GASTRIC CANCER DR AMIR ASHRAFI
|
|
|
- Karin Chambers
- 5 years ago
- Views:
Transcription

1 GASTRIC CANCER DR AMIR ASHRAFI
2 Epidemiology Aetiologic factors Classification Clinical features Investigations Staging Treatment
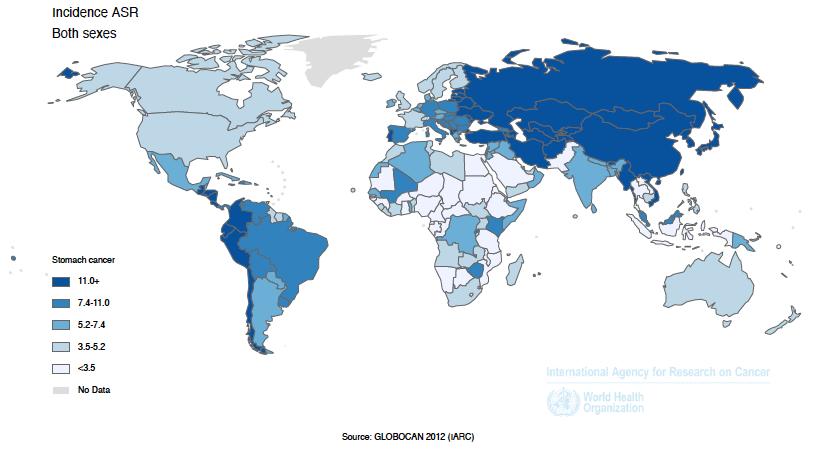
3 EPIDEMIOLOGY AND FACTS ü Worldwide, gastric cancer is the fourth most common cancer and the second leading cause of cancer death. ü It is especially prevalent in East Asia and South America and has been increasing in developing countries, which now have almost two thirds of all distal gastric cancer cases. ü Among developed countries, Japan and Korea have the highest rates of the disease. Gastric cancer is the most common cancer in Japan but mortality dropped 50% with screening in 1970s. ü In 2010, there were 1,999 new cases of stomach cancer in Australia (1,314 new cases in men and 685 new cases in women), accounting for 1.7 per cent of all new cancers ü Stomach cancer is more common in men: In 2010, 11.9 cases per 100,000 men, compared with 5.2 cases per 100,000 women. ü It is a disease of older individuals, with peak incidence in the seventh decade of life. ü In 2011, there were 1,140 deaths from stomach cancer (715 men and 425 women), accounting for 2.6 per cent of all cancer deaths in Australia. ü Between the periods and , five-year relative survival increased in Australia from 17.2 % to 26.7%
4
5 WHAT CAUSES GASTRIC CANCER?
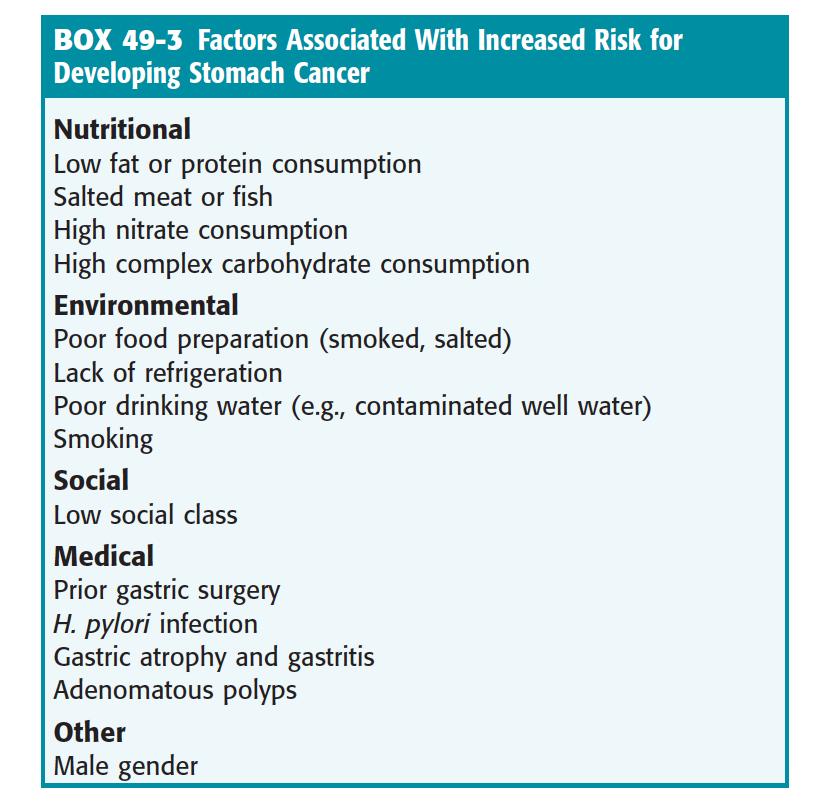
6 FACTORS INCREASING OR DECREASING GASTRIC CA Increase risk Family history Diet (high in nitrates, salt, fat) Familial polyposis Gastric adenomas Hereditary nonpolyposis colorectal cancer Helicobacter pylori infection Atrophic gastritis, intestinal metaplasia, dysplasia Previous gastrectomy or gastrojejunostomy (>10 y ago) Tobacco use Ménétrier s disease Blood Group A Decrease risk Aspirin Diet (high fresh fruit and vegetable intake) Vitamin C
7 GASTRIC CANCER GENETIC MUTATIONS Deletion or suppression of p53 Overexpression of COX- 2 CDH1
8

9 H. PYLORI AND GASTRIC CA The presence of the cytoxan-associated gene A (caga) is associated with increased virulence and risk of gastric cancer. Countries with high levels of gastric cancer, such as Japan, have a much higher rate of caga-positive H. pylori infection There is likely synergism between diet and H. pylori infection, with the bacteria increasing carcinogen production and inhibiting its removal. H. pylori has been shown to promote the growth of the bacteria that generate the carcinogenic N-nitroso compounds. Patients on long term PPI can colonies H. pylori which leads to corpus gastritis and 1/3 will get atrophic gastritis which is a risk factor for gastric Ca. So they should be monitored for and have eradication of H. Pylori (Still no evidence)
10 CLASSIFICATION
11 BORRMANN CLASSIFICATION SYSTEM (1926)
12 LAUREN CLASSIFICATION SYSTEM (1967) 1. Intestinal: resembles colon cancer, can be polypoid or ulcerated, occurs usually in the distal stomach and has a prolonged pre-cancerous phase. 2. Difusse: Extends widely with no distinct margins and the glandular structure is rarely present. Patients tend to be younger and have a worst prognosis.

13 LAUREN CLASSIFICATION SYSTEM (1967)
14 WHO SYSTEM Adenocarcinoma (papillary, tubular, mucinous, and signet ring) Adenosquamous cell carcinoma Squamous cell carcinoma Undifferentiated carcinoma Unclassified carcinoma
15 DIAGNOSIS approximately 50 percent have disease that extends beyond locoregional confines, and only one-half of those who appear to have locoregional tumor involvement can undergo a potentially curative resection Surgically curable early gastric cancers are usually asymptomatic and only infrequently detected outside the realm of a screening program. Countries with screening program: Japan, Venezuela, and Chile.
