The melanoma epidemic Benefits of early detection Risks of the
Mole mapping and monitoring Dr Stephen Hayes Associate Specialist in Dermatology, University Hospital Southampton Outline of presentation The melanoma epidemic Benefits of early detection Risks of the
Case Report Micromelanomas: A Review of Melanomas 2mmand a Case Report
 Case Reports in Oncological Medicine, Article ID 206260, 4 pages http://dx.doi.org/10.1155/2014/206260 Case Report Micromelanomas: A Review of Melanomas 2mmand a Case Report Sharad P. Paul 1,2,3 1 Skin
Case Reports in Oncological Medicine, Article ID 206260, 4 pages http://dx.doi.org/10.1155/2014/206260 Case Report Micromelanomas: A Review of Melanomas 2mmand a Case Report Sharad P. Paul 1,2,3 1 Skin
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
PHILIP E. LEBOIT. Histological Diagnosis of Nevi and Melanoma
 GUIDO MASSI PHILIP E. LEBOIT Histological Diagnosis of Nevi and Melanoma GUIDO MASSI PHILIP E. LEBOIT Histological Diagnosis of Nevi and Melanoma With Contributions by PAOLA PASQUINI and FRANCESCO FEDERICO,
GUIDO MASSI PHILIP E. LEBOIT Histological Diagnosis of Nevi and Melanoma GUIDO MASSI PHILIP E. LEBOIT Histological Diagnosis of Nevi and Melanoma With Contributions by PAOLA PASQUINI and FRANCESCO FEDERICO,
BAP-oma & BEYOND MICHAEL A NOWAK, MD
 BAP-oma & BEYOND MICHAEL A NOWAK, MD CONFLICTS No conflicts with the content of this lecture BAP-oma Wiesner 2011: Families with multiple tan dome-shaped papules of head, neck, trunk, and extremities.
BAP-oma & BEYOND MICHAEL A NOWAK, MD CONFLICTS No conflicts with the content of this lecture BAP-oma Wiesner 2011: Families with multiple tan dome-shaped papules of head, neck, trunk, and extremities.
Clinicopathologic Self- Assessment S003 AAD 2017
 Clinicopathologic Self- Assessment S003 AAD 2017 Clay J. Cockerell, M.D. Director, Cockerell Dermatopathology Director, Division of Dermatopathology UT Southwestern Medical Center July 2017 No relevant
Clinicopathologic Self- Assessment S003 AAD 2017 Clay J. Cockerell, M.D. Director, Cockerell Dermatopathology Director, Division of Dermatopathology UT Southwestern Medical Center July 2017 No relevant
04/09/2018. Squamous Cell Neoplasia and Precursor Lesions. Agenda. Squamous Dysplasia. Squamo-proliferative lesions. Architectural features
 Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Among the benign intraepithelial melanocytic proliferations, Inflamed Conjunctival Nevi. Histopathological Criteria. Resident Short Reviews
 Resident Short Reviews Inflamed conjunctival nevi (ICN) may suggest malignancy because of their rapid growth and atypical histology. The objective of this study was to characterize the diagnostic features
Resident Short Reviews Inflamed conjunctival nevi (ICN) may suggest malignancy because of their rapid growth and atypical histology. The objective of this study was to characterize the diagnostic features
Histopathology of Melanoma
 THE YALE JOURNAL OF BIOLOGY AND MEDICINE 48, 409-416 (1975) Histopathology of Melanoma G. J. WALKER SMITH Department ofpathology, Yale University School ofmedicine, 333 Cedar Street, New Haven, Connecticut
THE YALE JOURNAL OF BIOLOGY AND MEDICINE 48, 409-416 (1975) Histopathology of Melanoma G. J. WALKER SMITH Department ofpathology, Yale University School ofmedicine, 333 Cedar Street, New Haven, Connecticut
Page 1 of 3. We suggest the following changes:
 Page 1 of 3 Loren E. Clarke, M.D. Myriad Genetic Laboratories, Inc. 320 Wakara Way, Salt Lake City, UT 84108 Phone: 801.883.3470 Email: lclarke@myriad.com Date of Request: June 2017 NCCN Guidelines Panel:
Page 1 of 3 Loren E. Clarke, M.D. Myriad Genetic Laboratories, Inc. 320 Wakara Way, Salt Lake City, UT 84108 Phone: 801.883.3470 Email: lclarke@myriad.com Date of Request: June 2017 NCCN Guidelines Panel:
Lentigo Maligna: Striking a Balance With the Risk-Benefit Ratio. Glen M. Bowen, MD Huntsman Cancer Institute University of Utah
 Lentigo Maligna: Striking a Balance With the Risk-Benefit Ratio Glen M. Bowen, MD Huntsman Cancer Institute University of Utah I. Objectives: a. Review the terminology of LM/LMM b. Understand the relative
Lentigo Maligna: Striking a Balance With the Risk-Benefit Ratio Glen M. Bowen, MD Huntsman Cancer Institute University of Utah I. Objectives: a. Review the terminology of LM/LMM b. Understand the relative
Skin Cancer. 5 Warning Signs. American Osteopathic College of Occupational and Preventive Medicine OMED 2012, San Diego, Monday, October 8, 2012 C-1
 Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor
 Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
21/07/2017. The «gray zone» of diagnosis is visible. Nevus Atypical nevus Melanoma. Melanoma ex-blue nevus
 Update on the Clinico- Pathological and Molecular Diagnosis of Melanocytic Lesions None to declare Conflicts of interest Belfast pathology Arnaud de la Fouchardière MD, PhD Lyon, France What is new? Today
Update on the Clinico- Pathological and Molecular Diagnosis of Melanocytic Lesions None to declare Conflicts of interest Belfast pathology Arnaud de la Fouchardière MD, PhD Lyon, France What is new? Today
K Blessing, J J H Grant, D S A Sanders, M M Kennedy, A Husain, P Coburn
 J Clin Pathol 2000;53:591 595 591 Papers Pathology, Aberdeen University, Foresterhill, Aberdeen AB25 2ZD, K Blessing Pathology, Birmingham University, Birmingham B15 2TT, D S A Sanders Pathology, Heartlands
J Clin Pathol 2000;53:591 595 591 Papers Pathology, Aberdeen University, Foresterhill, Aberdeen AB25 2ZD, K Blessing Pathology, Birmingham University, Birmingham B15 2TT, D S A Sanders Pathology, Heartlands
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors
 The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
NAACCR Webinar Series 1
 Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Melanoma 6/2/2011. Classification and Prognosis. Melanoma Statistics. American Cancer Society
 University of Pennsylvania, Ben Franklin in front of Charles Addams Building Melanoma Classification and Prognosis Emphasizing Pathology & History David Elder University of Pennsylvania Melanoma Statistics
University of Pennsylvania, Ben Franklin in front of Charles Addams Building Melanoma Classification and Prognosis Emphasizing Pathology & History David Elder University of Pennsylvania Melanoma Statistics
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
Corporate Medical Policy
 Corporate Medical Policy Gene Expression Profiling for Cutaneous Melanoma File Name: Origination: Last CAP Review: Next CAP Review: Last Review: gene_expression_profiling_for_cutaneous_melanoma 5/2018
Corporate Medical Policy Gene Expression Profiling for Cutaneous Melanoma File Name: Origination: Last CAP Review: Next CAP Review: Last Review: gene_expression_profiling_for_cutaneous_melanoma 5/2018
Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 2. Variations on the acquired nevus 3. Dermal melanocytosis
 Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 1 1A. Lentigo simplex 4 1B. Psoralens and ultraviolet A (PUVA) lentigo 6 1C. Solar lentigo 8 1D. Café au lait macule 10 1E. Ink-spot
Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 1 1A. Lentigo simplex 4 1B. Psoralens and ultraviolet A (PUVA) lentigo 6 1C. Solar lentigo 8 1D. Café au lait macule 10 1E. Ink-spot
Michael T. Tetzlaff MD, PhD
 Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
SKIN CANCER. Most common cancer diagnosis 40% of all cancers
 SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Oncology and surgery. Dra. Irene Palacios. Clínica Universidad de Navarra
 Oncology and surgery Dra. Irene Palacios. Clínica Universidad de Navarra HOW TO MANAGE HIGH RISK SCC Yaouhi Gloria Xu Anokhi Jambusaria-Pahlajani HOW TO STAGE SCC Problem with tumor depth Often not posible
Oncology and surgery Dra. Irene Palacios. Clínica Universidad de Navarra HOW TO MANAGE HIGH RISK SCC Yaouhi Gloria Xu Anokhi Jambusaria-Pahlajani HOW TO STAGE SCC Problem with tumor depth Often not posible
Specialist Referral Service Willows Information Sheets. Cancer in cats and dogs: Assessment of the patient
 Specialist Referral Service Willows Information Sheets Cancer in cats and dogs: Assessment of the patient Cancer in cats and dogs: Assessment of the patient Cancer is common in human and veterinary medicine.
Specialist Referral Service Willows Information Sheets Cancer in cats and dogs: Assessment of the patient Cancer in cats and dogs: Assessment of the patient Cancer is common in human and veterinary medicine.
Simulators of melanoma
 Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
Ductal Carcinoma-in-Situ: New Concepts and Controversies
 Ductal Carcinoma-in-Situ: New Concepts and Controversies James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Ductal Carcinoma-in-Situ: New Concepts and Controversies James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Contrast with Australian Guidelines A/Pr Pascale Guitera,
 Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Dr Rosalie Stephens. Mr Richard Martin. Medical Oncologist Auckland City Hospital Auckland
 Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
Diplomate of the American Board of Pathology in Anatomic and Clinical Pathology
 A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
MELANOMA. Some people are more likely to get a m Melanoma than others:
 MELANOMA This leaflet has been written to help you understand more about Melanoma. It tells you what is it, what causes it, what can be done about it, how it can be prevented, and where you can find out
MELANOMA This leaflet has been written to help you understand more about Melanoma. It tells you what is it, what causes it, what can be done about it, how it can be prevented, and where you can find out