Mycobacterial Ocular Inflammation. Akbar Shakoor, M.D. John A. Moran Eye Center, University of Utah
|
|
|
- Steven Howard
- 5 years ago
- Views:
Transcription


1 Mycobacterial Ocular Inflammation Akbar Shakoor, M.D. John A. Moran Eye Center, University of Utah
2 Financial Disclosure I have no financial interests or relationships to disclose.
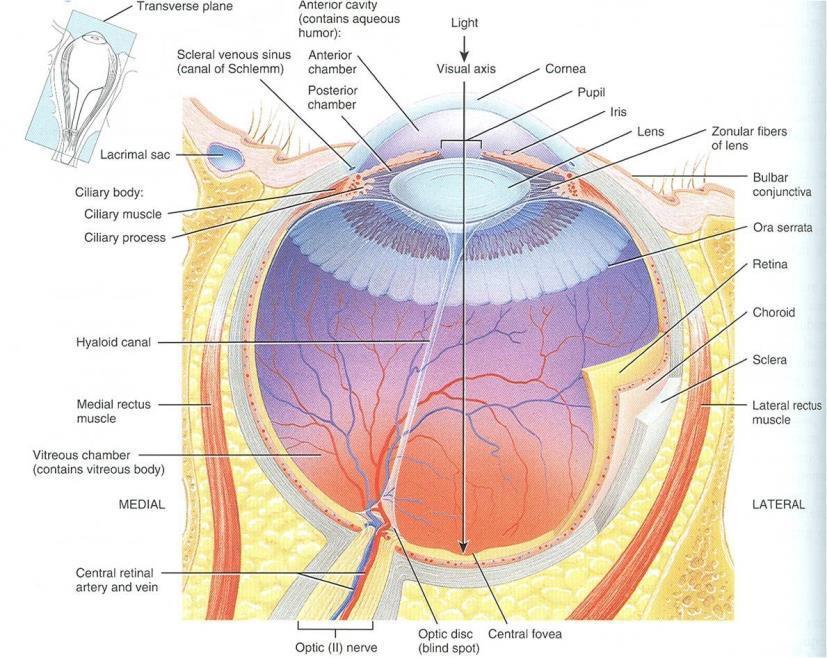
3 Applied anatomy What structures may be involved in ocular inflammatory diseases?
4
5

6
7
8
9
10
11

12 Anatomical location of inflammation 12
13 Ocular immune diseases Uvea - Uveitis Iridocylcitis/iritis Trabeculitis Parsplanitis Choroiditis Vasculature - Vasculitis Connective tissue Scleritis Orbital inflammatory disease
14 Patient CF 28 year old gentleman from Haiti Pain and blurry vision in his left eye for 3 months

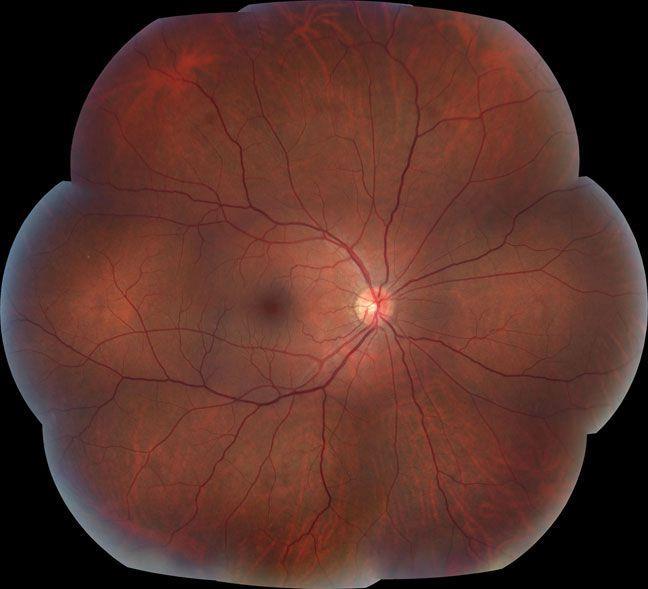
15 Unremarkable right fundus photograph

16 Left fundus: Vitreitis/ hazy view with significant macular scarring and inferior retinochoroidal granuloma

17 Choroidal granuloma with overlying vitreous opacity and surrounding choroidal nodules

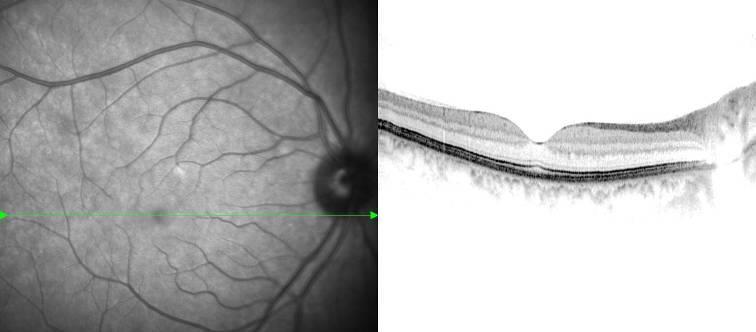
18 Optical coherence tomography: Normal right macula

19 Optical coherence tomography: Abnormal left macula with vitreitis and epiretinal membrane
20 Vitrectomy with large volume vitreous aspirate sent for PCR Negative for mycobacterial DNA PPD positive, Quanteferon gold positive Good response to 4 drug therapy
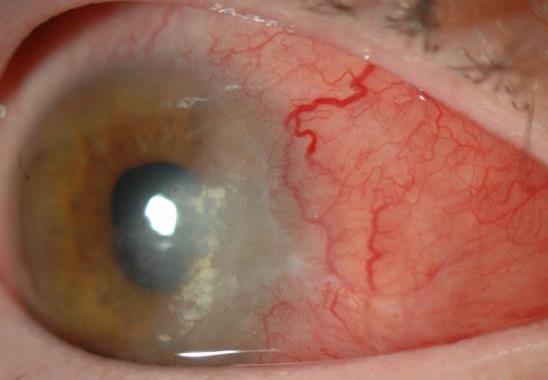
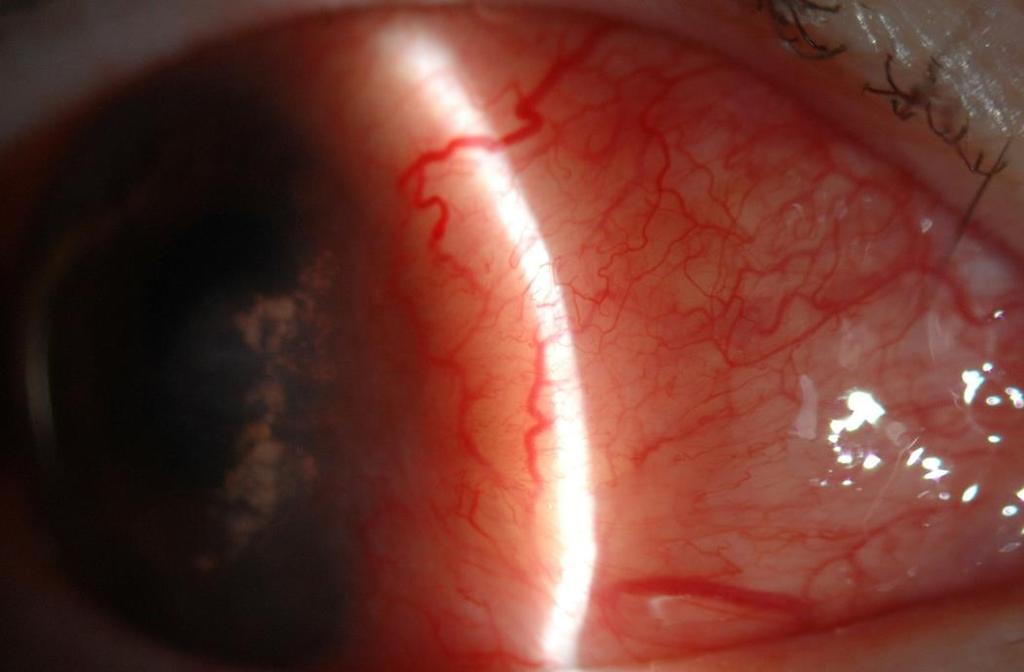
21 Patient MS 54-year-old woman originally from Mexico Redness and pain OD for 6 months, diagnosed with nodular scleritis Did not improve with PO prednisone and referred in 2015 PMH: diabetes on insulin, hypertension, hypercholesterolemia, atrial fibrillation on Coumadin Courtesy Sarju Patel M.D. Cornell

22 Patient MS Large yellow nodules consistent with infectious scleritis QuantiFERON positive CXR and CT chest bilateral hilar adenopathy

23 Patient MS Started on 4 drug therapy for TB, continued on prednisone, variable doses, MTX added Scleritis progressed
24 Patient MS Scleral biopsy Gram stains, AFB stain and bacterial cultures negative Microscopy: extensive scleral necrosis without classic granuloma formation Tissue Gram stain and stains for AFB (Ziehl-Nielson and Fite stains) were negative On and off TB therapy and multiple IMT elsewhere Returned 4 months later to ER Not compliant with TB meds Not taking insulin Still taking Coumadin but not obtaining lab tests Vomiting, in DKA ER noted blood from eye

25
26 Histopathology of globe Extensive necrotizing scleral and uveal inflammation Stains for AFB and cultures were negative Ocular Pathology Laboratory, Doheny Eye Institute (Narsing Rao) Realtime PCR revealed M tuberculosis genome 702 copies of mycobacteria in four 20-μm histologic sections Histopathologic detection of acid fast organisms is not a sensitive method if the bacteria are few in number
27 Patient MKS 60 year old Caucasian woman seen first 2010 Worsening eye pain and redness OD Extensive prior work up negative Poor response to local and systemic corticosteroids
28

29 MKS QuantiFERON positive CXR normal ID would not treat as TB Progressive worsening of scleritis


30 Biopsy of conjunctival lesions contralateral eye revealed caseating granulomas PCR 4 of 5 bands positive for M TB genome

31 MKS 4 drug TB therapy finally started Prednisone, Cellcept Despite this, globe perforated 10 months after presentation Pathology: mass composed of caseating granulomas with central abscesses
32 Tuberculosis: Etiology/Epidemiology M. tuberculosis infection or inflammatory reaction Worldwide: 9 million cases million TB related deaths USA: 9,582 active cases reported to CDC /100, deaths % to 2% systemic TB develop ocular disease High rates among Endemic areas HIV, immigrants, elderly and minority populations Elderly highest non-hiv case rate Chan et al., Clin Immunol 2004;110: 2 Munsiff et al.,acquir Immne Defic Syndr Hum Retrovirol 1998; 19:361
 Vitritis Retinal vasculitis Panuveitis External disease Tubercles: lids/conjunctiva Corneal phlyctenule Conjunctivitis Scleritis Interstitial keratitis Biswas et al Retina")
33 Tuberculosis: Ocular Findings Intraocular inflammation Posterior uveitis (most common presentation) Tuberculoma (immunocompromised host) Multifocal choroiditis ( miliary disease) Anterior uveitis (granulomatous/nongranulom) Vitritis Retinal vasculitis Panuveitis External disease Tubercles: lids/conjunctiva Corneal phlyctenule Conjunctivitis Scleritis Interstitial keratitis Biswas et al Retina 1995;15:461 Gupta et al., 2003 Ophthalmology; 110:1744
34
 Evidence ocular or non-ocular TB PPD, QuantiFERON gold CXR, PCR (AC, vitreous) Non-contiguous multifocal choroiditis diffuse plaque-like choroiditis Bilateral (60%) Vitritis (80%) Treatment ATT and")
35 Multifocal Serpiginous Choroiditis M (70%)> F Middle age (mean 33 yrs.) Evidence ocular or non-ocular TB PPD, QuantiFERON gold CXR, PCR (AC, vitreous) Non-contiguous multifocal choroiditis diffuse plaque-like choroiditis Bilateral (60%) Vitritis (80%) Treatment ATT and corticosteroids IMT for progression Bansal R, et al. Ophthalmology 2012;119; 2334 Khanamiri NH, Rao NA. SurvOphthalmol. 2013;58:203 Courtesy Narsing Rao, MD

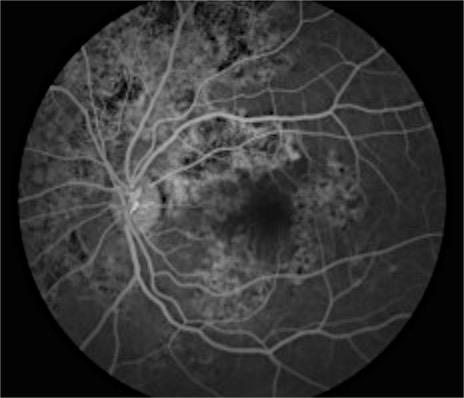
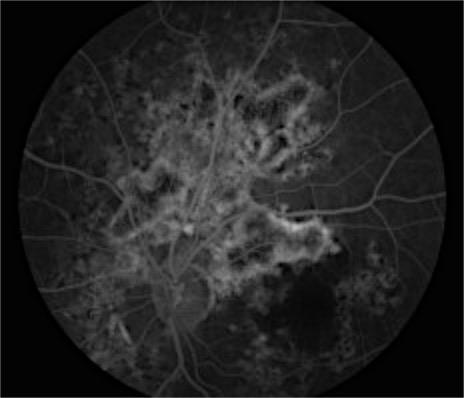
36 Multifocal serpiginoid choroiditis 62 year old male referred with worsening serpiginous after two years prednisone and IMT. Had subtle interstitial keratitis right eye PPD positive. Note peripheral lesions
37 Serpiginous choroiditis vs infectious multifocal serpiginoid choroiditis Features suggesting TB (Narsing Rao) Endemic area Multifocality of lesions Unilaterality of lesions Vitreous or AC reaction Early lesions are macular rather than peri-papillary Response to ATT Survey of ophthalmology (3):



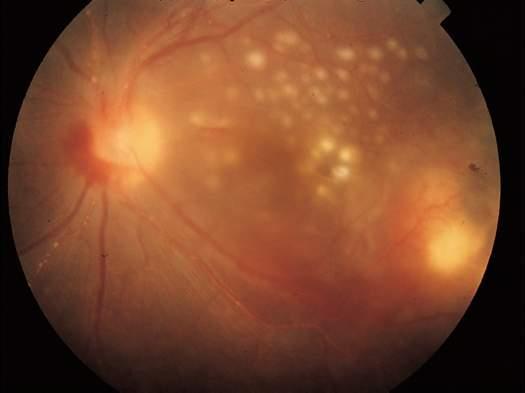
38 60 year old Caucasian woman from Poland Positive Quantiferon, CT chest evidence prior granulomatous disease Note appearance of choroidal lesion
39 Tuberculous Uveitis 39 Photograph courtesy of Narsing A. Rao, MD
40 Patient SA 32 year old physician Unilateral choroidal lesions Painless loss of vision 1 week prior to presentation

41
42
43 43 Tuberculous Uveitis
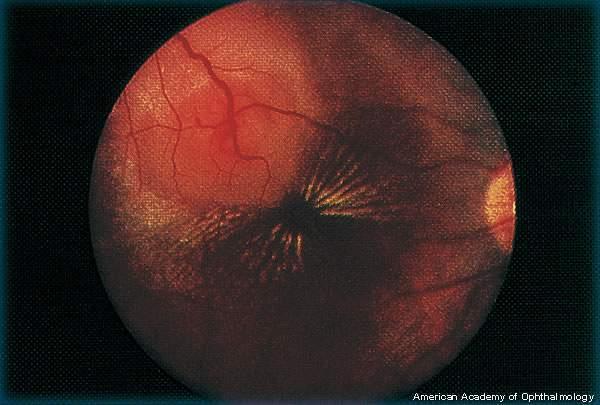
44 44 Tuberculous Uveitis
45 Tuberculous Uveitis Multiple presentations No consensus thus far on classic features Can affect all tunics of the eye
46
47 Ocular Tuberculosis: Diagnosis Presumptive No pulmonary/systemic disease Tuberculin skin test (PPD) > 5 mm HIV + > 10 mm health care worker > 15 mm everyone else QuantiFERON gold assay Latent disease Chest x-ray Normal 50% patients with ocular TB Ocular tissue, intraocular fluid analysis Acid-fast bacilli Culture more sensitive PCR ( AC, vitreous) Diagnosis in response to empiric TX alone
48 Ocular TB Uncommon Biswas reported ocular morbidity in only 1.39% of 1005 patients with active pulmonary and extrapulmonary TB in southern India Definitive diagnosis difficult Acid-fast smear, tissue culture, PCR from ocular tissues May be negative because of low bacterial load Natural inhibitors of Taq polymerase in vitreous decrease yield of PCR Sensitivity of PCR in vitreous samples 33.3% -46.9% Int Ophthalmol ;19(5): Ophthalmology. 2009;116(7): Tuber Lung Dis. 1999; 79(4):
49 PCR diagnosis PCR on aqueous samples from eyes with granulomatous uveitis Twenty out of the 53 samples (37.7%) in the study group were positive One sample out of 17 in the disease control group (5.7%) showed a weakly positive band. No sample from the healthy control group showed a positive PCR. Arora SK, Biswas et al. Diagnostic efficacy of polymerase chain reaction in granulomatous uveitis. Tuber Lung Dis. 1999;79(4):
50 Case FB 54 year old Samoan gentleman with vascular sheathing noted on exam after cataract surgery in the left eye Positive Quanteferon gold TB Vitreous sample negative for TB by PCR Chest Xray unremarkable Started on INH and prednisone

51

52

53 6 weeks later returns with

54 Baysean analysis of TB testing in uveitis Positive predictive value is higher in endemic areas It makes sense to exclude patients with syndromic uveitis Pre immunosuppressive TB testing
55 Should we be testing all comers with ocular inflammatory disease for TB? Non syndromic uveitis Atypical features Endemic regions Granulomatous disease
56 But ocular TB is really tough to treat A Delay in diagnosis and institution of treatment is associated with increased morbidity Therapy reported to be effective in only 40% - 70% of published cases Enucleation rates of up to 30% Eye (Lond). 2011;25(4): Am J Ophthalmol. 2008;146(5): Retina. 1995;15(6):
57 Largest case series from North America 17 patients included with definite ocular TB
58 Mycobacterial Ocular Inflammation Retrospective study Inclusion criteria Positive screening test (TST and/or QuantiFERON) AND response of eye disease to anti-tb therapy Clinical/radiographic evidence of TB elsewhere in body AND response of eye disease to anti-tb therapy Positive biopsy/culture diagnosis elsewhere in body AND response of eye disease to anti-tb therapy Positive culture, PCR or histologic diagnosis from ocular tissue, regardless of response to therapy Patel, Saraiya, Tessler, Goldstein. JAMA Ophthalmol (6);752-8
59 Methods Inclusion criteria: at least one of the following Scleritis Granulomatous iridocyclitis Granulomatous panuveitis Serpiginous-like choroditis Exclusion criteria Purely non-granulomatous anterior uveitis Other diagnosis to explain ocular findings Behcet s disease, other culture or biopsy proven infection



60 Courtesy Sarju Patel M.D. Cornell Deborah Goldstein M.D. NWU
61 Results 17 patients included in the analysis 14 M tuberculosis infection 3 nontuberculous mycobacterial infection African American: 7 (41.2%) Hispanic: 5 (29.4%) White, non-hispanic: 3 (17.6%) 8/17 patients (47%) were born in the United States 12 patients (71%) had a history of possible TB contacts 5 patients (29%) had no identifiable exposure risk
62 Results 17 patients, 9 (53%) had bilateral disease 26 eyes 4 scleritis (15%) 2 granulomatous anterior uveitis (8%) 11 posterior uveitis (42%) 9 panuveitis (35%) Posterior uveitis tended to be bilateral (P =.001) All scleritis was unilateral
63 TB testing 12 of 13 (92.3%) available TST results were positive 7 of 8 (87.5%) QuantiFERON-TB Gold were positive 13 of 15 patients (86.7%) had at least one positive test 2 patients with negative screening test results had localized nontuberculous mycobacterial infection diagnosed with biopsy
64 Chest imaging 4 of 15 (27%) with available results had CXR consistent with tuberculous disease 5 of 9 (56%) had positive CT chest 7 of 15 patients (47%) had any chest imaging consistent with current or prior granulomatous disease
65 Systemic infection 13 of 17 patients (76%) had isolated ocular disease Only 4 (24%) had evidence of systemic TB 1 miliary tuberculosis (TB), 2 lymphadenopathy, 1 active pulmonary TB
66 Delay in referral Average delay in referral to the uveitis service days (range, days) Race was associated with delay in referral to a uveitis specialist on bivariate analysis All non-hispanic Caucasians were referred after 3 years of symptoms Asian patients from endemic countries were referred within 6 months (P =.045) Posterior uveitis was associated with longer delays till referral 1587 days vs 478 days for other manifestations
67 Delay in diagnosis Delay in diagnosis was associated with negative CT chest The 5 patients with CT chest findings c/w TB were diagnosed on average 241 days from symptom onset vs. 989 days for the 4 patients with negative imaging (P =.03; r2 = 0.61)
68 Visual loss Ten eyes (39%) of 8 patients (47%) had irreversible vision loss secondary to TB with best-corrected visual acuity of 20/200 Four of the 13 patients (31%) with disease controlled with antimycobacterial therapy had irreversible profound vision loss All 4 with uncontrolled disease had vision loss (P =.03) Profound visual loss was associated with delay in diagnosis Patients diagnosed and treated after 500 days were more likely to have vision loss than those diagnosed earlier (OR, 20.0; 95% CI, ; P =.03). Those with profound irreversible vision loss were diagnosed in 1260 days on average, compared with 475 days for those without irreversible visual loss
69 Disease control Average time to control of disease (in those patients for whom disease could be controlled) was days ( days) after initiation of ATT Five cases took more than 200 days to achieve control Supplemental use of steroids to control inflammation after initiation of ATT was not associated with shorter periods until control of disease
70 Disease relapse Ten eyes (39%) of 6 patients (35%) had relapsing course Only 2 patients relapsed after a complete course of therapy both of whom had multifocal serpiginous-like choroidopathy 1 after 8 months of isoniazid and rifabutin 1 after 9 months of RIPE Both responded to reinstatement of ATT alone Three patients with multifocal choroiditis relapsed with decrease in ATT between 1 and 4 months but responded when multidrug therapy was reinstituted
71 Disease relapse Relapsing course 80% of patients with posterior uveitis 17% of other patients including panuveitis (P =.03). Relapse was associated with supplemental steroid use Those treated with supplemental oral steroids after instituting ATT were 10 X more likely to relapse compared with those not so treated (univariate analysis (OR, 10.1; 95% CI, ; P =.01)) No correlation between relapse rate and cumulative dose or duration of steroid treatment (data not shown)

72 3 eyes enucleated Loss of the eye 2 after spontaneous perforation from uncontrolled necrotizing nodular scleritis 1 panuveitis in heart transplant patient
73 In summary Think about TB The prognosis for mycobacterial ocular disease is still not great Longer therapy usually required than for systemic disease At least for patients with scleritis, perhaps we should be considering local therapy
74 Conclusions Ocular mycobacterial infection is uncommon 0.5% of 3606 new uveitis referrals seen at a US tertiary referral uveitis service over 15-years met study inclusion criteria Ocular TB typically occurs without clinically apparent systemic disease Absence of pulmonary TB should not delay or prevent anti-tb therapy
75 Conclusions Consider the diagnosis of TB, even in patients who are not from or have not been to endemic countries, regardless of race Caucasians in this series had significant delay in diagnosis, which clearly correlates with increased morbidity

76 Aknoledgements Sarju Patel M.D. Cornell Albert Vitale M.D. Moran Eye Center Photography departments at UIC, Moran Eye Center, UCSF and SUNY Stonybrook
Bilateral multiple choroidal granulomas and systemic vasculitis as presenting features of tuberculosis in an immunocompetent patient
 Kumar et al. Journal of Ophthalmic Inflammation and Infection (2016) 6:40 DOI 10.1186/s12348-016-0109-9 Journal of Ophthalmic Inflammation and Infection BRIEF REPORT Open Access Bilateral multiple choroidal
Kumar et al. Journal of Ophthalmic Inflammation and Infection (2016) 6:40 DOI 10.1186/s12348-016-0109-9 Journal of Ophthalmic Inflammation and Infection BRIEF REPORT Open Access Bilateral multiple choroidal
Role of high-resolution computerized tomography chest in identifying tubercular etiology in patients diagnosed as Eales disease
 Kharel (Sitaula) et al. Journal of Ophthalmic Inflammation and Infection (2017) 7:4 DOI 10.1186/s12348-016-0120-1 Journal of Ophthalmic Inflammation and Infection ORIGINAL RESEARCH Open Access Role of
Kharel (Sitaula) et al. Journal of Ophthalmic Inflammation and Infection (2017) 7:4 DOI 10.1186/s12348-016-0120-1 Journal of Ophthalmic Inflammation and Infection ORIGINAL RESEARCH Open Access Role of
Re-emerging infections: Syphilis & Tuberculosis
 Re-emerging infections: Syphilis & Tuberculosis Nicholas Jones Manchester Royal Eye Hospital Syphilis and TB - historical plagues? Syphilis incidence over 40yrs Manchester: Manchester: The Syphilis Capital
Re-emerging infections: Syphilis & Tuberculosis Nicholas Jones Manchester Royal Eye Hospital Syphilis and TB - historical plagues? Syphilis incidence over 40yrs Manchester: Manchester: The Syphilis Capital
Management of uveitis
 Management of uveitis DR. ANUPAMA KARANTH Anti-inflammatory agents -itis = inflammation Treatment : stop inflammation Use anti-inflammatory drugs Most potent of such agents : Corticosteroids Corticosteroids
Management of uveitis DR. ANUPAMA KARANTH Anti-inflammatory agents -itis = inflammation Treatment : stop inflammation Use anti-inflammatory drugs Most potent of such agents : Corticosteroids Corticosteroids
Acute Retinal Necrosis Secondary to Varicella Zoster Virus in an Immunosuppressed Post-Kidney Transplant Patient
 CM&R Rapid Release. Published online ahead of print September 20, 2012 as Aperture Acute Retinal Necrosis Secondary to Varicella Zoster Virus in an Immunosuppressed Post-Kidney Transplant Patient Elizabeth
CM&R Rapid Release. Published online ahead of print September 20, 2012 as Aperture Acute Retinal Necrosis Secondary to Varicella Zoster Virus in an Immunosuppressed Post-Kidney Transplant Patient Elizabeth
In our paper, we suggest that tuberculosis and sarcoidosis are two ends of the same spectrum. Given the pathophysiological and clinical link between
 In our paper, we suggest that tuberculosis and sarcoidosis are two ends of the same spectrum. Given the pathophysiological and clinical link between the two, we also propose a classification system for
In our paper, we suggest that tuberculosis and sarcoidosis are two ends of the same spectrum. Given the pathophysiological and clinical link between the two, we also propose a classification system for
Sarcoidosis and Uveitis
 Sarcoidosis and Uveitis Nicholas Jones Royal Eye Hospital Manchester, UK Sarcoidosis a multisystem chronic inflammation causing multifocal non-caseating granulomas BUT Diagnosis often made indirectly (without
Sarcoidosis and Uveitis Nicholas Jones Royal Eye Hospital Manchester, UK Sarcoidosis a multisystem chronic inflammation causing multifocal non-caseating granulomas BUT Diagnosis often made indirectly (without
Eye (2013) 27, & 2013 Macmillan Publishers Limited All rights reserved X/13 S Basu, S Nayak, TR Padhi and T Das
 27, & 2013 Macmillan Publishers Limited All rights reserved X/13 S Basu, S Nayak, TR Padhi and T Das") (2013) 27, 657 662 & 2013 Macmillan Publishers Limited All rights reserved 0950-222X/13 www.nature.com/eye Progressive ocular inflammation following antitubercular therapy for presumed ocular tuberculosis
(2013) 27, 657 662 & 2013 Macmillan Publishers Limited All rights reserved 0950-222X/13 www.nature.com/eye Progressive ocular inflammation following antitubercular therapy for presumed ocular tuberculosis
Ocular Tuberculosis- An update
 December 2009 Biswas - Ocular tuberculosis 351 MAJOR REVIEW Ocular Tuberculosis- An update Dr. J. Biswas MS Introduction Tuberculosis (TB) is an air-borne disease that affects one-third of the world s
December 2009 Biswas - Ocular tuberculosis 351 MAJOR REVIEW Ocular Tuberculosis- An update Dr. J. Biswas MS Introduction Tuberculosis (TB) is an air-borne disease that affects one-third of the world s
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculous uveitis: association between anti-tuberculous therapy and clinical response in a non-endemic country
 Bajema et al. Journal of Ophthalmic Inflammation and Infection (2017) 7:19 DOI 10.1186/s12348-017-0137-0 Journal of Ophthalmic Inflammation and Infection ORIGINAL RESEARCH Open Access Tuberculous uveitis:
Bajema et al. Journal of Ophthalmic Inflammation and Infection (2017) 7:19 DOI 10.1186/s12348-017-0137-0 Journal of Ophthalmic Inflammation and Infection ORIGINAL RESEARCH Open Access Tuberculous uveitis:
Various presentations of herpes simplex retinochoroiditis A case series
 Various presentations of herpes simplex retinochoroidits 47 Various presentations of herpes simplex retinochoroiditis A case series M. T. K. Perera 1, T. S. Keragala 1, M. Gamage 2 The Journal of the College
Various presentations of herpes simplex retinochoroidits 47 Various presentations of herpes simplex retinochoroiditis A case series M. T. K. Perera 1, T. S. Keragala 1, M. Gamage 2 The Journal of the College
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Intraocular Tuberculosis
 Eye (1990) 4, 486-492 Intraocular Tuberculosis P. H. ROSEN*, D. 1. SPALTON and E. M. GRAHAM London Summary 1Welve patients with a diagnosis of intraocular tuberculosis are described. Nine patients presented
Eye (1990) 4, 486-492 Intraocular Tuberculosis P. H. ROSEN*, D. 1. SPALTON and E. M. GRAHAM London Summary 1Welve patients with a diagnosis of intraocular tuberculosis are described. Nine patients presented
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
Rare Presentation of Ocular Toxoplasmosis
 Case Report Rare Presentation of Ocular Toxoplasmosis Rakhshandeh Alipanahi MD From Department of Ophthalmology, Nikookari Eye Hospital, Tabriz University of Medical Sciences, Tabriz, Iran. Correspondence:
Case Report Rare Presentation of Ocular Toxoplasmosis Rakhshandeh Alipanahi MD From Department of Ophthalmology, Nikookari Eye Hospital, Tabriz University of Medical Sciences, Tabriz, Iran. Correspondence:
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Moncef Khairallah, MD
 Moncef Khairallah, MD Department of Ophthalmology, Fattouma Bourguiba University Hospital Faculty of Medicine, University of Monastir Monastir, Tunisia INTRODUCTION IU: anatomic form of uveitis involving
Moncef Khairallah, MD Department of Ophthalmology, Fattouma Bourguiba University Hospital Faculty of Medicine, University of Monastir Monastir, Tunisia INTRODUCTION IU: anatomic form of uveitis involving
Case Study: TB-HIV co-infection
 Case Study: TB-HIV co-infection Julia Greenleaf, RN, MPH Public Health Nurse Public Health Madison & Dane County With guest appearance by Julie Tans-Kersten, MS, BSMT (ASCP) Director, WI TB Program 33
Case Study: TB-HIV co-infection Julia Greenleaf, RN, MPH Public Health Nurse Public Health Madison & Dane County With guest appearance by Julie Tans-Kersten, MS, BSMT (ASCP) Director, WI TB Program 33
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Characteristics of Mycobacterium
 Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Scleritis LEN V KOH OD
 Scleritis LEN V KOH OD 2014 PUCO 1 Introduction A painful, destructive, and potentially blinding disorder Highly symptomatic High association with systemic disease Immunosuppresssive agents 2014 PUCO 2
Scleritis LEN V KOH OD 2014 PUCO 1 Introduction A painful, destructive, and potentially blinding disorder Highly symptomatic High association with systemic disease Immunosuppresssive agents 2014 PUCO 2
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of
 TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
My heart is racing. Managing Complex Cases. Case 1. Case 1
 Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Choroidal Neovascularization in Sympathetic Ophthalmia
 Choroidal Neovascularization in Sympathetic Ophthalmia Lucia Sobrin, Miguel Cordero Coma, C. Stephen Foster Case Report A 49-year-old man presented after a ruptured globe repair of his left eye status
Choroidal Neovascularization in Sympathetic Ophthalmia Lucia Sobrin, Miguel Cordero Coma, C. Stephen Foster Case Report A 49-year-old man presented after a ruptured globe repair of his left eye status
o White dot syndromes pattern recognition o Activity and damage o Quality of life o Key points o Idiopathic o Sarcoidosis o Multiple sclerosis
 Introduction Clinical Assessment of Posterior Uveitis Philip I. Murray Centre for Translational Inflammation Research University of Birmingham Birmingham and Midland Eye Centre o Classification of uveitis
Introduction Clinical Assessment of Posterior Uveitis Philip I. Murray Centre for Translational Inflammation Research University of Birmingham Birmingham and Midland Eye Centre o Classification of uveitis
Optical coherence tomography findings in a child with posterior scleritis
 European Journal of Ophthalmology / Vol. 18 no. 6, 2008 / pp. 1007-1010 SHORT OMMUNITIONS & SE REPORTS Optical coherence tomography findings in a child with posterior scleritis H. ERDÖL, M. KOL,. TÜRK
European Journal of Ophthalmology / Vol. 18 no. 6, 2008 / pp. 1007-1010 SHORT OMMUNITIONS & SE REPORTS Optical coherence tomography findings in a child with posterior scleritis H. ERDÖL, M. KOL,. TÜRK
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
BroadcastMed Unilateral Panuveitis
 BroadcastMed Unilateral Panuveitis WENDY SMITH: Hello, I'm Dr. Wendy Smith of the Department of Ophthalmology. I'm happy to be here today to discuss an interesting case involving a patient with panuveitis.
BroadcastMed Unilateral Panuveitis WENDY SMITH: Hello, I'm Dr. Wendy Smith of the Department of Ophthalmology. I'm happy to be here today to discuss an interesting case involving a patient with panuveitis.
Tuberculosis Populations at Risk
 Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
TB Intensive San Antonio, Texas December 1-3, 2010
 TB Intensive San Antonio, Texas December 1-3, 2010 TB Case Presentations Doug Hornick, MD; Iowa U Medical School December 1, 2010 Pulmonary Fascinomas with a Tuberculous Attitude Douglas B. Hornick, MD
TB Intensive San Antonio, Texas December 1-3, 2010 TB Case Presentations Doug Hornick, MD; Iowa U Medical School December 1, 2010 Pulmonary Fascinomas with a Tuberculous Attitude Douglas B. Hornick, MD
Uveitis. Pt Info Brochure. Q: What is Uvea?
 Pt Info Brochure Uveitis Q: What is Uvea? A: Uvea is the middle layer of the eye. It is the most vascular structure of the eye. It provides nutrition to the other parts of the eye. The uvea is made up
Pt Info Brochure Uveitis Q: What is Uvea? A: Uvea is the middle layer of the eye. It is the most vascular structure of the eye. It provides nutrition to the other parts of the eye. The uvea is made up
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Misdiagnosed Vogt-Koyanagi-Harada (VKH) disease and atypical central serous chorioretinopathy (CSC)
 disease and atypical central serous chorioretinopathy (CSC)") HPTER 12 Misdiagnosed Vogt-Koyanagi-Harada (VKH) disease and atypical central serous chorioretinopathy (S) linical Features VKH disease is a bilateral granulomatous panuveitis often associated with exudative
HPTER 12 Misdiagnosed Vogt-Koyanagi-Harada (VKH) disease and atypical central serous chorioretinopathy (S) linical Features VKH disease is a bilateral granulomatous panuveitis often associated with exudative
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Diagnosis Latent Tuberculosis. Disclosures. Case
 Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Eye Signs in Tuberculosis
 Eye Signs in Tuberculosis HL Trivedi*, Ramesh Venkatesh** Introduction Tuberculosis is very common in India and hence it is very essential for the general practitioners treating patients to be aware of
Eye Signs in Tuberculosis HL Trivedi*, Ramesh Venkatesh** Introduction Tuberculosis is very common in India and hence it is very essential for the general practitioners treating patients to be aware of
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
UVEITIS. Dr. Yılmaz ÖZYAZGAN
 UVEITIS Dr. Yılmaz ÖZYAZGAN UVEITIS DEFINITION BY STRICT DEFINITION, UVEITIS IS AN INFLAMMATION OF UVEAL TRACT. BUT IN PRACTICAL, IT IS GENERALLY NOT RESTRICTED TO THE UVEA AND INVOLVES OTHER ADJACENT
UVEITIS Dr. Yılmaz ÖZYAZGAN UVEITIS DEFINITION BY STRICT DEFINITION, UVEITIS IS AN INFLAMMATION OF UVEAL TRACT. BUT IN PRACTICAL, IT IS GENERALLY NOT RESTRICTED TO THE UVEA AND INVOLVES OTHER ADJACENT
Cases CFEH. CFEH Facebook Case #4
 CFEH Cases CFEH Facebook Case #4 A 42 year old female has noticed a floater in her left eye for many years but no flashes. She also reports hazy vision in this eye that has been present all her life. She
CFEH Cases CFEH Facebook Case #4 A 42 year old female has noticed a floater in her left eye for many years but no flashes. She also reports hazy vision in this eye that has been present all her life. She
TB Intensive San Antonio, Texas November 29-December 2, 2011
 TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
Uveitis unplugged: systemic therapy
 Uveitis unplugged: systemic therapy Hobart 2017 Peter McCluskey Save Sight Institute Sydney Eye Hospital Sydney Medical School University of Sydney Sydney Australia No financial or proprietary interest
Uveitis unplugged: systemic therapy Hobart 2017 Peter McCluskey Save Sight Institute Sydney Eye Hospital Sydney Medical School University of Sydney Sydney Australia No financial or proprietary interest
Objectives. Highlight typical feature of TB pericarditis. How to make a diagnosis. How to treat TB pericarditis
 Dr. Conteh Objectives Highlight typical feature of TB pericarditis How to make a diagnosis How to treat TB pericarditis New evidence for adjunctive corticosteroid Introduction TB pericarditis occurs in
Dr. Conteh Objectives Highlight typical feature of TB pericarditis How to make a diagnosis How to treat TB pericarditis New evidence for adjunctive corticosteroid Introduction TB pericarditis occurs in
Nasreen A. Syed, MD F.C. Blodi Eye Pathology Laboratory University of Iowa
 Nasreen A. Syed, MD F.C. Blodi Eye Pathology Laboratory University of Iowa No financial interest in any of the material discussed in this presentation There will be discussion of off label use of medications,
Nasreen A. Syed, MD F.C. Blodi Eye Pathology Laboratory University of Iowa No financial interest in any of the material discussed in this presentation There will be discussion of off label use of medications,
Retina Grand Rounds. Stephen Huddleston MD Charles Retina Institute University of Tennessee Hamilton Eye Institute
 Retina Grand Rounds Stephen Huddleston MD Charles Retina Institute University of Tennessee Hamilton Eye Institute Fundus Autoflourescence 2013 2016 Plaquenil Toxicity Excellent treatment for a variety
Retina Grand Rounds Stephen Huddleston MD Charles Retina Institute University of Tennessee Hamilton Eye Institute Fundus Autoflourescence 2013 2016 Plaquenil Toxicity Excellent treatment for a variety
TB in Foreign Born and High Risk Populations
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 TB in Foreign Born and High Risk Populations John J. Nava, M.D. December 9, 2009 Tuberculosis in High Risk Populations and the Foreign Born
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 TB in Foreign Born and High Risk Populations John J. Nava, M.D. December 9, 2009 Tuberculosis in High Risk Populations and the Foreign Born
Surgery in patients with uveitis. Lyndell Lim and Anthony Hall
 Surgery in patients with uveitis Lyndell Lim and Anthony Hall Disclosures Off label treatments Paid advisory board Bayer Paid research support Allergan (makers of Ozurdex) Paid research support B and L
Surgery in patients with uveitis Lyndell Lim and Anthony Hall Disclosures Off label treatments Paid advisory board Bayer Paid research support Allergan (makers of Ozurdex) Paid research support B and L
Uveitis literature 2014: the year in review. Russell N. Van Gelder, MD, PhD Department of Ophthalmology University of Washington Seattle, WA
 Uveitis literature 2014: the year in review Russell N. Van Gelder, MD, PhD Department of Ophthalmology University of Washington Seattle, WA Disclosures RVG serves as Associate Editor of IOVS Editorial
Uveitis literature 2014: the year in review Russell N. Van Gelder, MD, PhD Department of Ophthalmology University of Washington Seattle, WA Disclosures RVG serves as Associate Editor of IOVS Editorial
Directed conjunctival biopsy and impact of histologic sectioning methodology on the diagnosis of ocular sarcoidosis
 Bui et al. Journal of Ophthalmic Inflammation and Infection 2014, 4:8 ORIGINAL RESEARCH Directed conjunctival biopsy and impact of histologic sectioning methodology on the diagnosis of ocular sarcoidosis
Bui et al. Journal of Ophthalmic Inflammation and Infection 2014, 4:8 ORIGINAL RESEARCH Directed conjunctival biopsy and impact of histologic sectioning methodology on the diagnosis of ocular sarcoidosis
Evolving therapies for posterior uveitis. Infliximab (Remicade) Infliximab: pharmacology. FDA-approved monoclonal antibody therapy Target
 Infliximab: pharmacology. FDA-approved monoclonal antibody therapy Target") Evolving therapies for posterior uveitis Sam Dahr, M.D. September 17, 2005 Midwest Ophthalmology Conference Infliximab (Remicade) FDA approved for Crohn s disease, rheumatoid arthritis, and psoriatic arthritis
Evolving therapies for posterior uveitis Sam Dahr, M.D. September 17, 2005 Midwest Ophthalmology Conference Infliximab (Remicade) FDA approved for Crohn s disease, rheumatoid arthritis, and psoriatic arthritis
TB Classification (ATS/CDC)
") bits and pieces Lisa Chen, MD UCSF Pulmonary/Critical Care Curry International Tuberculosis Center 10/2017 TB Classification (ATS/CDC) TB0 No tuberculosis exposure, not infected TB1 Tuberculosis exposure,
bits and pieces Lisa Chen, MD UCSF Pulmonary/Critical Care Curry International Tuberculosis Center 10/2017 TB Classification (ATS/CDC) TB0 No tuberculosis exposure, not infected TB1 Tuberculosis exposure,
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers
 Questions and Answers for Health Care Providers") Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Imaging in uveitis. Anthony Hall
 Imaging in uveitis Anthony Hall Causes of Vision Loss in Uveitis 1. Cystoid macular oedema 26% 2. Cataract 19% 3. Glaucoma 11% 4. Permanent macular damage 5% Rothova et al BJO 1996; 80: 332-336 Macular
Imaging in uveitis Anthony Hall Causes of Vision Loss in Uveitis 1. Cystoid macular oedema 26% 2. Cataract 19% 3. Glaucoma 11% 4. Permanent macular damage 5% Rothova et al BJO 1996; 80: 332-336 Macular
Tuberculosis Update. Topics to be Addressed
 Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Differential diagnosis of posterior uveitis
 Differential diagnosis of posterior uveitis Diagnostic approach 45-year old male. Floaters and decreased vision since 1 week Fever, lymphadenopathy, myalgias, night sweats, two months ago Oral ulcer sporadically
Differential diagnosis of posterior uveitis Diagnostic approach 45-year old male. Floaters and decreased vision since 1 week Fever, lymphadenopathy, myalgias, night sweats, two months ago Oral ulcer sporadically
Macular Hole Associated with Vogt-Koyanagi-Harada Disease at the Acute Uveitic Stage
 Published online: September 15, 2015 2015 The Author(s) Published by S. Karger AG, Basel 1663 2699/15/0063 0328$39.50/0 This article is licensed under the Creative Commons Attribution-NonCommercial 4.0
Published online: September 15, 2015 2015 The Author(s) Published by S. Karger AG, Basel 1663 2699/15/0063 0328$39.50/0 This article is licensed under the Creative Commons Attribution-NonCommercial 4.0
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Uveitis. What is Uveitis?
 Uveitis What is Uveitis? Uveitis [u-vee-i-tis] is a term for inflammation of the eye. It can occur in one eye or both eyes and affects the layer of the eye called the uvea [u-vee-uh]. It also can be associated
Uveitis What is Uveitis? Uveitis [u-vee-i-tis] is a term for inflammation of the eye. It can occur in one eye or both eyes and affects the layer of the eye called the uvea [u-vee-uh]. It also can be associated
Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts
 Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Patient AB. Born in 1961 PED
 Clinical Atlas Patient AB Born in 1961 PED Autofluorescence Dilated 45 EasyScan Zero-dilation IR 45 Fundus Dilated 45 In the fundus photos (Canon CX1) the PED is not able to be seen. However, the extent
Clinical Atlas Patient AB Born in 1961 PED Autofluorescence Dilated 45 EasyScan Zero-dilation IR 45 Fundus Dilated 45 In the fundus photos (Canon CX1) the PED is not able to be seen. However, the extent
Why Is Imaging Critical in My Uveitis Practice?
 Why Is Imaging Critical in My Uveitis Practice? Dilraj S. Grewal, MD Developed in collaboration Imaging Is the Backbone of Uveitis Workup and Monitoring Treatment Response FP FAF B- scan Multimodal Imaging
Why Is Imaging Critical in My Uveitis Practice? Dilraj S. Grewal, MD Developed in collaboration Imaging Is the Backbone of Uveitis Workup and Monitoring Treatment Response FP FAF B- scan Multimodal Imaging
Nausheen Khuddus, MD Melissa Elder, MD, PhD
 Nausheen Khuddus, MD Melissa Elder, MD, PhD Nausheen Khuddus, MD Pediatric Ophthalmologist and Strabismus Specialist Accent Physicians Gainesville, Florida What Is Uveitis? Uveitis is caused by inflammatory
Nausheen Khuddus, MD Melissa Elder, MD, PhD Nausheen Khuddus, MD Pediatric Ophthalmologist and Strabismus Specialist Accent Physicians Gainesville, Florida What Is Uveitis? Uveitis is caused by inflammatory
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Disseminated Nocardiosis with subretinal abscess in a patient with nephrotic syndrome-a case report
 Xu et al. BMC Ophthalmology (2018) 18:234 https://doi.org/10.1186/s12886-018-0883-2 CASE REPORT Open Access Disseminated Nocardiosis with subretinal abscess in a patient with nephrotic syndrome-a case
Xu et al. BMC Ophthalmology (2018) 18:234 https://doi.org/10.1186/s12886-018-0883-2 CASE REPORT Open Access Disseminated Nocardiosis with subretinal abscess in a patient with nephrotic syndrome-a case
Head prof. MUDr. E. Vlková, CSc.
 MUDr. Karkanová Michala, Oční klinika LF MU a FN Brno Head prof. MUDr. E. Vlková, CSc. 3 parts: iris (iris) ciliary body (corpus ciliare) choroid (choroidea) Function: regulating the entry of light into
MUDr. Karkanová Michala, Oční klinika LF MU a FN Brno Head prof. MUDr. E. Vlková, CSc. 3 parts: iris (iris) ciliary body (corpus ciliare) choroid (choroidea) Function: regulating the entry of light into
11/1/2017. Disclosures. Update In Tuberculosis, Indiana Outline/Objectives. Pathogenesis of M.tb Global/U.S. TB Burden, 2016
 Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,
Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,
Research in Tuberculosis: Translation into Practice
 Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
Annual Tuberculosis Report Oregon 2007
 Annual Tuberculosis Report Oregon 7 Oregon Department of Human Services Public Health Division TB Program April 8 Page 2 Table of Contents Charts Chart 1 TB Incidence in the US and Oregon, 1985-7.. page
Annual Tuberculosis Report Oregon 7 Oregon Department of Human Services Public Health Division TB Program April 8 Page 2 Table of Contents Charts Chart 1 TB Incidence in the US and Oregon, 1985-7.. page
The Diagnosis of Active TB. Deborah McMahan, MD TB Intensive September 28, 2017
 The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
Recognizing MDR-TB in Children. Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention February 2016
 Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Department of Ophthalmology
 Department of Ophthalmology Period : 02/July/18 to 30/August/18 Semester : 7 th Semester Lecture Lesson Plan Sr. Date Topic Lesson plan Name of Faculty No. 1 02.07.18 Lens- Lens-Anatomy, Classification
Department of Ophthalmology Period : 02/July/18 to 30/August/18 Semester : 7 th Semester Lecture Lesson Plan Sr. Date Topic Lesson plan Name of Faculty No. 1 02.07.18 Lens- Lens-Anatomy, Classification
Rehuka Khurana, MD, MPH has the following disclosures to make:
 Case Presentation Steps to a Systematic Approach to Diagnosis of TB Case Presentation Steps to a Systematic Approach to Diagnosis of TB Renuka Khurana, MD, MPH March 13, 2015 TB for Pulmonologist March
Case Presentation Steps to a Systematic Approach to Diagnosis of TB Case Presentation Steps to a Systematic Approach to Diagnosis of TB Renuka Khurana, MD, MPH March 13, 2015 TB for Pulmonologist March
Utilizing All the Tools in the TB Toolbox
 Utilizing All the Tools in the TB Toolbox Sandra Morano, B.A., R.N. Public Health Nurse, City of Stamford, CT TB Talk The New England TB Consortium March 18, 2010 Background TB Program, City of Stamford,
Utilizing All the Tools in the TB Toolbox Sandra Morano, B.A., R.N. Public Health Nurse, City of Stamford, CT TB Talk The New England TB Consortium March 18, 2010 Background TB Program, City of Stamford,
Ocular Pathology. I. Congenital and/or developmental. A. Trisomy 21. Hypertelorism (widely spaced eyes) Keratoconus (cone shaped cornea)
 Keratoconus (cone shaped cornea)") I. Congenital and/or developmental Robbins Pathologic Basis of Disease, 6 th Ed. A. Trisomy 21 Hypertelorism (widely spaced eyes) Keratoconus (cone shaped cornea) Focal hypoplasia of iris Cataracts frequently
I. Congenital and/or developmental Robbins Pathologic Basis of Disease, 6 th Ed. A. Trisomy 21 Hypertelorism (widely spaced eyes) Keratoconus (cone shaped cornea) Focal hypoplasia of iris Cataracts frequently
Tuberculosis Screening and Targeted Testing of College and University Students: Developing a Best Practice Approach:
 Tuberculosis Screening and Targeted Testing of College and University Students: Developing a Best Practice Approach: Lori A. Soos MA, BSN, RN, Niagara University Deborah Penoyer, MS, RN, SUNY Geneseo Learning
Tuberculosis Screening and Targeted Testing of College and University Students: Developing a Best Practice Approach: Lori A. Soos MA, BSN, RN, Niagara University Deborah Penoyer, MS, RN, SUNY Geneseo Learning
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
TB the basics. (Dr) Margaret (DHA) and John (INZ)
 Margaret (DHA) and John (INZ)") TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
Pre-Treatment Evaluation. Treatment of Latent TB Infection (LTBI) Initiating Treatment: Patient Education. Before initiating treatment for LTBI:
 Initiating Treatment: Patient Education. Before initiating treatment for LTBI:") Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
LATENT TUBERCULOSIS. Robert F. Tyree, MD
 LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
Pattern of Uveitis in Saudi Female Patients in Western Region of Saudi Arabia
 JKAU: Med. Sci., Vol. 19 No. 3, pp: 73-83 (2012 A.D. / 1433 A.H.) DOI: 10.4197/Med. 19-3.6 Pattern of Uveitis in Saudi Female Patients in Western Region of Saudi Arabia Nizamuddin Shaik Hakim Mohammad
JKAU: Med. Sci., Vol. 19 No. 3, pp: 73-83 (2012 A.D. / 1433 A.H.) DOI: 10.4197/Med. 19-3.6 Pattern of Uveitis in Saudi Female Patients in Western Region of Saudi Arabia Nizamuddin Shaik Hakim Mohammad
Dr. D. Y. Patil Medical College, Pimpri, Pune
 Dr. D. Y. Patil Medical College, Pimpri, Pune - 411 018 Period : 04/July/16 to 22/September/16 Semester : 7 th Semester Department : Ophthalmology Lecture Lesson Plan Sr No Date Topic Learning objectives
Dr. D. Y. Patil Medical College, Pimpri, Pune - 411 018 Period : 04/July/16 to 22/September/16 Semester : 7 th Semester Department : Ophthalmology Lecture Lesson Plan Sr No Date Topic Learning objectives
Approaches to LTBI Diagnosis
 Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Multimodal imaging of retinal metastasis masquerading as an acute retinal necrosis
 https://doi.org/10.1186/s40942-018-0149-4 International Journal of Retina and Vitreous CASE REPORT Multimodal imaging of retinal metastasis masquerading as an acute retinal necrosis Fukutaro Mano 1*, Stephen
https://doi.org/10.1186/s40942-018-0149-4 International Journal of Retina and Vitreous CASE REPORT Multimodal imaging of retinal metastasis masquerading as an acute retinal necrosis Fukutaro Mano 1*, Stephen
Necrotizing retinitis of multifactorial etiology
 Romanian Journal of Ophthalmology, Volume 61, Issue 1, January-March 2017. pp:49-53 CASE REPORT Necrotizing retinitis of multifactorial etiology Pirvulescu Ruxandra Angela* **, Popa Cherecheanu Alina*
Romanian Journal of Ophthalmology, Volume 61, Issue 1, January-March 2017. pp:49-53 CASE REPORT Necrotizing retinitis of multifactorial etiology Pirvulescu Ruxandra Angela* **, Popa Cherecheanu Alina*
Difficult Diagnosis: Case History. 7 months prior, she happened to have undergone a C-spine MRI after a car accident
 Relevant Disclosures: None Difficult Diagnosis: Recent Advances in Neurology 2013 Jeffrey M. Gelfand, MD Assistant Professor UCSF Neuroinflammation and MS Center UCSF Department of Neurology Case History
Relevant Disclosures: None Difficult Diagnosis: Recent Advances in Neurology 2013 Jeffrey M. Gelfand, MD Assistant Professor UCSF Neuroinflammation and MS Center UCSF Department of Neurology Case History
Syphilis: Management Challenges
 Syphilis: Management Challenges Khalil Ghanem & Susan Tuddenham Johns Hopkins University School of Medicine Baltimore, MD USA uwptc@uw.edu uwptc.org 206-685-9850 Patient 1 36 year old gay man with sudden
Syphilis: Management Challenges Khalil Ghanem & Susan Tuddenham Johns Hopkins University School of Medicine Baltimore, MD USA uwptc@uw.edu uwptc.org 206-685-9850 Patient 1 36 year old gay man with sudden
LABORATORY SCIENCES. Experimental Ocular Tuberculosis in Guinea Pigs
 LABORATORY SCIENCES Experimental Ocular Tuberculosis in Guinea Pigs Narsing A. Rao, MD; Thomas A. Albini, MD; Mirnalini Kumaradas, MD; Michael L. Pinn, BS; Mostafa M. Fraig, MD; Petros C. Karakousis, MD
LABORATORY SCIENCES Experimental Ocular Tuberculosis in Guinea Pigs Narsing A. Rao, MD; Thomas A. Albini, MD; Mirnalini Kumaradas, MD; Michael L. Pinn, BS; Mostafa M. Fraig, MD; Petros C. Karakousis, MD
Case Report Pulmonary Sarcoidosis following Etanercept Treatment
 Case Reports in Rheumatology Volume 2012, Article ID 724013, 4 pages doi:10.1155/2012/724013 Case Report Pulmonary Sarcoidosis following Etanercept Treatment Kuljeet Bhamra and Richard Stevens Department
Case Reports in Rheumatology Volume 2012, Article ID 724013, 4 pages doi:10.1155/2012/724013 Case Report Pulmonary Sarcoidosis following Etanercept Treatment Kuljeet Bhamra and Richard Stevens Department
ISPUB.COM. An Atypical Presentation of Posterior Scleritis. A Ramanathan, A Gaur CASE REPORT
 ISPUB.COM The Internet Journal of Ophthalmology and Visual Science Volume 8 Number 2 A Ramanathan, A Gaur Citation A Ramanathan, A Gaur.. The Internet Journal of Ophthalmology and Visual Science. 2009
ISPUB.COM The Internet Journal of Ophthalmology and Visual Science Volume 8 Number 2 A Ramanathan, A Gaur Citation A Ramanathan, A Gaur.. The Internet Journal of Ophthalmology and Visual Science. 2009
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash