Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors
|
|
|
- Howard Cole
- 5 years ago
- Views:
Transcription

1 Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Frédéric Bibeau, MD, PhD Pathology department Biopathology unit Institut du Cancer de Montpellier France

2 Quality and rules of a good pathology report Simple but rigourous
3 Useful histopronostic factors Early colorectal cancer (CRC)

4 Useful histopronostic factors Micrometastatic disease Adjuvant chemotherapy
5 Useful histopronostic factors Content - Tumour - Depth of invasion - Distant extension - Margins
6 Useful histopronostic factors - Tumour - Depth of invasion - Distant extension - Margins

7 Colorectal cancer (CRC): heterogeneous disease Different histologic types

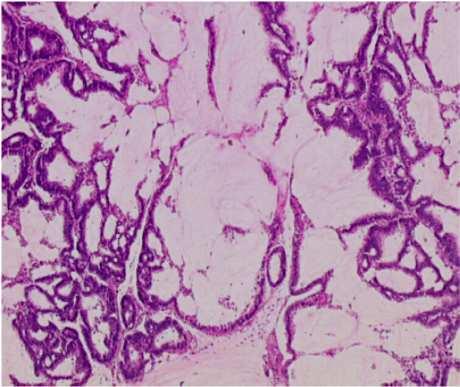





8 CRC histologic types 90% Lieberkühnian Mucinous micropapillary adenosquamous Signet ring cells Serrated Small cells Medullary Adenocarcinoma Carcinoma



9 MSI histologic features Tumour Microenvironment Mucinous Crohn-like reaction Signet ring cells Medullary Lymphocytic infiltrate CD3+
 modulation according to MSI")
10 CRC grading Low grade (well, moderatly differenciated) High grade (low, indifferenciated) modulation according to MSI status
11 Useful histopronostic factors - Tumour - Depth of invasion - Distant extension - Margins
12 ptnm classification MUCOSA Muscularis Muscosae --> SUB-MUCOSA MUSCULARIS SUB-SEROSA --> SEROSA --> pt Tis T1 T2 T3 T4 pn pm N0 : no positive lymph node (LN) N1 : 3 positive LN N2 : 4 positive LN M0 : No distant metastasis M1 : Distant metastasis TNM UICC th Classification Organe infiltration and / or visceral peritoneal perforation
13 ptnm classification MUCOSA Muscularis Muscosae --> SUB-MUCOSA MUSCULARIS SUB-SEROSA --> SEROSA --> pt Tis T1 T2 T3 T4 pn pm N0 : no positive lymph node (LN) N1 : 3 positive LN N2 : 4 positive LN M0 : No distant metastasis M1 : Distant metastasis TNM UICC th Classification Organe infiltration and / or visceral peritoneal perforation
14 Serosal involvement Gross examination +++

15 Serosal involvement pt4a 7 th TNM UICC 2009 classification Frankel et al. Mod Pathol 2015

16 Serosal involvement Deeper block levels pt4a 7 th TNM UICC 2009 classification Frankel et al. Mod Pathol 2015

17 Serosal involvement pt4a 7 th TNM UICC 2009 classification Frankel et al. Mod Pathol 2015

18 Invasion front Expansive Infiltrative Svrcek et al. Cancero Dig. 2012


19 Tumour budding Invasion front Wang LM, Am J Surg Path 2009



20 Tumour budding Which method? Lugli et al. Br J cancer 2012


21 Immune adaptative microenvironment Galon et al. Cancer Res 2007
22 Prognostic impact of immune response


23 Immune infiltrate evaluation Which method? Which markers? Intra and peri-tumoral? Linear quantification? Pagès et al., New Engl J Med 2005 Allard et al. Diagnostic Pathology 2014
24 Pronostic impact of the immune response - Treatment for particular stage II? - No treatment for certain stage III? Not enough data in 2016 (May 20 th )
")
25 Pronostic impact of the immune response - Treatment for particular stage II? - No treatment for certain stage III? But new data at 2016 ASCO (June 5 th )
26 Useful histopronostic factors - Tumour - Depth of invasion - Distant extension - Margins
27 ptnm classification MUCOSA Muscularis Muscosae --> SUB-MUCOSA MUSCULARIS SUB-SEROSA --> SEROSA --> pt Tis T1 T2 T3 T4 pn N0 : no positive lymph node (LN) N1 : 3 positive LN N2 : 4 positive LN N+ Organe infiltration and / or visceral peritoneal perforation pm M0 : No distant metastasis M1 : Distant metastasis Adjuvant chemotherapy TNM UICC th Classification
28 Distant extension: lymph nodes Recommendations > 12 But Goldstein et al. Am J Surg Pathol 2002

29 Distant extension: lymph nodes Gross examination +++ No magic number! More = better

30 Distant extension: lymph nodes Tougeron et al. Modern Path 2009.
31 Distant extension : tumour deposits Nx N0 N1 N2 N1a N1b N1c N2a N2b Statut ganglionnaire non évaluable No positive regional lymph node Metastase(s) in 1-3 regional lymph node(s) 1 positive lymph node 2-3 positive regional lymph node Tumour deposits, satellites, in the sub-serosa or peri-rectal or peri-colic non peritonised tissue, without regional metastatic lymph node 4 or more positive regional lymph nodes 4-6 regional positive lymph nodes 7 regional positive lymph nodes TNM UICC th Classification

32 Distant extension : tumour deposits TNM 5 th edition TNM 6 th edition TNM 7 th edition >3 mm Lymph node Smooth shape Lymph node No residual lymph node Tumour deposit Frankel et al. Mod Pathol 2015


33 Distant extension : tumour deposits Pericolic or -rectal tissu location Puppa et al. Modern Pathol 2007
34 Impact of «tumour deposits» (N1c) P< Jin et al. Am J Surg Path 2014
35 Impact of «tumour deposits» (N1c) P= Jin et al. Am J Surg Path 2014
36 Distant extension : tumour deposits Recommendations for interprétation (F.A.Q*) - N1c only if negative lymph node - No N1c if positive lymph node - Do not add tumour deposits to positive lymph node - Do not modify T stage *Frequently Asked Question
37 Distant extension : tumour deposits Nx N0 N1 N2 N1a N1b N1c N2a N2b Statut ganglionnaire non évaluable No positive regional lymph node Metastase(s) in 1-3 regional lymph node(s) 1 positive lymph node 2-3 positive regional lymph node Tumour deposits, satellites, in the sub-serosa or peri-rectal or peri-colic non peritonised tissu without regional metastatic lymph node 4 or more positive regional lymph nodes 4-6 regional positive lymph nodes 7 regional positive lymph nodes TNM UICC th Classification Clinical trials



38 Distant extension : VELIPI* Lymphatic invasion Venous invasion Perineural invasion Harris et al, Am J Surg Path 2008 Mori et al. Histopathology 2009 Liebig et al J Clin Oncol 2010 *Venous emboli and lymphatic and perineural invasion


39 Extra-mural venous invasion 30%: frequent underestimation? Nagtegaal et al. histopathology 2015
40 Perineural invasion OS DFS CSS Knijn et al. Am J Surg Path 2015
41 Useful histopronostic factors - Tumour - Depth of invasion - Distant extension - Margins

42 Margins Distal ans proximal very rarely positive

43 Useful histopronostic factors - Tumour - Depth of invasion - Distant extension - Margins
 Immunohistochemistry Molecular biology")

44 Molecular profile Microsatellite instability (15%) Immunohistochemistry Molecular biology Normal DNA MSI tumour Less or supplementary nucleotides Favorable prognosis in CCR stage II
45 Molecular profile Impact of KRAS et BRAF mutations Poor prognosis in stage III CRC (MSS)* Not used as prognostic factors in 2016 Stratification for clinical trials? MSI, RAS, BRAF status for all CRC, tomorrow? *Taieb et al JAMA Oncol 2016
46 Useful histopronostic factors for treatment Early CRC in ptnm - Grade - VELIPI - MSI
47 Useful histopronostic factors for treatment Early CRC in 2016 Stage III - ptnm N+ (including N1c= tumour dep.) adjuvant CT - Grade - VELIPI - MSI
48 Useful histopronostic factors for treatment Early CRC in 2016 Stage II - ptnm N0 pt4 (serosa +), <12 N - Grade high (poor differenciation) - VELIPI + - MSI - Adjuvant CT (Multidisciplinary team discussion)

 -")


49 Pathology report key elements OMS Histologic type Differenciation (Grade) Extension - Tumour (pt) - Lymph node (pn) Margins - Distal/proximal - Circumferential (Rectum) Lymphatics Veins Nerves Vasculo-lymphatic and perineural invasions
50 Translationnal research
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors
 Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Pr Frédéric Bibeau, MD, PhD Head, Pathology department CHU de Caen, Normandy University, France ESMO preceptorship,
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Pr Frédéric Bibeau, MD, PhD Head, Pathology department CHU de Caen, Normandy University, France ESMO preceptorship,
Microsatellite instability and other molecular markers: how useful are they?
 Microsatellite instability and other molecular markers: how useful are they? Pr Frédéric Bibeau, MD, PhD Head, Pathology department CHU de Caen, Normandy University, France ESMO preceptorship, Barcelona,
Microsatellite instability and other molecular markers: how useful are they? Pr Frédéric Bibeau, MD, PhD Head, Pathology department CHU de Caen, Normandy University, France ESMO preceptorship, Barcelona,
WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER?
 CANCER STAGING TNM and prognosis in CRC WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER? Alessandro Lugli, MD Institute of Pathology University of Bern Switzerland Maastricht, June 19
CANCER STAGING TNM and prognosis in CRC WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER? Alessandro Lugli, MD Institute of Pathology University of Bern Switzerland Maastricht, June 19
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Microsatellite instability and other molecular markers: how usefulare they? Pr Frédéric Bibeau, MD, PhD Pathology Department CHU de Caen France
 Microsatellite instability and other molecular markers: how usefulare they? Pr Frédéric Bibeau, MD, PhD Pathology Department CHU de Caen France Content - Colorectal cancer context - CRC molecular classification
Microsatellite instability and other molecular markers: how usefulare they? Pr Frédéric Bibeau, MD, PhD Pathology Department CHU de Caen France Content - Colorectal cancer context - CRC molecular classification
Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Disclosures. Outline. What IS tumor budding?? Tumor Budding in Colorectal Carcinoma: What, Why, and How. I have nothing to disclose
 Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
What Pathology can tell us in the approach of localized colorectal cancer
 What Pathology can tell us in the approach of localized colorectal cancer A/Prof Tony Lim Kiat Hon Department of Anatomical Pathology Singapore General Hospital ESMO 2017 Singapore Nov 1 2 Do we still
What Pathology can tell us in the approach of localized colorectal cancer A/Prof Tony Lim Kiat Hon Department of Anatomical Pathology Singapore General Hospital ESMO 2017 Singapore Nov 1 2 Do we still
Update on Colorectal Cancer: Integrating the Host Immune Response 3 rd Emirates Surgical Pathology Conference 15 December 2017 Dubai, UAE
 Update on Colorectal Cancer: Integrating the Host Immune Response 3 rd Emirates Surgical Pathology Conference 15 December 2017 Dubai, UAE Martine McManus, MD, FCAP Pathology & Laboratory Medicine Institute
Update on Colorectal Cancer: Integrating the Host Immune Response 3 rd Emirates Surgical Pathology Conference 15 December 2017 Dubai, UAE Martine McManus, MD, FCAP Pathology & Laboratory Medicine Institute
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Rectal Cancer Cookbook Update. A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux
 Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
Effect of Tumor Deposits on Overall Survival in Colorectal Cancer Patients with Regional Lymph Node Metastases
 J Rural Med 2014; 9(1): 20 26 Original article Effect of Tumor Deposits on Overall Survival in Colorectal Cancer Patients with Regional Lymph Node Metastases Eiichi Yabata, Masaru Udagawa and Hiroyuki
J Rural Med 2014; 9(1): 20 26 Original article Effect of Tumor Deposits on Overall Survival in Colorectal Cancer Patients with Regional Lymph Node Metastases Eiichi Yabata, Masaru Udagawa and Hiroyuki
Histo-prognostic factors what histopathology has to offer for clinical decision making
 Histo-prognostic factors what histopathology has to offer for clinical decision making Daniela E. Aust Institute for Pathology, University Hospital Dresden, Germany Center for Molecular Tumor Diagnostics
Histo-prognostic factors what histopathology has to offer for clinical decision making Daniela E. Aust Institute for Pathology, University Hospital Dresden, Germany Center for Molecular Tumor Diagnostics
Colorectal cancer Chapelle, J Clin Oncol, 2010
 Colorectal cancer Chapelle, J Clin Oncol, 2010 Early-Stage Colorectal cancer: Microsatellite instability, multigene assay & emerging molecular strategy Asit Paul, MD, PhD 11/24/15 Mr. X: A 50 yo asymptomatic
Colorectal cancer Chapelle, J Clin Oncol, 2010 Early-Stage Colorectal cancer: Microsatellite instability, multigene assay & emerging molecular strategy Asit Paul, MD, PhD 11/24/15 Mr. X: A 50 yo asymptomatic
High risk stage II colon cancer
 High risk stage II colon cancer Joel Gingerich, MD, FRCPC Assistant Professor Medical Oncologist University of Manitoba CancerCare Manitoba Disclaimer No conflict of interests 16 October 2010 Overview
High risk stage II colon cancer Joel Gingerich, MD, FRCPC Assistant Professor Medical Oncologist University of Manitoba CancerCare Manitoba Disclaimer No conflict of interests 16 October 2010 Overview
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Please Silence Your Cell Phones. Thank You
 Please Silence Your Cell Phones Thank You TUMOR BUDDING IN PRE OPERATIVE BIOPSIES AND RESECTIONS Alessandro Lugli, MD Institute of Pathology and Translational Research Unit (TRU) University of Bern Bern,
Please Silence Your Cell Phones Thank You TUMOR BUDDING IN PRE OPERATIVE BIOPSIES AND RESECTIONS Alessandro Lugli, MD Institute of Pathology and Translational Research Unit (TRU) University of Bern Bern,
Diagnostic Difficulties Encountered Among Colorectal Polyps
 Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Colorectal Carcinoma Reporting in 2009
 Colorectal Carcinoma Reporting in 2009 Overview Colorectal carcinoma- new and confusing AJCC TNM issues Wendy L. Frankel, M.D. Vice-Chair and Director of AP Department of Pathology The Ohio State University
Colorectal Carcinoma Reporting in 2009 Overview Colorectal carcinoma- new and confusing AJCC TNM issues Wendy L. Frankel, M.D. Vice-Chair and Director of AP Department of Pathology The Ohio State University
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Gastric Cancer Staging AJCC eighth edition. Duncan McLeod Westmead Hospital, NSW
 Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Formula One Study. Assessment criteria of pathological parameters. Ver.2. UK Japan Joint Study for Risk Factors of Lymph Node
 APPENDIX 01: Assessment criteria Formula One Study UK Japan Joint Study for Risk Factors of Lymph Node Metastasis in Submucosal Invasive (pt1) Colorectal Cancer Assessment criteria of pathological parameters
APPENDIX 01: Assessment criteria Formula One Study UK Japan Joint Study for Risk Factors of Lymph Node Metastasis in Submucosal Invasive (pt1) Colorectal Cancer Assessment criteria of pathological parameters
Nodal staging of colorectal cancer, TNM and practical issues
 Nodal staging of colorectal cancer, TNM and practical issues Gábor Cserni 1. Bács-Kiskun County Teaching Hospital, Kecskemét 2. University of Szeged, Szeged Different staging systems: A,B,C,(D) Same letters
Nodal staging of colorectal cancer, TNM and practical issues Gábor Cserni 1. Bács-Kiskun County Teaching Hospital, Kecskemét 2. University of Szeged, Szeged Different staging systems: A,B,C,(D) Same letters
Adjuvant/neoadjuvant systemic treatment of colorectal cancer
 5th ESO-ESMO Eastern Europe and Balkan Region Masterclass in Medical Oncology Belgrade, June 19 th 2018 Adjuvant/neoadjuvant systemic treatment of colorectal cancer Carlotta Antoniotti Polo Oncologico
5th ESO-ESMO Eastern Europe and Balkan Region Masterclass in Medical Oncology Belgrade, June 19 th 2018 Adjuvant/neoadjuvant systemic treatment of colorectal cancer Carlotta Antoniotti Polo Oncologico
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Signet-Ring Cell Carcinoma of the Colon: A Case Report and Review of the Literature
 Published online: November 4, 2015 2015 The Author(s) Published by S. Karger AG, Basel 1662 6575/15/0083 0466$39.50/0 This article is licensed under the Creative Commons Attribution-NonCommercial 4.0 International
Published online: November 4, 2015 2015 The Author(s) Published by S. Karger AG, Basel 1662 6575/15/0083 0466$39.50/0 This article is licensed under the Creative Commons Attribution-NonCommercial 4.0 International
Mismatch repair status, inflammation and outcome in patients with primary operable colorectal cancer
 Mismatch repair status, inflammation and outcome in patients with primary operable colorectal cancer Park JH, Powell AG, Roxburgh CSD, Richards CH, Horgan PG, McMillan DC, Edwards J James Park Clinical
Mismatch repair status, inflammation and outcome in patients with primary operable colorectal cancer Park JH, Powell AG, Roxburgh CSD, Richards CH, Horgan PG, McMillan DC, Edwards J James Park Clinical
Overview. Collecting Cancer Data: Colon 11/5/2009. Collecting Cancer Data: NAACCR Webinar Series 1. Agenda NAACCR WEBINAR SERIES
 Collecting Cancer Data: Colon 11/5/2009 Collecting Cancer Data: Colon/Rectum/Appendix NAACCR 2009 2010 WEBINAR SERIES Agenda Overview Treatment MP/H Rules CSv2 2 Overview Colon/Rectum/Appendix 2009 2010
Collecting Cancer Data: Colon 11/5/2009 Collecting Cancer Data: Colon/Rectum/Appendix NAACCR 2009 2010 WEBINAR SERIES Agenda Overview Treatment MP/H Rules CSv2 2 Overview Colon/Rectum/Appendix 2009 2010
COLORECTAL CANCER: PROGNOSTIC VALUES
 & COLORECTAL CANCER: PROGNOSTIC VALUES Suzana Manxhuka-Kerliu¹*, Skender Telaku², Halil Ahmetaj³, Arijeta Baruti¹, Sadushe Loxha¹, Agron Kerliu³ ¹ Institute of Pathology, Faculty of Medicine, University
& COLORECTAL CANCER: PROGNOSTIC VALUES Suzana Manxhuka-Kerliu¹*, Skender Telaku², Halil Ahmetaj³, Arijeta Baruti¹, Sadushe Loxha¹, Agron Kerliu³ ¹ Institute of Pathology, Faculty of Medicine, University
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma
 Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Early (and not so early) colorectal cancer: The pathologist s point of view
 colorectal cancer: The pathologist s point of view") Early (and not so early) colorectal cancer: The pathologist s point of view Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Disclosure slide I Member of advisory board for
Early (and not so early) colorectal cancer: The pathologist s point of view Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Disclosure slide I Member of advisory board for
Peritoneal Involvement in Stage II Colon Cancer
 Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
NUMERATOR: Reports that include the pt category, the pn category and the histologic grade
 Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Ritu Nayar, MD Professor and Vice Chair of Pathology Northwestern University, Feinberg School of Medicine Chicago, IL
 Ritu Nayar, MD Professor and Vice Chair of Pathology Northwestern University, Feinberg School of Medicine Chicago, IL email: r-nayar@northwestern.edu Nothing to disclose College of American Pathologists
Ritu Nayar, MD Professor and Vice Chair of Pathology Northwestern University, Feinberg School of Medicine Chicago, IL email: r-nayar@northwestern.edu Nothing to disclose College of American Pathologists
NUMERATOR: Reports that include the pt category, the pn category and the histologic grade
 Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Molecular markers in colorectal cancer. Wolfram Jochum
 Molecular markers in colorectal cancer Wolfram Jochum Biomarkers in cancer Patient characteristics Tumor tissue Normal cells Serum Body fluids Predisposition Diagnostic marker Specific diagnosis Prognostic
Molecular markers in colorectal cancer Wolfram Jochum Biomarkers in cancer Patient characteristics Tumor tissue Normal cells Serum Body fluids Predisposition Diagnostic marker Specific diagnosis Prognostic
Disclosure slide I Member of advisory board for AMGEN, ROCHE, BOEHRINGER I Speaker honoraria from FALK Pharma, Pfizer, Lilly and ROCHE I Third party f
 Early (and not so early) colorectal cancer: The pathologist s point of view Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Disclosure slide I Member of advisory board for
Early (and not so early) colorectal cancer: The pathologist s point of view Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Disclosure slide I Member of advisory board for
AJCC Cancer Staging 8 th Edition
 AJCC Cancer Staging 8 th Edition Colon and Rectal Cancer Staging Update Webinar George J Chang, MD, MS Deputy Chair, Department of Surgical Oncology Chief, Colon and Rectal Surgery Professor of Surgical
AJCC Cancer Staging 8 th Edition Colon and Rectal Cancer Staging Update Webinar George J Chang, MD, MS Deputy Chair, Department of Surgical Oncology Chief, Colon and Rectal Surgery Professor of Surgical
The pathological phenotype of colon cancer with microsatellite instability
 Dan Med J 63/2 February 2016 danish medical JOURNAL 1 The pathological phenotype of colon cancer with microsatellite instability Helene Schou Andersen 1, 2, Claus Anders Bertelsen 1, Rikke Henriksen 1,
Dan Med J 63/2 February 2016 danish medical JOURNAL 1 The pathological phenotype of colon cancer with microsatellite instability Helene Schou Andersen 1, 2, Claus Anders Bertelsen 1, Rikke Henriksen 1,
L impatto dell imaging sulla definizione della strategia terapeutica
 GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
05/07/2018. Organisation. The English screening programme what is happening? Organisation. Bowel cancer screening in the UK is:
 Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
2014/2015 FCDS Educational Webcast Series
 2014/2015 FCDS Educational Webcast Series February 19, 2015 Steven Peace, CTR 2015 Update; Background, Anatomy, Risk Factors, Screening Guidelines, MPH Rules Review AJCC TNM 7 th ed, SS2000, CSv02.05 and
2014/2015 FCDS Educational Webcast Series February 19, 2015 Steven Peace, CTR 2015 Update; Background, Anatomy, Risk Factors, Screening Guidelines, MPH Rules Review AJCC TNM 7 th ed, SS2000, CSv02.05 and
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Protocol for the Examination of Specimens from Patients with Primary Carcinoma of the Colon and Rectum
 Protocol for the Examination of Specimens from Patients with Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. This modified NB
Protocol for the Examination of Specimens from Patients with Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. This modified NB
Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE
 Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE Neoadjuvant Chemotherapy Indications: Management of locally advanced invasive breast cancers including inflammatory breast
Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE Neoadjuvant Chemotherapy Indications: Management of locally advanced invasive breast cancers including inflammatory breast
Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum
 Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
INMUNOTERAPIA EN CANCER COLORRECTAL METASTASICO. CCRm MSI-H NUEVO ESTANDAR EN PRIMERA LINEA Y/O PRETRATADOS?
 INMUNOTERAPIA EN CANCER COLORRECTAL METASTASICO CCRm MSI-H NUEVO ESTANDAR EN PRIMERA LINEA Y/O PRETRATADOS? V. Alonso Servicio de Oncologia Medica H. U. Miguel Servet Zaragoza MSI-H mcrc Clinical and Pathological
INMUNOTERAPIA EN CANCER COLORRECTAL METASTASICO CCRm MSI-H NUEVO ESTANDAR EN PRIMERA LINEA Y/O PRETRATADOS? V. Alonso Servicio de Oncologia Medica H. U. Miguel Servet Zaragoza MSI-H mcrc Clinical and Pathological
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER. Guidelines for the assessment of mismatch. Colorectal Cancer
 COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer March 2017 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer March 2017 1 Background Mismatch repair (MMR) deficiency is seen in approximately
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM
 OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ]
![Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ]](/thumbs/82/86264030.jpg "Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ]") Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ] CS Tumor Size 000 No mass/tumor found 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters or larger 990 Microscopic
Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ] CS Tumor Size 000 No mass/tumor found 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters or larger 990 Microscopic
COLORECTAL CANCER STAGING in 2010
 COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER. Guidelines for the assessment of mismatch. Colorectal Cancer
 COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer January 2015 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer January 2015 1 Background Mismatch repair (MMR) deficiency is seen in approximately
SEER EOD AND SUMMARY STAGE ABSTRACTORS TRAINING
 SEER EOD AND SUMMARY STAGE ABSTRACTORS TRAINING OVERVIEW What is SEER EOD Ambiguous Terminology General Guidelines EOD Primary Tumor EOD Regional Nodes EOD Mets Site Specific Data Items (SSDI) SEER Summary
SEER EOD AND SUMMARY STAGE ABSTRACTORS TRAINING OVERVIEW What is SEER EOD Ambiguous Terminology General Guidelines EOD Primary Tumor EOD Regional Nodes EOD Mets Site Specific Data Items (SSDI) SEER Summary
A Comparative Study of Rectal and Colonic Carcinoma: Demographic, Pathologic and TNM Staging Analysis
 Journal of the Egyptian Nat. Cancer Inst., Vol. 18, 3, September: 2-263, 2006 A Comparative Study of Rectal and ic Carcinoma: Demographic, Pathologic and TNM Staging Analysis TAREK N. EL-BOLKAINY, M.D.;
Journal of the Egyptian Nat. Cancer Inst., Vol. 18, 3, September: 2-263, 2006 A Comparative Study of Rectal and ic Carcinoma: Demographic, Pathologic and TNM Staging Analysis TAREK N. EL-BOLKAINY, M.D.;
Management of pt1 polyps. Maria Pellise
 Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Serrated Polyps and a Classification of Colorectal Cancer
 Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum
 Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
Gastric Cancer in a Young Postpartum Female. Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012
 Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Staging for Residents, Nurses, and Multidisciplinary Health Care Team
 Staging for Residents, Nurses, and Multidisciplinary Health Care Team Donna M. Gress, RHIT, CTR Validating science. Improving patient care. Learning Objectives Introduce the concept and history of stage
Staging for Residents, Nurses, and Multidisciplinary Health Care Team Donna M. Gress, RHIT, CTR Validating science. Improving patient care. Learning Objectives Introduce the concept and history of stage
The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
 30 th Congress of the European Society of Pathology Tuesday, September 11, 2018 The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
30 th Congress of the European Society of Pathology Tuesday, September 11, 2018 The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
Carcinoma of the Renal Pelvis and Ureter Histopathology
 Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer
 status in Colorectal Cancer") Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer Start date: May 2015 Review date: April 2018 1 Background Mismatch repair (MMR) deficiency is seen in approximately 15%
Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer Start date: May 2015 Review date: April 2018 1 Background Mismatch repair (MMR) deficiency is seen in approximately 15%
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do?
 Exercise 1 Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do? : 1. I mention both categories that are in consideration, e.g. pt1-2 2. I classify as
Exercise 1 Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do? : 1. I mention both categories that are in consideration, e.g. pt1-2 2. I classify as
3/23/2017. Disclosure of Relevant Financial Relationships. Pathologic Staging Updates in Lung Cancer T STAGE OUTLINE SURVIVAL ACCORDING TO SIZE ONLY
 Pathologic Staging Updates in Lung Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
Pathologic Staging Updates in Lung Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
ESD for EGC with undifferentiated histology
 ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
Multiple localized metachronous recurrences in a patient of colon cancer and therapeutic controversies in stage II colon cancer
 Case Report Multiple localized metachronous recurrences in a patient of colon cancer and therapeutic controversies in stage II colon cancer Vijai Simha, Rakesh Kapoor, Saniya Sharma Post Graduate Institute
Case Report Multiple localized metachronous recurrences in a patient of colon cancer and therapeutic controversies in stage II colon cancer Vijai Simha, Rakesh Kapoor, Saniya Sharma Post Graduate Institute
CHAPTER 7 Concluding remarks and implications for further research
 CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
Studies of Squamous Cell Carcinoma of the Tongue (TSCC), with Focus on Histological Factors
, with Focus on Histological Factors") Studies of Squamous Cell Carcinoma of the Tongue (TSCC), with Focus on Histological Factors Oskar Jonsson Filip Papic Supervised by Karin Nylander, professor Department of Medical Biosciences Umeå University.
Studies of Squamous Cell Carcinoma of the Tongue (TSCC), with Focus on Histological Factors Oskar Jonsson Filip Papic Supervised by Karin Nylander, professor Department of Medical Biosciences Umeå University.
Protocol for the Examination of Specimens from Patients with Primary Carcinomas of the Colon and Rectum
 Protocol for the Examination of Specimens from Patients with Primary Carcinomas of the Colon and Rectum Well differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Protocol for the Examination of Specimens from Patients with Primary Carcinomas of the Colon and Rectum Well differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Esophageal cancer: Biology, natural history, staging and therapeutic options
 EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Colorectal cancer: pathology
 UK NEQAS for Molecular Pathology Colorectal cancer: pathology Nick West Pathology & Tumour Biology May 2013 Colorectal cancer (CRC) 40,695 new cases in 2010 15,708 deaths Management of CRC Surgery Main
UK NEQAS for Molecular Pathology Colorectal cancer: pathology Nick West Pathology & Tumour Biology May 2013 Colorectal cancer (CRC) 40,695 new cases in 2010 15,708 deaths Management of CRC Surgery Main
Primary tumor with synchronous metastases
 Metastatic colorectal cancer: special clinical situations Primary tumor with synchronous metastases Stefan Heinrich & Hauke Lang Department of General, Visceral and Transplantation Surgery University Hospital
Metastatic colorectal cancer: special clinical situations Primary tumor with synchronous metastases Stefan Heinrich & Hauke Lang Department of General, Visceral and Transplantation Surgery University Hospital
TREATMENT OF PERITONEAL COLORECTAL CARCINOMATOSIS
 TREATMENT OF PERITONEAL COLORECTAL CARCINOMATOSIS Anna Lepistö, MD, PhD Department of Colorectal Surgery, Abdominal Center, Helsinki University Hospital Incidence, prevalence and risk factors for peritoneal
TREATMENT OF PERITONEAL COLORECTAL CARCINOMATOSIS Anna Lepistö, MD, PhD Department of Colorectal Surgery, Abdominal Center, Helsinki University Hospital Incidence, prevalence and risk factors for peritoneal
Ramya Thota 1, Xiang Fang 2, Shanmuga Subbiah 3. Introduction
 Original Article Clinicopathological features and survival outcomes of primary signet ring cell and mucinous adenocarcinoma of colon: retrospective analysis of VACCR database Ramya Thota 1, Xiang Fang
Original Article Clinicopathological features and survival outcomes of primary signet ring cell and mucinous adenocarcinoma of colon: retrospective analysis of VACCR database Ramya Thota 1, Xiang Fang
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
Should we still be performing IHC on all sentinel nodes?
 Miami Breast Cancer Conference 31 st Annual Conference March 8, 2014 Should we still be performing IHC on all sentinel nodes? Donald L. Weaver, MD Professor of Pathology University of Vermont USA Miami
Miami Breast Cancer Conference 31 st Annual Conference March 8, 2014 Should we still be performing IHC on all sentinel nodes? Donald L. Weaver, MD Professor of Pathology University of Vermont USA Miami
Handling & Grossing of Colo-rectal Specimens for Tumours. for Medical Officers in Pathology
 Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Xiang Hu*, Liang Cao*, Yi Yu. Introduction
 Original Article Prognostic prediction in gastric cancer patients without serosal invasion: comparative study between UICC 7 th edition and JCGS 13 th edition N-classification systems Xiang Hu*, Liang
Original Article Prognostic prediction in gastric cancer patients without serosal invasion: comparative study between UICC 7 th edition and JCGS 13 th edition N-classification systems Xiang Hu*, Liang
Short and longterm outcomes after endoscopic resection of malignant polyps.
 Short and longterm outcomes after endoscopic resection of malignant polyps. Short and longterm outcomes High risk features Lymph node metastasis Lymph node metastases sm1 sm2 sm3 Son 2008 3.1 % 14.9% 25.0
Short and longterm outcomes after endoscopic resection of malignant polyps. Short and longterm outcomes High risk features Lymph node metastasis Lymph node metastases sm1 sm2 sm3 Son 2008 3.1 % 14.9% 25.0
Pathohistological Assessment of the Circular Margin of Resection During Total Mesorectal Excision, Conducted on The Malignant Formations of the Rectum
 International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment
International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment