Survival Outcomes with Short-Course Radiotherapy in Elderly Patients with Glioblastoma: Data from a Randomized Phase III Trial
|
|
|
- Randolf O’Connor’
- 5 years ago
- Views:
Transcription
30738-1 10.1016/j.")
1 Accepted Manuscript Survival Outcomes with Short-Course Radiotherapy in Elderly Patients with Glioblastoma: Data from a Randomized Phase III Trial Douglas Guedes de Castro, Juliana Matiello, Wilson Roa, Sunita Ghosh, Lucyna Kepka, Narendra Kumar, Valery Sinaika, Darejan Lomidze, Dalenda Hentati, Eduardo Rosenblatt, Elena Fidarova PII: DOI: Reference: ROB S (17) /j.ijrobp To appear in: International Journal of Radiation Oncology Biology Physics Received Date: 1 November 2016 Revised Date: 12 March 2017 Accepted Date: 22 March 2017 Please cite this article as: Guedes de Castro D, Matiello J, Roa W, Ghosh S, Kepka L, Kumar N, Sinaika V, Lomidze D, Hentati D, Rosenblatt E, Fidarova E, Survival Outcomes with Short-Course Radiotherapy in Elderly Patients with Glioblastoma: Data from a Randomized Phase III Trial, International Journal of Radiation Oncology Biology Physics (2017), doi: /j.ijrobp This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
2 Survival Outcomes with Short-Course Radiotherapy in Elderly Patients with Glioblastoma: Data from a Randomized Phase III Trial Short-Course Radiotherapy in Elderly Patients with Glioblastoma - Douglas Guedes de Castro o AC Camargo Cancer Center, São Paulo, Brazil. o Corresponding Author, address: rua Alice de Castro, 67, apt. 61, São Paulo - SP, Brazil, ZIP Code: dougguedes@uol.com.br, phone number: Juliana Matiello o Irmandade da Santa Casa de Miresicórdia de Porto Alegre, Porto Alegre, Brazil. - Wilson Roa o University of Alberta, Alberta Health Services-Cancer Control, Edmonton, Canada. - Sunita Ghosh o University of Alberta, Alberta Health Services-Cancer Control, Edmonton, Canada. - Lucyna Kepka o Warmia and Mazury Oncology Center, Olsztyn, Poland. - Narendra Kumar o Postgraduate Institute of Medical Education and Research, Chandigarh, India.
3 - Valery Sinaika o N.N. Alexandrov National Cancer Centre of Belarus, Minsk, Belarus. - Darejan Lomidze o High Technology Medical Center, Tbilisi, Georgia. - Dalenda Hentati o Institut National de Cancer Salah Azaiz, Bab Saadoum, Tunisia. - Eduardo Rosenblatt o International Atomic Energy Agency, Vienna, Austria. - Elena Fidarova o International Atomic Energy Agency, Vienna, Austria. The authors declare that they have no confict of interest. The original trial, from which we did this post-hoc analysis, was supported by International Atomic Energy Agency.
4 Summary In this post-hoc, subset analysis of an International Atomic Energy Agency randomized phase III trial restricted to elderly patients 65 years, the shortcourse radiotherapy regimen of 25 Gy in 5 fractions was not inferior to commonly used regimen of 40 Gy in 15 fractions in terms of overall and progression-free survival.
5 Survival Outcomes with Short-Course Radiotherapy in Elderly Patients with Glioblastoma: Data from a Randomized Phase III Trial. Abstract Purpose: To perform a subset analysis of survival outcomes in elderly patients with glioblastoma (GBM) from a randomized phase III trial comparing two short-course radiotherapy (RT) regimens in elderly and/or frail patients. Methods and Materials: The original trial population included elderly and/or frail patients diagnosed with GBM. Patients joined the phase III, randomized, multicenter, prospective, non-inferiority trial and were assigned to one of two groups in a 1:1 ratio to either shortcourse RT (25 Gy in 5 fractions, arm 1) or commonly used RT (40 Gy in 15 fractions, arm 2) and stratified by age (< and 65 years), Karnofsky performance status, and extent of surgery. For the subset analysis in this study, only patients 65 years were evaluated (elderly and frail patients were defined as age 65 years and KPS 50-70%; elderly and not frail patients were defined as age 65 years and KPS %), resulting in 61 out of 98 initial patients, with 26 patients randomized to arm 1 and 35 to arm 2. Results: In this unplanned analysis, the short-course RT results were not statistically significant different to commonly used RT in elderly patients. The median overall survival time was 6.8 months (95% CI, 4.5 to 9.1 months) in arm 1 and 6.2 months (95% CI, 4.7 to 7.7 months) in arm 2 (P = 0.936). Median progression-free survival time was 4.3 months (95% CI, 2.6 to 5.9 months) in arm 1 and 3.2 months (95% CI,.1 to 6.3 months) in arm 2 (P = 0.706). Conclusions: A short-course RT regimen of 25 Gy in 5 fractions is an acceptable treatment option for patients over 65 years old, mainly for those with poor performance or contraindication to chemotherapy, which would be indicated in cases of methylated MGMT promoted tumors.
6 Introduction Glioblastoma (GBM) is the most frequent malignant primary brain tumor, with an increasing incidence-adjusted rate for the age and nearly half of patients being older than 65 years (1,2). The therapeutic management of older patients with GBM is challenging as they tend to have limited survival and there are scarce phase III data to support treatment choices. Keime-Guibert et al. assessed, in a prospective, randomized trial, supportive care versus supportive care plus radiation therapy (RT) with 50 Gy in 25 daily fractions in patients older than 70 years and demonstrated that the combined approach fared better, with a median survival time of 29.1 weeks compared with 16.9 weeks, with no further deterioration in the performance status, health-related quality of life or cognitive functions (3). Roa et al. prospectively demonstrated no difference in the survival results in elderly patients with GBM receiving 60 Gy in 30 fractions versus 40 Gy in 15 fractions, with an overall survival (OS) of 5.1 versus 5.5 months, respectively (4). Because GBM patients with unfavorable prognostic factors benefit less from aggressive treatment, new approaches are needed. The optimization of the RT in this patient population may include shorter RT regimens with the understanding that palliative approach must be set from the outset. In a context with limited resources, shorter courses of RT with similar survival and quality of life (QoL) outcomes would be even more appealing. The XXXX trial compared a RT regimen of 40 Gy in 15 fractions (arm 2) to a short-course RT regimen of 25 Gy in 5 fractions (arm 1) for elderly and/or frail patients with GBM and found no significant difference in OS (7.9 versus 6.4 months, respectively) and QoL (5). In a post-hoc, subset analysis of the XXXX trial, we examined survival and QoL outcomes between the 2 arms only in elderly patients. Methods and Matherials Study Design and Random Assignment Patients joined the phase III, randomized, international, multicenter, prospective, non-inferiority trial (ClinicalTrials.gov identifier: XXXXXX) and were randomly assigned to one of two groups in a 1:1 ratio to either short-course RT (25 Gy in 5 fractions delivered in 1 week, arm 1) or commonly used RT (40 Gy in 15 fractions delivered in 3 weeks, arm 2) and stratified by age (< and 65 years), Karnofsky performance status (KPS), and extent
7 of surgery (near total/ complete/ gross total or incomplete/ partial resection). Random assignment was performed using Excel with the RAND option function (Microsoft, Redmond, WA). All eligible patients admitted to the trial were observed until death. The median OS of elderly patients with GBM treated by RT alone is approximately 6 months (3). The trial was designed to establish, with 80% power and an alpha of 0.05, that short-course RT results in median OS is not lower by more than 15% than the commonly used regimen of 40 Gy in 15 fractions. A pre-planned interim analysis with respect to the primary endpoint was conducted when 2/3 of the planned total number of patients had been accrued for observed events (ie, approximately 96 patients). The primary endpoint in this subset analysis of the pre-planned interim evaluation was to compare OS, as in the primary publication. The secondary endpoints were to compare progression free-survival (PFS), QoL and toxicity between the two treatment arms. Study Population The trial population included in this analysis were elderly patients diagnosed with GBM, with frail performance or not. Elderly and frail patients were defined as age 65 years and KPS 50-70%; elderly and not frail patients were defined as age 65 years and KPS %. Prior to trial admission, patients were screened by treating physicians and were required to meet all eligibility criteria: 1) histopathologically confirmed newly diagnosed GBM (WHO grade IV) made by biopsy or neurosurgical tumor resection; 2) initial surgery/biopsy at diagnosis performed 6 weeks prior to randomization; 3) age 65 years at time of entry; 4) KPS 50; 5) no previous chemotherapy or radiotherapy exposure; 6) ability and willingness to complete quality of life questionnaires with baseline assessment completed prior to start of radiotherapy; 7) ability and willingness to give informed consent based on local institutional policy; 8) accessibility for treatment and follow-up and documentation of treatment, adverse events, and follow-up; and 9) delivery of protocol beginning within 2 weeks of patient randomization. Patients fulfilling any of the following criteria were not eligible for the study: 1) history of other malignancy, except adequately treated non-melanoma skin cancer, curatively treated in-situ cancer of the cervix, or other solid tumors curatively treated without evidence of disease 3 years at time of entry; and 2) patients with a serious active infection or underlying medical condition that would impair the ability of the patient to receive protocol treatment and/or comply with protocol.
8 All patients completed a pre-treatment evaluation within 14 days prior to randomization that included history (previous therapy, medical history, and concomitant medications), physical examination, documentation of KPS, clinical tumor status, blood work with a complete blood count, and a mini-mental status exam. After surgery, patients were imaged with gadolinium-enhanced magnetic resonance imaging (MRI) or contrastenhanced computed tomography (CT) of the brain. If imaging was not available postoperatively, a pre-operative CT scan or MRI was admissible if completed within 14 days prior to surgery. Quality of Life Evaluation Quality of life was evaluated in all patients at baseline and during follow-up. Assessments consisted of the self-administered European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire Core-30 (QLQ-C30) and EORTC Quality of Life Questionnaire Brain Cancer Module (QLQ-BN20). The QLQ-C30 questionnaire includes five functional scales (physical, role, emotional, cognitive, and social), three symptom scales (fatigue, nausea/vomiting, and pain), and six single-item scales (dyspnea, insomnia, appetite loss, constipation, and treatment-related financial effect). The QLQ-BN20 includes 20 items within four domains (visual disorders, communication deficits, motor disturbances, and future uncertainty) and 7 single items (headache, seizure, drowsiness, hair loss, itching, bilateral leg weakness, bladder control difficulty). All scales and single items are scored categorically and linearly transformed to scales. Treatment Patients were to start treatment within two weeks of randomization and a central radiotherapy quality assurance was required for each participating center. Radiotherapy treatments were delivered in a similar fashion for both arms. Patients were treated on megavoltage equipment, Cobalt 60 or linear accelerator beams with a minimal nominal energy of 1.25MV. Treatment volumes were to be covered based on tumor location, size, and CTplanning with various field arrangements, accepting dose homogeneity within the volume of ± 10%. Three-dimensional conformal radiotherapy was a requirement for the study. Only one volume was considered with no cone-down or boost-volume. Gross-tumor volume (GTV) was defined as the entire postoperative enhancing tumor and surgical cavity. The clinical target volume (CTV) added a 2.0 cm margin to the GTV with no
9 expansion beyond anatomical boundaries (e.g. skull). The planning target volume (PTV) equaled the CTV cm in all directions. Organs at risk were delineated for all treatments. Treatment consisted of a total dose of 25 Gy in 5 daily fractions (dose/fraction = 5.00 Gy) over one week in Arm 1 and Gy in 15 daily fractions (dose/fraction = 2.67 Gy) over three weeks in Arm 2. Monitoring/ Follow-up Patients were assessed weekly during treatment, including history, physical and KPS completed by their physician. Patients were then assessed four weeks after completing radiotherapy with repeat history, physical, imaging of the brain and also Mini- Mental State Examination (MMSE), and then every three months thereafter until death. At disease progression, patients were required to complete a physical exam and adverse event evaluation. Recording of both acute and late adverse events were graded according to the Common Terminology Criteria for Adverse Events (NCI-CTCAE 3.0); this was evaluated weekly during radiotherapy, at four weeks after radiotherapy, and every three months until tumor progression after which were only reported in case of grade 3 or higher toxicity. EORTC QLQ-C30 and QLQ-BN20 questionnaires were completed four weeks after radiotherapy and then every three months. An interim analysis for comparison of treatment groups was performed with respect to the primary endpoint when two-thirds of the planned patient population had been accrued. Statistical Analysis In the original trial, analysis was conducted as per protocol as well as per intent to treat, as recommended for non-inferiority trial (6). For the purpose of this unplanned secondary evaluation, all analyses were restricted to patients 65 years. Descriptive statistics were used to report baseline characteristics. Mean and standard deviation (SD) were used for normally distributed continuous variables; median and range were used for non-normally distributed continuous variables. Frequency and proportions were reported for categorical data. Student s t-test was used to compare the continuous variables of the two study arm and Chi-square tests were used to compare the categorical variables. Overall survival was calculated from the date of randomization to the date of death, and the subjects who were alive at the date of last follow-up were censored from the analysis. Progression-free survival (PFS) was calculated from the date of treatment to the date of progression or date of death. Patients who did not have any documented disease
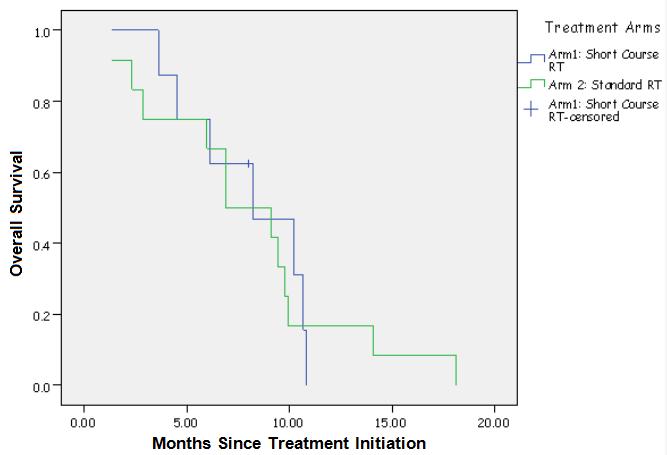
10 progression and were alive at the last follow-up were censored. Kaplan-Meier estimates were used to obtain the median survival and the corresponding 95% confidence interval. Log-rank tests were used to compare the survival of the two study arms. An independent t- test was used to compare the mean quality of life between the two arms. A P-value < 0.05 was used for all statistical significance and two sided tests for the study. SAS (SAS Institute Inc., Cary, NC) version 9.3 was used to conduct all statistical analysis. Results A total of 98 patients from 12 institutions worldwide were randomly assigned in a 1:1 fashion, 48 and 50 in the arm 1 and arm 2, respectively, in the main analysis. Among the 61 patients 65 years, which represented the patient population for the present analysis, 26 were randomized to the arm 1 and 35 to the arm 2. Both groups were similar in baseline characteristics, with no significant differences in country, KPS, sex, imaging modality (CT or MRI), tumor location, surgical procedure and the use of corticosteroids (Table 1). Time between surgical resection/biopsy and RT start, largest tumor diameter, MMSE, hemoglobin and dose of corticosteroids were all also similar between both arms at baseline (Table 2). There was no grade 3 acute toxicity. The mean global health status/qol scores at baseline, 4 and 8 weeks after treatment were similar in both groups (Table 3). After study entry, 2 patients were lost to follow-up as a result of unavoidable situations (1 patient each in arms 1 and 2) and were not included in the OS (Fig.1) and PFS (Fig. 2) analyses. Hence, the survival analysis was conducted as a per-protocol analysis on a total of 59 patients (25 patients in arm 1 and 34 patients in arm 2). At the time of statistical analysis, 96% of patients (24 of 25 patients) in arm 1 and 100% of patients (34 of 34 patients) in arm 2 had died, and 100% of patients in both arms had experienced disease progression. Median OS difference was not statistically significant in patients in arm 1 (6.8 months; 95% CI 4.5 to 9.1 months) compared with patients in arm 2 (6.2 months; 95% CI 4.7 to 7.7 months; P = 0.936). Median PFS difference was also not statistically significant in arm 1 versus arm 2 (4.3 months [95% CI, 2.6 to 5.9 months] v 3.2 months [95% CI,.1 to 6.3 months]; P = 0.706). Analyses were conducted per intent to treat as well, with no difference in median OS or PFS. Additionally, elderly and not frail had same median OS in arm 1 and arm 2 (8.0 months; [95% CI 5.9 to 10.0 months v 8.0 months; 95% CI 5.3 to
11 10.3 months] P = 0.904), (Fig. 3). Elderly and frail was also similar in respect to median OS, 7.5 months in arm 1 (95% CI 5.3 to 9.7 months) and 6.7 months in arm 2 (95% CI 4.5 to 8.9; P =.0890), (Fig. 4). Discussion This subset analysis demonstrated that survival outcomes in the short-course RT arm were not statistically significant different to the commonly used 3-week course of RT in patients 65 years. The median OS and PFS were, respectively, 6.8 and 4.3 months in arm 1 and 6.2 and 3.2 months in arm 2. These results were very similar to the original analysis in the whole group, in which an approximate median OS of 7 months and PFS 4 months were seen in both arms (5). Of note, almost 2/3 of patients in our post-hoc analysis had a KPS 70%. Despite its limitations, chronological age is the main factor of decreasing survival of GBM patients (7). It is expected there is a reduced functional reserve, poorer performance status and additional medical co-morbidities in this specific group of patients and the necessity to face this setting in a particular view. Therefore, observational and prospective trials are used to search for a better modality to treat older patients. Isolated hypofractionated radiotherapy or chemotherapy and both together are the scope of the current trials. Radiation therapy results in improvement of OS in elderly GBM patients compared to supportive care and it has been proved by a prospective trial (3). Data from another randomized prospective trial comparing older patients ( 60 years) receiving 60 Gy in 30 fractions over 6 weeks with 40 Gy in 15 fractions over 3 weeks demonstrated similar survival and palliative benefit in both groups (OS 5.6 months to 3-weeks group and 5.1 months to 6-weeks group (P = 0.57) (4). Therefore, the patient whose treatment was realized in 6 weeks, spent one third of the remaining life in RT, while the patient treated in 3 weeks could have the double time to stay away from the hospital. Following this tendency, the International XXXX proposed a randomized trial comparing 25 Gy in 5 fractions over 1 week against 40 Gy in 15 fractions over 3 weeks. The design was accomplished to reach a non-inferiority overall survival between the two arms. In this subset analysis of patients 65 years, the median overall survival was 6.8 months in 1- week group (25 Gy in 5 fractions) and 6.2 months in 3-week (40 Gy in 15 fractions), which is not statistically different.
12 Although temozolomide (TMZ) concomitant and adjuvant demonstrated a survival advantage added to a standard course of RT (60Gy in 30 daily fraction over 6 weeks) (8), the same benefit of this treatment was not reproduced in older or poor performance status patients (9). Retrospective analyses of hypofractionated RT with or without concurrent TMZ in elderly patients showed the same survival in both groups, 6.9 months for RT +TMZ and 9.3 months for RT alone (P = 0.351). On the other hand, the same review demonstrated that patients treated with salvage TMZ had increased median OS of 13.3 months (P = 0.012) (10). Of course, the bias of this data could exist. Probably, patients with a better performance status received chemotherapy. In a prospective trial, the NCIC CE.6, recently published in abstract form, good performance status (ECOG 0-2) patients had an improvement of OS when TMZ was added to hypofractionated RT. Patients 65 years old had an increase in survival of 1.7 month, extending median OS from 7.6 months with RT alone to 9.3 months with the addition of TMZ (P < ). Patients with methylated O6 methylguanine-dnamethyltransferase (MGMT) promoter tumors had the most important benefit, with a median OS of 13 months (11). In order to analyze the success of TMZ alone, the Nordic trial enrolled GBM patients 60 years old with ECOG 0-2 to either standard RT (60 Gy in 2 Gy fraction over 6 weeks), hypofractionated RT (34 Gy in 10 fractions over 2 weeks) and 6 cycles of chemotherapy with TMZ (200 mg/m2 day 1-5 every 28 days). The median OS was 8.3 months to TMZ, 7.5 months to hypofractionated RT and 6 months for standard RT. There was significant difference for OS between TMZ and standard RT arms (P = 0.01), but no difference between TMZ and hypofractionated arms (P = 0.24). For age older than 70 years, OS was better with TMZ and with hypofractionated RT than with standard RT (hazard ratio [HR] for TMZ versus standard RT 0.35 [95% CI ], P < ; HR for hypofractionated vs standard RT 0.59 [ ], P = 0.02). Patients treated with TMZ who had tumor MGMT promoter methylation had significantly longer survival than those without MGMT promoter methylation (9.7 months [95% CI } versus 6.8 months [ ]; HR 0.56 [ ], P = 0.02), but no difference was noted between those with methylated and unmethylated MGMT promoter treated with RT (HR 0.97 [95% CI ]; P = 0.81). From these data, both TMZ and hypofractionated RT should be considered as standard treatment options in elderly patients with GBM and MGMT promoter methylation status might be a useful predictive marker for benefit from TMZ (12). A similar finding was reported in the NOA-08 trial, which compared dose-dense TMZ alone versus RT alone with 60 Gy in 30 fractions over 6 weeks. The median OS was 8.6 months
13 (95% CI ) in the TMZ group versus 9.6 months ( ) in the RT group (HR 1.09, 95% CI , P (non-inferiority) = 0.033), with a longer event-free survival in patients with MGMT promoter methylation who received TMZ than in those who underwent RT (13). Although the OS was not different between the groups of isolated hypofractionated RT or TMZ, it is expected more toxicity in chemotherapy group as seen in the German trial (13). Besides the toxicity of TMZ, the decision to use it alone instead of hypofractionated RT is a more expensive choice (14). It is important that in elderly population the costeffectiveness is evaluated when the treatment option is made (15). In our study, TMZ was not prescribed concomitant or adjuvant in both groups of RT. It was allowed prescribing chemotherapy in case of disease progression after initial RT at the discretion of the clinical oncologist. It is important to highlight that almost all patients in our analysis had a worse performance status, i.e. 70% of them were ECOG 2-3, opposite of NCIC CE.6 patients, which were ECOG 0-2. Taking into account that 40 Gy in 3 weeks was similar to 25 Gy in 1 week regarding OS, PFS and QoL, the choice of 1-week schedule for patient whose age is over 65 years old, with poor performance status or when TMZ is toxic, seems acceptable. These findings must be counterbalanced with the limitations of this study, which are the small number of patients and the post-hoc analysis. The short-course RT regimen has additional advantages, including improved patient convenience, survival-to-treatment time ratio and reduced travel costs. Patients submitted to the short-course arm spent one-third of the duration of treatment time compared to the commonly used RT arm, which is significant in a population with a median survival time less than 9 months. Conclusions A short-course RT regimen of 25 Gy in 5 fractions is an acceptable treatment option for patients over 65 years old, mainly for those with poor performance or contraindication to chemotherapy, which would be indicated in cases of methylated MGMT promoted tumors.
14 References 1. Bauchet L, Zouaoui S, Darlix A, et al. Assessment and treatment relevance in elderly glioblastoma patients. Neuro Oncol 2014;16: Ferguson M, Rodrigues G, Cao J, et al. Management of high grade gliomas in the elderly. Semin Radiat Oncol 2014;24: Keime-Guibert F, Chinot O, Taillandier L, et al. Radiotherapy for glioblastoma in the elderly. N Engl J Med 2007;356: Roa W, Brasher PM, Bauman G, et al. Abbreviated course of radiation therapy in older patients with glioblastoma multiforme: A prospective randomized clinical trial. J Clin Oncol 2004;22: Roa W, Kepka L, Kumar N, et al. An IAEA randomized phase III study of radiation therapy in elderly and/or frail patients with newly diagnosed glioblastoma multiforme. J Clin Oncol 2015;33: Shah PB: Intention-to-treat and per-protocol analysis. CMAJ 2011;183: Li J, Wang M, Won M, et al. Validation and simplification of the Radiation Therapy Oncology Group recursive partitioning analysis classification for glioblastoma. Int J Radiat Oncol Biol Phys 2011;81: Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Eng J Med 2005;352: Miramanoff RO, Gorlia T, Mason W, et al. Radiotherapy and temozolomide for newly diagnosed glioblastoma: recursive partitioning analysis of the EORTC 26981/22981-NCIC CE3 phase III randomized trial. J Clin Oncol 2006;24: Cao JQ, Fisher BJ, Bauman GS, et al. Hypofractionated radiotherapy with or without concurrent temozolomide in elderly patients with glioblastoma multiforme: a review of tenyear single institutional experience. J Neurooncol 2012;107:
15 11. Perry J, Laperriere N, O Callaghan C, et al. A phase III randomized controlled trial of short-course radiotherapy with or without concomitant and adjuvant temozolomide in elderly patients with glioblastoma (CCTG CE.6, EORTC , TROG 08.02, NCT ). J Clin Oncol 2016;34 (suppl; abstr LBA2). 12. Malmström A, Grønberg BH, Marosi C, et al. Temozolomide versus standard 6-week radiotherapy versus hypofractionated radiotherapy in patients older than 60 years with glioblastoma: the Nordic randomised, phase 3 trial. Lancet Oncol 2012;13: Wick W, Platten M, Meisner C, et al. Temozolomide chemotherapy alone versus radiotherapy alone for malignant astrocytoma in the elderly: the NOA-08 randomised, phase 3 trial. Lancet Oncol 2012;13: Burton E, Ugiliweneza B, Woo S, et al. A Surveillance, Epidemiology and End Results- Medicare data analysis of elderly patients with glioblastoma multiforme: Treatment patterns, outcomes and cost. Mol Clin Oncol 2015;3: Lievens Y, Grau C. Health Economics in Radiation Oncology: Introducing the ESTRO HERO project. Radiother Oncol 2012;103: Figure Legends Fig. 1. Overall survival (OS), elderly patients ( 65 years). Kaplan-Meier plots of OS according to the treatment arm. Fig. 2. Progression-free survival (PFS), elderly patients ( 65 years). Kaplan-Meier plots of PFS according to the treatment arm. Fig. 3. Overall survival (OS), elderly ( 65 years) and not frail patients. Kaplan-Meier plots of OS according to the treatment arm. Fig. 4. Overall survival (OS), elderly ( 65 years) and frail patients. Kaplan-Meier plots of OS according to the treatment arm.
16 Tables Table 1. Patient Baseline Characteristics (categorical variables) Number of Patients (%) Country KPS Sex Characteristic Arm 1 (n = 26) Arm 2 (n = 35) P.783 Belarus 6 (23) 8 (23) Brazil - PA 3 (12) 2 (6) Brazil - SP 0 (0) 1 (3) Georgia 1 (4) 3 (8) Greece 0 (0) 1 (3) India 4 (15) 5 (14) Ireland 1 (4) 0 (0) Poland 11 (42) 13 (37) Thailand 0 (0) 1 (3) Tunisia 0 (0) 1 (3) (12) 4 (11) 60 9 (34) 10 (29) 70 6 (23) 8 (23) 80 6 (23) 9 (26) 90 2 (8) 4 (11).438 Female 17 (66) 19 (55) Male 9 (34) 16 (45) Imaging modality.596 CT 9 (34) 15 (42) MRI 17 (66) 19 (55) Tumor location.638 Unilobar* 22 (85) 26 (76) Multilobar 4 (15) 6 (18) Basal Nuclei 0 (0) 1 (3) Corpus Callosum 0 (0) 1 (3)
17 Surgical procedure.921 Not defined 1 (4) 2 (6) Stereotactic biopsy 3 (12) 5 (15) Partial resection 15 (57) 20 (58) Total macroscopic resection 7 (27) 7 (21) Corticosteroid therapy.794 Yes 12 (48) 15 (42) No 13 (52) 20 (58) Abbreviations: CT, computed tomography; KPS, Karnofsky performance status; MRI, magnetic resonance imaging; PA, Porto Alegre; SP, São Paulo. * Left/Right frontal, occipital, parietal or temporal lobe. Table 2. Patient Baseline Characteristics (continuous variables) Characteristic Arm 1 Arm 2 P Treatment time*.664 No. of patients Mean (±SD), days 32.1 (±10.3) 32.4 (±9.3) Largest tumor diameter.892 No. of patients Mean (±SD), cm 5.9 (±3.8) 5.6 (±4.0) MMSE baseline**.714 No. of patients Mean (±SD), score 20.9 (±6.9) 21.1 (±6.5) Hemoglobin.924 No. of patients Mean (±SD), g/dl 12.1 (±1.2) 12.4 (±1.2) Dose of corticosteroids.302 No. of patients Mean (±SD), mg/d 6.0 (±4.0) 6.4 (±2.5) Abbreviations: MMSE, Mini-Mental State Examination; SD, standard deviation. * Treatment time is time between surgery and start of radiotherapy. ** Maximum score is 30; scores above 26 are defined as normal mental status.
18 Table 3. Global Health Status (QoL) Global Health Status/QoL* Arm 1 Arm 2 P Baseline.556 No. of patients Mean (±SD), score 47.1 (±22.5) 50.2 (±17.2) 4 weeks after treatment.581 No. of patients Mean (±SD), score 51.7 (±18.0) 48.3 (±19.8) 8 weeks after treatment 1.00 No. of patients Mean (±SD), score 48.6 (±18.4) 48.6 (±15.4) Abbreviations: QoL, quality of life; SD, standard deviation. * QoL measured using European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire C30 and EORTC Quality of Life Questionnaire Brain cancer Module. Categorical scales are transformed to linear 0 to 100 scale.

19

20

21
22
Treatment and outcomes for glioblastoma in elderly compared with non-elderly patients: a population-based study
 ORIGINAL ARTICLE Treatment and outcomes for glioblastoma in elderly compared with non-elderly patients: a population-based study E.R. Morgan md,* A. Norman md, K. Laing md, and M.D. Seal md ABSTRACT Purpose
ORIGINAL ARTICLE Treatment and outcomes for glioblastoma in elderly compared with non-elderly patients: a population-based study E.R. Morgan md,* A. Norman md, K. Laing md, and M.D. Seal md ABSTRACT Purpose
21/03/2017. Disclosure. Practice Changing Articles in Neuro Oncology for 2016/17. Gliomas. Objectives. Gliomas. No conflicts to declare
 Practice Changing Articles in Neuro Oncology for 2016/17 Disclosure No conflicts to declare Frances Cusano, BScPharm, ACPR April 21, 2017 Objectives Gliomas To describe the patient selection, methodology
Practice Changing Articles in Neuro Oncology for 2016/17 Disclosure No conflicts to declare Frances Cusano, BScPharm, ACPR April 21, 2017 Objectives Gliomas To describe the patient selection, methodology
Survival of High Grade Glioma Patients Treated by Three Radiation Schedules with Chemotherapy: A Retrospective Comparative Study
 Original Article Research in Oncology June 2017; Vol. 13, No. 1: 18-22. DOI: 10.21608/resoncol.2017.552.1022 Survival of High Grade Glioma Patients Treated by Three Radiation Schedules with Chemotherapy:
Original Article Research in Oncology June 2017; Vol. 13, No. 1: 18-22. DOI: 10.21608/resoncol.2017.552.1022 Survival of High Grade Glioma Patients Treated by Three Radiation Schedules with Chemotherapy:
Scottish Medicines Consortium
 Scottish Medicines Consortium temozolomide 5, 20, 100 and 250mg capsules (Temodal ) Schering Plough UK Ltd No. (244/06) New indication: for the treatment of newly diagnosed glioblastoma multiforme concomitantly
Scottish Medicines Consortium temozolomide 5, 20, 100 and 250mg capsules (Temodal ) Schering Plough UK Ltd No. (244/06) New indication: for the treatment of newly diagnosed glioblastoma multiforme concomitantly
Elderly Patients with Glioblastoma Multiforme Treated with Concurrent Temozolomide and Standard- versus Abbreviated-Course Radiotherapy
 Elderly Patients with Glioblastoma Multiforme Treated with Concurrent Temozolomide and Standard- versus Abbreviated-Course Radiotherapy Christine N Chang-Halpenny, MD; Jekwon Yeh, MD; Winston W Lien, MD
Elderly Patients with Glioblastoma Multiforme Treated with Concurrent Temozolomide and Standard- versus Abbreviated-Course Radiotherapy Christine N Chang-Halpenny, MD; Jekwon Yeh, MD; Winston W Lien, MD
Hypofractionated radiation therapy for glioblastoma
 Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study
 temozolomide and radiation to treat glioblastoma: A retrospective study") Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study T Sridhar 1, A Gore 1, I Boiangiu 1, D Machin 2, R P Symonds 3 1. Department of Oncology, Leicester
Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study T Sridhar 1, A Gore 1, I Boiangiu 1, D Machin 2, R P Symonds 3 1. Department of Oncology, Leicester
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
Temozolomide Concomitant and Adjuvant to Radiotherapy in Elderly Patients With Glioblastoma
 Temozolomide Concomitant and Adjuvant to Radiotherapy in Elderly Patients With Glioblastoma Correlation With MGMT Promoter Methylation Status Alba A. Brandes, MD 1 ; Enrico Franceschi, MD 1 ; Alicia Tosoni,
Temozolomide Concomitant and Adjuvant to Radiotherapy in Elderly Patients With Glioblastoma Correlation With MGMT Promoter Methylation Status Alba A. Brandes, MD 1 ; Enrico Franceschi, MD 1 ; Alicia Tosoni,
3-D conformal radiotherapy with concomitant and adjuvant temozolomide for patients with glioblastoma multiforme and evaluation of prognostic factors
 research article 213 3-D conformal radiotherapy with concomitant and adjuvant temozolomide for patients with glioblastoma multiforme and evaluation of prognostic factors Yilmaz Tezcan and Mehmet Koc Department
research article 213 3-D conformal radiotherapy with concomitant and adjuvant temozolomide for patients with glioblastoma multiforme and evaluation of prognostic factors Yilmaz Tezcan and Mehmet Koc Department
Radiation and concomitant chemotherapy for patients with glioblastoma multiforme
 Chinese Journal of Cancer Review Radiation and concomitant chemotherapy for patients with glioblastoma multiforme Salvador Villà 1, Carme Balañà 2 and Sílvia Comas 1 Abstract Postoperative external beam
Chinese Journal of Cancer Review Radiation and concomitant chemotherapy for patients with glioblastoma multiforme Salvador Villà 1, Carme Balañà 2 and Sílvia Comas 1 Abstract Postoperative external beam
Concurrent Chemoradiotherapy Versus Radiotherapy Alone for Biopsy-Only Glioblastoma Multiforme
 Concurrent Chemoradiotherapy Versus Radiotherapy Alone for Biopsy-Only Glioblastoma Multiforme Adam J. Kole, MD, PhD 1 ; Henry S. Park, MD, MPH 1 ; Debra N. Yeboa, MD 1 ; Charles E. Rutter, MD 1 ; Christopher
Concurrent Chemoradiotherapy Versus Radiotherapy Alone for Biopsy-Only Glioblastoma Multiforme Adam J. Kole, MD, PhD 1 ; Henry S. Park, MD, MPH 1 ; Debra N. Yeboa, MD 1 ; Charles E. Rutter, MD 1 ; Christopher
Josh is JB s brother and caregiver.
 PUT GBM ON PAUSE PUT LIFE ON PLAY Josh is JB s brother and caregiver. JB is an Optune user. OPTUNE + TMZ HAS BEEN PROVEN TO PROVIDE LONG-TERM QUALITY SURVIVAL TO PATIENTS WITH NEWLY DIAGNOSED GBM1,2,*
PUT GBM ON PAUSE PUT LIFE ON PLAY Josh is JB s brother and caregiver. JB is an Optune user. OPTUNE + TMZ HAS BEEN PROVEN TO PROVIDE LONG-TERM QUALITY SURVIVAL TO PATIENTS WITH NEWLY DIAGNOSED GBM1,2,*
Oncological Management of Brain Tumours. Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013
 Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia
 for Brain Metastasis in Nova Scotia") A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia Gaurav Bahl, Karl Tennessen, Ashraf Mahmoud-Ahmed, Dorianne Rheaume, Ian Fleetwood,
A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia Gaurav Bahl, Karl Tennessen, Ashraf Mahmoud-Ahmed, Dorianne Rheaume, Ian Fleetwood,
University of Zurich. Temozolomide and MGMT forever? Zurich Open Repository and Archive. Weller, M. Year: 2010
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich Year: 2010 Temozolomide and MGMT forever? Weller, M Weller, M (2010). Temozolomide and MGMT forever? Neuro-Oncology,
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich Year: 2010 Temozolomide and MGMT forever? Weller, M Weller, M (2010). Temozolomide and MGMT forever? Neuro-Oncology,
Contemporary Management of Glioblastoma
 Contemporary Management of Glioblastoma Incidence Rates of Primary Brain Tumors Central Brain Tumor Registry of the United States, 1992-1997 100 Number of Cases per 100,000 Population 10 1 0.1 x I x I
Contemporary Management of Glioblastoma Incidence Rates of Primary Brain Tumors Central Brain Tumor Registry of the United States, 1992-1997 100 Number of Cases per 100,000 Population 10 1 0.1 x I x I
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
Proton beam therapy with concurrent chemotherapy for glioblastoma multiforme: comparison of nimustine hydrochloride and temozolomide
 J Neurooncol DOI 1.17/s11-1-2228-4 CLINIcAL STUDY Proton beam therapy with concurrent chemotherapy for glioblastoma multiforme: comparison of nimustine hydrochloride and temozolomide Masashi Mizumoto 1
J Neurooncol DOI 1.17/s11-1-2228-4 CLINIcAL STUDY Proton beam therapy with concurrent chemotherapy for glioblastoma multiforme: comparison of nimustine hydrochloride and temozolomide Masashi Mizumoto 1
Radioterapia no Tratamento dos Gliomas de Baixo Grau
 Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
doi: /bjr/
 doi: 10.1259/bjr/29022270 Prognostic factors in the consecutive institutional series of glioblastoma multiforme patients who received high-dose particle radiotherapy or conventional radiotherapy Masahide
doi: 10.1259/bjr/29022270 Prognostic factors in the consecutive institutional series of glioblastoma multiforme patients who received high-dose particle radiotherapy or conventional radiotherapy Masahide
THE EFFECTIVE OF BRAIN CANCER AND XAY BETWEEN THEORY AND IMPLEMENTATION. Mustafa Rashid Issa
 THE EFFECTIVE OF BRAIN CANCER AND XAY BETWEEN THEORY AND IMPLEMENTATION Mustafa Rashid Issa ABSTRACT: Illustrate malignant tumors that form either in the brain or in the nerves originating in the brain.
THE EFFECTIVE OF BRAIN CANCER AND XAY BETWEEN THEORY AND IMPLEMENTATION Mustafa Rashid Issa ABSTRACT: Illustrate malignant tumors that form either in the brain or in the nerves originating in the brain.
Cilengitide (Impetreve) for glioblastoma multiforme. February 2012
 for glioblastoma multiforme. February 2012") Cilengitide (Impetreve) for glioblastoma multiforme February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Cilengitide (Impetreve) for glioblastoma multiforme February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Survival Analysis of Glioblastoma Multiforme
 DOI:10.22034/APJCP.2018.19.9.2613 RESEARCH ARTICLE Editorial Process: Submission:04/24/2018 Acceptance:08/19/2018 Supapan Witthayanuwat, Montien Pesee*, Chunsri Supaadirek, Narudom Supakalin, Komsan Thamronganantasakul,
DOI:10.22034/APJCP.2018.19.9.2613 RESEARCH ARTICLE Editorial Process: Submission:04/24/2018 Acceptance:08/19/2018 Supapan Witthayanuwat, Montien Pesee*, Chunsri Supaadirek, Narudom Supakalin, Komsan Thamronganantasakul,
FACT SHEET. About Optune
 About Optune Optune is the Tumor Treating Fields (TTFields) delivery system that is approved by the United States (US) Food and Drug Administration (FDA) for the treatment of adult patients with glioblastoma.
About Optune Optune is the Tumor Treating Fields (TTFields) delivery system that is approved by the United States (US) Food and Drug Administration (FDA) for the treatment of adult patients with glioblastoma.
Glioblastoma: Current Treatment Approach 8/20/2018
 Glioblastoma: Current Treatment Approach 8/20/2018 Overview What is Glioblastoma? How is it diagnosed How is it treated? Principles of Treatment Surgery, Radiation, Chemotherapy Current Standard of care
Glioblastoma: Current Treatment Approach 8/20/2018 Overview What is Glioblastoma? How is it diagnosed How is it treated? Principles of Treatment Surgery, Radiation, Chemotherapy Current Standard of care
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES
 DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
PROCARBAZINE, lomustine, and vincristine (PCV) is
 is") RAPID PUBLICATION Procarbazine, Lomustine, and Vincristine () Chemotherapy for Anaplastic Astrocytoma: A Retrospective Review of Radiation Therapy Oncology Group Protocols Comparing Survival With Carmustine
RAPID PUBLICATION Procarbazine, Lomustine, and Vincristine () Chemotherapy for Anaplastic Astrocytoma: A Retrospective Review of Radiation Therapy Oncology Group Protocols Comparing Survival With Carmustine
Systemic Treatment. Third International Neuro-Oncology Course. 23 May 2014
 Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
Optimal Management of Isolated HER2+ve Brain Metastases
 Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
University of Alberta. Evaluation of Concomitant Temozolomide Treatment in Glioblastoma Multiforme Patients in Two Canadian Tertiary Care Centers
 University of Alberta Evaluation of Concomitant Temozolomide Treatment in Glioblastoma Multiforme Patients in Two Canadian Tertiary Care Centers by Ibrahim Alnaami A thesis submitted to the Faculty of
University of Alberta Evaluation of Concomitant Temozolomide Treatment in Glioblastoma Multiforme Patients in Two Canadian Tertiary Care Centers by Ibrahim Alnaami A thesis submitted to the Faculty of
Primary Endpoint The primary endpoint is overall survival, measured as the time in weeks from randomization to date of death due to any cause.
 CASE STUDY Randomized, Double-Blind, Phase III Trial of NES-822 plus AMO-1002 vs. AMO-1002 alone as first-line therapy in patients with advanced pancreatic cancer This is a multicenter, randomized Phase
CASE STUDY Randomized, Double-Blind, Phase III Trial of NES-822 plus AMO-1002 vs. AMO-1002 alone as first-line therapy in patients with advanced pancreatic cancer This is a multicenter, randomized Phase
Related Policies None
 Medical Policy MP 2.04.113 BCBSA Ref. Policy: 2.04.113 Last Review: 05/30/2018 Effective Date: 05/30/2018 Section: Medicine Related Policies None DISCLAIMER Our medical policies are designed for informational
Medical Policy MP 2.04.113 BCBSA Ref. Policy: 2.04.113 Last Review: 05/30/2018 Effective Date: 05/30/2018 Section: Medicine Related Policies None DISCLAIMER Our medical policies are designed for informational
Lynn S. Ashby 1*, Kris A. Smith 2 and Baldassarre Stea 3
 Ashby et al. World Journal of Surgical Oncology (2016) 14:225 DOI 10.1186/s12957-016-0975-5 REVIEW Gliadel wafer implantation combined with standard radiotherapy and concurrent followed by adjuvant temozolomide
Ashby et al. World Journal of Surgical Oncology (2016) 14:225 DOI 10.1186/s12957-016-0975-5 REVIEW Gliadel wafer implantation combined with standard radiotherapy and concurrent followed by adjuvant temozolomide
Chika Nwachukwu, Ph.D. MS IV Radiation Oncology Rotation
 Chika Nwachukwu, Ph.D. MS IV Radiation Oncology Rotation Background Histology/Tumor Characteristics Presenting Symptoms/diagnosis Treatment/outcome Patient cohort Research on HRQOL Slow growing indolent
Chika Nwachukwu, Ph.D. MS IV Radiation Oncology Rotation Background Histology/Tumor Characteristics Presenting Symptoms/diagnosis Treatment/outcome Patient cohort Research on HRQOL Slow growing indolent
Incidence of Early Pseudo-progression in a Cohort of Malignant Glioma Patients Treated With Chemoirradiation With Temozolomide
 405 Incidence of Early Pseudo-progression in a Cohort of Malignant Glioma Patients Treated With Chemoirradiation With Temozolomide Walter Taal, MD 1 Dieta Brandsma, MD, PhD 1 Hein G. de Bruin, MD, PhD
405 Incidence of Early Pseudo-progression in a Cohort of Malignant Glioma Patients Treated With Chemoirradiation With Temozolomide Walter Taal, MD 1 Dieta Brandsma, MD, PhD 1 Hein G. de Bruin, MD, PhD
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
Institute of Oncology & Radiobiology. Havana, Cuba. INOR
 Institute of Oncology & Radiobiology. Havana, Cuba. INOR 1 Transition from 2-D 2 D to 3-D 3 D conformal radiotherapy in high grade gliomas: : our experience in Cuba Chon. I, MD - Chi. D, MD - Alert.J,
Institute of Oncology & Radiobiology. Havana, Cuba. INOR 1 Transition from 2-D 2 D to 3-D 3 D conformal radiotherapy in high grade gliomas: : our experience in Cuba Chon. I, MD - Chi. D, MD - Alert.J,
Technology appraisal guidance Published: 27 June 2007 nice.org.uk/guidance/ta121
 Carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma Technology appraisal guidance Published: 27 June 2007 nice.org.uk/guidance/ta121 NICE 2018. All rights reserved.
Carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma Technology appraisal guidance Published: 27 June 2007 nice.org.uk/guidance/ta121 NICE 2018. All rights reserved.
Antiangiogenic drugs in unresectable glioblastoma. Dra. Carmen Balañá. /
 Antiangiogenic drugs in unresectable glioblastoma Dra. Carmen Balañá. / Outcome for unresectable GBM Overall survival for unresectable GBM without further treatment is: 3 months at most. Radiotherapy increases
Antiangiogenic drugs in unresectable glioblastoma Dra. Carmen Balañá. / Outcome for unresectable GBM Overall survival for unresectable GBM without further treatment is: 3 months at most. Radiotherapy increases
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS
 UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
SYNOPSIS PROTOCOL N UC-0107/1602
 SYNOPSIS PROTOCOL N UC-0107/1602 A) TRIAL IDENTIFICATION SPONSOR PROTOCOL CODE NUMBER: UC-0107/1602 VERSION (NR & DATE): 0.1, MARCH 2016 TRIAL TITLE: Extracranial Stereotactic Body Radiation Therapy (SBRT)
SYNOPSIS PROTOCOL N UC-0107/1602 A) TRIAL IDENTIFICATION SPONSOR PROTOCOL CODE NUMBER: UC-0107/1602 VERSION (NR & DATE): 0.1, MARCH 2016 TRIAL TITLE: Extracranial Stereotactic Body Radiation Therapy (SBRT)
Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma
 National Institute for Health and Clinical Excellence Health Technology Appraisal Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma Personal statement Conventional
National Institute for Health and Clinical Excellence Health Technology Appraisal Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma Personal statement Conventional
Paolo Tini 1,3 M.D. :
 Correlazione tra espressione di Epidermal Growth Factor Receptor (EGFR) e Patterns di recidiva/progressione di malattia dopo trattamento radio-chemioterapico in pazienti affetti da Glioblastoma (GB). Paolo
Correlazione tra espressione di Epidermal Growth Factor Receptor (EGFR) e Patterns di recidiva/progressione di malattia dopo trattamento radio-chemioterapico in pazienti affetti da Glioblastoma (GB). Paolo
Efficacy of Treatment for Glioblastoma Multiforme in Elderly Patients (65+): A Retrospective Analysis
: A Retrospective Analysis") Efficacy of Treatment for Glioblastoma Multiforme in Elderly Patients (65+): A Retrospective Analysis Igal Kushnir MD 1 * and Tzahala Tzuk-Shina MD 2 1 Oncology Insitute, Tel Aviv Sourasky Medical Center,
Efficacy of Treatment for Glioblastoma Multiforme in Elderly Patients (65+): A Retrospective Analysis Igal Kushnir MD 1 * and Tzahala Tzuk-Shina MD 2 1 Oncology Insitute, Tel Aviv Sourasky Medical Center,
Zurich Open Repository and Archive. Long-term survival of glioblastoma patients treated with radiotherapy and lomustine plus temozolomide
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 19 CH-857 Zurich http://www.zora.uzh.ch Year: 29 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 19 CH-857 Zurich http://www.zora.uzh.ch Year: 29 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
Department of Medical Oncology, National Cancer Institute of Aviano, Aviano (PN) Italy 3
 Italy 3") WCRJ 2014; 1 (4): e401 RADIOCHEMOTHERAPY FOR UNRESECTABLE GLIOBLASTOMA MULTIFORME: A MONO- INSTITUTIONAL EXPERIENCE M. COLELLA 1, F. FIORICA 1, P. API 1, A. STEFANELLI 1, B. URBINI 2, A. SGUALDO 1, D.
WCRJ 2014; 1 (4): e401 RADIOCHEMOTHERAPY FOR UNRESECTABLE GLIOBLASTOMA MULTIFORME: A MONO- INSTITUTIONAL EXPERIENCE M. COLELLA 1, F. FIORICA 1, P. API 1, A. STEFANELLI 1, B. URBINI 2, A. SGUALDO 1, D.
Arecent randomized controlled trial (RCT) established
 established") Neuro-Oncology 12(2):190 198, 2010. doi:10.1093/neuonc/nop004 NEURO-ONCOLOGY The timing of cranial radiation in elderly patients with newly diagnosed glioblastoma multiforme Rose Lai, Dawn L. Hershman,
Neuro-Oncology 12(2):190 198, 2010. doi:10.1093/neuonc/nop004 NEURO-ONCOLOGY The timing of cranial radiation in elderly patients with newly diagnosed glioblastoma multiforme Rose Lai, Dawn L. Hershman,
A new score predicting the survival of patients with spinal cord compression from myeloma
 Douglas et al. BMC Cancer 2012, 12:425 RESEARCH ARTICLE Open Access A new score predicting the survival of patients with spinal cord compression from myeloma Sarah Douglas 1, Steven E Schild 2 and Dirk
Douglas et al. BMC Cancer 2012, 12:425 RESEARCH ARTICLE Open Access A new score predicting the survival of patients with spinal cord compression from myeloma Sarah Douglas 1, Steven E Schild 2 and Dirk
Prior to 1993, the only data available in the medical
 Neuro-Oncology Prospective clinical trials of intracranial low-grade glioma in adults and children Edward G. Shaw 1 and Jeffrey H. Wisoff Department of Radiation Oncology, Wake Forest University School
Neuro-Oncology Prospective clinical trials of intracranial low-grade glioma in adults and children Edward G. Shaw 1 and Jeffrey H. Wisoff Department of Radiation Oncology, Wake Forest University School
Zurich Open Repository and Archive. Long-term survival of glioblastoma patients treated with radiotherapy and lomustine plus temozolomide
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2009 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2009 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
ORE Open Research Exeter
 ORE Open Research Exeter TITLE Temozolomide for high grade glioma AUTHORS Hart, MG; Garside, R; Rogers, G; et al. JOURNAL Cochrane Database Of Systematic Reviews DEPOSITED IN ORE 22 October 2013 This version
ORE Open Research Exeter TITLE Temozolomide for high grade glioma AUTHORS Hart, MG; Garside, R; Rogers, G; et al. JOURNAL Cochrane Database Of Systematic Reviews DEPOSITED IN ORE 22 October 2013 This version
ORIGINAL PAPERS. The Impact of Surgery on the Efficacy of Adjuvant Therapy in Glioblastoma Multiforme
 ORIGINAL PAPERS Adv Clin Exp Med 2015, 24, 2, 279 287 DOI: 10.17219/acem/40456 Copyright by Wroclaw Medical University ISSN 1899 5276 Anna Brzozowska 1, 2, A D, Anna Toruń 3, G, Maria Mazurkiewicz1, 2,
ORIGINAL PAPERS Adv Clin Exp Med 2015, 24, 2, 279 287 DOI: 10.17219/acem/40456 Copyright by Wroclaw Medical University ISSN 1899 5276 Anna Brzozowska 1, 2, A D, Anna Toruń 3, G, Maria Mazurkiewicz1, 2,
성균관대학교삼성창원병원신경외과학교실신경종양학 김영준. KNS-MT-03 (April 15, 2015)
") 성균관대학교삼성창원병원신경외과학교실신경종양학 김영준 INTRODUCTIONS Low grade gliomas (LGG) - heterogeneous group of tumors with astrocytic, oligodendroglial, ependymal, or mixed cellular histology - In adults diffuse, infiltrating
성균관대학교삼성창원병원신경외과학교실신경종양학 김영준 INTRODUCTIONS Low grade gliomas (LGG) - heterogeneous group of tumors with astrocytic, oligodendroglial, ependymal, or mixed cellular histology - In adults diffuse, infiltrating
Neuro-Oncology Program
 Neuro-Oncology Program The goals of the Neuro-oncology Committee are: 1) to improve duration and quality of life of brain tumor patients; 2) to assess disease and treatment-related effects on neurocognitive
Neuro-Oncology Program The goals of the Neuro-oncology Committee are: 1) to improve duration and quality of life of brain tumor patients; 2) to assess disease and treatment-related effects on neurocognitive
Adjuvant treatment of high grade gliomas
 17 (Supplement 10): x186 x190, 2006 doi:10.1093/annonc/mdl258 Adjuvant treatment of high grade gliomas M. J. van den Bent Department of Neuro-Oncology, Erasmus University Hospital Rotterdam/Rotterdam Cancer
17 (Supplement 10): x186 x190, 2006 doi:10.1093/annonc/mdl258 Adjuvant treatment of high grade gliomas M. J. van den Bent Department of Neuro-Oncology, Erasmus University Hospital Rotterdam/Rotterdam Cancer
CNS Tumors: The Med Onc Perspective. Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U.
 CNS Tumors: The Med Onc Perspective Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U. Disclosure Speakers Bureau, Merck Basic Oncology Concepts Tissue Diagnosis Stage
CNS Tumors: The Med Onc Perspective Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U. Disclosure Speakers Bureau, Merck Basic Oncology Concepts Tissue Diagnosis Stage
J Clin Oncol 27: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 27 NUMBER 8 MARCH 10 2009 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Recurrence Pattern After Temozolomide Concomitant With and Adjuvant to Radiotherapy in Newly Diagnosed Patients
VOLUME 27 NUMBER 8 MARCH 10 2009 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Recurrence Pattern After Temozolomide Concomitant With and Adjuvant to Radiotherapy in Newly Diagnosed Patients
Introduction ORIGINAL RESEARCH
 Cancer Medicine ORIGINAL RESEARCH Open Access The effect of radiation therapy in the treatment of adult soft tissue sarcomas of the extremities: a long- term community- based cancer center experience Jeffrey
Cancer Medicine ORIGINAL RESEARCH Open Access The effect of radiation therapy in the treatment of adult soft tissue sarcomas of the extremities: a long- term community- based cancer center experience Jeffrey
Short-Course Radiation plus Temozolomide in Elderly Patients with Glioblastoma
 Original Article Short-Course Radiation plus Temozolomide in Elderly Patients with Glioblastoma James R. Perry, M.D., Normand Laperriere, M.D., Christopher J. O Callaghan, D.V.M., Alba A. Brandes, M.D.,
Original Article Short-Course Radiation plus Temozolomide in Elderly Patients with Glioblastoma James R. Perry, M.D., Normand Laperriere, M.D., Christopher J. O Callaghan, D.V.M., Alba A. Brandes, M.D.,
Health-Related Quality of Life in Brain Tumor Patients Treated with Surgery: Preliminary Result of a Single Institution
 ORIGINAL ARTICLE Brain Tumor Res Treat 2016;4(2):87-93 / pissn 2288-2405 / eissn 2288-2413 http://dx.doi.org/10.14791/btrt.2016.4.2.87 Health-Related Quality of Life in Brain Tumor Patients Treated with
ORIGINAL ARTICLE Brain Tumor Res Treat 2016;4(2):87-93 / pissn 2288-2405 / eissn 2288-2413 http://dx.doi.org/10.14791/btrt.2016.4.2.87 Health-Related Quality of Life in Brain Tumor Patients Treated with
Glioblastoma (GBM) is the most common and
 is the most common and") Neuro-Oncology 12(6):595 602, 2010. doi:10.1093/neuonc/noq008 Advance Access publication February 11, 2010 NEURO-ONCOLOGY Prolonged survival for patients with newly diagnosed, inoperable glioblastoma with
Neuro-Oncology 12(6):595 602, 2010. doi:10.1093/neuonc/noq008 Advance Access publication February 11, 2010 NEURO-ONCOLOGY Prolonged survival for patients with newly diagnosed, inoperable glioblastoma with
Low grade glioma: a journey towards a cure
 Editorial Page 1 of 5 Low grade glioma: a journey towards a cure Ali K. Choucair SIU School of Medicine, Springfield, IL, USA Correspondence to: Ali K. Choucair, MD. Professor of Neurology, Director of
Editorial Page 1 of 5 Low grade glioma: a journey towards a cure Ali K. Choucair SIU School of Medicine, Springfield, IL, USA Correspondence to: Ali K. Choucair, MD. Professor of Neurology, Director of
Management of Glioma: The Basics Glioma Update The clinical challenge. Glioma a malignant disease of the CNS
 Management of Glioma: The Basics Glioma Update 3 oger Stupp, MD Department of Oncology & Cancer Center University Hospital Zurich, Switzerland (roger.stupp@usz.ch) Bern, 3. August 3 The clinical challenge
Management of Glioma: The Basics Glioma Update 3 oger Stupp, MD Department of Oncology & Cancer Center University Hospital Zurich, Switzerland (roger.stupp@usz.ch) Bern, 3. August 3 The clinical challenge
Clinical Study Hypofractionated High-Dose Irradiation with Positron Emission Tomography Data for the Treatment of Glioblastoma Multiforme
 BioMed Research International Volume 14, Article ID 26, 9 pages http://dx.doi.org/.1155/14/26 Clinical Study Hypofractionated High-Dose Irradiation with Positron Emission Tomography Data for the Treatment
BioMed Research International Volume 14, Article ID 26, 9 pages http://dx.doi.org/.1155/14/26 Clinical Study Hypofractionated High-Dose Irradiation with Positron Emission Tomography Data for the Treatment
Bevacizumab rescue therapy extends the survival in patients with recurrent malignant glioma
 Original Article Bevacizumab rescue therapy extends the survival in patients with recurrent malignant glioma Lin-Bo Cai, Juan Li, Ming-Yao Lai, Chang-Guo Shan, Zong-De Lian, Wei-Ping Hong, Jun-Jie Zhen,
Original Article Bevacizumab rescue therapy extends the survival in patients with recurrent malignant glioma Lin-Bo Cai, Juan Li, Ming-Yao Lai, Chang-Guo Shan, Zong-De Lian, Wei-Ping Hong, Jun-Jie Zhen,
REVISITING ICRU VOLUME DEFINITIONS. Eduardo Rosenblatt Vienna, Austria
 REVISITING ICRU VOLUME DEFINITIONS Eduardo Rosenblatt Vienna, Austria Objective: To introduce target volumes and organ at risk concepts as defined by ICRU. 3D-CRT is the standard There was a need for a
REVISITING ICRU VOLUME DEFINITIONS Eduardo Rosenblatt Vienna, Austria Objective: To introduce target volumes and organ at risk concepts as defined by ICRU. 3D-CRT is the standard There was a need for a
PRESURGICAL PLANNING. Strongly consider neuropsychological evaluation before functional imaging study Strongly consider functional imaging study
 NOTE: Consider Clinical Trials as treatment options for eligible patients. Page 1 of 6 RADIOLOGICAL PRESENTATION PRESURGICAL PLANNING TREATMENT Imaging study suggestive of glioma 1 Left hemisphere speech/motor
NOTE: Consider Clinical Trials as treatment options for eligible patients. Page 1 of 6 RADIOLOGICAL PRESENTATION PRESURGICAL PLANNING TREATMENT Imaging study suggestive of glioma 1 Left hemisphere speech/motor
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924
 EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
Bevacizumab in combination with temozolomide and regional radiation therapy for up-front treatment of patients with newly-diagnosed glioblastoma
 Bevacizumab in combination with temozolomide and regional radiation therapy for up-front treatment of patients with newly-diagnosed glioblastoma Design and analysis of single-arm Phase II clinical trial
Bevacizumab in combination with temozolomide and regional radiation therapy for up-front treatment of patients with newly-diagnosed glioblastoma Design and analysis of single-arm Phase II clinical trial
Report on Radiation Disaster Recovery Studies
 Report on Radiation Disaster Recovery Studies Course: Radiation Disaster Medicine Name: Uranchimeg Tsegmed Radiation Disaster Recovery Studies Nowadays, applications of nuclear technology in different
Report on Radiation Disaster Recovery Studies Course: Radiation Disaster Medicine Name: Uranchimeg Tsegmed Radiation Disaster Recovery Studies Nowadays, applications of nuclear technology in different
Citation Pediatrics international (2015), 57.
, 57.") Title Long-term efficacy of bevacizumab a pediatric glioblastoma. Umeda, Katsutsugu; Shibata, Hirofum Author(s) Hiramatsu, Hidefumi; Arakawa, Yoshi Nishiuchi, Ritsuo; Adachi, Souichi; Ken-Ichiro Citation
Title Long-term efficacy of bevacizumab a pediatric glioblastoma. Umeda, Katsutsugu; Shibata, Hirofum Author(s) Hiramatsu, Hidefumi; Arakawa, Yoshi Nishiuchi, Ritsuo; Adachi, Souichi; Ken-Ichiro Citation
This study was designed to evaluate an online prognosis
 Neuro-Oncology 15(8):1074 1078, 2013. doi:10.1093/neuonc/not033 Advance Access publication March 29, 2013 NEURO-ONCOLOGY Can the prognosis of individual patients with glioblastoma be predicted using an
Neuro-Oncology 15(8):1074 1078, 2013. doi:10.1093/neuonc/not033 Advance Access publication March 29, 2013 NEURO-ONCOLOGY Can the prognosis of individual patients with glioblastoma be predicted using an
Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy
 Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy Guidelines for postoperative irradiation of cervical cancer Contents: 1. Treatment planning for EBRT. 2 2. Target definition for
Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy Guidelines for postoperative irradiation of cervical cancer Contents: 1. Treatment planning for EBRT. 2 2. Target definition for
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES
 MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
Intensity modulated radiotherapy (IMRT) for treatment of post-operative high grade glioma in the right parietal region of brain
 for treatment of post-operative high grade glioma in the right parietal region of brain") 1 Carol Boyd March Case Study March 11, 2013 Intensity modulated radiotherapy (IMRT) for treatment of post-operative high grade glioma in the right parietal region of brain History of Present Illness:
1 Carol Boyd March Case Study March 11, 2013 Intensity modulated radiotherapy (IMRT) for treatment of post-operative high grade glioma in the right parietal region of brain History of Present Illness:
Marizomib (MRZ): Brain Penetrant Irreversible Pan-Proteasome Inhibitor
: Brain Penetrant Irreversible Pan-Proteasome Inhibitor") MARIZOMIB (MRZ) WITH BEVACIZUMAB (BEV) IN WHO GRADE IV MALIGNANT GLIOMA (G4 MG): FULL ENROLLMENT RESULTS FROM THE PHASE 1, MULTICENTER, OPEN-LABEL STUDY Daniela Bota, MD, PhD 1, Annick Desjardins, MD,
MARIZOMIB (MRZ) WITH BEVACIZUMAB (BEV) IN WHO GRADE IV MALIGNANT GLIOMA (G4 MG): FULL ENROLLMENT RESULTS FROM THE PHASE 1, MULTICENTER, OPEN-LABEL STUDY Daniela Bota, MD, PhD 1, Annick Desjardins, MD,
Evaluation of Three-dimensional Conformal Radiotherapy and Intensity Modulated Radiotherapy Techniques in High-Grade Gliomas
 1 Carol Boyd Comprehensive Case Study July 11, 2013 Evaluation of Three-dimensional Conformal Radiotherapy and Intensity Modulated Radiotherapy Techniques in High-Grade Gliomas Abstract: Introduction:
1 Carol Boyd Comprehensive Case Study July 11, 2013 Evaluation of Three-dimensional Conformal Radiotherapy and Intensity Modulated Radiotherapy Techniques in High-Grade Gliomas Abstract: Introduction:
Efficacy of neuroradiological imaging, neurological examination, and symptom status in follow-up assessment of patients with high-grade gliomas
 J Neurosurg 93:201 207, 2000 Efficacy of neuroradiological imaging, neurological examination, and symptom status in follow-up assessment of patients with high-grade gliomas EVANTHIA GALANIS, M.D., JAN
J Neurosurg 93:201 207, 2000 Efficacy of neuroradiological imaging, neurological examination, and symptom status in follow-up assessment of patients with high-grade gliomas EVANTHIA GALANIS, M.D., JAN
Accepted Manuscript. Surgery for mesothelioma: less is more, more or less. Steven Milman, MD, Thomas Ng, MD
 Accepted Manuscript Surgery for mesothelioma: less is more, more or less Steven Milman, MD, Thomas Ng, MD PII: S0022-5223(17)32706-X DOI: 10.1016/j.jtcvs.2017.11.029 Reference: YMTC 12266 To appear in:
Accepted Manuscript Surgery for mesothelioma: less is more, more or less Steven Milman, MD, Thomas Ng, MD PII: S0022-5223(17)32706-X DOI: 10.1016/j.jtcvs.2017.11.029 Reference: YMTC 12266 To appear in:
BC Cancer Protocol Summary for Treatment of Elderly Newly Diagnosed Glioma Patient with Concurrent and Adjuvant Temozolomide and Radiation Therapy
 BC Cancer Protocol Summary for Treatment of Elderly Newly Diagnosed Glioma Patient with Concurrent Adjuvant Temozolomide Radiation Therapy Protocol Code Tumour Group Contact Physician CNELTZRT Neuro-Oncology
BC Cancer Protocol Summary for Treatment of Elderly Newly Diagnosed Glioma Patient with Concurrent Adjuvant Temozolomide Radiation Therapy Protocol Code Tumour Group Contact Physician CNELTZRT Neuro-Oncology
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Long GV, Hauschild A, Santinami M, et al. Adjuvant dabrafenib
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Long GV, Hauschild A, Santinami M, et al. Adjuvant dabrafenib
Accepted Manuscript. Keeping Surgery Relevant in Oligometastatic Non-Small Cell Lung Cancer. Jessica S. Donington, MD, MSCR
 Accepted Manuscript Keeping Surgery Relevant in Oligometastatic Non-Small Cell Lung Cancer Jessica S. Donington, MD, MSCR PII: S0022-5223(18)32903-9 DOI: https://doi.org/10.1016/j.jtcvs.2018.10.124 Reference:
Accepted Manuscript Keeping Surgery Relevant in Oligometastatic Non-Small Cell Lung Cancer Jessica S. Donington, MD, MSCR PII: S0022-5223(18)32903-9 DOI: https://doi.org/10.1016/j.jtcvs.2018.10.124 Reference:
Epidemiology and outcome research of glioma patients in Southern Switzerland: A population based analysis
 Epidemiology and outcome research of glioma patients in Southern Switzerland: A population based analysis G. Pesce 1, A. Bordoni, F. Montanaro, R. Renella 3, A. Richetti 1, D. Boscherini 3, S. Mauri 4,
Epidemiology and outcome research of glioma patients in Southern Switzerland: A population based analysis G. Pesce 1, A. Bordoni, F. Montanaro, R. Renella 3, A. Richetti 1, D. Boscherini 3, S. Mauri 4,
Impact of pre-treatment symptoms on survival after palliative radiotherapy An improved model to predict prognosis?
 Impact of pre-treatment symptoms on survival after palliative radiotherapy An improved model to predict prognosis? Thomas André Ankill Kämpe 30.05.2016 MED 3950,-5 year thesis Profesjonsstudiet i medisin
Impact of pre-treatment symptoms on survival after palliative radiotherapy An improved model to predict prognosis? Thomas André Ankill Kämpe 30.05.2016 MED 3950,-5 year thesis Profesjonsstudiet i medisin
VAL-083: Validated DNA-targeting Agent for Underserved Cancer Patients. September 2018
 VAL-083: Validated DNA-targeting Agent for Underserved Cancer Patients September 2018 Forward-Looking Statements Any statements contained in this presentation that do not describe historical facts may
VAL-083: Validated DNA-targeting Agent for Underserved Cancer Patients September 2018 Forward-Looking Statements Any statements contained in this presentation that do not describe historical facts may
Background. Central nervous system (CNS) tumours. High-grade glioma
 tumours. High-grade glioma") 25 4. Central nervous system (CNS) tumours Background Two important considerations underpin the choice of treatment fractionation in neurooncology. First, the results of treatment vary widely and, second,
25 4. Central nervous system (CNS) tumours Background Two important considerations underpin the choice of treatment fractionation in neurooncology. First, the results of treatment vary widely and, second,
Radiation Therapy for Soft Tissue Sarcomas
 Radiation Therapy for Soft Tissue Sarcomas Alexander R. Gottschalk, MD, PhD Assistant Professor, Radiation Oncology University of California, San Francisco 1/25/08 NCI: limb salvage vs. amputation 43 patients
Radiation Therapy for Soft Tissue Sarcomas Alexander R. Gottschalk, MD, PhD Assistant Professor, Radiation Oncology University of California, San Francisco 1/25/08 NCI: limb salvage vs. amputation 43 patients
Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey
 Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
SUCCESSFUL TREATMENT OF METASTATIC BRAIN TUMOR BY CYBERKNIFE: A CASE REPORT
 SUCCESSFUL TREATMENT OF METASTATIC BRAIN TUMOR BY CYBERKNIFE: A CASE REPORT Cheng-Ta Hsieh, 1 Cheng-Fu Chang, 1 Ming-Ying Liu, 1 Li-Ping Chang, 2 Dueng-Yuan Hueng, 3 Steven D. Chang, 4 and Da-Tong Ju 1
SUCCESSFUL TREATMENT OF METASTATIC BRAIN TUMOR BY CYBERKNIFE: A CASE REPORT Cheng-Ta Hsieh, 1 Cheng-Fu Chang, 1 Ming-Ying Liu, 1 Li-Ping Chang, 2 Dueng-Yuan Hueng, 3 Steven D. Chang, 4 and Da-Tong Ju 1
An international study under the guidance of the European Organization
 2617 COMMENTARY Chemotherapy for Glioblastoma Is Costly Better? Ute Linz, MD, PhD Juelich Research Center, IKP/INB, Juelich, Germany. Address for reprints: Ute Linz, MD, PhD, Forschungszentrum J ulich
2617 COMMENTARY Chemotherapy for Glioblastoma Is Costly Better? Ute Linz, MD, PhD Juelich Research Center, IKP/INB, Juelich, Germany. Address for reprints: Ute Linz, MD, PhD, Forschungszentrum J ulich
Brain Tumor Treatment
 Scan for mobile link. Brain Tumor Treatment Brain Tumors Overview A brain tumor is a group of abnormal cells that grows in or around the brain. Tumors can directly destroy healthy brain cells. They can
Scan for mobile link. Brain Tumor Treatment Brain Tumors Overview A brain tumor is a group of abnormal cells that grows in or around the brain. Tumors can directly destroy healthy brain cells. They can
Early postoperative tumor progression predicts clinical outcome in glioblastoma implication for clinical trials
 J Neurooncol (2017) 132:249 254 DOI 10.1007/s11060-016-2362-z CLINICAL STUDY Early postoperative tumor progression predicts clinical outcome in glioblastoma implication for clinical trials Andreas Merkel
J Neurooncol (2017) 132:249 254 DOI 10.1007/s11060-016-2362-z CLINICAL STUDY Early postoperative tumor progression predicts clinical outcome in glioblastoma implication for clinical trials Andreas Merkel
Newcastle Neuro-oncology Team Audit of Outcome of Glioblastoma Multiforme Chemoradiotherapy Treatment
 Newcastle Neuro-oncology Team Audit of Outcome of Glioblastoma Multiforme Chemoradiotherapy Treatment Jennifer Wright Neurosurgery SSC Audit Team Jennifer Wright, Rachel Tresman, Cyril Dubois, Surash Surash,
Newcastle Neuro-oncology Team Audit of Outcome of Glioblastoma Multiforme Chemoradiotherapy Treatment Jennifer Wright Neurosurgery SSC Audit Team Jennifer Wright, Rachel Tresman, Cyril Dubois, Surash Surash,
Going Past the Data for Temozolomide. J. Lee Villano, M.D., Ph.D., Nathalie Letarte, B.Pharm, M.Sc, Linda R. Bressler, Pharm. D.
 Going Past the Data for Temozolomide J. Lee Villano, M.D., Ph.D., Nathalie Letarte, B.Pharm, M.Sc, Linda R. Bressler, Pharm. D. Departments of Medicine (JLV), Neurosurgery (JLV) and Pharmacy Practice (LRB)
Going Past the Data for Temozolomide J. Lee Villano, M.D., Ph.D., Nathalie Letarte, B.Pharm, M.Sc, Linda R. Bressler, Pharm. D. Departments of Medicine (JLV), Neurosurgery (JLV) and Pharmacy Practice (LRB)
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms. Overall Clinical Significance 8/3/13
 Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
IAN CROCKER = TIM HOWARD
 Winship Cancer Institute of Emory University Radiation as Consolidation in the Treatment of Newly Diagnosed CNS Lymphoma versus After Failure of Chemotherapy Pro: Upfront Radiation Ian Crocker MD, FACR,
Winship Cancer Institute of Emory University Radiation as Consolidation in the Treatment of Newly Diagnosed CNS Lymphoma versus After Failure of Chemotherapy Pro: Upfront Radiation Ian Crocker MD, FACR,
CHMP Type II variation assessment report
 26 January 2017 EMA/CHMP/59238/2017 Invented name: Avastin International non-proprietary name: bevacizumab Procedure No. EMEA/H/C/000582/II/0093 Marketing authorisation holder (MAH): Roche Registration
26 January 2017 EMA/CHMP/59238/2017 Invented name: Avastin International non-proprietary name: bevacizumab Procedure No. EMEA/H/C/000582/II/0093 Marketing authorisation holder (MAH): Roche Registration
See the corresponding editorial in this issue, pp 1 2. J Neurosurg 115:3 8, An extent of resection threshold for newly diagnosed glioblastomas
 See the corresponding editorial in this issue, pp 1 2. J Neurosurg 115:3 8, 2011 An extent of resection threshold for newly diagnosed glioblastomas Clinical article Nader Sanai, M.D., 1 Mei-Yin Polley,
See the corresponding editorial in this issue, pp 1 2. J Neurosurg 115:3 8, 2011 An extent of resection threshold for newly diagnosed glioblastomas Clinical article Nader Sanai, M.D., 1 Mei-Yin Polley,
Interferon β and temozolomide combination therapy for temozolomide monotherapy refractory malignant gliomas
 MOLECULAR AND CLINICAL ONCOLOGY 3: 909-913, 2015 Interferon β and temozolomide combination therapy for temozolomide monotherapy refractory malignant gliomas HIROSHI KAWAJI, TSUTOMU TOKUYAMA, TOMOHIRO YAMASAKI,
MOLECULAR AND CLINICAL ONCOLOGY 3: 909-913, 2015 Interferon β and temozolomide combination therapy for temozolomide monotherapy refractory malignant gliomas HIROSHI KAWAJI, TSUTOMU TOKUYAMA, TOMOHIRO YAMASAKI,