Harmesh Naik, MD. GME Presentation to Family Practice Residents October 16, 2013.
|
|
|
- Kelley Rice
- 6 years ago
- Views:
Transcription

1 Harmesh Naik, MD. GME Presentation to Family Practice Residents October 16, 2013.
2 Lymphoma: Lympho-proliferative disorders arising from lymphocytes Heterogeneous group of disorders Differing patterns of behaviors and response to treatment One of the most curable and treatable malignancy Lymphoma biology and management has led to several major breakthroughs in cancer treatments
3 Blood cell development
4 Incidence Lymphoma incidence is increasing About 79,000 new cases with 20,000 deaths from lymphoma in 2013 per ACS estimate About 9200 cases annually with about 1180 deaths annually (2013 estimate)

5 Lymphomas T cell/nk cell 10% HL 10% B Cell NHL 80%
6 Ann Arbor staging : Summary I: Involvement of a single nodal site or local involvement of single extra nodal site - IE II: Two or more nodal areas on same side of diaphragm III: Involvement of nodal areas on both sides of diaphragm IV: Diffuse or disseminated involvement of one or more extra lymphatic organs, with or without associated lymph node involvement
7 B symptoms A notation of B symptoms is made along with stage Unexplained loss of more than 10% of body weight in the 6 months before diagnosis. Unexplained fever with temperatures above 38 C. Drenching night sweats.
8
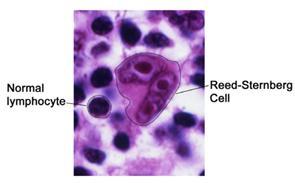
9 HODGKIN S LYMPHOMA B cell neoplasm Characteristic cell is Sternberg Reed cell Disease spread is generally contiguous Exploratory laparotomy and splenectomy are no longer used for staging Over 75% of cases are potentially cured
10
11 RISK FACTORS Etiology is unknown Association with EB virus Risk of HD is increased 3 fold in people with history of infectious mononucleosis About half of Hodgkin nodes show evidence of EBV DNA in Stenberg reed cells genome Not all Hodgkin s cases are EBV positive.
12 SYMPTOMS / SIGNS Pain less lymphadenopathy Splenomegaly B symptoms: Fever, drenching night seats, weight loss Pruritus Pain in nodal area after alcohol consumption
13 HISTOLOGY: WHO classification Classical Hodgkin s lymphoma 95% of all cases Nodular Lymphocyte predominant Hodgkin s lymphoma -About 5% of total cases % cases Classic Lym Predom
14 STAGING WORK UP History and physical examination Excisional lymph node biopsy with histology and immune phenotype CBC diff, Liver enzyme testing, LDH, Sed rate Chest x-ray or CT chest CT abdomen and pelvis PET scan Bone marrow aspiration and biopsy (if advanced stage or B symptoms)
15 ADDITIONAL MEASURES Fertility preservation evaluation if applicable Pulmonary function testing Cardiac ejection fraction tests HIV testing Vaccination if splenectomy is planned or splenic RT is given
16 PROGNOSIC FACTORS: International prognostic Score (IPS) FDG PET scan after two cycles of ABVD
17 TREATMENT Curable in majority of patients Combination chemotherapy is standard of care for Classical Hodgkin s disease Number of courses of chemotherapy varies with stage Involved field radiotherapy is used following short course of chemotherapy in early stage Hodgkin s disease Role of radiotherapy is undergoing reevaluation.
18 TREATMENT Early favorable: Stage IA and IIA non- bulky favorable Short course of chemotherapy (2-4 cycles ) followed by involved field radiation therapy (20 Gy) Cure rate of 90-95% Early unfavorable Stage I and II with bulky disease / Bulky disease : Six cycles of chemotherapy followed by involved field Radiation
19 TREATMENT Advanced disease: Stage III and IV up to 30% are at risk of death ABVD is standard of care in United States ABVD is more effective and less toxic than MOPP Stanford V and BEACOPP regimens are designed to reduce cumulative toxicity of several drugs and to improve outcomes Role of consolidation RT in patients with stage III and IV disease remain controversial
20 RELAPSED HODGKIN S LYMPHOMA Initial RT alone ABVD -long term disease free survival in 50-80% Initial ABVD Salvage second line regimens (ICE etc.) 15% 5 year disease free survival High dose therapy and stem cell transplant in selected scenarios
21 Nodular Lymphocyte predominant Hodgkin s lymphoma - treatment Early stage / localized Involved field RT is used for early stage local disease Relapse/Recurrence after local RT: Single agent Rituximab (70-100% Response rate) Or with combination ABVD Disseminated Generally it is treated with ABVD. Rituximab has been used successfully as well in some situations.
22 Purpose of long term follow up: To monitor for relapse To monitor for late effects of treatment MDS Leukemia Hypothyroidism Premature coronary artery disease Pulmonary toxicity -Bleomycin Infertility To monitor for new primary cancer
23
24 NHL: Cell types NHL B cell T cell NK cell
25 NHL: Clinical types Indolent lymphoma: (Slow growing, low grade, incurable) Aggressive lymphoma: ( fast growing, intermediate grade, potential curable) Highly aggressive (high grade, very fast growing, potential curable)
26 Working formulation classification (Old) Low grade Intermediate grade High grade
27 WHO classification: B cell Precursor B-cell neoplasm: precursor B-acute lymphoblastic leukemia/lymphoblastic lymphoma (LBL). Peripheral B-cell neoplasms. B-cell chronic lymphocytic leukemia/small lymphocytic lymphoma. B-cell prolymphocytic leukemia. Lymphoplasmacytic lymphoma/immunocytoma. Mantle cell lymphoma. Follicular lymphoma. Extranodal marginal zone B-cell lymphoma of mucosa-associated lymphatic tissue (MALT) type. Nodal marginal zone B-cell lymphoma (± monocytoid B-cells). Splenic marginal zone lymphoma (± villous lymphocytes). Hairy cell leukemia. Plasmacytoma/plasma cell myeloma. Diffuse large B-cell lymphoma. Burkitt lymphoma.
28 WHO classification: T cell T-cell and putative NK-cell neoplasms Precursor T-cell neoplasm: precursor T-acute lymphoblastic leukemia/lbl. Peripheral T-cell and NK-cell neoplasms. T-cell chronic lymphocytic leukemia/prolymphocytic leukemia. T-cell granular lymphocytic leukemia. Mycosis fungoides/sézary syndrome. Peripheral T-cell lymphoma, not otherwise characterized. Hepatosplenic gamma/delta T-cell lymphoma. Subcutaneous panniculitis-like T-cell lymphoma. Angioimmunoblastic T-cell lymphoma. Extranodal T-/NK-cell lymphoma, nasal type. Enteropathy-type intestinal T-cell lymphoma. Adult T-cell lymphoma/leukemia (human T-lymphotrophic virus [HTLV] 1+). Anaplastic large cell lymphoma, primary systemic type. Anaplastic large cell lymphoma, primary cutaneous type. Aggressive NK-cell leukemia.
29 RISK FACTORS Etiology is unknown for most cases Suspected but not conclusively proven: Pesticides, Chemicals, Smoking, Hair dyes, toxins Immuno compromised state increase risk of NHL Drug treatments: Cyclosporine, OKT 3 in transplant patients, etc. Infections: HIV Inherited immune defects Collagen vascular diseases: Rheumatoid arthritis Stem cell transplantation or solid organ transplantation
30 Association between infectious agent and specific type of lymphoma Epstein Barr virus Hodgkin s lymphoma Post transplant lympho-proliferative disorders (PTLD) Human Herpes virus 8 Body cavity lymphoma Castleman disease HIV related Kaposi s sarcoma Hepatitis C virus Immunocytoma Splenic marginal zone lymphoma Human T cell Lymphoma virus Adult T cell leukemia/lymphoma Helicobacter pylori Chlamydia Psitacci Campylobacter jejuni Borrelia burgdorferi Gastric mucosa associated lymphoid tissue lymphoma (MALTOMA) Orbital adnexal lymphoma Immunoproliferative small bowel disease Cutaneous MALT lymphoma
31 DIAGNOSIS Excisional node biopsy is preferred for histology and flow cytometry FNA- high false negative Core biopsy helpful at times but may not provide adequate histology Bone marrow biopsy Flow cytometry and molecular genetic studies are increasingly useful in diagnosis
32 STAGING WORK UP History and physical examination CBC diff, Liver enzyme testing, LDH CT chest CT abdomen and pelvis PET scan Bone marrow aspiration and biopsy
33 STAGING SYSTEM Ann Arbor staging system NHL often presents at advanced stage. Ann Arbor staging system is less relevant for NHL then for HL.
34
35 Indolent (Low grade) NHL Small lymphocytic lymphoma (SLL) / Chronic lymphocytic leukemia (CLL) Follicular lymphoma - grades I and II Marginal zone lymphoma (MZL) Lympho-plasmacytic lymphoma - LPL (Immunocytoma and Waldenstorm s Macroglobulinemia)
36 Indolent (Low grade) NHL Relatively better prognosis Median survival up to 10 years on average Most are non curable Responsive to treatment, however, has constant rate of recurrence Bone marrow involvement is seen in up to 40% indolent lymphoma
37 BCL-2 Rearrangement of the bcl-2 gene is present in more than 90% of patients with follicular lymphoma Over-expression of the bcl-2 protein is associated with the inability to eradicate the lymphoma by inhibiting apoptosis Immortality gene
38 Follicular Lymphoma International Prognostic Index [FLIPI] An international index for follicular lymphoma identified five significant risk factors prognostic of overall survival (OS): Age ( 60 y vs. >60 y). Serum lactate dehydrogenase (LDH) (normal vs. elevated). Stage (stage I or stage II vs. stage III or stage IV). Hemoglobin level ( 120 g/l vs. <120 g/l). Number of nodal areas ( 4 vs. >4).
39 Prognosis: FLIPI index Risk factors and 10 yr OS or more 10 yr OS
40 Follicular lymphoma Grade I and II are treated like indolent lymphoma Grade III are treated like Diffuse large cell lymphoma
41 TREATMENT CHOICES In general there is no consensus on best treatment. Many options are available including observation.
42 Indications for treatment Cancer related symptoms B symptoms Threatened organ function Steady progression Transformation Cytopenias Recurrent infections Patient preference
43 Indolent lymphoma: treatment options Clinical trials Observation- watchful waiting Local RT Rituximab Chemotherapy Chemotherapy-immunotherapy Radio-immunotherapy
44 Treatment selection: Role of molecular markers Alemtuzumab preferred for SLL patients with del 17 p (p 53 mutation)
45 High dose therapy / stem cell transplant For refractory follicular lymphoma cases Generally not curative Under evaluation for upfront therapy
46 Treatment observations Chemotherapy + Rituximab might be better (6-13% benefit at 4 years per meta analysis) in symptomatic patients Rituximab maintenance may improve progression free survival (given for 2 years)
47 Marginal zone lymphoma Stomach MALTOMA Anti H. Pylori therapy is effective t(11,18) predicts poor response to anti H. Pylori treatment Rituximab, Local radiation etc. are reserved for refractory disease Non gastric extra nodal MALTOMAs Surgery + RT Chemo - immunotherapy
48 Splenic marginal zone lymphoma Rituximab very effective Chemo-immunotherapy Splenectomy may produce prolonged remission Chemotherapy might be less effective Hepatitis C treatment may induce remission
49 Remission duration: Indolent NHL First line Second line Third line Fourth line
50 HAIRY CELL LEUKEMIA Splenomegaly, Leukopenia / pancytopenia and marrow infiltration with hairy cells (cytoplasm projections)- TRAP stain positive cells Marrow is fibrotic and hard to aspirate ( Dry tap is common) Purine analogues (Cladarabine or Pentostatin) are effective in inducing prolonged remission lasting for up to 8-12 years Cure is not expected like other indolent lymphomas
51 Waldenström s macroglobulinemia Lymphoplasmacytic lymphoma usually associated with a monoclonal serum paraprotein of immunoglobulin M (IgM) type Hyper viscosity syndrome : Requires plasmapheresis General management is similar to that of other low-grade lymphomas
52 Immune cytopenias in NHL ITP and AIHA Prednisone IVIG Rituximab Splenectomy for refractory cases Chemotherapy Pure red cell aplasia Prednisone ATG or Cyclosporine
53 Recurrent infections in NHL IVIG may help in selected cases particularly with infections from encapsulated organisms

54
55 DIFFUSE LARGE CELL B CELL LYMPHOMA (DBCL) Most common NHL 30% -35% of total B cells are positive for CD 19 and CD 20 Most present with rapidly developing masses, systemic symptoms or weight loss IPI is used to estimate prognosis and to classify patient in to risk groups
56 Aggressive NHL Diffuse large cell B cell lymphoma (DBCL) Mantle cell lymphoma (MCL) Burkitt s lymphoma Lymphoblastic lymphoma
57 DIFFUSE LARGE CELL B CELL LYMPHOMA (DBCL): Localized DBCL About 20% cases Stage I or non bulky stage II Potentially Curable R-CHOP x 3 with Radiation is used commonly in USA after SWOG trial
58 DIFFUSE LARGE CELL B CELL LYMPHOMA (DBCL): Advanced DBCL CHOP alone % CR and plateau at DFS at around 30% R-CHOP versus CHOP: R-CHOP improved CR, TTP and overall survival in GELA study (Rituximab improves cure rate by about 10-15%) R-CHOP is current standard of care for DBCL More than half can be cured with R-CHOP
59 DIFFUSE LARGE CELL B CELL LYMPHOMA (DBCL): Relapsed DBCL Re-induction with aggressive chemotherapy regimen such as RICE remission is of short duration and few are cured Consolidation stem cell transplantation may cure some relapsed patients with chemo-sensitive disease Stem cell transplant is less effective for primary refractory disease Repeat biopsy may help since 10-15% may have lower grade follicular recurrence
60 MANTLE CELL LYMPHOMA (MCL) Characterized by t (11,14) translocation and over expression of BCL 1 cycling D1 protein May have diffuse bowel involvement (lymphomatous polyposis) Median survival is shorter than other lymphomas Doxorubicin based chemotherapy may not cure MCL Hyper CVAD followed by High dose therapy and stem cell transplantation in first CR is considered better option and is recommended in fit patients
61 BURKITT LYMPHOMA Highly aggressive lymphoma with explosive presentation Starry sky pattern on histology All cases possess c-myc oncogene at band 8q24 {associated with t (8,14) mostly but sometimes with t(2,8) or t (8, 22) } Common in pediatric population ( Endemic in Africa jaw tumors and associated with EBV) Most common lymphoma in AIDS patients Non endemic Burkit s is seen in US GI tract (ileo-cecal mass) is commonly involved LDH is very high
62 BURKITT LYMPHOMA Very intensive treatment regimen (R-hyper CVD or R-CODOX-M/IVAC) and CNS prophylaxis may cure some patients (60% -74% DFS at 5 years in adults) Fatal tumor lysis is possibility precautions are necessary Stem cell transplantation is recommended for those in first CR with high risk of recurrence (Stages III or IV, high LDH and tumor masses more than 10 cm)
63 PRIMARY CNS LYMPHOMA Aggressive B cell lymphoma in cranio-spinal axis without systemic disease Seen Denovo or in immuno compromised patients Age over 60 and HIV are poor prognosticators Whole brain RT is standard but unsatisfactory treatment CHOP does not work well RT with or without chemotherapy is neurotoxic Radiation sparing regimens: Chemotherapy alone with high dose Methotrexate and Leucovorin rescues is being tried with better response than RT.
64 LYMPHOBLASATIC LYMPHOMA Highly aggressive lymphoma of precursor T or B cells Explosive onset: Commonly with blasts in blood, marrow, mediastinal and other adenopathy, younger age, cytopenia. About 30% experience CNS involvement Induction therapy: Intensive multi-agent chemotherapy in hospital setting. Hyper CVAD results in 90% CR in low risk patients Consolidation: Stem cell translation CNS prophylaxis and radiation to bulky tumor are important components of treatment Testis and CNS are sanctuary sites Testicular RT is incorporated in treatment protocols
65
66 CUTANEOUS T CELL LYMPHOMA CTCL (Mycosis Fungoides) Indolent T cell (helper cell CD 4 phenotype) lymphoma of skin Waxing and waning eczematous skin patches or plaques for long periods (5-15 years) Advanced disease: Nodular tumors with ulceration or systemic visceral involvement Treatment options are many including PUVA (Psoralen and ultraviolet A therapy), local radiation, retinoids, interferon, Denilukin IL2 fusion toxin, topical chemotherapy or purine analogues or liposomal doxorubicin or Vorinostat) Patient can die from infections good skin care and antibiotics are important components
67 CUTANEOUS T CELL LYMPHOMA CTCL (Mycosis Fungoides) Sezary syndrome: Generalized erythema and circulating Sezary cells in blood median survival is short about 2 years with Sezary syndrome The only curative therapy is allergenic stem cell transplant option for a small number of patients
68 PLEASE SEE HANDOUT FOR MORE DETAILED INFORMATION

69
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Indolent Lymphomas. Dr. Melissa Toupin The Ottawa Hospital
 Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Indolent Lymphomas: Current. Dr. Laurie Sehn
 Indolent Lymphomas: Current Dr. Laurie Sehn Why does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with current standard
Indolent Lymphomas: Current Dr. Laurie Sehn Why does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with current standard
Lymphatic system component
 Introduction Lymphatic system component Statistics Overview Lymphoma Non Hodgkin s Lymphoma Non- Hodgkin's is a type of cancer that originates in the lymphatic system. It is estimated to be the sixth most
Introduction Lymphatic system component Statistics Overview Lymphoma Non Hodgkin s Lymphoma Non- Hodgkin's is a type of cancer that originates in the lymphatic system. It is estimated to be the sixth most
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center
 LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center Lymphoma is cancer of the lymphatic system. The lymphatic system is made up of organs all over the body that make up and store cells
LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center Lymphoma is cancer of the lymphatic system. The lymphatic system is made up of organs all over the body that make up and store cells
WHO Classification. B-cell chronic lymphocytic leukemia/small T-cell granular lymphocytic leukemia
 Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
LEUKAEMIA and LYMPHOMA. Dr Mubarak Abdelrahman Assistant Professor Jazan University
 LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
Lymphoid Neoplasms. Sylvie Freeman Department of Clinical Immunology, University of Birmingham
 Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
Non-Hodgkin lymphoma
 Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Lymphoma: The Basics. Dr. Douglas Stewart
 Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Aggressive Lymphomas - Current. Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre
 Aggressive Lymphomas - Current Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre Conflicts of interest I have no conflicts of interest to declare Outline What does aggressive lymphoma
Aggressive Lymphomas - Current Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre Conflicts of interest I have no conflicts of interest to declare Outline What does aggressive lymphoma
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
Understanding your diagnosis. Dr Graham Collins Consultant Haemtologist Oxford University Hospitals
 Understanding your diagnosis Dr Graham Collins Consultant Haemtologist Oxford University Hospitals Common questions I get asked What is lymphoma? What subtype do I have and what does that mean? What are
Understanding your diagnosis Dr Graham Collins Consultant Haemtologist Oxford University Hospitals Common questions I get asked What is lymphoma? What subtype do I have and what does that mean? What are
Head and Neck: DLBCL
 Head and Neck: DLBCL Nikhil G. Thaker Chelsea C. Pinnix Valerie K. Reed Bouthaina S. Dabaja Department of Radiation Oncology MD Anderson Cancer Center Case 60 yo male Presented with right cervical LAD
Head and Neck: DLBCL Nikhil G. Thaker Chelsea C. Pinnix Valerie K. Reed Bouthaina S. Dabaja Department of Radiation Oncology MD Anderson Cancer Center Case 60 yo male Presented with right cervical LAD
Change Summary - Form 2018 (R3) 1 of 12
 1 of 12") Summary - Form 2018 (R3) 1 of 12 Form Question Number (r3) Type Description New Text Previous Text Today's date was removed 2018 N/A Today's Date Removed from Key Fields 2018 N/A HCT Type 2018 N/A Product
Summary - Form 2018 (R3) 1 of 12 Form Question Number (r3) Type Description New Text Previous Text Today's date was removed 2018 N/A Today's Date Removed from Key Fields 2018 N/A HCT Type 2018 N/A Product
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
LYMPHOMAS an overview of some subtypes of NHLs
 One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
Classifications of lymphomas
 Classifications of lymphomas Lukes and Collins Kiel classification Working formulation REAL classification (1994) WHO classification (2000) WHO CLASSIFICATIONF OF NEOPLASMS HAEMATOPETIC AND LYMPHOID TISSUES
Classifications of lymphomas Lukes and Collins Kiel classification Working formulation REAL classification (1994) WHO classification (2000) WHO CLASSIFICATIONF OF NEOPLASMS HAEMATOPETIC AND LYMPHOID TISSUES
2010 Hematopoietic and Lymphoid ICD-O Codes - Alphabetical List THIS TABLE REPLACES ALL ICD-O-3 Codes
 Acute basophilic leukemia 9870/3 Acute biphenotypic leukemia [OBS] 9805/3 Acute erythroid leukemia 9840/3 Acute megakaryoblastic leukemia 9910/3 Acute monoblastic and monocytic leukemia 9891/3 Acute myeloid
Acute basophilic leukemia 9870/3 Acute biphenotypic leukemia [OBS] 9805/3 Acute erythroid leukemia 9840/3 Acute megakaryoblastic leukemia 9910/3 Acute monoblastic and monocytic leukemia 9891/3 Acute myeloid
2012 Hematopoietic and Lymphoid ICD-O Codes - Numerical List THIS TABLE REPLACES ALL ICD-O-3 Codes
 Malignant lymphoma, NOS 9590/3 Non-Hodgkin lymphoma, NOS 9591/3 B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma 9596/3 Primary
Malignant lymphoma, NOS 9590/3 Non-Hodgkin lymphoma, NOS 9591/3 B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma 9596/3 Primary
Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma:
 1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
Non-Hodgkin Lymphoma in Clinically Difficult Situations
 Winship Cancer Institute of Emory University Non-Hodgkin Lymphoma in Clinically Difficult Situations James Armitage, MD Professor, Department of Internal Medicine Joe Shapiro Distinguished Chair of Oncology
Winship Cancer Institute of Emory University Non-Hodgkin Lymphoma in Clinically Difficult Situations James Armitage, MD Professor, Department of Internal Medicine Joe Shapiro Distinguished Chair of Oncology
Lymphoma and Myeloma Kris3ne Kra4s, M.D.
 Lymphoma and Myeloma Kris3ne Kra4s, M.D. Hematologic Malignancies Leukemia Malignancy of hematopoie3c cells Starts in bone marrow, can spread to blood, nodes Myeloid or lymphoid Acute or chronic Lymphoma
Lymphoma and Myeloma Kris3ne Kra4s, M.D. Hematologic Malignancies Leukemia Malignancy of hematopoie3c cells Starts in bone marrow, can spread to blood, nodes Myeloid or lymphoid Acute or chronic Lymphoma
Small B-cell (Histologically Low Grade) Lymphoma
 Lymphoma") Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
MANAGEMENT OF LYMPHOMAS
 MANAGEMENT OF LYMPHOMAS Challenges & Recommendations F. Chite Asirwa, MD. Internal Medicine Physician Medical Oncologist & Hematologist Director-AMPATH Oncology & Hematology @Kenya Physicians Association
MANAGEMENT OF LYMPHOMAS Challenges & Recommendations F. Chite Asirwa, MD. Internal Medicine Physician Medical Oncologist & Hematologist Director-AMPATH Oncology & Hematology @Kenya Physicians Association
Clinical Policy: Bendamustine (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307
 Reference Number: PA.CP.PHAR.307") Clinical Policy: (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that
Clinical Policy: (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that
B Cell Lymphoma: Aggressive
 B Cell Lymphoma: Aggressive UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Ibrutinib approved for mantle cell lymphoma as 2nd line therapy. - Aggressive lymphomas are a group of malignant
B Cell Lymphoma: Aggressive UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Ibrutinib approved for mantle cell lymphoma as 2nd line therapy. - Aggressive lymphomas are a group of malignant
Non-Hodgkin Lymphoma. Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract.
 Non-Hodgkin Lymphoma Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract. Protocol revision date: January 2005 No AJCC/UICC staging system Procedures Cytology
Non-Hodgkin Lymphoma Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract. Protocol revision date: January 2005 No AJCC/UICC staging system Procedures Cytology
What is a hematological malignancy? Hematology and Hematologic Malignancies. Etiology of hematological malignancies. Leukemias
 Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
During past decades, because of the lack of knowledge
 Staging and Classification of Lymphoma Ping Lu, MD In 2004, new cases of non-hodgkin s in the United States were estimated at 54,370, representing 4% of all cancers and resulting 4% of all cancer deaths,
Staging and Classification of Lymphoma Ping Lu, MD In 2004, new cases of non-hodgkin s in the United States were estimated at 54,370, representing 4% of all cancers and resulting 4% of all cancer deaths,
C r h ist s op o h p e h r e R. R F l F ow o er e s, s M D, D M S
 1 Christopher R. Flowers, MD, MS Associate Professor of Hematology and Medical Oncology Winship Cancer Institute Emory University School of Medicine Atlanta, Georgia 2 1 Anyone can get blood cancer One
1 Christopher R. Flowers, MD, MS Associate Professor of Hematology and Medical Oncology Winship Cancer Institute Emory University School of Medicine Atlanta, Georgia 2 1 Anyone can get blood cancer One
Bone Marrow. Procedures Blood Film Aspirate, Cell Block Trephine Biopsy, Touch Imprint
 Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Lymphomas and multiple myeloma 12/23/2018 1
 60 Lymphomas and multiple myeloma 12/23/2018 1 Lymphomas Lymphoma is cancer of the lymphatic system. Lymphomas are subdivided into two main categories: Hodgkin's lymphoma (HL) and non- Hodgkin's lymphoma
60 Lymphomas and multiple myeloma 12/23/2018 1 Lymphomas Lymphoma is cancer of the lymphatic system. Lymphomas are subdivided into two main categories: Hodgkin's lymphoma (HL) and non- Hodgkin's lymphoma
Lymphoma 101. Nathalie Johnson, MDPhD. Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University
 Lymphoma 101 Nathalie Johnson, MDPhD Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University Disclosures Consultant and Advisory boards for multiple companies
Lymphoma 101 Nathalie Johnson, MDPhD Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University Disclosures Consultant and Advisory boards for multiple companies
Aggressive NHL and Hodgkin Lymphoma. Dr. Carolyn Faught November 10, 2017
 Aggressive NHL and Hodgkin Lymphoma Dr. Carolyn Faught November 10, 2017 What does aggressive mean? Shorter duration of symptoms Generally need treatment at time of diagnosis Immediate, few days, few weeks
Aggressive NHL and Hodgkin Lymphoma Dr. Carolyn Faught November 10, 2017 What does aggressive mean? Shorter duration of symptoms Generally need treatment at time of diagnosis Immediate, few days, few weeks
FOLLICULARITY in LYMPHOMA
 FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes on the next page
 COME HOME Non-Hodgkin pathway development worksheet, v6 September 2014 1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes
COME HOME Non-Hodgkin pathway development worksheet, v6 September 2014 1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes
2012 by American Society of Hematology
 2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and
NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and
Update in Lymphoma Imaging
 Update in Lymphoma Imaging Victorine V. Muse, MD Lymphoma Update in Lymphoma Imaging Victorine V Muse, MD Heterogeneous group of lymphoid neoplasms divided into two broad histological categories Hodgkin
Update in Lymphoma Imaging Victorine V. Muse, MD Lymphoma Update in Lymphoma Imaging Victorine V Muse, MD Heterogeneous group of lymphoid neoplasms divided into two broad histological categories Hodgkin
HAEMATOLOGICAL MALIGNANCY
 HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
SURVIVORSHIP WITH LYMPHOMA APRIL SHAMY MD,CM JEWISH GENERAL HOSPITAL MCGILL UNIVERSITY
 SURVIVORSHIP WITH LYMPHOMA APRIL SHAMY MD,CM JEWISH GENERAL HOSPITAL MCGILL UNIVERSITY Some Statistics Approximately 1 in 2 Canadians develop cancer 25% of Canadians die of cancer 2009: 810,000 Canadians
SURVIVORSHIP WITH LYMPHOMA APRIL SHAMY MD,CM JEWISH GENERAL HOSPITAL MCGILL UNIVERSITY Some Statistics Approximately 1 in 2 Canadians develop cancer 25% of Canadians die of cancer 2009: 810,000 Canadians
Lymphocyte Predominant Hodgkin s Lymphoma. Case Presentation. How would you treat the patient?
 Lymphocyte Predominant Hodgkin s Lymphoma Wei Ai, MD, PhD Assistant Clinical Professor University of California, San Francisco January 2010 Case Presentation 32 yo male, diagnosed with stage IIIA lymphocyte
Lymphocyte Predominant Hodgkin s Lymphoma Wei Ai, MD, PhD Assistant Clinical Professor University of California, San Francisco January 2010 Case Presentation 32 yo male, diagnosed with stage IIIA lymphocyte
Combinations of morphology codes of haematological malignancies (HM) referring to the same tumour or to a potential transformation
 referring to the same tumour or to a potential transformation") Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas. Original Policy Date
 MP 7.03.13 Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013
MP 7.03.13 Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013
Patterns of Lymphoid Neoplasia in Peripheral Blood. Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure
 Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Lymphoma: What You Need to Know
 Lymphoma: What You Need to Know www.lymphoma.org.au Lymphoma What You Need to Know Whilst Lymphoma Australia (LA) has made every effort to confirm the accuracy of the information contained herein, it makes
Lymphoma: What You Need to Know www.lymphoma.org.au Lymphoma What You Need to Know Whilst Lymphoma Australia (LA) has made every effort to confirm the accuracy of the information contained herein, it makes
Blood Cancers. Blood Cells. Blood Cancers: Progress and Promise. Bone Marrow and Blood. Lymph Nodes and Spleen
 Blood Cancers: Progress and Promise Mike Barnett & Khaled Ramadan Division of Hematology Department of Medicine Providence Health Care & UBC Blood Cancers Significant health problem Arise from normal cells
Blood Cancers: Progress and Promise Mike Barnett & Khaled Ramadan Division of Hematology Department of Medicine Providence Health Care & UBC Blood Cancers Significant health problem Arise from normal cells
Patient underwent hemicolectomy: 7 x 4.5 cm intusscepted segment of ileum in colon - mucosal
 Extranodal Lymphomas Rena Buckstein Odette Cancer Center Case: JT 69 yo male COO software company PMHx: basal cell back, cholesterol Presents to ER with severe abdominal pain, bloody diarrhea x 2d In ER
Extranodal Lymphomas Rena Buckstein Odette Cancer Center Case: JT 69 yo male COO software company PMHx: basal cell back, cholesterol Presents to ER with severe abdominal pain, bloody diarrhea x 2d In ER
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
LYMPHOPROLIFERATIVE DISORDERS. Dr Mere Kende MBBS, MMED (Path), MACTM, MACRRM, MAACB Lecturer: SMHS, UPNG
, MACTM, MACRRM, MAACB Lecturer: SMHS, UPNG") LYMPHOPROLIFERATIVE DISORDERS Dr Mere Kende MBBS, MMED (Path), MACTM, MACRRM, MAACB Lecturer: SMHS, UPNG Outline What are lymphoproliferative Disorders? Examples of LPD Classification Causes Clinical Features
LYMPHOPROLIFERATIVE DISORDERS Dr Mere Kende MBBS, MMED (Path), MACTM, MACRRM, MAACB Lecturer: SMHS, UPNG Outline What are lymphoproliferative Disorders? Examples of LPD Classification Causes Clinical Features
Hodgkin's Lymphoma. Symptoms. Types
 Hodgkin's lymphoma (Hodgkin's disease) usually develops in the lymphatic system, a part of the body's immune system. This system carries disease-fighting white blood cells throughout the body. Lymph tissue
Hodgkin's lymphoma (Hodgkin's disease) usually develops in the lymphatic system, a part of the body's immune system. This system carries disease-fighting white blood cells throughout the body. Lymph tissue
Non-Hodgkin s Lymphoma
 Non-Hodgkin s Lympoma Non-Hodgkin s Lymphomas Janet H. Van Cleave MSN, ACNP-CS, CS, AOCN Acute Care Nurse Practitioner The Mount Sinai Medical Center of New York City Doctoral Student, Yale University
Non-Hodgkin s Lympoma Non-Hodgkin s Lymphomas Janet H. Van Cleave MSN, ACNP-CS, CS, AOCN Acute Care Nurse Practitioner The Mount Sinai Medical Center of New York City Doctoral Student, Yale University
Recent diagnostic and therapeutic innovations of T-cell-lymphoma. Prof. Nossrat Firusian, Recklinghausen, Germany
 Recent diagnostic and therapeutic innovations of T-cell-lymphoma Prof. Nossrat Firusian, Recklinghausen, Germany NODAL Angioimmunoblastic T-cell Lymphoma Peripheral T-cell-Lymphoma Anaplastic Large-cell-Lymphoma
Recent diagnostic and therapeutic innovations of T-cell-lymphoma Prof. Nossrat Firusian, Recklinghausen, Germany NODAL Angioimmunoblastic T-cell Lymphoma Peripheral T-cell-Lymphoma Anaplastic Large-cell-Lymphoma
HODGKIN LYMPHOMA Updated February 2016 by Dr. Manna (PGY 5 Hematology Resident, University of Calgary)
") HODGKIN LYMPHOMA Updated February 2016 by Dr. Manna (PGY 5 Hematology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff
HODGKIN LYMPHOMA Updated February 2016 by Dr. Manna (PGY 5 Hematology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff
The Lymphomas. An overview..
 The Lymphomas An overview.. Peter Anglin MD, FRCPC, MBA Stronach Regional Cancer Centre Newmarket, ON The lymphomas are an important part of the history of medicine 1666 Magpighi publishes first recorded
The Lymphomas An overview.. Peter Anglin MD, FRCPC, MBA Stronach Regional Cancer Centre Newmarket, ON The lymphomas are an important part of the history of medicine 1666 Magpighi publishes first recorded
Contents. vii. Preface... Acknowledgments... v xiii
 Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
HIV and Malignancy Alaka Deshpande, Himanshu Soni
 HIV and Malignancy Alaka Deshpande, Himanshu Soni Emergence of new infectious disease was documented in 1981. Within a short span of time it became a pandemic. It was Acquired Immunodeficiency Syndrome
HIV and Malignancy Alaka Deshpande, Himanshu Soni Emergence of new infectious disease was documented in 1981. Within a short span of time it became a pandemic. It was Acquired Immunodeficiency Syndrome
Hematologic Malignancies. Anna Schaal, RN, MSN, arnp Norris Cotton Cancer Center Lebanon, New Hampshire
 Hematologic Malignancies Anna Schaal, RN, MSN, arnp Norris Cotton Cancer Center Lebanon, New Hampshire Objectives At the end of the session, the oncology nurse will be able to: Explain the pathophysiology
Hematologic Malignancies Anna Schaal, RN, MSN, arnp Norris Cotton Cancer Center Lebanon, New Hampshire Objectives At the end of the session, the oncology nurse will be able to: Explain the pathophysiology
Lymphoma Read with the experts
 Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
LYMPHOMA DIAGNOSIS and PROGNOSIS. LC Lim Dept of Hematology Singapore General Hospital
 LYMPHOMA DIAGNOSIS and PROGNOSIS LC Lim Dept of Hematology Singapore General Hospital OUTLINE Accurate diagnosis Define subtype : WHO classification Staging : Defines extent of involvement Prognosis Determining
LYMPHOMA DIAGNOSIS and PROGNOSIS LC Lim Dept of Hematology Singapore General Hospital OUTLINE Accurate diagnosis Define subtype : WHO classification Staging : Defines extent of involvement Prognosis Determining
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113)
") Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
Clinical Practice Guidelines FOR THE DIAGNOSIS AND MANAGEMENT OF LYMPHOMA APPROVED BY
 Clinical Practice Guidelines FOR THE DIAGNOSIS AND MANAGEMENT OF LYMPHOMA APPROVED BY Clinical Practice Guidelines for the Diagnosis and Management of Lymphoma APPROVED BY THE NHMRC ON 8 DECEMBER 2005
Clinical Practice Guidelines FOR THE DIAGNOSIS AND MANAGEMENT OF LYMPHOMA APPROVED BY Clinical Practice Guidelines for the Diagnosis and Management of Lymphoma APPROVED BY THE NHMRC ON 8 DECEMBER 2005
A CASE OF PRIMARY THYROID LYMPHOMA. Prof Dr.Dilek Gogas Yavuz Marmara University School of Medicine Endocrinology and Metabolism Istanbul, Turkey
 A CASE OF PRIMARY THYROID LYMPHOMA Prof Dr.Dilek Gogas Yavuz Marmara University School of Medicine Endocrinology and Metabolism Istanbul, Turkey 38 year old female She recognized a mass in her right neck
A CASE OF PRIMARY THYROID LYMPHOMA Prof Dr.Dilek Gogas Yavuz Marmara University School of Medicine Endocrinology and Metabolism Istanbul, Turkey 38 year old female She recognized a mass in her right neck
Pediatric Oncology. Vlad Radulescu, MD
 Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
PET-imaging: when can it be used to direct lymphoma treatment?
 PET-imaging: when can it be used to direct lymphoma treatment? Luca Ceriani Nuclear Medicine and PET-CT centre Oncology Institute of Southern Switzerland Bellinzona Disclosure slide I declare no conflict
PET-imaging: when can it be used to direct lymphoma treatment? Luca Ceriani Nuclear Medicine and PET-CT centre Oncology Institute of Southern Switzerland Bellinzona Disclosure slide I declare no conflict
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma
 with classical Hodgkin lymphoma") PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
Rituximab and Combination Chemotherapy in Treating Patients With Non- Hodgkin's Lymphoma
 Page 1 of 5 Home Search Study Topics Glossary Search Full Text View Tabular View No Study Results Posted Related Studies Rituximab and Combination Chemotherapy in Treating Patients With Non- Hodgkin's
Page 1 of 5 Home Search Study Topics Glossary Search Full Text View Tabular View No Study Results Posted Related Studies Rituximab and Combination Chemotherapy in Treating Patients With Non- Hodgkin's
Overview of Cutaneous Lymphomas: Diagnosis and Staging. Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology
 Overview of Cutaneous Lymphomas: Diagnosis and Staging Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology Definition of Lymphoma A cancer or malignancy that comes from
Overview of Cutaneous Lymphomas: Diagnosis and Staging Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology Definition of Lymphoma A cancer or malignancy that comes from
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Corporate Medical Policy
 Corporate Medical Policy Hematopoietic Stem-Cell Transplant for Non-Hodgkin Lymphomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplant_for_non_hodgkin_lymphomas
Corporate Medical Policy Hematopoietic Stem-Cell Transplant for Non-Hodgkin Lymphomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplant_for_non_hodgkin_lymphomas
Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies
![Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies](/thumbs/90/104309591.jpg "Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies") Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies UNCONTROLLED WHEN PRINTED Note: NOSCAN Haematology MCN has approved the information contained within this document to guide
Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies UNCONTROLLED WHEN PRINTED Note: NOSCAN Haematology MCN has approved the information contained within this document to guide
 Page 1 of 9 Title Authored By Course No Contact Hours 2 ABCs of Lymphoma Anita Rothera RNC, BS, CDE LYM020108 Purpose The goal of this course is to help health care professionals learn about the different
Page 1 of 9 Title Authored By Course No Contact Hours 2 ABCs of Lymphoma Anita Rothera RNC, BS, CDE LYM020108 Purpose The goal of this course is to help health care professionals learn about the different
Hepatic Lymphoma Diagnosis An Algorithmic Approach
 Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
T-cell Lymphomas Biology and Management
 T-cell Lymphomas Biology and Management March-27-2017 Outline Epidemiology Initial Work-up International Prognostic Index Treatment of Diffuse Large B-cell Lymphoma: -Limited Stage -Advanced Stage Frontline:
T-cell Lymphomas Biology and Management March-27-2017 Outline Epidemiology Initial Work-up International Prognostic Index Treatment of Diffuse Large B-cell Lymphoma: -Limited Stage -Advanced Stage Frontline:
Printed by Martina Huckova on 10/3/2011 3:04:43 PM. For personal use only. Not approved for distribution. Copyright 2011 National Comprehensive
 NCCN Categories of Evidence and Consensus Category 1: The recommendation is based on high-level evidence (e.g. randomized controlled trials) and there is uniform NCCN consensus. Category 2A: The recommendation
NCCN Categories of Evidence and Consensus Category 1: The recommendation is based on high-level evidence (e.g. randomized controlled trials) and there is uniform NCCN consensus. Category 2A: The recommendation
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin s Lymphomas
 Hematopoietic Stem-Cell Transplantation for Non-Hodgkin s Lymphomas Policy Number: 8.01.20 Last Review: 7/2014 Origination: 7/2002 Next Review: 7/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin s Lymphomas Policy Number: 8.01.20 Last Review: 7/2014 Origination: 7/2002 Next Review: 7/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue
2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA
 2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA SUSQUEHANNA HEALTH David B. Nagel, M.D. April 11, 2008 Hodgkin s lymphoma was first described by Thomas Hodgkin in 1832. It remained an incurable malignancy until
2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA SUSQUEHANNA HEALTH David B. Nagel, M.D. April 11, 2008 Hodgkin s lymphoma was first described by Thomas Hodgkin in 1832. It remained an incurable malignancy until
Pathology of Hematopoietic and Lymphoid tissue
 CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
Pathology of the indolent B-cell lymphomas Elias Campo
 Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
BACKGROUND INFORMATION ON NON-HODGKIN S LYMPHOMA
 BACKGROUND INFORMATION ON NON-HODGKIN S LYMPHOMA General Non-Hodgkin s lymphomas (NHLs) encompass several unique malignant lymphoid disease entities that vary in clinical behavior, morphologic appearance,
BACKGROUND INFORMATION ON NON-HODGKIN S LYMPHOMA General Non-Hodgkin s lymphomas (NHLs) encompass several unique malignant lymphoid disease entities that vary in clinical behavior, morphologic appearance,
NICE guideline Published: 20 July 2016 nice.org.uk/guidance/ng52
 Non-Hodgkin s lymphoma: diagnosis and management NICE guideline Published: 20 July 2016 nice.org.uk/guidance/ng52 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Non-Hodgkin s lymphoma: diagnosis and management NICE guideline Published: 20 July 2016 nice.org.uk/guidance/ng52 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Hematopoietic Cell Transplantation for Non-Hodgkin's Lymphomas
 Medical Policy Manual Transplant, Policy No. 45.23 Hematopoietic Cell Transplantation for Non-Hodgkin's Lymphomas Next Review: September 2018 Last Review: December 2017 Effective: January 1, 2018 IMPORTANT
Medical Policy Manual Transplant, Policy No. 45.23 Hematopoietic Cell Transplantation for Non-Hodgkin's Lymphomas Next Review: September 2018 Last Review: December 2017 Effective: January 1, 2018 IMPORTANT
Pathology #07. Hussein Al-Sa di. Dr. Sohaib Al-Khatib. Mature B-Cell Neoplasm. 0 P a g e
 Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Pathology of Hematopoietic and Lymphoid tissue
 Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
 Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas Policy Number: Original Effective Date: MM.07.018 04/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO 03/27/2015 Section:
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas Policy Number: Original Effective Date: MM.07.018 04/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO 03/27/2015 Section:
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Parts 2 and 3
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Parts 2 and 3 NEOPLASTIC LYMPHOID DISEASES Introduction o The bone marrow is the source of all cells in the
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Parts 2 and 3 NEOPLASTIC LYMPHOID DISEASES Introduction o The bone marrow is the source of all cells in the
88-year-old Female with Lymphadenopathy. Faizi Ali, MD
 88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
Nephrology Grand Rounds
 Nephrology Grand Rounds PTLD in Kidney Transplantation Charles Le University of Colorado 6/15/12 Objectives Background Pathogenesis Epidemiology and Clinical Manifestation Incidence Risk Factors CNS Lymphoma
Nephrology Grand Rounds PTLD in Kidney Transplantation Charles Le University of Colorado 6/15/12 Objectives Background Pathogenesis Epidemiology and Clinical Manifestation Incidence Risk Factors CNS Lymphoma
Hematopoietic Stem-Cell & Clinical Coverage Policy No: 11A-11 Bone Marrow Transplantation Amended Date: March 1, 2017 For Non-Hodgkin s Lymphoma
 Hematopoietic Stem-Cell & Clinical Coverage Policy No: 11A-11 Bone Marrow Transplantation Amended Date: March 1, 2017 For Non-Hodgkin s Lymphoma Table of Contents 1.0 Description of the Procedure, Product,
Hematopoietic Stem-Cell & Clinical Coverage Policy No: 11A-11 Bone Marrow Transplantation Amended Date: March 1, 2017 For Non-Hodgkin s Lymphoma Table of Contents 1.0 Description of the Procedure, Product,
Indolent B-Cell Non-Hodgkin s Lymphomas
 Review Article [1] December 01, 1997 Myelodysplastic Syndromes [2] By John E. Seng, MD [3] and Bruce A. Peterson, MD [4] The indolent B-cell non-hodgkin s lymphomas are a diverse group of disorders that
Review Article [1] December 01, 1997 Myelodysplastic Syndromes [2] By John E. Seng, MD [3] and Bruce A. Peterson, MD [4] The indolent B-cell non-hodgkin s lymphomas are a diverse group of disorders that
Dr. Noelle O Rourke Beatson Oncology Centre, Glasgow RADIOTHERAPY FOR LYMPHOMA???
 Dr. Noelle O Rourke Beatson Oncology Centre, Glasgow RADIOTHERAPY FOR LYMPHOMA??? History of Radiotherapy 1895 Rontgen describes X-rays 1896 Becquerel radioactivity 1905 Radiation is used to treat tumours
Dr. Noelle O Rourke Beatson Oncology Centre, Glasgow RADIOTHERAPY FOR LYMPHOMA??? History of Radiotherapy 1895 Rontgen describes X-rays 1896 Becquerel radioactivity 1905 Radiation is used to treat tumours
Conflict of Interest Disclosure Form NAME :James O. Armitage, M.D AFFILIATION: University of Nebraska Medical Center
 What Is Personalized Medicine For Patients With Lymphoma? Conflict of Interest Disclosure Form NAME :James O. Armitage, M.D AFFILIATION: University of Nebraska Medical Center DISCLOSURE I have no potential
What Is Personalized Medicine For Patients With Lymphoma? Conflict of Interest Disclosure Form NAME :James O. Armitage, M.D AFFILIATION: University of Nebraska Medical Center DISCLOSURE I have no potential
Lymphoma in South East Asia
 Lymphoma in South East Asia 45-yo man presented with cervical LNs enlargement for 3 months He reported low grade fever in the evening with dry cough for 4 weeks He has no known medical history Positive
Lymphoma in South East Asia 45-yo man presented with cervical LNs enlargement for 3 months He reported low grade fever in the evening with dry cough for 4 weeks He has no known medical history Positive
Update: Non-Hodgkin s Lymphoma
 2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)