Clinical Pathological Conference. Malignant Melanoma of the Vulva
|
|
|
- Shannon Warren
- 5 years ago
- Views:
Transcription
1 Clinical Pathological Conference Malignant Melanoma of the Vulva

2 History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge Not painful Consulted TKO Hospital and examination showed 3x1 cm vulval mass at left labia minor near the urethral meatus Biopsy showed malignant melanoma
3 Physical Examination General examination unremarkable No peripheral lymphadenopathy in supraclavicular fossa or groin PV showed a 3.5 x 1.5 cm polypoid growth arising from the inner aspect of left labia minora 1cm from the urethral meatus Vagina and cervix normal Uterus normal size and no adnexal mass felt

4 Right Left Tumour

5 Tumour Urethral Meatus

6 Urethral Meatus Pigmentation Tumour
7 Investigations CXR: No metastasis PET-CT scan: No evidence of regional or distant metastasis
8 Treatment Radical vulvectomy with removal of the distal 1cm urethra (at least 2cm margin) En bloc bilateral groin lymph node dissection performed in November 2004 Post-operative normal micturation, no incontinence, normal stream Wound healing well, no breakdown
9 Pathology Pathology: Malignant melanoma Polypoid growth with surface ulceration No lymphovascular permeation Maximum thickness from the ulcer base 12.5mm Resection margin not involved Bilateral groin lymph nodes no malignancy
10 Malignant Melanoma of Vulval (MMV) % of all melanomas in women 8-11% of all vulval malignancy Second most common malignancy after squamous cell carcinoma Mean age (cutaneous melanoma 30-40) Exposure to UV radiation: unlikely No association with parity or hormones
11 Malignant Melanoma of Vulval (MMV) - 2 Presentation: Mass Bleeding Pruritus Ulceration and discharge Change in pre-existing nevus (de novo) Constitutional symptoms ~70% no clinically detectable LN or distant metastasis DDX: Seborrhoeic keratosis, haemangioma, dermatofibroma, VIN
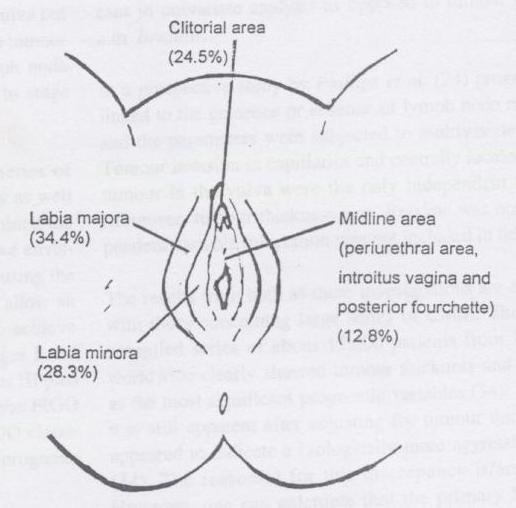
12 Distribution
13 Staging - 1 Microstaging systems for primary lesion: Clark s (1969) Breslow s (1970) Chung s (1975) Staging systems: AJCC FIGO

14 Staging - 2 Clark s: Level I-V based on dermal connective tissue plane Breslow s: Tumour thickness Chung s: Modified Clark s and Breslow s system due to lack of well defined papillary dermis of vulva

15 Staging - 3 Chung s Clark s Intraepithelial Into papillary dermis Filling papillary dermis Into reticular dermis Into subcutaneous fat
16 Staging - 4 Staging system: AJCC 1992 (American Joint Committee on Cancer) - Stage I-IV Based on microstaging of the primary lesion (including Clark s and Breslow s level) and the status of regional LN and distant sites (TMN concept) Independent prognostic factor by GOG prospective study FIGO Stage I-IV Based on tumour size and extension to adjacent organs as well as regional LN and distant metastasis Not prognostic since more influenced by depth of invasion than by tumour size
17 Prognosis - 1 Overall 5 yr survival 8-55%, mean 36 months (CMM: 72-81%)? Due to advanced stage at presentation? Advanced age of presentation? More aggressive nature? Anatomical constraints prevent proper surgical treatment Local recurrence 30-51% most commonly groin and perineum (poor outcome with median survival 5-6 months) Metastasis: Lung, liver, brain
18 Prognostic Factors - 1 Microstaging (Depth/thickness): Predicts regional node metastasis and correlates with recurrence / survival Risk of occult LN metastasis: <1mm: <5% >4mm: 70% 5 yr survival: Level I/II approaching 100% Level III/IV ~ 30-40% Level V 23-33%
19 Prognostic Factors - 2 AJCC (1992) Stages Independent prognostic factor by GOG 5-yr survival: Stage I 85%, Stage II 40%, Stage III 25% FIGO stage Not prognostic since more influenced by depth of invasion than by tumour size Ulceration, mitotic activity, nodular melanoma, lymphocytic infiltration, LVP, groin LN metastasis, central location, advanced age
20 Treatment - 1 Surgery offers the only effective therapy for control and potential cure Traditionally radical vulvectomy with bilateral groin LN dissection, but considerable morbidity Research on CMM: Treatment should be individualised according to risk factors such as microstaging Because of rarity of MMV, retrospective data only. Therapy based on treatment data of CMM
21 Treatment - 2 Treatment consideration include: Extent of the resection Regional lymph node dissection
22 Extent of Resection - 1 Based on randomised trials for CMM Thickness <1mm: 1cm margin Thickness 1-4mm: 2cm margin (2cm VS 4cm margins same 10 yr local recurrence / survival) Studies on MMV Retrospective studies similar survival associated with radical wide local excision with radical vulvectomy
23 Extent of Resection - 2 Due to morbidity associated with radical vulvectomy Trend towards more conservative resection as for CMM However, radical vulvectomy may sometimes be necessary to achieve adequate margins in bulky central mucosal lesions
24 Regional LN Dissection - 1 For clinically involved LNs without distant metastasis: Therapeutic with better outcome (CMM) For clinically no palpable LN: Controversial Provides prognostic information,? better control of disease and? determine adjuvant treatment Thin tumours <0.76mm (LN metastasis <5% if <1mm): No survival benefit Intermediate thickness (1-4mm) Intergroup Surgical Melanoma Program Better survival for subgroup: 1-2mm, <= 60 yrs, without tumour ulceration Thick tumours >4mm (LN metastasis > 70%): No survival benefit May improve outcome if regional micrometastasis are isolated sufficiently to prevent further dissemination to distant sites
25 Regional LN Dissection - 2 Sentinel node assessment: Presumed regional lymphadenectomy prolongs survival The Multicenter Selective Lymphadenectomy Trial (MSLT) for CMM: Wide local excision alone VS wide local excision plus sentinel node assessment with SCLND (Selective Complete LN Dissection) for tumour >1mm without clinically regional LN metastasis
26 Adjuvant Treatment Adjuvant therapy for deep lesions and positive LNs/metastatic disease: Radiotherapy: radio-resistant (may respond to higher dosage) Chemotherapy (Dacabazine VS combination): palliative Chemotherapy with tamoxifen Immunotherapy: High dose interferon alfa-2b in patients with +ve LNs Limited by high toxicity, at least 67% grade 3 toxicity, 1/3 require dose delay or reduction, life threatening hepatotoxicity Vaccines Clinical Trials
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR Last Revision Date July 2015 1 Site Group: Gynecologic Cancer Vulvar Author: Dr. Stephane Laframboise 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR Last Revision Date July 2015 1 Site Group: Gynecologic Cancer Vulvar Author: Dr. Stephane Laframboise 1. INTRODUCTION
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Proposed All Wales Vulval Cancer Guidelines. Dr Amanda Tristram
 Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
Guideline for the Management of Vulval Cancer
 Version History Guideline for the Management of Vulval Cancer Version Date Brief Summary of Change Issued 2.0 20.02.08 Endorsed by the Governance Committee 2.1 19.11.10 Circulated at NSSG meeting 2.2 13.04.11
Version History Guideline for the Management of Vulval Cancer Version Date Brief Summary of Change Issued 2.0 20.02.08 Endorsed by the Governance Committee 2.1 19.11.10 Circulated at NSSG meeting 2.2 13.04.11
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG
 Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Epithelial Cancer- NMSC & Melanoma
 Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
SCAN Gynaecological Group. Clinical Management Protocols vulval cancer
 SE Scotland Cancer Network SCAN Gynaecological Group Clinical Management Protocols vulval cancer 2009 www.scan.scot.nhs.uk August 2001 updated annually, most recently INTRODUCTION The South East Scotland
SE Scotland Cancer Network SCAN Gynaecological Group Clinical Management Protocols vulval cancer 2009 www.scan.scot.nhs.uk August 2001 updated annually, most recently INTRODUCTION The South East Scotland
Vaginal intraepithelial neoplasia
 Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
Vulvar Carcinoma. Definition: Cases should be classified as carsinoma of the vulva when the primary site growth is in the vulva Malignant melanoma sho
 Carcinoma Vulva & Vagina Subdivisi Onkologi Ginekologi Bagian Obgin FK USU Vulvar Carcinoma. Definition: Cases should be classified as carsinoma of the vulva when the primary site growth is in the vulva
Carcinoma Vulva & Vagina Subdivisi Onkologi Ginekologi Bagian Obgin FK USU Vulvar Carcinoma. Definition: Cases should be classified as carsinoma of the vulva when the primary site growth is in the vulva
Update on SLN and Melanoma: DECOG and MSLT-II. Gordon H. Hafner, MD, FACS
 Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment. Justin Rivard MD, MSc, FRCSC September 21, 2018
 You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Malignant melanoma: assessment and management of malignant melanoma 1.1 Short title Malignant Melanoma 2 The remit The Department
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Malignant melanoma: assessment and management of malignant melanoma 1.1 Short title Malignant Melanoma 2 The remit The Department
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective
 Procedure: An Oncologic Surgeon s Perspective") Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures
Primary Malignant Melanoma of the Vagina: Report of Two Cases and Review of the Literature
 Archives of Clinical and Medical Case Reports doi: 10.26502/acmcr.9655007 Volume 1, Issue 2 Case Report Primary Malignant Melanoma of the Vagina: Report of Two Cases and Review of the Literature Guler
Archives of Clinical and Medical Case Reports doi: 10.26502/acmcr.9655007 Volume 1, Issue 2 Case Report Primary Malignant Melanoma of the Vagina: Report of Two Cases and Review of the Literature Guler
Printed by Martina Huckova on 10/3/2011 3:04:54 PM. For personal use only. Not approved for distribution. Copyright 2011 National Comprehensive
 Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
Topics for Discussion. Malignant Melanoma. Surgical Treatment. Current Treatment of Cutaneous Melanoma 5/17/2013. Lymph Regional nodes:
 Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter.
 Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Skin Cancer. 5 Warning Signs. American Osteopathic College of Occupational and Preventive Medicine OMED 2012, San Diego, Monday, October 8, 2012 C-1
 Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Primary Cutaneous Melanoma Pathology Reporting Proforma DD MM YYYY. *Tumour site. *Specimen laterality. *Specimen type
 Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
3/25/2019. J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse
 J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse 1 4 th most common GYN cancer 5% of malignancies of GYN type. 4850 new cases annually 1030 deaths Cigarette smoking Vulvar dystrophy (Lichen
J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse 1 4 th most common GYN cancer 5% of malignancies of GYN type. 4850 new cases annually 1030 deaths Cigarette smoking Vulvar dystrophy (Lichen
Rebecca Vogel, PGY-4 March 5, 2012
 Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
Controversies and Questions in the Surgical Treatment of Melanoma
 Controversies and Questions in the Surgical Treatment of Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Division of Endocrine and Oncologic Surgery University of Pennsylvania School
Controversies and Questions in the Surgical Treatment of Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Division of Endocrine and Oncologic Surgery University of Pennsylvania School
NAACCR Webinar Series 1
 Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Surgery for Breast Cancer
 Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
WHAT DOES THE PATHOLOGY REPORT MEAN?
 Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Vulva Cancer Histopathology Reporting Proforma
 Vulva Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Ethnicity Unknown AboriginalTorres
Vulva Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Ethnicity Unknown AboriginalTorres
Melanoma Surgery Update James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division
 Melanoma Surgery Update 2018 James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division Surgery for Melanoma Mainstay of treatment for potentially
Melanoma Surgery Update 2018 James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division Surgery for Melanoma Mainstay of treatment for potentially
Cervical cancer presentation
 Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Malignant tumors of melanocytes : Part 3. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
GUIDELINES ON PENILE CANCER
 GUIDELINES ON PENILE CANCER (Text updated March 2005) G. Pizzocaro (chairman), F. Algaba, S. Horenblas, H. van der Poel, E. Solsona, S. Tana, N. Watkin 58 Penile Cancer Eur Urol 2004;46(1);1-8 Introduction
GUIDELINES ON PENILE CANCER (Text updated March 2005) G. Pizzocaro (chairman), F. Algaba, S. Horenblas, H. van der Poel, E. Solsona, S. Tana, N. Watkin 58 Penile Cancer Eur Urol 2004;46(1);1-8 Introduction
Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy
 American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
Merkel Cell Carcinoma Case # 2
 DISCHARGE SUMMARY Admitted: 10/11/2010 Discharged: 10/13/2010 Merkel Cell Carcinoma Case # 2 Chief Compliant: A 79 year old lady status post tumor on the scalp excision and left neck likely dissection
DISCHARGE SUMMARY Admitted: 10/11/2010 Discharged: 10/13/2010 Merkel Cell Carcinoma Case # 2 Chief Compliant: A 79 year old lady status post tumor on the scalp excision and left neck likely dissection
Cervical Cancer 3/25/2019. Abnormal vaginal bleeding
 Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Melanoma Quality Reporting
 Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Vulvar cancer: Know what to expect
 Vulvar cancer: Know what to expect For women with vulvar cancer What is the vulva? The vulva is the external (outside) part of the female genitals. The vulva includes the outer and inner lip, the clitoris,
Vulvar cancer: Know what to expect For women with vulvar cancer What is the vulva? The vulva is the external (outside) part of the female genitals. The vulva includes the outer and inner lip, the clitoris,
VULVAR CARCINOMA. Page 1 of 5
 VULVAR CARCINOMA EXAMPLE OF A VULVAR CARCINOMA USING PROPOSED TEMPLATE Case: Invasive squamous cell carcinoma arising in D-VIN Tumor in left labia major Left partial vaginectomy and sentinel lymph node
VULVAR CARCINOMA EXAMPLE OF A VULVAR CARCINOMA USING PROPOSED TEMPLATE Case: Invasive squamous cell carcinoma arising in D-VIN Tumor in left labia major Left partial vaginectomy and sentinel lymph node
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012
 Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Subject Index. Dry desquamation, see Skin reactions, radiotherapy
 Subject Index Actinic keratosis disseminated disease 42 surgical excision 42 AIDS, see Kaposi s sarcoma Amifostine, skin reaction prophylaxis 111 Basal cell carcinoma, superficial X-ray therapy Bowen s
Subject Index Actinic keratosis disseminated disease 42 surgical excision 42 AIDS, see Kaposi s sarcoma Amifostine, skin reaction prophylaxis 111 Basal cell carcinoma, superficial X-ray therapy Bowen s
Dr Rosalie Stephens. Mr Richard Martin. Medical Oncologist Auckland City Hospital Auckland
 Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
Melanoma Underwriting Presented at 2018 AHOU Conference. Hank George FALU
 Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Da Costa was the first to coin the term. Marjolin s Ulcer: A Case Report and Literature Review. Case Report. Introduction
 E-Da Medical Journal 2016;3(2):24-28 Case Report Marjolin s Ulcer: A Case Report and Literature Review Yue-Chiu Su 1, Li-Ren Chang 2 Marjolin s ulcer is an aggressive cutaneous malignancy, which is common
E-Da Medical Journal 2016;3(2):24-28 Case Report Marjolin s Ulcer: A Case Report and Literature Review Yue-Chiu Su 1, Li-Ren Chang 2 Marjolin s ulcer is an aggressive cutaneous malignancy, which is common
Melanoma. Kaushik Mukherjee MD A. Scott Pearson MD
 Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
NEW SURGICAL APPROACHES TO MELANOMA THERAPY
 NEW SURGICAL APPROACHES TO MELANOMA THERAPY Melanoma 2003: New Insights Into Therapy & Treatment Douglas L. Fraker, M.D. University of Pennsylvania Surgical Treatment of Melanoma Primary resection margins
NEW SURGICAL APPROACHES TO MELANOMA THERAPY Melanoma 2003: New Insights Into Therapy & Treatment Douglas L. Fraker, M.D. University of Pennsylvania Surgical Treatment of Melanoma Primary resection margins
SKIN CANCER. Most common cancer diagnosis 40% of all cancers
 SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
Impact of Prognostic Factors
 Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Polypoid Melanoma, A Virulent Variant of the Nodular Growth Pattern
 Polypoid Melanoma, A Virulent Variant of the Nodular Growth Pattern ELIZABETH A. MANCI, M.D., CHARLES M. BALCH, M.D..TARIQ M. MURAD, M.D., PH.D., AND SENG/JAW SOONG, PH.D. Manci, Elizabeth A., Balch, Charles
Polypoid Melanoma, A Virulent Variant of the Nodular Growth Pattern ELIZABETH A. MANCI, M.D., CHARLES M. BALCH, M.D..TARIQ M. MURAD, M.D., PH.D., AND SENG/JAW SOONG, PH.D. Manci, Elizabeth A., Balch, Charles
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
Staging and Treatment Update for Gynecologic Malignancies
 Staging and Treatment Update for Gynecologic Malignancies Bunja Rungruang, MD Medical College of Georgia No disclosures 4 th most common new cases of cancer in women 5 th and 6 th leading cancer deaths
Staging and Treatment Update for Gynecologic Malignancies Bunja Rungruang, MD Medical College of Georgia No disclosures 4 th most common new cases of cancer in women 5 th and 6 th leading cancer deaths
أملس عضلي غرن = Leiomyosarcoma. Leiomyosarcoma 1 / 5
 Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
1. Opdivo + Ipilumimab is now the first line therapy for metastatic melanoma.
 Melanoma UpToDate: Introduction: Risk Factors: 1. Opdivo + Ipilumimab is now the first line therapy for metastatic melanoma. Median age = 50 yrs Incidence is rising - Sun exposure: UVB (290-320nm) > UVA
Melanoma UpToDate: Introduction: Risk Factors: 1. Opdivo + Ipilumimab is now the first line therapy for metastatic melanoma. Median age = 50 yrs Incidence is rising - Sun exposure: UVB (290-320nm) > UVA
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Melanoma: The Basics. What is a melanocyte?
 Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival
 MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
Index. Note: Page numbers of article titles are in boldface type. A Age as factor in melanoma, Anorectal melanoma RT for, 1035
 Index Note: Page numbers of article titles are in boldface type. A Age as factor in melanoma, 947 948 Anorectal melanoma RT for, 1035 B Bacille Calmette-Guerin (BCG) in melanoma, 1008 BCG. See Bacille
Index Note: Page numbers of article titles are in boldface type. A Age as factor in melanoma, 947 948 Anorectal melanoma RT for, 1035 B Bacille Calmette-Guerin (BCG) in melanoma, 1008 BCG. See Bacille
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type)
") Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
Common Benign Lesions and Skin Cancers. 22nd May 2015 Dr Mark Foley
 Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Is Hepatic Resection Needed in the Patients with Peritoneal Side T2 Gallbladder Cancer?
 Is Hepatic Resection Needed in the Patients with Peritoneal Side T2 Gallbladder Cancer? Lee H, Park JY, Youn S, Kwon W, Heo JS, Choi SH, Choi DW Department of Surgery, Samsung Medical Center Sungkyunkwan
Is Hepatic Resection Needed in the Patients with Peritoneal Side T2 Gallbladder Cancer? Lee H, Park JY, Youn S, Kwon W, Heo JS, Choi SH, Choi DW Department of Surgery, Samsung Medical Center Sungkyunkwan
Surgical Issues in Melanoma
 Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
NAACCR Hospital Registry Webinar Series
 NAACCR Hospital Registry Webinar Series October 4, 2007 Abstracting Melanoma Cancer Incidence and Treatment Data Image source: commons.wikimedia.org/wiki/image.melanoma.jpg Sites include Melanoma Skin
NAACCR Hospital Registry Webinar Series October 4, 2007 Abstracting Melanoma Cancer Incidence and Treatment Data Image source: commons.wikimedia.org/wiki/image.melanoma.jpg Sites include Melanoma Skin
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R
 Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
47. Melanoma of the Skin
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD
 Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Major Topic. Malignant Melanoma Plastic and Reconstructive Surgery R3 陸尊惠 /VS 吳瑞星
 Major Topic Malignant Melanoma Plastic and Reconstructive Surgery R3 陸尊惠 /VS 吳瑞星 Patient Data Name: OOO Age: 70 Gender: Male Date of admission: Day 1 Chief Complaint Black skin tumor at the back of the
Major Topic Malignant Melanoma Plastic and Reconstructive Surgery R3 陸尊惠 /VS 吳瑞星 Patient Data Name: OOO Age: 70 Gender: Male Date of admission: Day 1 Chief Complaint Black skin tumor at the back of the
INTRODUCTION TO CANCER STAGING
 INTRODUCTION TO CANCER STAGING Patravoot Vatanasapt, MD Dept. Otorhinolaryngology Khon Kaen Cancer Registry Faculty of Medicine Khon Kaen University THAILAND Staging is the attempt to assess the size
INTRODUCTION TO CANCER STAGING Patravoot Vatanasapt, MD Dept. Otorhinolaryngology Khon Kaen Cancer Registry Faculty of Medicine Khon Kaen University THAILAND Staging is the attempt to assess the size
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
University of Kentucky. Markey Cancer Center
 University of Kentucky Markey Cancer Center Invasive Cancer of the Vagina and Urethra Fred Ueland, MD No matter what you accomplish in your life, the size of your funeral will still be determined by the
University of Kentucky Markey Cancer Center Invasive Cancer of the Vagina and Urethra Fred Ueland, MD No matter what you accomplish in your life, the size of your funeral will still be determined by the
Case Report Long Term Survival and Continued Complete Response of Vemurafenib in a Metastatic Melanoma Patient with BRAF V600K Mutation
 Case Reports in Oncological Medicine Volume 2016, Article ID 2672671, 4 pages http://dx.doi.org/10.1155/2016/2672671 Case Report Long Term Survival and Continued Complete Response of Vemurafenib in a Metastatic
Case Reports in Oncological Medicine Volume 2016, Article ID 2672671, 4 pages http://dx.doi.org/10.1155/2016/2672671 Case Report Long Term Survival and Continued Complete Response of Vemurafenib in a Metastatic
Molecular Enhancement of Sentinel Node Evaluation
 Cochran Illustrations 060104 Molecular Enhancement of Sentinel Node Evaluation Alistair Cochran, MD and Rong Huang MD Departments of Pathology and Laboratory Medicine and Surgery, David Geffen School of
Cochran Illustrations 060104 Molecular Enhancement of Sentinel Node Evaluation Alistair Cochran, MD and Rong Huang MD Departments of Pathology and Laboratory Medicine and Surgery, David Geffen School of
GUIDELINES ON PENILE CANCER
 46 E. Solsona (chairman), F. Algaba, S. Horenblas, G. Pizzocaro, T. Windahl Eur Urol 2002;42(3):199-203 Introduction Penile carcinoma is an uncommon malignant disease with an incidence ranging from 0.1
46 E. Solsona (chairman), F. Algaba, S. Horenblas, G. Pizzocaro, T. Windahl Eur Urol 2002;42(3):199-203 Introduction Penile carcinoma is an uncommon malignant disease with an incidence ranging from 0.1
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology
 Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
17 th ESO-ESMO Masterclass in clinical Oncology
 17 th ESO-ESMO Masterclass in clinical Oncology Cervical and endometrial Cancer Cristiana Sessa IOSI Bellinzona, Switzerland Berlin, March 28 th, 2018 Presenter Disclosures None Cervical Cancer Estimated
17 th ESO-ESMO Masterclass in clinical Oncology Cervical and endometrial Cancer Cristiana Sessa IOSI Bellinzona, Switzerland Berlin, March 28 th, 2018 Presenter Disclosures None Cervical Cancer Estimated
Ano-uro-genital Melanoma
 Ano-uro-genital Melanoma Appendices Published May 2018 Commissioning and funding innovative research, while providing support and information for patients, carers and healthcare professionals 1 Introduction...
Ano-uro-genital Melanoma Appendices Published May 2018 Commissioning and funding innovative research, while providing support and information for patients, carers and healthcare professionals 1 Introduction...
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Review Article Selective Inguinal Lymphadenectomy in the Treatment of Invasive Squamous Cell Carcinoma of the Vulva
 Hindawi Publishing Corporation International Journal of Surgical Oncology Volume 2011, Article ID 284374, 6 pages doi:10.1155/2011/284374 Review Article Selective Inguinal Lymphadenectomy in the Treatment
Hindawi Publishing Corporation International Journal of Surgical Oncology Volume 2011, Article ID 284374, 6 pages doi:10.1155/2011/284374 Review Article Selective Inguinal Lymphadenectomy in the Treatment
Michael T. Tetzlaff MD, PhD
 Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Disclosures. SLNB for Melanoma 25/02/2014 SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION
 8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
Modalities of Radiation
 Modalities of Radiation Superficial radiotherapy Orthovoltage Megavoltage Photons Electrons Brachytherapy Interstitial Moulds When to refer? The vast majority of skin cancers will be managed without any
Modalities of Radiation Superficial radiotherapy Orthovoltage Megavoltage Photons Electrons Brachytherapy Interstitial Moulds When to refer? The vast majority of skin cancers will be managed without any
SENTINEL NODES FOR EARLY VULVAL CANCER:
 SENTINEL NODES FOR EARLY VULVAL CANCER: FEASIBILITY AND SAFETY IN A LOW RESOURCE SETTING LINDA ROGERS RCOG Congress 2017 None Declaration of Interests Vulval Cancer Rare 4% of all gynaecological malignancies
SENTINEL NODES FOR EARLY VULVAL CANCER: FEASIBILITY AND SAFETY IN A LOW RESOURCE SETTING LINDA ROGERS RCOG Congress 2017 None Declaration of Interests Vulval Cancer Rare 4% of all gynaecological malignancies
Malignant Melanoma Introduction increasing incidence increasing mortality skin >50% normal skin pigmented lesion
 1 Malignant Melanoma Introduction Melanoma is a malignant tumor of melanocytes, cells that are derived from the neural crest. There is an increasing incidence of melanoma, as well as an increasing mortality,
1 Malignant Melanoma Introduction Melanoma is a malignant tumor of melanocytes, cells that are derived from the neural crest. There is an increasing incidence of melanoma, as well as an increasing mortality,
What is endometrial cancer?
 Uterine cancer What is endometrial cancer? Endometrial cancer is the growth of abnormal cells in the lining of the uterus. The lining is called the endometrium. Endometrial cancer usually occurs in women
Uterine cancer What is endometrial cancer? Endometrial cancer is the growth of abnormal cells in the lining of the uterus. The lining is called the endometrium. Endometrial cancer usually occurs in women
Twenty-first refresher course. Chan Kit Sheung
 Twenty-first refresher course Chan Kit Sheung 7-5-2015 Case 1 Case 1, 29y old, G3P2, referred from MCHC Cervical smear on 27-9-2013: LGSIL, defaulted appointment Cervical smear in 12/2014: negative Colposcopy
Twenty-first refresher course Chan Kit Sheung 7-5-2015 Case 1 Case 1, 29y old, G3P2, referred from MCHC Cervical smear on 27-9-2013: LGSIL, defaulted appointment Cervical smear in 12/2014: negative Colposcopy
Citation for published version (APA): Francken, A. B. (2007). Primary and metastatic melanoma: aspects of follow-up and staging s.n.
: Francken, A. B. (2007). Primary and metastatic melanoma: aspects of follow-up and staging s.n.") University of Groningen Primary and metastatic melanoma Francken, Anne Brecht IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check
University of Groningen Primary and metastatic melanoma Francken, Anne Brecht IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check
Gynecological Cancers in Primary Care
 Gynecological Cancers in Primary Care Nora M. Lersch MSN CRNP AOCNP Division of Gynecological Oncology Objectives Identify the incidence of ovarian, cervical, vulvar and endometrial cancer Identify common
Gynecological Cancers in Primary Care Nora M. Lersch MSN CRNP AOCNP Division of Gynecological Oncology Objectives Identify the incidence of ovarian, cervical, vulvar and endometrial cancer Identify common
Quiz. b. 4 High grade c. 9 Unknown
 Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Directly Coded Summary Stage Melanoma
 Directly Coded Summary Stage Melanoma National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention and Control, National Program of Cancer Registries Directly Coded
Directly Coded Summary Stage Melanoma National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention and Control, National Program of Cancer Registries Directly Coded
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma. Michael T. Tetzlaff MD, PhD
 Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
BREAST CANCER SURGERY. Dr. John H. Donohue
 Dr. John H. Donohue HISTORY References to breast surgery in ancient Egypt (ca 3000 BCE) Mastectomy described in numerous medieval texts Petit formulated organized approach in 18 th Century Improvements
Dr. John H. Donohue HISTORY References to breast surgery in ancient Egypt (ca 3000 BCE) Mastectomy described in numerous medieval texts Petit formulated organized approach in 18 th Century Improvements
Metastatic Melanoma. Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds
 Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
How to Manage a Case of Stage-I Oropharyngeal Cancer with Very Close Cutting End Post-Operatively?
 How to Manage a Case of Stage-I Oropharyngeal Cancer with Very Close Cutting End Post-Operatively? Case Number: RT2008-07(M) Potential Audiences: Intent Doctor, Oncology Special Nurse, Resident Doctor
How to Manage a Case of Stage-I Oropharyngeal Cancer with Very Close Cutting End Post-Operatively? Case Number: RT2008-07(M) Potential Audiences: Intent Doctor, Oncology Special Nurse, Resident Doctor
Index. pet.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A C a-aminobutyric acid, carbon-labeled, 94 ABCD(E)s, of melanoma, 2 Acral-lentiginous melanoma, 3 Adrenal glands, metastasis to, structural imaging
Note: Page numbers of article titles are in boldface type. A C a-aminobutyric acid, carbon-labeled, 94 ABCD(E)s, of melanoma, 2 Acral-lentiginous melanoma, 3 Adrenal glands, metastasis to, structural imaging
receive adjuvant chemotherapy
 Women with high h risk early stage endometrial cancer should receive adjuvant chemotherapy Michael Friedlander The Prince of Wales Cancer Centre and Royal Hospital for Women The Prince of Wales Cancer
Women with high h risk early stage endometrial cancer should receive adjuvant chemotherapy Michael Friedlander The Prince of Wales Cancer Centre and Royal Hospital for Women The Prince of Wales Cancer