Rebecca Vogel, PGY-4 March 5, 2012
|
|
|
- Dominick Perry
- 6 years ago
- Views:
Transcription

1 Rebecca Vogel, PGY-4 March 5, 2012

2 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here
3 Cutaneous melanoma has become an increasingly growing problem, with a rapid rise in incidence rates in the United States over the last several decades Melanoma now accounts for 5% of all cancers diagnosed According to the American Cancer Society an estimated 62,190 new cases of melanoma were diagnosed in 2006, and approximately 7,910 patients will die of this disease



4 Several mummies of pre-colombian Incas of Peru, some estimated to be 2,400 years old, which show diffuse metastases to bones, particularly of the skull and extremities

5 Everything in excess is opposed to nature. Hippocrates John Hunter is reported to be the first to operate on metastatic melanoma in 1787 Cancerous fungous excrescence The excised tumor was preserved in the Royal College of Surgeons of England It was not until 1968 that microscopic examination of the specimen revealed it to be an example of metastatic melanoma

6 René Laennec, a French physician, was the first to describe melanoma as a disease entity Presented during a lecture for the Faculté de Médecine de Paris in 1804 and then published as a bulletin in 1806
7 As early as the mid-19th century, British surgeon William Norris recognized the importance of treatment margins in primary melanoma: Not only remove the disease, but cut away some of the healthy parts. I would, after excising the part, touch the wound with caustic so as not to leave an atom of the disease, if possible, and occasionally apply the same remedy to the skin in the vicinity
8 In the late 1800s, Herbert Snow initiated a surgical controversy by recommending elective removal of clinically normal regional lymph nodes in patients with cutaneous melanoma He believed that early removal of infected lymph nodes would prevent subsequent metastasis to distant sites and therefore improve patient outcomes
9 DIFFERENCES FROM 2002 TNM SYSTEM Mitotic rate, defined as mitoses/mm2, has been incorporated as a primary prognostic factor in defining the tumor (T) stage The Clark level of invasion, which was used in conjunction with tumor thickness in the sixth version of the TNM system, is not a statistically significant prognostic factor on multivariate analysis and is no longer utilized Immunohistochemical detection of melanoma in regional lymph nodes is now acceptable evidence of disease involvement, rather than just hematoxylin and eosin There is no minimum tumor burden to define positive regional lymph node involvement. Previously tumor deposits <0.2 mm in diameter were not considered clinically significant Isolated metastases arising in lymph nodes, skin, or subcutaneous tissue, without an identifiable primary, are classified as stage III rather than stage IV

10

11
12

13
14 For patients with nodal disease limited to micrometastases, the most important factor affecting prognosis was the number of nodes involved Five-year survival rates with one, two, or three positive lymph nodes were 71, 65, and 61 percent, respectively Other factors independently affecting prognosis: age, anatomic site, thickness, ulceration, and mitotic rate For patients with macrometastases in the regional nodes, the number of nodes was significantly associated with prognosis Five-year survival rates one, two, or three positive lymph nodes were 50, 43, and 40 percent, respectively The characteristics of the primary tumor were not independently associated with prognosis
15
16 The number of tumor-positive lymph nodes is the single most important prognostic factor in AJCC stage III melanoma CLND allows accurate assessment of the regional extent of disease and is the only effective therapeutic option for local control and potential cure
17 This analysis included 274 patients with at least one positive SLN who underwent CLND of 282 involved regional nodal basins Of the 282 SLN-positive nodal basins, 45 (16%) were found to have positive NSNs in the CLND specimen When a positive SLN is identified on either H&E staining or IHC, CLND should be performed routinely
, and macro-metastatic pattern (70%) On the other hand, NSLN involvement after a positive SLN was found in 11.")
18 The highest percentages of NSLN involvement were found in patients with Breslow thickness >4 mm (52%), ulceration (53.6%), and macro-metastatic pattern (70%) On the other hand, NSLN involvement after a positive SLN was found in 11.5% of patients with thin primary (between 1 and 2 mm)
19
20 The presence of at least one of these adverse factors identify patients in whom CLND is mandatory On the other hand, the finding of no adverse indicators identify patients who could be spared from CLND in the presence of significant co-morbidities or elderly age
21
22

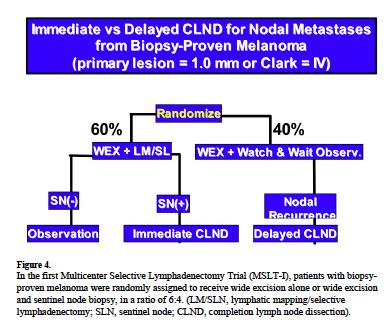
23 1269 patients: sentinel- node biopsy provided important prognostic information for the staging of intermediate thickness 1.2 to 3.5 mm Survival could be prolonged be immediate lymphadenectomy The 5-year survival rate was higher among those who underwent immediate lymphadenectomy than among those in whom lymphadenectomy was delayed (72.3±4.6% vs. 52.4±5.9%)
24 Impact of MSLT-I Early CLND was performed in 225 patients, and in the wide excision-alone arm 132 have undergone delayed CLND The two groups were similar for primary tumor features, body mass index, basin location and demographics except age, which was higher for delayed CLND The number of nodes evaluated and the number of positive nodes was greater for delayed CLND Lymphedema was significantly higher in the delayed CLND group (20.4% vs. 12.4%, p=0.04) Length of inpatient hospitalization was longer for delayed CLND
25 A retrospective analysis of 760/2313 patients with stage III melanoma who underwent lymphadenectomy for node-positive melanoma Conditional disease-specific survival (the survival probability after a given length of survival) improved from 78 to 90 percent from year 0 to year 5 for patients with stage IIIa melanoma, and from 54 to 79 percent and 39 to 78 percent for those with stage IIIb and IIIc disease
26 Compared with SLNB alone, CLND does not seem to be associated with improved survival however there was CLND was an associated improved diseasespecific survival at 5 years for a subgroup of patients Age <60 years with nonulcerated tumors 2 mm
27 CLND is considered the standard of care in melanoma patients found to have SLN metastasis Additional disease in the CLND specimen can dramatically impact survival
28 PROS CONS A CLND helps to accurately determine the stage of the melanoma, which assists with recommendations for adjuvant treatment The number of nodes containing melanoma cells is a predictor of survival for patients who have stage III disease, and only a CLND can provide this information Some studies show that 20% of patients who undergo a CLND immediately after finding out they have a positive sentinel lymph node experience improved survival. This is especially true for patients who had intermediate-thickness tumors on their skin (1.2 to 3.5 mm) By stopping the spread of melanoma at the lymph nodes, a CLND optimizes the chance for a cure Complications of a CLND occur in up to 67% of patients, especially in those over 60. These include: Seroma Infection Lymphedema Numbness, tingling, or pain in the surgical area Sloughing of skin over the area
29 MSLT-II Ongoing phase III trial comparing immediate completion lymph node dissection with a strategy of observation and completion lymph node dissection if there is evidence of regional lymph node recurrence This trial is limited to patients with a primary melanoma that has a Breslow thickness of 1.20 mm or greater and Clark Level III or is a Clark Level IV or V regardless of Breslow thickness Results for the primary endpoint, melanoma-specific survival, are not anticipated until 2022
30 Primary Outcome Measures: Melanoma-specific survival This is defined as the time between the date of a subject's randomization (or date of CLND for those randomized to the CLND arm) and the date of death due to melanoma. Subjects are followed until death or 10yrs Secondary Outcome Measures: Disease-free survival over 10 years of follow up Recurrence during 10 years of follow up

31
32 Conclusion Early CLND, guided by SLN biopsy is the cornerstone of treatment for patients with intermediate thickness melanoma Benefits of this treatment paradigm include: Unequaled prognostic value of regional nodal status Ability to select patients for adjuvant therapy or clinical trials Improved disease-free survival For those with regional micrometastases at presentation, improved melanoma-specific survival
33 Boughton B (2009). Should lymphadenectomy be the standard of care in melanoma metastasis to the sentinel lymph nodes? Oncology News Intl. 18(5). Morton DL, Thompson JF, Cochran A, et al (2006). Sentinel-node biopsy or nodal observation in melanoma. N Engl J Med Sep 28;355(13): Thomas JM (2005). Time to Re-Evaluate Sentinel Node Biopsy in Melanoma Post-Multicenter Selective Lymphadenectomy Trial. J Clin Oncol Dec 20;23(36): van Akkooi AC, Rutkowski P, van der Ploeg IM, et al (2009). Long-term follow-up of patients with minimal sentinel node tumor burden (< 0.1mm) according to Rotterdam criteria: A study of the EORTC Melanoma Group. J Clin Oncol 27:15s, 2009 (suppl; abstr 9005). Gershenwald JE, Berman RS, Porter G, et al. Regional nodal basin control is not compromised by previous sentinel lymph node biopsy in patients with melanoma. Ann Surg Oncol 2000; 7: Wong, Sandra et al. Melanoma Patients with Positive Sentinel Nodes Who Did Not Undergo Completion Lymphadenectomy: A Multi-Institutional Study. Annals of Surgical Oncology, 13(6): 809)816 DOI: /ASO Balch CM, Gershenwald JE, Soong SJ, et al. Multivariate analysis of prognostic factors among 2,313 patients with stage III melanoma: comparison of nodal micrometastases versus macrometastases. J Clin Oncol 2010; 28:2452 Farin Amersi, MD and Donald L. Morton, MD. THE ROLE OF SENTINEL LYMPH NODE BIOPSY IN THE MANAGEMENT OF MELANOMA. Published in final edited form as: Adv Surg ; 41: Iris M. C. van der Ploeg, MD, et al. Is Completion Lymph Node Dissection Needed in Case of Minimal Melanoma Metastasis in the Sentinel Node? Annals of Surgery Volume 249, Number 6, June 2009 Mark B. Faries, MD, John F. Thompson Ann Surg Oncol December ; 17(12): doi: /s Current Management of Melanoma: Benefits of Surgical Staging and Adjuvant TherapyKELLY M. McMASTERS, MD, PhD1* AND SUSAN M. SWETTER, MD2. Journal of Surgical Oncology 2003;82: ON THE ANTIQUITY OF MELANOMA OSCARU RTEACBA., MD, AND GEORGTE. PACK, MD. CANCER May 1966 McLeod, G.; Davis, N.; Sober, A. A history of melanoma from Hunter to Clark. In: Balch, C.; Houghton, A.; Sober, A.; Soong, S., editors. Cutaneous Melanoma. 4. St. Louis: Quality Medical Publishing; p. 1-11
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective
 Procedure: An Oncologic Surgeon s Perspective") Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures
Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy
 American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
Controversies and Questions in the Surgical Treatment of Melanoma
 Controversies and Questions in the Surgical Treatment of Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Division of Endocrine and Oncologic Surgery University of Pennsylvania School
Controversies and Questions in the Surgical Treatment of Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Division of Endocrine and Oncologic Surgery University of Pennsylvania School
Surgical Issues in Melanoma
 Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy
 Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy Dale Han, MD Assistant Professor Department of Surgery Section of Surgical Oncology No disclosures Background Desmoplastic melanoma (DM)
Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy Dale Han, MD Assistant Professor Department of Surgery Section of Surgical Oncology No disclosures Background Desmoplastic melanoma (DM)
Disclosures. SLNB for Melanoma 25/02/2014 SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION
 8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
Talk to Your Doctor. Fact Sheet
 Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
Nodal Treatment in Melanoma: Snow to MSLT-II
 Nodal Treatment in Melanoma: Snow to MSLT-II Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Program Director, JWCI Complex General Surgical Oncology Fellowship Director,
Nodal Treatment in Melanoma: Snow to MSLT-II Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Program Director, JWCI Complex General Surgical Oncology Fellowship Director,
Update on SLN and Melanoma: DECOG and MSLT-II. Gordon H. Hafner, MD, FACS
 Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
No Benefit to Routine Completion Lymphadenectomy for Sentinel Lymph Node Positive Melanoma
 No Benefit to Routine Completion Lymphadenectomy for Sentinel Lymph Node Positive Melanoma Michael Lowe, MD Assistant Professor of Surgery Winship Cancer Institute Emory University School of Medicine July
No Benefit to Routine Completion Lymphadenectomy for Sentinel Lymph Node Positive Melanoma Michael Lowe, MD Assistant Professor of Surgery Winship Cancer Institute Emory University School of Medicine July
Sentinel Node Alphabet Soup: MSLT-1, DeCOG-SLT, MSLT-2, UNC
 Sentinel Node Alphabet Soup: MSLT-1, DeCOG-SLT, MSLT-2, UNC David W. Ollila MD James and Jesse Millis Professor of Surgery University of North Carolina, Chapel Hill Disclosures: None July 15, 2018 AJCC
Sentinel Node Alphabet Soup: MSLT-1, DeCOG-SLT, MSLT-2, UNC David W. Ollila MD James and Jesse Millis Professor of Surgery University of North Carolina, Chapel Hill Disclosures: None July 15, 2018 AJCC
Morphological characteristics of the primary tumor and micrometastases in sentinel lymph nodes as a predictor of melanoma progression
 Morphological characteristics of the primary tumor and micrometastases in sentinel lymph nodes as a predictor of melanoma progression M.N. Kukushkina, S.I. Korovin, O.I. Solodyannikova, G.G. Sukach, A.Yu.
Morphological characteristics of the primary tumor and micrometastases in sentinel lymph nodes as a predictor of melanoma progression M.N. Kukushkina, S.I. Korovin, O.I. Solodyannikova, G.G. Sukach, A.Yu.
Molecular Enhancement of Sentinel Node Evaluation
 Cochran Illustrations 060104 Molecular Enhancement of Sentinel Node Evaluation Alistair Cochran, MD and Rong Huang MD Departments of Pathology and Laboratory Medicine and Surgery, David Geffen School of
Cochran Illustrations 060104 Molecular Enhancement of Sentinel Node Evaluation Alistair Cochran, MD and Rong Huang MD Departments of Pathology and Laboratory Medicine and Surgery, David Geffen School of
Update on Lymph Node Management in Melanoma
 Update on Lymph Node Management in Melanoma John T. Vetto MD, FACS Professor of Surgery Division of Surgical Oncology Oregon Health & Science University Portland, Oregon Lymph Nodes in Melanoma Outline
Update on Lymph Node Management in Melanoma John T. Vetto MD, FACS Professor of Surgery Division of Surgical Oncology Oregon Health & Science University Portland, Oregon Lymph Nodes in Melanoma Outline
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment. Justin Rivard MD, MSc, FRCSC September 21, 2018
 You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
Melanoma Surgery Update James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division
 Melanoma Surgery Update 2018 James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division Surgery for Melanoma Mainstay of treatment for potentially
Melanoma Surgery Update 2018 James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division Surgery for Melanoma Mainstay of treatment for potentially
Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival
 MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
Melanoma Quality Reporting
 Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
Predictive Factors for the Positivity of the Sentinel Lymph Node in Malignant Melanoma
 ORIGINAL RESEARCH SURGERY // ANATOMO-PATHOLOGY Predictive Factors for the Positivity of the Sentinel Lymph Node in Malignant Melanoma Călin Crăciun, Orsolya Hankó- Bauer, Zalán Benedek, Sorin Sorlea, Marius
ORIGINAL RESEARCH SURGERY // ANATOMO-PATHOLOGY Predictive Factors for the Positivity of the Sentinel Lymph Node in Malignant Melanoma Călin Crăciun, Orsolya Hankó- Bauer, Zalán Benedek, Sorin Sorlea, Marius
Topics for Discussion. Malignant Melanoma. Surgical Treatment. Current Treatment of Cutaneous Melanoma 5/17/2013. Lymph Regional nodes:
 Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature. Sasha Jenkins
 Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature By Sasha Jenkins A Master s Paper submitted to the faculty of the University of North Carolina at Chapel Hill in
Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature By Sasha Jenkins A Master s Paper submitted to the faculty of the University of North Carolina at Chapel Hill in
SENTINEL LYMPH node (SLN) biopsy has become
 biopsy has become") COMMENTARY Sentinel Lymph Node Biopsy for Melanoma: Controversy Despite Widespread Agreement By Kelly M. McMasters, Douglas S. Reintgen, Merrick I. Ross, Jeffrey E. Gershenwald, Michael J. Edwards, Arthur
COMMENTARY Sentinel Lymph Node Biopsy for Melanoma: Controversy Despite Widespread Agreement By Kelly M. McMasters, Douglas S. Reintgen, Merrick I. Ross, Jeffrey E. Gershenwald, Michael J. Edwards, Arthur
ORIGINAL ARTICLE PROGNOSTIC IMPLICATION OF SENTINEL LYMPH NODE BIOPSY IN CUTANEOUS HEAD AND NECK MELANOMA
 ORIGINAL ARTICLE PROGNOSTIC IMPLICATION OF SENTINEL LYMPH NODE BIOPSY IN CUTANEOUS HEAD AND NECK MELANOMA Benjamin E. Saltman, MD, 1 Ian Ganly, MD, 2 Snehal G. Patel, MD, 2 Daniel G. Coit, MD, 3 Mary Sue
ORIGINAL ARTICLE PROGNOSTIC IMPLICATION OF SENTINEL LYMPH NODE BIOPSY IN CUTANEOUS HEAD AND NECK MELANOMA Benjamin E. Saltman, MD, 1 Ian Ganly, MD, 2 Snehal G. Patel, MD, 2 Daniel G. Coit, MD, 3 Mary Sue
Tumor Mitotic Rate Added to the Equation: Melanoma Prognostic Factors Changed?
 Ann Surg Oncol (2015) 22:2978 2987 DOI 10.1245/s10434-014-4349-3 ORIGINAL ARTICLE MELANOMAS Tumor Mitotic Rate Added to the Equation: Melanoma Prognostic Factors Changed? A Single-Institution Database
Ann Surg Oncol (2015) 22:2978 2987 DOI 10.1245/s10434-014-4349-3 ORIGINAL ARTICLE MELANOMAS Tumor Mitotic Rate Added to the Equation: Melanoma Prognostic Factors Changed? A Single-Institution Database
Sentinel Lymph Node Biopsy: Current Evidence for its Role in Managing Melanoma
 Sentinel Lymph Node Biopsy: Current Evidence for its Role in Managing Melanoma John A Zitelli MD Adjunct Clinical Associate Professor Dermatology, Otolaryngology, Plastic Surgery University of Pittsburgh
Sentinel Lymph Node Biopsy: Current Evidence for its Role in Managing Melanoma John A Zitelli MD Adjunct Clinical Associate Professor Dermatology, Otolaryngology, Plastic Surgery University of Pittsburgh
PAPER. Prognostic Information From Sentinel Lymph Node Biopsy in Patients With Thick Melanoma
 PAPER Prognostic Information From Sentinel Lymph Node Biopsy in Patients With Thick Melanoma Charles R. Scoggins, MD, MBA; Adrianne L. Bowen, MD; Robert C. Martin II, MD, PhD; Michael J. Edwards, MD; Douglas
PAPER Prognostic Information From Sentinel Lymph Node Biopsy in Patients With Thick Melanoma Charles R. Scoggins, MD, MBA; Adrianne L. Bowen, MD; Robert C. Martin II, MD, PhD; Michael J. Edwards, MD; Douglas
NEW SURGICAL APPROACHES TO MELANOMA THERAPY
 NEW SURGICAL APPROACHES TO MELANOMA THERAPY Melanoma 2003: New Insights Into Therapy & Treatment Douglas L. Fraker, M.D. University of Pennsylvania Surgical Treatment of Melanoma Primary resection margins
NEW SURGICAL APPROACHES TO MELANOMA THERAPY Melanoma 2003: New Insights Into Therapy & Treatment Douglas L. Fraker, M.D. University of Pennsylvania Surgical Treatment of Melanoma Primary resection margins
1
 www.clinicaloncology.com.ua 1 Prognostic factors of appearing micrometastases in sentinel lymph nodes in skin melanoma M.N.Kukushkina, S.I.Korovin, O.I.Solodyannikova, G.G.Sukach, A.Yu.Palivets, A.N.Potorocha,
www.clinicaloncology.com.ua 1 Prognostic factors of appearing micrometastases in sentinel lymph nodes in skin melanoma M.N.Kukushkina, S.I.Korovin, O.I.Solodyannikova, G.G.Sukach, A.Yu.Palivets, A.N.Potorocha,
Sentinel Lymph Node Biopsy Is Valuable For All Cancer. Surgery Grand Rounds Debate October 6, 2008 Joel Baumgartner
 Sentinel Lymph Node Biopsy Is Valuable For All Cancer Surgery Grand Rounds Debate October 6, 2008 Joel Baumgartner History Lymphatics first described by Rasmus Bartholin in 1653 Rudolf Virchow postulated
Sentinel Lymph Node Biopsy Is Valuable For All Cancer Surgery Grand Rounds Debate October 6, 2008 Joel Baumgartner History Lymphatics first described by Rasmus Bartholin in 1653 Rudolf Virchow postulated
Surgical Oncology Perspective of Melanoma
 Surgical Oncology Perspective of Melanoma Hans F. Schoellhammer, MD, FACS Assistant Clinical Professor Division of Surgical Oncology September 20, 2018 Nothing to disclose DISCLOSURE Discussion Objectives
Surgical Oncology Perspective of Melanoma Hans F. Schoellhammer, MD, FACS Assistant Clinical Professor Division of Surgical Oncology September 20, 2018 Nothing to disclose DISCLOSURE Discussion Objectives
ORIGINAL ARTICLE MELANOMAS. Ann Surg Oncol (2015) 22: DOI /s z
 22: DOI /s z") Ann Surg Oncol (2015) 22:2972 2977 DOI 10.1245/s10434-015-4615-z ORIGINAL ARTICLE MELANOMAS Detailed Pathological Examination of Completion Node Dissection Specimens and Outcome in Melanoma Patients with
Ann Surg Oncol (2015) 22:2972 2977 DOI 10.1245/s10434-015-4615-z ORIGINAL ARTICLE MELANOMAS Detailed Pathological Examination of Completion Node Dissection Specimens and Outcome in Melanoma Patients with
Michael T. Tetzlaff MD, PhD
 American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
Sentinel Lymph Node Biopsy: Past and Present Implications for the Management of Cutaneous Melanoma with Nodal Metastasis
 American Journal of Clinical Dermatology (2018) 19 (Suppl 1):S24 S30 https://doi.org/10.1007/s40257-018-0379-0 REVIEW ARTICLE Sentinel Lymph Node Biopsy: Past and Present Implications for the Management
American Journal of Clinical Dermatology (2018) 19 (Suppl 1):S24 S30 https://doi.org/10.1007/s40257-018-0379-0 REVIEW ARTICLE Sentinel Lymph Node Biopsy: Past and Present Implications for the Management
Prognosis of Sentinel Node Staged Patients with Primary Cutaneous Melanoma
 Prognosis of Sentinel Node Staged Patients with Primary Cutaneous Melanoma Otmar Elsaeßer 1., Ulrike Leiter 1 *., Petra G. Buettner 2, Thomas K. Eigentler 1, Friedegund Meier 1, Benjamin Weide 1, Gisela
Prognosis of Sentinel Node Staged Patients with Primary Cutaneous Melanoma Otmar Elsaeßer 1., Ulrike Leiter 1 *., Petra G. Buettner 2, Thomas K. Eigentler 1, Friedegund Meier 1, Benjamin Weide 1, Gisela
Clinical Pathological Conference. Malignant Melanoma of the Vulva
 Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases
 Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases Faruk Tas, Sidika Kurul, Hakan Camlica and Erkan Topuz Institute of Oncology, Istanbul University, Istanbul, Turkey Received
Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases Faruk Tas, Sidika Kurul, Hakan Camlica and Erkan Topuz Institute of Oncology, Istanbul University, Istanbul, Turkey Received
Therapeutic Lymph Node Dissection in Melanoma: Different Prognosis for Different Macrometastasis Sites?
 Ann Surg Oncol (01) 19:91 91 DOI.14/s44-01-401- ORIGINAL ARTICLE MELANOMAS Therapeutic Lymph Node Dissection in Melanoma: Different Prognosis for Different Macrometastasis Sites? K. P. Wevers, MD, E. Bastiaannet,
Ann Surg Oncol (01) 19:91 91 DOI.14/s44-01-401- ORIGINAL ARTICLE MELANOMAS Therapeutic Lymph Node Dissection in Melanoma: Different Prognosis for Different Macrometastasis Sites? K. P. Wevers, MD, E. Bastiaannet,
ORIGINAL ARTICLE. Clinical Node-Negative Thick Melanoma
 ORIGINAL ARTICLE Clinical Node-Negative Thick Melanoma George I. Salti, MD; Ashwin Kansagra, MD; Michael A. Warso, MD; Salve G. Ronan, MD ; Tapas K. Das Gupta, MD, PhD, DSc Background: Patients with T4
ORIGINAL ARTICLE Clinical Node-Negative Thick Melanoma George I. Salti, MD; Ashwin Kansagra, MD; Michael A. Warso, MD; Salve G. Ronan, MD ; Tapas K. Das Gupta, MD, PhD, DSc Background: Patients with T4
Surgery for Melanoma and What s on the Horizon
 and What s on the Horizon Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background/Overview 76,870 cases of melanoma estimated
and What s on the Horizon Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background/Overview 76,870 cases of melanoma estimated
When Do I Consider Myself Cured?
 The Melanoma Patient Symposium - Science to Survivorship When Do I Consider Myself Cured? 26 September 2009 Jeffrey E. Gershenwald, MD, FACS Professor of Surgery, Dept. of Surgical Oncology Professor,
The Melanoma Patient Symposium - Science to Survivorship When Do I Consider Myself Cured? 26 September 2009 Jeffrey E. Gershenwald, MD, FACS Professor of Surgery, Dept. of Surgical Oncology Professor,
Impact of Prognostic Factors
 Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer
 - Official Statement - Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer Sentinel lymph node (SLN) biopsy has replaced axillary lymph node dissection (ALND) for the
- Official Statement - Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer Sentinel lymph node (SLN) biopsy has replaced axillary lymph node dissection (ALND) for the
AJCC 8 Implementation January 1, 2018 Melanoma of the Skin. Suraj Venna
 AJCC 8 Implementation January 1, 2018 Melanoma of the Skin Suraj Venna Personalized Medicine AJCC 8 th Edition This Time It s Personal Traditional AJCC (TNM) population-based analyses of large databases
AJCC 8 Implementation January 1, 2018 Melanoma of the Skin Suraj Venna Personalized Medicine AJCC 8 th Edition This Time It s Personal Traditional AJCC (TNM) population-based analyses of large databases
Increasing Age Is Associated with Worse Prognostic Factors and Increased Distant Recurrences despite Fewer Sentinel Lymph Node Positives in Melanoma
 Increasing Age Is Associated with Worse Prognostic Factors and Increased Distant Recurrences despite Fewer Sentinel Lymph Node Positives in Melanoma A. J. Page, Emory University A. Li, Emory University
Increasing Age Is Associated with Worse Prognostic Factors and Increased Distant Recurrences despite Fewer Sentinel Lymph Node Positives in Melanoma A. J. Page, Emory University A. Li, Emory University
Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients
 2018 AAD Annual Meeting, San Diego, CA Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients Susan M. Swetter, MD, FAAD Professor of Dermatology Director, Pigmented Lesion
2018 AAD Annual Meeting, San Diego, CA Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients Susan M. Swetter, MD, FAAD Professor of Dermatology Director, Pigmented Lesion
University of Groningen
 University of Groningen Nodular Histologic Subtype and Ulceration are Tumor Factors Associated with High Risk of Recurrence in Sentinel Node-Negative Melanoma Patients Faut, Marloes; Wevers, Kevin; van
University of Groningen Nodular Histologic Subtype and Ulceration are Tumor Factors Associated with High Risk of Recurrence in Sentinel Node-Negative Melanoma Patients Faut, Marloes; Wevers, Kevin; van
Clinical Case Conference Melanoma
 Clinical Case Conference Melanoma Epidemiology ~60,000 cases and 8,000 deaths per year in US Caucasian:African American = 10:1 15% arise from existing nevi 91% are cutaneous 15% are LN+ at presentation
Clinical Case Conference Melanoma Epidemiology ~60,000 cases and 8,000 deaths per year in US Caucasian:African American = 10:1 15% arise from existing nevi 91% are cutaneous 15% are LN+ at presentation
An estimated 76,690 patients will be diagnosed with invasive
 SONDAK ET AL Evidence-Based Clinical Practice Guidelines on the Use of Sentinel Lymph Node Biopsy in Melanoma Vernon K. Sondak, MD, Sandra L. Wong, MD, Jeffrey E. Gershenwald, MD, and John F. Thompson,
SONDAK ET AL Evidence-Based Clinical Practice Guidelines on the Use of Sentinel Lymph Node Biopsy in Melanoma Vernon K. Sondak, MD, Sandra L. Wong, MD, Jeffrey E. Gershenwald, MD, and John F. Thompson,
Epithelial Cancer- NMSC & Melanoma
 Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
ABSTRACT. Background Sentinel-node biopsy, a minimally invasive procedure for regional melanoma staging, was evaluated in a phase 3 trial.
 The new england journal of medicine established in 1812 february 13, 214 vol. 37 no. 7 Final Trial Report of Sentinel-Node Biopsy versus Nodal Observation in Melanoma D.L. Morton, J.F. Thompson, A.J. Cochran,
The new england journal of medicine established in 1812 february 13, 214 vol. 37 no. 7 Final Trial Report of Sentinel-Node Biopsy versus Nodal Observation in Melanoma D.L. Morton, J.F. Thompson, A.J. Cochran,
Sentinel Lymph Node Biopsy for Melanoma: Indications and Rationale
 Sentinel lymph node biopsy is recommended for most patients with melanomas 0.76 mm and for all good surgical candidates with melanomas 1.0 mm. Catherine Hickson. Figs in Alizarin Crimson. Oil on Belgian
Sentinel lymph node biopsy is recommended for most patients with melanomas 0.76 mm and for all good surgical candidates with melanomas 1.0 mm. Catherine Hickson. Figs in Alizarin Crimson. Oil on Belgian
Long-Term Survival Analysis and Clinical Follow-Up in Acral Lentiginous Malignant Melanoma Undergoing Sentinel Lymph Node Biopsy in Korean Patients
 Ann Dermatol Vol. 26, No. 2, 2014 http://dx.doi.org/10.5021/ad.2014.26.2.177 ORIGINAL ARTICLE Long-Term Survival Analysis and Clinical Follow-Up in Acral Lentiginous Malignant Melanoma Undergoing Sentinel
Ann Dermatol Vol. 26, No. 2, 2014 http://dx.doi.org/10.5021/ad.2014.26.2.177 ORIGINAL ARTICLE Long-Term Survival Analysis and Clinical Follow-Up in Acral Lentiginous Malignant Melanoma Undergoing Sentinel
Is There a Benefit to Sentinel Lymph Node Biopsy in Patients With T4 Melanoma?
 Is There a Benefit to Sentinel Lymph Node Biopsy in atients With T4 Melanoma? Csaba Gajdos, MD 1 ; Kent A. Griffith, MH, MS 2 ; Sandra L. Wong, MD 1 ; Timothy M. Johnson, MD 1,3 ; Alfred E. Chang, MD 1
Is There a Benefit to Sentinel Lymph Node Biopsy in atients With T4 Melanoma? Csaba Gajdos, MD 1 ; Kent A. Griffith, MH, MS 2 ; Sandra L. Wong, MD 1 ; Timothy M. Johnson, MD 1,3 ; Alfred E. Chang, MD 1
Clinical utilities and biological characteristics of melanoma sentinel lymph nodes
 W J C O World Journal of Clinical Oncology Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.5306/wjco.v7.i2.174 World J Clin Oncol 2016 April
W J C O World Journal of Clinical Oncology Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.5306/wjco.v7.i2.174 World J Clin Oncol 2016 April
Precision Surgery for Melanoma
 Precision Surgery for Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background 87,110 cases of melanoma estimated in
Precision Surgery for Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background 87,110 cases of melanoma estimated in
Research Article Prediction of Sentinel Node Status and Clinical Outcome in a Melanoma Centre
 Skin Cancer Volume 2013, Article ID 904701, 7 pages http://dx.doi.org/10.1155/2013/904701 Research Article Prediction of Sentinel Node Status and Clinical Outcome in a Melanoma Centre Vera Teixeira, 1
Skin Cancer Volume 2013, Article ID 904701, 7 pages http://dx.doi.org/10.1155/2013/904701 Research Article Prediction of Sentinel Node Status and Clinical Outcome in a Melanoma Centre Vera Teixeira, 1
MELANOMA LETTER. Surgical Treatment of Primary Melanoma: Where Do We Stand After MSLT-II? THE. From the Editors MSLT-II. SkinCancer.
 THE MELANOMA LETTER A PUBLICATION OF THE SKIN CANCER FOUNDATION DEBORAH S. SARNOFF, MD, President WINTER 2017, Vol. 35 DAN LATORE, Executive Director Surgical Treatment of Primary Melanoma: Where Do We
THE MELANOMA LETTER A PUBLICATION OF THE SKIN CANCER FOUNDATION DEBORAH S. SARNOFF, MD, President WINTER 2017, Vol. 35 DAN LATORE, Executive Director Surgical Treatment of Primary Melanoma: Where Do We
Inguinal or inguino-iliac/obturator lymph node dissection after positive inguinal sentinel lymph node in patients with cutaneous melanoma
 258 research article Inguinal or inguino-iliac/obturator lymph node dissection after positive inguinal sentinel lymph node in patients with cutaneous melanoma Nebojsa Glumac 1, Marko Hocevar 1, Vesna Zadnik
258 research article Inguinal or inguino-iliac/obturator lymph node dissection after positive inguinal sentinel lymph node in patients with cutaneous melanoma Nebojsa Glumac 1, Marko Hocevar 1, Vesna Zadnik
Thin Melanoma with Nodal Involvement: Analysis of Demographic, Pathologic, and Treatment Factors with Regard to Prognosis
 Ann Surg Oncol DOI 10.1245/s10434-016-5646-9 ORIGINAL ARTICLE MELANOMAS Thin Melanoma with Nodal Involvement: Analysis of Demographic, Pathologic, and Treatment Factors with Regard to Prognosis Giorgos
Ann Surg Oncol DOI 10.1245/s10434-016-5646-9 ORIGINAL ARTICLE MELANOMAS Thin Melanoma with Nodal Involvement: Analysis of Demographic, Pathologic, and Treatment Factors with Regard to Prognosis Giorgos
UvA-DARE (Digital Academic Repository) Who needs adjuvant therapy in stage III melanoma? Madu, M.F. Link to publication
 Who needs adjuvant therapy in stage III melanoma? Madu, M.F. Link to publication") UvA-DARE (Digital Academic Repository) Who needs adjuvant therapy in stage III melanoma? Madu, M.F. Link to publication Citation for published version (APA): Madu, M. F. (2018). Who needs adjuvant therapy
UvA-DARE (Digital Academic Repository) Who needs adjuvant therapy in stage III melanoma? Madu, M.F. Link to publication Citation for published version (APA): Madu, M. F. (2018). Who needs adjuvant therapy
Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact
 Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact Bjørn Hagen, MD, PhD St Olavs Hospital Trondheim University Hospital Trondheim, Norway Endometrial Cancer (EC) The most
Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact Bjørn Hagen, MD, PhD St Olavs Hospital Trondheim University Hospital Trondheim, Norway Endometrial Cancer (EC) The most
Abstract. Background We evaluated the contribution of sentinel-node biopsy to outcomes in patients with newly diagnosed melanoma.
 The new england journal of medicine established in 112 september 2, 6 vol. 355 no. 13 Sentinel-Node Biopsy or Nodal in Melanoma Donald L. Morton, M.D., John F. Thompson, M.D., Alistair J. Cochran, M.D.,
The new england journal of medicine established in 112 september 2, 6 vol. 355 no. 13 Sentinel-Node Biopsy or Nodal in Melanoma Donald L. Morton, M.D., John F. Thompson, M.D., Alistair J. Cochran, M.D.,
Melanoma of the Skin INTRODUCTION SUMMARY OF CHANGES
 24 Melanoma of the Skin C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of other and unspecified parts of face C44.4 Skin of scalp and neck C44.5 Skin of trunk C44.6 Skin of upper limb
24 Melanoma of the Skin C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of other and unspecified parts of face C44.4 Skin of scalp and neck C44.5 Skin of trunk C44.6 Skin of upper limb
Should we still be performing IHC on all sentinel nodes?
 Miami Breast Cancer Conference 31 st Annual Conference March 8, 2014 Should we still be performing IHC on all sentinel nodes? Donald L. Weaver, MD Professor of Pathology University of Vermont USA Miami
Miami Breast Cancer Conference 31 st Annual Conference March 8, 2014 Should we still be performing IHC on all sentinel nodes? Donald L. Weaver, MD Professor of Pathology University of Vermont USA Miami
Breast Surgery When Less is More and More is Less. E MacIntosh, MD June 6, 2015
 Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Melanoma of the Skin
 24 Melanoma of the Skin C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of other and unspecified parts of face C44.4 Skin of scalp and neck C44.5 Skin of trunk C44. Skin of upper limb
24 Melanoma of the Skin C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of other and unspecified parts of face C44.4 Skin of scalp and neck C44.5 Skin of trunk C44. Skin of upper limb
Quality ID #397: Melanoma Reporting National Quality Strategy Domain: Communication and Care Coordination
 Quality ID #397: Melanoma Reporting National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Outcome DESCRIPTION: Pathology
Quality ID #397: Melanoma Reporting National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Outcome DESCRIPTION: Pathology
Results, morbidity, and quality of life of melanoma patients undergoing sentinel lymph node staging Vries, Mattijs de
 University of Groningen Results, morbidity, and quality of life of melanoma patients undergoing sentinel lymph node staging Vries, Mattijs de IMPORTANT NOTE: You are advised to consult the publisher's
University of Groningen Results, morbidity, and quality of life of melanoma patients undergoing sentinel lymph node staging Vries, Mattijs de IMPORTANT NOTE: You are advised to consult the publisher's
Sentinel Lymph Node Biopsy for Head and Neck Cutaneous Melanoma
 Sentinel Lymph Node Biopsy for Head and Neck Cutaneous Melanoma S. Ross Patton, MD - PGY III Faculty Mentor: Susan McCammon, MD The University of Texas Medical Branch (UTMB Health) Department of Otolaryngology
Sentinel Lymph Node Biopsy for Head and Neck Cutaneous Melanoma S. Ross Patton, MD - PGY III Faculty Mentor: Susan McCammon, MD The University of Texas Medical Branch (UTMB Health) Department of Otolaryngology
47. Melanoma of the Skin
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Surgical Treatment of Melanoma Across the Disease Spectrum:
 AOCD Annual Fall Meeting October 28 th, 2017 New Orleans, Louisiana Surgical Treatment of Melanoma Across the Disease Spectrum: Standards of Care and Evolving Paradigms Merrick Ross, M.D. Professor of
AOCD Annual Fall Meeting October 28 th, 2017 New Orleans, Louisiana Surgical Treatment of Melanoma Across the Disease Spectrum: Standards of Care and Evolving Paradigms Merrick Ross, M.D. Professor of
Sentinel Lymph Node Biopsy for the T1 (Thin) Melanoma: Is It Necessary?
 Melanoma: Is It Necessary?") Sentinel Lymph Node Biopsy for the T1 (Thin) Melanoma: Is It Necessary? Maurice Y. Nahabedian, MD Anthony P. Tufaro, MD Paul N. Manson, MD The use of sentinel lymph node biopsy for the T1 melanoma is controversial.
Sentinel Lymph Node Biopsy for the T1 (Thin) Melanoma: Is It Necessary? Maurice Y. Nahabedian, MD Anthony P. Tufaro, MD Paul N. Manson, MD The use of sentinel lymph node biopsy for the T1 melanoma is controversial.
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology
 Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
PAPER. Is Completion Lymphadenectomy After a Positive Sentinel Lymph Node Biopsy for Cutaneous Melanoma Always Necessary?
 PAPER Is Completion Lymphadenectomy After a Positive Sentinel Lymph Node Biopsy for Cutaneous Melanoma Always Necessary? Nahel Elias, MD; Kenneth K. Tanabe, MD; Arthur J. Sober, MD; Michele A. Gadd, MD;
PAPER Is Completion Lymphadenectomy After a Positive Sentinel Lymph Node Biopsy for Cutaneous Melanoma Always Necessary? Nahel Elias, MD; Kenneth K. Tanabe, MD; Arthur J. Sober, MD; Michele A. Gadd, MD;
Citation for published version (APA): Francken, A. B. (2007). Primary and metastatic melanoma: aspects of follow-up and staging s.n.
: Francken, A. B. (2007). Primary and metastatic melanoma: aspects of follow-up and staging s.n.") University of Groningen Primary and metastatic melanoma Francken, Anne Brecht IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check
University of Groningen Primary and metastatic melanoma Francken, Anne Brecht IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check
Kentaro Tanaka, 1 Hiroki Mori, 1 Mutsumi Okazaki, 1 Aya Nishizawa, 2 and Hiroo Yokozeki Introduction. 2. Case Presentation
 Case Reports in Oncological Medicine Volume 2013, Article ID 259326, 4 pages http://dx.doi.org/10.1155/2013/259326 Case Report Long-Term Treatment Outcome after Only Popliteal Lymph Node Dissection for
Case Reports in Oncological Medicine Volume 2013, Article ID 259326, 4 pages http://dx.doi.org/10.1155/2013/259326 Case Report Long-Term Treatment Outcome after Only Popliteal Lymph Node Dissection for
PAPER. Importance of Sentinel Lymph Node Biopsy in Patients With Thin Melanoma
 PAPER Importance of Sentinel Lymph Node Biopsy in Patients With Thin Melanoma Byron E. Wright, MD; Randall P. Scheri, MD; Xing Ye, MS; Mark B. Faries, MD; Roderick R. Turner, MD; Richard Essner, MD; Donald
PAPER Importance of Sentinel Lymph Node Biopsy in Patients With Thin Melanoma Byron E. Wright, MD; Randall P. Scheri, MD; Xing Ye, MS; Mark B. Faries, MD; Roderick R. Turner, MD; Richard Essner, MD; Donald
Nodal staging in localized melanoma. The experience of the Brescia Melanoma Unit
 The British Association of Plastic Surgeons (2003) 56, 534 539 Nodal staging in localized melanoma. The experience of the Brescia Melanoma Unit Giorgio Manca a, *, Fabio Facchetti b, Claudio Pizzocaro
The British Association of Plastic Surgeons (2003) 56, 534 539 Nodal staging in localized melanoma. The experience of the Brescia Melanoma Unit Giorgio Manca a, *, Fabio Facchetti b, Claudio Pizzocaro
Primary Cutaneous Melanoma Pathology Reporting Proforma DD MM YYYY. *Tumour site. *Specimen laterality. *Specimen type
 Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Therapeutic Surgical Management of Palpable Melanoma Groin Metastases: Superficial or Combined Superficial and Deep Groin Lymph Node Dissection
 Ann Surg Oncol () : DOI.45/s44--74- ORIGINAL ARTICLE MELANOMAS Therapeutic Surgical Management of Palpable Melanoma Groin Metastases: Superficial or Combined Superficial and Deep Groin Lymph Node Dissection
Ann Surg Oncol () : DOI.45/s44--74- ORIGINAL ARTICLE MELANOMAS Therapeutic Surgical Management of Palpable Melanoma Groin Metastases: Superficial or Combined Superficial and Deep Groin Lymph Node Dissection
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma. Michael T. Tetzlaff MD, PhD
 Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
WHAT DOES THE PATHOLOGY REPORT MEAN?
 Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Melanoma: Therapeutic Progress and the Improvements Continue
 Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
SLN Mapping in Cervical Cancer. Memorial Sloan Kettering Cancer Center New York, USA
 Lead Grou p Log SLN Mapping in Cervical Cancer Nadeem R. Abu-Rustum, M.D. Memorial Sloan Kettering Cancer Center New York, USA Conflict of Interest Disclosure Nadeem R. Abu-Rustum, M.D. I have no financial
Lead Grou p Log SLN Mapping in Cervical Cancer Nadeem R. Abu-Rustum, M.D. Memorial Sloan Kettering Cancer Center New York, USA Conflict of Interest Disclosure Nadeem R. Abu-Rustum, M.D. I have no financial
Results of the ACOSOG Z0011 Trial
 DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
Sentinel Lymph Node Biopsy for Breast Cancer
 Sentinel Lymph Node Biopsy for Breast Cancer Registrar Tutorial Adam Cichowitz Surgical Registrar The Royal Melbourne Hospital Sentinel Lymph Node Biopsy Axillary LN status important prognostic factor
Sentinel Lymph Node Biopsy for Breast Cancer Registrar Tutorial Adam Cichowitz Surgical Registrar The Royal Melbourne Hospital Sentinel Lymph Node Biopsy Axillary LN status important prognostic factor
Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy
 Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy Rebecca Warburton MD Department of Surgery, University of British Columbia Mount Saint Joseph Hospital, Providence Health Care
Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy Rebecca Warburton MD Department of Surgery, University of British Columbia Mount Saint Joseph Hospital, Providence Health Care
Chapter 2 Staging of Breast Cancer
 Chapter 2 Staging of Breast Cancer Zeynep Ozsaran and Senem Demirci Alanyalı 2.1 Introduction Five decades ago, Denoix et al. proposed classification system (tumor node metastasis [TNM]) based on the dissemination
Chapter 2 Staging of Breast Cancer Zeynep Ozsaran and Senem Demirci Alanyalı 2.1 Introduction Five decades ago, Denoix et al. proposed classification system (tumor node metastasis [TNM]) based on the dissemination
> 6000 Mutations in Melanoma. Tests That Cay Be Employed. FISH for Additions/Deletions. Comparative Genomic Hybridization
 Winter Clinical 2017: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of Colorado
Winter Clinical 2017: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of Colorado
Printed by Martina Huckova on 10/3/2011 3:04:54 PM. For personal use only. Not approved for distribution. Copyright 2011 National Comprehensive
 Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD
 Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
J Clin Oncol 27: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 27 NUMBER 36 DECEMBER 2 29 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T From Johns Hopkins Medical Institutions, Baltimore, MD; The University of Texas M. D. Anderson Cancer Center,
VOLUME 27 NUMBER 36 DECEMBER 2 29 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T From Johns Hopkins Medical Institutions, Baltimore, MD; The University of Texas M. D. Anderson Cancer Center,
Updates on management of the axilla in breast cancer the surgical point of view
 Updates on management of the axilla in breast cancer the surgical point of view Edwige Bourstyn Centre des maladies du sein Hôpital Saint Louis Paris Sentinel lymph node biopsy (SLNB) is the standard of
Updates on management of the axilla in breast cancer the surgical point of view Edwige Bourstyn Centre des maladies du sein Hôpital Saint Louis Paris Sentinel lymph node biopsy (SLNB) is the standard of
Measure #397: Melanoma Reporting National Quality Strategy Domain: Communication and Care Coordination
 Measure #397: Melanoma Reporting National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION: Pathology reports
Measure #397: Melanoma Reporting National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION: Pathology reports
Prognostic Variables and Surgical Management of Foot Melanoma: Review of a 25-Year Institutional Experience
 Virginia Commonwealth University VCU Scholars Compass Surgery Publications Dept. of Surgery 11 Prognostic Variables and Surgical Management of Foot Melanoma: Review of a 5-Year Institutional Experience
Virginia Commonwealth University VCU Scholars Compass Surgery Publications Dept. of Surgery 11 Prognostic Variables and Surgical Management of Foot Melanoma: Review of a 5-Year Institutional Experience
How can we reduce the mortality from melanoma in Australia?
 How can we reduce the mortality from melanoma in Australia? Professor Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia University of Melbourne, Parkville, Australia What is melanoma?
How can we reduce the mortality from melanoma in Australia? Professor Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia University of Melbourne, Parkville, Australia What is melanoma?
Debate Axillary dissection - con. Prof. Dr. Rodica Anghel Institute of Oncology Bucharest
 Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,