Overview of AJCC 8 th Staging in Pathologic Aspects
|
|
|
- Britney Todd
- 5 years ago
- Views:
Transcription

1 Overview of AJCC 8 th Staging in Pathologic Aspects Jee Yeon KIM, M.D.,Ph.D. Department of Pathology, Pusan National University, College of Medicine, Pusan National University Yangsan Hospital, KOREA
2 Major Changes to AJCC 8 th edition Inclusion of biologic factors in staging Tumor grade, HER-2, ER, PR and genomic assays Two stage groups (anatomic and prognostic staging) options Lobular Carcinoma In Situ removed from ptis category
3 Contents Changes and clarification for T, N, M changes Clarifications for post-neoadjuvant therapy classification Inclusion of grade, HER2, ER, PR Inclusion of multigene panels Two stage group options: Anatomic for use where biomarker (grade, ER, PR, HER2) not available Prognostic for use on all USA pts
4 T, N, M Changes T Category
5 T Category Changes to AJCC 8 th edition LCIS is removed as a ptis category Pleomorphic LCIS ; also not included in a ptis category due to insufficient evidence for definitive treatment recommendations ptis (DCIS): ductal carcinoma in situ ptis (Paget): Paget disease of the nipple not associated with invasive carcinoma and/or carcinoma in situ (DCIS and/or LCIS) in the underlying breast parenchyma
6 T Category Changes to AJCC 8 th edition Rounding tumor size Do not apply for tumors between 1.0 and 1.5mm so as to not classify these cancers as microinvasive (T1mi) carcinomas (defined as invasive tumor foci 1.0mm or smaller) 1.0mm= pt1mi >1.0mm = pt1a Tumors > 1mm and < 2mm should be reported rounding to 2mm.


7 Microinvasion Most commonly seen in association with large, high-grade DCIS No focus more than 0.1 cm in greatest dimension Surrounded by dense lymphoid infiltrate or desmoplastic stroma As an indication for sentinel node biopsy or other forms of axillary node examination
8 T Category Clarification from AJCC 7 th edition Multiple tumors in same breast T category based on a single largest tumor focus Don t include satellite foci when measuring tumor size If multiple foci of microinvasion, report the number of foci and the size of the largest focus (don t combine) Use (m) modifier

9 Invasive carcinom a #1 Invasive carcinom a #2 DCIS
10 T Category Clarification from AJCC 7 th edition Multiple tumors in bilateral breast Stage each side separately
 Direct extension into skin and skin involvement only identified microscopically are NOT categorized as pt4b Such tumors are categorized based on tumor")
11 T Category Clarification from AJCC 7 th edition Skin involvement Satellite skin foci must be macroscopically identified and separate from the primary tumor (not contiguouse) Direct extension into skin and skin involvement only identified microscopically are NOT categorized as pt4b Such tumors are categorized based on tumor size

, dermal lymphatic tumor emboli are NOT")
12 T Category Clarification from AJCC 7 th edition Skin involvement In the absence of clinical findings of inflammatory carcinoma (erythema and edema involving 1/3 of breast skin), dermal lymphatic tumor emboli are NOT categorized as pt4b




13




14 T staging: pt3 (m) No inflammatory ca, no skin ulcer, not pt4
15 T, N, M Changes N Category
16 N Category Clarification from AJCC 7 th edition The criteria for pathological measurement of lymph node metastases are clearly defined. The dimension of the area containing several or multiple tumor deposits is NOT used to determined pn category. The largest contiguous tumor deposit is used for pn; adjacent satellite tumor deposits are not added.
17 N Category Clarification from AJCC 7 th edition pno (i) ITC (isolated tumor cell clusters) pn1mi, micrometast asis pn1 The largest contiguous tumor deposit must be no larger than 0.2mm. Multiple ITCs are often clustered and multiple foci are frequently present in a single node. The size of areas of noncontiguous adjacent ITCs are not added. When more than 200 singe tumor cells are present in a single lymph node cross section, this signifies that the size of the deposits= is likely greater than 0.2mm and this should be classified as a micrometastasis. At least one contiguous tumor deposit must be larger than 0.2mm and the largest contiguous tumor deposit must be no larger than 2.0mm. The sizes of noncontiguous adjacent tumor deposits are not added. Multiple micrometastases may be present in a single lymph node. At least one contiguous tumor deposit must be larger than 2.0mm
18 N Category Clarification from AJCC 7 th edition Assessment of N category Invasive tumor nodules in axillary fat without apparent nodal tissue are classified as regional lymph node metastases (pn)
19 N Category Clarification from AJCC 7 th edition Assessment of N category Metastasis to lymph nodes from the following sites are regional nodes and categorized as pn Axillary, intramammary, interpectoral, internal mammary and supraclavicular Metastases to any other lymph nodes (including cervical or contralateral internal mammary or contralateral axillary lymph nodes) are categorized as pm1
20 N Category Changes to AJCC 8 th edition (f) modifier added to the N category confirmation of metastasis by either FNA or core needle biopsy, with NO further resection of nodes Usually applies to cn staging before definitive resection or neoadjuvant therapy
 S16-7402")



21 S (Right Breast) S (Left Lymph Node) ctnm staging: Right ct1c (f) cn0 cm0 ctnm staging: Left ctx cn1(f) cm0 ptnm staging: pt1c pn0 (sn) pm1
22 N Category Clarification from AJCC 7 th edition Assessment of N category Nodes with isolated tumor cells (ITCs) only are not included in the overall count of positive nodes When measuring ITCs, report size of largest contiguous focus (NOT the overall area in which the ITCs are found) Example 10 nodes: 2 with macromets; 2 with ITCs No. of positive nodes is 2 out of 10 pn1a (not 4/10 = pn2a)
23 T, N, M Changes M Category
24 M Category Clarification from AJCC 7 th edition pm0 is not a valid category Valid M categories for clinical and pathological staging cm0: no signs or symptoms of distant metastasis cm1: signs, symptoms, or imaging evidence of distant metastasis pm1: microscopic confirmation of distant metastasis
25 Post Neoadjuvant Therapy Staging
26 Post Neoadjuvant Theraphy Staging Clarification from AJCC 7 th edition Assigined after neoadjuvant therapy and surgical resection ypt category Largest focus of residual tumor Treatment-related fiborosis near invasive tumor NOT used Multiple foci of residual tumor, use (m) modifier
27 Post Neoadjuvant Theraphy Staging Clarification from AJCC 7 th edition Assigined after neoadjuvant therapy and surgical resection ypn category Largest focus of residual tumor in nodes Treatment-related fiborosis near invasive tumor NOT used
28 Post Neoadjuvant Theraphy Staging Clarification from AJCC 7 th edition Assigined after neoadjuvant therapy and surgical resection M category If M1 prior to therapy, remains M1 following neoadjuvant therapy Regardless of observed response to therapy
29 Post Neoadjuvant Theraphy Staging Clarification from AJCC 7 th edition pcr pcr(pathological complete response) No sidual tumor ypt0 ypn0 cm0 any residual invasive carcinoma detected by pathological examination in the breast, including cancer within blood or lymph vessels (LVI) or lymph nodes precludes posttreatment classification as a complete pathological response (pcr). no stage group assigned, under preparation





30 Post Neoadjuvant Therapy ypt0 yn1mi cm0
31 Biologic Markers Histologic Grade
32 Biomarker Categories Modified Nottingham (Bloom Scarf Richardson) tumor grade should be documented All invasive carcinomas should have the following determined by appropriate assays whenever possible ER status PR status HER2 status Marker of proliferatio if also recommended Ki67
33 Histologic Grade All invasive carcinoma of breast should be assigned histologic grade Nottingham modification of SBR grading system recommended Nottingham modification of the Bloom Richardson system Tubule formation 1 point: Tubular formations in >75% of the tumor 2 points: Tubular formations in 10 75% of the tumor 3 points: Tubular formations in <10% of the tumor Note: For scoring tubule formations, the overall appearance of the tumor has to be taken into consideration. Nuclear pleomorphism 1 point: Nuclei with minimal variation in size and shape 2 points: Nuclei with moderate variation in size and shape 3 points: Nuclei with marked variation in size and shape Note: The tumor areas having cells with greatest atypia should be evaluated. Mitotic count 1, 2, or 3 points, according to Table 20.5






34 Histologic Grade Tubule Formation Score 1 Tubule formations in >75% Score 2 in10-75% Nuclear Grade Score 3 In <10% Score 1 Score 2 Score 3
 Leitz or Ortholux 25x objective or comparable with field diameter of 0.")
35 Histologic Grade Mitotic Count Number of mitotic figures in most active area, counting 10 high power fields: (a) (b) (c) 1 point: points: points: (a) Nikon or Labophot 40x objective or comparable with field diameter of 0.44 mm (b) Leitz or Ortholux 25x objective or comparable with field diameter of 0.59 mm (c) Leitz or Diaplan 40x objective or comparable with field diameter of 0.63 mm Notes: Count mitotic figures at periphery of tumor in most mitotically active area; count 10 high power fields in the same area, but not necessarily contiguous; select fields with as much tumor as possible; avoid poorly preserved areas; ignore cells with hyperchromatic and pyknotic nuclei, which may be undergoing apoptosis Quick scan mitotic impression is less accurate (Hum Pathol 2008;39:584) Calibration of microscopc magnification: NHSBSP No 58, Jan 2005:80,
36 Calibration of microscopc magnification: NHSBSP No 58, Jan 2005:80,
37 Histologic Grade Nottingham s combined histologic grade G1. Well Differentiated: - score 5 G2. Moderately Differentiated: score 6,7 G3. Poorly Differentiated: score 8,9 Sum of the scores of tubule formation + nuclear grade+ mitosis
38 Nuclear grade of DCIS Features Pleomorphism Size Chromatin Grade I (Low) Monotonous (monomorphic) 1.5X to 2X the size of a normal RBC or a normal duct epithelial cell nucleus Usually diffuse, finely dispersed chromatin Grade II (Intermediate) Intermediate Intermediate Intermediate Grade III (High) Markedly pleomorphic > 2X the size of a normal RBC or a normal duct epithelial cell nucleus Usually vesicular with irregular chromatin distribution Nucleoli Only occasional Intermediate Prominent, often multiple Mitoses Only occasional Intermediate May be frequent Orientation Polarized toward luminal spaces Intermediate Usually not polarized toward the luminal space Schwartz GF, Lagios MD, Carter D, et al. Cancer 1997;80:
39 Biologic Markers ER, PR and HER2


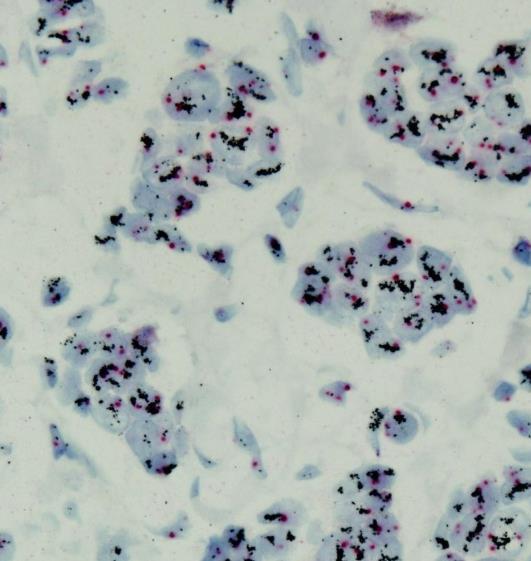
40 ER and PR ER & PR expression measured primarily by IHC 1% of cells stained considered positive for ER & PR Multiple results always use positive results If biopsy and resection specimens are tested, and One is positive, while the other is negative, then Use the positive results to assign the stage group ER PR
41 American Society of Clinical Oncology/College of American Pathologists Guideline Recommendations for Immunohistochemical Testing of Estrogen and Progesterone Receptors in Breast Cancer Reporting elements for ER and PR IHC assay Percentage of invasive tumor cells exhibiting nuclear staining Intensity of staining: strong, medium, or weak Interpretation: Positive, negative, or uninterpretable Internal and external contrils (positive, negative, or not present) Standard assay conditions met/not met (including cold ischemic time and fixation parameters) Positive for ER or PR if finding of 1% of tumor cell nuclei are immunoreactive Negative for ER or PR if finding of <1% of tumor cell nuclei are immunoreactive in the presence of evidence that the sample can express ER or PR (positive internal control) Uninterpretable for ER, or PR if finding that no tumor nuclei are immunoreactive and that internal controls lack any nuclear staining Hammond et al. J Clin Oncol Jun 1; 28(16):