16 NON-SPECIFIC CLINICAL FEATURES (FOUND AT AN EARLY STAGE)

17 INDIGESTION, HEARTBURN, BLOATING OF THE STOMACH AFTER MEAL OR VAGUE EPIGASTRIC DISCOMFORT
 WHICH IS NOT RELATED TO FOOD")
18 CONSTANT, NON-RADIATING UPPER ABDOMINAL PAIN (USUALLY NOT SEVERE) WHICH IS NOT RELATED TO FOOD INTAKE




19 WEIGHT LOSS WEAKNESS AND FATIGUE LOSS OF APPETITE EARLY SATIETY
20 CLINICAL FEATURES
21 Occult GI bleeding with or without IDA is common overt bleeding (melena or hematemesis) is seen in less than 20 percent of cases. Pseudoachalasia syndrome: may occur as the result of involvement of Auerbach's plexus due to local extension or to malignant obstruction near the gastroesophageal junction. So in older patients coming with Achalasia think of Gastric Cancer 25 % of patients have a history of gastric ulcer. All gastric ulcers should be followed to complete healing, and those that do not heal should undergo resection
22 METASTATIC DISTRIBUTION Common sites: liver Peritoneal surfaces Non-regional or distant lymph nodes. Less commonly: ovaries central nervous system bone pulmonary soft tissue


23 LYMPHATIC SPREAD - left supraclavicular adenopathy (a Virchow's node or signal node ) - Left Anterior Axillary node (Irish node)

24 Rudolph Virchow

25 - Periumblical nodule (Sister Mary Joseph s node)
 - mass in the cul-de-sac on")

26 PERITONEAL SPREAD can present with : - enlarged ovary (Krukenberg's tumor) - mass in the cul-de-sac on rectal examination (Blumer's shelf) - Ascites can also be the first indication of - peritoneal carcinomatosis.
27 Liver: - A palpable liver mass can indicate metastases, but metastatic disease to the liver is often multifocal or diffuse. - Liver involvement is often, but not always, associated with an elevation in ALP. - Jaundice or clinical evidence of liver failure is seen in the preterminal stages of metastatic disease.



28 PARANEOPLASTIC MANIFESTATIONS sudden appearance of diffuse seborrheic keratoses (sign of Leser-Trelat) Acnathosis Nigricancs microangiopathic hemolytic anemia hypercoagulable states Polyarteritis nodosa (single manifestation of an early and surgically curable gastric cancer)
29 DIAGNOSTIC MODALITIES v Endoscopy v Barium Studies v Endoscopic Ultrasound (EUS) v CT Abdo/Pelvis v Tumor Markers v PET/CT v Laparoscopy
30 ENDOSCOPY 5 % of malignant ulcers appear benign grossly A single biopsy has a 70% sensitivity Seven biopsies from the ulcer margin and base: >98% Sensitive (Prospective evaluation of biopsy number in the diagnosis of esophageal and gastric carcinoma. Graham DY, at al, Gastroenterology. 1982;82(2):228.) Linitis Plastica (5% of cases) is difficult to diagnose endoscopically and superficial biopsies will be negative
