ADVANCES IN COLORECTAL CANCERS IS THERE HOPE? Dr Lim Hwee Yong Medical Oncologist
|
|
|
- Jerome Hardy
- 5 years ago
- Views:
Transcription

1 ADVANCES IN COLORECTAL CANCERS IS THERE HOPE? Dr Lim Hwee Yong Medical Oncologist
2 CRC: Epidemiology in 2012 Third most common cancer diagnosis in US [1] Estimated 143,460 new cases in 2012; 1:1 male:female ratio [2] At diagnosis, 39% localized (stage 0-II), 37% regional (stage III), 20% metastatic (stage IV) [3] Steady decrease in ageadjusted incidence rates of distal colon, proximal colon, and rectal cancers in [4] Third leading cause of cancer deaths in 2011 (estimated 49,380 deaths) [1] Race/Ethnicity Death Rates in 2008, per 100,000 [3] All races 16.4 White 15.8 African American 23.0 Asian/Pacific Islander 11.5 American Indian/ Alaska Native 19.1 Hispanic American Cancer Society. Colorectal cancer facts & figures Siegel R, et al. CA Cancer J Clin. 2012;62: SEER. Stat fact sheets: colon and rectum. 4. Cheng L, et al. Am Clin Oncol. 2011;34:
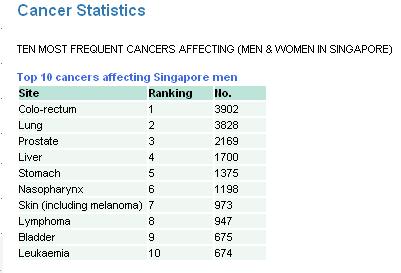
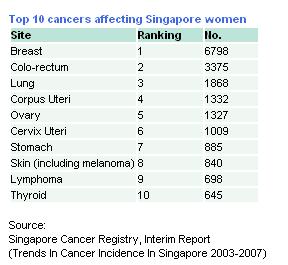
3 Introduction Colorectal cancer is the most common cancer in Singapore According to the 5yearly report ( ) from the Singapore Cancer Registry, it has the highest incidence amongst malignancies in male & is second only to breast cancer in female
4 Introduction 4

5 Introduction 5
6 Introduction 6
7 Major Risk Factors for CRC Factors That Increase Risk Heredity and Medical History Family history 1 first-degree relative More than 1 relative Relative with diagnosis before 45 yrs of age Inflammatory bowel disease Crohn s disease Ulcerative colitis (colon) * Relative risk compares risk of disease in people with exposure to risk of people without exposure. American Cancer Society. Colorectal cancer facts & figures Relative Risk* Diabetes 1.2 Smoking 1.2 Factors that decrease risk are physical activity (in colon cancer), calcium, and consumption of milk
8 Impact of Personal and Family History in CRC 20% of patients with CRC have close relative with CRC 5% of CRC cases are associated with genetic syndrome Lynch syndrome (HNPCC) most common, accounting for 2% to 4% of all cases Higher risk of other cancers (eg, endometrial, ovarian, pancreatic) Familial adenomatous polyposis, second most common and associated with nearly 100% lifetime risk of CRC without intervention BRCA associated with increased risk of CRC Previous history of localized CRC associated with increased risk of new CRC tumors American Cancer Society. Colorectal cancer facts & figures
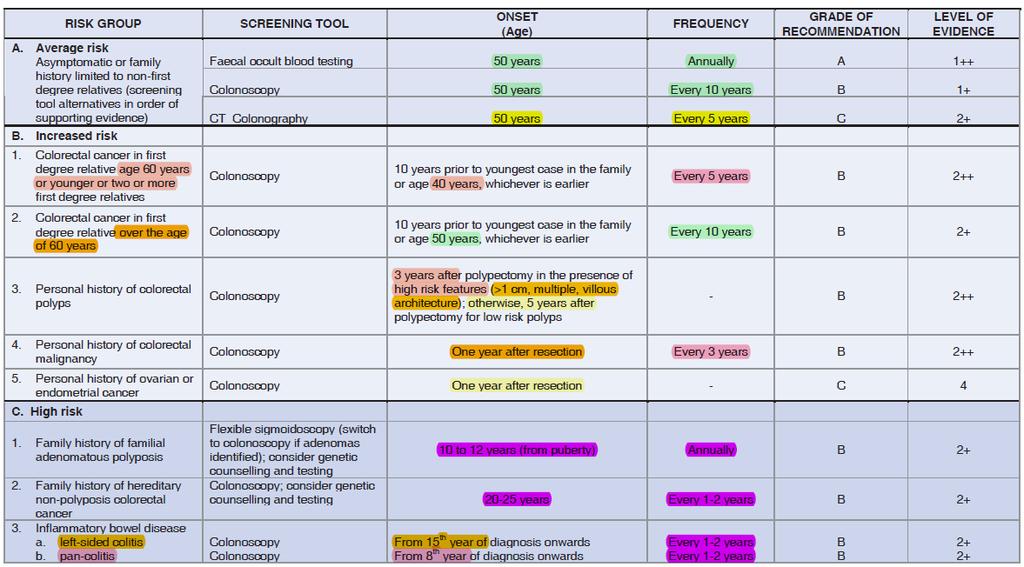
9 Screening
10 Young Colorectal CA
11 FAP AD. Germline mutation of tumour suppressor gene APC in short arm of chromosome 5 1% of all CRCs; Prevalence 1: and penetrance is 100% Characterized by multiple polyps(> 100, less in AAPC) appearing during childhood, symptomatic by 16 yrs. 90% devt Ca at 45 years. Variants include Turcot s (AR), Gardner s (AD) and attenuated adenomatous polyposis coli (AAPC) Some patients have congenital hypertrophy of the retinal pigment epithelium (CHRPE), the presence of which may provide a clue toward the diagnosis In addition to colorectal adenocarcinoma, patients with FAP are at risk for several extracolonic malignancies including: Duodenal ampullary carcinoma, Follicular or papillary thyroid cancer, Childhood hepatoblastoma,gastric carcinoma, CNS tumors (mostly medulloblastomas) Genetic testing: should be done on a known affected family member first to determine if there is a detectable mutation
12 Screening/ Mx in FAP Families FAP index pt APC mutation +ve APC testing in relatives +ve -ve Prophylactic total colectomy (10-19yo) No surg/ surveillance needed APC mutation -ve No need for APC testing in relatives Annual colonoscopic surveillance If polyps +ve, total colectomy
13 HNPCC AD. 1-5% of all CRCs. Gene mutation affecting DNA mismatch repair, commonly hmsh2 and hmlh1 (95% of HNPCC) confers at least a 25% risk of developing colorectal cancer by age 50 and a 70% to 80% risk by age 70 Amsterdam Criteria: a) >/=3 relatives with colorectal cancer (1 of whom is the first-degree relative of the other 2) b) >/ 2 generations affected c) >/ 1 of those affected diagnosed at age <50 Colonoscopic surveillance biannually from 20yo (or 5yr earlier than the youngest case of CRC in family), annually from 40yo
14 Primary tumor (T)* Tis T1 T2 T3 T4 Carcinoma in situ; intraepithelial (within glandular basement membrane) or invasion of lamina propria (intramucosal) Tumor invades submucosa Tumor invades muscularis propria Tumor invades through the muscularis propria into the subserosa, or into non-peritonealized pericolic or perirectal tissues Tumor directly invades other organs or structures, and/or perforates visceral peritoneum Regional lymph node (N) NX Regional nodes cannot be assessed N0 No regional nodal metastases N1 Metastasis in 1 to 3 regional lymph nodes N2 Metastasis in 4 or more regional lymph nodes Distant metastasis (M) MX Distant metastasis cannot be assessed M0 No distant metastasis M1 Distant metastasis Stage Groupings Stage 0 Tis N0 M0 Stage I T1-2 N0 M0 Stage IIA T3 N0 M0 Stage IIB T4 N0 M0 Stage IIIA T1-2 N1 M0 Stage IIIB T3-4 N1 M0 Stage IIIC Any T N2 M0 Stage IV Any T Any N M1
15 TNM staging Dukes staging NEED >= 12 LYMPH NODES
16 Survival SEER Stage 5 year survival I 93% II A B 85% 72% III A 83% B 64% C 44% IV 8%
17 Adjuvant Treatment FU/LEV 5FU/LV 5FU/LV = 5FU/LEV 6 mos = 12 mos HDLV = LDLV Weekly = Monthly Oral 5FU = BIV 5FU CIV 5FU = BIV 5FU FOLFOX > 5FU/LV Bevacizumab not useful in adj Rx Cetuximab not useful in adj Rx
18 Adjuvant Treatment To remember 5FU Capecitabine (Oral 5FU prodrug) Combination with Oxaliplatin Stage III High risk Stage II T4, perforation, obstruction, perineural invasion, lymphovascular invasion Inadequate Lymph nodes sampling, poorly differentiated histology
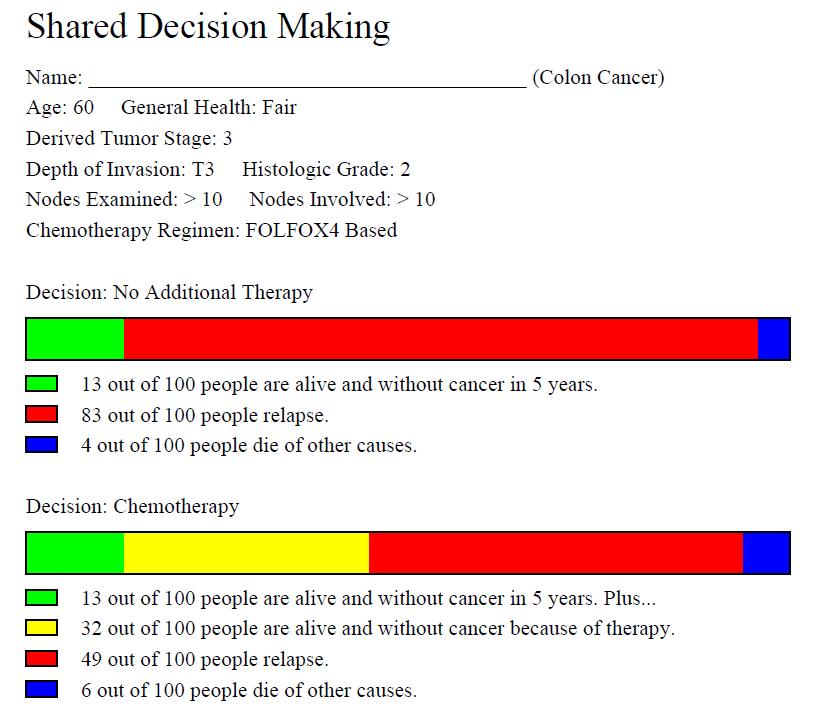
19 ADJUVANT CHEMOTHERAPY Adjuvant online
20
21 Rectal cancer
22 Epidemiology 2008: 40,740 new cases (23,490 men; 17,250 women) Lumped with colon cancer as the 3 rd most common cancer in the US (112,340 new cases in US in 2007)
23 PRE-OP STAGING EUS v. MRI Both are 94% sensitive to determine invasion into muscularis Specificity: EUS 86%, MRI 69% Considered equal for evaluating lymph nodes, but understages 1/5 of patients Mercury trial - Radiology Apr;243(1): Epub 2007 Feb % CI to +/- 0.5mm
24 DEFINING THE RECTUM
25 WHY IS THE RECTUM SO SPECIAL? Sphinter: Preservation = QOL Close proximity to other organs (hard to get wide margins = higher local relapse) absence of serosa fixed in space
26 Rectal cancer Different surgical approach APR, LAR Total Mesorectal resection Chemo-radiation therapy (usually neoadjuvant) T3, T4, node positive.
27 METASTATIC DISEASES

28 HOW CANCER GROWS

29 Paradigm Shift Breakthroughs in molecular biology Identification of distinctive molecular signatures Allows targeting of these molecular signatures Era of rational therapy (as opposed to empiric)

30 Systemic anti-cancer therapy Cytotoxic therapy, e.g. 5 Fluorouriacil, Oxaliplatin Hormonal therapy, e.g. tamoxifen Immunological therapy, e.g. interferon Targeted therapy, e.g. imatinib (Glivec)
31 Treatment approach Liver only/ Lung only Resectable Neoadjuvant with Cytotoxic chemorx + Biologics Surgery Adjuvant ChemoRx * M 1 Abdominal/ peritoneal disease/ Multifocal disease/ Not resectable Unresectable Palliative ChemoRx Surgery Chemotherapy adjuvant intent
32 Treatment - Metastatic Metastatectomy? Isolated mets? Curable? Neoadjuvant chemotx? 5FU/LV Oxaliplatin Irinotecan Cetuximab Panitumumab Bevacizumab Aflibercept? (VEGF trap)

33 TARGETED THERAPY
34

35 Monoclonal antibodies (MABs)


36 Tyrosine kinase inhibitors (TKIs)
 Cetuximab (EGFR)")
 Gefitinib (EGFR) Lapatinib")
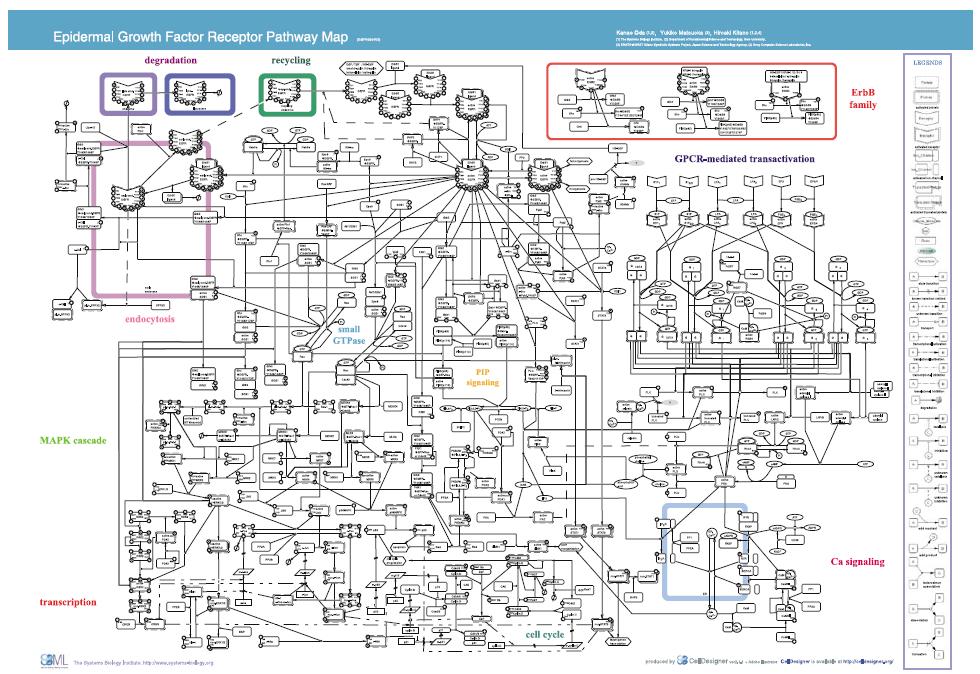
37 EGFR-mediated pathway MABs Trastuzumab (HER2) Cetuximab (EGFR) Panitumumab (EGFR) TKIs Erlotinib (EGFR) Gefitinib (EGFR) Lapatinib (EGFR/HER2)

38 CETUXIMAB-INDUCED SKIN RASH Acneiform rashes
 Multitargeted TKIs Sunitinib")
")
39 VEGFR-mediated pathways MAB Bevacizumab (VEGF) Multitargeted TKIs Sunitinib (PDGF, C- KIT, FLT3, VEGFR) Sorafinib (PDGF, C- KIT, FLT3, VEGFR, RAF) Thalidomide
40 Considerations Quality-Adjusted Time Without Symptoms or Toxicity (Q-TWiST) Functional status ECOG or KPS
41 Treatment Stage I: Resection. (T1-2, N0, M0) Stage II: Resection. Consider adjuvant chemotherapy? (T3-4, N0, M0) Stage III: Surgery plus adjuvant chemotherapy. (any T, N1-2, M0) Stage IV: Chemotherapy. Surgery in selected cases (Any T, any N, M1)
42 Surveillance Hx/ PE every 3m for 2y; then every 6m for total 5y CEA every 3m for 2y; then every 6m for total 5y (for T2 or greater) CT T/A/P yearly for up to 5y for pt at high risk of recurrence For M1 disease: CT every 3-6m x 2y, then every 6-12m for total 5y Colonoscopy in 1y ; if abnormal, repeat in 1y, if advanced adenoma repeat in 3y and if normal, repeat in 5y
43 Questions 45 yo man is brought from his job on a constuction site to the emergency department with acute right sided abdominal pain, nausea and vomiting. CT scans shows inflamed area in the right lower abdominal quadrant. Intraoperatively, he is found to have an obstructing lesion in the cecum. Frozen section confirms high garde adenocarcinoma and right hemi-colectomy and lymph node dissection are done. Biopsy specimens confirms Stage III T3 N2 colon cancer with 5 of lymph nodes positive for metastatic disease. Post operative CT scans of Thorax, Abdomen and Pelvis and complete colonoscopy show no synchronous lesions or distant metastases.
44 Questions Which of the following is the most appropriate post operative management A) Chemotherapy B) Chemotherapy and radiation therapy C) Radiation therapy D) Observation
45 Questions If the patient has node negative disease and the final staging is T3 N0 M0 disease, Which of the following is the most appropriate post operative management A) Chemotherapy B) Chemotherapy and radiation therapy C) Radiation therapy D) Observation
46 Questions A 56 year old woman undergoes initial screening colonoscopy. An abnormality is found 10 cm from the anal verge. Biopsy specimens confirm the diagnosis of a moderately differentiated adenocarcinoma. MRI pelvis shows that the tumor has extended into the perirectal fat, but no lymphadenopathy is noted. Chest radiograph and CT scans of the Thorax, Abdomen shows no metastatic disease.
47 Questions Which of the following is the most appropriate treatment at this time: A) Neo-adjuvant Chemoradiation followed by surgical resection B) Surgery and followed by adjuvant chemotherapy C) Radiation therapy alone D) Chemotherapy alone E) Surgical resection postoperative radiation alone

48 Thank You
Gastric and Colon Cancer. Dr. Andres Wiernik 2017
 Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
Navigators Lead the Way
 RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
By: Tania Cortas, MD Arizona Oncology 03/10/2015
 By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
2014/2015 FCDS Educational Webcast Series
 2014/2015 FCDS Educational Webcast Series February 19, 2015 Steven Peace, CTR 2015 Update; Background, Anatomy, Risk Factors, Screening Guidelines, MPH Rules Review AJCC TNM 7 th ed, SS2000, CSv02.05 and
2014/2015 FCDS Educational Webcast Series February 19, 2015 Steven Peace, CTR 2015 Update; Background, Anatomy, Risk Factors, Screening Guidelines, MPH Rules Review AJCC TNM 7 th ed, SS2000, CSv02.05 and
Clinical Colon Cancer Abby Siegel MD COLON CANCER. 1. Epidemiology 2. Risk factors 3. Manifestations 4. Treatment
 Clinical Colon Cancer 2008 Abby Siegel MD COLON CANCER 1. Epidemiology 2. Risk factors 3. Manifestations 4. Treatment 1 1. EPIDEMIOLOGY - Colorectal cancer is the third most common cancer in the United
Clinical Colon Cancer 2008 Abby Siegel MD COLON CANCER 1. Epidemiology 2. Risk factors 3. Manifestations 4. Treatment 1 1. EPIDEMIOLOGY - Colorectal cancer is the third most common cancer in the United
COLORECTAL CANCER CASES
 COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
Disclosures. Colorectal Cancer Update GAFP November Risk Assessment. Colon and Rectal Cancer The Challenge. Issues in Colon and Rectal Cancer
 Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
David P. Ryan, M.D. Clinical Director, MGH Cancer Center Chief, Hematology-Oncology, MGH
 Colon Cancer 2015 David P. Ryan, M.D. Clinical Director, MGH Cancer Center Chief, Hematology-Oncology, MGH Colon Cancer Case presentation 72yo woman presented 1/03 abd discomfort and nausea Found to have
Colon Cancer 2015 David P. Ryan, M.D. Clinical Director, MGH Cancer Center Chief, Hematology-Oncology, MGH Colon Cancer Case presentation 72yo woman presented 1/03 abd discomfort and nausea Found to have
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE
 COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
A Brief Overview of Screening and Management of Colorectal Cancer
 A Brief Overview of Screening and Management of Colorectal Cancer Gentry King MD Assistant Professor Hematology and Medical Oncology University of Colorado Disclosures Nothing to disclose Objectives Review
A Brief Overview of Screening and Management of Colorectal Cancer Gentry King MD Assistant Professor Hematology and Medical Oncology University of Colorado Disclosures Nothing to disclose Objectives Review
Quiz. b. 4 High grade c. 9 Unknown
 Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
EARLY DETECTION OF COLORECTAL CANCER. Epidemiology of CRC
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
CHEMOTHERAPY FOR COLON CANCER OUTLINE OF TODAY S TALK. Colon Cancer Epidemiology 11/6/2012 GATRA/GCCR FALL CONFERENCE NOVEMBER 14 16, 2012
 CHEMOTHERAPY FOR COLON CANCER JONATHAN C. BENDER,MD MEDICAL DIRECTOR OF PIEDMONT FAYETTE CANCER CENTER OUTLINE OF TODAY S TALK 1. Overview of Colon Cancer in the US 2. Colon Cancer staging and risks of
CHEMOTHERAPY FOR COLON CANCER JONATHAN C. BENDER,MD MEDICAL DIRECTOR OF PIEDMONT FAYETTE CANCER CENTER OUTLINE OF TODAY S TALK 1. Overview of Colon Cancer in the US 2. Colon Cancer staging and risks of
THE CROSSROADS: Drug Development, Biomarkers, and Colorectal Cancer
 THE CROSSROADS: Drug Development, Biomarkers, and Colorectal Cancer SANJAY GOEL, M.D., M.S. PROFESSOR OF MEDICINE ALBERT EINSTEIN COLLEGE OF MEDICINE MONTEFIORE MEDICAL CENTER DEPT. OF ONCOLOGY JUN 22,
THE CROSSROADS: Drug Development, Biomarkers, and Colorectal Cancer SANJAY GOEL, M.D., M.S. PROFESSOR OF MEDICINE ALBERT EINSTEIN COLLEGE OF MEDICINE MONTEFIORE MEDICAL CENTER DEPT. OF ONCOLOGY JUN 22,
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Colon, or Colorectal, Cancer Information
 Colon, or Colorectal, Cancer Information Definition Colon, or colorectal, cancer is cancer that starts in the large intestine (colon) or the rectum (end of the colon). Other types of cancer can affect
Colon, or Colorectal, Cancer Information Definition Colon, or colorectal, cancer is cancer that starts in the large intestine (colon) or the rectum (end of the colon). Other types of cancer can affect
Alison Douglass Gillian Lieberman, MD. November. Colon Cancer. Alison Douglass, Harvard Medical School Year III Gillian Lieberman, MD
 November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
A superficial radiotherapy B single pass curettage C excision with 2 mm margins D excision with 5 mm margins E Mohs micrographic surgery.
 1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
Locally Advanced Colon Cancer. Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery
 Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION
 CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
For identification, support and follow up related to Familial Gastrointestinal Cancer conditions. South Island Cancer Nurses Network September 2013
 For identification, support and follow up related to Familial Gastrointestinal Cancer conditions South Island Cancer Nurses Network September 2013 Who are we? Specialist multidisciplinary team: Nurse coordinators,
For identification, support and follow up related to Familial Gastrointestinal Cancer conditions South Island Cancer Nurses Network September 2013 Who are we? Specialist multidisciplinary team: Nurse coordinators,
COME HOME Innovative Oncology Business Solutions, Inc.
 COME HOME Rectal Cancer Pathway V8, April 2015 Diagnostic Workup: Bethesda Criteria: Pathology Review All patients H&P All patients Biopsy All patients Colonoscopy All patients CEA All Patients Chest/Abdominal/Pelvic
COME HOME Rectal Cancer Pathway V8, April 2015 Diagnostic Workup: Bethesda Criteria: Pathology Review All patients H&P All patients Biopsy All patients Colonoscopy All patients CEA All Patients Chest/Abdominal/Pelvic
Colorectal Cancer Treatment
 Colorectal Cancer Treatment Syed Husain, MD, FACS, FASCRS Assistant Professor of Surgery Department of Surgery Division of Colon and Rectal Surgery The Ohio State University Wexner Medical Center Introduction
Colorectal Cancer Treatment Syed Husain, MD, FACS, FASCRS Assistant Professor of Surgery Department of Surgery Division of Colon and Rectal Surgery The Ohio State University Wexner Medical Center Introduction
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Preoperative Data Colorectal Cancer Database
 Preoperative Data Please place patient label here Patient Information Patient s Last Name First Middle Initial UR MH MP Birth Date Sex Post Code / / M F ECOG (see codes below) Date of Diagnosis Consultant
Preoperative Data Please place patient label here Patient Information Patient s Last Name First Middle Initial UR MH MP Birth Date Sex Post Code / / M F ECOG (see codes below) Date of Diagnosis Consultant
Colorectal Cancer Treatment
 Colorectal Cancer Treatment Introduction Scope of the problem Screening protocols Syed Husain, MD, FACS, FASCRS Assistant Professor of Surgery Department of Surgery Division of Colon and Rectal Surgery
Colorectal Cancer Treatment Introduction Scope of the problem Screening protocols Syed Husain, MD, FACS, FASCRS Assistant Professor of Surgery Department of Surgery Division of Colon and Rectal Surgery
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015
: Imaging Guidelines September 2015") Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colorectal Cancer Update Dr. Barb Melosky
 Colorectal Cancer Update 2017 Dr. Barb Melosky bmelosky@bccancer.bc.ca Disclosure Research Support/P.I. Honoraria/Advisory Board Bayer Roche, Amgen, Bayer, Lilly Objectives 1) Demonstrate knowledge of
Colorectal Cancer Update 2017 Dr. Barb Melosky bmelosky@bccancer.bc.ca Disclosure Research Support/P.I. Honoraria/Advisory Board Bayer Roche, Amgen, Bayer, Lilly Objectives 1) Demonstrate knowledge of
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
Rectal Cancer. GI Practice Guideline
 Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Outline. Colon and Rectal Cancers. Overview. Overview. Anatomic Distribution. Incidence and Mortality 12/12/2013
 Colon and Rectal Cancers FCDS 2013-2014 Educational Webcast Series December 12, 2013 Mayra Espino, BA, RHIT, CTR Steven Peace, BS, CTR FCDS QC Staff 1 Outline Overview Incidence/Mortality/Survival Risk
Colon and Rectal Cancers FCDS 2013-2014 Educational Webcast Series December 12, 2013 Mayra Espino, BA, RHIT, CTR Steven Peace, BS, CTR FCDS QC Staff 1 Outline Overview Incidence/Mortality/Survival Risk
Neoplasms of the Colon and of the Rectum
 Neoplasms of the Colon and of the Rectum 2 0 1 5-2 0 1 6 F C D S E D U C A T I O N A L W E B C A S T S E R I E S S T E V E N P E A C E, B S, C T R F E B R U A R Y 1 8, 2 0 1 6 2016 Focus o Anatomy o SS
Neoplasms of the Colon and of the Rectum 2 0 1 5-2 0 1 6 F C D S E D U C A T I O N A L W E B C A S T S E R I E S S T E V E N P E A C E, B S, C T R F E B R U A R Y 1 8, 2 0 1 6 2016 Focus o Anatomy o SS
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Colon and Rectal Cancers. Outline. Overview 12/12/2013. FCDS Educational Webcast Series December 12, 2013
 Colon and Rectal Cancers FCDS 2013-2014 Educational Webcast Series December 12, 2013 Mayra Espino, BA, RHIT, CTR Steven Peace, BS, CTR FCDS QC Staff 1 Outline Overview Incidence/Mortality/Survival Risk
Colon and Rectal Cancers FCDS 2013-2014 Educational Webcast Series December 12, 2013 Mayra Espino, BA, RHIT, CTR Steven Peace, BS, CTR FCDS QC Staff 1 Outline Overview Incidence/Mortality/Survival Risk
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM
 OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Resident Seminar Aug 19 th, 2015 Colon: Neoplastic. Scott Rieder Dr. Colquhoun
 Resident Seminar Aug 19 th, 2015 Colon: Neoplastic Scott Rieder Dr. Colquhoun Objectives Medical Expert: 1. The biologic basis of colon neoplasia 2. Colon cancer screening (guidelines and evidence) 3.
Resident Seminar Aug 19 th, 2015 Colon: Neoplastic Scott Rieder Dr. Colquhoun Objectives Medical Expert: 1. The biologic basis of colon neoplasia 2. Colon cancer screening (guidelines and evidence) 3.
Anaplastic A term used to describe cancer cells that divide rapidly and have little or no resemblance to normal cells.
 Oncology Terminology A Adenocarcinoma A cancerous tumor that arises in or resembles glandular tissue. Adjunct agent In cancer therapy, a drug or substance used in addition to the primary therapy. Adjuvant
Oncology Terminology A Adenocarcinoma A cancerous tumor that arises in or resembles glandular tissue. Adjunct agent In cancer therapy, a drug or substance used in addition to the primary therapy. Adjuvant
Seventh Edition Staging 2017 Colorectum. Overview. This webinar is sponsored by. the Centers for Disease Control and Prevention.
 Seventh Edition Staging 2017 Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express
Seventh Edition Staging 2017 Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express
North of Scotland Cancer Network Clinical Management Guideline for Carcinoma of the Uterine Cervix
 THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
RECTAL CANCER CLINICAL CASE PRESENTATION
 RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
Familial Adenomatous Polyposis
 Familial Adenomatous Polyposis 1 in 10,000 incidence 100 s to 1000 s of colonic adenomas by teens Cancer risk: colon, gastric, duodenum (periampulla), small bowel, pancreas, papillary thyroid, childhood
Familial Adenomatous Polyposis 1 in 10,000 incidence 100 s to 1000 s of colonic adenomas by teens Cancer risk: colon, gastric, duodenum (periampulla), small bowel, pancreas, papillary thyroid, childhood
COLON CANCER PROFILE 2012} Cancer Outcomes Analysis Report. The Institute for. Cancer Care
 COLON CANCER PROFILE 2012} Cancer Outcomes Analysis Report The Institute for Cancer Care FACT} People with a first-degree relative (parent, sibling, or children) who has colon cancer are between two and
COLON CANCER PROFILE 2012} Cancer Outcomes Analysis Report The Institute for Cancer Care FACT} People with a first-degree relative (parent, sibling, or children) who has colon cancer are between two and
Colorectal Carcinoma Reporting in 2009
 Colorectal Carcinoma Reporting in 2009 Overview Colorectal carcinoma- new and confusing AJCC TNM issues Wendy L. Frankel, M.D. Vice-Chair and Director of AP Department of Pathology The Ohio State University
Colorectal Carcinoma Reporting in 2009 Overview Colorectal carcinoma- new and confusing AJCC TNM issues Wendy L. Frankel, M.D. Vice-Chair and Director of AP Department of Pathology The Ohio State University
GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS. Family Health Clinical Genetics. Clinical Genetics department
 GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS Full Title of Guideline: Author (include email and role): Division & Speciality: GUIDELINES FOR THE GENETIC MANAGEMENT OF A FAMILY
GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS Full Title of Guideline: Author (include email and role): Division & Speciality: GUIDELINES FOR THE GENETIC MANAGEMENT OF A FAMILY
Bowel cancer. A guide for the GP
 THEME GI malignancies Bowel cancer A guide for the GP Paul McMurrick FRACS, is a colorectal surgeon, Malvern, and Senior Lecturer in Surgery, Cabrini Monash University Academic Surgical Department, Victoria.
THEME GI malignancies Bowel cancer A guide for the GP Paul McMurrick FRACS, is a colorectal surgeon, Malvern, and Senior Lecturer in Surgery, Cabrini Monash University Academic Surgical Department, Victoria.
Colon, Rectum, and Appendix
 Colon, Rectum, and Appendix 2011 Reporting Requirements and CSv02.03.02 NCCN/ASCO Treatment Guidelines by Stage FCDS 2011 Educational Webcast Series September 15, 2011 Steven Peace, CTR Presentation Outline
Colon, Rectum, and Appendix 2011 Reporting Requirements and CSv02.03.02 NCCN/ASCO Treatment Guidelines by Stage FCDS 2011 Educational Webcast Series September 15, 2011 Steven Peace, CTR Presentation Outline
Colon, Rectum, and Appendix. Presentation Outline. Overview Tumor Characteristics
 Colon, Rectum, and Appendix 2011 Reporting Requirements and CSv02.03.02 NCCN/ASCO Treatment Guidelines by Stage FCDS 2011 Educational Webcast Series September 15, 2011 Steven Peace, CTR Presentation Outline
Colon, Rectum, and Appendix 2011 Reporting Requirements and CSv02.03.02 NCCN/ASCO Treatment Guidelines by Stage FCDS 2011 Educational Webcast Series September 15, 2011 Steven Peace, CTR Presentation Outline
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Physician Follow-Up and Guideline Adherence in Post- Treatment Surveillance of Colorectal Cancer
 Physician Follow-Up and Guideline Adherence in Post- Treatment Surveillance of Colorectal Cancer Gabriela M. Vargas, MD Kristin M. Sheffield, PhD, Abhishek Parmar, MD, Yimei Han, MS, Kimberly M. Brown,
Physician Follow-Up and Guideline Adherence in Post- Treatment Surveillance of Colorectal Cancer Gabriela M. Vargas, MD Kristin M. Sheffield, PhD, Abhishek Parmar, MD, Yimei Han, MS, Kimberly M. Brown,
Microsatellite instability and other molecular markers: how useful are they?
 Microsatellite instability and other molecular markers: how useful are they? Pr Frédéric Bibeau, MD, PhD Head, Pathology department CHU de Caen, Normandy University, France ESMO preceptorship, Barcelona,
Microsatellite instability and other molecular markers: how useful are they? Pr Frédéric Bibeau, MD, PhD Head, Pathology department CHU de Caen, Normandy University, France ESMO preceptorship, Barcelona,
Gallbladder Cancer. GI Practice Guideline. Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist)
 Barbara Fisher, MD, FRCPC (Radiation Oncologist)") Gallbladder Cancer GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: September 2006 This guideline is a statement of
Gallbladder Cancer GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: September 2006 This guideline is a statement of
Colorectal Cancer. Mark Chapman. MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist
 21 st March 2018 Consultant Coloproctologist") Colorectal Cancer Mark Chapman MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist Overview Epidemiology of colorectal cancer Adenoma carcinoma sequence Tumour diagnosis & staging Treatment
Colorectal Cancer Mark Chapman MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist Overview Epidemiology of colorectal cancer Adenoma carcinoma sequence Tumour diagnosis & staging Treatment
Medical Therapy of Colorectal Cancer in the Biomarker Era
 Medical Therapy of Colorectal Cancer in the Biomarker Era Axel Grothey Professor of Oncology Mayo Clinic College of Medicine Rochester, Minnesota Disclosures Consulting activities (honoraria went to the
Medical Therapy of Colorectal Cancer in the Biomarker Era Axel Grothey Professor of Oncology Mayo Clinic College of Medicine Rochester, Minnesota Disclosures Consulting activities (honoraria went to the
2/20/14& Medical Management of Colon and Rectal Cancer: An Overview. Outline / Learning Objectives. How common is colon cancer?
 Medical Management of Colon and Rectal Cancer: An Overview Jonathan Grim, MD, PhD VA Puget Sound Health Care System Fred Hutchinson Cancer Research Center UW Medicine Outline / Learning Objectives Epidemiology
Medical Management of Colon and Rectal Cancer: An Overview Jonathan Grim, MD, PhD VA Puget Sound Health Care System Fred Hutchinson Cancer Research Center UW Medicine Outline / Learning Objectives Epidemiology
Colorectal Neoplasia. Dr. Smita Devani MBChB, MRCP. Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi
 Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
UPDATE IN THE MANAGEMENT AND TREATMENT OF COLORECTAL CANCER. Edwin A. Empaynado, MD Advocare Colon and Rectal Surgical Specialists
 UPDATE IN THE MANAGEMENT AND TREATMENT OF COLORECTAL CANCER Edwin A. Empaynado, MD Advocare Colon and Rectal Surgical Specialists WHAT IS COLON CANCER? WHAT CAUSES COLORECTAL CANCER? WHAT ARE THE RISK
UPDATE IN THE MANAGEMENT AND TREATMENT OF COLORECTAL CANCER Edwin A. Empaynado, MD Advocare Colon and Rectal Surgical Specialists WHAT IS COLON CANCER? WHAT CAUSES COLORECTAL CANCER? WHAT ARE THE RISK
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
[A RESEARCH COORDINATOR S GUIDE]
![[A RESEARCH COORDINATOR S GUIDE]](/thumbs/88/117127924.jpg "[A RESEARCH COORDINATOR S GUIDE]") 2013 COLORECTAL SURGERY GROUP Dr. Carl J. Brown Dr. Ahmer A. Karimuddin Dr. P. Terry Phang Dr. Manoj J. Raval Authored by Jennifer Lee A cartoon about colonoscopies. 1 [A RESEARCH COORDINATOR S GUIDE]
2013 COLORECTAL SURGERY GROUP Dr. Carl J. Brown Dr. Ahmer A. Karimuddin Dr. P. Terry Phang Dr. Manoj J. Raval Authored by Jennifer Lee A cartoon about colonoscopies. 1 [A RESEARCH COORDINATOR S GUIDE]
What All of Us Should Know About Cancer and Genetics
 What All of Us Should Know About Cancer and Genetics Beth A. Pletcher, MD, FAAP, FACMG Associate Professor of Pediatrics UMDNJ- New Jersey Medical School Disclosures I have no relevant financial relationships
What All of Us Should Know About Cancer and Genetics Beth A. Pletcher, MD, FAAP, FACMG Associate Professor of Pediatrics UMDNJ- New Jersey Medical School Disclosures I have no relevant financial relationships
Newton Wellesley Hospital 2013
 Newton Wellesley Hospital 20 Standard 4.6 Assessment and Evaluation of Treatment Planning Endometrial Cancer Each year a physician member of the cancer committee conducts a study to ensure that diagnostic
Newton Wellesley Hospital 20 Standard 4.6 Assessment and Evaluation of Treatment Planning Endometrial Cancer Each year a physician member of the cancer committee conducts a study to ensure that diagnostic
Pancreatic Cancer. BIOLOGY: Not well defined (genetic and enviromental factors) CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.
 CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.") EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
Classification of polyposis syndromes two major groups. Adenomatous polyposis syndromes. Hamartomatous polyposis syndromes
 Hereditary polyposis syndromes Classification of polyposis syndromes two major groups adenomatous and non-adenomatous polyposis syndromes Adenomatous polyposis syndromes Familial adenomatous polyposis(fap)
Hereditary polyposis syndromes Classification of polyposis syndromes two major groups adenomatous and non-adenomatous polyposis syndromes Adenomatous polyposis syndromes Familial adenomatous polyposis(fap)
Stage: The Language of Cancer
 Stage: The Language of Cancer American Joint Committee on Cancer American College of Surgeons Chicago, IL Validating science. Improving patient care. No materials in this presentation may be repurposed
Stage: The Language of Cancer American Joint Committee on Cancer American College of Surgeons Chicago, IL Validating science. Improving patient care. No materials in this presentation may be repurposed
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
The Rodger C. Haggitt Memorial Lecture
 The Rodger C. Haggitt Memorial Lecture I got an email on 4/22/14 from Hala El Zamaity inviting me to give this lecture and giving me this topic: The ever changing TNM classification and its implication
The Rodger C. Haggitt Memorial Lecture I got an email on 4/22/14 from Hala El Zamaity inviting me to give this lecture and giving me this topic: The ever changing TNM classification and its implication
Guide to Colorectal Cancer
 Guide to Colorectal Cancer Comprehensive, oncologist-approved cancer information from the American Society of Clinical Oncology (ASCO) www.cancer.net Made available through: ABOUT ASCO The American Society
Guide to Colorectal Cancer Comprehensive, oncologist-approved cancer information from the American Society of Clinical Oncology (ASCO) www.cancer.net Made available through: ABOUT ASCO The American Society
Mr Chris Wakeman. General Surgeon University of Otago, Christchurch. 12:15-12:40 Management of Colorectal Cancer
 Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Treatment strategy of metastatic rectal cancer
 35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
Colon and Rectum 5/1/14
 Collecting Cancer Data: Colon and Rectum 2013 2014 NAACCR Webinar Series May 1, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data: Colon and Rectum 2013 2014 NAACCR Webinar Series May 1, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
PeaceHealth Physicians Journal Volume 5, Number 1, Fall 2012
 Exceptional Medicine PeaceHealth Physicians Journal Volume 5, Number 1, Fall 2012 Mortality from colorectal cancer has declined over the last three decades mainly related to earlier diagnosis through screening
Exceptional Medicine PeaceHealth Physicians Journal Volume 5, Number 1, Fall 2012 Mortality from colorectal cancer has declined over the last three decades mainly related to earlier diagnosis through screening
Cancer Genomics 101. BCCCP 2015 Annual Meeting
 Cancer Genomics 101 BCCCP 2015 Annual Meeting Objectives Identify red flags in a person s personal and family medical history that indicate a potential inherited susceptibility to cancer Develop a systematic
Cancer Genomics 101 BCCCP 2015 Annual Meeting Objectives Identify red flags in a person s personal and family medical history that indicate a potential inherited susceptibility to cancer Develop a systematic
reviews Staging, and in the Diagnosis, Managed Care Considerations therapy
 reviews therapy Managed Care Considerations in the Diagnosis, Staging, and Treatment of Colorectal Cancer by Johanna Bendell, MD, Director, GI Oncology Research; Associate Director, Drug Development Unit,
reviews therapy Managed Care Considerations in the Diagnosis, Staging, and Treatment of Colorectal Cancer by Johanna Bendell, MD, Director, GI Oncology Research; Associate Director, Drug Development Unit,
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
General Surgery Grand Grounds
 General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
Gastric Cancer in a Young Postpartum Female. Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012
 Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Radiation Oncology MOC Study Guide
 Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)
Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)