42 ER and PR Allred score= PS + IS (range 0~8)
 Wolff et al. J Clin Oncol.")
43 Evaluation of HER2 Proteon Expression by IHC (2013 ASCO/CAP Guideline) Wolff et al. J Clin Oncol. 2013; 31:
 Wolff et al. J Clin Oncol.")
44 Evaluation of HER2 Gene Amplification by ISH (2013 ASCO/CAP Guideline) Wolff et al. J Clin Oncol. 2013; 31:
 Wolff et al. J Clin Oncol.")
45 Evaluation of HER2 Gene Amplification by ISH (2013 ASCO/CAP Guideline) Wolff et al. J Clin Oncol. 2013; 31:







46 Her2 IHC Negative Equivocale Positive Her2 SISH Not Amplified Amplified NA NA A A
47 Multigene Panels
48 Inclusion of Multigene Panels (when available) as Stage Modifiers T1 and T2 HR-positive, HER-2 negative and LN negative tumors ==== T1aT1bN0M0 21 Gene Recurrence Score (Oncotype Dx) : RS < 11 Breast Cancer Index: Low risk range EndoPredict: low risk score Mammaprint: low risk score PAM 50 (Prosigna): low range ROR
49 Two Stage Groups Anatomic Pathologic
50 Pathologic Prognostic Groups Based on pathologic findings at definitive surgery and biomarkers (grade, ER, PR, and HER2, multigene prognostic panels) Relavant to all patients treated with definitive surgery as initial treatment Not appropriate for patients reveiving neoadjuvant systemic or radiation treatment It is the recommended staiging system for use in the USA by all tumor registries
51 Cases






52




, PR")
53 ER PR pt2(m) pn0 cm0 Anatomic Stage Group IIA Moderately differentiated, score 7 (2+3+2) Pathologic Prognostic Stage ER(+), PR (+), HER2 (-), Ki67 50% Group IA





54




55 Lymph node metastasis pt2 (m) pn1 cm0 Anatomic Stage Group IIB Histologic grade: poorly differentiated by Nottingham's combined histologic grade (total score = 9; tubule formation=3, nuclear grade=3, mitosis=3) Pathologic Prognostic Stage Group IIIA ER(-), PR (-), HER2(-) Ki67 50%






56
 Nottingham's Anatomic combined Stage histologic Group grade IIA Mass #2 2.0x1.2cm x 2.")
57 Medial Slice #1 pt2 (m) pn0 cm0 Lateral Slice #21 Mass #1 0.9x0.4cm x 0.5cm(slice 8) Mass #6 Histologic grade: moderately differentiated 0.3x0.3cm by X0.5cm (slice 12) Nottingham's Anatomic combined Stage histologic Group grade IIA Mass #2 2.0x1.2cm x 2.0cm(slice 8 to 11) (total score = 7; tubule formation= 2, nuclear grade= 3, mitosis= 2)) Pathologic Prognostic Stage Group IA Mass #3 0.6x0.6cm X 0.5cm (slice 8) Mass #4 0.8x0.4cm X0.5cm (slice 8) ER(+), PR (+), HER2(-) Ki67 10% Mass #7 3.4x1.0cm X3.0cm(slice 13 to 18) Mass #5 0.7x0.7cm X1.5cm (slice 10 to 12)




58
 Mass #3 0.5x0.2x0.")



59 Mass #1 3.0x1.3x0.7cm (slice 6 to 11) Mass #2 0.7x0.5X0.5cm (slice 8) Mass #3 0.5x0.2x0.2cm (slice 10) pt2 (m) pn0 (sn) cm0 Anatomic Stage Group IIA Histologic grade: well differentiated by Nottingham's combined histologic grade (total score = 4; tubule formation=1, nuclear grade=2, mitosis=1) Pathologic Prognostic Stage Group IA Mass #4 0.5x0.1x0.1cm (slice 10) ER(+), PR (+), HER2(2+) FISH NA Ki67 1%
60 Summary Changes and clarification for T, N, M changes Clarifications for post-neoadjuvant therapy classification Inclusion of grade, HER2, ER, PR Inclusion of multigene panels Two stage group options: Anatomic for use where biomarker (grade, ER, PR, HER2) not available Prognostic for use on all USA pts

61 Thank you for your attention!
3/23/2017. Disclosure of Relevant Financial Relationships. Pathologic Staging Updates in Breast Cancer. Pathologic Staging Updates Breast Cancer
 Pathologic Staging Updates in Breast Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
Pathologic Staging Updates in Breast Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
STAGE CATEGORY DEFINITIONS
 CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
Descriptor Definition Author s notes TNM descriptors Required only if applicable; select all that apply multiple foci of invasive carcinoma
 S5.01 The tumour stage and stage grouping must be recorded to the extent possible, based on the AJCC Cancer Staging Manual (7 th Edition). 11 (See Tables S5.01a and S5.01b below.) Table S5.01a AJCC breast
S5.01 The tumour stage and stage grouping must be recorded to the extent possible, based on the AJCC Cancer Staging Manual (7 th Edition). 11 (See Tables S5.01a and S5.01b below.) Table S5.01a AJCC breast
Completing the Puzzle AJCC TNM Staging Breast. Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017
 Completing the Puzzle AJCC TNM Staging Breast Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017 OBJECTIVES Understanding of Breast TNM staging Identify clinical
Completing the Puzzle AJCC TNM Staging Breast Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017 OBJECTIVES Understanding of Breast TNM staging Identify clinical
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
UN KEY ARTICLE PER UN ANATOMOPATOLOGO. Dr. Davide Balmativola Prof.ssa Anna Sapino Dr.ssa Isabella Castellano
 UN KEY ARTICLE PER UN ANATOMOPATOLOGO Dr. Davide Balmativola Prof.ssa Anna Sapino Dr.ssa Isabella Castellano ptnm staging IL RUOLO PIÙIMPORTANTE DEL SISTEMA DI STAGING: CA Cancer J Clin 2006;56:37 47 Raggruppare
UN KEY ARTICLE PER UN ANATOMOPATOLOGO Dr. Davide Balmativola Prof.ssa Anna Sapino Dr.ssa Isabella Castellano ptnm staging IL RUOLO PIÙIMPORTANTE DEL SISTEMA DI STAGING: CA Cancer J Clin 2006;56:37 47 Raggruppare
B REAST STAGING FORM. PATHOLOGIC Extent of disease through completion of definitive surgery. CLINICAL Extent of disease before any treatment
 B REAST STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi c a b c d TUMOR SIZE:
B REAST STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi c a b c d TUMOR SIZE:
Protocol for the Examination of Specimens From Patients With Invasive Carcinoma of the Breast
 Protocol for the Examination of Specimens From Patients With Invasive Carcinoma of the Breast Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Protocol for the Examination of Specimens From Patients With Invasive Carcinoma of the Breast Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Chapter 2 Staging of Breast Cancer
 Chapter 2 Staging of Breast Cancer Zeynep Ozsaran and Senem Demirci Alanyalı 2.1 Introduction Five decades ago, Denoix et al. proposed classification system (tumor node metastasis [TNM]) based on the dissemination
Chapter 2 Staging of Breast Cancer Zeynep Ozsaran and Senem Demirci Alanyalı 2.1 Introduction Five decades ago, Denoix et al. proposed classification system (tumor node metastasis [TNM]) based on the dissemination
B REAST STAGING FORM. PATHOLOGIC Extent of disease through completion of definitive surgery. CLINICAL Extent of disease before any treatment
 B REAST STAGING FORM Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi a b c a b c d TUMOR SIZE: S TAGE
B REAST STAGING FORM Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi a b c a b c d TUMOR SIZE: S TAGE
ACRIN 6666 Therapeutic Surgery Form
 S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
Q&A. Fabulous Prizes. Collecting Cancer Data: Breast 4/4/13. NAACCR Webinar Series Collecting Cancer Data Breast
 Collecting Cancer Data Breast NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Collecting Cancer Data Breast NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer
 Young Investigator Award, Global Breast Cancer Conference 2018 Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer ㅑ Running head: Revisiting estrogen positive tumors
Young Investigator Award, Global Breast Cancer Conference 2018 Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer ㅑ Running head: Revisiting estrogen positive tumors
Protocol for the Examination of Specimens from Patients with Invasive Carcinoma of the Breast
 Protocol for the Examination of Specimens from Patients with Invasive Carcinoma of the Breast Protocol applies to all invasive carcinomas of the breast, including ductal carcinoma in situ (DCIS) with microinvasion.
Protocol for the Examination of Specimens from Patients with Invasive Carcinoma of the Breast Protocol applies to all invasive carcinomas of the breast, including ductal carcinoma in situ (DCIS) with microinvasion.
Protocol for the Examination of Resection Specimens From Patients With Invasive Carcinoma of the Breast
 Protocol for the Examination of Specimens From Patients With Invasive Carcinoma of the Breast Version: Breast Invasive 4.2.0.0 Protocol Posting Date: February 2019 CAP Laboratory Accreditation Program
Protocol for the Examination of Specimens From Patients With Invasive Carcinoma of the Breast Version: Breast Invasive 4.2.0.0 Protocol Posting Date: February 2019 CAP Laboratory Accreditation Program
Seventh Edition Staging 2017 Breast
 Seventh Edition Staging 2017 Breast Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express written
Seventh Edition Staging 2017 Breast Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express written
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Breast Cancer SOLID TUMOR RULES 2018 MORE CHANGES MPH MAJOR CHANGES
 1 SOLID TUMOR RULES 2018 Breast Cancer Changes in 2018 Use ICD-O without publication number (not ICD-O-3) Use rule set based on DATE OF DIAGNOSIS Biomarkers influence unknown in histology Do NOT use to
1 SOLID TUMOR RULES 2018 Breast Cancer Changes in 2018 Use ICD-O without publication number (not ICD-O-3) Use rule set based on DATE OF DIAGNOSIS Biomarkers influence unknown in histology Do NOT use to
A712(19)- Test slide, Breast cancer tissues with corresponding normal tissues
- Test slide, Breast cancer tissues with corresponding normal tissues") A712(19)- Test slide, Breast cancer tissues with corresponding normal tissues (formalin fixed) For research use only Specifications: No. of cases: 12 Tissue type: Breast cancer tissues with corresponding
A712(19)- Test slide, Breast cancer tissues with corresponding normal tissues (formalin fixed) For research use only Specifications: No. of cases: 12 Tissue type: Breast cancer tissues with corresponding
Evaluation of Breast Specimens Removed by Needle Localization Technique
 Evaluation of Breast Specimens Removed by Needle Localization Technique Specimen Handling: The breast specimen when received should be measured and grossly inspected for any orientation designated by the
Evaluation of Breast Specimens Removed by Needle Localization Technique Specimen Handling: The breast specimen when received should be measured and grossly inspected for any orientation designated by the
Case Scenario 1 History and Physical 3/15/13 Imaging Pathology
 Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Protocol for the Examination of Biopsy Specimens From Patients With Invasive Carcinoma of the Breast
 Protocol for the Examination of Specimens From Patients With Invasive Carcinoma of the Breast Version: BreastInvasive 1.0.0.0 Protocol Posting Date: February 2019 Accreditation Requirements The use of
Protocol for the Examination of Specimens From Patients With Invasive Carcinoma of the Breast Version: BreastInvasive 1.0.0.0 Protocol Posting Date: February 2019 Accreditation Requirements The use of
6. Cervical Lymph Nodes and Unknown Primary Tumors of the Head and Neck
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Post Neoadjuvant therapy: issues in interpretation
 Post Neoadjuvant therapy: issues in interpretation Disclosure: Overview D Prognostic features in assessment of post treatment specimens: Tumor size Cellularity Grade Receptors LN Neoadjuvant chemotherapy:
Post Neoadjuvant therapy: issues in interpretation Disclosure: Overview D Prognostic features in assessment of post treatment specimens: Tumor size Cellularity Grade Receptors LN Neoadjuvant chemotherapy:
AJCC Cancer Staging Manual Eighth Edition FOR PERSONAL USE ONLY
 AJCC Cancer Staging Manual Eighth Edition Contents Authors... 4 Chapter Summary... 4 Cancers Staged Using This Staging System... 4 Cancers Not Staged Using This Staging System... 4 Summary of Changes...
AJCC Cancer Staging Manual Eighth Edition Contents Authors... 4 Chapter Summary... 4 Cancers Staged Using This Staging System... 4 Cancers Not Staged Using This Staging System... 4 Summary of Changes...
Sentinel nodes. Location: Location: S1.04 Principal clinician. G1.01 Record other relevant information. S2.01 Number of specimens submitted
 Invasive Breast Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth DD MM YYYY
Invasive Breast Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth DD MM YYYY
Reporting of Breast Cancer Do s and Don ts
 Reporting of Breast Cancer Do s and Don ts 7 th SGH Annual Breast Pathology Course Professor Michael Bilous Conjoint Professor Western Sydney University Consultant Pathologist, Australian Clinical Labs,
Reporting of Breast Cancer Do s and Don ts 7 th SGH Annual Breast Pathology Course Professor Michael Bilous Conjoint Professor Western Sydney University Consultant Pathologist, Australian Clinical Labs,
Q: How do you clinically code the N if the nodes are stated to be positive on mammogram/us or other imaging? No biopsy of nodes was done.
 Q&A Breast Webinar Q: One of my investigators is interested in knowing when Oncotype DX data collection was implemented. That data is collected in SSFs 22 and 23. I remember that the SSFs for breast were
Q&A Breast Webinar Q: One of my investigators is interested in knowing when Oncotype DX data collection was implemented. That data is collected in SSFs 22 and 23. I remember that the SSFs for breast were
Breast cancer staging update. Ekaterini Tsiapali, MD, FACS MedStar Regional Breast Program Site Director
 Breast cancer staging update Ekaterini Tsiapali, MD, FACS MedStar Regional Breast Program Site Director 1 1 Review of the AJCC 8 th edition breast cancer staging Review of genomic assays as stage modifiers
Breast cancer staging update Ekaterini Tsiapali, MD, FACS MedStar Regional Breast Program Site Director 1 1 Review of the AJCC 8 th edition breast cancer staging Review of genomic assays as stage modifiers
Collecting Cancer Data: Breast. Prizes! Collecting Cancer Data: Breast 8/4/ NAACCR Webinar Series 1. NAACCR Webinar Series
 Collecting Cancer Data: Breast NAACCR 2008 2009 Webinar Series Prizes! Question of the Month! The participant that submits the best question of the session will receive a fbl fabulous Pi Prize! Shannon
Collecting Cancer Data: Breast NAACCR 2008 2009 Webinar Series Prizes! Question of the Month! The participant that submits the best question of the session will receive a fbl fabulous Pi Prize! Shannon
PART VII Breast. Breast 345
 PART VII Breast Breast 345 3 2 Breast At-A-Glance SUMMARY OF CHANGES Tumor (T) Identified specific imaging modalities that can be used to estimate clinical tumor size, including mammography, ultrasound,
PART VII Breast Breast 345 3 2 Breast At-A-Glance SUMMARY OF CHANGES Tumor (T) Identified specific imaging modalities that can be used to estimate clinical tumor size, including mammography, ultrasound,
Case Scenario 1. 2/15/2011 The patient received IMRT 45 Gy at 1.8 Gy per fraction for 25 fractions.
 Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer. Pathology. AGO e. V. in der DGGG e.v. sowie in der DKG e.v.
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Pathology Pathology Versions 2004 2017: Blohmer / Costa / Fehm / Friedrichs / Huober / Kreipe / Lück / Schneeweis / Sinn /
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Pathology Pathology Versions 2004 2017: Blohmer / Costa / Fehm / Friedrichs / Huober / Kreipe / Lück / Schneeweis / Sinn /
Staging for Residents, Nurses, and Multidisciplinary Health Care Team
 Staging for Residents, Nurses, and Multidisciplinary Health Care Team Donna M. Gress, RHIT, CTR Validating science. Improving patient care. Learning Objectives Introduce the concept and history of stage
Staging for Residents, Nurses, and Multidisciplinary Health Care Team Donna M. Gress, RHIT, CTR Validating science. Improving patient care. Learning Objectives Introduce the concept and history of stage
Pathology Report Patient Companion Guide
 Pathology Report Patient Companion Guide Breast Cancer - Understanding Your Pathology Report Pathology Reports can be overwhelming. They contain scientific terms that are unfamiliar and might be a bit
Pathology Report Patient Companion Guide Breast Cancer - Understanding Your Pathology Report Pathology Reports can be overwhelming. They contain scientific terms that are unfamiliar and might be a bit
Breast cancer: Molecular STAGING classification and testing. Korourian A : AP,CP ; MD,PHD(Molecular medicine)
") Breast cancer: Molecular STAGING classification and testing Korourian A : AP,CP ; MD,PHD(Molecular medicine) Breast Cancer Theory: Halsted Operative breast cancer is a local-regional disease The positive
Breast cancer: Molecular STAGING classification and testing Korourian A : AP,CP ; MD,PHD(Molecular medicine) Breast Cancer Theory: Halsted Operative breast cancer is a local-regional disease The positive
Surgical Pathology Issues of Practical Importance
 Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
47. Melanoma of the Skin
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]
![Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]](/thumbs/82/86783199.jpg "Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]") CS Tumor Size Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ] Note: the specific tumor size as documented in the medical record. If the ONLY information regarding tumor size is the physician's
CS Tumor Size Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ] Note: the specific tumor size as documented in the medical record. If the ONLY information regarding tumor size is the physician's
Evaluation of Pathologic Response in Breast Cancer Treated with Primary Systemic Therapy
 Evaluation of Pathologic Response in Breast Cancer Treated with Primary Systemic Therapy Eun Yoon Cho, MD, PhD Department of Pathology and Translational Genomics Samsung Medical Center Sungkyunkwan University
Evaluation of Pathologic Response in Breast Cancer Treated with Primary Systemic Therapy Eun Yoon Cho, MD, PhD Department of Pathology and Translational Genomics Samsung Medical Center Sungkyunkwan University
A712(18)- Test slide, Breast cancer tissues with corresponding normal tissues
- Test slide, Breast cancer tissues with corresponding normal tissues") A712(18)- Test slide, Breast cancer tissues with corresponding normal tissues (formalin fixed) For research use only Specifications: No. of cases: 12 Tissue type: Breast cancer tissues with corresponding
A712(18)- Test slide, Breast cancer tissues with corresponding normal tissues (formalin fixed) For research use only Specifications: No. of cases: 12 Tissue type: Breast cancer tissues with corresponding
CPC 4 Breast Cancer. Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast.
 CPC 4 Breast Cancer Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast. 1. What are the most likely diagnoses of this lump? Fibroadenoma
CPC 4 Breast Cancer Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast. 1. What are the most likely diagnoses of this lump? Fibroadenoma
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine
 Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Breast pathology. 2nd Department of Pathology Semmelweis University
 Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
46. Merkel Cell Carcinoma
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Barriers to Understanding
 Behind the Scenes: The Critical Importance of Cancer Cell Pathology and the Pathologist Sherry T. Emery, M.D., Chief of Pathology Northeast Health System Barriers to Understanding Questions for 2010 What
Behind the Scenes: The Critical Importance of Cancer Cell Pathology and the Pathologist Sherry T. Emery, M.D., Chief of Pathology Northeast Health System Barriers to Understanding Questions for 2010 What
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Breast Cancer. Dr Rodney Itaki Anatomical Pathology Discipline Division of Pathology
 Breast Cancer Dr Rodney Itaki Anatomical Pathology Discipline Division of Pathology Muscles Muscles underneath the breasts separating them from the ribs Breast has no muscle tissue 2 Female Breast Anatomy
Breast Cancer Dr Rodney Itaki Anatomical Pathology Discipline Division of Pathology Muscles Muscles underneath the breasts separating them from the ribs Breast has no muscle tissue 2 Female Breast Anatomy
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Registrar s Guide to Chapter 1, AJCC Seventh Edition. Overview. Learning Objectives. Describe intent and purpose of AJCC staging
 Registrar s Guide to Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers for Disease Control
Registrar s Guide to Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers for Disease Control
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
10. HPV-Mediated (p16+) Oropharyngeal Cancer
 Oropharyngeal Cancer") 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
SEER Summary Stage Still Here!
 SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
AJCC CANCER STAGE. Site-Specific Instructions - BREAST. Reference: AJCC Cancer Staging Manual, 7 th Edition
 Slide 1 AJCC CANCER STAGE Site-Specific Instructions - BREAST Reference: AJCC Cancer Staging Manual, 7 th Edition In this presentation, we are going to review the AJCC Cancer Staging criteria for the breast
Slide 1 AJCC CANCER STAGE Site-Specific Instructions - BREAST Reference: AJCC Cancer Staging Manual, 7 th Edition In this presentation, we are going to review the AJCC Cancer Staging criteria for the breast
5/8/2014. AJCC Stage Introduction and General Rules. Acknowledgements* Introduction. Melissa Pearson, CTR North Carolina Central Cancer Registry
 AJCC Stage Introduction and General Rules Linda Mulvihill Public Health Advisor NCRA Annual Meeting May 2014 National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention
AJCC Stage Introduction and General Rules Linda Mulvihill Public Health Advisor NCRA Annual Meeting May 2014 National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention
Diseases of the breast (2 of 2) Breast cancer
 Breast cancer") Diseases of the breast (2 of 2) Breast cancer Epidemiology & etiology The most common type of cancer & the 2 nd most common cause of cancer death in women 1 of 8 women in USA Affects 7% of women Peak at
Diseases of the breast (2 of 2) Breast cancer Epidemiology & etiology The most common type of cancer & the 2 nd most common cause of cancer death in women 1 of 8 women in USA Affects 7% of women Peak at
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
The Voyage to Direct Coding of AJCC TNM & Stage... Jayne Holubowsky, CTR DelMarVa-DC Educational Meeting Annapolis, MD October 8, 2015.
 The Voyage to Direct Coding of AJCC TNM & Stage... Jayne Holubowsky, CTR DelMarVa-DC Educational Meeting Annapolis, MD October 8, 2015 outline Evolution General Rules Site-specific Rules How well do you
The Voyage to Direct Coding of AJCC TNM & Stage... Jayne Holubowsky, CTR DelMarVa-DC Educational Meeting Annapolis, MD October 8, 2015 outline Evolution General Rules Site-specific Rules How well do you
CLINICAL SIGNIFICANCE OF BENIGN EPITHELIAL CHANGES
 Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Major Rule Changes. Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging
 AJCC 8 th Edition Staging Major Rule Changes Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving patient
AJCC 8 th Edition Staging Major Rule Changes Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving patient
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Case Scenario 1: Breast
 Case Scenario 1: Breast A 63 year old white female presents with a large mass in her left breast. 4/15/13 Mammogram/US: 1. Left breast mammographic and sonographic at 3:00 measuring 7.1 cm highly suggestive
Case Scenario 1: Breast A 63 year old white female presents with a large mass in her left breast. 4/15/13 Mammogram/US: 1. Left breast mammographic and sonographic at 3:00 measuring 7.1 cm highly suggestive
Jose A Torres, MD 1/12/2017
 Jose A Torres, MD 1/12/2017 Background Globally leading cause of cancer related death in women ~249,000 Americans diagnosed with invasive breast cancer ~40,890 will die of their disease Breast cancer risk
Jose A Torres, MD 1/12/2017 Background Globally leading cause of cancer related death in women ~249,000 Americans diagnosed with invasive breast cancer ~40,890 will die of their disease Breast cancer risk
Collaborative Stage Site-Specific Instructions - BREAST
 Slide 1 Collaborative Stage Site-Specific Instructions - BREAST In this presentation, we are going to review the CS Data Items and coding instructions for the breast primary site. Slide 2 Reading Assignments
Slide 1 Collaborative Stage Site-Specific Instructions - BREAST In this presentation, we are going to review the CS Data Items and coding instructions for the breast primary site. Slide 2 Reading Assignments
ROBINSON CYTOLOGICAL GRADING OF BREAST CARCINOMA ON FINE NEEDLE ASPIRATION CYTOLOGY- AN OVERVIEW
 Page564 Research Article Biological Sciences ROBINSON CYTOLOGICAL GRADING OF BREAST CARCINOMA ON FINE NEEDLE ASPIRATION CYTOLOGY- AN OVERVIEW Charusheela Rajesh Gore, Chandanwale Shirish S, Ruchika Aggarwal,
Page564 Research Article Biological Sciences ROBINSON CYTOLOGICAL GRADING OF BREAST CARCINOMA ON FINE NEEDLE ASPIRATION CYTOLOGY- AN OVERVIEW Charusheela Rajesh Gore, Chandanwale Shirish S, Ruchika Aggarwal,
Retrospective analysis to determine the use of tissue genomic analysis to predict the risk of recurrence in early stage invasive breast cancer.
 Retrospective analysis to determine the use of tissue genomic analysis to predict the risk of recurrence in early stage invasive breast cancer. Goal of the study: 1.To assess whether patients at Truman
Retrospective analysis to determine the use of tissue genomic analysis to predict the risk of recurrence in early stage invasive breast cancer. Goal of the study: 1.To assess whether patients at Truman
Recent advances in breast cancers
 Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Contemporary Classification of Breast Cancer
 Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
FOR PERSONAL USE ONLY
 Members of the Breast Expert Panel Sunil S. Badve, MD Peter D. Beitsch, MD, FACS Shikha Bose, MD David R. Byrd, MD, FACS Vivien W. Chen, PhD Data Collection Core Representative James L. Connolly, MD Basak
Members of the Breast Expert Panel Sunil S. Badve, MD Peter D. Beitsch, MD, FACS Shikha Bose, MD David R. Byrd, MD, FACS Vivien W. Chen, PhD Data Collection Core Representative James L. Connolly, MD Basak
Papillary Lesions of the Breast: WHO Update
 Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Carcinome du sein Biologie moléculaire. Thomas McKee Service de Pathologie Clinique Genève
 Carcinome du sein Biologie moléculaire Thomas McKee Service de Pathologie Clinique Genève Pathology Diagnostic Prognostic information Predictive information The information provided depends on the available
Carcinome du sein Biologie moléculaire Thomas McKee Service de Pathologie Clinique Genève Pathology Diagnostic Prognostic information Predictive information The information provided depends on the available
Breast Pathology Post-Neoadjuvant Chemotherapy. Megan Troxell, MD/PhD Stanford Pathology
 Breast Pathology Post-Neoadjuvant Chemotherapy Megan Troxell, MD/PhD Stanford Pathology 2 mm Objectives Develop a framework for gross analysis of post-chemotherapy breast specimens. Recognize histologic
Breast Pathology Post-Neoadjuvant Chemotherapy Megan Troxell, MD/PhD Stanford Pathology 2 mm Objectives Develop a framework for gross analysis of post-chemotherapy breast specimens. Recognize histologic
3/23/2017. Disclaimer. Common Changes in TNM Staging. Overview. Overview. Understanding Terminology. Overview
 Common Changes in TNM Staging Understanding the General Rules of Cancer Staging Thomas P. Baker, MD FCAP March 5, 2017 Disclaimer The identification of specific products or scientific instrumentation is
Common Changes in TNM Staging Understanding the General Rules of Cancer Staging Thomas P. Baker, MD FCAP March 5, 2017 Disclaimer The identification of specific products or scientific instrumentation is
A Retrospective Analysis of Clinical Utility of AJCC 8th Edition Cancer Staging System for Breast Cancer
 Elmer ress Original Article World J Oncol. 2017;8(3):71-75 A Retrospective Analysis of Clinical Utility of AJCC 8th Edition Cancer Staging System for Breast Cancer Hui Hu a, Wei Wei a, Xin Yi a, Ling Xin
Elmer ress Original Article World J Oncol. 2017;8(3):71-75 A Retrospective Analysis of Clinical Utility of AJCC 8th Edition Cancer Staging System for Breast Cancer Hui Hu a, Wei Wei a, Xin Yi a, Ling Xin
LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL
 LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL ( ) Tx Primary tumor cannot be assessed, or tumor proven by the presence of malignant cells in sputum or bronchial washings but not visualized by imaging
LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL ( ) Tx Primary tumor cannot be assessed, or tumor proven by the presence of malignant cells in sputum or bronchial washings but not visualized by imaging
14. Mucosal Melanoma of the Head and Neck
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1. Guidelines for Reporting Carcinoma of the Breast
 1 2 1. Guidelines for Reporting Carcinoma of the Breast Compilation and editing of this volume: Prof. Dilani Lokuhetty (Consultant Histopathologist) List of contributors Consultant Histopathologists Dr.
1 2 1. Guidelines for Reporting Carcinoma of the Breast Compilation and editing of this volume: Prof. Dilani Lokuhetty (Consultant Histopathologist) List of contributors Consultant Histopathologists Dr.
Evaluación de la respuesta patológica completa tras tratamiento neoadyuvante en cáncer de mama. José Palacios Calvo Servicio de Anatomía Patológica
 Evaluación de la respuesta patológica completa tras tratamiento neoadyuvante en cáncer de mama José Palacios Calvo Servicio de Anatomía Patológica E-Cadherin HER2 HER2 p63 Pathological Response Pathological
Evaluación de la respuesta patológica completa tras tratamiento neoadyuvante en cáncer de mama José Palacios Calvo Servicio de Anatomía Patológica E-Cadherin HER2 HER2 p63 Pathological Response Pathological
Disclosures. Outline. What IS tumor budding?? Tumor Budding in Colorectal Carcinoma: What, Why, and How. I have nothing to disclose
 Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
ONLINE CONTINUING EDUCATION ACTIVITY
 ONLNE CONTNUNG EDUCATON ACTVTY Take free quizzes online at acsjournals.com/ce ARTCLE TTLE: Breast Cancer Major Changes in the American Joint Committee on Cancer Eighth Edition Cancer Staging Manual CONTNUNG
ONLNE CONTNUNG EDUCATON ACTVTY Take free quizzes online at acsjournals.com/ce ARTCLE TTLE: Breast Cancer Major Changes in the American Joint Committee on Cancer Eighth Edition Cancer Staging Manual CONTNUNG
Breast Cancer TREATMENT APPROACHES STAGING TUMOUR BIOLOGY. Breast Cancer
 45 Dr K Tabane MBChB,FCP(SA); Certificate of Medical Oncology (Physicians) Specialist Physician, Medical Oncologist, Director: Sandton Oncology According to the CANSA statistics, breast cancer is the most
45 Dr K Tabane MBChB,FCP(SA); Certificate of Medical Oncology (Physicians) Specialist Physician, Medical Oncologist, Director: Sandton Oncology According to the CANSA statistics, breast cancer is the most
MCR: MANAGEMENT OF 2018 CHANGES. By: Maricarmen Traverso-Ortiz MPH, CGG, CTR
 MCR: MANAGEMENT OF 2018 CHANGES By: Maricarmen Traverso-Ortiz MPH, CGG, CTR LEARNING OBJECTIVES Discuss a summary of the new changes for 2018 Overview of how the Maryland Cancer Registry is managing and
MCR: MANAGEMENT OF 2018 CHANGES By: Maricarmen Traverso-Ortiz MPH, CGG, CTR LEARNING OBJECTIVES Discuss a summary of the new changes for 2018 Overview of how the Maryland Cancer Registry is managing and
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Papillary Lesions of the Breast
 Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
Seventh Edition Staging 2017 Melanoma. Overview. This webinar is sponsored by. the Centers for Disease Control and Prevention.
 Seventh Edition Staging 2017 Melanoma Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express written
Seventh Edition Staging 2017 Melanoma Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express written
Your Guide to the Breast Cancer Pathology. Report. Key Questions. Here are important questions to be sure you understand, with your doctor s help:
 Your Guide to the Breast Cancer Pathology Report Key Questions Here are important questions to be sure you understand, with your doctor s help: Your Guide to the Breast Cancer Pathology Report 1. Is this
Your Guide to the Breast Cancer Pathology Report Key Questions Here are important questions to be sure you understand, with your doctor s help: Your Guide to the Breast Cancer Pathology Report 1. Is this
Instructions for Coding Grade for 2014+
 Instructions for Coding for 2014+ GRADE, DIFFERENTIATION OR CELL INDICATOR Item Length: 1 NAACCR Item #: 440 NAACCR Name:, Differentiation for solid tumors (Codes 1, 2, 3, 4, 9) and Cell Indicator for
Instructions for Coding for 2014+ GRADE, DIFFERENTIATION OR CELL INDICATOR Item Length: 1 NAACCR Item #: 440 NAACCR Name:, Differentiation for solid tumors (Codes 1, 2, 3, 4, 9) and Cell Indicator for
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ]
![Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ]](/thumbs/71/65936251.jpg "Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ]") MelanomaSkin CS Tumor Size Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ] Code 000 No mass/tumor found Description 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters
MelanomaSkin CS Tumor Size Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ] Code 000 No mass/tumor found Description 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters
Gene Expression Profiling for Managing Breast Cancer Treatment. Policy Specific Section: Medical Necessity and Investigational / Experimental
 Medical Policy Gene Expression Profiling for Managing Breast Cancer Treatment Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Laboratory/Pathology Original Policy Date:
Medical Policy Gene Expression Profiling for Managing Breast Cancer Treatment Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Laboratory/Pathology Original Policy Date:
Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do?
 Exercise 1 Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do? : 1. I mention both categories that are in consideration, e.g. pt1-2 2. I classify as
Exercise 1 Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do? : 1. I mention both categories that are in consideration, e.g. pt1-2 2. I classify as
FISH mcgh Karyotyping ISH RT-PCR. Expression arrays RNA. Tissue microarrays Protein arrays MS. Protein IHC
 Classification of Breast Cancer in the Molecular Era Susan J. Done University Health Network, Toronto Why classify? Prognosis Prediction of response to therapy Pathogenesis Invasive breast cancer can have
Classification of Breast Cancer in the Molecular Era Susan J. Done University Health Network, Toronto Why classify? Prognosis Prediction of response to therapy Pathogenesis Invasive breast cancer can have