31
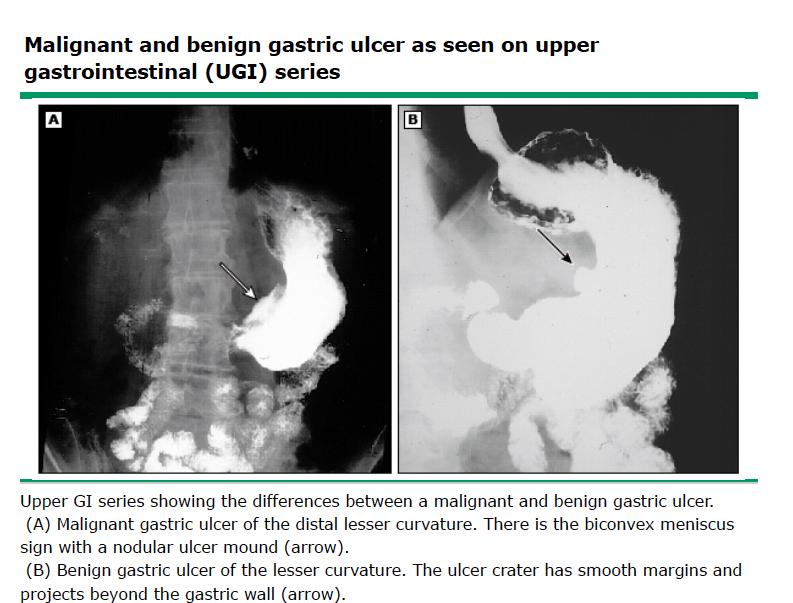
32 BARIUM STUDIES can identify both malignant gastric ulcers and infiltrating lesions 50% False negative sensitivity of barium meals as low as 14 percent in early stages
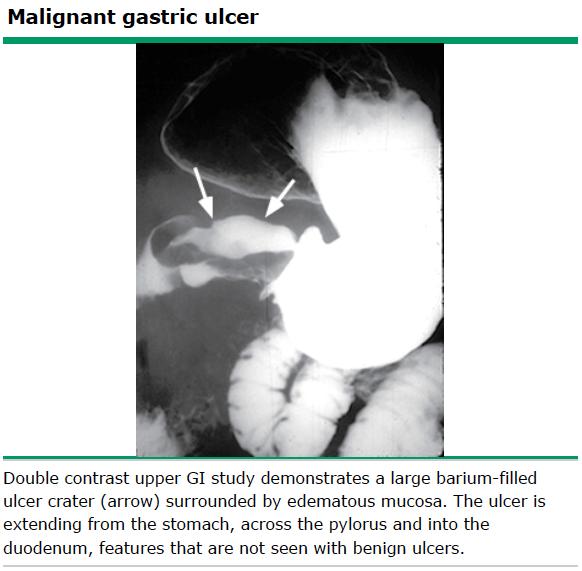
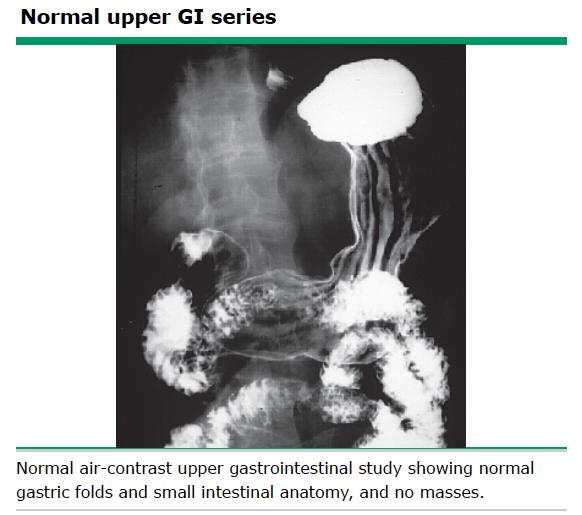
33

34 BARIUM STUDIES Superior to upper endoscopy in patients linitis plastica. decreased distensibility of the stiff, "leather-flask" appearing stomach is more obvious on the radiographic study, and the endoscopic appearance may be relatively normal
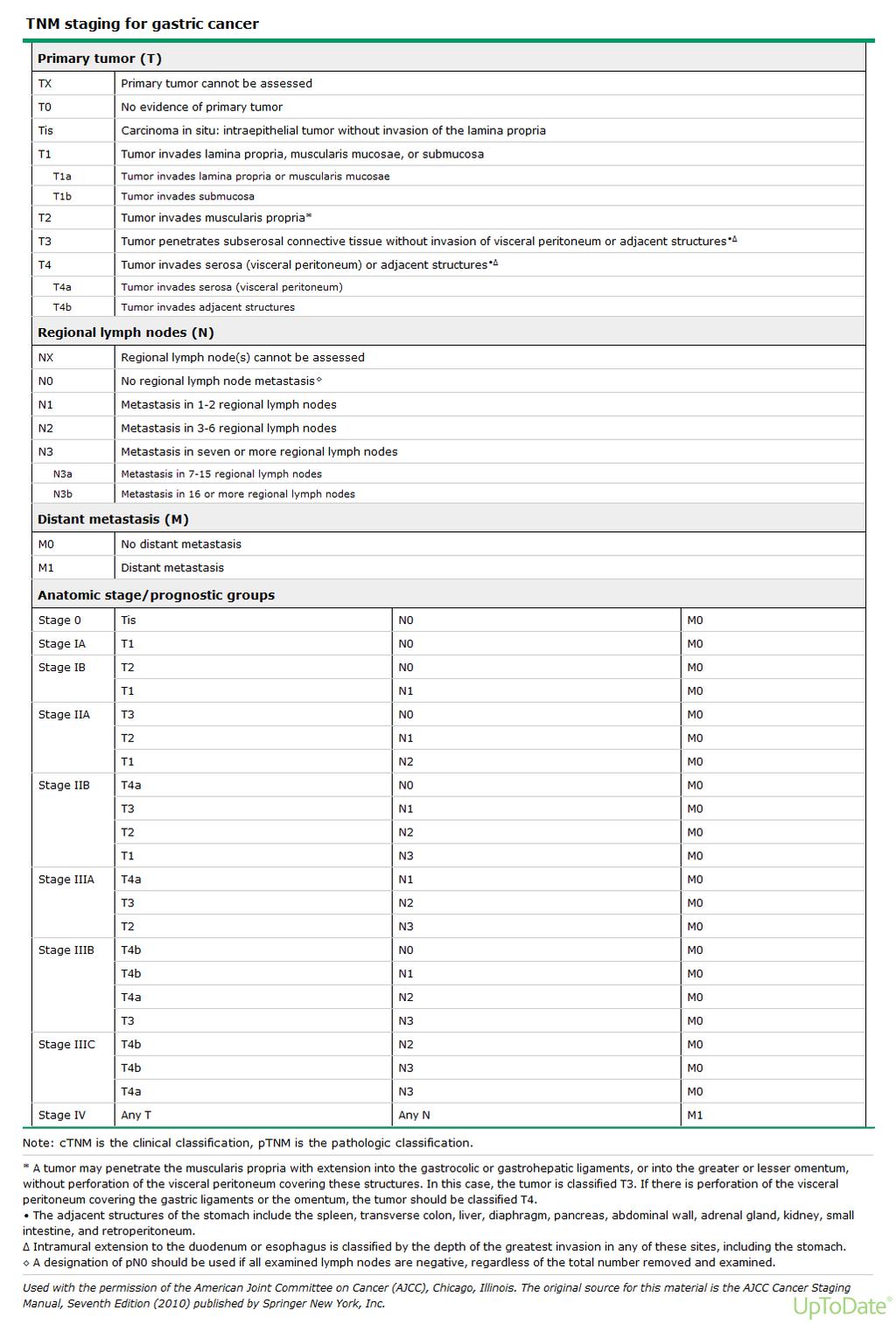
35 STAGING SYSTEMS Japanese classification: based upon refined anatomic location, particularly of the lymph node stations TMN: The staging schema of the AJCC/UICC is based upon tumor (T), node (N), and metastasis (M) classifications T stage is dependent on depth of tumor invasion and not size. Nodal stage is based upon the number of positive lymph nodes rather than the proximity of the nodes to the primary tumor
36 GASTRIC CANCER TNM STAGING Tis T1 T2 T3 T4 Intaepithelial tumour Tumour invades LP or submucosa Tumour invades muscularis propria or subserosa Tumour penetrates serosa without invasion of adjacent structures Tumour invades adjacent structures
37
38 GASTRIC CANCER TNM STAGING N0 N1 N2 N3 No regional lymph node metastases Metastasis in 1 to 6 regional lymph nodes Metastasis in 7 to 15 regional lymph nodes Metastasis in more than 15 regional lymph nodes
39 GASTRIC CANCER TNM STAGING M0 M1 No distant metastasis Distant metastasis
40
41
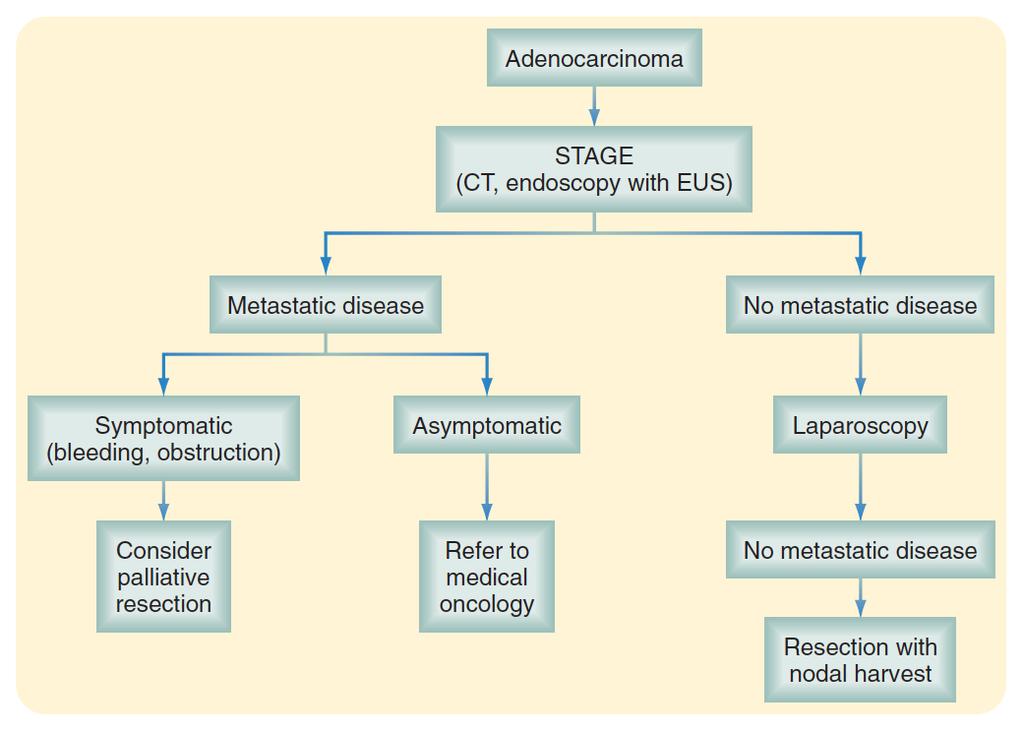
42 CLINICAL STAGING AND THE SELECTION OF TREATMENT locoregional disease (stage I to III) after preoperative testing are potentially curable All patients with a primary tumor that is considered to invade through the submucosa (T2 or higher) or with a high suspicion of nodal involvement on pretreatment staging studies should be referred for multidisciplinary evaluation to identify the best treatment strategy. Patients with advanced stage IV disease are usually referred for palliative therapy depending on their symptoms and functional status.
43 PREOPERATIVE EVALUATION Indicators of unresectability: Ø distant metastases Ø invasion of a major vascular structure, such as the aorta, disease encasement or occlusion of the hepatic artery or celiac axis/proximal splenic artery. Ø Distal splenic artery involvement is not an indicator of unresectability; the vessel can be resected en bloc with a left upper quadrant exenteration: stomach, spleen and distal pancreas.
44 PREOPERATIVE EVALUATION Patients who have bulky adenopathy fixed to the pancreatic head that might indicate the need for a Whipple procedure are at a high risk for occult metastatic disease. In these cases, it is probably best to consider staging laparoscopy or upfront chemotherapy or combined modality therapy rather than surgery initially. (Performance of a Whipple for gastric cancer is an extremely rare occurrence.) Linitis plastica has an extremely poor prognosis, and many surgeons consider its presence to be a contraindication to potentially curative resection.
45 ABDOMINOPELVIC CT SCAN performed early in the preoperative evaluation after the diagnosis of Gastric Ca hepatic or adnexal metastases, ascites, or distant nodal spread can be identified and unnecessary surgery avoided Peritoneal metastases and hematogenous metastases smaller than 5 mm are frequently missed by CT negative CT : 20 to 30 % of chance of intraperitoneal disease to be found at either staging laparoscopy or at open exploration CT accuracy in T stage of the primary tumor : only 50 to 70 % for regional nodal metastases: sensitivity 65 to 97 %, and specificity 49 to 90 %
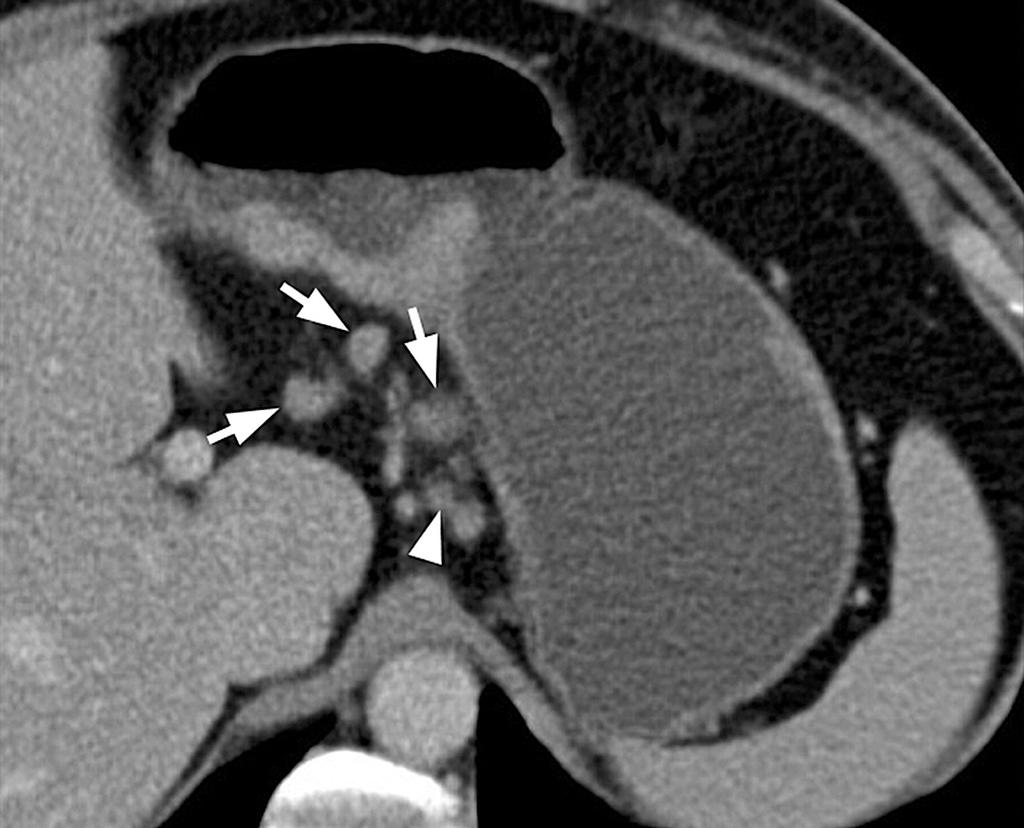
46
47 ENDOSCOPIC ULTRASONOGRAPHY most reliable nonsurgical method available for evaluating the depth of invasion of primary gastric cancers, particularly for early (T1) lesions The accuracy of EUS for differentiation of individual tumor stages (T1 to T4) ranges from 77 to 93 percent depending on the operator experience newer CT techniques (such as three-dimensional multidetector row CT) and MRI may achieve similar results in terms of diagnostic accuracy in T staging accuracy for nodal staging (65 to 90 %) is only slightly greater with EUS as compared to CT Neoadjuvant chemotherapy or chemoradiotherapy may be recommended for patients with a primary tumor that is considered to invade into the muscularis propria (T2 or higher) or with a high suspicion of nodal involvement on pretreatment staging studies. EUS is also of value for patients with early gastric cancer because accurate assessment of submucosal invasion is essential before considering the option of endoscopic mucosal resection.
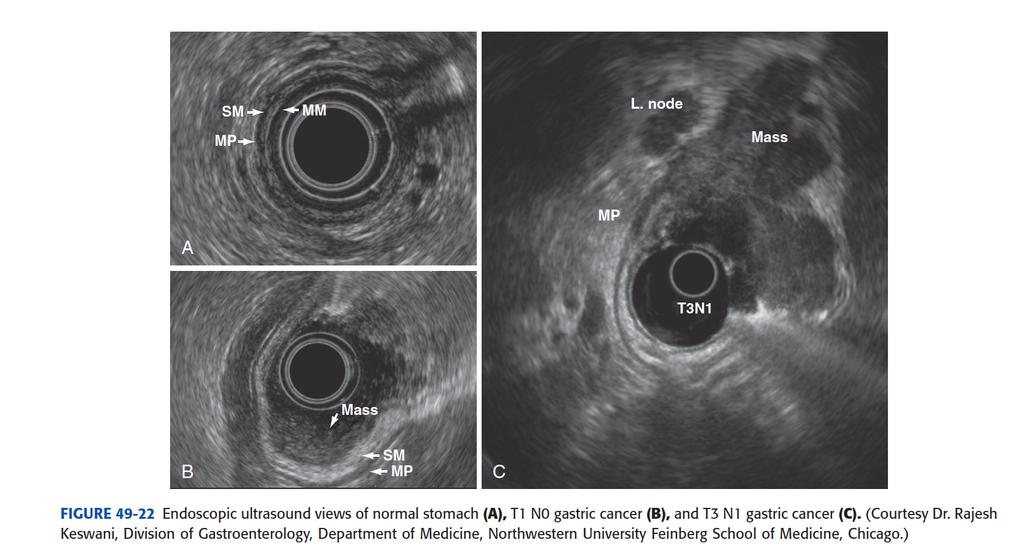
48
49 PET SCAN PET/CT imaging can be useful to confirm malignant involvement of CT-detected lymphadenopathy a negative PET is not helpful since even large tumors with a diameter of several centimeters can be falsely negative if the tumor cells have a fairly low metabolic activity most diffuse type gastric cancers (signet ring carcinomas) are not FDG avid The main benefit of PET is that it is more sensitive than CT for the detection of distant metastases sensitivity of PET scanning for peritoneal carcinomatosis is only approximately 50 percent so cant replace staging laparoscopy PET response to neoadjuvant therapy strongly correlates with survival, with PET response seen within 14 days of treatment. PET may be an effective modality for monitoring response to these therapies, sparing unresponsive patients further toxic treatment
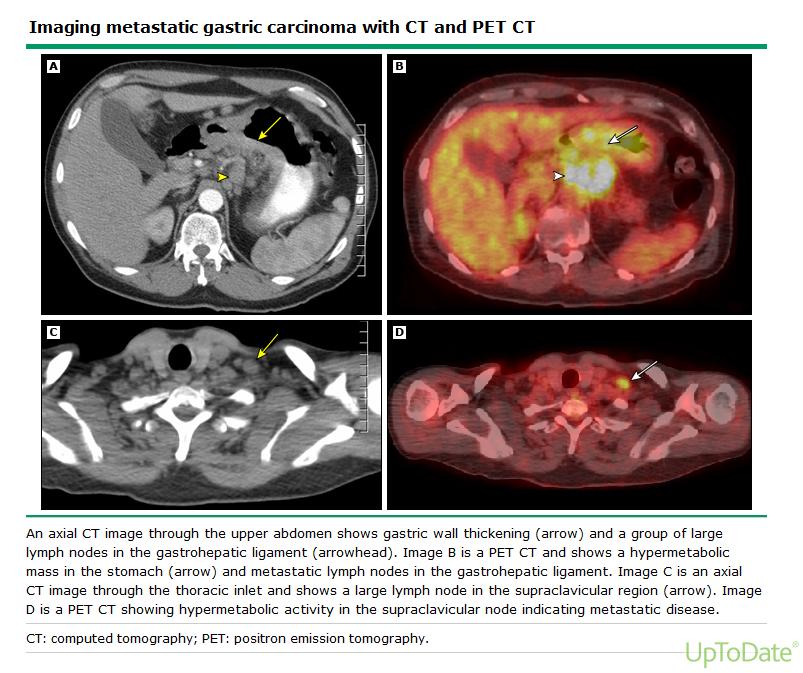
50
51 SEROLOGIC MARKERS CEA CA 125 CA 19 9 CA 72 4 AFP (Hepatoid Adenocarcinomas of the stomach, poor prognosis) a drop in an elevated level of CEA and/or CA 125 may correlate with response to preoperative therapy,
52 STAGING LAPAROSCOPY 20 and 30 % of patients with T1 and above on EUS will be found to have peritoneal metastases despite having a negative CT scan 50% of T3-4 Gastric Ca will avoid unnecessary laparotomy opportunity to perform peritoneal cytology in patients who have no visible evidence of peritoneal spread (predicts for early peritoneal relapse) avoiding laparotomy also means avoiding a delay in starting chemotherapy for patients with metastatic disease and limited life expectancy Many centers do it as a routine for the workup for most Gastric Ca patients and can be planned as a single stage procedure as resection
53 SUMMARY OF DIAGNOSTIC RECOMMENDATION Abdominopelvic CT scan is indicated to look for metastatic disease (M stage); it should not be relied upon for assessing T / N staging or the presence of peritoneal metastases. Suspicious visceral lesions require biopsy confirmation. Paracentesis for cytology should be performed when ascites is detected A preoperative chest x-ray is recommended; chest CT scan is preferred (particularly for patients with a proximal gastric cancer Endoscopic ultrasound (EUS) is better than CT at assessing tumor depth (T stage) and perhaps lymph node involvement (N stage), particularly if fine-needle aspiration is also performed.
54 SUMMARY OF DIAGNOSTIC RECOMMENDATION If the radiographic staging evaluation is otherwise negative for metastatic disease, integrated PET/CT is a reasonable addition to the preoperative staging evaluation for patients with T2N0 disease, mainly to screen for distant metastases. As with CT, suspicious visceral lesions warrant biopsy. Serum tumor markers (including CEA and CA 125) are of limited utility, and we do not routinely assay for them, unless a patient is undergoing neoadjuvant therapy. staging laparoscopy is indicated in all medically fit patients > T1 lesion on EUS, no histologic confirmation of stage IV disease, (and who would not otherwise require a palliative gastrectomy) Diagnostic laparoscopy should also be undertaken in patients who are being considered for neoadjuvant therapy.
55
56 SURGICAL MARGINS Subtotal vs. Total Gastrectomy? Factors Influencing Operation Extent of disease Histological type Diffuse total gastrectomy Intestinal potentially subtotal gastrectomy Location (for intestinal type) Lower subtotal gastrectomy Mid near-total gastrectomy Upper total gastrectomy < 2 cm of GE junction- Esophagogastrectomy
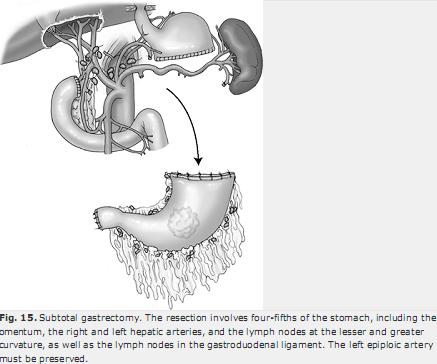
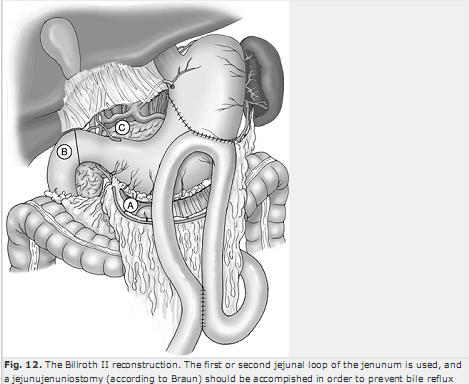
57 SURGICAL THERAPY For cancers of the distal stomach, including the body and antrum, a distal gastrectomy is the appropriate operation. The proximal stomach is transected at the level of the incisura at a margin of at least 6 cm, because studies have documented tumor spread as far as 5 cm laterally from the primary tumor. The distal margin is the proximal duodenum. The possibility of recurrence in the tumor bed (duodenal suture line and surface of the pancreas) suggest a Billroth II reconstruction rather than a Billroth I, which will result in less risk of gastric outlet obstruction secondary to tumor recurrence.
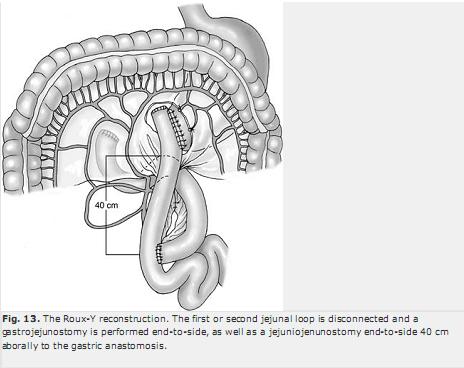
58 SURGICAL THERAPY For proximal lesions of the fundus or cardia, a total gastrectomy with a Roux-en-Y esophagojejunostomy or proximal gastrectomy is equivalent from an oncologic perspective. The postoperative anastomotic leak rate is higher for an esophagojejunostomy, but the margin will typically be larger than for a gastrojejunostomy Laparoscopy has the same 5 yr survival as open but shorter time to start feeding and earlier DC from hospital
59
60
61
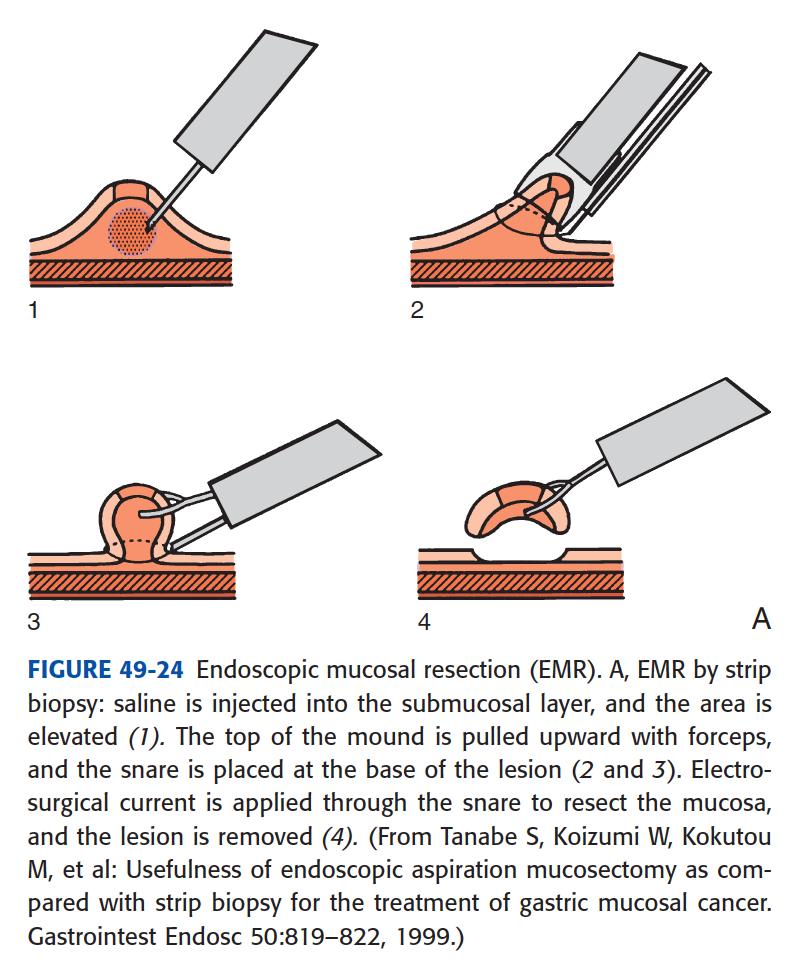
62 ENDOSCOPIC MUCOSAL RESECTION For early gastric cancer with limited penetration of the gastric wall and no evidence of lymph node metastases, purely endoscopic mucosal resection Widely practiced in Japan no randomized controlled trials comparing endoscopic mucosal resection with gastrectomy for early gastric cancer If no lymphatic vessel invasion, histologic ulceration of the tumor, and or larger size ( 30 mm) there is only 0.36% chance of Lymph node mets
63 GENERAL GUIDELINES FOR ENDOSCOPIC RESECTION OF EARLY GASTRIC CANCER Based on these data, the are as follows: (1) tumor limited to the mucosa; (2) no lymphovascular invasion; (3) tumor smaller than 2 cm; and (4) no ulceration.
64
65 RECURRENCE 40% to 80%, recurrence rate after gastrectomy Most recurrences occur within the first 3 years Isolated distant metastases are uncommon because most patients with distant failure also have locoregional recurrence. The most common sites of locoregional recurrence are the gastric remnant at the anastomosis, in the gastric bed, and in the regional nodes. Hematogenous spread occurs to the liver, lung, and bone.
66 FOLLOW-UP complete history and physical examination every 4 months for 1 year every 6 months for 2 years, and then annually thereafter. Laboratory tests: FBC, LFTs as clinically indicated. Many clinicians obtain chest x-rays and CT scans of the abdomen and pelvis routinely, whereas others obtain studies only when clinically suspicious of a recurrence. Annual endoscopy should be considered for patients who have undergone a subtotal gastrectomy.
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Gastric Cancer: Surgery and Regional Therapy. Epidemiology. Risk factors
 Gastric Cancer: Surgery and Regional Therapy Timothy J. Kennedy, MD Montefiore Medical Center Assistant Professor of Surgery Upper Gastrointestinal and Pancreas Surgery December 15, 2012 1 Epidemiology
Gastric Cancer: Surgery and Regional Therapy Timothy J. Kennedy, MD Montefiore Medical Center Assistant Professor of Surgery Upper Gastrointestinal and Pancreas Surgery December 15, 2012 1 Epidemiology
Gastric Cancer in a Young Postpartum Female. Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012
 Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Gastrointestinal Tract Cancer
 Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Gastric Tumors Dr. Taha
 Gastric Tumors Dr. Taha BENIGN TUMORS: Leiomyomas: smooth muscle tumors, equal in men /women, typically located in the middle &distal stomach. Can grow into the lumen with secondary ulceration & bleeding.
Gastric Tumors Dr. Taha BENIGN TUMORS: Leiomyomas: smooth muscle tumors, equal in men /women, typically located in the middle &distal stomach. Can grow into the lumen with secondary ulceration & bleeding.
By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ.
 Professor of Surgery, Taibah Univ.") By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ. Objectives Types Incidence Risk factors (& prevention) Pathology: Gross, microscopic, spread, staging,
By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ. Objectives Types Incidence Risk factors (& prevention) Pathology: Gross, microscopic, spread, staging,
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
GASTRIC CANCER. Joyce Au SUNY Downstate Grand Rounds July 11, 2013
 GASTRIC CANCER Joyce Au SUNY Downstate Grand Rounds July 11, 2013 xxm with gastric adenocarcinoma on biopsy of antral lesion on EGD at outside hospital PMH: residual schizophrenia, HTN PSH: exploratory
GASTRIC CANCER Joyce Au SUNY Downstate Grand Rounds July 11, 2013 xxm with gastric adenocarcinoma on biopsy of antral lesion on EGD at outside hospital PMH: residual schizophrenia, HTN PSH: exploratory
CT EVALUATION OF GASTRIC LESIONS:
 CT EVALUATION OF GASTRIC LESIONS: Pictural essay Hasni Bouraoui I, Kahloun A, Jemni H, Elouni F, Moulahi H, Daadoucha A, Ben Ali A, Sriha B, Tlili Graies K Departments of Radiology, Gastro enterology,
CT EVALUATION OF GASTRIC LESIONS: Pictural essay Hasni Bouraoui I, Kahloun A, Jemni H, Elouni F, Moulahi H, Daadoucha A, Ben Ali A, Sriha B, Tlili Graies K Departments of Radiology, Gastro enterology,
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Gastric Cancer Staging AJCC eighth edition. Duncan McLeod Westmead Hospital, NSW
 Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 Final Pathology:
 Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Patient. Male 76 year old C.C: abdominal pain
 Patient Male 76 year old C.C: abdominal pain Bowel stool retention Suspected pulmonary TB at right upper lung Infiltration in right lower lung Pleural thickening at the Right chest Localized dilated small
Patient Male 76 year old C.C: abdominal pain Bowel stool retention Suspected pulmonary TB at right upper lung Infiltration in right lower lung Pleural thickening at the Right chest Localized dilated small
Birthday: 1952/07/31 Date of admission:1999/12/30 Age:48 y/o Past medication:esrd under regular HD for 5+ years; denied DM and HTN
 Birthday: 1952/07/31 Date of admission:1999/12/30 Age:48 y/o Past medication:esrd under regular HD for 5+ years; denied DM and HTN Chief Complaint : 1)intermittent LLQ cramping pain for 2 months 2) LGI
Birthday: 1952/07/31 Date of admission:1999/12/30 Age:48 y/o Past medication:esrd under regular HD for 5+ years; denied DM and HTN Chief Complaint : 1)intermittent LLQ cramping pain for 2 months 2) LGI
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS
 COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
سرطان المعدة. Gastric Cancer حمود حامد
 سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
Polyps in general: is a descriptive term of forming a mass that is exophytic & polypoid.
 ميحرلا نمحرلا هللا مسب Gastric Tumors: Benign tumours & tumor-like conditions: -Mucosal: Gastric polyps (they are uncommon) -Mesenchymal tumours: Leiomyoma & Lipoma (can occur anywhere in the body) Malignant:
ميحرلا نمحرلا هللا مسب Gastric Tumors: Benign tumours & tumor-like conditions: -Mucosal: Gastric polyps (they are uncommon) -Mesenchymal tumours: Leiomyoma & Lipoma (can occur anywhere in the body) Malignant:
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD
 Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012
 Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Gastric (Stomach) Cancer
 Cancer") Gastric (Stomach) Cancer Gastric cancer is a disease in which malignant (cancer) cells form in the lining of the stomach. The stomach is a J-shaped organ in the upper abdomen. It is part of the digestive
Gastric (Stomach) Cancer Gastric cancer is a disease in which malignant (cancer) cells form in the lining of the stomach. The stomach is a J-shaped organ in the upper abdomen. It is part of the digestive
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
SMALL BOWEL ADENOCARCINOMA. Dr. C. Jeske
 SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer
 Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer Locoregional (N stage) disease was redefined in the seventh edition of the AJCC Cancer Staging Manual as any periesophageal lymph
Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer Locoregional (N stage) disease was redefined in the seventh edition of the AJCC Cancer Staging Manual as any periesophageal lymph
SURGICAL MANAGEMENT OF GASTRIC CANCER
 SURGICAL MANAGEMENT OF GASTRIC CANCER Irina Kovatch, PGY 4 Kings County Medical Center Morbidity and Mortality January 13, 2011 Case Presentation 60 yo M admitted to medicine on 10/24/2010 with c/o persistent
SURGICAL MANAGEMENT OF GASTRIC CANCER Irina Kovatch, PGY 4 Kings County Medical Center Morbidity and Mortality January 13, 2011 Case Presentation 60 yo M admitted to medicine on 10/24/2010 with c/o persistent
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY GASTRIC CARCINOMA E PANIERI G CHINNERY B ROBERTSON INTRODUCTION Gastric neoplasms are common, and because they often present late, they arefrequently incurable.
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY GASTRIC CARCINOMA E PANIERI G CHINNERY B ROBERTSON INTRODUCTION Gastric neoplasms are common, and because they often present late, they arefrequently incurable.
SETTING Fudan University Shanghai Cancer Center. RESPONSIBLE PARTY Haiquan Chen MD.
 OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
Navigators Lead the Way
 RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
GASTROINTESTINAL MALIGNANCIES
 Outline GASTROINTESTINAL MALIGNANCIES Bassel F. El-Rayes Winship Cancer Institute Emory University Colorectal Cancer Pancreas Cancer Gastric Cancer Hepatobiliary Cancer Anal Cancer Introduction Epidemiology
Outline GASTROINTESTINAL MALIGNANCIES Bassel F. El-Rayes Winship Cancer Institute Emory University Colorectal Cancer Pancreas Cancer Gastric Cancer Hepatobiliary Cancer Anal Cancer Introduction Epidemiology
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
The surface mucous cells and the cardiac and pyloric glands secrete mucus which protects the stomach from self-digestion.
 PATHOLOGY OF THE STOMACH Stomach mucosa Gastric mucosa is covered by a layer of mucus. The mucosal glands comprise the cardiac glands, the fundic glands in the fundus and body of the stomach, and the pyloric
PATHOLOGY OF THE STOMACH Stomach mucosa Gastric mucosa is covered by a layer of mucus. The mucosal glands comprise the cardiac glands, the fundic glands in the fundus and body of the stomach, and the pyloric
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
B Breast cancer, managing risk of lobular, in hereditary diffuse gastric cancer, 51
 Index Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, gastric. See also Gastric cancer. D2 nodal dissection for 57 70 Adjuvant therapy, for gastric cancer, impact of D2 dissection
Index Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, gastric. See also Gastric cancer. D2 nodal dissection for 57 70 Adjuvant therapy, for gastric cancer, impact of D2 dissection
A218 : Esophagus cancer tissues. (formalin fixed)
") (formalin fixed) For research use only Specifications: No. of cases: 40 Tissue type: Esophagus cancer tissues No. of spots: 2 spots from each cancer case (80 spots) 4 non-neoplastic spots (4 spots) Total
(formalin fixed) For research use only Specifications: No. of cases: 40 Tissue type: Esophagus cancer tissues No. of spots: 2 spots from each cancer case (80 spots) 4 non-neoplastic spots (4 spots) Total
Cancer of the Stomach
 Cancer of the Stomach Review of Consecutive Ten Year Intervals KENNETH ADASHEK, M.D.,* JAMES SANGER, M.D.,t WILLIAM P. LONGMIRE, JR., M.D.* Records were reviewed for all patients who underwent primary
Cancer of the Stomach Review of Consecutive Ten Year Intervals KENNETH ADASHEK, M.D.,* JAMES SANGER, M.D.,t WILLIAM P. LONGMIRE, JR., M.D.* Records were reviewed for all patients who underwent primary
We are IntechOpen, the first native scientific publisher of Open Access books. International authors and editors. Our authors are among the TOP 1%
 We are IntechOpen, the first native scientific publisher of Open Access books 3,350 108,000 1.7 M Open access books available International authors and editors Downloads Our authors are among the 151 Countries
We are IntechOpen, the first native scientific publisher of Open Access books 3,350 108,000 1.7 M Open access books available International authors and editors Downloads Our authors are among the 151 Countries
TUMORS OF THE STOMACH AND SMALL BOWEL
 gastrointestinal tract and abdomen TUMORS OF THE STOMACH AND SMALL BOWEL L. Mark Knab, MD, David J. Bentrem, MD, FACS, and Jeffrey D. Wayne, MD, FACS * Gastric Adenocarcinoma The incidence of gastric carcinoma
gastrointestinal tract and abdomen TUMORS OF THE STOMACH AND SMALL BOWEL L. Mark Knab, MD, David J. Bentrem, MD, FACS, and Jeffrey D. Wayne, MD, FACS * Gastric Adenocarcinoma The incidence of gastric carcinoma
Approaches to Surgical Treatment of Gastric Cancer. Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service
 Approaches to Surgical Treatment of Gastric Cancer Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service Disclosures I do not have anything to disclose Outline Background Diagnosis Histology Staging Surgery
Approaches to Surgical Treatment of Gastric Cancer Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service Disclosures I do not have anything to disclose Outline Background Diagnosis Histology Staging Surgery
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours?
 Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Esophageal cancer: Biology, natural history, staging and therapeutic options
 EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM
 OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
General Data. Gender : Male Birthday and age : 12/07/24,80 y/o Occupation : 無 Date of Admission :
 General Data Gender : Male Birthday and age : 12/07/24,80 y/o Occupation : 無 Date of Admission : 92-07-09 1 Chief complaint Upper abdominal fullness 30 minutes after having foods with sometimes epigastralgia
General Data Gender : Male Birthday and age : 12/07/24,80 y/o Occupation : 無 Date of Admission : 92-07-09 1 Chief complaint Upper abdominal fullness 30 minutes after having foods with sometimes epigastralgia
How to recognize them. H. Vahedi MD Gastroenterologist Associate Professor of Medicine DDRI
 Gastrointestinal Cancers: How to recognize them H. Vahedi MD Gastroenterologist Associate Professor of Medicine DDRI The GI tract, including the: -hollow organs of the gut -and pancreas, liver -and biliary
Gastrointestinal Cancers: How to recognize them H. Vahedi MD Gastroenterologist Associate Professor of Medicine DDRI The GI tract, including the: -hollow organs of the gut -and pancreas, liver -and biliary
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID
 ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
 Hindawi Publishing Corporation Journal of Oncology Volume 2008, Article ID 212067, 5 pages doi:10.1155/2008/212067 Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
Hindawi Publishing Corporation Journal of Oncology Volume 2008, Article ID 212067, 5 pages doi:10.1155/2008/212067 Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R
 Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012
 Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers
 Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
PANCREAS DUCTAL ADENOCARCINOMA PDAC
 CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
Gastric and Colon Cancer. Dr. Andres Wiernik 2017
 Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Imaging techniques in the diagnosis, staging and follow up of GI cancers. Moderators: Banke Agarwal, MD and Paul Schultz, MD
 Imaging techniques in the diagnosis, staging and follow up of GI cancers Moderators: Banke Agarwal, MD and Paul Schultz, MD Panelists Axel Grothey, MD Professor of Oncology Division of Medical Oncology
Imaging techniques in the diagnosis, staging and follow up of GI cancers Moderators: Banke Agarwal, MD and Paul Schultz, MD Panelists Axel Grothey, MD Professor of Oncology Division of Medical Oncology
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Mediastinal Staging. Samer Kanaan, M.D.
 Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Peptic ulcer disease. Nomin-Erdene. D SOM-531
 Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
7/20/2017. Esophageal Cancer: A Less Common But Deadly Cancer. Objectives. Disclosure Statement NYNPA Conference October Saratoga New York
 Esophageal Cancer: A Less Common But Deadly Cancer 2017 NYNPA Conference October 18-22 Saratoga New York Mary McGreal DNP, RN, ANP-C, CCRN, CMC, Adjunct Professor at Stony Brook University School of Nursing
Esophageal Cancer: A Less Common But Deadly Cancer 2017 NYNPA Conference October 18-22 Saratoga New York Mary McGreal DNP, RN, ANP-C, CCRN, CMC, Adjunct Professor at Stony Brook University School of Nursing
Alison Douglass Gillian Lieberman, MD. November. Colon Cancer. Alison Douglass, Harvard Medical School Year III Gillian Lieberman, MD
 November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
Afternoon Session Cases
 Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Esophageal Cancer. What is esophageal cancer?
 Scan for mobile link. Esophageal Cancer Esophageal cancer occurs when cancer cells develop in the esophagus. The two main types are squamous cell carcinoma and adenocarcinoma. Esophageal cancer may not
Scan for mobile link. Esophageal Cancer Esophageal cancer occurs when cancer cells develop in the esophagus. The two main types are squamous cell carcinoma and adenocarcinoma. Esophageal cancer may not
A superficial radiotherapy B single pass curettage C excision with 2 mm margins D excision with 5 mm margins E Mohs micrographic surgery.
 1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
COLORECTAL CANCER STAGING in 2010
 COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
Gastric and GE Junction Cancer: Epidemiology and Clinical Presentation
 Gastric and GE Junction Cancer: Epidemiology and Clinical Presentation ESMO Preceptorship Programme Gastrointestinal Tumours Singapore 20-22 November, 2018 Dr. Cheng Ean CHEE Consultant Medical Oncologist
Gastric and GE Junction Cancer: Epidemiology and Clinical Presentation ESMO Preceptorship Programme Gastrointestinal Tumours Singapore 20-22 November, 2018 Dr. Cheng Ean CHEE Consultant Medical Oncologist
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Esophageal Cancer Staging Essentials: The New TNM Staging System (7th edition) and Clinicoradiologic Implications
 and Clinicoradiologic Implications") Esophageal Cancer Staging Essentials: The New TNM Staging System (7th edition) and Clinicoradiologic Implications Poster No.: E-0060 Congress: ESTI 2012 Type: Scientific Exhibit Authors: K. Lee, T. J.
Esophageal Cancer Staging Essentials: The New TNM Staging System (7th edition) and Clinicoradiologic Implications Poster No.: E-0060 Congress: ESTI 2012 Type: Scientific Exhibit Authors: K. Lee, T. J.
위 ESD 후내시경소견 성균관대학교의과대학내과이준행
 위 ESD 후내시경소견 성균관대학교의과대학내과이준행 문제의식 위궤양, 조기위암, 진행위암의내시경소견은배운다. 위암수술후소견은가끔배운다. 위암내시경시술후소견은배운적이없다. 관찰과조직검사에대한가이드라인이없다. ESD 후정상내시경소견 성균관대학교의과대학내과이준행 처음의뢰되었을때의사진 ESD M/D, 18mm, LP, RM (-), L/V (-) 추적내시경소견 2
위 ESD 후내시경소견 성균관대학교의과대학내과이준행 문제의식 위궤양, 조기위암, 진행위암의내시경소견은배운다. 위암수술후소견은가끔배운다. 위암내시경시술후소견은배운적이없다. 관찰과조직검사에대한가이드라인이없다. ESD 후정상내시경소견 성균관대학교의과대학내과이준행 처음의뢰되었을때의사진 ESD M/D, 18mm, LP, RM (-), L/V (-) 추적내시경소견 2
International Journal of Medical Science and Health Research
 A Retrospective Study of Clinicopathological Profiles of Proximal Gastrectomy Vs Distal Gastrectomy in Carcinoma Stomach and Its Incidence in our Population Dr Magesh kumar J 1, Dr V Naveen Kumar 2, Dr
A Retrospective Study of Clinicopathological Profiles of Proximal Gastrectomy Vs Distal Gastrectomy in Carcinoma Stomach and Its Incidence in our Population Dr Magesh kumar J 1, Dr V Naveen Kumar 2, Dr
PANCREATIC CANCER GUIDELINES
 PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Totally laparoscopic distal gastrectomy reconstructed by Rouxen-Y with D2 lymphadenectomy and needle catheter jejunostomy for gastric cancer
 Masters of Gastrointestinal Surgery Totally laparoscopic distal gastrectomy reconstructed by Rouxen-Y with D2 lymphadenectomy and needle catheter jejunostomy for gastric cancer Xin Ye, Jian-Chun Yu, Wei-Ming
Masters of Gastrointestinal Surgery Totally laparoscopic distal gastrectomy reconstructed by Rouxen-Y with D2 lymphadenectomy and needle catheter jejunostomy for gastric cancer Xin Ye, Jian-Chun Yu, Wei-Ming
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015
: Imaging Guidelines September 2015") Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci. Colon polyps. Colorectal cancer
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Satisfactory surgical outcome of T2 gastric cancer after modified D2 lymphadenectomy
 Original Article Satisfactory surgical outcome of T2 gastric cancer after modified D2 lymphadenectomy Shupeng Zhang 1, Liangliang Wu 2, Xiaona Wang 2, Xuewei Ding 2, Han Liang 2 1 Department of General
Original Article Satisfactory surgical outcome of T2 gastric cancer after modified D2 lymphadenectomy Shupeng Zhang 1, Liangliang Wu 2, Xiaona Wang 2, Xuewei Ding 2, Han Liang 2 1 Department of General
Evidence tabel stadiering
 Evidence tabel stadiering Auteurs, T stage Syst Reviews Kwee, 2007 Systematic review Studies included up to aug 2006 Kelly, 2001 Systematic review Studies included from 1991-1996 steekproefgrootte) Included
Evidence tabel stadiering Auteurs, T stage Syst Reviews Kwee, 2007 Systematic review Studies included up to aug 2006 Kelly, 2001 Systematic review Studies included from 1991-1996 steekproefgrootte) Included
FDG PET/CT STAGING OF LUNG CANCER. Dr Shakher Ramdave
 FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
Pre-operative assessment of patients for cytoreduction and HIPEC
 Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer
 SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
Management of Neck Metastasis from Unknown Primary
 Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
North of Scotland Cancer Network Clinical Management Guideline for Carcinoma of the Uterine Cervix
 THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake