Clinical Practice Guidelines
|
|
|
- Duane Banks
- 5 years ago
- Views:
Transcription
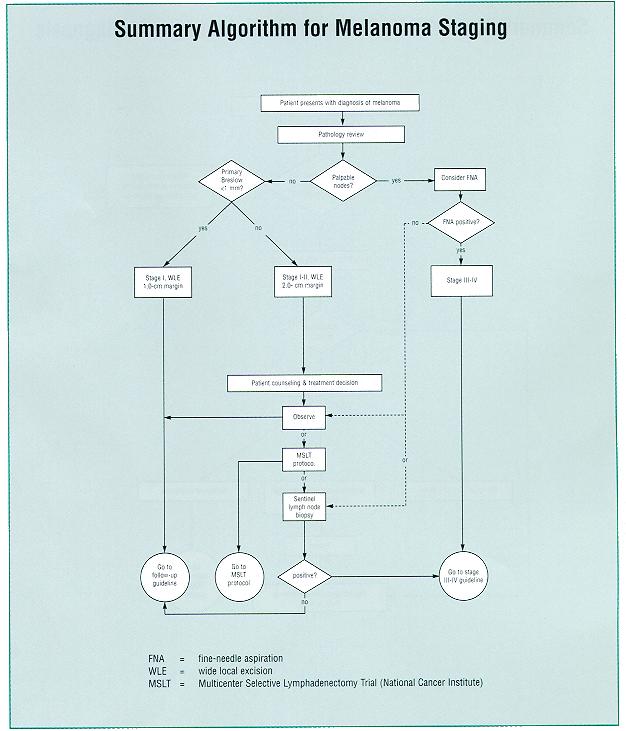
1 Clinical Practice Guidelines Clinical Practice Guidelines for Melanoma Douglas Reintgen, MD, et al H. Lee Moffitt Cancer Center & Research Institute These clinical practice guidelines for melanoma have been developed at H. Lee Moffitt Cancer Center & Research Institute under the direction of Douglas Reintgen, MD, Program Leader of the Cutaneous Oncology Program, and the following program members: Frank Glass, MD; Neil Fenske, MD; C. Wayne Cruse, MD; David Rapaport, MD; Jane Messina, MD; Karen E. Wells, MD; Ronald DeConti, MD, and Jan Marshburn, MPH. Algorithms are provided for melanoma screening and diagnosis, staging, stage III and IV management, and recurrence. Follow-up guidelines are also included. Melanoma Screening and Diagnosis Individuals with a personal or family history of melanoma or dysplastic nevi have a 10- to 100-fold increased relative risk of melanoma 1 and are eligible for screening. Those with skin phenotypes I and II (fair skin, blond or red hair, blue eyes, freckles), those raised in the sunbelt, and those with a past history of other skin cancers also have an increased relative risk of melanoma. 2 Patients with a family or personal history of dysplastic nevus, with early-onset melanoma, or who are members of a melanoma-prone family are screened for the dysplastic nevus syndrome 3 and/or the p16 gene mutation. 4 The initial screening for the p16 gene mutation will occur in the proband identified with melanoma. If the mutation is found, screening will be offered to family members. A total body skin examination performed by trained personnel identifies 90% of melanomas. 5 An excisional biopsy technique is used for suspicious lesions, and an incisional biopsy technique of the most nodular part of the lesion is used for lesions greater than 2 cm in diameter. Lesions that are found to be benign and dysplastic are followed, if the margins of excision are clear. The diagnosis of melanoma requires wide local excision (WLE), depending on the size. Melanoma Staging In order to ensure agreement with the diagnosis and depth of the melanoma, a formal pathology review is required for patients who present with a diagnosis of melanoma. This review has resulted in the remicrostaging of 5% of the melanomas reviewed. If the regional nodes are palpable and suspicious for tumor, fine needle aspiration (FNA) is performed. Those with a positive regional nodal FNA have stage III disease, and management is described in the stage III algorithm. Patients with melanomas less than 1 mm in tumor thickness are treated with a 1-cm WLE per the World Health Organization trial, 6 followed by observation. Those with melanomas equal to or greater than 1 mm in thickness are treated with a 2-cm WLE as dictated by the Intergroup Melanoma Trial. 7 For tumors greater than 4 mm in thickness, our policy is to use 2-cm margins of excision. Physicians have leeway in the size of the margin of excision for their patients with melanoma in cosmeticconcerned areas of the body (eg, the face) or functional areas of the body (eg, palms and fingers). Clear margins must be obtained. Patients are offered three choices for the management of the regional nodal basin: (1) observation of the nodes, (2) sentinel node biopsy of all basins at risk for disease, 8,9 or (3) the NCI-sponsored Multicenter Selective Lymphadenectomy Trial, 10 which randomizes patients between WLE of the primary site plus observation of their nodes vs WLE of the primary site, lymphatic mapping, and sentinel lymph node biopsy. If lymphatic mapping is not possible, patients are managed with either observation or elective node dissection. 11 If the biopsy of the sentinel lymph node is positive, the patient has stage III disease and is treated according to the stage III algorithm. Stage III and Stage IV Disease A chest radiograph and computed tomography (CT) scan of the abdomen are obtained for patients with proven metastatic melanoma. Magnetic resonance imaging of the head is performed for those with central nervous system symptoms, and a CT scan of the pelvis is obtained for patients with lower extremity or lower abdomen primary sites that demonstrate cutaneous drainage to the groin. 12 Patients with documented stage III disease and no demonstrable systemic disease undergo therapeutic regional node dissection if the disease is deemed resectable. Unresectable lesions are debulked if possible. Patients with positive margins or extranodal disease following the debulking process or a therapeutic node dissection are considered for adjuvant radiation therapy according to Radiation Therapy Oncology Group protocols. 13 These patients are at risk for systemic recurrence and also are candidates for adjuvant or unresectable stage III protocols. Patients with stage III disease that has been resected are candidates for adjuvant interferon alfa-2b according to the Eastern Cooperative Oncology Group (ECOG) Trial Those with stage IV disease with solitary metastases after staging are candidates for surgical resection and adjuvant therapy on research protocols. Patients with a positive resection margin of stage IV disease are candidates for radiation. Those with solitary and isolated metastases to the central nervous system are candidates for corticosteroids, resection, radiation therapy, and perhaps systemic therapy. 15 Patients with solitary metastases also may be treated on stage IVresearch protocols using DTIC (dacarbazine), the Dartmouth regimen, 16 BOLD (bleomycin, oncovin, lomustine, dacarbazine) chemotherapy, 17 or interferon alfa-2b. Patients with unresectable solitary metastases may be candidates for radiation therapy and/or systemic therapies. Spine metastases are treated with radiation therapy followed by chemotherapy. Patients with multiple metastases or multiple sites of metastases who are ECOG status 1 and 2 are candidates for stage IV research protocols using interferon alfa-2b plus DTIC, the Dartmouth regimen, 16 or BOLD chemotherapy. 17 Patients with an ECOG performance status worse than 2 receive palliative care. Recurrence Local and/or intransit recurrences of extremity melanoma that are confined to the extremity are treated with resection for clear margins and hyperthermic, isolated limb

2 perfusion. 18 If the tumor cannot be completely resected, a hyperthermic isolated limb perfusion is performed for palliation. Distant cutaneous or soft-tissue recurrence can be resected. Positive margins can be radiated, or patients can be treated with stage IV protocols or systemic therapies. Follow-up Follow-up guidelines for patients with melanoma are presented in the Table. Those with melanoma in situ or thin melanomas are followed with a complete skin examination to detect a second melanoma, which will occur in 5% of the population. 19 Those with intermediate-size melanoma undergo a baseline liver function and a chest radiograph; they are then followed with a physical examination of the local-regional distribution, a complete skin examination, and an evaluation of any symptom that could be a sign of systemic disease. The local-regional physical examination is expected to find 80% of all melanoma recurrences, with the remainder being marked by the appearance of systemic symptoms. 20 Patients with thick stage II and stage III disease have baseline liver function tests, a chest radiograph, and CT scan of the abdomen for staging. A CT scan of the pelvis is performed for those with metastatic disease to the groin. Patients are followed with a local-regional physical examination, a complete skin examination, and questions for systemic symptoms. Follow-up of patients with unresectable stage III and stage IV disease is guided by research or in-house protocols.
3

4 References 1. Garbe C, Buttner P, Weiss J, et al. Risk factors for developing cutaneous melanoma and criteria for identifying persons at risk: multicenter case-control study of the Central Malignant Melanoma Registry of the German Dermatological Society. J Invest Dermatol. 1994;102: Kopf A, Marghoob A, Slade J, et al. Basal and squamous cell carcinomas: risk factors for cutaneous malignant melanoma. Presented at the Sixth World Congress on Cancers of the Skin; September 16-17, 1885; Buenos Aires, Argentina. 3. Elder DE, Goldman LI, Goldman SC, et al. Dysplastic nevus syndrome: a phenotypic association of sporadic cutaneous melanoma. Cancer. 1980;46: Kamb A, Shattuck-Eidens D, Eeles R, et al. Analysis of the p16 gene (CDKN2) as a candidate for the chromosome 9p melanoma susceptibility locus. Nat Genet. 1994;8: Rigel DS, Friedman R, Kopf A, et al. Importance of complete skin exam for the detection of malignant melanoma. J Am Acad Dermatol. 1986;14: Veronesi U, Cascinelli N. Narrow excision (1-cm margin): a safe procedure for thin cutaneous melanoma. Arch Surg. 1991;126: Balch CH, Urist MM, Karakousis CP, et al. Efficacy of 2-cm surgical margins for intermediate-thickness melanoma (1 to 4 mm): results of a multi-institutional randomized surgical trial. Ann Surg. 1993;218: Norman J, Cruse CW, Espinosa C, et al. Redefinition of cutaneous lymphatic drainage with the use of lymphoscintigraphy for malignant melanoma. Am J Surg. 1991;162:
5 9. Reintgen DS, Cruse CW, Wells K, et al. The orderly progression of melanoma nodal metastases. Ann Surg. 1994;220: Multicenter Selective Lymphadenectomy Trial. National Cancer Institute Grant No. PO1 CA Balch CM, Soong SJ, Bartolucci A, et al. Efficacy of an elective lymph node dissection of 1 to 4 mm thick melanomas for patients 60 years of age and younger. Ann Surg. 1996;224: Buzaid AC, Tinoco L, Ross M, et al. Role of CT scans in the staging of melanoma patients with local-regional disease. Proc Annu Meet Am Soc Clin Oncol. 1995;14:411. Abstract A Ang KK, Byers RM, Peters LJ, et al. Regional radiotherapy as adjuvant treatment for head and neck malignancy melanoma. Arch Otolaryngol Head Neck Surg. 1990;116: Kirkwood JM, Strawderman MH, Ernstoff MS, et al. Interferon alfa-2b adjuvant therapy of high-risk resected cutaneous melanoma: the Eastern Cooperative Oncology Group Trial J Clin Oncol. 1996;14: Amer MH, Al-Sarraf M, Baker LH, et al. Malignant melanoma and central nervous system metastases: incidence, diagnosis, treatment and survival. Cancer. 1978;42: Del Prete SA, Maurer LH, O'Donnell J, et al. Combination chemotherapy with cisplatin, carmustine, dacarbazine, and tamoxifen in metastatic melanoma. Cancer Treat Rep. 1984;68: Seigler HF, Lucas VS Jr, Pickett NJ, et al. DTIC, CCNU, bleomycin and vincristine (BOLD) in metastatic melanoma. Cancer. 1980;46: Krementz ET, Ryan RF, Muchmore JH, et al. Hyperthermic regional perfusion for melanoma of the limbs. In: Balch CM, Houghton AN, Milton GW, et al, eds. Cutaneous Melanoma. 2nd ed. Philadelphia, Pa: JB Lippincott; 1992: Brobeil A, Rapaport D, Wells K, et al. Multiple primary melanomas: implications for screening and follow-up programs for melanoma. Ann Surg Oncol. 1997;4: Reintgen DS, Vollmer R, Tso CY, et al. Prognosis for recurrent stage I malignant melanoma. Arch Surg. 1987;122:
SENTINEL LYMPH node (SLN) biopsy has become
 biopsy has become") COMMENTARY Sentinel Lymph Node Biopsy for Melanoma: Controversy Despite Widespread Agreement By Kelly M. McMasters, Douglas S. Reintgen, Merrick I. Ross, Jeffrey E. Gershenwald, Michael J. Edwards, Arthur
COMMENTARY Sentinel Lymph Node Biopsy for Melanoma: Controversy Despite Widespread Agreement By Kelly M. McMasters, Douglas S. Reintgen, Merrick I. Ross, Jeffrey E. Gershenwald, Michael J. Edwards, Arthur
Nodal staging in localized melanoma. The experience of the Brescia Melanoma Unit
 The British Association of Plastic Surgeons (2003) 56, 534 539 Nodal staging in localized melanoma. The experience of the Brescia Melanoma Unit Giorgio Manca a, *, Fabio Facchetti b, Claudio Pizzocaro
The British Association of Plastic Surgeons (2003) 56, 534 539 Nodal staging in localized melanoma. The experience of the Brescia Melanoma Unit Giorgio Manca a, *, Fabio Facchetti b, Claudio Pizzocaro
NEW SURGICAL APPROACHES TO MELANOMA THERAPY
 NEW SURGICAL APPROACHES TO MELANOMA THERAPY Melanoma 2003: New Insights Into Therapy & Treatment Douglas L. Fraker, M.D. University of Pennsylvania Surgical Treatment of Melanoma Primary resection margins
NEW SURGICAL APPROACHES TO MELANOMA THERAPY Melanoma 2003: New Insights Into Therapy & Treatment Douglas L. Fraker, M.D. University of Pennsylvania Surgical Treatment of Melanoma Primary resection margins
ORIGINAL ARTICLE. Clinical Node-Negative Thick Melanoma
 ORIGINAL ARTICLE Clinical Node-Negative Thick Melanoma George I. Salti, MD; Ashwin Kansagra, MD; Michael A. Warso, MD; Salve G. Ronan, MD ; Tapas K. Das Gupta, MD, PhD, DSc Background: Patients with T4
ORIGINAL ARTICLE Clinical Node-Negative Thick Melanoma George I. Salti, MD; Ashwin Kansagra, MD; Michael A. Warso, MD; Salve G. Ronan, MD ; Tapas K. Das Gupta, MD, PhD, DSc Background: Patients with T4
1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter.
 Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Cancer Registry Report. Cancer Focus: Melanoma
 Cancer Registry Report Cancer Focus: Melanoma In 2005, nearly 60,000 patients were diagnosed with melanoma, resulting in about 7800 deaths Fortunately, melanoma is often diagnosed in an early stage when
Cancer Registry Report Cancer Focus: Melanoma In 2005, nearly 60,000 patients were diagnosed with melanoma, resulting in about 7800 deaths Fortunately, melanoma is often diagnosed in an early stage when
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival
 MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
Melanoma Quality Reporting
 Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Index. Note: Page numbers of article titles are in boldface type. A Age as factor in melanoma, Anorectal melanoma RT for, 1035
 Index Note: Page numbers of article titles are in boldface type. A Age as factor in melanoma, 947 948 Anorectal melanoma RT for, 1035 B Bacille Calmette-Guerin (BCG) in melanoma, 1008 BCG. See Bacille
Index Note: Page numbers of article titles are in boldface type. A Age as factor in melanoma, 947 948 Anorectal melanoma RT for, 1035 B Bacille Calmette-Guerin (BCG) in melanoma, 1008 BCG. See Bacille
Topics for Discussion. Malignant Melanoma. Surgical Treatment. Current Treatment of Cutaneous Melanoma 5/17/2013. Lymph Regional nodes:
 Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
Melanoma Surgery Update James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division
 Melanoma Surgery Update 2018 James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division Surgery for Melanoma Mainstay of treatment for potentially
Melanoma Surgery Update 2018 James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division Surgery for Melanoma Mainstay of treatment for potentially
Printed by Martina Huckova on 10/3/2011 3:04:54 PM. For personal use only. Not approved for distribution. Copyright 2011 National Comprehensive
 Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
Clinical Pathological Conference. Malignant Melanoma of the Vulva
 Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases
 Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases Faruk Tas, Sidika Kurul, Hakan Camlica and Erkan Topuz Institute of Oncology, Istanbul University, Istanbul, Turkey Received
Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases Faruk Tas, Sidika Kurul, Hakan Camlica and Erkan Topuz Institute of Oncology, Istanbul University, Istanbul, Turkey Received
ORIGINAL ARTICLE. Linh Lam, MD; Edward Krementz, MD; Clifton McGinness, MD; Richard Godfrey, MD
 Melanoma of the Clavicular Region Multimodal Treatment ORIGINAL ARTICLE Linh Lam, MD; Edward Krementz, MD; Clifton McGinness, MD; Richard Godfrey, MD Hypothesis: Treatment for melanoma that has metastasized
Melanoma of the Clavicular Region Multimodal Treatment ORIGINAL ARTICLE Linh Lam, MD; Edward Krementz, MD; Clifton McGinness, MD; Richard Godfrey, MD Hypothesis: Treatment for melanoma that has metastasized
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Melanoma: The Basics. What is a melanocyte?
 Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010
 Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment. Justin Rivard MD, MSc, FRCSC September 21, 2018
 You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
Melanoma. Lynn Schuchter, M.D. Associate Professor of Medicine Abramson Cancer Center of the University of Pennsylvania
 Melanoma Lynn Schuchter, M.D. Associate Professor of Medicine Abramson Cancer Center of the University of Pennsylvania WHAT IS MELANOMA? Melanoma is a type of skin cancer (a serious skin cancer because
Melanoma Lynn Schuchter, M.D. Associate Professor of Medicine Abramson Cancer Center of the University of Pennsylvania WHAT IS MELANOMA? Melanoma is a type of skin cancer (a serious skin cancer because
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Guideline for the Management of Vulval Cancer
 Version History Guideline for the Management of Vulval Cancer Version Date Brief Summary of Change Issued 2.0 20.02.08 Endorsed by the Governance Committee 2.1 19.11.10 Circulated at NSSG meeting 2.2 13.04.11
Version History Guideline for the Management of Vulval Cancer Version Date Brief Summary of Change Issued 2.0 20.02.08 Endorsed by the Governance Committee 2.1 19.11.10 Circulated at NSSG meeting 2.2 13.04.11
Melanoma. Kaushik Mukherjee MD A. Scott Pearson MD
 Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy
 Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy Dale Han, MD Assistant Professor Department of Surgery Section of Surgical Oncology No disclosures Background Desmoplastic melanoma (DM)
Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy Dale Han, MD Assistant Professor Department of Surgery Section of Surgical Oncology No disclosures Background Desmoplastic melanoma (DM)
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
K Sodhi, A Chaturvedi, S Misra, V Kumar, M Athar, M Srivastava, N Husain
 ISPUB.COM The Internet Journal of Oncology Volume 5 Number 2 Merkel cell carcinoma: Report Of Two Patients K Sodhi, A Chaturvedi, S Misra, V Kumar, M Athar, M Srivastava, N Husain Citation K Sodhi, A Chaturvedi,
ISPUB.COM The Internet Journal of Oncology Volume 5 Number 2 Merkel cell carcinoma: Report Of Two Patients K Sodhi, A Chaturvedi, S Misra, V Kumar, M Athar, M Srivastava, N Husain Citation K Sodhi, A Chaturvedi,
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R
 Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
THORACIC MALIGNANCIES
 THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012
 Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Breast Cancer Diagnosis, Treatment and Follow-up
 Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Talk to Your Doctor. Fact Sheet
 Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
Malignant Melanoma of the Head and Neck: A Brief Review of Pathophysiology, Current Staging, and Management
 The Ochsner Journal 8:181 185, 2008 f Academic Division of Ochsner Clinic Foundation Malignant Melanoma of the Head and Neck: A Brief Review of Pathophysiology, Current Staging, and Management Christian
The Ochsner Journal 8:181 185, 2008 f Academic Division of Ochsner Clinic Foundation Malignant Melanoma of the Head and Neck: A Brief Review of Pathophysiology, Current Staging, and Management Christian
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology
 Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Epithelial Cancer- NMSC & Melanoma
 Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Five years of sentinel node biopsy for melanoma: the St George s Melanoma Unit experience
 The British Association of Plastic Surgeons (2004) 57, 97 104 Five years of sentinel node biopsy for melanoma: the St George s Melanoma Unit experience Adam Topping a, *, Donald Dewar a, Victoria Rose
The British Association of Plastic Surgeons (2004) 57, 97 104 Five years of sentinel node biopsy for melanoma: the St George s Melanoma Unit experience Adam Topping a, *, Donald Dewar a, Victoria Rose
ORIGINAL ARTICLE. Patterns of Recurrence in Patients With Melanoma After Radical Lymph Node Dissection
 ORIGINAL ARTICLE Patterns of Recurrence in Patients With Melanoma After Radical Lymph Node Dissection Nir Nathansohn, MD, MHA; Jacob Schachter, MD; Haim Gutman, MD Hypothesis: Previous interventions (excisional
ORIGINAL ARTICLE Patterns of Recurrence in Patients With Melanoma After Radical Lymph Node Dissection Nir Nathansohn, MD, MHA; Jacob Schachter, MD; Haim Gutman, MD Hypothesis: Previous interventions (excisional
Recent Advances in Melanoma Staging and Therapy
 Annals of Surgical Oncology, 6(5):467 475 Published by Lippincott Williams & Wilkins 1999 The Society of Surgical Oncology, Inc. Recent Advances in Melanoma Staging and Therapy Kelly M. McMasters, MD,
Annals of Surgical Oncology, 6(5):467 475 Published by Lippincott Williams & Wilkins 1999 The Society of Surgical Oncology, Inc. Recent Advances in Melanoma Staging and Therapy Kelly M. McMasters, MD,
Malignant Melanoma among Older Adults
 Cancer Malignant Melanoma among Older Adults Wey Leong, MSc, MD, Department of Surgical Oncology, Princess Margaret Hospital, University Health Network, University of Toronto, ON. Alexandra M. Easson,
Cancer Malignant Melanoma among Older Adults Wey Leong, MSc, MD, Department of Surgical Oncology, Princess Margaret Hospital, University Health Network, University of Toronto, ON. Alexandra M. Easson,
Management of Cutaneous Melanoma of the Head and Neck and a bit about SCCA/BCC. Irvin Pathak
 Management of Cutaneous Melanoma of the Head and Neck and a bit about SCCA/BCC Irvin Pathak Objectives Risk Factors Biopsy techniques Current surgical treatment Current Status of Adjuvant Therapies Epidemiology
Management of Cutaneous Melanoma of the Head and Neck and a bit about SCCA/BCC Irvin Pathak Objectives Risk Factors Biopsy techniques Current surgical treatment Current Status of Adjuvant Therapies Epidemiology
Melanoma 10/12/18 Justin J. Baker, M.D.
 Objectives Review Incidence Risk Factors for Development Detection 10/12/18 Justin J. Baker, M.D. Treatment of Surgery Medicine Radiation What is Incidence Cancer of Melanocytes Melanocytes are normal
Objectives Review Incidence Risk Factors for Development Detection 10/12/18 Justin J. Baker, M.D. Treatment of Surgery Medicine Radiation What is Incidence Cancer of Melanocytes Melanocytes are normal
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD
 Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Principles of Surgical Oncology. Winnie Achilles Tierklinik Hollabrunn Lastenstrasse Hollabrunn
 Principles of Surgical Oncology Winnie Achilles Tierklinik Hollabrunn Lastenstrasse 2 2020 Hollabrunn boexi@gmx.de The first surgery provides the best chance for a cure in an animal with a tumor Clinical
Principles of Surgical Oncology Winnie Achilles Tierklinik Hollabrunn Lastenstrasse 2 2020 Hollabrunn boexi@gmx.de The first surgery provides the best chance for a cure in an animal with a tumor Clinical
Disclosures. SLNB for Melanoma 25/02/2014 SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION
 8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
Multiorgan Resection (Including the Pancreas) for Metastasis of Cutaneous Malignant Melanoma
 for Metastasis of Cutaneous Malignant Melanoma") MULTIMEDIA ARTICLE - Clinical Imaging Multiorgan Resection (Including the Pancreas) for Metastasis of Cutaneous Malignant Melanoma Tibor Belágyi, Péter Zsoldos, Roland Makay, Ákos Issekutz, Attila Oláh
MULTIMEDIA ARTICLE - Clinical Imaging Multiorgan Resection (Including the Pancreas) for Metastasis of Cutaneous Malignant Melanoma Tibor Belágyi, Péter Zsoldos, Roland Makay, Ákos Issekutz, Attila Oláh
LYMPHATIC DRAINAGE PATTERNS OF HEAD AND NECK CUTANEOUS MELANOMA OBSERVED ON LYMPHOSCINTIGRAPHY AND SENTINEL LYMPH NODE BIOPSY
 LYMPHATIC DRAINAGE PATTERNS OF HEAD AND NECK CUTANEOUS MELANOMA OBSERVED ON LYMPHOSCINTIGRAPHY AND SENTINEL LYMPH NODE BIOPSY Doris Lin, MD, 1 Benjamin L. Franc, MD, 2 Mohammed Kashani-Sabet, MD, 3 Mark
LYMPHATIC DRAINAGE PATTERNS OF HEAD AND NECK CUTANEOUS MELANOMA OBSERVED ON LYMPHOSCINTIGRAPHY AND SENTINEL LYMPH NODE BIOPSY Doris Lin, MD, 1 Benjamin L. Franc, MD, 2 Mohammed Kashani-Sabet, MD, 3 Mark
Therapeutic Lymph Node Dissection in Melanoma: Different Prognosis for Different Macrometastasis Sites?
 Ann Surg Oncol (01) 19:91 91 DOI.14/s44-01-401- ORIGINAL ARTICLE MELANOMAS Therapeutic Lymph Node Dissection in Melanoma: Different Prognosis for Different Macrometastasis Sites? K. P. Wevers, MD, E. Bastiaannet,
Ann Surg Oncol (01) 19:91 91 DOI.14/s44-01-401- ORIGINAL ARTICLE MELANOMAS Therapeutic Lymph Node Dissection in Melanoma: Different Prognosis for Different Macrometastasis Sites? K. P. Wevers, MD, E. Bastiaannet,
North of Scotland Cancer Network Clinical Management Guideline for Malignant Melanoma
 Nth of Scotland Cancer Netwk Clinical Management Guideline f Malignant Melanoma Based on WOSCAN CMG with further consultation within NOSCAN UNCONTROLLED WHEN PRINTED Prepared by Approved by Issue date
Nth of Scotland Cancer Netwk Clinical Management Guideline f Malignant Melanoma Based on WOSCAN CMG with further consultation within NOSCAN UNCONTROLLED WHEN PRINTED Prepared by Approved by Issue date
Metastatic Melanoma. Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds
 Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
Sentinel Lymph Node Biopsy for the T1 (Thin) Melanoma: Is It Necessary?
 Melanoma: Is It Necessary?") Sentinel Lymph Node Biopsy for the T1 (Thin) Melanoma: Is It Necessary? Maurice Y. Nahabedian, MD Anthony P. Tufaro, MD Paul N. Manson, MD The use of sentinel lymph node biopsy for the T1 melanoma is controversial.
Sentinel Lymph Node Biopsy for the T1 (Thin) Melanoma: Is It Necessary? Maurice Y. Nahabedian, MD Anthony P. Tufaro, MD Paul N. Manson, MD The use of sentinel lymph node biopsy for the T1 melanoma is controversial.
Surgical Issues in Melanoma
 Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
Management of Neck Metastasis from Unknown Primary
 Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Update on SLN and Melanoma: DECOG and MSLT-II. Gordon H. Hafner, MD, FACS
 Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
J Clin Oncol 25: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 25 NUMBER 9 MARCH 2 27 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Adjuvant Radiation Therapy Is Associated With Improved Survival in Merkel Cell Carcinoma of the Skin Pablo Mojica,
VOLUME 25 NUMBER 9 MARCH 2 27 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Adjuvant Radiation Therapy Is Associated With Improved Survival in Merkel Cell Carcinoma of the Skin Pablo Mojica,
Malignant Melanoma Early Stage. A guide for patients
 This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR Last Revision Date July 2015 1 Site Group: Gynecologic Cancer Vulvar Author: Dr. Stephane Laframboise 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR Last Revision Date July 2015 1 Site Group: Gynecologic Cancer Vulvar Author: Dr. Stephane Laframboise 1. INTRODUCTION
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Malignant melanoma: assessment and management of malignant melanoma 1.1 Short title Malignant Melanoma 2 The remit The Department
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Malignant melanoma: assessment and management of malignant melanoma 1.1 Short title Malignant Melanoma 2 The remit The Department
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Survival impact of cervical metastasis in squamous cell carcinoma of hard palate
 Vol. 116 No. 1 July 2013 Survival impact of cervical metastasis in squamous cell carcinoma of hard palate Quan Li, MD, a Di Wu, MD, b,c Wei-Wei Liu, MD, PhD, b,c Hao Li, MD, PhD, b,c Wei-Guo Liao, MD,
Vol. 116 No. 1 July 2013 Survival impact of cervical metastasis in squamous cell carcinoma of hard palate Quan Li, MD, a Di Wu, MD, b,c Wei-Wei Liu, MD, PhD, b,c Hao Li, MD, PhD, b,c Wei-Guo Liao, MD,
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective
 Procedure: An Oncologic Surgeon s Perspective") Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Dr Rosalie Stephens. Mr Richard Martin. Medical Oncologist Auckland City Hospital Auckland
 Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
Katsuhiro Yamada, Natsuko Noguti, Masaaki Tsuda, Hazime Nagato, Naoko Hasunuma, Yoshihiro Umebayashi and Motomu Manabe
 Akita J Med 36 : 45-52, 2009 45 Katsuhiro Yamada, Natsuko Noguti, Masaaki Tsuda, Hazime Nagato, Naoko Hasunuma, Yoshihiro Umebayashi and Motomu Manabe (Received 22 December 2008, Accepted 15 January 2009)
Akita J Med 36 : 45-52, 2009 45 Katsuhiro Yamada, Natsuko Noguti, Masaaki Tsuda, Hazime Nagato, Naoko Hasunuma, Yoshihiro Umebayashi and Motomu Manabe (Received 22 December 2008, Accepted 15 January 2009)
Proposed All Wales Vulval Cancer Guidelines. Dr Amanda Tristram
 Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
STAGING, BIOPSY AND NATURAL HISTORY OF TUMORS SCOTT D WEINER MD
 STAGING, BIOPSY AND NATURAL HISTORY OF TUMORS SCOTT D WEINER MD WHAT DO YOU DO WHEN THIS SHOWS UP IN YOUR OFFICE? besides panicking KEY PRINCIPLE!!! Reactive zone is the edema, neovascularity and inflammation
STAGING, BIOPSY AND NATURAL HISTORY OF TUMORS SCOTT D WEINER MD WHAT DO YOU DO WHEN THIS SHOWS UP IN YOUR OFFICE? besides panicking KEY PRINCIPLE!!! Reactive zone is the edema, neovascularity and inflammation
GUIDELINES ON PENILE CANCER
 GUIDELINES ON PENILE CANCER (Text updated March 2005) G. Pizzocaro (chairman), F. Algaba, S. Horenblas, H. van der Poel, E. Solsona, S. Tana, N. Watkin 58 Penile Cancer Eur Urol 2004;46(1);1-8 Introduction
GUIDELINES ON PENILE CANCER (Text updated March 2005) G. Pizzocaro (chairman), F. Algaba, S. Horenblas, H. van der Poel, E. Solsona, S. Tana, N. Watkin 58 Penile Cancer Eur Urol 2004;46(1);1-8 Introduction
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Management of Head and Neck Melanoma
 Management of Head and Neck Melanoma 3 James H F Shaw and Michael Fay Auckland Hospital, Great Mercury Island New Zealand 1. Introduction The incidence of melanoma in New Zealand (NZ) is one of the highest
Management of Head and Neck Melanoma 3 James H F Shaw and Michael Fay Auckland Hospital, Great Mercury Island New Zealand 1. Introduction The incidence of melanoma in New Zealand (NZ) is one of the highest
Citation for published version (APA): Francken, A. B. (2007). Primary and metastatic melanoma: aspects of follow-up and staging s.n.
: Francken, A. B. (2007). Primary and metastatic melanoma: aspects of follow-up and staging s.n.") University of Groningen Primary and metastatic melanoma Francken, Anne Brecht IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check
University of Groningen Primary and metastatic melanoma Francken, Anne Brecht IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check
Vernon K. Sondak. Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida
 Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
Major Topic. Malignant Melanoma Plastic and Reconstructive Surgery R3 陸尊惠 /VS 吳瑞星
 Major Topic Malignant Melanoma Plastic and Reconstructive Surgery R3 陸尊惠 /VS 吳瑞星 Patient Data Name: OOO Age: 70 Gender: Male Date of admission: Day 1 Chief Complaint Black skin tumor at the back of the
Major Topic Malignant Melanoma Plastic and Reconstructive Surgery R3 陸尊惠 /VS 吳瑞星 Patient Data Name: OOO Age: 70 Gender: Male Date of admission: Day 1 Chief Complaint Black skin tumor at the back of the
Reference No: Author(s) September Approval date: committee. Operational Date: August Review:
 September Approval date: committee. Operational Date: August Review:") Reference No: Title: Author(s) Ownership: Approval by: Operational Date: Systemic Anti-Cancer Therapy (SACT) guidelines for the management of malignant melanoma Dr Vicky Coyle Consultant Medical Oncologist
Reference No: Title: Author(s) Ownership: Approval by: Operational Date: Systemic Anti-Cancer Therapy (SACT) guidelines for the management of malignant melanoma Dr Vicky Coyle Consultant Medical Oncologist
The Itracacies of Staging Patients with Suspected Lung Cancer
 The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
Da Costa was the first to coin the term. Marjolin s Ulcer: A Case Report and Literature Review. Case Report. Introduction
 E-Da Medical Journal 2016;3(2):24-28 Case Report Marjolin s Ulcer: A Case Report and Literature Review Yue-Chiu Su 1, Li-Ren Chang 2 Marjolin s ulcer is an aggressive cutaneous malignancy, which is common
E-Da Medical Journal 2016;3(2):24-28 Case Report Marjolin s Ulcer: A Case Report and Literature Review Yue-Chiu Su 1, Li-Ren Chang 2 Marjolin s ulcer is an aggressive cutaneous malignancy, which is common
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine
 What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
PAPER. Prognostic Information From Sentinel Lymph Node Biopsy in Patients With Thick Melanoma
 PAPER Prognostic Information From Sentinel Lymph Node Biopsy in Patients With Thick Melanoma Charles R. Scoggins, MD, MBA; Adrianne L. Bowen, MD; Robert C. Martin II, MD, PhD; Michael J. Edwards, MD; Douglas
PAPER Prognostic Information From Sentinel Lymph Node Biopsy in Patients With Thick Melanoma Charles R. Scoggins, MD, MBA; Adrianne L. Bowen, MD; Robert C. Martin II, MD, PhD; Michael J. Edwards, MD; Douglas
Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy
 American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
Melanoma of the Skin INTRODUCTION SUMMARY OF CHANGES
 24 Melanoma of the Skin C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of other and unspecified parts of face C44.4 Skin of scalp and neck C44.5 Skin of trunk C44.6 Skin of upper limb
24 Melanoma of the Skin C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of other and unspecified parts of face C44.4 Skin of scalp and neck C44.5 Skin of trunk C44.6 Skin of upper limb
Canadian Scientific Journal. Intraoperative color detection of lymph nodes metastases in thyroid cancer
 Canadian Scientific Journal 2 (2014) Contents lists available at Canadian Scientific Journal Canadian Scientific Journal journal homepage: Intraoperative color detection of lymph nodes metastases in thyroid
Canadian Scientific Journal 2 (2014) Contents lists available at Canadian Scientific Journal Canadian Scientific Journal journal homepage: Intraoperative color detection of lymph nodes metastases in thyroid
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
1. Opdivo + Ipilumimab is now the first line therapy for metastatic melanoma.
 Melanoma UpToDate: Introduction: Risk Factors: 1. Opdivo + Ipilumimab is now the first line therapy for metastatic melanoma. Median age = 50 yrs Incidence is rising - Sun exposure: UVB (290-320nm) > UVA
Melanoma UpToDate: Introduction: Risk Factors: 1. Opdivo + Ipilumimab is now the first line therapy for metastatic melanoma. Median age = 50 yrs Incidence is rising - Sun exposure: UVB (290-320nm) > UVA
Melanoma of the Skin
 24 Melanoma of the Skin C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of other and unspecified parts of face C44.4 Skin of scalp and neck C44.5 Skin of trunk C44. Skin of upper limb
24 Melanoma of the Skin C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of other and unspecified parts of face C44.4 Skin of scalp and neck C44.5 Skin of trunk C44. Skin of upper limb
Sentinel Lymph Node Biopsy in Other Tumours: Sentinel Lymph Node Biopsy in Other Tumours. Methodology. Results. Key Questions to Consider
 Sentinel Lymph Node Biopsy in Other Tumours Dr. Rona Cheifetz Surgical Oncology Update November 24, 2006 Sentinel Lymph Node Biopsy in Other Tumours: An Operation Looking for an Application Dr. Rona Cheifetz
Sentinel Lymph Node Biopsy in Other Tumours Dr. Rona Cheifetz Surgical Oncology Update November 24, 2006 Sentinel Lymph Node Biopsy in Other Tumours: An Operation Looking for an Application Dr. Rona Cheifetz
Surgical Oncology Perspective of Melanoma
 Surgical Oncology Perspective of Melanoma Hans F. Schoellhammer, MD, FACS Assistant Clinical Professor Division of Surgical Oncology September 20, 2018 Nothing to disclose DISCLOSURE Discussion Objectives
Surgical Oncology Perspective of Melanoma Hans F. Schoellhammer, MD, FACS Assistant Clinical Professor Division of Surgical Oncology September 20, 2018 Nothing to disclose DISCLOSURE Discussion Objectives
ORIGINAL ARTICLE PROGNOSTIC IMPLICATION OF SENTINEL LYMPH NODE BIOPSY IN CUTANEOUS HEAD AND NECK MELANOMA
 ORIGINAL ARTICLE PROGNOSTIC IMPLICATION OF SENTINEL LYMPH NODE BIOPSY IN CUTANEOUS HEAD AND NECK MELANOMA Benjamin E. Saltman, MD, 1 Ian Ganly, MD, 2 Snehal G. Patel, MD, 2 Daniel G. Coit, MD, 3 Mary Sue
ORIGINAL ARTICLE PROGNOSTIC IMPLICATION OF SENTINEL LYMPH NODE BIOPSY IN CUTANEOUS HEAD AND NECK MELANOMA Benjamin E. Saltman, MD, 1 Ian Ganly, MD, 2 Snehal G. Patel, MD, 2 Daniel G. Coit, MD, 3 Mary Sue
Kentaro Tanaka, 1 Hiroki Mori, 1 Mutsumi Okazaki, 1 Aya Nishizawa, 2 and Hiroo Yokozeki Introduction. 2. Case Presentation
 Case Reports in Oncological Medicine Volume 2013, Article ID 259326, 4 pages http://dx.doi.org/10.1155/2013/259326 Case Report Long-Term Treatment Outcome after Only Popliteal Lymph Node Dissection for
Case Reports in Oncological Medicine Volume 2013, Article ID 259326, 4 pages http://dx.doi.org/10.1155/2013/259326 Case Report Long-Term Treatment Outcome after Only Popliteal Lymph Node Dissection for
General Information Key Points
 The content of this booklet was adapted from content originally published by the National Cancer Institute. Male Breast Cancer Treatment (PDQ ) Patient Version. Updated September 29,2017. https://www.cancer.gov/types/breast/patient/male-breast-treatment-pdq
The content of this booklet was adapted from content originally published by the National Cancer Institute. Male Breast Cancer Treatment (PDQ ) Patient Version. Updated September 29,2017. https://www.cancer.gov/types/breast/patient/male-breast-treatment-pdq
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Surgical Margins in Cutaneous Melanoma (2 cm Versus 5 cm for Lesions Measuring Less Than 2.1-mm Thick)
") 1941 Surgical Margins in Cutaneous Melanoma (2 cm Versus 5 cm for Lesions Measuring Less Than 2.1-mm Thick) Long-Term Results of a Large European Multicentric Phase III Study David Khayat, M.D., Ph.D.
1941 Surgical Margins in Cutaneous Melanoma (2 cm Versus 5 cm for Lesions Measuring Less Than 2.1-mm Thick) Long-Term Results of a Large European Multicentric Phase III Study David Khayat, M.D., Ph.D.
Is There a Benefit to Sentinel Lymph Node Biopsy in Patients With T4 Melanoma?
 Is There a Benefit to Sentinel Lymph Node Biopsy in atients With T4 Melanoma? Csaba Gajdos, MD 1 ; Kent A. Griffith, MH, MS 2 ; Sandra L. Wong, MD 1 ; Timothy M. Johnson, MD 1,3 ; Alfred E. Chang, MD 1
Is There a Benefit to Sentinel Lymph Node Biopsy in atients With T4 Melanoma? Csaba Gajdos, MD 1 ; Kent A. Griffith, MH, MS 2 ; Sandra L. Wong, MD 1 ; Timothy M. Johnson, MD 1,3 ; Alfred E. Chang, MD 1
Rebecca Vogel, PGY-4 March 5, 2012
 Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
BACK TO TABLE OF CONTENTS FOCUS ON MELANOMA Oncology Annual Report BAPTIST HEALTH LEXINGTON ONCOLOGY ANNUAL REPORT
 FOCUS ON MELANOMA 2014 Oncology Annual Report BAPTIST HEALTH LEXINGTON 1 2014 ONCOLOGY ANNUAL REPORT TABLE OF CONTENTS What is melanoma?...3 Who is at risk for melanoma?...3 What causes melanoma?...4 What
FOCUS ON MELANOMA 2014 Oncology Annual Report BAPTIST HEALTH LEXINGTON 1 2014 ONCOLOGY ANNUAL REPORT TABLE OF CONTENTS What is melanoma?...3 Who is at risk for melanoma?...3 What causes melanoma?...4 What
SKIN CANCER. Most common cancer diagnosis 40% of all cancers
 SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
Patent Blue Dye (P.B.D) tums.ac.ir
 tums.ac.ir") 80-84 1387 2 66 80 : 30 :.. 1385 1382.. Patent Blue Dye (P.B.D). 48 :. - (%47)13 19 195 17.. :.. : * * 88723410 : email: omranipour@ tums.ac.ir. 4 5. Patent Blue Dye (P.B.D) 6-8 %13. %20 1 2. 3 1992 Morton.
80-84 1387 2 66 80 : 30 :.. 1385 1382.. Patent Blue Dye (P.B.D). 48 :. - (%47)13 19 195 17.. :.. : * * 88723410 : email: omranipour@ tums.ac.ir. 4 5. Patent Blue Dye (P.B.D) 6-8 %13. %20 1 2. 3 1992 Morton.
EAU GUIDELINES ON PENILE CANCER
 EAU GUIDELINES ON PENILE CANCER (Text update April 2014) O.W. Hakenberg (Chair), E. Compérat, S. Minhas, A. Necchi, C. Protzel, N. Watkin Guidelines Associate: R. Robinson Introduction and epidemiology
EAU GUIDELINES ON PENILE CANCER (Text update April 2014) O.W. Hakenberg (Chair), E. Compérat, S. Minhas, A. Necchi, C. Protzel, N. Watkin Guidelines Associate: R. Robinson Introduction and epidemiology
Surgery for Melanoma and What s on the Horizon
 and What s on the Horizon Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background/Overview 76,870 cases of melanoma estimated
and What s on the Horizon Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background/Overview 76,870 cases of melanoma estimated