Diagnostic Difficulties Encountered Among Colorectal Polyps
|
|
|
- Daniela Horn
- 5 years ago
- Views:
Transcription
1 Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical College, New York, NY Case 1 Geneticist colleague I had my first colonoscopy yesterday upon turning 50 last week (I know I don t look a day over 49) Three polyps removed 0.7 cm polyp in rectosigmoid colon 0.5 cm flat lesion in mid transverse colon 0.5 cm flat lesion in descending colon No family history of cancer 1






2 Polyps of Distal Colon Descending colon Rectosigmoid colon Mid-Transverse Colon Polyp 2
 tubular adenomas of the distal colon One 5 mm non-dysplastic serrated polyp of the transverse colon Management")

3 Summary of Findings Two small (<1.0 cm) tubular adenomas of the distal colon One 5 mm non-dysplastic serrated polyp of the transverse colon Management dictated by tubular adenomas, so transverse colon polyp is mostly irrelevant.but what do we call the serrated polyp? Classification of Serrated Polyps Yes Is Dysplasia Present? No Serrated Adenoma Sessile Serrated Polyp with Dysplasia Hyperplastic Polyp Sessile Serrated Polyp Complete removal, followed similar to tubular and villous adenomas 3

: 65-81.")

 Atypical")
4 Hyperplastic Polyps Microvesicular Goblet cell rich -Small - More common in distal colon Mucin-poor Torlakovic, et al. Am J Surg Pathol 2003; 27(1): Sessile Serrated Polyp/Adenoma More common among women More common among older patients Predilection for abdominal colon, proximal to splenic flexure May be large (>1 cm) Atypical features not seen in hyperplastic polyps 4



5 Sessile Serrated Polyp/Adenoma Adherent mucus cap Mostly flat or thickened fold Sessile Serrated Polyp/Adenoma Expanded mucosa reflects elongated crypts 5





6 Sessile Serrated Polyp/Adenoma Dilated crypts flatten on muscularis mucosae and show lateral branching Non-Dysplastic Serrated Polyps Hyperplastic polyp Sessile serrated polyp 6




7 Proliferation in Serrated Polyps Hyperplastic polyp Sessile serrated polyp Symmetric proliferative zone Asymmetric proliferative zone Sessile Serrated Polyp/Adenoma Prevalence 2% of colonoscopy patients in general population 8% of colonoscopy patients in general population when evaluated by experienced gastroenterologist 20% of non-dysplastic serrated polyps in pathology material Payne, et al. Gastroenterol Hepatol 2014; 12:
 Rex, et al. Am J Gastroenterol 2012; 107: 1315-1329.")
8 Sessile Serrated Polyp with Dysplasia Mixed Adenomatous/Hyperplastic Polyp Non-dysplastic epithelium Dysplasia Non-Dysplastic Serrated Polyps Cancer Risk Number Few Many Size Small Large Type Hyperplastic polyp Sessile serrated polyp Location Left Right Increasing cancer risk (7% at 5 years in serrated polyposis syndrome) Rex, et al. Am J Gastroenterol 2012; 107:
 Small (<5 mm) Molecular Features Ki-67")
 Yes Yes MUC6 (pyloric gland mucin) Common (53-90%) Occasional (17-27%)")
 Common (~80%) CIMP high Common (~75%) Common (33-50%) Partial loss of MLH-1 staining Common")
9 Subclassifying Serrated Polyps Sessile Serrated Polyp Microvesicular Hyperplastic Polyp Clinical Features Location Proximal Distal Size Large (>1 cm) Small (<5 mm) Molecular Features Ki-67 distribution (proliferation) Abnormal Normal MUC2 (colonic goblet cell mucin) Yes Yes MUC5AC (gastric foveolar cell mucin) Yes Yes MUC6 (pyloric gland mucin) Common (53-90%) Occasional (17-27%) Annexin A10 Common (100%) Common (>50%) KRAS mutation Infrequent Infrequent BRAF mutation Common (~80%) Common (~80%) CIMP high Common (~75%) Common (33-50%) Partial loss of MLH-1 staining Common Occasional MSI-H No No 9


10 We recommend that a single unequivocal architecturally distorted, dilated, and/or horizontally branched crypt, particularly if it is associated with inverted maturation, is sufficient for a diagnosis of SSA/P. Clinical recommendations made here are considered strong by the panel, but are supported by low quality or very low quality evidence, and are likely to change when higher quality evidence becomes available. Rex, et al. Am J Gastroenterol 2012; 107: Sessile Serrated Polyp Goals of Detection Identify a potential precursor to sporadic colon cancers with MSI-H Usually proximal colon of older women How frequently do we see sporadic MSI-H cancers in rectum? Uncommon (we have not had a case yet, despite universal MSI testing for several years) No prospective data suggesting a single abnormal crypt is important 10
11 Take Home Points Most non-dysplastic serrated polyps are easily classified Polyps distal to splenic flexure are usually hyperplastic Proximal colonic lesions are sessile serrated polyps Difficult polyps with a few dilated crypts I don t make a diagnosis of sessile serrated polyp in the rectum, unless the findings are unequivocal We aren t trying to prevent rectal cancer Hyperplastic polyp with atypical features is difficult to defend in the ascending colon Biologically important polyps are likely the minority (larger than 1 cm, proximal to splenic flexure) Case 2 50-year old man with family history of colon cancer Mother had rectal cancer at age 60 Endoscopy revealed two polyps in ascending colon Small nodule that proved to be a prominent lymphoid aggregate Large non-bleeding sessile polyp Received fragmented polypectomy specimen 11


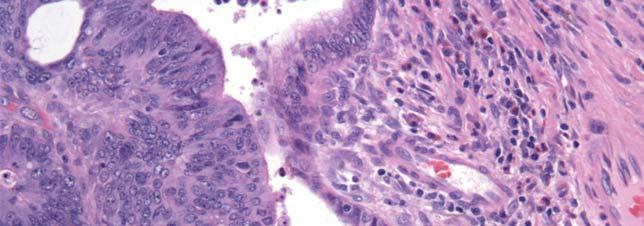
12 Histologic Features Histologic Features 12
13 Histologic Features Is that still in the mucosa? Histologic Features What about this? Is the tumor in the muscularis mucosae, or through it? 13
14 Summary of Findings Epithelial neoplasm with high-grade dysplasia and infiltrating cancer cells Location of infiltrating component is not entirely clear (intramucosal carcinoma vs. invasive adenocarcinoma) Infiltrating tumor cells have high-grade cytologic atypia Signet rings cells are present Diagnostic Considerations Invasive adenocarcinoma, high-grade, with signet ring cells Intramucosal adenocarcinoma with signet ring cells (ptis) Are these two situations equivalent (i.e. are signet ring cells bad, even if they are limited to the mucosa)? 14



: 1882-1886.")
15 Intramucosal High-Grade Carcinoma 15 patients 7 had no endoscopic recurrence or resection 7 underwent resection after polypectomy 5 with no lymph node metastases or residual disease 1 with a second carcinoma in resection specimen (intramucosal lesion, presumed metastasis) 1 with perianal Paget disease Polypectomy adequate therapy for lesions confined to muscularis mucosae Lewin, et al. Am J Surg Pathol 2007; 31(12): High-Grade Intramucosal Carcinoma 15
16 On High-Grade Intramucosal Carcinoma Be careful Cancer in the mucosa does not elicit desmoplasia, even if it is present in the submucosa or deeper wall I generally don t make a diagnosis of intramucosal carcinoma unless I have the entire lesion (i.e. polypectomy) If everyone is confident that disease is confined to mucosa, additional surgery (colectomy) may not be necessary Diagnosis Invasive adenocarcinoma, arising in a tubulovillous adenoma Superficial fragments of adenocarcinoma associated with an adenoma probably ok as alternate diagnosis Once we ve decided the patient has cancer, are we done? 16


17 Histologic Risk Factors in Malignant Polyps Feature Residual Disease Recurrent Disease Lymph Node Metastases Hematogenous Metastases Mortality Resection Margin Positive 30% 17% 7% 9% 8% Negative 3% 1% 9% 1% 1% Odds Ratio Poor Differentiation Present 18% 0% 23% 20% 15% Absent 9% 0% 7% 3% 9% Odds Ratio Vascular Invasion Positive 18% 0% 35% 5% 3% Negative 15% 0% 7% 2% 1% Odds Ratio Hassan, et al. Dis Colon Rectum 2005; 48: Status of Resection Margin <1 mm 17
18 Diagnosis Invasive adenocarcinoma, high-grade with signet ring cells, arising in a tubulovillous adenoma Note: The lesion is not adequately excised. No vascular invasion identified. So the patient will get a colectomy Now, are we done? Histologic Features Signet ring cells Tumor infiltrating lymphocytes 18








19 MLH1 PMS2 MSH2 MSH6 Follow-Up Germline evaluation MLH1 exon 7-8 deletion Patient had Lynch syndrome Colonic resection Invasive adenocarcinoma extending into muscularis propria Eighteen negative regional lymph nodes 19
20 Take Home Points Be careful when thinking about high-grade dysplasia and intramucosal adenocarcinoma (ptis) in polypectomy and biopsy specimens Invasive carcinoma in the mucosa generally lacks a desmoplastic stromal reaction Colonized mucosa can look adenomatous Report on tumor grade, vascular invasion, and margin status when cancers come in polyps Tumor (or adenoma) infiltrating lymphocytes and heterogeneous patterns should prompt consideration of MSI-H Recognition important if Lynch syndrome is a consideration Case 3 78-year old male with rectal bleeding and elevated serum CEA Underwent colonoscopy 20

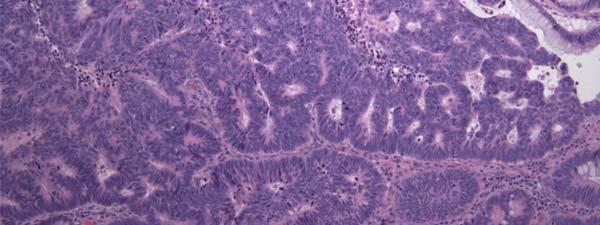
21 Endoscopic Findings Histologic Features 21




22 Histologic Features High-grade dysplasia Histologic Features Submucosal epithelium Extruded mucin pools 22


23 Histologic Features High-grade cytologic and architectural atypia Diagnostic Considerations Invasive adenocarcinoma Adenoma with misplaced epithelium and high-grade dysplasia/intramucosal adenocarcinoma 23


24 Histologic Features So we are really only worried about this This is in the mucosa Histologic Features Lobular arrangement of glands 24


25 Histologic Features Lamina propria Histologic Features 25


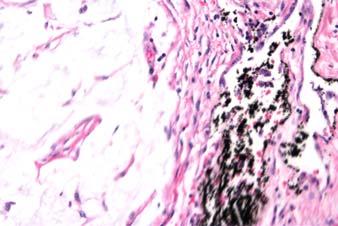
26 Histologic Features Hemosiderin deposits Diagnosis Adenoma with high-grade dysplasia and misplaced epithelium 26
 Presumably subjected to luminal trauma Lobular aggregates of mucosal")

27 Adenoma with Misplaced Epithelium Classic Features Pedunculated polyps of sigmoid colon (85% of cases) Presumably subjected to luminal trauma Lobular aggregates of mucosal elements in submucosa Inflammatory-type changes Fibrosis and splayed smooth muscle cells Hemosiderin and blood Extruded mucin pools, dilated crypts Adenoma with Misplaced Epithelium 27







28 Differential Diagnosis Invasive Adenocarcinoma Adenoma with Misplaced Epithelium Differential Diagnosis Invasive Adenocarcinoma Adenoma with Misplaced Epithelium 28


29 Adenoma with Misplaced Epithelium Background of benign mucosal elements Immunohistochemistry P53 in Cancer P53 in Adenoma Yantiss, et al. Am J Surg Pathol 2002; 26(2):
30 Take Home Points Think about submucosal epithelial misplacement Lobular arrangement of submucosal epithelium Associated lamina propria or non-neoplastic epithelium Inflammatory changes A few paucicellular mucin pools in submucosa Hemorrhage or hemosiderin Circumferential arrangement of fibrosis and smooth muscle around submucosal epithelium Think about carcinoma More than mild cytologic atypia Infiltrative appearance Numerous, irregular mucin pools, especially if there is a lot of associated epithelium Case 4 75-year old man underwent colonoscopy for clinical history of polyps Found to have a 3 cm sessile polyp in the right colon Mostly (70%) resected to reveal tubulovillous adenoma with low-grade dysplasia Patient underwent surgical resection 35 days after initial colonoscopy and biopsy 14 negative lymph nodes Margins free of adenoma 30




31 Histologic Features Histologic Features 31
32 Histologic Features Histologic Features 32
33 Diagnostic Considerations Invasive adenocarcinoma with mucinous areas Not cancer Adenoma with misplaced epithelium (weird for a sessile polyp in the right colon) Adenoma with misplaced epithelium for other reasons (i.e. endoscopic manipulation) Histologic Features Benign Rounded contour, communication with luminal surface 33




34 Histologic Features Associated lamina propria Histologic Features Associated with edge of benign gland and lamina propria 34




35 Histologic Features Disrupted, benign-appearing glands Histologic Features Disrupted, benign-appearing glands 35





36 Histologic Features Not overtly malignant, no stromal reaction Ki-67 Immunohistochemistry 36


37 P53 Immunohistochemistry Diagnosis Epithelial displacement (misplacement) in an adenoma secondary to endoscopic manipulation 37




38 Biopsy Related Changes in Adenomas Similar histologic features compared to adenomas with misplaced epithelium, although more closely mimic carcinoma Features typical of polyps that are not completely resected at first procedure Usually in right colon (polyps with misplaced epithelium occur in sigmoid colon) Often sessile Frequently large Another Case Layered fibrin and granulation tissue with entrapped epithelium 38






39 Another Case Epithelium and granulation tissue Mimics of Submucosal Invasion Biopsy-Related Changes 39




40 Mimics of Submucosal Invasion Biopsy-Related Changes Mucin pools in adenoma with low-grade dysplasia Mimics of Submucosal Invasion Biopsy-Related Changes Erosion or disruption of crypt with granulation tissue 40

 High-grade dysplasia 1/16 (6%) Submucosal epithelium Low-grade")
 Lamina propria 14/16 (88%) Extruded mucin 12/16 (75%) Granulation tissue 3/16 (19%)")
 Disrupted benign glands 3/16 (19%) Panarelli, et al.")
41 Mimics of Submucosal Invasion Biopsy-Related Changes Single cells associated with disrupted, regenerative crypts Pathologic Features of Sampled Adenomas Histologic feature Adenomas with Biopsy-Related Displaced Epithelium Cytologic Features Overlying surface adenoma Low-grade dysplasia 15/16 (94%) High-grade dysplasia 1/16 (6%) Submucosal epithelium Low-grade dysplasia 15/16 (94%) High-grade dysplasia 0 (0%) Other Features Single cells/clusters 6/16 (38%) Lamina propria 14/16 (88%) Extruded mucin 12/16 (75%) Granulation tissue 3/16 (19%) Fibrosis with fibroblastic proliferation 4/16 (25%) Hemorrhage/hemosiderin 7/16 (44%) Erosions or ulcers 7/16 (44%) Disrupted benign glands 3/16 (19%) Panarelli, et al. Mod Pathol 2015; 28(Suppl 2): 183A. 41

42 Take Home Points Think about prior manipulation of polyp Atypical epithelium associated with clearly benign epithelium and lamina propria in submucosa Gland disruption Apparently infiltrative cells embedded in granulation tissue or fibrin Myofibroblastic stromal response, not clearly desmoplasia Tattoo pigment or other evidence of procedure Clinical history of prior biopsy is not always provided Thank You 42
43 Difficulties in Staging Colorectal Cancers Rhonda K. Yantiss, MD Professor Department of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Medical College of Cornell University Colorectal Carcinoma Pathologic Assessment of Specimens Gold standard for evaluating extent of disease Identify histologic prognostic factors Measure efficacy of neoadjuvant therapy Facilitate ancillary (molecular) studies Provide quality assessment (surgery, radiology, pathology) Guide treatment decisions (adjuvant therapy and clinical trials) 43
44 Treatment Implications of Stage Stage I (T1-T2, N0, M0): Surgical resection Stage II (T3-T4, N0, M0): Surgical resection, potential adjuvant chemotherapy in high-risk cases Stage III (any T, N1 or N2, M0): Surgical resection and adjuvant/neoadjuvant chemotherapy + radiation Stage IV (any T, any N, M1): Chemotherapy with potential surgery Colorectal Cancer Reporting in 2015 Selected Problematic Issues Subjective interpretative issues How do I recognize a T4 tumor? Microscopic disease in lymph nodes Can I ignore isolated tumor cells? Tumor deposits and lymph nodes 44
45 Recognition of pt4 TNM Staging AJCC 7th Edition Tumor (T) ptis: Tumor limited to muscularis mucosae pt1: Tumor limited to submucosa pt2: Tumor limited to muscularis propria pt3: Tumor extends into pericolic tissue pt4: Tumor penetrates serosa (pt4a) or invades adjacent organs (pt4b)* *AJCC 6th edition: pt4a=invasion of adjacent organs pt4b=serosal penetration 45
46 Changing Definitions of pt4a and pt4b Overestimated bad prognosis of serosal penetration (6 th edition) Inability to recognize subtle (most) cases Data skewed in direction of patients with extensive serosal involvement (and a bad prognosis) Makes sense Tumor that invades another organ should do worse than one that is less extensive CAP Cancer Staging Protocol/AJCC Staging Tumor present at peritoneal surface Tumor cells on peritoneal surface 46

47 The Importance of Gross Examination The Importance of Gross Examination Fat is not circumferential on the abdominal colon 47





48 Recognizing Serosal Penetration Gross Examination Recognizing Serosal Penetration Gross Examination 48






49 Recognizing Serosal Penetration Gross Examination Recognizing Serosal Penetration Gross Examination 49




50 Recognizing Serosal Penetration Gross Examination Features of Serosal Penetration (Localized Peritoneal Involvement) 50


 Tumor within 1 mm of serosa associated with a serosal reaction (LP2)")
 Shepherd, et al.")
51 CAP Cancer Staging Protocol/AJCC Staging Tumor present at peritoneal surface Tumor cells on peritoneal surface Present in nearly one-third of surgically resected colonic carcinomas Serosal Penetration Relationship between serosa and tumor classified as local peritoneal involvement Free tumor cells on serosal surface (LP4) Tumor present at surface in association with serosal reaction (LP3) Tumor within 1 mm of serosa associated with a serosal reaction (LP2) Mesothelial hyperplasia Fibroinflammatory response Fibrin on serosa Tumor clear of serosa without any reaction (LP1) Shepherd, et al. Gastroenterology 1997; 112:




52 Serosal Penetration Tumor <1 mm from the peritoneal surface with a reaction Recognizing Serosal Penetration Tumor <1 mm from Serosal Reaction (LP2) Fibrin on serosa (erosion/ulcer) 52
53 Survival of Patients with Peritoneal Involvement LP1 LP3 LP2 LP4 Shepherd, et al. Gastroenterology 1997; 112: Gaps Between Recommendations and Clinical Practice 102 pathologists polled in North America and United Kingdom 45 teaching hospitals and 57 community practices 49 GI and 53 general pathologists To which of the following scenarios would you assign a stage of pt4a? 92%: Tumor at or on the serosal surface or free within peritoneal cavity (LP3 and LP4) 49%: Tumor <1mm from the serosal surface with a fibroinflammatory and serosal reaction (LP2) 7%: Tumor <1 mm from the serosal surface without any fibroinflammatory serosal reaction (LP1) Cancer present <1 mm from the serosal surface with a fibroinflammatory peritoneal reaction is best staged as: pt4a (45%) [For GI pathologists: Canada 32%, USA 87%, UK 50%] pt3 without a comment (7%) pt3 with a comment to suggest that there could be a breach of the peritoneum, and the tumor may behave like a pt4a tumor (48%) Driman, et al Mod Pathol 2015; 28(Suppl 2): 170A. 53



: 1252-1258.")
54 Recognizing Serosal Penetration Cytology 120 colon cancers staged according to AJCC 7 th ed. Serosal cytology smears Positive cytology in 55% of tumors at serosal surface (pt4a) 46% of tumors <1 mm from serosa that showed a tissue reaction (pt3 by strict criteria) Panarelli, et al. Am J Surg Pathol 2013; 37(8): Recognizing Serosal Penetration 54







55 Recognizing Serosal Penetration Entrapped Mesothelium Near Serosa Serosa Mesothelium Recognizing Serosal Penetration Clefts between Fat Lobules 55








56 Recognizing Serosal Penetration Clefts between Fat Lobules Mesothelium Recognizing Serosal Penetration Entrapped Mesothelium Cancer Mesothelium 56

57 Gross Perforation Through Tumor is at Least pt4a, Regardless of Histologic Findings Recognizing Tumoral Perforation Gross Examination 57






58 Recognizing Tumoral Perforation Microscopic Examination Recognizing Tumoral Perforation Microscopic Examination 58



59 Recognizing Tumoral Perforation Microscopic Examination Perpendicular arrays of capillaries Fibrin on serosa Recognizing Tumoral Perforation?Mesothelium Fibrin Cancer 59


60 Ancillary Techniques Assessment for Serosal Penetration Elastin Stains Subserosal elastic lamina Directly subjacent to visceral peritoneum Destruction by invasive carcinoma Detected with elastin stains Surrogate marker of serosal penetration by tumor 60








61 Assessment for Serosal Penetration Elastin Stains Assessment for Serosal Penetration Elastin Stains Tumor confined to muscularis propria 61




62 Assessment for Serosal Penetration Elastin Stains No elastic lamina Normal serosa Problematic Issues Elastin Stains Elastic lamina may not be present in all cases, especially tumors of right colon Elastic lamina may be retracted or incomplete at advancing front of cancer due to fibrosis Elastic fibrils may be present at advancing front of tumors that are not close to the peritoneal surface Disruption of these fibrils does not necessarily imply serosal penetration 62
63 Lymph Nodes and Tumor Deposits High-Risk Stage II Cancers NCCN Guidelines Clinical features Colonic obstruction by tumor Colonic perforation Pathologic features Tumor penetration of serosa (pt4a) Close, indeterminate, or positive margins Inadequate lymph node sampling (<12 negative nodes) High-grade (G3-G4) features in a microsatellite stable (MSS) tumor Lymphovascular or venous invasion Perineural invasion 63
64 TNM Staging Regional Lymph Nodes (N) All grossly negative nodes entirely submitted Minimum required number: Clarifying solutions, additional sections No definite minimum after neoadjuvant treatment of rectal cancer Fewer identified lymph nodes may be a marker of better response to therapy Lymph node detection Patient factors (sex, obesity) Length of resected colon Surgeon and pathologist skill and experience Ratio (number positive/number collected) may be better prognostic indicator than number positive Sugimoto, et al. Ann Surg Oncol 2015; 22(2): Small Lymph Node Deposits Micrometastases (0.2-2 mm) Classified as positive node Categorized as pn1 (mic) Isolated tumor cells (single clusters <0.2 mm) Classified as negative node If only positive node has a tiny cluster (<0.2 mm), then categorized as pn0 (i+) Denotes isolated tumor cells, not immunopositive 64
 Isolated tumor cells (single clusters): pn0 (i+) Courtesy")
65 AJCC and CAP Guidelines Regional Lymph Nodes (N) pn1 (mic) for deposits mm Courtesy of Dr. Alexandros Polydorides, Mount Sinai Medical School, NY, NY AJCC and CAP Guidelines Regional Lymph Nodes (N) Isolated tumor cells (single clusters): pn0 (i+) Courtesy of Dr. Alexandros Polydorides, Mount Sinai Medical School, NY, NY 65
66 AJCC and CAP Guidelines Regional Lymph Nodes (N) Isolated tumor cells (single clusters): pn0 (i+) Courtesy of Dr. Alexandros Polydorides, Mount Sinai Medical School, NY, NY Isolated Tumor Cells (i+) Biologic significance not entirely clear Limited data, mostly in breast cancer Guanylyl cyclase 2C (GUCY2C) Colonic epithelium and adenocarcinoma Stage II colon cancer at risk for recurrence Sargent, et al., Ann Surg Oncol 2011; 18(12):
67 Tumor Deposits Peritumoral nodule of cancer without residual nodal structure Within regional lymph drainage of tumor Possible explanations Lymph node metastasis with complete effacement of residual lymph node Lymphovascular, venous, or perineural invasion with extavascular/extraneural extension Biologic importance Poor prognostic factor, independent of T and N Ueno, et al. Am J Surg Pathol 2014; 207(1): TNM Staging Revisions Over Time Tumor Deposits TNM Staging System AJCC 4 th edition (1987) AJCC 5 th edition (1997) AJCC 6 th edition (2002) AJCC 7 th edition (2009) Major Changes Introduction of N3 category (tumor along a named artery) Removal of N3 category Tumor deposit 3 mm rule 3 mm rule replaced by contour rule Isolated tumor cells considered negative Subclassification of N1 (N1a and N1b) and N2 (N2a and N2b) Peritumoral deposits classified as N1c, if no other regional lymph node metastases 67
 >3 mm considered replaced lymph node Staged in N category Reproducible, but clinically irrelevant")

68 TNM Staging AJCC 5th Edition 3 mm Rule for Classifying Deposits <3 mm considered extension of tumor Staged in T category (pt3) >3 mm considered replaced lymph node Staged in N category Reproducible, but clinically irrelevant TNM Staging AJCC 6th Edition Contour Rule for Classifying Deposits Round nodule considered lymph node Staged in N category Irregular nodule considered perineural or vascular invasion Staged in T category (problematic if tumor T1 or T2) 68
69 TNM Staging AJCC 7th Edition pn1c Classification of Deposits Intended to identify patients with stage I or II disease at risk for recurrence Classified in the N category to upstage patients for potential adjuvant therapy N1c chosen to denote these individuals for long term follow up in large, multiinstitutional studies Intended to be used with T1-T2 tumors Now applied to T3 and T4 as well Effects of Survival Number and Type of Tumor Deposits Puppa et al. Mod Pathol 2007; 20:

 Sometimes near arteries (reflecting effaced veins) Rock, et al. Arch Pathol Lab Med 2014; 138(5): 636-642.")
70 TNM Staging AJCC 7th Edition Reporting of Peritumoral Deposits If subjective impression is that a tumor nodule represents a replaced lymph node, it is staged as N1a, N1b, N2a, or N2b Tumor deposits are prognostically important and counted Staged as N1c if all nodes negative Helpful Diagnostic Features Effaced lymph node Round shape Peripheral rim of lymphocytes Capsule Peripheral lymphoid follicles Subcapsular sinus Tumor deposits Irregular contour No organized lymphoid tissue Not surrounded by capsule (parallel collagen fibrils) Sometimes near arteries (reflecting effaced veins) Rock, et al. Arch Pathol Lab Med 2014; 138(5):




71 Lymph Node or Tumor Deposit? Nagtegaal, et al, Histopathology 2007;51:141-9 Tumor Deposits vs. Lymph Node Metastases Mountains out of Molehills 71



72 Mimics of Tumor Deposits Venous Invasion Clear cut venous invasion is not a tumor deposit Mimics of Tumor Deposits Peritoneal Seeding (M1) Tumor spread along peritoneal surface is not a tumor deposit 72
73 Reporting Tumor Deposits and N1c Tumor nodule in regional lymph drainage No residual lymph node architecture Tumor deposit may be considered if a nodule cannot be classified as Lymph node Lymphatic vessel invasion Venous invasion Perineural invasion Reporting Tumor Deposits and N1c Tumor deposits do not affect T stage Do not add tumor deposits to total positive lymph node count Separately documented (and counted) Do not use N1c if any lymph nodes contain metastases N1c does not imply more advanced stage than N1a or N1b 73

74 Colorectal Cancer Staging Take Home Points Tumor staging Serosal penetration is underdiagnosed and likely single most important feature to identify Can affect management (chemotherapy for Stage II) Lymph node issues Inadequate harvest can affect management Isolated tumor cells (<0.2 mm) are not currently classified as positive lymph nodes Documening tumor deposits Do not add to lymph node count or tumor stage N1c limited to cases that are otherwise node-negative Distinction from effaced nodes largely academic 74
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors
 Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Frédéric Bibeau, MD, PhD Pathology department Biopathology unit Institut du Cancer de Montpellier France Quality
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Frédéric Bibeau, MD, PhD Pathology department Biopathology unit Institut du Cancer de Montpellier France Quality
Disclosures. Outline. What IS tumor budding?? Tumor Budding in Colorectal Carcinoma: What, Why, and How. I have nothing to disclose
 Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer
 General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Update on Colonic Serrated (and Conventional) Adenomatous Polyps
 Adenomatous Polyps") Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN
 Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
Serrated Colorectal Polyps New Challenges to Old Dogma. Kenneth Batts, M.D. Abbott Northwestern Hospital Minneapolis, MN
 Serrated Colorectal Polyps New Challenges to Old Dogma Kenneth Batts, M.D. Abbott Northwestern Hospital Minneapolis, MN A Sneak Preview.... This was in the good old days: Adenomas HPPs Mixed Polyps A Sneak
Serrated Colorectal Polyps New Challenges to Old Dogma Kenneth Batts, M.D. Abbott Northwestern Hospital Minneapolis, MN A Sneak Preview.... This was in the good old days: Adenomas HPPs Mixed Polyps A Sneak
Neoplasms of the Colon and of the Rectum
 Neoplasms of the Colon and of the Rectum 2 0 1 5-2 0 1 6 F C D S E D U C A T I O N A L W E B C A S T S E R I E S S T E V E N P E A C E, B S, C T R F E B R U A R Y 1 8, 2 0 1 6 2016 Focus o Anatomy o SS
Neoplasms of the Colon and of the Rectum 2 0 1 5-2 0 1 6 F C D S E D U C A T I O N A L W E B C A S T S E R I E S S T E V E N P E A C E, B S, C T R F E B R U A R Y 1 8, 2 0 1 6 2016 Focus o Anatomy o SS
Case presentation. Eran Zittan. MD Mount Sinai Hospital, Toronto, Canada. Emek Medical Center, Afula, Israel. March, 2016
 Case presentation Eran Zittan. MD Mount Sinai Hospital, Toronto, Canada. Emek Medical Center, Afula, Israel. March, 2016 60 y/o man with long standing UC+PSC. Last 10 years on clinical and endoscopic remission.
Case presentation Eran Zittan. MD Mount Sinai Hospital, Toronto, Canada. Emek Medical Center, Afula, Israel. March, 2016 60 y/o man with long standing UC+PSC. Last 10 years on clinical and endoscopic remission.
Large Colorectal Adenomas An Approach to Pathologic Evaluation
 Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
References. GI Biopsies. What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD
 What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School
 Precursors of Colorectal Carcinoma Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Hyperplastic polyp Adenomatous polyp Colorectal carcinoma IBD-associated (1-2%) Sporadic
Precursors of Colorectal Carcinoma Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Hyperplastic polyp Adenomatous polyp Colorectal carcinoma IBD-associated (1-2%) Sporadic
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
5/2/2018. Low Grade Dysplasia of GI Tract. High Grade Dysplasia of GI Tract. Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues
 Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Overview. Collecting Cancer Data: Colon 11/5/2009. Collecting Cancer Data: NAACCR Webinar Series 1. Agenda NAACCR WEBINAR SERIES
 Collecting Cancer Data: Colon 11/5/2009 Collecting Cancer Data: Colon/Rectum/Appendix NAACCR 2009 2010 WEBINAR SERIES Agenda Overview Treatment MP/H Rules CSv2 2 Overview Colon/Rectum/Appendix 2009 2010
Collecting Cancer Data: Colon 11/5/2009 Collecting Cancer Data: Colon/Rectum/Appendix NAACCR 2009 2010 WEBINAR SERIES Agenda Overview Treatment MP/H Rules CSv2 2 Overview Colon/Rectum/Appendix 2009 2010
Serrated Lesions in the Bowel Cancer Screening Programme
 Serrated Lesions in the Bowel Cancer Screening Programme Mark Arends Cambridge & Edinburgh Serrated Lesions of Large Bowel 1. Hyperplastic polyp 2. Serrated adenoma 3. Mixed polyp 4. Sessile serrated lesion
Serrated Lesions in the Bowel Cancer Screening Programme Mark Arends Cambridge & Edinburgh Serrated Lesions of Large Bowel 1. Hyperplastic polyp 2. Serrated adenoma 3. Mixed polyp 4. Sessile serrated lesion
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Adenoma Low-grade appendiceal mucinous neoplasm High-grade appendiceal mucinous neoplasm Adenocarcinoma Serrated
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Adenoma Low-grade appendiceal mucinous neoplasm High-grade appendiceal mucinous neoplasm Adenocarcinoma Serrated
Seventh Edition Staging 2017 Colorectum. Overview. This webinar is sponsored by. the Centers for Disease Control and Prevention.
 Seventh Edition Staging 2017 Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express
Seventh Edition Staging 2017 Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express
Sessile Serrated Polyps
 Årsmøtet i Den norske Patologforening 2014 Sessile Serrated Polyps Tor J. Eide Oslo Universitetssykehus The term serrated include a group of lesions with a sawtoothlike appearance of the crypts and the
Årsmøtet i Den norske Patologforening 2014 Sessile Serrated Polyps Tor J. Eide Oslo Universitetssykehus The term serrated include a group of lesions with a sawtoothlike appearance of the crypts and the
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Physician s Cognitive and Communication Failures Result in Cancer Treatment Delay
 1 Physician s Cognitive and Communication Failures Result in Cancer Treatment Delay Abstract: The estate of a 60 year old male alleged negligence against a gastroenterologist in failing to properly evaluate
1 Physician s Cognitive and Communication Failures Result in Cancer Treatment Delay Abstract: The estate of a 60 year old male alleged negligence against a gastroenterologist in failing to properly evaluate
A WHO update on Serrated Polyps
 A WHO update on Serrated Polyps Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Am J Gastroenterol. 2010 Nov 2. [Epub ahead of The Clinical Significance of Serrated Polyps.
A WHO update on Serrated Polyps Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Am J Gastroenterol. 2010 Nov 2. [Epub ahead of The Clinical Significance of Serrated Polyps.
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
SEER EOD AND SUMMARY STAGE ABSTRACTORS TRAINING
 SEER EOD AND SUMMARY STAGE ABSTRACTORS TRAINING OVERVIEW What is SEER EOD Ambiguous Terminology General Guidelines EOD Primary Tumor EOD Regional Nodes EOD Mets Site Specific Data Items (SSDI) SEER Summary
SEER EOD AND SUMMARY STAGE ABSTRACTORS TRAINING OVERVIEW What is SEER EOD Ambiguous Terminology General Guidelines EOD Primary Tumor EOD Regional Nodes EOD Mets Site Specific Data Items (SSDI) SEER Summary
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
6/5/2010. Renal vein invasion & Capsule Penetration (T3a) Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4).
 Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4).") GU Cancer Staging: Updates and Challenging Areas 13 th Current Issues in Surgical Pathology San Francisco, CA June 5, 2010 Jeffry P. Simko, PhD, MD Associate Professor Departments of Urology and Anatomic
GU Cancer Staging: Updates and Challenging Areas 13 th Current Issues in Surgical Pathology San Francisco, CA June 5, 2010 Jeffry P. Simko, PhD, MD Associate Professor Departments of Urology and Anatomic
Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum
 Tsumura T, et al 1 Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum T. Tsumura a T. Hiyama d S. Tanaka b M. Yoshihara d K. Arihiro c K. Chayama a Departments
Tsumura T, et al 1 Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum T. Tsumura a T. Hiyama d S. Tanaka b M. Yoshihara d K. Arihiro c K. Chayama a Departments
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you)
") What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci. Colon polyps. Colorectal cancer
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
05/07/2018. Organisation. The English screening programme what is happening? Organisation. Bowel cancer screening in the UK is:
 Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
polyps of the colon and rectum
 J. clin. Path., 1973, 26, 25-31 Pseudo-carcinomatous invasion in adenomatous polyps of the colon and rectum T. MUTO, H. J. R. BUSSEY, AND B. C. MORSON From St Mark's Hospital, London SYNOPSIS The histology
J. clin. Path., 1973, 26, 25-31 Pseudo-carcinomatous invasion in adenomatous polyps of the colon and rectum T. MUTO, H. J. R. BUSSEY, AND B. C. MORSON From St Mark's Hospital, London SYNOPSIS The histology
What Pathology can tell us in the approach of localized colorectal cancer
 What Pathology can tell us in the approach of localized colorectal cancer A/Prof Tony Lim Kiat Hon Department of Anatomical Pathology Singapore General Hospital ESMO 2017 Singapore Nov 1 2 Do we still
What Pathology can tell us in the approach of localized colorectal cancer A/Prof Tony Lim Kiat Hon Department of Anatomical Pathology Singapore General Hospital ESMO 2017 Singapore Nov 1 2 Do we still
Colon and Rectum 5/1/14
 Collecting Cancer Data: Colon and Rectum 2013 2014 NAACCR Webinar Series May 1, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data: Colon and Rectum 2013 2014 NAACCR Webinar Series May 1, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Formula One Study. Assessment criteria of pathological parameters. Ver.2. UK Japan Joint Study for Risk Factors of Lymph Node
 APPENDIX 01: Assessment criteria Formula One Study UK Japan Joint Study for Risk Factors of Lymph Node Metastasis in Submucosal Invasive (pt1) Colorectal Cancer Assessment criteria of pathological parameters
APPENDIX 01: Assessment criteria Formula One Study UK Japan Joint Study for Risk Factors of Lymph Node Metastasis in Submucosal Invasive (pt1) Colorectal Cancer Assessment criteria of pathological parameters
Management of pt1 polyps. Maria Pellise
 Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
AJCC 7 th Edition Staging Disease Site Webinar Colorectum
 AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310
AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310
7 th Edition Staging. AJCC 7 th Edition Staging. Disease Site Webinar. Colorectum. Overview. This webinar is sponsored by
 AJCC 7 th Edition Staging Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers
AJCC 7 th Edition Staging Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers
Rectal Cancer Cookbook Update. A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux
 Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
Nodal staging of colorectal cancer, TNM and practical issues
 Nodal staging of colorectal cancer, TNM and practical issues Gábor Cserni 1. Bács-Kiskun County Teaching Hospital, Kecskemét 2. University of Szeged, Szeged Different staging systems: A,B,C,(D) Same letters
Nodal staging of colorectal cancer, TNM and practical issues Gábor Cserni 1. Bács-Kiskun County Teaching Hospital, Kecskemét 2. University of Szeged, Szeged Different staging systems: A,B,C,(D) Same letters
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
Pseudoinvasion and how to deal with it
 Pseudoinvasion and how to deal with it Professor Neil A Shepherd Gloucester & Cheltenham, UK European Society of Pathology Bilboa, 12 June 2018 Enterprise Interest None Pseudoinvasion and how to deal with
Pseudoinvasion and how to deal with it Professor Neil A Shepherd Gloucester & Cheltenham, UK European Society of Pathology Bilboa, 12 June 2018 Enterprise Interest None Pseudoinvasion and how to deal with
[A RESEARCH COORDINATOR S GUIDE]
![[A RESEARCH COORDINATOR S GUIDE]](/thumbs/88/117127924.jpg "[A RESEARCH COORDINATOR S GUIDE]") 2013 COLORECTAL SURGERY GROUP Dr. Carl J. Brown Dr. Ahmer A. Karimuddin Dr. P. Terry Phang Dr. Manoj J. Raval Authored by Jennifer Lee A cartoon about colonoscopies. 1 [A RESEARCH COORDINATOR S GUIDE]
2013 COLORECTAL SURGERY GROUP Dr. Carl J. Brown Dr. Ahmer A. Karimuddin Dr. P. Terry Phang Dr. Manoj J. Raval Authored by Jennifer Lee A cartoon about colonoscopies. 1 [A RESEARCH COORDINATOR S GUIDE]
Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ]
![Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ]](/thumbs/82/86264030.jpg "Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ]") Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ] CS Tumor Size 000 No mass/tumor found 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters or larger 990 Microscopic
Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ] CS Tumor Size 000 No mass/tumor found 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters or larger 990 Microscopic
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
AJCC Cancer Staging 8 th Edition
 AJCC Cancer Staging 8 th Edition Colon and Rectal Cancer Staging Update Webinar George J Chang, MD, MS Deputy Chair, Department of Surgical Oncology Chief, Colon and Rectal Surgery Professor of Surgical
AJCC Cancer Staging 8 th Edition Colon and Rectal Cancer Staging Update Webinar George J Chang, MD, MS Deputy Chair, Department of Surgical Oncology Chief, Colon and Rectal Surgery Professor of Surgical
3/30/2017. Disclosure of Relevant Financial Relationships. Case 5: Polypoid mass in ulcerative colitis. Case 5. TC Smyrk
 Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma
 Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
Disorders of Cell Growth & Neoplasia. Histopathology Lab
 Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Despite advances in our understanding of appendiceal. An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms
 REVIEW ARTICLE An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms Mark A. Valasek, MD, PhD* and Reetesh K. Pai, MD Abstract: Despite advances in our understanding of appendiceal
REVIEW ARTICLE An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms Mark A. Valasek, MD, PhD* and Reetesh K. Pai, MD Abstract: Despite advances in our understanding of appendiceal
2014/2015 FCDS Educational Webcast Series
 2014/2015 FCDS Educational Webcast Series February 19, 2015 Steven Peace, CTR 2015 Update; Background, Anatomy, Risk Factors, Screening Guidelines, MPH Rules Review AJCC TNM 7 th ed, SS2000, CSv02.05 and
2014/2015 FCDS Educational Webcast Series February 19, 2015 Steven Peace, CTR 2015 Update; Background, Anatomy, Risk Factors, Screening Guidelines, MPH Rules Review AJCC TNM 7 th ed, SS2000, CSv02.05 and
Adenoma and Malignant Colorectal Polyp: Pathological Considerations and Clinical Applications
 Adenoma and Malignant Colorectal Polyp: Pathological Considerations and Clinical Applications Authors: *Emil Salmo, 1 Najib Haboubi 2 1. Department of Histopathology, The Pennine Acute Hospitals NHS Trust,
Adenoma and Malignant Colorectal Polyp: Pathological Considerations and Clinical Applications Authors: *Emil Salmo, 1 Najib Haboubi 2 1. Department of Histopathology, The Pennine Acute Hospitals NHS Trust,
Histo-prognostic factors what histopathology has to offer for clinical decision making
 Histo-prognostic factors what histopathology has to offer for clinical decision making Daniela E. Aust Institute for Pathology, University Hospital Dresden, Germany Center for Molecular Tumor Diagnostics
Histo-prognostic factors what histopathology has to offer for clinical decision making Daniela E. Aust Institute for Pathology, University Hospital Dresden, Germany Center for Molecular Tumor Diagnostics
NUMERATOR: Reports that include the pt category, the pn category and the histologic grade
 Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
The Rodger C. Haggitt Memorial Lecture
 The Rodger C. Haggitt Memorial Lecture I got an email on 4/22/14 from Hala El Zamaity inviting me to give this lecture and giving me this topic: The ever changing TNM classification and its implication
The Rodger C. Haggitt Memorial Lecture I got an email on 4/22/14 from Hala El Zamaity inviting me to give this lecture and giving me this topic: The ever changing TNM classification and its implication
Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum
 Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Pathology Today American Society for Clinical Pathology Annual Meeting Workshop No: 1340 Gastrointestinal Pathology: New Approaches to Old Problems
 Pathology Today American Society for Clinical Pathology Annual Meeting Workshop No: 1340 Gastrointestinal Pathology: New Approaches to Old Problems ASCP Annual Meeting/WASPaLM XXVI World Congress Las Vegas,
Pathology Today American Society for Clinical Pathology Annual Meeting Workshop No: 1340 Gastrointestinal Pathology: New Approaches to Old Problems ASCP Annual Meeting/WASPaLM XXVI World Congress Las Vegas,
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Histopathology: gastritis and peptic ulceration
 Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
NUMERATOR: Reports that include the pt category, the pn category and the histologic grade
 Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE
 COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
High risk stage II colon cancer
 High risk stage II colon cancer Joel Gingerich, MD, FRCPC Assistant Professor Medical Oncologist University of Manitoba CancerCare Manitoba Disclaimer No conflict of interests 16 October 2010 Overview
High risk stage II colon cancer Joel Gingerich, MD, FRCPC Assistant Professor Medical Oncologist University of Manitoba CancerCare Manitoba Disclaimer No conflict of interests 16 October 2010 Overview
Neoplasia literally means "new growth.
 NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
Gastric Cancer Staging AJCC eighth edition. Duncan McLeod Westmead Hospital, NSW
 Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Malignant colorectal polyps: venous invasion and
 774 Gut, 1991,32, 774-778 Malignant colorectal polyps: venous invasion and successful treatment by endoscopic polypectomy Department of Pathology J M Geraghty Endoscopy Unit C B Williams and ICRF Colorectal
774 Gut, 1991,32, 774-778 Malignant colorectal polyps: venous invasion and successful treatment by endoscopic polypectomy Department of Pathology J M Geraghty Endoscopy Unit C B Williams and ICRF Colorectal
Colorectal carcinoma: Pathologic aspects
 Review Article Colorectal carcinoma: Pathologic aspects Matthew Fleming*, Sreelakshmi Ravula*, Sergei F. Tatishchev*, Hanlin L. Wang Department of Pathology and Laboratory Medicine, David Geffen School
Review Article Colorectal carcinoma: Pathologic aspects Matthew Fleming*, Sreelakshmi Ravula*, Sergei F. Tatishchev*, Hanlin L. Wang Department of Pathology and Laboratory Medicine, David Geffen School
Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum
 Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Handling & Grossing of Colo-rectal Specimens for Tumours. for Medical Officers in Pathology
 Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Peritoneal Involvement in Stage II Colon Cancer
 Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
A superficial radiotherapy B single pass curettage C excision with 2 mm margins D excision with 5 mm margins E Mohs micrographic surgery.
 1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
Protocol for the Examination of Specimens from Patients with Primary Carcinomas of the Colon and Rectum
 Protocol for the Examination of Specimens from Patients with Primary Carcinomas of the Colon and Rectum Well differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Protocol for the Examination of Specimens from Patients with Primary Carcinomas of the Colon and Rectum Well differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments