Scaling up LTBI Treatment with Short Course Regimens
|
|
|
- Kimberly Cross
- 6 years ago
- Views:
Transcription
1 April 2016 Scaling up LTBI Treatment with Short Course Regimens Carol Dukes Hamilton, MD, MHS Director, Scientific Affairs, FHI 360 Professor of Medicine, Duke University

2 Disclosures past 12 months No financial disclosures Will be discussing off-label use for rifampin for treatment of latent TB infection (LTBI) Investigator/author on 2 referenced studies Sterling et al; N Engl J Med 2011;365: TB Trials Consortium Holland et al; PLoS ONE, vol 6; 2011; e22276 Investigator with the TB Trials Consortium
3 Scaling Up Treatment of LTBI Objectives: Recognize the benefits and risks of LTBI treatment options in order to reduce morbidity from LTBI treatment Understand and be able to use new LTBI treatment options to increase the number of patients completing treatment for LTBI
4 Scaling up : Ingredients? Ramp up, expand coverage, broaden application Specific product (e.g., mobile phones) Strategy (e.g., provider-initiated HIV C&T) Rationale: What are we trying to achieve? TB Elimination, draining the reservoir of latent TB Evidence of efficacy, effectiveness Affordable Hopefully evidence of cost-effectiveness Steady supply if product-based
5 Scaling up: Getting There? Systematize Put in existing system, e.g., routine contact investigation leads to identification of high-risk LTBI If no systems, create Educate Private and public health care providers Public (targeted? Who, where?) Fund Measure progress
6 Scaling up : Rationale It is estimated that as much of 1/3 of world s population has evidence of latent TB infection Serves as reservoir of future cases Proportion of local population that progresses to active TB depends on population co-factors: o Innate immunity & ongoing community transmission o Burden of silicosis, HIV/AIDS, diabetes mellitus, smoking, iatrogenic immunosuppression o Socioeconomics: crowded living conditions, malnutrition, poor education 6

7 Scope of Problem: Enormous Reservoir of Latent TB ~ 1/3 world s population with LTBI Progress to Active TB


8 Spillover to active TB can be. Modest.think Mexico, much of Latin America A trickle e.g., USA, Canada, Europe, New Zealand, Australia, Japan 8


9 Spillover to active TB can be. Frequent, potentially accelerating. Think countries of former Soviet Union eastern Europe, parts of Asia Overwhelming. Southern Africa coinciding with HIV/AIDS epidemic 9
10 Impact of Addressing the Reservoirs US & Canada: Scope & Impact of Treating LTBI Studied LTBI practices in % of LTBI identified and treated in public health clinics Immigrant/refugee clinics (6.4%), correctional/detention centers 6.1% Drying up the reservoir! Extrapolated to estimate that between 4-11,000 future TB cases prevented by activities that year Sterling, TB Epi Consortium; AJRCCM, 2006,
11 Most Effective Interventions? Or, where to spend the $$? Number of cases Number of deaths Treating LTBI Treating LTBI TB Morbidity TB Morality Abu-Raddad et al; PNAS 106: ; 2009
12 Scaling up : Ingredients? Ramp up, expand coverage, broaden application Specific product (e.g., mobile phones) Strategy (e.g., provider-initiated HIV C&T) Rationale: What are we trying to achieve? TB Elimination, draining the reservoir of latent TB Evidence of efficacy, effectiveness Affordable Hopefully evidence of cost-effectiveness Steady supply if product-based
13 Latent TB Infection (LTBI) Active TB Continuum from exposure to infection to latency to active disease Opportunity to intervene

14 Latent TB Infection (LTBI): Not Really Latent Trends in Microbiology, Young, 2009,
15 Latent TB Infection (LTBI) Active TB Continuum from exposure to infection to latency to active disease Opportunity to intervene Certain populations EXTREMELY vulnerable Recent close contacts to a case, especially infants and children <4 years HIV/AIDS; other immunosuppressed (TNF-inhibitors) Newly arriving immigrants with abnormal chest x-rays Identifying vulnerable populations can lead to efficient targeted testing for LTBI
16 Evidence for Long-course treatment LTBI with INH Isoniazid (INH) discovered and determined effective for treatment of active TB in 1952 Rapidly bactericidal in animal models and humans disease Let to large scale clinical trials of INH to prevent development of disease
17 Evidence for Long-course treatment LTBI with INH Union (IUAT) trials of 27,830 subjects with TST+ and fibrotic lesions on CXR in eastern Europe Placebo-controlled randomized clinical trial (INH versus placebo) Compared 12-week to 24 weeks to 52 weeks INH/placebo Bull WHO 60: ; 1982
18 Evidence for Long-course treatment LTBI with INH Completion: Shorter is better 87% completed 12 weeks 78% completed 24 weeks 68% completed 52 weeks Efficacy: Longer is better 21% reduction in TB cases with 12 weeks treatment 65% reduction.. with 24 weeks treatment 75% reduction.. with 52 weeks treatment Bull WHO 60: ; 1982

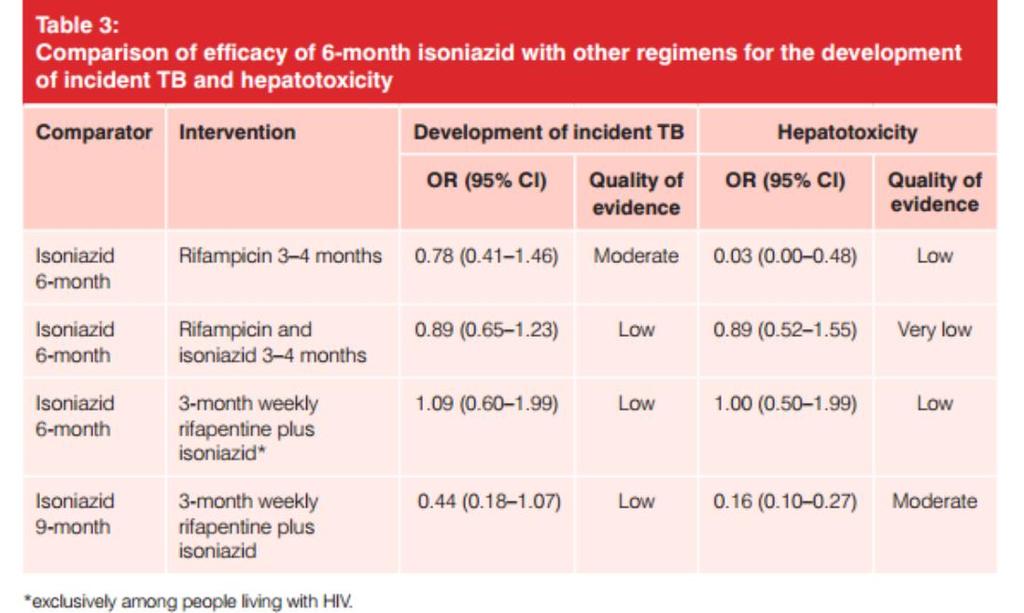
19 Evidence for Long-course treatment LTBI with INH WHO LTBI Guidelines, 2015, evidence table
20 Long-course treatment LTBI with INH: Limitations TBESC study (Colson et al, 2013, IJTLD) 29% eligible for TLTBI refused to participate in study Of those enrolled in study, 89% agreed to TLTBI Completion of 6-9 month INH 20-60% range Boston study, mostly foreign-born population, 29% finished 6 months INH (Shieh et al; 2006, AJRCCM) Multi-site study of close contacts, 63% completed (Fiske et al, 2014, IJTLD) Commonly sited reasons for discontinuation: Side effects, time away from work or family, resistance to taking medicine when not sick *LoBue, Moser; AJRCCM 168; 443-7; 2003
21 Long-course treatment LTBI with INH: Is There a Better Way? WHO LTBI Guidelines, 2015, evidence table
22 Scaling up : Ingredients? Ramp up, expand coverage, broaden application Specific product (e.g., mobile phones) Strategy (e.g., provider-initiated HIV C&T) Rationale: What are we trying to achieve? TB Elimination, draining the reservoir of latent TB Evidence of efficacy, effectiveness Affordable Hopefully evidence of cost-effectiveness Steady supply if product-based


23 Scaling up : Current Approach Not Working NEED A SHORTER DRUG REGIMEN THAN 9 months IPT!
24 PREVENT TB*: RCT 9H versus 3HP 9 INH Arm INH 300 mg Self-administered Daily, 9 months 3HP Arm INH 900 mg + RPT 900 mg DOT Weekly, 3 months TB Trials Consortium study: US, Canada, Brazil, Spain & Hong Kong enrolled high risk adults and children with LTBI (e.g., recent contacts to a case, recent conversions), (children > age 2) and HIV-infected (not on ARV) Followed each for 2 years after end of treatment *Sterling et al; N Engl J Med 2011;365: (adults); pediatric data in press; HIV data CROI
25 PREVENT TB: RCT 9H versus 3HP Conclusions for all populations studied (adults, children, HIV+): Weekly 3HP by DOT was at least as effective as 9H by selfadministration Met non-inferiority criteria Among adults, 3HP TB rate was approximately half that of 9H in adult, non-hiv The 3HP completion rate was significantly higher than 9H 3HP was safe relative to 9H Lower rates of any adverse event, and less hepatotoxicity attributable to study drug ClinicalTrials.gov: NCT

")
26 Subsequent Studies show it is safe and effective in: *children down to age 2 *persons living with HIV/AIDS (caution RPT drug-drug-interaction) *self-administered
27 Scaling up : Ingredients? Ramp up, expand coverage, broaden application Specific product (e.g., mobile phones) Strategy (e.g., provider-initiated HIV C&T) Rationale: What are we trying to achieve? TB Elimination, draining the reservoir of latent TB Evidence of efficacy, effectiveness Manage side-effects, toxicities Affordable Hopefully evidence of cost-effectiveness Steady supply if product-based
28 Overview Toxicities of All LTBI Treatment Regimens Hepatotoxicity Less if regimen excludes daily INH Drug-drug interactions Many if regimen w/rif or RPT Syncope/hypersensitivity syndrome: Unique to 12 HP Requires counseling and education Serious episodes rare, but potential for harm Mild: Dizziness, rash can try a second dose Moderate to severe (syncope) or allergic reactions: bronchospasm/wheezing, urticarial, angioedema No further doses; manage as other allergy/anaphylaxic
29 Scaling up : Ingredients? Ramp up, expand coverage, broaden application Specific product (e.g., mobile phones) Strategy (e.g., provider-initiated HIV C&T) Rationale: What are we trying to achieve? TB Elimination, draining the reservoir of latent TB Evidence of efficacy, effectiveness Manage side-effects, toxicities Affordable Hopefully evidence of cost-effectiveness Steady supply if product-based
30 Scaling up : Affordability of 3 HP Expense of PRIFTIN Started at $52/32-tablet blister pack : $32/pack (need 2.25 packs per course, adults) 2016: Course of treatment Rifapentine & INH $ $1.00* *California FAQ sheet estimates total $147/month with clinic visit and DOT Modeling study** showed that even at $52/pack and with DOT, 3-month HP more cost effective than 9H Fewer TB cases because of greater uptake, completion, less toxicity **Holland et al; PLoS ONE, vol 6; 2011; e22276
31 Scaling up 3 HP: DOT and the iadhere Study iadhere randomized participants into selfadministered, with or without SMS reminders, compared to DOPT Recognizing that DOPT is almost certainly going to result in higher completion rates, but affordable, sustainable? Therefore planned on a non-inferiority statistical approach, i.e., will SA no more than than 15% lessgood than DOPT
32 Belknap R et al; CROI 2015, manuscript in preparation iadhere: Comparable Completion Rates Selfadministered Compared to DOPT
* Hong")
33 Shorter Treatment Options for LTBI? 2 months rifampin and pyrazinamide Efficacy similar to INH But significant hepatotoxicity outside HIV+ populations INH and rifampin for 3 months 5 trials, total of 1,926 adults (meta-analysis)* Hong Kong, Spain, Uganda Estimated similar efficacy to INH, also similar toxicity Rifampin for 3 months One study (silicosis + TST+) showed 63% efficacy Less toxicity than INH Rifampin for 4 months RIF 4 months has become default regimen in many places due to higher uptake, low toxicity, despite very limited data Currently being evaluated in RCT (Menzies et al) *Ena, Valls; CID 40:670-6; 2005

34 Toxicities of Regimens Hepatotoxicity Less with any regimen that excludes INH Drug-drug interactions More with any regimen that includes rifampin or rifapentine Syncope/hypersensitivity syndrome Associated with once-weekly HP Requires counseling and education Discontinuation if occurs Serious episodes rare, but potential for harm
35
36 Scaling up : Ingredients? Ramp up, expand coverage, broaden application Specific product (e.g., mobile phones) Strategy (e.g., provider-initiated HIV C&T) Rationale: What are we trying to achieve? TB Elimination, draining the reservoir of latent TB Evidence of efficacy, effectiveness Manage side-effects, toxicities Affordable Hopefully evidence of cost-effectiveness Steady supply if product-based Assume YES
37 Scaling up: Getting There? Systematize Put in existing system, e.g., routine contact investigation leads to identification of high-risk LTBI Educate If no systems, create Give practitioners experience Private and public health care providers Public (targeted? Who, where?) Fund Measure progress
38 Post-marketing Project Objectives Monitor for adverse events with 3HP in non-research settings Track number of patients started on regimen Note if certain populations, risk factors or settings are associated with adverse effects (AE) more often Assess compliance and treatment completion Assess impact of 3HP on programs Staffing Costs Match patients with TB registry at 2 years Observational measurement of effectiveness Surveillance for drug-resistant TB after LTBI treatment Near-final data, with permission, Ho, Nwana, et al, CDC Field Services Branch, Presentation 2015 Union meetings, Cape Town
 discontinued treatment 2,867 (87.2%) completed treatment 246 (7.")
39 Post-marketing 3HP Surveillance Project Patients Started on 3HP, June 2011 December ,327 patients started on 3HP 39 Ineligible to complete Index-case resistant: 20 QFT negative/not LTBI: 2 Active TB case: 1 Pregnant: 14 HIV + receiving HAART: 2 3,288 patients eligible to complete treatment 421 (12.8%) discontinued treatment 2,867 (87.2%) completed treatment 246 (7.5%) discontinued with symptoms 175 (5.3%) discontinued due to other reasons


40 Treatment Completion Rate (%) Range of Treatment Completion Across 16 U.S. Sites, June 2011 December * L E J A F D I N K H O P C B G M Participating Site Number of participants at each site ranged from 14 to 1,018 Completion ranged from % Discontinuation while reporting symptoms ranged from 0 16% * Proportion completing treatment among those eligible to complete at that site Near-final data, with permission, Ho, Nwana, et al, CDC Field Services Branch, Presentation 2015 Union meetings, Cape Town
41 Demographic Factors and Treatment Reasons Associated with Discontinuation of 3HP, N=3,288 Discontinued Multivariate Completed Univariate N p-value arr N (%) RR (%) p-value Age (years) 1.01 <.001 (2-17) (94.5) (5.5) >=65 Race/Ethnicity Non-Hispanic White Treatment Reason Contact Corrections Homeless Student 154 (78.6) 595 (82.5) 751 (91.5) 451 (87.4) 147 (81.2) 123 (94.6) 42 (21.4) 126 (17.5) 70 (8.5) 65 (12.6) 34 (18.8) 7 (5.4) 1.72 < <


42 Scaling up: Getting There? Education, Systemization California TBCB 3 HP FAQ Sheet
43 Scaling up: Getting There? Systematize Put in existing system, e.g., routine contact investigation leads to identification of high-risk LTBI Educate If no systems, create Give practitioners experience Private and public health care providers Public (targeted? Who, where?) Fund Measure progress
44
45 Reported Symptoms for Patients on 3HP and Treatment Completion % 12% 5% 3% 8% 8% 7% 6% 6% 6% 3% 2% 5% 3% 4% 4% 2% 2% 3% 2% 4% 1% 1% 1% 0.7% 10% 9% 5% 5% 3% 4% 4% 3% 3% 3% 3% 5% Completed Tx Discontinued Tx Other symptoms reported by one or more patients include: Dermatological-related Symptom, Gastro-Intestinal related Symptoms, Cough, Mental Health Symptom, Weight Loss, Blurred Vision, Flu-like Symptoms, Breathing Problem, Back Pain, Gynecological-related Symptoms, Chest Pain, Diaphoresis, Angioedema, Bleeding, Palpitation, Ease Bruising, Edema, Neurologic Symptoms, Hypotension, Flushing, Red Eyes, URI, Genitourinary Symptoms, Other Eye Symptom, Black Stool, Pain, Pneumonia, and Sepsis. *Patients can have more than one symptom


46 Updating LTBI Testing and Treatment Guidelines Updating the 2000 LTBI Guidelines In process since 2011 Co-sponsored by ATS (MTPI Assembly), CDC and IDSA and in-kind author support from institutions Working with NTCA to create companion how-to document
47 Conclusions: Scaling Up Treatment of LTBI Targeted testing and treatment of high-risk individuals is necessary for TB Elimination in the US We now have important new tools IGRAs more specific, may help with FB populations Shorter regimens higher acceptance and completion Agreement across international normative bodies embracing short-course regimens ATS/CDC/IDSA LTBI treatment guideline update in progress Canada, WHO embrace
48 Acknowledgements Conveners of Annual meeting for invitation Charlie Crane National TB Controllers Association Review and work together on guidelines, and guideline supplement CDC s ongoing support for TB Trials Consortium Ken Castro, Andy Vernon Tim Sterling, Elsa Villarino and all other TBTC investigators for Study 26/PREVENT TB Chistine Ho, Nwana, et al, CDC Field Services Branch, for generously sharing their data Jason Stout (Duke), David Holland
Scaling up LTBI Treatment with Short Course Regimens to Eliminate TB
 August 2016 Scaling up LTBI Treatment with Short Course Regimens to Eliminate TB Carol Dukes Hamilton, MD, MHS Director, Scientific Affairs and Leader, TB Portfolio, FHI 360 Professor of Medicine, Duke
August 2016 Scaling up LTBI Treatment with Short Course Regimens to Eliminate TB Carol Dukes Hamilton, MD, MHS Director, Scientific Affairs and Leader, TB Portfolio, FHI 360 Professor of Medicine, Duke
Disclosures. Public Health Motivation 6/6/2012. The 12-Dose INH-Rifapentine Once-Weekly DOT Regimen: What Next?
 The 12-Dose INH-Rifapentine Once-Weekly DOT Regimen: What Next? NTCA Conference June 14, 2012 John Jereb, FSEB, DTBE, CDC Special thanks to Christine Ho, Elsa Villarino, and Andrey Borisov The findings
The 12-Dose INH-Rifapentine Once-Weekly DOT Regimen: What Next? NTCA Conference June 14, 2012 John Jereb, FSEB, DTBE, CDC Special thanks to Christine Ho, Elsa Villarino, and Andrey Borisov The findings
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Sharing the Care: Working Together on LTBI Treatment and Management Webinar. September 24, Curry International Tuberculosis Center
 TB Infection Diagnostics and Treatment Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention 1 Curry International
TB Infection Diagnostics and Treatment Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention 1 Curry International
The Role of Rifampin for the Treatment of Latent TB Infection. Introduction. Introduction
 The Role of Rifampin for the Treatment of Latent TB Infection March 26, 2008 Alfred A. Lardizabal, MD Associate Professor of Medicine New Jersey Medical School Global Tuberculosis institute Treatment of
The Role of Rifampin for the Treatment of Latent TB Infection March 26, 2008 Alfred A. Lardizabal, MD Associate Professor of Medicine New Jersey Medical School Global Tuberculosis institute Treatment of
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Tuberculosis: Where Are We Now?
 Tuberculosis: Where Are We Now? Amee Patrawalla MD MPH Rutgers - NJ Medical School Global TB Institute Rutgers, The State University of New Jersey Learning Objectives Understand the current epidemiologic
Tuberculosis: Where Are We Now? Amee Patrawalla MD MPH Rutgers - NJ Medical School Global TB Institute Rutgers, The State University of New Jersey Learning Objectives Understand the current epidemiologic
LTBI: Who to Test & When to Treat
 LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
The Tip of the Iceberg: Addressing Latent Tuberculosis Infection to Accelerate Tuberculosis Elimination
 Four Corners TB and HIV Conference November 3, 2015 Durango, CO The Tip of the Iceberg: Addressing Latent Tuberculosis Infection to Accelerate Tuberculosis Elimination Philip LoBue, MD National Center
Four Corners TB and HIV Conference November 3, 2015 Durango, CO The Tip of the Iceberg: Addressing Latent Tuberculosis Infection to Accelerate Tuberculosis Elimination Philip LoBue, MD National Center
TB PREVENTION: TREATMENT OF LATENT TB INFECTION AND BCG VACCINATION
 TB PREVENTION: TREATMENT OF LATENT TB INFECTION AND BCG VACCINATION Michelle Haas, M.D. Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES
TB PREVENTION: TREATMENT OF LATENT TB INFECTION AND BCG VACCINATION Michelle Haas, M.D. Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES
Pediatric Tuberculosis in Los Angeles County: An Update
 Pediatric Tuberculosis in Los Angeles County: An Update Julie Higashi, MD PhD Director, Tuberculosis Control Program March 2, 2019 0 Pediatricians will be the driving force of TB elimination in California
Pediatric Tuberculosis in Los Angeles County: An Update Julie Higashi, MD PhD Director, Tuberculosis Control Program March 2, 2019 0 Pediatricians will be the driving force of TB elimination in California
Disclosures. Updates in TB for the PCP: Opportunities for Prevention. Objectives PART 1: WHY TEST? 4/14/2016. None
 Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Expanding Latent Tuberculosis Infection Testing and Treatment to Accelerate Tuberculosis Elimination
 IUATLD North American Region Conference February 24, 2017 Vancouver, BC Expanding Latent Tuberculosis Infection Testing and Treatment to Accelerate Tuberculosis Elimination Philip LoBue, MD National Center
IUATLD North American Region Conference February 24, 2017 Vancouver, BC Expanding Latent Tuberculosis Infection Testing and Treatment to Accelerate Tuberculosis Elimination Philip LoBue, MD National Center
Ruth Moro M.D., M.P.H. Medical Epidemiologist. CDC, Division of Tuberculosis Elimination Clinical Research Branch Tuberculosis Trials Consortium
 Factors Associated with Non-completion of Latent Tuberculosis Infection (LTBI) Treatment: Reasons other than Adverse Events (AE) The TB Trials Consortium PREVENT TB Study 26 Ruth Moro M.D., M.P.H. Medical
Factors Associated with Non-completion of Latent Tuberculosis Infection (LTBI) Treatment: Reasons other than Adverse Events (AE) The TB Trials Consortium PREVENT TB Study 26 Ruth Moro M.D., M.P.H. Medical
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents
 New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
State of the State in TB Control
 State of the State in TB Control Jason Stout, MD, MHS Wake County TB Medical Consultant NC TB Medical Director Division of Infectious Diseases, Duke University Medical Center Disclosures-Funding NIH (grant)
State of the State in TB Control Jason Stout, MD, MHS Wake County TB Medical Consultant NC TB Medical Director Division of Infectious Diseases, Duke University Medical Center Disclosures-Funding NIH (grant)
Jeffrey R. Starke, M.D. has the following disclosures to make:
 AAP 2018 Red Book Tuberculosis: IGRAs and Treatment of TB Infection Jeffrey R. Starke, M.D. May 31, 2018 AAP 2018 Red Book Childhood Tuberculosis: IGRAs and Treatment of TB Infection May 31, 2018 WEBINAR
AAP 2018 Red Book Tuberculosis: IGRAs and Treatment of TB Infection Jeffrey R. Starke, M.D. May 31, 2018 AAP 2018 Red Book Childhood Tuberculosis: IGRAs and Treatment of TB Infection May 31, 2018 WEBINAR
Modeling LTBI What are the key issues to consider? Dr Dick Menzies, Montreal Chest Institute, McGill International TB Centre
 Modeling LTBI What are the key issues to consider? Dr Dick Menzies, Montreal Chest Institute, McGill International TB Centre Overview The problem Treating active TB does not seem to be enough The solution:
Modeling LTBI What are the key issues to consider? Dr Dick Menzies, Montreal Chest Institute, McGill International TB Centre Overview The problem Treating active TB does not seem to be enough The solution:
Breakout Session C2 Christine Ho April 21, 2017
 3HP (12 dose Weekly INH and Rifapentine) Today and Tomorrow Christine S. Ho, M.D., M.P.H. CDC Division of Tuberculosis Elimination National Tuberculosis Conference TB Infection Breakout Session April 21,
3HP (12 dose Weekly INH and Rifapentine) Today and Tomorrow Christine S. Ho, M.D., M.P.H. CDC Division of Tuberculosis Elimination National Tuberculosis Conference TB Infection Breakout Session April 21,
TB Infection Who is Testing and Treating? TB Control and Elimination: Current Dilemma. Span of TB Control: 2010
 TB Infection Who is Testing and Treating? Jennifer Flood, M.D., M.P.H. California Department of Public Health Tuberculosis Control Branch Jennifer.Flood@cdph.ca.gov 1 TB Control and Elimination: Current
TB Infection Who is Testing and Treating? Jennifer Flood, M.D., M.P.H. California Department of Public Health Tuberculosis Control Branch Jennifer.Flood@cdph.ca.gov 1 TB Control and Elimination: Current
The role of ART and IPT in TB prevention: Latest updates
 The role of ART and IPT in TB prevention: Latest updates Richard E. Chaisson, MD Center for Tuberculosis Research Johns Hopkins University Consortium to Respond Effectively To the AIDS-TB Epidemic (CREATE)
The role of ART and IPT in TB prevention: Latest updates Richard E. Chaisson, MD Center for Tuberculosis Research Johns Hopkins University Consortium to Respond Effectively To the AIDS-TB Epidemic (CREATE)
Please distribute a copy of this information to each provider in your organization.
 HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
Background. The global burden of latent M. tuberculosis. More than 2 billion people infected
 What s New in Treatment tof LTBI Alfred Lardizabal, MD November 17, 2011 Washington, D.C. Background The global burden of latent M. tuberculosis infection is enormous More than 2 billion people infected
What s New in Treatment tof LTBI Alfred Lardizabal, MD November 17, 2011 Washington, D.C. Background The global burden of latent M. tuberculosis infection is enormous More than 2 billion people infected
Disclosures. Outline. No disclosures or conflicts of interest to report. Special LTBI situations. H t it d id ff t
 Selected Topics in LTBI June 2, 2015 Bijan Ghassemieh, MD Senior Fellow UW Division of Pulmonary/Critical Care Disclosures No disclosures or conflicts of interest to report Outline Special LTBI situations
Selected Topics in LTBI June 2, 2015 Bijan Ghassemieh, MD Senior Fellow UW Division of Pulmonary/Critical Care Disclosures No disclosures or conflicts of interest to report Outline Special LTBI situations
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, TB Nurse Case Management September 12 14, 2017
 Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
The Epidemiology of Tuberculosis in Minnesota,
 The Epidemiology of Tuberculosis in Minnesota, 2011 2015 Minnesota Department of Health Tuberculosis Prevention and Control Program (651) 201-5414 Tuberculosis surveillance data for Minnesota are available
The Epidemiology of Tuberculosis in Minnesota, 2011 2015 Minnesota Department of Health Tuberculosis Prevention and Control Program (651) 201-5414 Tuberculosis surveillance data for Minnesota are available
Preventing TB: Recent Research Results and Novel Short Course Therapy for LTBI
 Preventing TB: Recent Research Results and Novel Short Course Therapy for LTBI Constance A. Benson, M.D. Professor of Medicine Director, UCSD AntiViral Research Unit PI, CD4 Collaborative HIV Clinical
Preventing TB: Recent Research Results and Novel Short Course Therapy for LTBI Constance A. Benson, M.D. Professor of Medicine Director, UCSD AntiViral Research Unit PI, CD4 Collaborative HIV Clinical
Contact Investigation
 Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Detection and Treatment of Tuberculosis in Correctional Facilities: Opportunities and Challenges
 Detection and Treatment of Tuberculosis in Correctional Facilities: Opportunities and Challenges David Karol, MD, MA Bureau of Prisons, FMC Butner Duke University Medical Center June 26, 2013 No Disclosures
Detection and Treatment of Tuberculosis in Correctional Facilities: Opportunities and Challenges David Karol, MD, MA Bureau of Prisons, FMC Butner Duke University Medical Center June 26, 2013 No Disclosures
Treatment of Tuberculosis, 2017
 Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal
 Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal Civil surgeons are required to report tuberculosis (TB) screening outcomes that result in latent TB
Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal Civil surgeons are required to report tuberculosis (TB) screening outcomes that result in latent TB
Disclosures. TB and CoMorbidities Challenges and Opportunities. Burden of TB. Outline of the lecture. Target testing for TB Infection TB HIV 3/25/2012
 Disclosures TB and CoMorbidities Challenges and Opportunities E. Jane Carter, M.D. Associate Professor of Medicine Alpert School of Medicine, Brown University Providence, Rhode Island No financial disclosures
Disclosures TB and CoMorbidities Challenges and Opportunities E. Jane Carter, M.D. Associate Professor of Medicine Alpert School of Medicine, Brown University Providence, Rhode Island No financial disclosures
Epidemiology of Tuberculosis Denver TB Course
 Epidemiology of Tuberculosis Denver TB Course Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver
Epidemiology of Tuberculosis Denver TB Course Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver
Clinical Trials Lecture 4: Data analysis
 Clinical Trials Lecture 4: Data analysis Dick Menzies, MD Respiratory Epidemiology and Clinical Research Unit Montreal Chest Institute TB Research methods course July 17, 2014 Lecture 4: Data analysis
Clinical Trials Lecture 4: Data analysis Dick Menzies, MD Respiratory Epidemiology and Clinical Research Unit Montreal Chest Institute TB Research methods course July 17, 2014 Lecture 4: Data analysis
TB is Global. Latent TB Infection (LTBI) Sharing the Care: Working Together. September 24, 2014
 Sharing the Care: Working Together. September 24, 2014") Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
TUBERCULOSIS CONTACT INVESTIGATION
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the criteria used
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the criteria used
Management of Patients with TB Infection Catalina Navarro, RN, BSN April 7, 2015
 Management of Patients with TB Infection Catalina Navarro, RN, BSN April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Catalina Navarro,
Management of Patients with TB Infection Catalina Navarro, RN, BSN April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Catalina Navarro,
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Santa Clara County Tuberculosis Screening Requirement for School Entrance Effective June 1, 2014
 Guidelines to Revisions to the School Mandate and Requirements 1) What are the tuberculosis (TB) screening requirements for school entrance in Santa Clara County? Students must undergo a TB risk assessment
Guidelines to Revisions to the School Mandate and Requirements 1) What are the tuberculosis (TB) screening requirements for school entrance in Santa Clara County? Students must undergo a TB risk assessment
Tuberculosis Populations at Risk
 Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
TB prevention studies in PLHIV: recent updates and what can they tell us for the future?
 TB prevention studies in PLHIV: recent updates and what can they tell us for the future? Richard E. Chaisson, MD Center for AIDS Research Center for TB Research Johns Hopkins University TB/HIV Working
TB prevention studies in PLHIV: recent updates and what can they tell us for the future? Richard E. Chaisson, MD Center for AIDS Research Center for TB Research Johns Hopkins University TB/HIV Working
Treatment of latent tuberculosis infection: An update
 INVITED REVIEW SERIES: TUBERCULOSIS SERIES EDITORS: WING WAI YEW, GIOVANNI B. MIGLIORI, CHRISTOPH LANGE Treatment of latent tuberculosis infection: An update PHILIP LOBUE 1 AND DICK MENZIES 2 1 Division
INVITED REVIEW SERIES: TUBERCULOSIS SERIES EDITORS: WING WAI YEW, GIOVANNI B. MIGLIORI, CHRISTOPH LANGE Treatment of latent tuberculosis infection: An update PHILIP LOBUE 1 AND DICK MENZIES 2 1 Division
Tuberculosis Elimination
 Tuberculosis Elimination Where We ve Been, Where We re Going Mark Lobato, MD New England TB Consultant Division of Tuberculosis Elimination Centers for Disease Control and Prevention Disclosures / Disclaimer
Tuberculosis Elimination Where We ve Been, Where We re Going Mark Lobato, MD New England TB Consultant Division of Tuberculosis Elimination Centers for Disease Control and Prevention Disclosures / Disclaimer
Therapy for Latent Tuberculosis Infection
 Screening and Treatment of LTBI in TB Control in the US Margarita Elsa Villarino MD MPH Division of TB Elimination, CDC April 14, 2004 TB Prevention and Control in the United States The fundamental strategies
Screening and Treatment of LTBI in TB Control in the US Margarita Elsa Villarino MD MPH Division of TB Elimination, CDC April 14, 2004 TB Prevention and Control in the United States The fundamental strategies
The American Experience with TB Elimination
 Reaching the Goal of TB Elimination by 2035 March 3, 2015 The American Experience with TB Elimination John Jereb, M.D. Medical officer Division of Tuberculosis Elimination National Center for HIV/AIDS,
Reaching the Goal of TB Elimination by 2035 March 3, 2015 The American Experience with TB Elimination John Jereb, M.D. Medical officer Division of Tuberculosis Elimination National Center for HIV/AIDS,
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
INH Prophylaxis Therapy (IPT) should NOT be implemented for all HIV patients in the Asia Pacific
 should NOT be implemented for all HIV patients in the Asia Pacific") INH Prophylaxis Therapy (IPT) should NOT be implemented for all HIV patients in the Asia Pacific Thuy Le, MD DPhil Duke University School of Medicine, USA Oxford University Clinical Research Unit Hospital
INH Prophylaxis Therapy (IPT) should NOT be implemented for all HIV patients in the Asia Pacific Thuy Le, MD DPhil Duke University School of Medicine, USA Oxford University Clinical Research Unit Hospital
CDC's Tuberculosis Trials Consortium
 CDC's Tuberculosis Trials Consortium Kayla Laserson, Andrew Vernon, Erin Bliven, Neil Schluger, William Burman, Fred Gordin, Tim Sterling, Carol Dukes Hamilton, Debra Benator, Donna Conwell, Nancy Dianis,
CDC's Tuberculosis Trials Consortium Kayla Laserson, Andrew Vernon, Erin Bliven, Neil Schluger, William Burman, Fred Gordin, Tim Sterling, Carol Dukes Hamilton, Debra Benator, Donna Conwell, Nancy Dianis,
Latent TB Infection Treatment
 Latent TB Infection Treatment Douglas B. Hornick, MD Pulmonologist w/ Infectious Attitude Division of Pulmonary/Critical Care/Occ Med UI Carver College of Medicine 2014 MFMER slide-1 Disclosures: None
Latent TB Infection Treatment Douglas B. Hornick, MD Pulmonologist w/ Infectious Attitude Division of Pulmonary/Critical Care/Occ Med UI Carver College of Medicine 2014 MFMER slide-1 Disclosures: None
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI)
") Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of
 TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
Supplement 2: Extracted studies
 Supplement 2: Extracted studies First author Journal Year Participants Country of study Drugs compared Participants Hepatotoxicity extractable? Development of active TB? Agarwal (42) Urology and Nephrology
Supplement 2: Extracted studies First author Journal Year Participants Country of study Drugs compared Participants Hepatotoxicity extractable? Development of active TB? Agarwal (42) Urology and Nephrology
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
2016 Annual Tuberculosis Report For Fresno County
 206 Annual Tuberculosis Report For Fresno County Cases Rate per 00,000 people 206 Tuberculosis Annual Report Fresno County Department of Public Health (FCDPH) Tuberculosis Control Program Tuberculosis
206 Annual Tuberculosis Report For Fresno County Cases Rate per 00,000 people 206 Tuberculosis Annual Report Fresno County Department of Public Health (FCDPH) Tuberculosis Control Program Tuberculosis
Diagnosis & Management of Latent TB Infection
 Diagnosis & Management of Latent TB Infection Prof. Ashok Rattan, MD, MAMS, INSA DFG, WHO Lab Director Academics, Industry: Research, Diagnosis, Public Health, Academics Adviser: Laboratory Operations,
Diagnosis & Management of Latent TB Infection Prof. Ashok Rattan, MD, MAMS, INSA DFG, WHO Lab Director Academics, Industry: Research, Diagnosis, Public Health, Academics Adviser: Laboratory Operations,
Experience with Pyrazinamide and Rifampin Regimens for Latent TB Infection
 Experience with Pyrazinamide and Rifampin Regimens for Latent TB Infection Krista Powell, MD, MPH Co-Project Officer, National Surveillance for Severe Adverse Events Associated with LTBI Treatment Lead,
Experience with Pyrazinamide and Rifampin Regimens for Latent TB Infection Krista Powell, MD, MPH Co-Project Officer, National Surveillance for Severe Adverse Events Associated with LTBI Treatment Lead,
TBTC research update: are we ready for 3 month treatment? 2009 TBTC Recompetition. NTCA presentation outline
 TBTC research update: are we ready for 3 month treatment? Stefan Goldberg, MD Project officer, TBTC Studies 27, 28, 29 Tuberculosis Trials Consortium (TBTC) CDC Division of TB Elimination NTCA breakout
TBTC research update: are we ready for 3 month treatment? Stefan Goldberg, MD Project officer, TBTC Studies 27, 28, 29 Tuberculosis Trials Consortium (TBTC) CDC Division of TB Elimination NTCA breakout
INDEX CASE INFORMATION
 Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
Tuberculosis Screening Protocol For Use In Marin County School Settings
 Tuberculosis Screening Protocol For Use In Marin County School Settings New Student no known history of positive skin test Kindergarten or First Grade entry (whichever comes first) All students, countywide,
Tuberculosis Screening Protocol For Use In Marin County School Settings New Student no known history of positive skin test Kindergarten or First Grade entry (whichever comes first) All students, countywide,
5. HIV-positive individuals treated with INH should receive Pyridoxine (B6) 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH
 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH") V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
Chapter 5 Treatment for Latent Tuberculosis Infection
 Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Isoniazid Preventive Therapy (IPT)
") Isoniazid Preventive Therapy (IPT) Josefina Cadorna-Carlos, M.D. Professor of Pediatrics U E R M M M C Objectives 1. Define IPT. 2. Discuss the indications for IPT. 3. Present RCT s for IPT (6H vs 9H).
Isoniazid Preventive Therapy (IPT) Josefina Cadorna-Carlos, M.D. Professor of Pediatrics U E R M M M C Objectives 1. Define IPT. 2. Discuss the indications for IPT. 3. Present RCT s for IPT (6H vs 9H).
U.S. Preventive Services Task Force Recommendation Statement: Screening for Latent Tuberculosis Infection (LTBI) in Adults
 in Adults") National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention U.S. Preventive Services Task Force Recommendation Statement: Screening for Latent Tuberculosis Infection (LTBI) in Adults Centers
National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention U.S. Preventive Services Task Force Recommendation Statement: Screening for Latent Tuberculosis Infection (LTBI) in Adults Centers
The Public Health Impact of TB in the Correctional System. Sarah Bur, RN, MPH Federal Bureau of Prisons Infection Prevention and Control Officer
 The Public Health Impact of TB in the Correctional System Sarah Bur, RN, MPH Federal Bureau of Prisons Infection Prevention and Control Officer The Public Health Impact of TB in the Correctional System
The Public Health Impact of TB in the Correctional System Sarah Bur, RN, MPH Federal Bureau of Prisons Infection Prevention and Control Officer The Public Health Impact of TB in the Correctional System
Disclosures. Current Issues and Controversies in Child and Adolescent Tuberculosis 02/24/2016. NSTC 2016 Annual Meeting
 Current Issues and Controversies in Child and Adolescent Tuberculosis Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea Cruz, M.D.] Disclosures Dr.
Current Issues and Controversies in Child and Adolescent Tuberculosis Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea Cruz, M.D.] Disclosures Dr.
TUBERCULOSIS AND THE TNF-α INHIBITORS. Lloyd Friedman, M.D. Yale University Milford Hospital
 TUBERCULOSIS AND THE TNF-α INHIBITORS Lloyd Friedman, M.D. Yale University Milford Hospital Outline TNF-α Anti-TNF-α medications Rates of tuberculosis Lower rates with etanercept Screening for latent tuberculosis
TUBERCULOSIS AND THE TNF-α INHIBITORS Lloyd Friedman, M.D. Yale University Milford Hospital Outline TNF-α Anti-TNF-α medications Rates of tuberculosis Lower rates with etanercept Screening for latent tuberculosis
Latent tuberculosis infection
 EXECUTIVE SUMMARY Latent tuberculosis infection Updated and consolidated guidelines for programmatic management Executive summary Latent tuberculosis infection (LTBI) is defined as a state of persistent
EXECUTIVE SUMMARY Latent tuberculosis infection Updated and consolidated guidelines for programmatic management Executive summary Latent tuberculosis infection (LTBI) is defined as a state of persistent
LTBI Videos-Treatment
 LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]
![CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]](/thumbs/89/99628771.jpg "CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]") CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
What more is required to use rifamycin regimens to prevent TB in people living with HIV in resource constrained settings?
 What more is required to use rifamycin regimens to prevent TB in people living with HIV in resource constrained settings? Gary Maartens Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI
What more is required to use rifamycin regimens to prevent TB in people living with HIV in resource constrained settings? Gary Maartens Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI
Drug Interactions Lisa Armitige, MD, PhD November 17, 2010
 Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Objectives. 3HP and Flu Syndrome What is the Underlying Mechanism? Case #1 3/23/2016. Christina T. Fiske, MD MPH March 30, 2016
 Objectives 3HP and Flu Syndrome What is the Underlying Mechanism? Christina T. Fiske, MD MPH March 30, 2016 Illustrate the side effect of 3HP flu like syndrome after its initiation to raise awareness in
Objectives 3HP and Flu Syndrome What is the Underlying Mechanism? Christina T. Fiske, MD MPH March 30, 2016 Illustrate the side effect of 3HP flu like syndrome after its initiation to raise awareness in
LTBI Treatment and Anti TNF alpha
 LTBI Treatment and Anti TNF alpha Therapy Julie Higashi, MD PhD Director, TB Control Section San Francisco Department of Public Health TNF alpha is important for the immune response against TB Macrophages
LTBI Treatment and Anti TNF alpha Therapy Julie Higashi, MD PhD Director, TB Control Section San Francisco Department of Public Health TNF alpha is important for the immune response against TB Macrophages
Isoniazid preventive therapy for HIV+:
 Isoniazid preventive therapy for HIV+: Controversial topics Gary Maartens Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Risk of TB disease after
Isoniazid preventive therapy for HIV+: Controversial topics Gary Maartens Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Risk of TB disease after
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University
 Lloyd Friedman, M.D. Milford Hospital Yale University") Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Global, National, Regional
 Epidemiology of TB: Global, National, Regional September 13, 211 Edward Zuroweste, MD Chief Medical Officer Migrant Clinicians Network Assistant Professor of Medicine Johns Hopkins School of Medicine Epidemiology
Epidemiology of TB: Global, National, Regional September 13, 211 Edward Zuroweste, MD Chief Medical Officer Migrant Clinicians Network Assistant Professor of Medicine Johns Hopkins School of Medicine Epidemiology
Programmatic management of LTBI : a two pronged approach for ending the TB epidemic. Haileyesus Getahun Global TB Programme WHO/HQ
 Programmatic management of LTBI : a two pronged approach for ending the TB epidemic Haileyesus Getahun Global TB Programme WHO/HQ What is latent TB infection? A state of persistent immune response to stimulation
Programmatic management of LTBI : a two pronged approach for ending the TB epidemic Haileyesus Getahun Global TB Programme WHO/HQ What is latent TB infection? A state of persistent immune response to stimulation
Tuberculosis Intensive November 17 20, 2015 San Antonio, TX
 Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
TB EPIDEMIOLOGY. Outline. Estimated Global TB Burden, TB epidemiology
 TB EPIDEMIOLOGY TB Clinical Intensive Course Curry International Tuberculosis Center September 30, 2015 Varsha Nimbal, MPH Tuberculosis Control Branch California Department of Public Health 1 Outline TB
TB EPIDEMIOLOGY TB Clinical Intensive Course Curry International Tuberculosis Center September 30, 2015 Varsha Nimbal, MPH Tuberculosis Control Branch California Department of Public Health 1 Outline TB
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB Epidemiology. Richard E. Chaisson, MD Johns Hopkins University Center for Tuberculosis Research
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Tuberculosis Exposure, Infection, and Disease Among Children with Medical Comorbidities
 Tuberculosis Exposure, Infection, and Disease Among Children with Medical Comorbidities Andrea T. Cruz, MD, MPH, Omar Merchant, Affan Zafar, and Jeffrey R. Starke, MD Department of Pediatrics February
Tuberculosis Exposure, Infection, and Disease Among Children with Medical Comorbidities Andrea T. Cruz, MD, MPH, Omar Merchant, Affan Zafar, and Jeffrey R. Starke, MD Department of Pediatrics February
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Global, National, Regional
 Epidemiology of TB: Global, National, Regional September 13, 211 Edward Zuroweste, MD Chief Medical Officer Migrant Clinicians Network Assistant Professor of Medicine Johns Hopkins School of Medicine Epidemiology
Epidemiology of TB: Global, National, Regional September 13, 211 Edward Zuroweste, MD Chief Medical Officer Migrant Clinicians Network Assistant Professor of Medicine Johns Hopkins School of Medicine Epidemiology
What Is New in Combination TB Prevention? Lisa J. Nelson Treatment and Care (TAC) Team HIV Department WHO HQ
 Team HIV Department WHO HQ") What Is New in Combination TB Prevention? Lisa J. Nelson Treatment and Care (TAC) Team HIV Department WHO HQ Outline Combination prevention for HIV Approaches to TB prevention Individual Household/key
What Is New in Combination TB Prevention? Lisa J. Nelson Treatment and Care (TAC) Team HIV Department WHO HQ Outline Combination prevention for HIV Approaches to TB prevention Individual Household/key
Tuberculosis Epidemiology
 Tuberculosis Epidemiology TB CLINICAL INTENSIVE COURSE Curry International Tuberculosis Center October 18, 2017 Varsha Hampole, MPH Tuberculosis Control Branch California Department Of Public Health Outline
Tuberculosis Epidemiology TB CLINICAL INTENSIVE COURSE Curry International Tuberculosis Center October 18, 2017 Varsha Hampole, MPH Tuberculosis Control Branch California Department Of Public Health Outline
Diagnosis Latent Tuberculosis. Disclosures. Case
 Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Coordinating with Public Health on Tuberculosis Testing & Treatment
 Coordinating with Public Health on Tuberculosis Testing & Treatment Bernadette Jakeman, PharmD, PhC, BCPS, AAHIVP Associate Professor University of New Mexico College of Pharmacy Objectives 1. Identify
Coordinating with Public Health on Tuberculosis Testing & Treatment Bernadette Jakeman, PharmD, PhC, BCPS, AAHIVP Associate Professor University of New Mexico College of Pharmacy Objectives 1. Identify
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TB Update: March 2012
 TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
Substance Abuse and Tuberculosis Springfield, IL April 27, 2011
 Substance Abuse and Tuberculosis Springfield, IL April 27, 2011 Co-morbidities in Substance Abuse that Impact Managing TB Lisa Armitige, MD, PhD April 27, 2011 Lisa Armitige, MD, PhD has the following
Substance Abuse and Tuberculosis Springfield, IL April 27, 2011 Co-morbidities in Substance Abuse that Impact Managing TB Lisa Armitige, MD, PhD April 27, 2011 Lisa Armitige, MD, PhD has the following
Treatment of Latent TB Infection (LTBI)
") Treatment of Latent TB Infection (LTBI) Mahesh C. Patel, MD June 14, 2017 2014 MFMER slide-1 Mahesh C. Patel, MD Associate Professor Treatment of LTBI Department of Internal Medicine, Division of Infectious
Treatment of Latent TB Infection (LTBI) Mahesh C. Patel, MD June 14, 2017 2014 MFMER slide-1 Mahesh C. Patel, MD Associate Professor Treatment of LTBI Department of Internal Medicine, Division of Infectious
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers
 Questions and Answers for Health Care Providers") Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Programmatic management of latent TB infection: Global perspective and updates. Haileyesus Getahun, MD, MPH, PhD.
 Programmatic management of latent TB infection: Global perspective and updates Haileyesus Getahun, MD, MPH, PhD. What is latent TB infection? A state of persistent immune response to stimulation by Mycobacterium
Programmatic management of latent TB infection: Global perspective and updates Haileyesus Getahun, MD, MPH, PhD. What is latent TB infection? A state of persistent immune response to stimulation by Mycobacterium
Tuberculosis and Diabetes Dec. 10, 2009 Dean Schillinger, M.D. and Gisela Schecter, M.D., M.P.H. 1 of 18
 Screening, Diagnosis, and Treatment of TB in Persons with Diabetes Dean Schillinger, M.D. University of California San Francisco CA Diabetes Program Gisela Schecter, M.D., M.P.H. TB Control Branch CA Department
Screening, Diagnosis, and Treatment of TB in Persons with Diabetes Dean Schillinger, M.D. University of California San Francisco CA Diabetes Program Gisela Schecter, M.D., M.P.H. TB Control Branch CA Department
Ongoing Research on LTBI and Research priorities in India
 Ongoing Research on LTBI and Research priorities in India Dr. C.Padmapriyadarsini, MD, MS ICMR-National Institute for Research in Tuberculosis Chennai, India Technical Consultation Meeting on Programmatic
Ongoing Research on LTBI and Research priorities in India Dr. C.Padmapriyadarsini, MD, MS ICMR-National Institute for Research in Tuberculosis Chennai, India Technical Consultation Meeting on Programmatic
11/1/2017. Disclosures. Update In Tuberculosis, Indiana Outline/Objectives. Pathogenesis of M.tb Global/U.S. TB Burden, 2016
 Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,
Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,