Sentinel Node Alphabet Soup: MSLT-1, DeCOG-SLT, MSLT-2, UNC
|
|
|
- Linda Ryan
- 5 years ago
- Views:
Transcription

1 Sentinel Node Alphabet Soup: MSLT-1, DeCOG-SLT, MSLT-2, UNC David W. Ollila MD James and Jesse Millis Professor of Surgery University of North Carolina, Chapel Hill Disclosures: None July 15, 2018
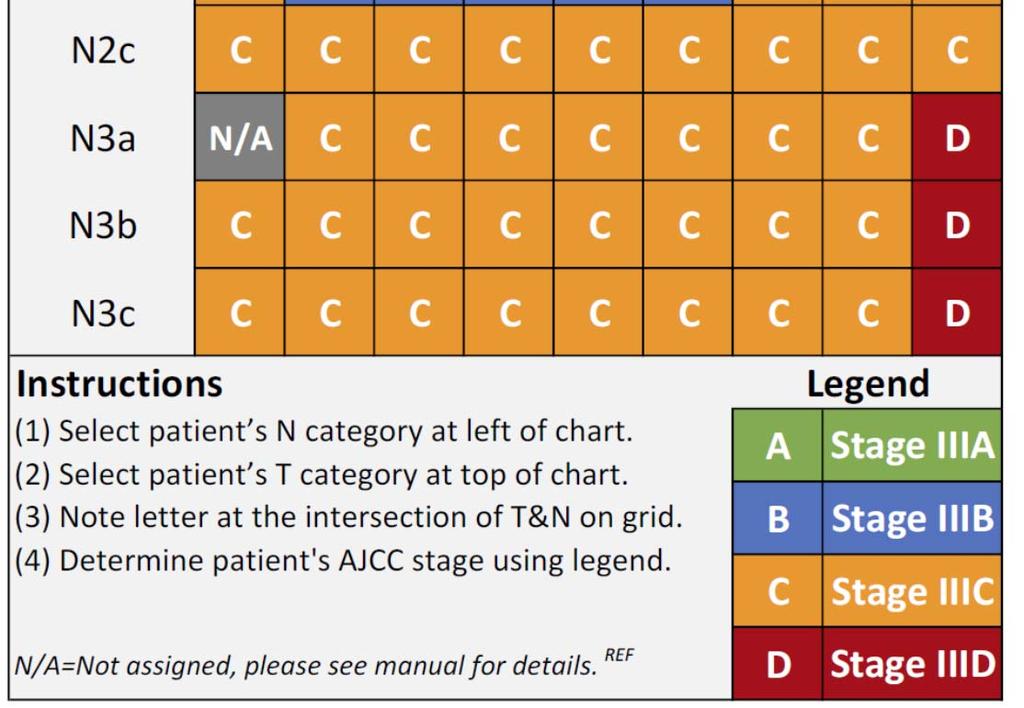
2 AJCC 8 th Edition 2018 Gershenwald et al.,
3 Comparisons of 7 th vs. 8th Balch, JCO 2009 Gershenwald et al.,2017 3
4 Comparisons of 7 th vs. 8th Balch, JCO 2009 Gershenwald et al.,2017 4
5 Comparisons of 7 th vs. 8th Balch, JCO 2009 Gershenwald et al.,2017 5
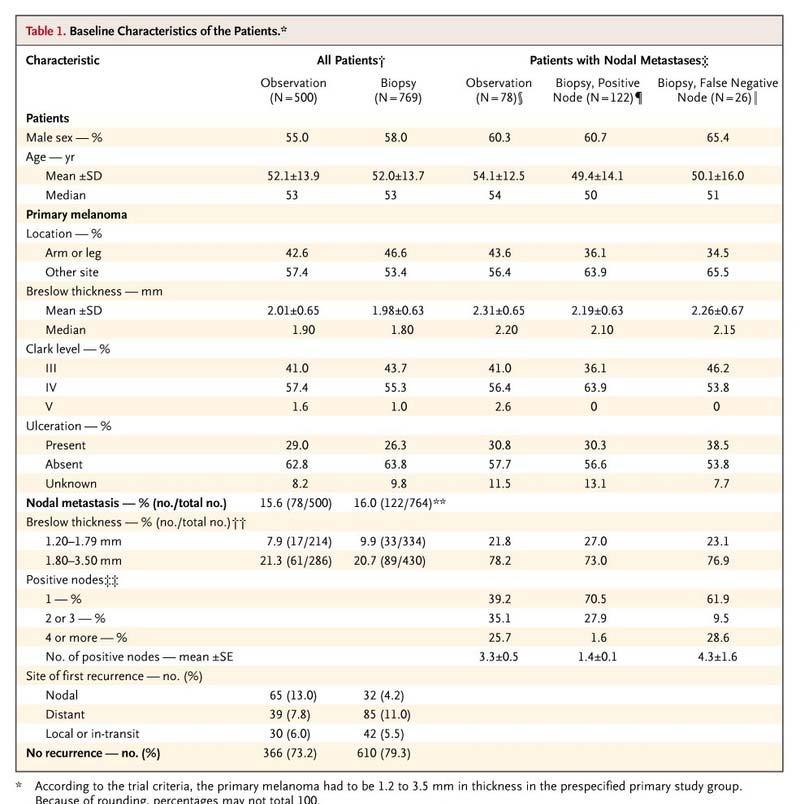
6 MSLT-1: Immediate vs. Delayed CLND Nodal Metastases Melanoma mm Randomized WEX + SNB 60% WEX + Watch & Wait Observ. 40% SN(-) SN(+) Nodal Recurrence Observation Immediate CLND Delayed CLND Overall Survival p=ns Morton, NEJM
7 7
8 Morton, NEJM
9 MSLT-1: Immediate vs. Delayed CLND Nodal Metastases Melanoma mm Randomized WEX + SNB 60% WEX + Watch & Wait Observ. 40% SN(-) SN(+) Nodal Recurrence Observation Immediate CLND Delayed CLND Mean # Nodes year Melanoma Survival: 90.2% 72.3% 52.4% HR 2.48; p<0.001 HR 0.51; p<0.001 Morton, NEJM
10 Morton, NEJM 2006 Patients with T2/T3 melanomas and nodal metastases derive a 20% absolute survival advantage with a SN procedure and CLND as compared to watchful waiting CAVEAT: DSMB advised release of data to physicians and public because multiple endpoints had been reached, but not overall survival 10


11 Standard of care for patients with T2 or T3 melanoma No survival advantage 1/ % False-positivity 1/


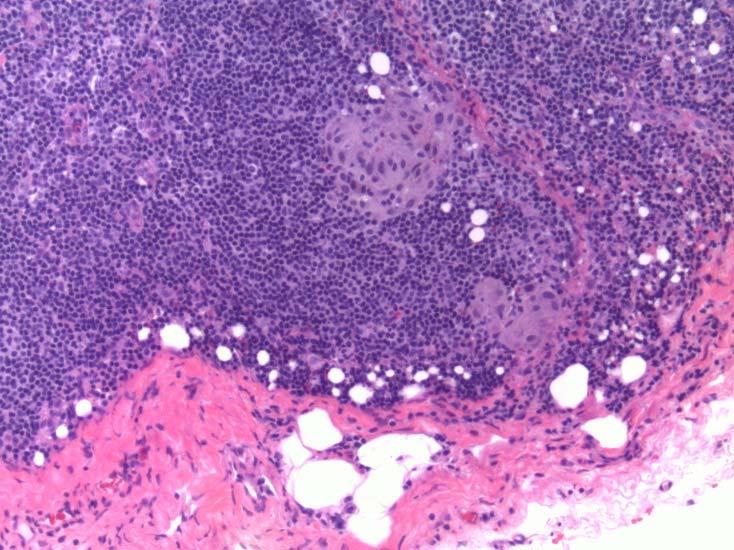
12 Demonstrating Biology Metastatic melanoma cells, regardless of the size of the cluster, have biologic relevance Ollila et al., JACS 2009 Society of Surgical Oncology Position Statement Annals of Surgical Oncology
13 Recurrence and Death events for each tumor burden group (n=578) Tumor Burden N (% ) Recurrence n(%) Distance Recurrence n(%) Death n(%) Node 488 (84%) 56 (11%) 35 (7%) 52 (11%) negative <0.1mm 33 (6%) 8 (24%) 5 (15%) 5 (15%) mm 27 (5%) 10 (37%) 6 (22%) 6 (22%) >1.0mm 30 (5%) 21 (70%) 14 (47%) 12 (40%) Ollila et al., JACS
14 MSLT-1: Immediate vs. Delayed CLND Nodal Metastases Melanoma mm Randomized WEX + SNB 60% WEX + Watch & Wait Observ. 40% SN(-) SN(+) Nodal Recurrence Observation Immediate CLND Delayed CLND Overall Survival: p=ns Morton, NEJM
15 MSLT-1: Immediate vs. Delayed CLND Nodal Metastases Melanoma mm Randomized WEX + SNB 60% WEX + Watch & Wait Observ. 40% SN(-) SN(+) Nodal Recurrence Observation Immediate CLND Delayed CLND Mean # Nodes year Melanoma Survival: 85.1% 62.1% 33.5% HR 3.09; p<0.001 HR 0.51; p<0.001 Morton, NEJM
 SN(+) Nodal Recurrence Observation Immediate CLND Delayed CLND Mean # Nodes 4.3 1.4 3.3 10 year Melanoma Survival: 85.1% 62.1% 33.5% HR 3.09; p<0.")
16 MSLT-1: Immediate vs. Delayed CLND Nodal Metastases Melanoma mm Randomized WEX + SNB 60% WEX + Watch & Wait Observ. 40% SN(-) SN(+) Nodal Recurrence Observation Immediate CLND Delayed CLND Mean # Nodes year Melanoma Survival: 85.1% 62.1% 33.5% HR 3.09; p<0.001 HR 0.51; p<0.001 Morton, NEJM
17 DeCOG-SLT and MSLT-2 SN+ Immediate CLND Active Surveillance: Ultrasound Leiter U et al., Lancet Oncol Faries MB et al., NEJM
18 DeCOG-SLT: Results Distant Metastasis-Free Survival Overall Survival Recurrence-Free Survival HR P-value HR P- HR P-value value Obs vs LND Tumor load in 2.33 < < < SLN ( 1 m v > 1) Tumor thickness 3.06 < < < ( 2 mm vs > 2) Ulceration (y/n) # SLNs + (1 vs ) IFN therapy (y/n) Median follow-up was 35 months 18 Leiter U et al., Lancet Oncol. 2016
19 DeCOG-SLT: Results Distant Metastasis-Free Survival Overall Survival Recurrence-Free Survival HR P-value HR P- HR P-value value Obs vs LND Tumor load in 2.33 < < < SLN ( 1 m v > 1) Tumor thickness 3.06 < < < ( 2 mm vs > 2) Ulceration (y/n) # SLNs + (1 vs ) IFN therapy (y/n) Median follow-up was 35 months 19 Leiter U et al., Lancet Oncol. 2016
20 DeCOG-SLT: Results Distant Metastasis-Free Survival Overall Survival Recurrence-Free Survival HR P-value HR P- HR P-value value Obs vs LND Tumor load in 2.33 < < < SLN ( 1 m v > 1) Tumor thickness 3.06 < < < ( 2 mm vs > 2) Ulceration (y/n) # SLNs + (1 vs ) IFN therapy (y/n) Median follow-up was 35 months 20 Leiter U et al., Lancet Oncol. 2016
21 DeCOG-SLT: Results A: Distant Metastasis-Free Survival B: Overall Survival C: Recurrence-Free Survival Leiter U et al., Lancet Oncol
22 DeCOG-SLT: Results A: Distant Metastasis-Free Survival B: Overall Survival C: Recurrence-Free Survival Leiter U et al., Lancet Oncol
23 DECOG: Conclusion A: Distant Metastasis-Free Survival B: Overall Survival Active ultrasound surveillance appears a reasonable alternative for T1,T2 N1 melanoma C: Recurrence-Free patients Survival with SN metastasis < 1mm Leiter U et al., Lancet Oncol
24 DeCOG-SLT and MSLT-2 SN+ Immediate CLND Active Surveillance: Ultrasound Leiter U et al., Lancet Oncol Faries MB et al., NEJM


25 25 Faries MB et al., NEJM 2017
26 MSLT-2 Results (n=1755) Overall Survival: CLND vs Observation 86±1% vs 86±1%,p=0.42 n=1934 ITT n=1755 per protocol Median: 43 months Disease-free Survival: CLND vs. observation 68±1% vs 63±1%,p= Faries MB et al., NEJM 2017
27 MSLT-2 Results (n=1755) Overall Survival: CLND vs Observation 86±1% vs 86±1%,p=0.42 n=1934 ITT n=1755 per protocol Median: 43 months Disease-free Survival: CLND vs. observation 68±1% vs 63±1%,p=0.05 Nonsentinel node metastases, identified in 11.5% of the patients in the dissection group, were an independent prognostic factor for recurrence (HR 1.78; p=0.005). Faries MB et al., NEJM
28 MSLT-2 Results (n=1755) Overall Survival: CLND vs Observation 86±1% vs 86±1%,p=0.42 n=1934 ITT n=1755 per protocol Median: 43 months Disease-free Survival: CLND vs. observation 68±1% vs 63±1%,p= Faries MB et al., NEJM 2017
29 MSLT-2 Conclusions Overall Survival: CLND vs Observation 86±1% vs 86±1%,p=0.42 n=1934 ITT n=1755 per protocol Median: 43 months Immediate CLND increased the rate of regional control and provided prognostic information but did not increase melanoma-specific survival in patients with SN metastases Disease-free Survival: CLND vs. observation 68±1% vs 63±1%,p=0.05 Faries MB et al., NEJM
30 Comparisons CLND DeCOG-SLT MSLT-2 UNC DeCOG SLT (n = 240) MSLT II (n=824) UNC (n=209) Breslow Depth (mm) median (range) 2.4 ( ) 2.1 ( ) 2.4 ( ) mean Not Available p= Ulceration n(%) present 90 (38) 316 (38.3) 86(41) absent 150 (63) 508(61.7) 123(59) p = NS p = NS SLN Met n(%) <=1mm 153 (63) 378 (46) 114 (54.6) >1mm 62 (26) 188 (23) 87 (41.6) size unknown 25(10) 258 (31) 8 (3.8) p=0.002 p=0.01 Total # SLN + n(%) (93) 678 (82) 167 (80) > 1 16 (7) 148 (18) 42 (20) unknown 2 (1) p<0.001 p = NS NSLN n(%) positive 43(18) x(11.5) 40 (22) negative 138 (58) 141 (78) unknown 59 (25) p = NS p<0.001 Time to Follow up (months) median (range) 33 (17 50) 43 40(6 196) 30
31 Comparisons CLND DeCOG-SLT MSLT-2 UNC DeCOG SLT (n = 240) MSLT II (n=824) UNC (n=209) Breslow Depth (mm) median (range) 2.4 ( ) 2.1 ( ) 2.4 ( ) mean Not Available p= Ulceration n(%) present 90 (38) 316 (38.3) 86(41) absent 150 (63) 508(61.7) 123(59) p = NS p = NS SLN Met n(%) <=1mm 153 (63) 378 (46) 114 (54.6) >1mm 62 (26) 188 (23) 87 (41.6) size unknown 25(10) 258 (31) 8 (3.8) p=0.002 p=0.01 Total # SLN + n(%) (93) 678 (82) 167 (80) > 1 16 (7) 148 (18) 42 (20) unknown 2 (1) p<0.001 p = NS NSLN n(%) positive 43(18) x(11.5) 40 (22) negative 138 (58) 141 (78) unknown 59 (25) p = NS p<0.001 Time to Follow up (months) median (range) 33 (17 50) 43 40(6 196) 31
 present 90 (38) 316 (38.3) 86(41) absent 150 (63) 508(61.7) 123(59) p = NS p = NS SLN Met n(%) <=1mm 153 (63) 378 (46) 114 (54.6) >1mm 62 (26) 188 (23) 87 (41.")
32 Comparisons CLND DeCOG-SLT MSLT-2 UNC DeCOG SLT (n = 240) MSLT II (n=824) UNC (n=209) Breslow Depth (mm) median (range) 2.4 ( ) 2.1 ( ) 2.4 ( ) mean Not Available p= Ulceration n(%) present 90 (38) 316 (38.3) 86(41) absent 150 (63) 508(61.7) 123(59) p = NS p = NS SLN Met n(%) <=1mm 153 (63) 378 (46) 114 (54.6) >1mm 62 (26) 188 (23) 87 (41.6) size unknown 25(10) 258 (31) 8 (3.8) p=0.002 p=0.01 Total # SLN + n(%) (93) 678 (82) 167 (80) > 1 16 (7) 148 (18) 42 (20) unknown 2 (1) p<0.001 p = NS NSLN n(%) positive 43(18) x(11.5) 40 (22) negative 138 (58) 141 (78) unknown 59 (25) p = NS p<0.001 Time to Follow up (months) median (range) 33 (17 50) 43 40(6 196) 32
33 UNC Overall Survival Kaplan Meier method disease specific survival SN metastases <=1mm vs >1mm. Log-rank tests performed to 5 yr survival <=1mm = 84% 5 yr survival >1mm = 41% 33




34 UNC Overall Survival 34
35 Comparisons CLND DeCOG-SLT MSLT-2 UNC DeCOG SLT (n = 240) MSLT II (n=824) UNC (n=209) Breslow Depth (mm) median (range) 2.4 ( ) 2.1 ( ) 2.4 ( ) mean Not Available p= Ulceration n(%) present 90 (38) 316 (38.3) 86(41) absent 150 (63) 508(61.7) 123(59) p = NS p = NS SLN Met n(%) <=1mm 153 (63) 378 (46) 114 (54.6) >1mm 62 (26) 188 (23) 87 (41.6) size unknown 25(10) 258 (31) 8 (3.8) p=0.002 p=0.01 Total # SLN + n(%) (93) 678 (82) 167 (80) > 1 16 (7) 148 (18) 42 (20) unknown 2 (1) p<0.001 p = NS NSLN n(%) positive 43(18) x(11.5) 40 (22) negative 138 (58) 141 (78) unknown 59 (25) p = NS p<0.001 Time to Follow up (months) median (range) 33 (17 50) 43 40(6 196) 35
36 UNC Approach 2018 SN indications: T1a: No T1b: Yes T2/T3: SOC T4a/b: Offer routinely after PET/CT CLND vs US surveillance T1/T2, SN met < 1mm: Offer active surveillance T1/T2, SN met > 1mm: Tilt towards CLND T3/T4, SN+: CLND + systemic therapy 36
37 Final Thoughts Gershenwald et al.,
38 AJCC March Melanoma 22, th Edition Newly created international database housed: MD Anderson Stages I-III N > 49,000 patients US, Australia, Europe (Italy, Greece, Spain) Additional sites onboarding for planned tool development Thirteenth Given the unprecedented changes in the still rapidly evolving landscape of the management of patients with stage IV melanoma, the Melanoma Expert Panel concluded that it was premature to embark on a broad-based analytic initiative involving data from patients with stage IV disease Gershenwald et al., CA Cancer J Clin. Dec

39 Thank you Nancy Thomas Ben Schmidt Surg Onc Fellow UNC Dermatology & Skin Cancer Center NC Cancer Hospital 39
40 Adjuvant Ipilimumab in Stage III Melanoma IIIa=186 IIIb=420 IIIc=345 OS due EORTC NCT , n=951 Eggermont Lancet Oncol
41 UNC Disease Specific Survival Kaplan Meier method depicting disease specific survival grouped by patients with melanoma sentinel lymph node metastases <=1mm vs >1mm. Log-rank tests performed to compare groups. 5 year survival <=1mm = 87% 5 year survival >1mm = 54% Events: death with disease present 41
42 Types of Recurrence Local Regional Distant <=1mm n(%) 3 (3) 13 (11) 19 (17) median time to recurrence (months) >1mm n(%) 0 (0) 26 (30) 19 (22) median time to recurrence (months)

43 43
44 New World Order: 8 th Edition AJCC Melanoma Staging System David W. Ollila MD James and Jesse Millis Distinguished Professor of Surgery University of North Carolina, Chapel Hill Disclosures: None May 14, 2018
45 Melanoma Staging Principle communication tool Clinician patient Clinician clinician Registry reporting Risk stratification defines groups of patients Treatment recommendations often stage-based Development of prognostic models and clinical tools Clinical trial eligibility, stratification, analysis 2


46 AJCC Melanoma Staging System 7 th Edition 8 th Edition Charles Balch Jeff Gershenwald Richard A. Scolyer MIA 3 CA Cancer J Clin Nov;67(6):


47 AJCC Melanoma 8 th Edition Chair: Jeff Gershenwald Vice Chair: Richard Scolyer Statistician: Ken Hess Expert Panel:» 25 other members worldwide Jeff Gershenwald Ken Hess 8th edition 4
48 AJCC Melanoma 8 th Edition Newly created international database housed: MD Anderson Stages I-III N > 49,000 patients US, Australia, Europe (Italy, Greece, Spain) Additional sites onboarding for planned tool development Gershenwald et al., CA Cancer J Clin. Dec

49 Gershenwald et al., CA Cancer J Clin. Dec
 prior to AJCC F2F Pathology staging")

50 International Melanoma Pathology Study Group Meet at UCSF(Nov 2015) prior to AJCC F2F Pathology staging issues discussed/voted AJCC pathologists took consensus to F2F Phil LeBoit Ray Barnhill Richard Scolyer Alistair Cochran 7
51 2010 AJCC T Classification 7 th Edition Stage Breslow Thickness (mm) Definition T a: No ulceration and <1 mitosis/mm 2 b: Ulceration or >1 mitosis/mm 2 T a: No ulceration b: Ulceration T a: No ulceration b: Ulceration T4 > 4.00 a: No ulceration b: Ulceration Balch, Gershenwald, Soong, et al. JCO 2009
52 Primary Tumor (T) - AJCC 8 th Edition Gershenwald et al., CA Cancer J Clin. Dec

53 Primary Tumor (T) - AJCC 8 th Edition Gershenwald et al., CA Cancer J Clin. Dec
54 Melanoma Institute Australia Data: n=


55 Richard A. Scolyer MIA Richard A. Scolyer MIA 12

56 13
57 Primary Tumor (T) - AJCC 8th Edition Tumors >1mm: Impracticality/imprecision measurements to nearest 0.01mm Recorded to nearest 0.1mm (not 0.01mm) Tumors 1mm: May be measured to nearest 0.01mm Reported rounded to the nearest 0.1mm 0.75mm to 0.84mm reported 0.8mm (T1b) 1.04mm reported 1.0mm (T1b) Gershenwald et al., CA Cancer J Clin. Dec 2017
 Tumors 1mm: May be measured to nearest 0.01mm Reported rounded to the nearest 0.1mm 0.75mm to 0.84mm reported 0.8mm (T1b) 1.04mm reported 1.")
58 Primary Tumor (T) - AJCC 8th Edition Tumors >1mm: Impracticality/imprecision measurements to nearest 0.01mm Recorded to nearest 0.1mm (not 0.01mm) Tumors 1mm: May be measured to nearest 0.01mm Reported rounded to the nearest 0.1mm 0.75mm to 0.84mm reported 0.8mm (T1b) 1.04mm reported 1.0mm (T1b) Implications for sentinel node procedure
59 Melanoma Specific Survival T category T stage group Gershenwald et al., CA Cancer J Clin. Dec
60 Occasional Difficulties in Staging Difficulty in determining Breslow thickness?ulceration vs trauma vs artefact What is a microsatellite? What happened to mitotic rate? 17



61 Difficulty in determining Breslow thickness H & E S100 Courtesy of Richard A. Scolyer MIA 18

62 Include Periadnexal Extension? Richard A. Scolyer MIA NO NO 19
63 Ulceration Courtesy of Richard A. Scolyer20 MIA
64 Ulceration Distinguish true ulceration from artefact Presence of fibrin or granulation tissue useful Iatrogenic vs non-iatrogenic may be difficult Courtesy of Richard A. Scolyer21 MIA

65 AJCC 7th edition: Microsatellites DEF: tumor nest >0.05mm in diameter that is separated by normal dermis from the main invasive component of melanoma by a distance of >0.5mm Problem: what appears a microsatellite on 1 section may be contiguous with primary on levels Balch, Gershenwald, Soong, et al. JCO

66 AJCC 7 th edition: Microsatellites DEF: tumor nest >0.05mm in diameter that is separated by normal dermis from the main invasive component of melanoma by a distance of >0.5mm Problem: what appears a microsatellite on 1 section may be contiguous with primary on levels Balch, Gershenwald, Soong, et al. JCO

67 AJCC 8 th edition: Microsatellites Microscopic metastasis adjacent/deep to 1 0 Identified on path exam primary tumor site Must be discontinuous from the primary Not separated only by fibrosis or inflammation No minimal size or distance from primary Balch, Gershenwald, Soong, et al. JCO
68 AJCC 8 th Edition N-category Regional nodes Non-nodal regional disease In-transits (ITM) Satellites Microsatellites Microsatellites/satellites/ITM grouped together for staging purposes Gershenwald et al., CA Cancer J Clin. Dec

69 Tumor Mitotic Rate (TMR) TMR: strongly independent prognostic factor Prognostic across as a continuous variable Removed as T1 staging criterion in 8 th ed» Fewer melanomas with TMR=0 after 7 th AJCC edition» Erroneously: only prognostic 0 vs 1 Record TMR in all T1-T4 primary melanomas Gershenwald et al., CA Cancer J Clin. Dec


70 Melanoma Specific Survival TMR *mitotic rate, mitoses/mm 2 Gershenwald et al., CA Cancer J Clin. Dec
71 MSS:T- and N-categories N1+ 28 Gershenwald et al., CA Cancer J Clin. Dec 2017

72 29
73 MSS according to Stage III Groups 8 th Edition international melanoma database Melanoma-Specific Survival Probability IIIA: N = 1006, 5yr = 93%, 10yr = 88% IIIB: N = 1170, 5yr = 83%, 10yr = 77% IIIC: N = 2201, 5yr = 69%, 10yr = 60% IIID: N = 205, 5yr = 32%, 10yr = 24% stage groups Significant heterogeneity Substage stratification: both T- and N-category criteria Tumor thickness Ulceration # LNs Microsat/ITM/satellites Years Since Diagnosis Gershenwald et al., CA Cancer J Clin. Dec
74 Comparisons of 7 th vs. 8th Balch, JCO 2009 Gershenwald et al.,
75 Comparisons of 7 th vs. 8th Balch, JCO 2009 Gershenwald et al.,
76 Comparisons of 7 th vs. 8th Balch, JCO 2009 Gershenwald et al.,

77 T category Summary: T Stage Breslow, Ulceration T stage group Gershenwald et al., CA Cancer J Clin. Dec

78 Summary: Stage III Melanoma-Specific Survival Probability IIIA: N = 1006, 5yr = 93%, 10yr = 88% IIIB: N = 1170, 5yr = 83%, 10yr = 77% IIIC: N = 2201, 5yr = 69%, 10yr = 60% IIID: N = 205, 5yr = 32%, 10yr = 24% Years Since Diagnosis Gershenwald et al., CA Cancer J Clin. Dec
79 AJCC 8th Edition: Factors NOT Included Primary tumour mitotic rate Level of invasion TILs Lymphovascular invasion Neurotropism SNs: Max dimension-largest deposit Extranodal extension in + nodes Richard A. Scolyer MIA 36
80 AJCC Melanoma 8 th Edition Newly created international database housed: MD Anderson Stages I-III N > 49,000 patients US, Australia, Europe (Italy, Greece, Spain) Additional sites onboarding for planned tool development Gershenwald et al., CA Cancer J Clin. Dec

81 AJCC Melanoma 8 th Edition Newly created international database housed: MD Anderson Stages I-III N > 49,000 patients US, Australia, Europe (Italy, Greece, Spain) Additional sites onboarding for planned tool development Given the unprecedented changes in the still rapidly evolving landscape of the management of patients with stage IV melanoma, the Melanoma Expert Panel concluded that it was premature to embark on a broad-based analytic initiative involving data with stage IV melanoma Gershenwald et al., CA Cancer J Clin. Dec
")


82 AJCC March Melanoma 22, th Edition Newly created international database housed: MD Anderson Stages I-III N > 49,000 patients US, Australia, Europe (Italy, Greece, Spain) Additional sites onboarding for planned tool development Thirteenth Given the unprecedented changes in the still rapidly evolving landscape of the management of patients with stage IV melanoma, the Melanoma Expert Panel concluded that it was premature to embark on a broad-based analytic initiative involving data from patients with stage IV disease Gershenwald et al., CA Cancer J Clin. Dec

83 Thank you Nancy Thomas Richard Scolyer AJCC Data UNC Dermatology & Skin Cancer Center NC Cancer Hospital 40
Melanoma: Therapeutic Progress and the Improvements Continue
 Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
No Benefit to Routine Completion Lymphadenectomy for Sentinel Lymph Node Positive Melanoma
 No Benefit to Routine Completion Lymphadenectomy for Sentinel Lymph Node Positive Melanoma Michael Lowe, MD Assistant Professor of Surgery Winship Cancer Institute Emory University School of Medicine July
No Benefit to Routine Completion Lymphadenectomy for Sentinel Lymph Node Positive Melanoma Michael Lowe, MD Assistant Professor of Surgery Winship Cancer Institute Emory University School of Medicine July
Surgical Issues in Melanoma
 Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy
 American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective
 Procedure: An Oncologic Surgeon s Perspective") Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures
Rebecca Vogel, PGY-4 March 5, 2012
 Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
The New AJCC: 8 th Edition and Beyond. 8th Edition AJCC Melanoma Staging System. Jeffrey E. Gershenwald, MD, FACS. AJCC Physician to Physician
 AJCC Physician to Physician 8th Edition AJCC Melanoma Staging System Jeffrey E. Gershenwald, MD, FACS Dr. John M. Skibber Professor, Department of Surgical Oncology Professor, Department of Cancer Biology
AJCC Physician to Physician 8th Edition AJCC Melanoma Staging System Jeffrey E. Gershenwald, MD, FACS Dr. John M. Skibber Professor, Department of Surgical Oncology Professor, Department of Cancer Biology
Controversies and Questions in the Surgical Treatment of Melanoma
 Controversies and Questions in the Surgical Treatment of Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Division of Endocrine and Oncologic Surgery University of Pennsylvania School
Controversies and Questions in the Surgical Treatment of Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Division of Endocrine and Oncologic Surgery University of Pennsylvania School
When Do I Consider Myself Cured?
 The Melanoma Patient Symposium - Science to Survivorship When Do I Consider Myself Cured? 26 September 2009 Jeffrey E. Gershenwald, MD, FACS Professor of Surgery, Dept. of Surgical Oncology Professor,
The Melanoma Patient Symposium - Science to Survivorship When Do I Consider Myself Cured? 26 September 2009 Jeffrey E. Gershenwald, MD, FACS Professor of Surgery, Dept. of Surgical Oncology Professor,
Nodal Treatment in Melanoma: Snow to MSLT-II
 Nodal Treatment in Melanoma: Snow to MSLT-II Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Program Director, JWCI Complex General Surgical Oncology Fellowship Director,
Nodal Treatment in Melanoma: Snow to MSLT-II Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Program Director, JWCI Complex General Surgical Oncology Fellowship Director,
Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy
 Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy Dale Han, MD Assistant Professor Department of Surgery Section of Surgical Oncology No disclosures Background Desmoplastic melanoma (DM)
Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy Dale Han, MD Assistant Professor Department of Surgery Section of Surgical Oncology No disclosures Background Desmoplastic melanoma (DM)
Update on SLN and Melanoma: DECOG and MSLT-II. Gordon H. Hafner, MD, FACS
 Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
Who is the Ideal Candidate for PEG Intron?
 Who is the Ideal Candidate for PEG Intron? Sanjiv S. Agarwala, MD Chief, Oncology & Hematology St. Luke s Cancer Center Professor, Temple University School of Medicine Philadelphia, PA, USA Overview Introduction
Who is the Ideal Candidate for PEG Intron? Sanjiv S. Agarwala, MD Chief, Oncology & Hematology St. Luke s Cancer Center Professor, Temple University School of Medicine Philadelphia, PA, USA Overview Introduction
47. Melanoma of the Skin
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
AJCC 8 Implementation January 1, 2018 Melanoma of the Skin. Suraj Venna
 AJCC 8 Implementation January 1, 2018 Melanoma of the Skin Suraj Venna Personalized Medicine AJCC 8 th Edition This Time It s Personal Traditional AJCC (TNM) population-based analyses of large databases
AJCC 8 Implementation January 1, 2018 Melanoma of the Skin Suraj Venna Personalized Medicine AJCC 8 th Edition This Time It s Personal Traditional AJCC (TNM) population-based analyses of large databases
Surgical Treatment of Melanoma Across the Disease Spectrum:
 AOCD Annual Fall Meeting October 28 th, 2017 New Orleans, Louisiana Surgical Treatment of Melanoma Across the Disease Spectrum: Standards of Care and Evolving Paradigms Merrick Ross, M.D. Professor of
AOCD Annual Fall Meeting October 28 th, 2017 New Orleans, Louisiana Surgical Treatment of Melanoma Across the Disease Spectrum: Standards of Care and Evolving Paradigms Merrick Ross, M.D. Professor of
Report Back 12 th Canadian Melanoma Conference February 22 24, 2018
 1 Report Back 12 th Canadian Melanoma Conference February 22 24, 2018 2 Below is a report back of major themes gleaned from the 12 th Annual Canadian Melanoma Conference along with some photos, anecdotes,
1 Report Back 12 th Canadian Melanoma Conference February 22 24, 2018 2 Below is a report back of major themes gleaned from the 12 th Annual Canadian Melanoma Conference along with some photos, anecdotes,
Molecular Enhancement of Sentinel Node Evaluation
 Cochran Illustrations 060104 Molecular Enhancement of Sentinel Node Evaluation Alistair Cochran, MD and Rong Huang MD Departments of Pathology and Laboratory Medicine and Surgery, David Geffen School of
Cochran Illustrations 060104 Molecular Enhancement of Sentinel Node Evaluation Alistair Cochran, MD and Rong Huang MD Departments of Pathology and Laboratory Medicine and Surgery, David Geffen School of
Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients
 2018 AAD Annual Meeting, San Diego, CA Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients Susan M. Swetter, MD, FAAD Professor of Dermatology Director, Pigmented Lesion
2018 AAD Annual Meeting, San Diego, CA Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients Susan M. Swetter, MD, FAAD Professor of Dermatology Director, Pigmented Lesion
Melanoma Underwriting Presented at 2018 AHOU Conference. Hank George FALU
 Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Disclosures. SLNB for Melanoma 25/02/2014 SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION
 8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
Michael T. Tetzlaff MD, PhD
 American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival
 MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
DENOMINATOR: All melanoma pathology reports for primary malignant cutaneous melanoma
 Quality ID #397: Melanoma Reporting National Quality Strategy Domain: Communication and Care Coordination Meaningful Measure Area: Transfer of Health Information and Interoperability 2019 COLLECTION TYPE:
Quality ID #397: Melanoma Reporting National Quality Strategy Domain: Communication and Care Coordination Meaningful Measure Area: Transfer of Health Information and Interoperability 2019 COLLECTION TYPE:
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma. Michael T. Tetzlaff MD, PhD
 Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
Melanoma Update: 8th Edition of AJCC Staging System
 Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Sentinel Lymph Node Biopsy: Current Evidence for its Role in Managing Melanoma
 Sentinel Lymph Node Biopsy: Current Evidence for its Role in Managing Melanoma John A Zitelli MD Adjunct Clinical Associate Professor Dermatology, Otolaryngology, Plastic Surgery University of Pittsburgh
Sentinel Lymph Node Biopsy: Current Evidence for its Role in Managing Melanoma John A Zitelli MD Adjunct Clinical Associate Professor Dermatology, Otolaryngology, Plastic Surgery University of Pittsburgh
Melanoma Surgery Update James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division
 Melanoma Surgery Update 2018 James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division Surgery for Melanoma Mainstay of treatment for potentially
Melanoma Surgery Update 2018 James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division Surgery for Melanoma Mainstay of treatment for potentially
Update on Lymph Node Management in Melanoma
 Update on Lymph Node Management in Melanoma John T. Vetto MD, FACS Professor of Surgery Division of Surgical Oncology Oregon Health & Science University Portland, Oregon Lymph Nodes in Melanoma Outline
Update on Lymph Node Management in Melanoma John T. Vetto MD, FACS Professor of Surgery Division of Surgical Oncology Oregon Health & Science University Portland, Oregon Lymph Nodes in Melanoma Outline
Surgical Oncology Perspective of Melanoma
 Surgical Oncology Perspective of Melanoma Hans F. Schoellhammer, MD, FACS Assistant Clinical Professor Division of Surgical Oncology September 20, 2018 Nothing to disclose DISCLOSURE Discussion Objectives
Surgical Oncology Perspective of Melanoma Hans F. Schoellhammer, MD, FACS Assistant Clinical Professor Division of Surgical Oncology September 20, 2018 Nothing to disclose DISCLOSURE Discussion Objectives
Adjuvant Therapy of High Risk Melanoma
 Adjuvant Therapy of High Risk Melanoma William Sharfman, MD, FACP Associate Professor of Oncology and Dermatology Johns Hopkins University School of Medicine July 5, 2012 Adjuvant options for Stage IIB/C
Adjuvant Therapy of High Risk Melanoma William Sharfman, MD, FACP Associate Professor of Oncology and Dermatology Johns Hopkins University School of Medicine July 5, 2012 Adjuvant options for Stage IIB/C
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know
 Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current
Impact of Prognostic Factors
 Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Morphological characteristics of the primary tumor and micrometastases in sentinel lymph nodes as a predictor of melanoma progression
 Morphological characteristics of the primary tumor and micrometastases in sentinel lymph nodes as a predictor of melanoma progression M.N. Kukushkina, S.I. Korovin, O.I. Solodyannikova, G.G. Sukach, A.Yu.
Morphological characteristics of the primary tumor and micrometastases in sentinel lymph nodes as a predictor of melanoma progression M.N. Kukushkina, S.I. Korovin, O.I. Solodyannikova, G.G. Sukach, A.Yu.
Topics for Discussion. Malignant Melanoma. Surgical Treatment. Current Treatment of Cutaneous Melanoma 5/17/2013. Lymph Regional nodes:
 Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
UvA-DARE (Digital Academic Repository) Who needs adjuvant therapy in stage III melanoma? Madu, M.F. Link to publication
 Who needs adjuvant therapy in stage III melanoma? Madu, M.F. Link to publication") UvA-DARE (Digital Academic Repository) Who needs adjuvant therapy in stage III melanoma? Madu, M.F. Link to publication Citation for published version (APA): Madu, M. F. (2018). Who needs adjuvant therapy
UvA-DARE (Digital Academic Repository) Who needs adjuvant therapy in stage III melanoma? Madu, M.F. Link to publication Citation for published version (APA): Madu, M. F. (2018). Who needs adjuvant therapy
What are the new AJCC Staging System changes, and how will they affect my patients?
 What are the new AJCC Staging System changes, and how will they affect my patients? Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine University of Pennsylvania
What are the new AJCC Staging System changes, and how will they affect my patients? Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine University of Pennsylvania
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment. Justin Rivard MD, MSc, FRCSC September 21, 2018
 You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
Should we still be performing IHC on all sentinel nodes?
 Miami Breast Cancer Conference 31 st Annual Conference March 8, 2014 Should we still be performing IHC on all sentinel nodes? Donald L. Weaver, MD Professor of Pathology University of Vermont USA Miami
Miami Breast Cancer Conference 31 st Annual Conference March 8, 2014 Should we still be performing IHC on all sentinel nodes? Donald L. Weaver, MD Professor of Pathology University of Vermont USA Miami
Lymph node ratio is an important and independent prognostic factor for patients with stage III melanoma.
 Thomas Jefferson University Jefferson Digital Commons Department of Surgery Faculty Papers Department of Surgery 1-1-2012 Lymph node ratio is an important and independent prognostic factor for patients
Thomas Jefferson University Jefferson Digital Commons Department of Surgery Faculty Papers Department of Surgery 1-1-2012 Lymph node ratio is an important and independent prognostic factor for patients
Primary Cutaneous Melanoma Pathology Reporting Proforma DD MM YYYY. *Tumour site. *Specimen laterality. *Specimen type
 Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD
 Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Melanoma Quality Reporting
 Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Sentinel Lymph Node Biopsy: Past and Present Implications for the Management of Cutaneous Melanoma with Nodal Metastasis
 American Journal of Clinical Dermatology (2018) 19 (Suppl 1):S24 S30 https://doi.org/10.1007/s40257-018-0379-0 REVIEW ARTICLE Sentinel Lymph Node Biopsy: Past and Present Implications for the Management
American Journal of Clinical Dermatology (2018) 19 (Suppl 1):S24 S30 https://doi.org/10.1007/s40257-018-0379-0 REVIEW ARTICLE Sentinel Lymph Node Biopsy: Past and Present Implications for the Management
Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases
 Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases Faruk Tas, Sidika Kurul, Hakan Camlica and Erkan Topuz Institute of Oncology, Istanbul University, Istanbul, Turkey Received
Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases Faruk Tas, Sidika Kurul, Hakan Camlica and Erkan Topuz Institute of Oncology, Istanbul University, Istanbul, Turkey Received
3/23/2017. Disclosure of Relevant Financial Relationships. Pathologic Staging Updates in Breast Cancer. Pathologic Staging Updates Breast Cancer
 Pathologic Staging Updates in Breast Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
Pathologic Staging Updates in Breast Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
Research Article Prediction of Sentinel Node Status and Clinical Outcome in a Melanoma Centre
 Skin Cancer Volume 2013, Article ID 904701, 7 pages http://dx.doi.org/10.1155/2013/904701 Research Article Prediction of Sentinel Node Status and Clinical Outcome in a Melanoma Centre Vera Teixeira, 1
Skin Cancer Volume 2013, Article ID 904701, 7 pages http://dx.doi.org/10.1155/2013/904701 Research Article Prediction of Sentinel Node Status and Clinical Outcome in a Melanoma Centre Vera Teixeira, 1
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection
 The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
Surgery for Melanoma and What s on the Horizon
 and What s on the Horizon Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background/Overview 76,870 cases of melanoma estimated
and What s on the Horizon Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background/Overview 76,870 cases of melanoma estimated
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
Clinical Case Conference Melanoma
 Clinical Case Conference Melanoma Epidemiology ~60,000 cases and 8,000 deaths per year in US Caucasian:African American = 10:1 15% arise from existing nevi 91% are cutaneous 15% are LN+ at presentation
Clinical Case Conference Melanoma Epidemiology ~60,000 cases and 8,000 deaths per year in US Caucasian:African American = 10:1 15% arise from existing nevi 91% are cutaneous 15% are LN+ at presentation
Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature. Sasha Jenkins
 Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature By Sasha Jenkins A Master s Paper submitted to the faculty of the University of North Carolina at Chapel Hill in
Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature By Sasha Jenkins A Master s Paper submitted to the faculty of the University of North Carolina at Chapel Hill in
MELANOMA: THE BEST OF THE YEAR Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone
 MELANOMA: THE BEST OF THE YEAR 2018 Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone The Best of the Year 2018: MELANOMA CHIRURGIA TERAPIA ADIUVANTE TERAPIA PER MALATTIA AVANZATA The Best of the Year
MELANOMA: THE BEST OF THE YEAR 2018 Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone The Best of the Year 2018: MELANOMA CHIRURGIA TERAPIA ADIUVANTE TERAPIA PER MALATTIA AVANZATA The Best of the Year
1
 www.clinicaloncology.com.ua 1 Prognostic factors of appearing micrometastases in sentinel lymph nodes in skin melanoma M.N.Kukushkina, S.I.Korovin, O.I.Solodyannikova, G.G.Sukach, A.Yu.Palivets, A.N.Potorocha,
www.clinicaloncology.com.ua 1 Prognostic factors of appearing micrometastases in sentinel lymph nodes in skin melanoma M.N.Kukushkina, S.I.Korovin, O.I.Solodyannikova, G.G.Sukach, A.Yu.Palivets, A.N.Potorocha,
Tumor Mitotic Rate Added to the Equation: Melanoma Prognostic Factors Changed?
 Ann Surg Oncol (2015) 22:2978 2987 DOI 10.1245/s10434-014-4349-3 ORIGINAL ARTICLE MELANOMAS Tumor Mitotic Rate Added to the Equation: Melanoma Prognostic Factors Changed? A Single-Institution Database
Ann Surg Oncol (2015) 22:2978 2987 DOI 10.1245/s10434-014-4349-3 ORIGINAL ARTICLE MELANOMAS Tumor Mitotic Rate Added to the Equation: Melanoma Prognostic Factors Changed? A Single-Institution Database
Prognosis of Sentinel Node Staged Patients with Primary Cutaneous Melanoma
 Prognosis of Sentinel Node Staged Patients with Primary Cutaneous Melanoma Otmar Elsaeßer 1., Ulrike Leiter 1 *., Petra G. Buettner 2, Thomas K. Eigentler 1, Friedegund Meier 1, Benjamin Weide 1, Gisela
Prognosis of Sentinel Node Staged Patients with Primary Cutaneous Melanoma Otmar Elsaeßer 1., Ulrike Leiter 1 *., Petra G. Buettner 2, Thomas K. Eigentler 1, Friedegund Meier 1, Benjamin Weide 1, Gisela
Talk to Your Doctor. Fact Sheet
 Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
NCCN Guidelines for Cutaneous Melanoma V Meeting on 06/20/18
 ME-1, ME-3, ME-B Submission from Castle Biosciences, Inc (05/30/18) to consider inclusion of the DecisionDx-Melanoma test in the guidelines as a prognostic test that provides stratification according to
ME-1, ME-3, ME-B Submission from Castle Biosciences, Inc (05/30/18) to consider inclusion of the DecisionDx-Melanoma test in the guidelines as a prognostic test that provides stratification according to
Precision Surgery for Melanoma
 Precision Surgery for Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background 87,110 cases of melanoma estimated in
Precision Surgery for Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background 87,110 cases of melanoma estimated in
46. Merkel Cell Carcinoma
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact
 Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact Bjørn Hagen, MD, PhD St Olavs Hospital Trondheim University Hospital Trondheim, Norway Endometrial Cancer (EC) The most
Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact Bjørn Hagen, MD, PhD St Olavs Hospital Trondheim University Hospital Trondheim, Norway Endometrial Cancer (EC) The most
Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove)
") Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove) Provincial Cancer Care Conference 2018 Ralph P.W. Wong MD FRCPC St Boniface Site Director
Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove) Provincial Cancer Care Conference 2018 Ralph P.W. Wong MD FRCPC St Boniface Site Director
Citation for published version (APA): Francken, A. B. (2007). Primary and metastatic melanoma: aspects of follow-up and staging s.n.
: Francken, A. B. (2007). Primary and metastatic melanoma: aspects of follow-up and staging s.n.") University of Groningen Primary and metastatic melanoma Francken, Anne Brecht IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check
University of Groningen Primary and metastatic melanoma Francken, Anne Brecht IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check
Increasing Age Is Associated with Worse Prognostic Factors and Increased Distant Recurrences despite Fewer Sentinel Lymph Node Positives in Melanoma
 Increasing Age Is Associated with Worse Prognostic Factors and Increased Distant Recurrences despite Fewer Sentinel Lymph Node Positives in Melanoma A. J. Page, Emory University A. Li, Emory University
Increasing Age Is Associated with Worse Prognostic Factors and Increased Distant Recurrences despite Fewer Sentinel Lymph Node Positives in Melanoma A. J. Page, Emory University A. Li, Emory University
PAPER. Prognostic Information From Sentinel Lymph Node Biopsy in Patients With Thick Melanoma
 PAPER Prognostic Information From Sentinel Lymph Node Biopsy in Patients With Thick Melanoma Charles R. Scoggins, MD, MBA; Adrianne L. Bowen, MD; Robert C. Martin II, MD, PhD; Michael J. Edwards, MD; Douglas
PAPER Prognostic Information From Sentinel Lymph Node Biopsy in Patients With Thick Melanoma Charles R. Scoggins, MD, MBA; Adrianne L. Bowen, MD; Robert C. Martin II, MD, PhD; Michael J. Edwards, MD; Douglas
Completing the Puzzle AJCC TNM Staging Breast. Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017
 Completing the Puzzle AJCC TNM Staging Breast Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017 OBJECTIVES Understanding of Breast TNM staging Identify clinical
Completing the Puzzle AJCC TNM Staging Breast Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017 OBJECTIVES Understanding of Breast TNM staging Identify clinical
Quality ID #397: Melanoma Reporting National Quality Strategy Domain: Communication and Care Coordination
 Quality ID #397: Melanoma Reporting National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Outcome DESCRIPTION: Pathology
Quality ID #397: Melanoma Reporting National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Outcome DESCRIPTION: Pathology
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
EORTC Melanoma Group
 EORTC Melanoma Group : Prospective registry of Sentinel Node (SN) positive melanoma patients with minimal SN tumor burden who undergo Completion Lymph Node Dissection (CLND) or Nodal Observation. EORTC
EORTC Melanoma Group : Prospective registry of Sentinel Node (SN) positive melanoma patients with minimal SN tumor burden who undergo Completion Lymph Node Dissection (CLND) or Nodal Observation. EORTC
Management of the patient with Lymph Node Involvement. Michael A Henderson Peter MacCallum Cancer Center Univ of Melbourne
 Management of the patient with Lymph Node Involvement Michael A Henderson Peter MacCallum Cancer Center Univ of Melbourne Lymph Node Field Recurrence Most important prognostic factor for early stage melanoma
Management of the patient with Lymph Node Involvement Michael A Henderson Peter MacCallum Cancer Center Univ of Melbourne Lymph Node Field Recurrence Most important prognostic factor for early stage melanoma
NAACCR Webinar Series 1
 Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Therapeutic Lymph Node Dissection in Melanoma: Different Prognosis for Different Macrometastasis Sites?
 Ann Surg Oncol (01) 19:91 91 DOI.14/s44-01-401- ORIGINAL ARTICLE MELANOMAS Therapeutic Lymph Node Dissection in Melanoma: Different Prognosis for Different Macrometastasis Sites? K. P. Wevers, MD, E. Bastiaannet,
Ann Surg Oncol (01) 19:91 91 DOI.14/s44-01-401- ORIGINAL ARTICLE MELANOMAS Therapeutic Lymph Node Dissection in Melanoma: Different Prognosis for Different Macrometastasis Sites? K. P. Wevers, MD, E. Bastiaannet,
Seventh Edition Staging 2017 Melanoma. Overview. This webinar is sponsored by. the Centers for Disease Control and Prevention.
 Seventh Edition Staging 2017 Melanoma Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express written
Seventh Edition Staging 2017 Melanoma Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express written
NEW SURGICAL APPROACHES TO MELANOMA THERAPY
 NEW SURGICAL APPROACHES TO MELANOMA THERAPY Melanoma 2003: New Insights Into Therapy & Treatment Douglas L. Fraker, M.D. University of Pennsylvania Surgical Treatment of Melanoma Primary resection margins
NEW SURGICAL APPROACHES TO MELANOMA THERAPY Melanoma 2003: New Insights Into Therapy & Treatment Douglas L. Fraker, M.D. University of Pennsylvania Surgical Treatment of Melanoma Primary resection margins
Descriptor Definition Author s notes TNM descriptors Required only if applicable; select all that apply multiple foci of invasive carcinoma
 S5.01 The tumour stage and stage grouping must be recorded to the extent possible, based on the AJCC Cancer Staging Manual (7 th Edition). 11 (See Tables S5.01a and S5.01b below.) Table S5.01a AJCC breast
S5.01 The tumour stage and stage grouping must be recorded to the extent possible, based on the AJCC Cancer Staging Manual (7 th Edition). 11 (See Tables S5.01a and S5.01b below.) Table S5.01a AJCC breast
ORIGINAL ARTICLE MELANOMAS. Ann Surg Oncol (2015) 22: DOI /s z
 22: DOI /s z") Ann Surg Oncol (2015) 22:2972 2977 DOI 10.1245/s10434-015-4615-z ORIGINAL ARTICLE MELANOMAS Detailed Pathological Examination of Completion Node Dissection Specimens and Outcome in Melanoma Patients with
Ann Surg Oncol (2015) 22:2972 2977 DOI 10.1245/s10434-015-4615-z ORIGINAL ARTICLE MELANOMAS Detailed Pathological Examination of Completion Node Dissection Specimens and Outcome in Melanoma Patients with
ORIGINAL ARTICLE PROGNOSTIC IMPLICATION OF SENTINEL LYMPH NODE BIOPSY IN CUTANEOUS HEAD AND NECK MELANOMA
 ORIGINAL ARTICLE PROGNOSTIC IMPLICATION OF SENTINEL LYMPH NODE BIOPSY IN CUTANEOUS HEAD AND NECK MELANOMA Benjamin E. Saltman, MD, 1 Ian Ganly, MD, 2 Snehal G. Patel, MD, 2 Daniel G. Coit, MD, 3 Mary Sue
ORIGINAL ARTICLE PROGNOSTIC IMPLICATION OF SENTINEL LYMPH NODE BIOPSY IN CUTANEOUS HEAD AND NECK MELANOMA Benjamin E. Saltman, MD, 1 Ian Ganly, MD, 2 Snehal G. Patel, MD, 2 Daniel G. Coit, MD, 3 Mary Sue
Predictive Factors for the Positivity of the Sentinel Lymph Node in Malignant Melanoma
 ORIGINAL RESEARCH SURGERY // ANATOMO-PATHOLOGY Predictive Factors for the Positivity of the Sentinel Lymph Node in Malignant Melanoma Călin Crăciun, Orsolya Hankó- Bauer, Zalán Benedek, Sorin Sorlea, Marius
ORIGINAL RESEARCH SURGERY // ANATOMO-PATHOLOGY Predictive Factors for the Positivity of the Sentinel Lymph Node in Malignant Melanoma Călin Crăciun, Orsolya Hankó- Bauer, Zalán Benedek, Sorin Sorlea, Marius
Is There a Benefit to Sentinel Lymph Node Biopsy in Patients With T4 Melanoma?
 Is There a Benefit to Sentinel Lymph Node Biopsy in atients With T4 Melanoma? Csaba Gajdos, MD 1 ; Kent A. Griffith, MH, MS 2 ; Sandra L. Wong, MD 1 ; Timothy M. Johnson, MD 1,3 ; Alfred E. Chang, MD 1
Is There a Benefit to Sentinel Lymph Node Biopsy in atients With T4 Melanoma? Csaba Gajdos, MD 1 ; Kent A. Griffith, MH, MS 2 ; Sandra L. Wong, MD 1 ; Timothy M. Johnson, MD 1,3 ; Alfred E. Chang, MD 1
University of Groningen
 University of Groningen Nodular Histologic Subtype and Ulceration are Tumor Factors Associated with High Risk of Recurrence in Sentinel Node-Negative Melanoma Patients Faut, Marloes; Wevers, Kevin; van
University of Groningen Nodular Histologic Subtype and Ulceration are Tumor Factors Associated with High Risk of Recurrence in Sentinel Node-Negative Melanoma Patients Faut, Marloes; Wevers, Kevin; van
Michael T. Tetzlaff MD, PhD
 Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Measure #397: Melanoma Reporting National Quality Strategy Domain: Communication and Care Coordination
 Measure #397: Melanoma Reporting National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION: Pathology reports
Measure #397: Melanoma Reporting National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION: Pathology reports
Treatment and management of advanced melanoma: Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC
 Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
WHAT DOES THE PATHOLOGY REPORT MEAN?
 Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
J Clin Oncol 27: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 27 NUMBER 36 DECEMBER 2 29 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T From Johns Hopkins Medical Institutions, Baltimore, MD; The University of Texas M. D. Anderson Cancer Center,
VOLUME 27 NUMBER 36 DECEMBER 2 29 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T From Johns Hopkins Medical Institutions, Baltimore, MD; The University of Texas M. D. Anderson Cancer Center,
8th Edition of the TNM Classification for Lung Cancer. Proposed by the IASLC
 8th Edition of the TNM Classification for Lung Cancer Proposed by the IASLC Introduction Stage classification - provides consistency in nomenclature - improves understanding of anatomic extent of tumour
8th Edition of the TNM Classification for Lung Cancer Proposed by the IASLC Introduction Stage classification - provides consistency in nomenclature - improves understanding of anatomic extent of tumour
Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer
 - Official Statement - Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer Sentinel lymph node (SLN) biopsy has replaced axillary lymph node dissection (ALND) for the
- Official Statement - Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer Sentinel lymph node (SLN) biopsy has replaced axillary lymph node dissection (ALND) for the
The 8th Edition Lung Cancer Stage Classification
 The 8th Edition Lung Cancer Stage Classification Elwyn Cabebe, M.D. Medical Oncology, Hematology, and Hospice and Palliative Care Valley Medical Oncology Consultants Director of Quality, Medical Oncology
The 8th Edition Lung Cancer Stage Classification Elwyn Cabebe, M.D. Medical Oncology, Hematology, and Hospice and Palliative Care Valley Medical Oncology Consultants Director of Quality, Medical Oncology
Thin Melanoma with Nodal Involvement: Analysis of Demographic, Pathologic, and Treatment Factors with Regard to Prognosis
 Ann Surg Oncol DOI 10.1245/s10434-016-5646-9 ORIGINAL ARTICLE MELANOMAS Thin Melanoma with Nodal Involvement: Analysis of Demographic, Pathologic, and Treatment Factors with Regard to Prognosis Giorgos
Ann Surg Oncol DOI 10.1245/s10434-016-5646-9 ORIGINAL ARTICLE MELANOMAS Thin Melanoma with Nodal Involvement: Analysis of Demographic, Pathologic, and Treatment Factors with Regard to Prognosis Giorgos
Melanoma. Kaushik Mukherjee MD A. Scott Pearson MD
 Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
6/22/2015. Original Paradigm. Correlating Histology and Molecular Findings in Melanocytic Neoplasms
 6 Correlating Histology and Molecular Findings in Melanocytic Neoplasms Pedram Gerami MD, Associate Professor of Dermatology and Pediatrics at Northwestern University Disclosures: I have been a consultant
6 Correlating Histology and Molecular Findings in Melanocytic Neoplasms Pedram Gerami MD, Associate Professor of Dermatology and Pediatrics at Northwestern University Disclosures: I have been a consultant
M D..,., M. M P.. P H., H, F. F A.. A C..S..
 Implications of NSABP B-32 and Loco-Regional Therapy Considerations After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H, F.A.C.S. Professor of Surgery Northeastern Ohio Medical University Medical
Implications of NSABP B-32 and Loco-Regional Therapy Considerations After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H, F.A.C.S. Professor of Surgery Northeastern Ohio Medical University Medical
Sentinel Node Biopsy. Is There Any Role for Axillary Dissection? JCCNB Nov 20, Stephen B. Edge, MD
 Sentinel Node Biopsy Is There Any Role for Axillary Dissection? JCCNB Nov 20, 2010 Tokyo, Japan Stephen B. Edge, MD Roswell Park Cancer Institute University at Buffalo Buffalo, NY USA SNB with Clinically
Sentinel Node Biopsy Is There Any Role for Axillary Dissection? JCCNB Nov 20, 2010 Tokyo, Japan Stephen B. Edge, MD Roswell Park Cancer Institute University at Buffalo Buffalo, NY USA SNB with Clinically
Epithelial Cancer- NMSC & Melanoma
 Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Radionuclide detection of sentinel lymph node
 Radionuclide detection of sentinel lymph node Sophia I. Koukouraki Assoc. Professor Department of Nuclear Medicine Medicine School, University of Crete 1 BACKGROUND The prognosis of malignant disease is
Radionuclide detection of sentinel lymph node Sophia I. Koukouraki Assoc. Professor Department of Nuclear Medicine Medicine School, University of Crete 1 BACKGROUND The prognosis of malignant disease is
STAGE CATEGORY DEFINITIONS
 CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
Johan Lyth, J Hansson, C Ingvar, E Mansson-Brahme, P Naredi, U Stierner, G Wagenius and C Lindholm. Linköping University Post Print
 Prognostic subclassifications of T1 cutaneous melanomas based on ulceration, tumour thickness and Clark s level of invasion: results of a population-based study from the Swedish Melanoma Register Johan
Prognostic subclassifications of T1 cutaneous melanomas based on ulceration, tumour thickness and Clark s level of invasion: results of a population-based study from the Swedish Melanoma Register Johan
Printed by Martina Huckova on 10/3/2011 3:04:54 PM. For personal use only. Not approved for distribution. Copyright 2011 National Comprehensive
 Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level