Type I. Type II. Excess estrogen Lynch Endometrioid adenocarcinoma PTEN. High grade More aggressive Serous, Clear Cell p53
|
|
|
- Ross Stevenson
- 5 years ago
- Views:
Transcription

1
2 Type I Excess estrogen Lynch Endometrioid adenocarcinoma PTEN Type II High grade More aggressive Serous, Clear Cell p53
3 Stage I IA IB Stage II Stage III IIIA IIIB IIIC IIIC1 IIIC2 Stage IV IVA IVB nodes Tumour confined to the corpus uteri No or less than half myometrial invasion Invasion equal to or more than half of the myometrium Tumour invades cervical stroma, but does not extend beyond the uterus Local and/or regional spread of the tumour Tumour invades the serosa of the corpus uteri and/or adnexae Vaginal and/or parametrial involvement Metastases to pelvic and/or para-aortic lymph nodes Positive pelvic nodes Positive para-aortic lymph nodes with or without positive pelvic lymph nodes Tumour invades bladder and/or bowel mucosa, and/or distant metastases Tumour invasion of bladder and/or bowel mucosa Distant metastases, including intra-abdominal metastases and/or inguinal lymph
4 IIIA- uterine serosal or adnexal involvement IIIB- vaginal and/or parametrial involvement IIIC- pelvic and/or para-aortic nodes (IIIC1- pelvic nodes; IIIC2- para-aortic nodes)
5 to be performed and reported separately ie not part of staging system significance to be discussed at MDTM
6 never had staging system previously carcinosarcomas staged as per uterine carcinomas staging system for leiomyosarcomas different system for ESS and adenosarcoma Local and hematogenous spread
7 Stage I IA IB Stage II IIA IIB Tumour limited to uterus <5 cm >5 cm Tumour extends to the pelvis Adnexal involvement Tumour extends to extrauterine pelvic tissue Stage III Tumour invades abdominal tissues (not just protruding into the abdomen) IIIA One site IIIB > one site IIIC Metastasis to pelvic and/or para-aortic lymph nodes Stage IV IVA IVB Tumour invades bladder and/or rectum Distant metastasis
8 Stage I IA IB IC Stage II IIA IIB Stage III IIIA IIIB IIIC Stage IV IVA IVB Tumour limited to uterus Tumour limited to endometrium/endocervix with no myometrial invasion Less than or equal to half myometrial invasion More than half myometrial invasion Tumour extends to the pelvis Adnexal involvement Tumour extends to extrauterine pelvic tissue Tumour invades abdominal tissues (not just protruding into the abdomen) One site > one site Metastasis to pelvic and/or para-aortic lymph nodes Tumour invades bladder and/or rectum Distant metastasis
9 Squamous Adenocarcinoma Adenosquamous Clinical staging
10 Stage I IA IA1 IA2 IB IB1 IB2 Stage II lower IIA IIA1 IIA2 IIB The carcinoma is strictly confined to the cervix (extension to the corpus would be disregarded) Invasive carcinoma which can be diagnosed only by microscopy, with deepest invasion <5 mm and the largest extension >7 mm Measured stromal invasion of <3.0 mm in depth and extension of <7.0 mm Measured stromal invasion of >3.0 mm and not >5.0 mm with an extension of not >7.0 mm Clinically visible lesions limited to the cervix uteri or pre-clinical cancers greater than stage IA Clinically visible lesion <4.0 cm in greatest dimension Clinically visible lesion >4.0 cm in greatest dimension Cervical carcinoma invades beyond the uterus, but not to the pelvic wall or to the third of the vagina Without parametrial invasion Clinically visible lesion <4.0 cm in greatest dimension Clinically visible lesion >4.0 cm in greatest dimension With obvious parametrial invasion
11
12 SCC Melanoma AdenoCa BCC Sarcoma Surgically staged
13 Stage I IA IB Stage II Stage III nodes. IIIA Tumour confined to the vulva Lesions <2 cm in size, confined to the vulva or perineum and with stromal invasions <1.0 mm*, no nodal metastasis Lesions >2 cm in size or with stromal invasion >1.0 mm* confined to the vulva or perineum, with negative nodes Tumour of any size with extension to adjacent perineal structures (1/3 lower urethra, 1/3 lower vagina, anus) with negative nodes Tumour of any size with or without extension to adjacent perineal structures (1/3 lower urethra, 1/3 lower vagina, anus) with positive inguino-femoral lymph (i) With 1 lymph node metastasis (>5 mm), or (ii) 1-2 lymph node metastasis(es) (<5 mm) IIIB (i) With 2 or more lymph node metastases (>5 mm), or (ii) 3 or more lymph node metastases (<5 mm) IIIC With positive nodes with extracapsular spread Stage IV Tumour invades other regional (2/3 upper urethra, 2/3 upper vagina), or distant structures. IVA Tumour invades any of the following: (i) upper urethral and/or vaginal mucosa, bladder mucosa, rectal mucosa, or fixed to pelvic bone, or (ii) fixed or ulcerated inguino-femoral lymph nodes IVB Any distant metastasis including pelvic lymph nodes * The depth of invasion is defined as the measurement of the tumour from the epithelialstromal junction of the adjacent most superficial dermal papilla to the deepest point of invasion.
14 IA- < 2cm, stromal invasion <1mm, confined to vulval or perineum, no nodal metastasis IB- previous IB and II combined- >2cm size or with stromal invasion >1mm, confined to vulval or perineum, no nodal metastasis
15 any size with extension to lower third of urethra, lower third of vagina or anus and negative nodes
16 any size, with or without extension to lower third of urethra, lower third of vagina or anus and positive inguino-femoral nodes IIIA- 1 nodal metastasis > 5mm or up to 2 nodes <5mm IIIB- 2 or more nodes >5mm or 3 or more nodes <5mm IIIC- extracapsular spread
17 upper two thirds of urethra or vagina or distant structures various substages bilateral nodal involvement now not taken into account
18 Surgery WLE- Stage O, stage IA SCC, Pagets, Radical partial vulvectomy all others that are amenable to surgery
19 LNs For greater than stage IA disease Unilateral lesion- unilateral LNDx Central lesion- Bilateral LNDx Sentinel LN Biopsy Radioactive label- Technicium Isosulphan blue intraop injected Resect all hot and blue nodes
20 Locally advanced disease Neoadjuvant chemoradiation
21 Pain and itching Hyperemic, well demarcated lesions, cake icing coating Patchy leukoplakia Approx 10-20% with associated local or distant adenocarcinoma
22 Intraepithelial lesion. Large cells, clear cytoplasm, confined to epidermis, can involve hair follicles. Wide Local Excision Recurrence common regardless of margin status.
23 Epithelial Germ Cell Sex Cord Stromal
24 Serous Mucionous Endometrioid Clear Cell Ca125, CEA, Ca19-9 Endometriosis link to clear cell and endometriois
25 Most sporadic Familial Breast Ovarian type BRCA 1 & 2 Carboplatin- N/V, hypersensitivity Paclitaxel- alopecia, neuropathy
26 Dysgerminoma +LDH Choriocarcinoma + HCG Yolk Sac Tumor + AFP Immature Teratoma
27 Chemosensitive Affects younger patients Fertility preservation Bleomycin- Pulm Fibrosis Etoposide- Secondary malignancy Cisplatin- Renal impairment
28 Granulosa Cell tumors Increased estrogen, concurrent endometrial Ca, Inhibin Fibro-thecomas Sertoli-Leydig tumors Virilising Gynandroblastoma
29 Rare More likely to be secondary than primary ca. If cervix or vulva involved, then is classified as this primary Types- SCC Clear cell Melanoma Sarcoma
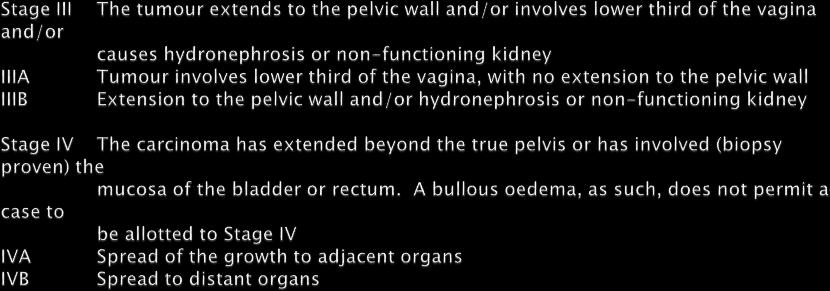
30 Staging- Clinical, not surgical, ie exam and imaging Stage 0-CIS Stage I- Vaginal Wall Stage II- Subvaginal wall Stage III-Pelvic wall Stage IVA- Invasion of rectal or bladder mucosa Stage IVB- Distant spread
31 Upper vagina, spread as for cervix ca Distal vagina, spread as for vulva ca Surgery an option for CIS and stage I disease. Radiation +/-chemo for others. External beam, tandem and ovoid or interstitial implant.
32 Clear cell ca Related to vaginal adenosis Linked to DES exposure, this population is aging out. Arise secondary to endometriosis.
33 Melanoma Typically advanced at diagnosis. Sarcoma Spindle cell- LMS, fibrosarcoma. Local excision and radiation
34 Sarcoma botryoides Children Anterior upper vagina Cluster of grapes, vaginal bleeding Rx- Chemotherapy, (VAC, vincrisitne, actinomycin D, cyclophosphimide), surgery, sometimes just chemoradiation if small lesion.
35 Partial Mole 69XXY Complete Mole 46XX
36 Invasive Mole Choriocarcinoma Placental site trophoblastic tumor Epithelioid trophoblastic tumor May follow any pregnancy, not just molar gestation
37 Stage I-Confined to uterus Stage II- Limited to genital structures Stage III- Lungs Stage IV- Any other spread WHO score Seven or greater is high risk disease (Age, Antecedant pregnancy, Time from pregnancy, HCG, Site, number and size of mets, prior chemo)
38 Non metastatic disease- single agent chemo Methotrexate vs actinomycin D Low risk metastatic- Single agents still, but more intense regimen High risk disease- Multiagent chemotherapy- EMACO
39 Treat until normal HCG then 2 further cycles. Survail for 12 months with monthly HCGs
40 Trophoblastic tumor- surgery, more chemoresistant.
Staging and Treatment Update for Gynecologic Malignancies
 Staging and Treatment Update for Gynecologic Malignancies Bunja Rungruang, MD Medical College of Georgia No disclosures 4 th most common new cases of cancer in women 5 th and 6 th leading cancer deaths
Staging and Treatment Update for Gynecologic Malignancies Bunja Rungruang, MD Medical College of Georgia No disclosures 4 th most common new cases of cancer in women 5 th and 6 th leading cancer deaths
The International Federation of Gynecology and Obstetrics (FIGO) updated the staging
 updated the staging") Continuing Education Column Revised FIGO Staging System Hee Sug Ryu, MD Department of Obstetrics and Gynecology, Ajou University School of Medicine E - mail : hsryu@ajou.ac.kr J Korean Med Assoc 2010;
Continuing Education Column Revised FIGO Staging System Hee Sug Ryu, MD Department of Obstetrics and Gynecology, Ajou University School of Medicine E - mail : hsryu@ajou.ac.kr J Korean Med Assoc 2010;
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR Last Revision Date July 2015 1 Site Group: Gynecologic Cancer Vulvar Author: Dr. Stephane Laframboise 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR Last Revision Date July 2015 1 Site Group: Gynecologic Cancer Vulvar Author: Dr. Stephane Laframboise 1. INTRODUCTION
New Cancer Cases By Site Breast 28% Lung 14% Colo-Rectal 10% Uterus 6% Thyroid 5% Lymphoma 4% Ovary 3%
 Uterine Malignancy New Cancer Cases By Site 2010 Breast 28% Lung 14% Colo-Rectal 10% Uterus 6% Thyroid 5% Lymphoma 4% Ovary 3% Cancer Deaths By Site 2010 Lung 26% Breast 15% Colo-Rectal 9% Pancreas 7%
Uterine Malignancy New Cancer Cases By Site 2010 Breast 28% Lung 14% Colo-Rectal 10% Uterus 6% Thyroid 5% Lymphoma 4% Ovary 3% Cancer Deaths By Site 2010 Lung 26% Breast 15% Colo-Rectal 9% Pancreas 7%
C ORPUS UTERI C ARCINOMA STAGING FORM (Carcinosarcomas should be staged as carcinomas)
") CLINICAL C ORPUS UTERI C ARCINOMA STAGING FORM PATHOLOGIC Extent of disease before S TAGE C ATEGORY D EFINITIONS Extent of disease through any treatment completion of definitive surgery y clinical staging
CLINICAL C ORPUS UTERI C ARCINOMA STAGING FORM PATHOLOGIC Extent of disease before S TAGE C ATEGORY D EFINITIONS Extent of disease through any treatment completion of definitive surgery y clinical staging
Proposed All Wales Vulval Cancer Guidelines. Dr Amanda Tristram
 Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
C ORPUS UTERI C ARCINOMA STAGING FORM (Carcinosarcomas should be staged as carcinomas)
") C ORPUS UTERI C ARCINOMA STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery Tis * T1 I T1a IA NX N0 N1 N2
C ORPUS UTERI C ARCINOMA STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery Tis * T1 I T1a IA NX N0 N1 N2
Staging. Carcinoma confined to the corpus. Carcinoma confined to the endometrium. Less than ½ myometrial invasion. Greater than ½ myometrial invasion
 5 th of June 2009 Background Most common gynaecological carcinoma in developed countries Most cases are post-menopausal Increasing incidence in certain age groups Increasing death rates in the USA 5-year
5 th of June 2009 Background Most common gynaecological carcinoma in developed countries Most cases are post-menopausal Increasing incidence in certain age groups Increasing death rates in the USA 5-year
Cervical Cancer: 2018 FIGO Staging
 Cervical Cancer: 2018 FIGO Staging Jonathan S. Berek, MD, MMS Laurie Kraus Lacob Professor Stanford University School of Medicine Director, Stanford Women s Cancer Center Senior Scientific Advisor, Stanford
Cervical Cancer: 2018 FIGO Staging Jonathan S. Berek, MD, MMS Laurie Kraus Lacob Professor Stanford University School of Medicine Director, Stanford Women s Cancer Center Senior Scientific Advisor, Stanford
3/25/2019. J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse
 J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse 1 4 th most common GYN cancer 5% of malignancies of GYN type. 4850 new cases annually 1030 deaths Cigarette smoking Vulvar dystrophy (Lichen
J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse 1 4 th most common GYN cancer 5% of malignancies of GYN type. 4850 new cases annually 1030 deaths Cigarette smoking Vulvar dystrophy (Lichen
Guideline for the Management of Vulval Cancer
 Version History Guideline for the Management of Vulval Cancer Version Date Brief Summary of Change Issued 2.0 20.02.08 Endorsed by the Governance Committee 2.1 19.11.10 Circulated at NSSG meeting 2.2 13.04.11
Version History Guideline for the Management of Vulval Cancer Version Date Brief Summary of Change Issued 2.0 20.02.08 Endorsed by the Governance Committee 2.1 19.11.10 Circulated at NSSG meeting 2.2 13.04.11
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
Janjira Petsuksiri, M.D
 GYN malignancies Janjira Petsuksiri, M.D Outlines Cervical cancer Endometrial cancer Ovarian cancer Vaginal cancer Vulva cancer 2 CA Cervix Epidemiology - Second most common female cancer Risk factors
GYN malignancies Janjira Petsuksiri, M.D Outlines Cervical cancer Endometrial cancer Ovarian cancer Vaginal cancer Vulva cancer 2 CA Cervix Epidemiology - Second most common female cancer Risk factors
Endometrial Cancer. Incidence. Types 3/25/2019
 Endometrial Cancer J. Anthony Rakowski DO, FACOOG MSU SCS Board Review Coarse Incidence 53,630 new cases yearly 8,590 deaths yearly 4 th most common malignancy in women worldwide Most common GYN malignancy
Endometrial Cancer J. Anthony Rakowski DO, FACOOG MSU SCS Board Review Coarse Incidence 53,630 new cases yearly 8,590 deaths yearly 4 th most common malignancy in women worldwide Most common GYN malignancy
3/25/2019. Rare uterine cancers ~3% Leiomyosarcoma Carcinosarcoma (MMMT) Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates
 Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates") J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse Rare uterine cancers ~3% Leiomyosarcoma Carcinosarcoma (MMMT) Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates Signs
J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse Rare uterine cancers ~3% Leiomyosarcoma Carcinosarcoma (MMMT) Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates Signs
2009 USCAP Gyn Pathology Evening Session Case #3. Richard J. Zaino, MD Hershey Medical Center Penn State University Hershey, PA
 2009 USCAP Gyn Pathology Evening Session Case #3 Richard J. Zaino, MD Hershey Medical Center Penn State University Hershey, PA rzaino@psu.edu Clinical history Middle aged woman with an exophytic mass of
2009 USCAP Gyn Pathology Evening Session Case #3 Richard J. Zaino, MD Hershey Medical Center Penn State University Hershey, PA rzaino@psu.edu Clinical history Middle aged woman with an exophytic mass of
Jacqui Morgan March 6, 2019
 Jacqui Morgan March 6, 2019 Case 1 25yo, G2P1 Here for WWE, no problems, healthy, needs refill on OCPs. Pap- Abnormal Glandular Cells-NOS Now What?? Case 1 Colposcopy What findings? Case 1 ECC Cervical
Jacqui Morgan March 6, 2019 Case 1 25yo, G2P1 Here for WWE, no problems, healthy, needs refill on OCPs. Pap- Abnormal Glandular Cells-NOS Now What?? Case 1 Colposcopy What findings? Case 1 ECC Cervical
North of Scotland Cancer Network Clinical Management Guideline for Carcinoma of the Uterine Cervix
 THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
University of Kentucky. Markey Cancer Center
 University of Kentucky Markey Cancer Center Invasive Cancer of the Vagina and Urethra Fred Ueland, MD No matter what you accomplish in your life, the size of your funeral will still be determined by the
University of Kentucky Markey Cancer Center Invasive Cancer of the Vagina and Urethra Fred Ueland, MD No matter what you accomplish in your life, the size of your funeral will still be determined by the
Gynecologic Oncologist. Surgery Chemotherapy Radiation Therapy Hormonal Therapy Immunotherapy. Cervical cancer
 Gynecologic Oncology Pre invasive vulvar, vaginal, & cervical disease Vulvar Cervical Endometrial Uterine Sarcoma Fallopian Tube Ovarian GTD Gynecologic Oncologist Surgery Chemotherapy Radiation Therapy
Gynecologic Oncology Pre invasive vulvar, vaginal, & cervical disease Vulvar Cervical Endometrial Uterine Sarcoma Fallopian Tube Ovarian GTD Gynecologic Oncologist Surgery Chemotherapy Radiation Therapy
Cervical Cancer 3/25/2019. Abnormal vaginal bleeding
 Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Uterine Malignancies. Collecting Cancer Data: Uterine Malignancies 10/7/2010. NAACCR Webinar Series 1. Questions. Fabulous Prizes!!!
 Uterine October 7, 2010 NAACCR 2010-2011 Webinar Series Session 1 1 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes!!! 3 NAACCR 2010-2011 Webinar
Uterine October 7, 2010 NAACCR 2010-2011 Webinar Series Session 1 1 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes!!! 3 NAACCR 2010-2011 Webinar
Vulvar Carcinoma. Definition: Cases should be classified as carsinoma of the vulva when the primary site growth is in the vulva Malignant melanoma sho
 Carcinoma Vulva & Vagina Subdivisi Onkologi Ginekologi Bagian Obgin FK USU Vulvar Carcinoma. Definition: Cases should be classified as carsinoma of the vulva when the primary site growth is in the vulva
Carcinoma Vulva & Vagina Subdivisi Onkologi Ginekologi Bagian Obgin FK USU Vulvar Carcinoma. Definition: Cases should be classified as carsinoma of the vulva when the primary site growth is in the vulva
Cervical cancer presentation
 Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Uterus Malignancies /5/15
 Collecting Cancer Data: Uterus 2014-2015 NAACCR Webinar Series February 5, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Uterus 2014-2015 NAACCR Webinar Series February 5, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Vaginal intraepithelial neoplasia
 Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
ARROCase: Locally Advanced Endometrial Cancer
 ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
Coversheet for Network Site Specific Group Agreed Documentation
 Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
North of Scotland Cancer Network Clinical Management Guideline for Endometrial Cancer
 THIS DOCUMENT North of Scotland Cancer Network Clinical Management Guideline for Endometrial Cancer Based on WOSCAN CMG with further extensive consultation within NOSCAN UNCONTROLLED WHEN PRINTED DOCUMENT
THIS DOCUMENT North of Scotland Cancer Network Clinical Management Guideline for Endometrial Cancer Based on WOSCAN CMG with further extensive consultation within NOSCAN UNCONTROLLED WHEN PRINTED DOCUMENT
SCAN Gynaecological Group. Clinical Management Protocols vulval cancer
 SE Scotland Cancer Network SCAN Gynaecological Group Clinical Management Protocols vulval cancer 2009 www.scan.scot.nhs.uk August 2001 updated annually, most recently INTRODUCTION The South East Scotland
SE Scotland Cancer Network SCAN Gynaecological Group Clinical Management Protocols vulval cancer 2009 www.scan.scot.nhs.uk August 2001 updated annually, most recently INTRODUCTION The South East Scotland
Adjuvant Therapies in Endometrial Cancer. Emma Hudson
 Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
receive adjuvant chemotherapy
 Women with high h risk early stage endometrial cancer should receive adjuvant chemotherapy Michael Friedlander The Prince of Wales Cancer Centre and Royal Hospital for Women The Prince of Wales Cancer
Women with high h risk early stage endometrial cancer should receive adjuvant chemotherapy Michael Friedlander The Prince of Wales Cancer Centre and Royal Hospital for Women The Prince of Wales Cancer
Gynaecological Malignancies
 Gynaecological Malignancies Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea Division of Pathology School of Medicine & Health Sciences Overview Genital tract tumors
Gynaecological Malignancies Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea Division of Pathology School of Medicine & Health Sciences Overview Genital tract tumors
Pathology of the female genital tract
 Pathology of the female genital tract Common illnesses of the female genital tract Before menarche Developmental anomalies Tumors (ovarial teratoma) Amenorrhea Fertile years PCOS, ovarian cysts Endometriosis
Pathology of the female genital tract Common illnesses of the female genital tract Before menarche Developmental anomalies Tumors (ovarial teratoma) Amenorrhea Fertile years PCOS, ovarian cysts Endometriosis
MPH Quiz. 1. How many primaries are present based on this pathology report? 2. What rule is this based on?
 MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
Essex & East Suffolk Gynae Cancer Supra-Network
 Essex & East Suffolk Gynae Cancer Supra-Network Gynaecological Cancers Referral, Diagnosis and Management Guidelines Constitution Version Number 9.0 Author Members of the NSSG Date Written August 2010
Essex & East Suffolk Gynae Cancer Supra-Network Gynaecological Cancers Referral, Diagnosis and Management Guidelines Constitution Version Number 9.0 Author Members of the NSSG Date Written August 2010
Annual report of Gynecologic Oncology Committee, Japan Society of Obstetrics and Gynecology, 2013
 bs_bs_banner doi:10.1111/jog.12360 J. Obstet. Gynaecol. Res. Vol. 40, No. 2: 338 348, February 2014 Annual report of Gynecologic Oncology Committee, Japan Society of Obstetrics and Gynecology, 2013 Daisuke
bs_bs_banner doi:10.1111/jog.12360 J. Obstet. Gynaecol. Res. Vol. 40, No. 2: 338 348, February 2014 Annual report of Gynecologic Oncology Committee, Japan Society of Obstetrics and Gynecology, 2013 Daisuke
ENDOMETRIAL CANCER Updated Apr 2017 by: Dr. Jenny Ko (Medical Oncologist, Abbotsford Cancer Centre)
") ENDOMETRIAL CANCER Updated Apr 2017 by: Dr. Jenny Ko (Medical Oncologist, Abbotsford Cancer Centre) Source: UpToDate 2017, ASCO/CCO/Alberta provincial guidelines, NCCN Reviewed by: Dr. Sarah Glaze (Gynecologic
ENDOMETRIAL CANCER Updated Apr 2017 by: Dr. Jenny Ko (Medical Oncologist, Abbotsford Cancer Centre) Source: UpToDate 2017, ASCO/CCO/Alberta provincial guidelines, NCCN Reviewed by: Dr. Sarah Glaze (Gynecologic
Referral and Management Guidelines for Gynaecological Cancers within North Trent
 North Trent Cancer Network Referral and Management Guidelines for Gynaecological Cancers within North Trent Final Version 3.0 August 2011 Review date : June 2013 Produced by the North Trent Cancer Network
North Trent Cancer Network Referral and Management Guidelines for Gynaecological Cancers within North Trent Final Version 3.0 August 2011 Review date : June 2013 Produced by the North Trent Cancer Network
VULVAR CARCINOMA. Page 1 of 5
 VULVAR CARCINOMA EXAMPLE OF A VULVAR CARCINOMA USING PROPOSED TEMPLATE Case: Invasive squamous cell carcinoma arising in D-VIN Tumor in left labia major Left partial vaginectomy and sentinel lymph node
VULVAR CARCINOMA EXAMPLE OF A VULVAR CARCINOMA USING PROPOSED TEMPLATE Case: Invasive squamous cell carcinoma arising in D-VIN Tumor in left labia major Left partial vaginectomy and sentinel lymph node
NAACCR Webinar Series /7/17
 COLLECTING CANCER DATA: UTERUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
COLLECTING CANCER DATA: UTERUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Invasive Cervical Cancer: Squamous Cell, Adenocarcinoma, Adenosquamous
 Note: If available, clinical trials should be considered as preferred treatment options for eligible patients (www.mdanderson.org/gynonctrials). Other co-morbidities are taken into consideration prior
Note: If available, clinical trials should be considered as preferred treatment options for eligible patients (www.mdanderson.org/gynonctrials). Other co-morbidities are taken into consideration prior
New FIGO Staging of Uterine malignancies with MR Imaging: Correlation with Surgical and Histopathologic Findings
 New FIGO Staging of Uterine malignancies with MR Imaging: Correlation with Surgical and Histopathologic Findings Poster No.: C-1548 Congress: ECR 2011 Type: Educational Exhibit Authors: J. Takahama, A.
New FIGO Staging of Uterine malignancies with MR Imaging: Correlation with Surgical and Histopathologic Findings Poster No.: C-1548 Congress: ECR 2011 Type: Educational Exhibit Authors: J. Takahama, A.
Current staging of endometrial carcinoma with MR imaging
 Current staging of endometrial carcinoma with MR imaging Poster No.: C-1436 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Magalhaes, H. Donato, C. B. Marques, P. Gomes, F. Caseiro Alves; Coimbra/PT
Current staging of endometrial carcinoma with MR imaging Poster No.: C-1436 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Magalhaes, H. Donato, C. B. Marques, P. Gomes, F. Caseiro Alves; Coimbra/PT
Gynaecology NSSG (Lancs & South Cumbria) Uterine Cancer Guidelines (V4.0)
 Uterine Cancer Guidelines (V4.0)") Gynaecology NSSG (Lancs & South Cumbria) Uterine Cancer Guidelines (V4.0) ** VALID ON DATE OF PRINTING ONLY all guidelines available on the Strategic Clinical Network website : GMLSC SCN Date first published
Gynaecology NSSG (Lancs & South Cumbria) Uterine Cancer Guidelines (V4.0) ** VALID ON DATE OF PRINTING ONLY all guidelines available on the Strategic Clinical Network website : GMLSC SCN Date first published
CARCINOMA CERVIX. Dr. PREETHI REDDY. B. M S OBG II yr POST GRADUATE.
 CARCINOMA CERVIX Dr. PREETHI REDDY. B M S OBG II yr POST GRADUATE. Introduction Cervical cancer is the second most common female malignancy worldwide. It is responsible for 4,66,000 deaths annually worldwide
CARCINOMA CERVIX Dr. PREETHI REDDY. B M S OBG II yr POST GRADUATE. Introduction Cervical cancer is the second most common female malignancy worldwide. It is responsible for 4,66,000 deaths annually worldwide
CREOG Review. Gynecologic Oncology
 CREOG Review Gynecologic Oncology 2016 American Cancer Society Statistics 2015 New Cases by Site Breast 231,840 Lung 105,590 Colo-Rectal 63,610 Uterus 54,870 Thyroid 47,230 N-H Lymphoma 32,000 Melanoma
CREOG Review Gynecologic Oncology 2016 American Cancer Society Statistics 2015 New Cases by Site Breast 231,840 Lung 105,590 Colo-Rectal 63,610 Uterus 54,870 Thyroid 47,230 N-H Lymphoma 32,000 Melanoma
Uterine Cervix. Protocol applies to all invasive carcinomas of the cervix.
 Uterine Cervix Protocol applies to all invasive carcinomas of the cervix. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Uterine Cervix Protocol applies to all invasive carcinomas of the cervix. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
ARRO Case: Early-stage Endometrial Cancer
 ARRO Case: Early-stage Endometrial Cancer Ankit Modh, MD (PGY-4) Faculty Advisor: Mohamed A Elshaikh, MD Department of Radiation Oncology Henry Ford Cancer Institute Case Presentation 70 y/o African American
ARRO Case: Early-stage Endometrial Cancer Ankit Modh, MD (PGY-4) Faculty Advisor: Mohamed A Elshaikh, MD Department of Radiation Oncology Henry Ford Cancer Institute Case Presentation 70 y/o African American
CPC on Cervical Pathology
 CPC on Cervical Pathology Dr. W.K. Ng Senior Medical Officer Department of Clinical Pathology Pamela Youde Nethersole Eastern Hospital Cervical Smear: High Grade SIL (CIN III) Cervical Smear: High Grade
CPC on Cervical Pathology Dr. W.K. Ng Senior Medical Officer Department of Clinical Pathology Pamela Youde Nethersole Eastern Hospital Cervical Smear: High Grade SIL (CIN III) Cervical Smear: High Grade
Case 1. Gynaecology Case Presentation. Objectives. Disclosures 22/10/ year old female Clinical history: Assess right ovarian cyst
 Gynaecology Case Presentation Organ Imaging 2016 University of Toronto Sarah Johnson 39 year old female Clinical history: Assess right ovarian cyst Clinically diagnosed endometriosis Started fertility
Gynaecology Case Presentation Organ Imaging 2016 University of Toronto Sarah Johnson 39 year old female Clinical history: Assess right ovarian cyst Clinically diagnosed endometriosis Started fertility
STUMPed for a Diagnosis Contemporary Management of Uterine Sarcomas
 UCSF Helen Diller Family Comprehensive Cancer Center Disclosures I have no financial disclosures STUMPed for a Diagnosis Contemporary Management of Uterine Sarcomas Lee-may Chen, MD Department of Obstetrics,
UCSF Helen Diller Family Comprehensive Cancer Center Disclosures I have no financial disclosures STUMPed for a Diagnosis Contemporary Management of Uterine Sarcomas Lee-may Chen, MD Department of Obstetrics,
GYNAECOLOGICAL CANCER CLINICAL GUIDELINES
 GYNAECOLOGICAL CANCER CLINICAL GUIDELINES Gynae-Oncology Expert Advisory Group Document Information Title: Cancer Alliance Gynae Cancer Clinical Guidelines Author: Gynae EAG Members Circulation List: See
GYNAECOLOGICAL CANCER CLINICAL GUIDELINES Gynae-Oncology Expert Advisory Group Document Information Title: Cancer Alliance Gynae Cancer Clinical Guidelines Author: Gynae EAG Members Circulation List: See
Testicular Malignancies /8/15
 Collecting Cancer Data: Testis 2014-2015 NAACCR Webinar Series January 8, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Testis 2014-2015 NAACCR Webinar Series January 8, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Endometrial Cancer. Saudi Gynecology Oncology Group (SGOG) Gynecological Cancer Treatment Guidelines
 Gynecological Cancer Treatment Guidelines") Saudi Gynecology Oncology Group (SGOG) Gynecological Cancer Treatment Guidelines Endometrial Cancer Emad R. Sagr, MBBS, FRCSC Consultant Gynecology Oncology Security forces Hospital, Riyadh Epidemiology
Saudi Gynecology Oncology Group (SGOG) Gynecological Cancer Treatment Guidelines Endometrial Cancer Emad R. Sagr, MBBS, FRCSC Consultant Gynecology Oncology Security forces Hospital, Riyadh Epidemiology
GYNAECOLOGICAL CANCER CLINICAL GUIDELINES
 Northern England Strategic Clinical Networks GYNAECOLOGICAL CANCER CLINICAL GUIDELINES Gynae-Oncology NSSG on behalf of NECN Document Information Title: NECN Gynae Cancer Clinical Guidelines Author: Gynae
Northern England Strategic Clinical Networks GYNAECOLOGICAL CANCER CLINICAL GUIDELINES Gynae-Oncology NSSG on behalf of NECN Document Information Title: NECN Gynae Cancer Clinical Guidelines Author: Gynae
The new FIGO classification in endometrial carcinoma
 The new FIGO classification in endometrial carcinoma Poster No.: C-1073 Congress: ECR 2012 Type: Educational Exhibit Authors: A. IGLESIAS CASTAÑON, M. Arias Gonzales, J. Mañas Uxó, 1 2 1 2 2 2 B. NIETO
The new FIGO classification in endometrial carcinoma Poster No.: C-1073 Congress: ECR 2012 Type: Educational Exhibit Authors: A. IGLESIAS CASTAÑON, M. Arias Gonzales, J. Mañas Uxó, 1 2 1 2 2 2 B. NIETO
L/O/G/O. Ovarian Tumor. Xiaoyu Niu Obstetrics and Gynecology Department Sichuan University West China Second Hospital
 L/O/G/O Ovarian Tumor Xiaoyu Niu Obstetrics and Gynecology Department Sichuan University West China Second Hospital Essentials classification of ovarian tumor clinical manifestation of ovarian tumor metastatic
L/O/G/O Ovarian Tumor Xiaoyu Niu Obstetrics and Gynecology Department Sichuan University West China Second Hospital Essentials classification of ovarian tumor clinical manifestation of ovarian tumor metastatic
UTERINE SARCOMAS CURRENT THERAPEUTIC OPTIONS
 Review Journal of Translational Medicine and Research, volume 19, no. 1-2, 2014 UTERINE SARCOMAS CURRENT THERAPEUTIC OPTIONS N. Bacalbaæa 1, A. Traistaru 2, I. Bãlescu 3 1 Carol Davila University of Medicine
Review Journal of Translational Medicine and Research, volume 19, no. 1-2, 2014 UTERINE SARCOMAS CURRENT THERAPEUTIC OPTIONS N. Bacalbaæa 1, A. Traistaru 2, I. Bãlescu 3 1 Carol Davila University of Medicine
UTERINE SARCOMA EXAMPLE OF A UTERINE SARCOMA USING PROPOSED TEMPLATE
 UTERINE SARCOMA EXAMPLE OF A UTERINE SARCOMA USING PROPOSED TEMPLATE Case: Adenosarcoma with heterologous elements and stromal overgrowth o TAH, BSO, omentectomy, staging biopsies of cul-de-sac, bladder
UTERINE SARCOMA EXAMPLE OF A UTERINE SARCOMA USING PROPOSED TEMPLATE Case: Adenosarcoma with heterologous elements and stromal overgrowth o TAH, BSO, omentectomy, staging biopsies of cul-de-sac, bladder
The Role of Radiation in the Management of Gynecologic Cancers. Scott Glaser, MD
 The Role of Radiation in the Management of Gynecologic Cancers Scott Glaser, MD Nothing to disclose DISCLOSURE Outline The role of radiation in: Endometrial Cancer Adjuvant Medically inoperable Cervical
The Role of Radiation in the Management of Gynecologic Cancers Scott Glaser, MD Nothing to disclose DISCLOSURE Outline The role of radiation in: Endometrial Cancer Adjuvant Medically inoperable Cervical
Gynecological Cancers in Primary Care
 Gynecological Cancers in Primary Care Nora M. Lersch MSN CRNP AOCNP Division of Gynecological Oncology Objectives Identify the incidence of ovarian, cervical, vulvar and endometrial cancer Identify common
Gynecological Cancers in Primary Care Nora M. Lersch MSN CRNP AOCNP Division of Gynecological Oncology Objectives Identify the incidence of ovarian, cervical, vulvar and endometrial cancer Identify common
Gynecologic Cancer Surveillance and Survivorship: Informing Practice and Policy
 Gynecologic Cancer Surveillance and Survivorship: Informing Practice and Policy Stephanie Yap, M.D. University Gynecologic Oncology Northside Cancer Institute Our Learning Objectives Review survival rates,
Gynecologic Cancer Surveillance and Survivorship: Informing Practice and Policy Stephanie Yap, M.D. University Gynecologic Oncology Northside Cancer Institute Our Learning Objectives Review survival rates,
Dr Sanjiv Manek Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
Gynecologic Malignancies. Kristen D Starbuck 4/20/18
 Gynecologic Malignancies Kristen D Starbuck 4/20/18 Outline Female Cancer Statistics Uterine Cancer Adnexal Cancer Cervical Cancer Vulvar Cancer Uterine Cancer Endometrial Cancer Uterine Sarcoma Endometrial
Gynecologic Malignancies Kristen D Starbuck 4/20/18 Outline Female Cancer Statistics Uterine Cancer Adnexal Cancer Cervical Cancer Vulvar Cancer Uterine Cancer Endometrial Cancer Uterine Sarcoma Endometrial
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER
 UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
GYNECOLOGIC MALIGNANCIES: Ovarian Cancer
 GYNECOLOGIC MALIGNANCIES: Ovarian Cancer KRISTEN STARBUCK, MD ROSWELL PARK CANCER INSTITUTE DEPARTMENT OF SURGERY DIVISION OF GYNECOLOGIC ONCOLOGY APRIL 19 TH, 2018 Objectives Basic Cancer Statistics Discuss
GYNECOLOGIC MALIGNANCIES: Ovarian Cancer KRISTEN STARBUCK, MD ROSWELL PARK CANCER INSTITUTE DEPARTMENT OF SURGERY DIVISION OF GYNECOLOGIC ONCOLOGY APRIL 19 TH, 2018 Objectives Basic Cancer Statistics Discuss
ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป
 ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป Brachytherapy การร กษาด วยร งส ระยะใกล Insertion การสอดใส แร Implantation การฝ งแร Surface application การวางแร physical benefit of brachytherapy - very high dose of radiation
ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป Brachytherapy การร กษาด วยร งส ระยะใกล Insertion การสอดใส แร Implantation การฝ งแร Surface application การวางแร physical benefit of brachytherapy - very high dose of radiation
Algorithms for management of Cervical cancer
 Algithms f management of Cervical cancer Algithms f management of cervical cancer are based on existing protocols and guidelines within the ESGO comunity and prepared by ESGO Educational Committe as a
Algithms f management of Cervical cancer Algithms f management of cervical cancer are based on existing protocols and guidelines within the ESGO comunity and prepared by ESGO Educational Committe as a
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type)
") Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
Annual report of the Committee on Gynecologic Oncology, the Japan Society of Obstetrics and Gynecology
 bs_bs_banner doi:10.1111/jog.12596 J. Obstet. Gynaecol. Res. Vol. 41, No. 2: 167 177, February 2015 Annual report of the Committee on Gynecologic Oncology, the Japan Society of Obstetrics and Gynecology
bs_bs_banner doi:10.1111/jog.12596 J. Obstet. Gynaecol. Res. Vol. 41, No. 2: 167 177, February 2015 Annual report of the Committee on Gynecologic Oncology, the Japan Society of Obstetrics and Gynecology
PORTEC-4. Patient seqnr. Age at inclusion (years) Hospital:
 Hospital:") May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
17 th ESO-ESMO Masterclass in clinical Oncology
 17 th ESO-ESMO Masterclass in clinical Oncology Cervical and endometrial Cancer Cristiana Sessa IOSI Bellinzona, Switzerland Berlin, March 28 th, 2018 Presenter Disclosures None Cervical Cancer Estimated
17 th ESO-ESMO Masterclass in clinical Oncology Cervical and endometrial Cancer Cristiana Sessa IOSI Bellinzona, Switzerland Berlin, March 28 th, 2018 Presenter Disclosures None Cervical Cancer Estimated
3 cell types in the normal ovary
 Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors (neoplasms) 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal
Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors (neoplasms) 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal
Chemotherapy in Gynecologic Malignancies
 Chemotherapy in Gynecologic Malignancies Dr U.D.Bafna Professor & Head, Department of Gynecologic Oncology, Kidwai Memorial Institute of Oncology, Bangalore Chemotherapy in solid tumors is mainly adjuvant
Chemotherapy in Gynecologic Malignancies Dr U.D.Bafna Professor & Head, Department of Gynecologic Oncology, Kidwai Memorial Institute of Oncology, Bangalore Chemotherapy in solid tumors is mainly adjuvant
UICC TNM 8 th Edition Errata
 UICC TNM 8 th Edition Errata ions are in italics Head and Neck Tumours Pages 20, p27, p34, p38, p41, and p49 ly pn2a Metastasis in a single ipsilateral lymph node, less than 3cm in greatest dimension with
UICC TNM 8 th Edition Errata ions are in italics Head and Neck Tumours Pages 20, p27, p34, p38, p41, and p49 ly pn2a Metastasis in a single ipsilateral lymph node, less than 3cm in greatest dimension with
Vulva Cancer Histopathology Reporting Proforma
 Vulva Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Ethnicity Unknown AboriginalTorres
Vulva Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Ethnicity Unknown AboriginalTorres
Interactive Staging Bee
 Interactive Staging Bee ROBIN BILLET, MA, CTR GA/SC REGIONAL CONFERENCE NOVEMBER 6, 2018? Clinical Staging includes any information obtained about the extent of cancer obtained before initiation of treatment
Interactive Staging Bee ROBIN BILLET, MA, CTR GA/SC REGIONAL CONFERENCE NOVEMBER 6, 2018? Clinical Staging includes any information obtained about the extent of cancer obtained before initiation of treatment
Clinical Pathological Conference. Malignant Melanoma of the Vulva
 Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
MRI in Cervix and Endometrial Cancer
 28th Congress of the Hungarian Society of Radiologists RCR Session Budapest June 2016 MRI in Cervix and Endometrial Cancer DrSarah Swift St James s University Hospital Leeds, UK Objectives Cervix and endometrial
28th Congress of the Hungarian Society of Radiologists RCR Session Budapest June 2016 MRI in Cervix and Endometrial Cancer DrSarah Swift St James s University Hospital Leeds, UK Objectives Cervix and endometrial
Chapter 8 Adenocarcinoma
 Page 80 Chapter 8 Adenocarcinoma Overview In Japan, the proportion of squamous cell carcinoma among all cervical cancers has been declining every year. In a recent survey, non-squamous cell carcinoma accounted
Page 80 Chapter 8 Adenocarcinoma Overview In Japan, the proportion of squamous cell carcinoma among all cervical cancers has been declining every year. In a recent survey, non-squamous cell carcinoma accounted
H&E, IHC anti- Cytokeratin
 Cat No: OVC2281 - Ovary cancer tissue array Lot# Cores Size Cut Format QA/QC OVC228101 228 1.1mm 4um 12X19 H&E, IHC anti- Cytokeratin Recommended applications: For Research use only. RNA or protein ovary
Cat No: OVC2281 - Ovary cancer tissue array Lot# Cores Size Cut Format QA/QC OVC228101 228 1.1mm 4um 12X19 H&E, IHC anti- Cytokeratin Recommended applications: For Research use only. RNA or protein ovary
GCIG Rare Tumour Brainstorming Day
 GCIG Rare Tumour Brainstorming Day Relatively (Not So) Rare Tumours Adenocarcinoma of Cervix Keiichi Fujiwara, Ros Glasspool Benedicte Votan, Jim Paul Aim of the Day To develop at least one clinical trial
GCIG Rare Tumour Brainstorming Day Relatively (Not So) Rare Tumours Adenocarcinoma of Cervix Keiichi Fujiwara, Ros Glasspool Benedicte Votan, Jim Paul Aim of the Day To develop at least one clinical trial
Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES CASE 1: FEMALE REPRODUCTIVE
 Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES PHYSICAL EXAMINATION CASE 1: FEMALE REPRODUCTIVE 3/5 Patient presents through the emergency room with
Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES PHYSICAL EXAMINATION CASE 1: FEMALE REPRODUCTIVE 3/5 Patient presents through the emergency room with
Gynecologic Cancer InterGroup Cervix Cancer Research Network. Management of Cervical Cancer in Resource Limited Settings.
 Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Endometrial adenocarcinoma icd 10 code
 Endometrial adenocarcinoma icd 10 code Gogamz Menu Cancer of the endometrium, adenocarcinoma ;. (mucous membrane that lines the endometrial cavity). ICD - 10 -CM C54.1 is grouped within. ICD-10 -CM Diagnosis
Endometrial adenocarcinoma icd 10 code Gogamz Menu Cancer of the endometrium, adenocarcinoma ;. (mucous membrane that lines the endometrial cavity). ICD - 10 -CM C54.1 is grouped within. ICD-10 -CM Diagnosis
29 Cancer of the Uterine Corpus
 29 Cancer of the Uterine Corpus Robbert Soeters INTRODUCTION Malignancies affecting the uterine corpus are endometrial adenocarcinoma and uterine sarcomas. ENDOMETRIAL ADENOCARCINOMA Endometrial adenocarcinoma
29 Cancer of the Uterine Corpus Robbert Soeters INTRODUCTION Malignancies affecting the uterine corpus are endometrial adenocarcinoma and uterine sarcomas. ENDOMETRIAL ADENOCARCINOMA Endometrial adenocarcinoma
This protocol is intended to assist pathologists in providing
 Protocol for the Examination of Specimens From Patients With Carcinomas of the Endometrium A Basis for Checklists Steven G. Silverberg, MD, for the Members of the Cancer Committee, College of American
Protocol for the Examination of Specimens From Patients With Carcinomas of the Endometrium A Basis for Checklists Steven G. Silverberg, MD, for the Members of the Cancer Committee, College of American
What is endometrial cancer?
 Uterine cancer What is endometrial cancer? Endometrial cancer is the growth of abnormal cells in the lining of the uterus. The lining is called the endometrium. Endometrial cancer usually occurs in women
Uterine cancer What is endometrial cancer? Endometrial cancer is the growth of abnormal cells in the lining of the uterus. The lining is called the endometrium. Endometrial cancer usually occurs in women
Hitting the High Points Gynecologic Oncology Review
 Hitting the High Points is designed to cover exam-based material, from preinvasive neoplasms of the female genital tract to the presentation, diagnosis and treatment, including surgery, chemotherapy, and
Hitting the High Points is designed to cover exam-based material, from preinvasive neoplasms of the female genital tract to the presentation, diagnosis and treatment, including surgery, chemotherapy, and
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
Gestational Trophoblastic Disease
 J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse Gestational Trophoblastic Disease Partial or complete mole based on pathology, morphology and karyotype Pathology Complete mole Absent
J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse Gestational Trophoblastic Disease Partial or complete mole based on pathology, morphology and karyotype Pathology Complete mole Absent
Endometrial adenocarcinoma icd 10 code
 P ford residence southampton, ny Endometrial adenocarcinoma icd 10 code Jun 24, 2014. Billable Medical Code for Malignant Neoplasm of Corpus Uteri, Except Isthmus Diagnosis Code for Reimbursement Claim:
P ford residence southampton, ny Endometrial adenocarcinoma icd 10 code Jun 24, 2014. Billable Medical Code for Malignant Neoplasm of Corpus Uteri, Except Isthmus Diagnosis Code for Reimbursement Claim:
7 Mousa. Obada Zalat. Mohammad Badi
 7 Mousa Obada Zalat Mohammad Badi Tumors of the ovaries Last lecture we talked about surface epithelial tumors of the ovaries (the most common type). But there are many other types of tumors of germ cell
7 Mousa Obada Zalat Mohammad Badi Tumors of the ovaries Last lecture we talked about surface epithelial tumors of the ovaries (the most common type). But there are many other types of tumors of germ cell
Sarah Burton. Lead Gynae Oncology Nurse Specialist Cancer Care Cymru
 Sarah Burton Lead Gynae Oncology Nurse Specialist Cancer Care Cymru Gynaecological Cancers Cervical Cancers Risk factors Presentation Early sexual activity Multiple sexual partners Smoking Human Papiloma
Sarah Burton Lead Gynae Oncology Nurse Specialist Cancer Care Cymru Gynaecological Cancers Cervical Cancers Risk factors Presentation Early sexual activity Multiple sexual partners Smoking Human Papiloma
Index. B Bilateral salpingo-oophorectomy (BSO), 69
, 69") A Advanced stage endometrial cancer diagnosis, 92 lymph node metastasis, 92 multivariate analysis, 92 myometrial invasion, 92 prognostic factors FIGO stage, 94 histological grade, 94, 95 histologic cell
A Advanced stage endometrial cancer diagnosis, 92 lymph node metastasis, 92 multivariate analysis, 92 myometrial invasion, 92 prognostic factors FIGO stage, 94 histological grade, 94, 95 histologic cell
Gynecologic Cancers. What is Gynecologic Cancer. Who is at risk for GYN cancer? 3/1/2018 1
 What is Gynecologic Cancer Gynecologic Cancers Marge Ramsdell RN, MN, OCN Madigan Army Medical Center Any cancer that starts in a woman s reproductive organs Each GYN cancer is unique 5 main types Cervical
What is Gynecologic Cancer Gynecologic Cancers Marge Ramsdell RN, MN, OCN Madigan Army Medical Center Any cancer that starts in a woman s reproductive organs Each GYN cancer is unique 5 main types Cervical
Anatomy of the Female Reproductive System. Overview of Major GYN Cancer Characteristics. Multiple Primary and Histology Coding Rules
 GYN Neoplasms Anatomy of the Female Reproductive System Overview of Major GYN Cancer Characteristics Multiple Primary and Histology Coding Rules FIGO IGCS, AJCC TNM 7 th ed. and Summary Stage 2000 Collaborative
GYN Neoplasms Anatomy of the Female Reproductive System Overview of Major GYN Cancer Characteristics Multiple Primary and Histology Coding Rules FIGO IGCS, AJCC TNM 7 th ed. and Summary Stage 2000 Collaborative