Rectal Cancer Location: the Surgical Perspective
|
|
|
- Gladys Barber
- 6 years ago
- Views:
Transcription


1 Rectal Cancer Location: the Surgical Perspective September 5, 2014 W. Donald Buie MD,MSc, FRCSC Associate Professor of Surgery University of Calgary I have no disclosures 1

2 Outline Surgical Anatomy review Location where is the tumour? Location and neoadjuvant therapy Location and surgery; LAR, APR or LE Location and surgeon experience 2

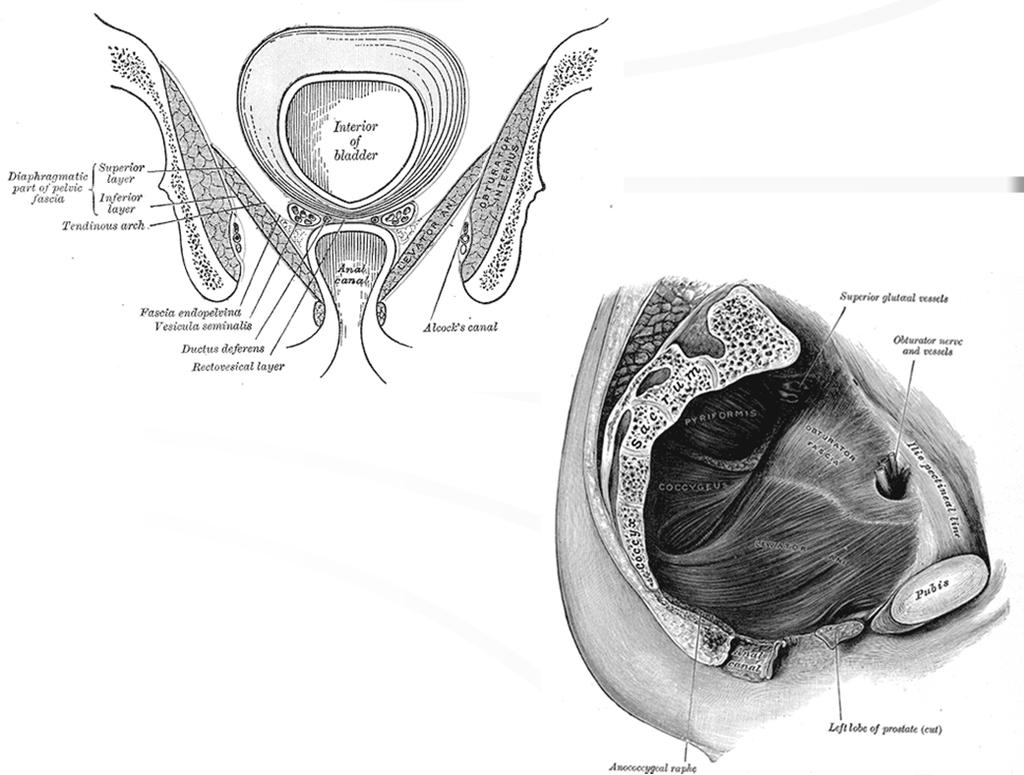
3 Male and Female pelvis Greys Anatomy Fig 402 and

4 Body Habitus The Mesorectum the rectum and its mesentery are a single fascia-enveloped unit, anatomically separate from surrounding pelvic structures Contains the blood vessels and lymphatics of the rectum It tapers down and ends just above the levator hiatus surgical violation of this anatomic package near a tumour may lead to a positive circumferential margin, a known predictor of local recurrence 4

5 Anterior vs posterior and Intraperitoneal vs extraperitoneal Anatomy summary Mesorectum ends just above the levator hiatus. The Anorectal junction abuts the levator hiatus Posterior tumours can be mobilized more as the rectal wall is longer More structures anteriorly Intraperitoneal vs extraperitoneal location is variable 5


6 11/09/2014 6

7 Why is location important? Height The height from the anal verge is of secondary importance What we really want to know is. proximity to anal sphincter proximity to pelvic floor levators Tumour height measured from Anal verge vs upper sphincter Shibab, Moran, Heald, Quirke, Brown. Eur Radiol 2009;19:


8 The levator and external sphincter are contiguous structures Shibab, Moran, Heald, Quirke, Brown. Eur Radiol 2009;19: The visible human project 8
9 The visible human project The visible human project 9

10 Tumour Clearance Shibab, Moran, Heald, Quirke, Brown. Eur Radiol 2009;19: Location (Local Regional Staging) 10
11 Staging if it would be possible to decide the category of the case before operating, this would be very useful information. Cuthbert Dukes, 1932 What do we want to know? Local regional variables: 1. Location of tumour 2. Depth of penetration of tumour through intestinal wall 3. Presence of regional lymph node metastasis 11
12 Why do we want to know it? Stage dictates THERAPY! Should we consider local excision? Should this patient have Neoadjuvant therapy? Stage dictates PROGNOSIS Local regional staging TRUS Most useful when considering local excision Limitations: Does not see mesorectal envelope well Tumour must be non obstructing Must be 10 cm or less for best images T-stage Accuracy 85% + Problem areas: T2 vs. T3 post radiation - edema vs. tumor overstaging (11-18%) and understaging (5-13%) 12
13 MRI The Gold Standard Technology evolving rapidly! Intramural staging improving (T1,T2) Evaluation of the integrity of the mesorectal envelope (CRM) Proximity of tumour to the surgical margin Proximity of the tumour to the sphincter/ levators Vascular invasion 13

 Specificity = 98% (215/219) NPV = 93% (215/230) MERCURY Study Group. BMJ.")
14 MRI Prediction of involved CRM 1 mm is considered positive; 1-2 mm borderline Beets-Tan 2004 MRI and Mesorectal Margin Histopathologic Examination Clear Involved Total MRI Prediction: Clear Involved Total Accuracy = 92% (226/245) Sensitivity = 42% (11/26) PPV = 73% (11/15) Specificity = 98% (215/219) NPV = 93% (215/230) MERCURY Study Group. BMJ. 2006;333:

15 Proximity of tumour to levators and sphincter complex myoma Location and neoadjuvant therapy 15
16 Pre-op Radiation Decreases Local Regional Recurrence and is Additive to Proper Surgical Technique Study Number Radiation Gy/ fraction Surgery alone Local Rec (%) Surgery/XRT Local Rec (%) St. Marks / * Bergen, Norway,1990 Manchester, / / * EORTC, / * MRC-2, / Stockholm, / * Sw Rectal Ca Trial, 1997 Dutch TME trial, 2002 (5yr) / * / * * Denotes results that are statistically significant Pre-op RT is more effective at decreasing local recurrence Study Number Rads 5 yr LR 5 yr OS Uppsala (SCRT) Pre-op Gy (1 wk) 13% 47% Post-op Gy (8 wk) 22%*(p=0.02) 40% NSABP R03 (CRT) Pre-op Gy 74% Post-op Gy 66% German Trial (LCCRT) Pre-op Gy 6% 76% Post-op Gy 13%*(p=0.006) 74% Note: Complete treatment in 90% of pre-op vs 50% of post-op Frykholm et al. DCR 1993; 36: Hyams et al. DCR 1997; 40: Sauer et al. N Engl J Med. 2004; 351:
17 What are the surgical advantages of Neoadjuvant Chemoradiation? Neoadjuvant LCCRT : Improve mobility - fixed / tethered tumours Improve circumferential margins Decrease tumour size (Bulky lesions)* Borderline reconstructable Large tumours small pelvis Male or obese Tumour regression may permit reanastomosis by improving technical issues (Sphincter sparing) We do not rely on neoadjuvant chemoradiation to sterilize the distal intramural margin How is MRI used to determine neoadjuvant therapy? Predicted CRM negative T1, T2, Early T3 < 5mm depth, N0 or N1; Predicted CRM negative but T3 > 5mm depth invasion T4, N2; Predicted CRM positive ( 1mm) includes all T2,T3,T4 below levators Requires an APR Lymph nodes near CRM Consider primary surgery neoadjuvant short course RT or long course CRT neoadjuvant long course CRT 17
18 Local Recurrence vs. Radial Margin in Rectal Cancer Adam, pt, 141 curative surgery Local Recurrence Positive 78 % CI (62-94) Local Recurrence Hazard ratio 12.2 CI ( ) Survival Hazard ratio 3.2 CI ( ) Negative 10% CI (4-16) 1 1 What is the Cost? Long term function following adjuvant radiotherapy Uppsala (Mean F/U 6.7 yrs) Stockholm I & II (mean F/U 15 yrs) Symptoms Sx (%) Sx/XRT (%) Sx (%) Sx/XRT (%) n=44 n=49 N=74 N=65 Frequency ( >5/d) 2 18 Loose liquid stool 2 25 Fecal urgency Fecal incontinence % 57% Use of pads 0 26 Differ. Stool/gas Social impact Antidiarrheal use Abdominal pain Dahlberg et.al. DCR. 1998; 41: Tenesmus 3 13 Pollack et.al. Br J Surg. 2006; 93:
19 Location and Surgery Should we consider local excision? Should this patient have a low anterior resection or an APR? Transanal Excision Suitable in 3-5% of pts. Criteria not well defined, but ideally: Distal 1/3 of rectum (except with TEM) Mobile (generally T1) < 1/3 circumference Polypoid > ulcerated Well / moderately well differentiated < 4cm in size No lymphovascular invasion No evidence of nodal metastases 19
20 RECTAL CANCER LOCAL EXCISION (trans anal excision) pro low morbidity/mortality avoids sexual/urinary/bowel dysfunction avoids colostomy con nodal status not pathologically assessed involved nodes not excised TMN - Total mesorectal neglect R Madoff Transanal Excision Local Recurrence Study / year No. of patients T1 Local Rec. T2 Local Rec. Stipa et.al % 20% Maeda et.al % 15% Gopaul et.al % 24% Gao et.al % 27% Patty et.al % 28% Garcia-Aguilar % 37% Mellgren et.al % 47% Chakravarti % Sticca et.al % 10% Baron et.al % 21% Total % 28% Compare to Dutch Rectal Cancer Trial - <1% in stage 1 pts 20

21 Total mesorectal neglect Risk of lymph node metastases Increased by: Lower 1/3 of rectum Poor differentiation* Lymphovascular invasion* Sm level 3 T1 sub staging (Kudo et al. Endoscopy. 1993;25: ) T1 Sub-staging 21
22 Sm Level and LNM Sm1 = 0%, Sm2 = 10%, Sm3 = 25%» Kikuchi et al.dcr. 1995;38: Sm1 = 3%, Sm2 = 11%, Sm3 = 34% Odds ratio Sm3 vs. Sm1 = 5» Nascimbeni et al. 2002;45: Transanal Excision Bottom Line Think this out carefully! Discuss with patient ahead of time! Use very selectively! Treat as an excisional biopsy 22

23 TEM Advantages of TEM TransEndoscopic Microsurgery Improved visibility Larger lesions can be taken out intact (not piecemeal) Access to mid and upper rectal lesions Potential sampling of lymph nodes Very good for large villous tumours Good for select T1 cancers with low risk of lymph node metastases Possibility for mesorectal excision?? 23
 may be the most significant intervention in resectable rectal cancer 3.")
24 Radical excision 1. Rectal cancer surgery is technically driven 2. The surgical procedure (surgeon) may be the most significant intervention in resectable rectal cancer 3. The principles of rectal cancer surgery can be learned but. it requires practice / practise 24
25 Outcome by Specialization Rectal subset Specialist Non-specialist P-value Patients yr overall Survival Rectum 5 yr cancer specific survival Rectum 58.6% 47.0% % 60.6% McArdle & Hole. Br J Surg. 2004; 91: Outcomes by Training and Volume >21 resections <21 resections Local Recurrence Colorectal trained 10.4% 21.1% non-colorectal trained 27.8% 44.6% Disease-specific survival Colorectal Trained 67.3% 54.5% Non-colorectal trained 49.0% 39.2% Porter et.al. Ann Surg. 1998;227:

26 Know your surgeon! Total Mesorectal Excision the rectum and its mesentery are a single fascia-enveloped unit, anatomically separate from surrounding pelvic structures surgical violation of this anatomic package leads to a positive circumferential margin 26
27 Summary of the importance of Circumferential resection margin (CRM) A positive CRM is an independent predictor of local recurrence and survival (Quirke, Adam) Risk for positive CRM increases with more advanced T and N stage (Nategaal/ Quirke) Risk for positive CRM increases with violation of the mesorectum (Quirke) Plane of Surgery Dictates local recurrence rates! 25 p = year local recurrence (%) 13 Quirke mesorectal 7 intramesorectal muscularis propria 27
28 Can Adjuvant Radiation Compensate for Surgical Technique? NO!! Radiation can decrease local recurrence by 50% from base line levels Pahlman Thus surgical technique is the most important variable!! Mesorectal Excision Total mesorectal excision refers to removal of the rectum and mesorectum down to the pelvic floor and the levator hiatus appropriate for tumors of the mid and lower rectum Tumour specific mesorectal excision refers to the removal of the rectum and mesorectum for a distance of 5 cm below the tumour (no coning) ( leave lower rectum with its mesorectum) appropriate for tumors of the upper rectum (> 10 cm) 28

29 myoma Surgical Technique 29


30 Tumour specific mesorectal excision Tumour at 11 cm female deep cul de sac 30

31 How low can we go? Coloanal stapled To the level of the levators Coloanal hand sewn Just above the dentate Intersphincteric To the level of the dentate removing a portion of the internal sphincter For an extended low resection below the mesorectum, a 1 cm margin is optimal, may accept less < 1 cm if post neoadjuvant Abdominoperineal resection and TME Indications for APR Invasion of the levator ani or sphincter complex Inability to obtain proper distal margin without resecting the sphincter Preoperative incontinence Technical morbid obesity Issues with APR Tumours located at the level of the levator hiatus Significantly more positive CRMs Significantly more perforations 31


32 Alberta Rectal Cancer Initiative (ARCI) Location and surgeon experience 32
 What needs to be done? Increase the number of high volume surgeons and provide them with the tools to do quality work.")
33 Rectal Cancer and Surgeon Volume Surgery is performed at 22 hospitals across Alberta 8 hospitals perform a mean of 3 cases per year Surgeon Volume top quintile = High volume (HV) Surgeons 9 surgeries/year (range 9-31 cases/yr) What needs to be done? Increase the number of high volume surgeons and provide them with the tools to do quality work. HV surgeons: completed 68% of rectal cancer surgeries in Alberta in 2011, up from 32% in 1997; we need to do better! Why? higher rates of grade 3 TME specimens lower rates of CRM positivity higher sphincter preservation rates lower 5-year local recurrence higher 5-year disease-specific survival 33
 May be at the local")

34 How? Education (AHS PRIHS Grant) Surgeons want to do the right thing Rectal Cancer School: Proper operative (TME) techniques Appropriate staging and interpretation of MRI Use of Multidisciplinary Tumour Boards Appropriate use of neo adjuvant therapy Centralization of rectal cancer surgery to high-volume surgeons (location, location, location ) May be at the local level Central referral of difficult cases Need for a Clinical Pathway Radiologists Goal Dedicated high resolution imaging (MRI) for all patients undergoing curative surgery for rectal cancer in a timely manner using a synoptic report MRI performed according to the Mercury protocol for T2 and T3 tumours Correlation of test results and management plan Ensure access within accepted timelines 34
 and offered Neoadjuvant therapy when appropriate Care plan based on preoperative staging Current guidelines in Alberta include neoadjuvant long course")

35 Need for a Clinical Pathway Medical and Radiation oncologists Neoadjuvant therapy Goal - All patients with locally advanced operable rectal cancer have the opportunity to be discussed at a multidisciplinary conference (MDC) and offered Neoadjuvant therapy when appropriate Care plan based on preoperative staging Current guidelines in Alberta include neoadjuvant long course chemoradiation or short course radiation Only 50% of Alberta patients with stage II and 66% of stage III rectal cancer received neoadjuvant therapy (2011) Pathologists Continuous Quality Improvement Goal Complete TME evaluation of every rectal cancer specimen based on Quirke methodology 22% of cases were not graded for TME CRM positivity reported 78% of the time Lymph node harvest mean 17 nodes Lymph node status not reported in 4% 35

36 Proposed Rectal Cancer Pathway (Stage II/III) Diagnosis Treatment Preoperative Staging Dedicated High- Resolution Rectal MRI (performed according to mercury protocol) Transrectal Ultrasound Decision to Treat Neoadjuvant Radiation +/- Chemotherapy For the following: T3, T4 Node positive Sphincter preservation TME TME as part of a low anterior or abdominoperineal resection Tumour specific mesorectal excision with a margin of at least 5 cms Adjuvant Chemotherapy All patients should receive a referral to an oncologist to determine adjuvant therapy Majority should receive adjuvant therapy Follow up Care by FP, Oncol,,Sur g Strong recommendation based on moderate quality evidence Strong recommendation based on high quality evidence Strong recommendation based on high quality evidence Strong recommendation based on high quality evidence Evidence: Practice Parameters for the Management of Rectal Cancer (Revised) Diseases of the Colon & Rectum Volume 56:5 (2013) Proposed Rectal Cancer Measures (Stage II/III) Diagnosis Treatment Preoperative Staging Decision to Treat Neoadjuvant Radiation +/- Chemotherapy TME Adjuvant Chemotherapy Follow up Care by Primary Physician Process Measures: Percentage of preoperative MRIs performed to accurately stage MRIs are appropriately performed according to mercury protocol Turnaround times for pre-operative workup Time to diagnosis from completion of staging; staging to neoadjuvant Outcome Measures: Patient Satisfaction Process Measures: Number of referrals / appropriate patients receiving neoadjuvant radiation Number of appropriate patients receiving short course; long course Time to consult; time to treatment; between neoadjuvant therapy and surgery Number of patients with dose reduction OR delays during treatment Outcome Measures: Patient Satisfaction Process Measures: Complete TME (negative margins, lymph nodes) Outcome Measures: Length of Stay Complication Rates (e.g. bowel obstruction, wound healing, anastomic leak) Patient Satisfaction Process Measures: Number of referrals / appropriate patients receiving adjuvant chemotherapy Time to consult; between surgery and adjuvant chemotherapy Type of therapy used Number of patients with dose reduction OR delays during treatment Outcome Measures: Patient Satisfaction Outcome Measures: Recurrence Rates (local and distant) 3 Yr Incidence in relapse Quality of Life (e.g. bladder, bowel incontinence, sexual dysfunction Survival Rates Post treatment hospital utilization rates 36
 What can we expect?")

37 Pathway is based on accepted standards of care Diseases of the Colon & Rectum Volume 56:5 (2013) What can we expect? Better more efficient care Major impact on immediate and long-term patient outcomes Impact on survival rates Decreased local recurrence rates Potential reduction in repeat surgeries 37
38 How will we accomplish this? Design and implement a knowledge translation strategy to promote uptake of a rectal cancer clinical pathway that can be tailored to each local practice environment Evidence-based strategies for improving rectal cancer outcomes: Physician education initiatives Outcomes reporting Centralized Care Project Overview Evidence-based strategies for improving rectal cancer outcomes Educational initiatives: Timeline Physician Education Days Outcomes reporting: Alberta Synoptic Reports Outcomes Reports Outcomes Reports Baseline Data Evaluation Increased case volumes: Strategies to increase volumes Implementation Strategies to tailor interventions to each local practice environment Surgical Facility Resource Assessment Strategies to address local implementation barriers 38
 Cross sectional imaging (Location) Concentration of surgical care (Location) Extension of transanal methods Integration of multidisciplinary care Standardized Care Pathways Appropriate use")
39 Overall Goal Optimal safe effective patient centered care for every rectal cancer patient in Alberta Summary Rectal cancer surgery has undergone a technical evolution Anatomic basis for resection (Location) Cross sectional imaging (Location) Concentration of surgical care (Location) Extension of transanal methods Integration of multidisciplinary care Standardized Care Pathways Appropriate use of neoadjuvant therapy Future Chemoradiation, transanal excision of residual tumour followed by observation 39

40 Acknowledgements Data Dr. Kevin Klingbeil Dr. Anthony MacLean Dr. Indraneel Datta Dr. John Heine Dr. Mantaj Brar Yvonne Iris Project Leadership Team Todd McMullen* Don Buie* Neil Hagen* Anthony MacLean* Haili Wang* Angela Estey Barb Sonneberg Adam Elwi Melissa Shea-Budgell Questions 40
11/09/2014. Update Management of Rectal Cancer. Outline. I have no disclosures
 Update Management of Rectal Cancer June 7, 2014 W. Donald Buie MD,MSc, FRCSC Associate Professor of Surgery University of Calgary I have no disclosures Outline Pre-operative staging Who needs neoadjuvant
Update Management of Rectal Cancer June 7, 2014 W. Donald Buie MD,MSc, FRCSC Associate Professor of Surgery University of Calgary I have no disclosures Outline Pre-operative staging Who needs neoadjuvant
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference
 Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Rectal Cancer: Classic Hits
 Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
Rectal Cancer Update 2008 The Last 5 cm. Consensus Building
 Rectal Cancer Update 2008 The Last 5 cm Consensus Building Case Distal Rectal Cancer 65 male physician Rectal mass: 5cm from anal verge, 1cm above sphincter? Imaging choice: CT vs MR vs ERUS? Adjuvant
Rectal Cancer Update 2008 The Last 5 cm Consensus Building Case Distal Rectal Cancer 65 male physician Rectal mass: 5cm from anal verge, 1cm above sphincter? Imaging choice: CT vs MR vs ERUS? Adjuvant
Rectal Cancer. Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco
 Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
COLON AND RECTAL CANCER
 COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
COLON AND RECTAL CANCER
 No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
Preoperative adjuvant radiotherapy
 Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh
 Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Carcinoma del retto: Highlights
 Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
L impatto dell imaging sulla definizione della strategia terapeutica
 GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
Local Excision of Rectal Cancer Techniques and Outcomes
 Local Excision of Rectal Cancer Techniques and Outcomes Manoj J. Raval, MD, MSc, FRCSC Clinical Assistant Professor, UBC Rectal Cancer Update 2008 October 25, 2008 Overview Techniques & Description Patient
Local Excision of Rectal Cancer Techniques and Outcomes Manoj J. Raval, MD, MSc, FRCSC Clinical Assistant Professor, UBC Rectal Cancer Update 2008 October 25, 2008 Overview Techniques & Description Patient
A Review of Rectal Cancer. Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center
 A Review of Rectal Cancer Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center No disclosures Disclosures About me.. Grew up in Southern Illinois
A Review of Rectal Cancer Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center No disclosures Disclosures About me.. Grew up in Southern Illinois
RECTAL CARCINOMA: A DISTANCE APPROACH. Stephanie Nougaret
 RECTAL CARCINOMA: A DISTANCE APPROACH Stephanie Nougaret stephanienougaret@free.fr Despite the major improvements that have been made due to total mesorectal excision (TME) management of rectal cancer
RECTAL CARCINOMA: A DISTANCE APPROACH Stephanie Nougaret stephanienougaret@free.fr Despite the major improvements that have been made due to total mesorectal excision (TME) management of rectal cancer
Role of MRI for Staging Rectal Cancer
 Role of MRI for Staging Rectal Cancer High-resolution MRI has supplanted endoscopic ultrasound for staging rectal cancer. High-resolution MR images closely match histology and can show details such as
Role of MRI for Staging Rectal Cancer High-resolution MRI has supplanted endoscopic ultrasound for staging rectal cancer. High-resolution MR images closely match histology and can show details such as
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015
: Imaging Guidelines September 2015") Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
State-of-the-art of surgery for resectable primary tumors
 Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Staging of rectal cancer on MRI: What the surgeons want to know.
 Staging of rectal cancer on MRI: What the surgeons want to know. Poster No.: C-1108 Congress: ECR 2014 Type: Educational Exhibit Authors: G. Ayub, R. Chittal, A. Lowe, A. S. Punekar ; Leeds/, 1 2 1 2 2
Staging of rectal cancer on MRI: What the surgeons want to know. Poster No.: C-1108 Congress: ECR 2014 Type: Educational Exhibit Authors: G. Ayub, R. Chittal, A. Lowe, A. S. Punekar ; Leeds/, 1 2 1 2 2
Laparoscopic Resection Of Colon & Rectal Cancers. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
COLORECTAL CANCER STAGING in 2010
 COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
UCL. Rectum Adenocarcinoma. Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans
 Rectum Adenocarcinoma Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans Fifth Belgian Surgical Week May 6th, 2004, Oostende SOR rectum adenocarcinoma Indication of radiotherapy
Rectum Adenocarcinoma Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans Fifth Belgian Surgical Week May 6th, 2004, Oostende SOR rectum adenocarcinoma Indication of radiotherapy
Large polyps: EMR, ESD, TEM and segmental resection. Terry Phang 2017 SON fall update
 Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
Handling & Grossing of Colo-rectal Specimens for Tumours. for Medical Officers in Pathology
 Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Radiotherapy for rectal cancer. Karin Haustermans Department of Radiation Oncology
 Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES. Devon Paula Richardson
 NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES by Devon Paula Richardson Submitted in partial fulfilment of the requirements for the degree of Master
NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES by Devon Paula Richardson Submitted in partial fulfilment of the requirements for the degree of Master
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Rectal Cancer. Rectal Cancer: The CCF perspective 16/11/2017. Meagan Costedio, MD, FACS, FASCRS. 38,220 new cases estimated in
 Rectal Cancer: The CCF perspective Meagan Costedio, MD, FACS, FASCRS Medical Director Colorectal Surgery University Hospitals Ahuja Medical Center Associate Professor - Division of Colorectal Surgery Rectal
Rectal Cancer: The CCF perspective Meagan Costedio, MD, FACS, FASCRS Medical Director Colorectal Surgery University Hospitals Ahuja Medical Center Associate Professor - Division of Colorectal Surgery Rectal
Rectal Cancer : Curative treatment without surgery
 Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
Operative Technique: Karen Horvath, MD, FACS. SCOAP Retreat June 17, 2011
 Operative Technique: Total Mesorectal Excision Karen Horvath, MD, FACS University it of Washington, Seattle SCOAP Retreat June 17, 2011 No Disclosures Purpose What is Total Mesorectal Excision (TME)? How
Operative Technique: Total Mesorectal Excision Karen Horvath, MD, FACS University it of Washington, Seattle SCOAP Retreat June 17, 2011 No Disclosures Purpose What is Total Mesorectal Excision (TME)? How
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
PROCARE FINAL FEEDBACK
 1 PROCARE FINAL FEEDBACK General report 2006-2014 Version 2.1 08/12/2015 PROCARE indicators 2006-2014... 3 Demographic Data... 3 Diagnosis and staging... 4 Time to first treatment... 6 Neoadjuvant treatment...
1 PROCARE FINAL FEEDBACK General report 2006-2014 Version 2.1 08/12/2015 PROCARE indicators 2006-2014... 3 Demographic Data... 3 Diagnosis and staging... 4 Time to first treatment... 6 Neoadjuvant treatment...
CRC Surgery Educational Slide Deck. Dr. Andy Smith Sunnybrook Surgical Oncology Research Group Department of Surgery University of Toronto
 CRC Surgery Educational Slide Deck Dr. Andy Smith Sunnybrook Surgical Oncology Research Group Department of Surgery University of Toronto Staging Our group has made a major contribution re N-issues We
CRC Surgery Educational Slide Deck Dr. Andy Smith Sunnybrook Surgical Oncology Research Group Department of Surgery University of Toronto Staging Our group has made a major contribution re N-issues We
Pathohistological Assessment of the Circular Margin of Resection During Total Mesorectal Excision, Conducted on The Malignant Formations of the Rectum
 International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment
International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/887/22038 holds various files of this Leiden University dissertation. Author: Swellengrebel, H.A.M. Title: Challenges in the multimodality treatment of rectal
Cover Page The handle http://hdl.handle.net/887/22038 holds various files of this Leiden University dissertation. Author: Swellengrebel, H.A.M. Title: Challenges in the multimodality treatment of rectal
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Short course radiation therapy for rectal cancer in the elderly: can radical surgery be avoided?
 Short communication Short course radiation therapy for rectal cancer in the elderly: can radical surgery be avoided? Michael A. Cummings 1, Kenneth Y. Usuki 1, Fergal J. Fleming 2, Mohamedtaki A. Tejani
Short communication Short course radiation therapy for rectal cancer in the elderly: can radical surgery be avoided? Michael A. Cummings 1, Kenneth Y. Usuki 1, Fergal J. Fleming 2, Mohamedtaki A. Tejani
CHAPTER 7 Concluding remarks and implications for further research
 CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
Innovations in Rectal Cancer Surgery
 Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
Rectal Cancer. GI Practice Guideline
 Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
Local Excision for early rectal cancer
 Local Excision for early rectal cancer M. Trompetto, E. Ganio, G. Clerico, A. Realis Luc, RJ Nicholls Colorectal Eporediensis Centre Clinica S. Rita Vercelli Gruppo Policlinico di Monza Mortality Morbidity
Local Excision for early rectal cancer M. Trompetto, E. Ganio, G. Clerico, A. Realis Luc, RJ Nicholls Colorectal Eporediensis Centre Clinica S. Rita Vercelli Gruppo Policlinico di Monza Mortality Morbidity
PROCARE FINAL FEEDBACK Definitions
 1 PROCARE FINAL FEEDBACK 2006-2014 Definitions Version 0.2 29/10/2015 2 Table of Contents Introduction... 3 Part 1: PROCARE indicators 2006-2014... 4 1.1. Methods... 4 1.1.1. Descriptive numbers... 4 1.1.2.
1 PROCARE FINAL FEEDBACK 2006-2014 Definitions Version 0.2 29/10/2015 2 Table of Contents Introduction... 3 Part 1: PROCARE indicators 2006-2014... 4 1.1. Methods... 4 1.1.1. Descriptive numbers... 4 1.1.2.
Index. Surg Oncol Clin N Am 14 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Opportunity for palliative care Research
 Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Dr. Anat Ravid Surgical Oncology Lead Erie St. Clair Regional Cancer Program May 1, 2014
 Preoperative Staging MRI in Rectal Cancer: Where Are We Going in the Pelvis? Dr. Anat Ravid Surgical Oncology Lead Erie St. Clair Regional Cancer Program May 1, 2014 Objectives: How are we looking? Who
Preoperative Staging MRI in Rectal Cancer: Where Are We Going in the Pelvis? Dr. Anat Ravid Surgical Oncology Lead Erie St. Clair Regional Cancer Program May 1, 2014 Objectives: How are we looking? Who
Current Issues and Controversies in the Management of Rectal Cancer
 Current Issues and Controversies in the Management of Rectal Cancer Ghazi M. Nsouli MD 11 th Annual Congress of the Lebanese Society of Gastroenterology November 16, 2012 GMN 20121116 1 Staging of rectal
Current Issues and Controversies in the Management of Rectal Cancer Ghazi M. Nsouli MD 11 th Annual Congress of the Lebanese Society of Gastroenterology November 16, 2012 GMN 20121116 1 Staging of rectal
RECTAL CANCER CLINICAL CASE PRESENTATION
 RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
Innovations in rectal cancer surgery TAMIS and transanal TME
 Innovations in rectal cancer surgery TAMIS and transanal TME A.D Hoore MD PhD, EBSQ CR Chair Departement of Abdominal Surgery University Hospitals Leuven, Belgium Actual treatment in rectal Early rectal
Innovations in rectal cancer surgery TAMIS and transanal TME A.D Hoore MD PhD, EBSQ CR Chair Departement of Abdominal Surgery University Hospitals Leuven, Belgium Actual treatment in rectal Early rectal
RECTAL CANCER: Adjuvant Therapy. Maury Rosenstein, MD Montefiore Medical Center December 2012
 RECTAL CANCER: Adjuvant Therapy Maury Rosenstein, MD Montefiore Medical Center December 2012 Overview Indications for adjuvant therapy Preoperative Postoperative New Advances Epidemiology Approximately
RECTAL CANCER: Adjuvant Therapy Maury Rosenstein, MD Montefiore Medical Center December 2012 Overview Indications for adjuvant therapy Preoperative Postoperative New Advances Epidemiology Approximately
The accuracy of the diagnostic pathway for staging of low-mid rectal tumours with endoscopic, MRI and Endorectal Ultrasound assessment.
 Carl Bradbury CoRIPS Research Award 130-9,963.00 The accuracy of the diagnostic pathway for staging of low-mid rectal tumours with endoscopic, MRI and Endorectal Ultrasound assessment. Lay Summary of Project
Carl Bradbury CoRIPS Research Award 130-9,963.00 The accuracy of the diagnostic pathway for staging of low-mid rectal tumours with endoscopic, MRI and Endorectal Ultrasound assessment. Lay Summary of Project
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS
 PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
Neoadjuvant Therapy for Rectal Cancer is Overrated. Joon H. Lee, Research Resident University of Colorado 8/31/2009
 Neoadjuvant Therapy for Rectal Cancer is Overrated Joon H. Lee, Research Resident University of Colorado 8/31/2009 Objectives Brief overview of staging rectal cancer Current guidelines for evaluation and
Neoadjuvant Therapy for Rectal Cancer is Overrated Joon H. Lee, Research Resident University of Colorado 8/31/2009 Objectives Brief overview of staging rectal cancer Current guidelines for evaluation and
Treatment of Locally Advanced Rectal Cancer: Current Concepts
 Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer
 SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Transanal Endoscopic Microsurgery
 Transanal Endoscopic Microsurgery Dana R. Sands, MD, FACS, FASCRS Director, Colorectal Physiology Center Staff Surgeon Department of Colorectal Surgery Cleveland Clinic Florida What is TEM? Minimally invasive
Transanal Endoscopic Microsurgery Dana R. Sands, MD, FACS, FASCRS Director, Colorectal Physiology Center Staff Surgeon Department of Colorectal Surgery Cleveland Clinic Florida What is TEM? Minimally invasive
Meta analysis in Rectal Cancer
 Meta analysis in Rectal Cancer Dr. Monica Irukulla Professor and Head Department of Radiation Oncology Nizam s Institute of Medical Sciences hyderabad Areas of meta analysis in rectal cancers Epidemiology
Meta analysis in Rectal Cancer Dr. Monica Irukulla Professor and Head Department of Radiation Oncology Nizam s Institute of Medical Sciences hyderabad Areas of meta analysis in rectal cancers Epidemiology
Patterns of local recurrence in rectal cancer; a study of the Dutch TME trial
 Chapter 3 3 Patterns of local recurrence in rectal cancer; a study of the Dutch TME trial 39 M. Kusters, C.A.M. Marijnen, C.J.H. van de Velde, H.J.T. Rutten, M.J. Lahaye, J.H. Kim, R.G.H. Beets-Tan, G.L.
Chapter 3 3 Patterns of local recurrence in rectal cancer; a study of the Dutch TME trial 39 M. Kusters, C.A.M. Marijnen, C.J.H. van de Velde, H.J.T. Rutten, M.J. Lahaye, J.H. Kim, R.G.H. Beets-Tan, G.L.
Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer
 Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer") Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer Emily Chan, Qian Shi, Julio Garcia-Aguilar, Peter Cataldo, Jorge
Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer Emily Chan, Qian Shi, Julio Garcia-Aguilar, Peter Cataldo, Jorge
Pelvic Organ Functions: Urinary, Sexual and Bowel Dysfunction after Rectal Surgery
 Pelvic Organ Functions: Urinary, Sexual and Bowel Dysfunction after Rectal Surgery Disclosure M ADHULIKA G. V ARMA M D PROFESSOR AND CHIEF S E CTION O F COLORECTAL S U R G ERY U N I V ERS ITY O F CALIFORNIA,
Pelvic Organ Functions: Urinary, Sexual and Bowel Dysfunction after Rectal Surgery Disclosure M ADHULIKA G. V ARMA M D PROFESSOR AND CHIEF S E CTION O F COLORECTAL S U R G ERY U N I V ERS ITY O F CALIFORNIA,
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
Differential lymph node retrieval in rectal cancer: associated factors and effect on survival
 Original Article Differential lymph node retrieval in rectal cancer: associated factors and effect on survival Cedrek McFadden 1, Brian McKinley 1, Brian Greenwell 2, Kaylee Knuckolls 1, Patrick Culumovic
Original Article Differential lymph node retrieval in rectal cancer: associated factors and effect on survival Cedrek McFadden 1, Brian McKinley 1, Brian Greenwell 2, Kaylee Knuckolls 1, Patrick Culumovic
Review Article Intersphincteric Resection for Low Rectal Cancer: An Overview
 International Surgical Oncology Volume 2012, Article ID 241512, 4 pages doi:10.1155/2012/241512 Review Article Intersphincteric Resection for Low Rectal Cancer: An Overview Constantine P. Spanos 1st Department
International Surgical Oncology Volume 2012, Article ID 241512, 4 pages doi:10.1155/2012/241512 Review Article Intersphincteric Resection for Low Rectal Cancer: An Overview Constantine P. Spanos 1st Department
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Rectal Cancer Cookbook Update. A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux
 Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
Innovative Surgical Management in the Treatment of Rectal Cancer: MIS, Robotic, and Beyond
 Innovative Surgical Management in the Treatment of Rectal Cancer: MIS, Robotic, and Beyond Jonathan E. Efron, MD, FACS, FASCRS The Mark M Ravitch, MD Endowed Professorship in Surgery Chief of the Ravitch
Innovative Surgical Management in the Treatment of Rectal Cancer: MIS, Robotic, and Beyond Jonathan E. Efron, MD, FACS, FASCRS The Mark M Ravitch, MD Endowed Professorship in Surgery Chief of the Ravitch
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
Sphincter Sparing Procedures: Is it a standard for Management of Low Rectal Cancer
 Journal of the Egyptian Nat. Cancer Inst., Vol. 16, No. 4, December: 210-215, 2004 Sphincter Sparing Procedures: Is it a standard for Management of Low Rectal Cancer EL-SAYED ASHRAF KHALIL, M.D.FRCS; MOHAMAD
Journal of the Egyptian Nat. Cancer Inst., Vol. 16, No. 4, December: 210-215, 2004 Sphincter Sparing Procedures: Is it a standard for Management of Low Rectal Cancer EL-SAYED ASHRAF KHALIL, M.D.FRCS; MOHAMAD
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
PREOPERATIVE STAGING AND RADIOTHERAPY IN RECTAL CANCER SURGERY
 From THE DEPARTMENTS OF CLINICAL SCIENCES, DANDERYD HOSPITAL and MOLECULAR MEDICINE AND SURGERY, KAROLINSKA UNIVERSITY HOSPITAL PREOPERATIVE STAGING AND RADIOTHERAPY IN RECTAL CANCER SURGERY Johan Pollack
From THE DEPARTMENTS OF CLINICAL SCIENCES, DANDERYD HOSPITAL and MOLECULAR MEDICINE AND SURGERY, KAROLINSKA UNIVERSITY HOSPITAL PREOPERATIVE STAGING AND RADIOTHERAPY IN RECTAL CANCER SURGERY Johan Pollack
MRI of Rectal Cancer
 MRI of Rectal Cancer Arnd-Oliver Schäfer Mathias Langer MRI of Rectal Cancer Clinical Atlas Prof. Dr. Arnd-Oliver Schäfer Department of Diagnostic Radiology Freiburg University Hospital Hugstetter Straße
MRI of Rectal Cancer Arnd-Oliver Schäfer Mathias Langer MRI of Rectal Cancer Clinical Atlas Prof. Dr. Arnd-Oliver Schäfer Department of Diagnostic Radiology Freiburg University Hospital Hugstetter Straße
Treatment strategy of metastatic rectal cancer
 35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
WHAT IS LARS? LOW ANTERIOR RESECTIONSYNDROME. Sophie Pilkington. Colorectal Surgeon University Hospital Southampton
 WHAT IS LARS? LOW ANTERIOR RESECTIONSYNDROME Sophie Pilkington Colorectal Surgeon University Hospital Southampton INTRODUCTION UK Bowel cancer 2013 41,100 new cases INTRODUCTION UK Bowel cancer 2013 41,100
WHAT IS LARS? LOW ANTERIOR RESECTIONSYNDROME Sophie Pilkington Colorectal Surgeon University Hospital Southampton INTRODUCTION UK Bowel cancer 2013 41,100 new cases INTRODUCTION UK Bowel cancer 2013 41,100
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
Advances in Imaging Technology In The Management of Colorectal Cancer
 Advances in Imaging Technology In The Management of Colorectal Cancer Dushyant Sahani, M.D Director of CT Associate Professor Department of Radiology Massachusetts General Hospital Harvard Medical School
Advances in Imaging Technology In The Management of Colorectal Cancer Dushyant Sahani, M.D Director of CT Associate Professor Department of Radiology Massachusetts General Hospital Harvard Medical School
Neoadjuvant treatment Evolution and Current Status
 Neoadjuvant treatment Evolution and Current Status Dr Andrew See Radiation Oncologist 2017 Rectal Cancer Symposium Friday 10 th November 2017 2 1 Major Randomised Trials Supporting Neoadjuvant CRT Trial
Neoadjuvant treatment Evolution and Current Status Dr Andrew See Radiation Oncologist 2017 Rectal Cancer Symposium Friday 10 th November 2017 2 1 Major Randomised Trials Supporting Neoadjuvant CRT Trial
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Postoperative morbidity and recurrence after local excision of rectal adenomas and rectal cancer by transanal endoscopic microsurgery
 Original article Postoperative morbidity and recurrence after local excision of rectal adenomas and rectal cancer by transanal endoscopic microsurgery B. H. Endreseth*, A. Wibe*, M. Svinsås*, R. Mårvik*
Original article Postoperative morbidity and recurrence after local excision of rectal adenomas and rectal cancer by transanal endoscopic microsurgery B. H. Endreseth*, A. Wibe*, M. Svinsås*, R. Mårvik*
Outcome of rectal cancer after radiotherapy with a long or short waiting period before surgery, a descriptive clinical study
 Original Article Outcome of rectal cancer after radiotherapy with a long or short waiting period before surgery, a descriptive clinical study Elmer E. van Eeghen 1, Frank den Boer 2, Sandra D. Bakker 1,
Original Article Outcome of rectal cancer after radiotherapy with a long or short waiting period before surgery, a descriptive clinical study Elmer E. van Eeghen 1, Frank den Boer 2, Sandra D. Bakker 1,
TME and autonomic nerve preservation techniques: based on Video and Cadaveric anatomy
 TME and autonomic nerve preservation techniques: based on Video and Cadaveric anatomy Nam Kyu Kim M.D., Ph.D., FACS, FRCS, FASCRS Professor Department of Surgery Yonsei University College of Medicine Seoul,
TME and autonomic nerve preservation techniques: based on Video and Cadaveric anatomy Nam Kyu Kim M.D., Ph.D., FACS, FRCS, FASCRS Professor Department of Surgery Yonsei University College of Medicine Seoul,
Original Policy Date
 MP 7.01.92 Transanal Endoscopic Microsurgery Medical Policy Section Surgery Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return to Medical
MP 7.01.92 Transanal Endoscopic Microsurgery Medical Policy Section Surgery Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return to Medical
Is adjuvant radiotherapy warranted in resected pt1-2 node-positive rectal cancer?
 Peng et al. Radiation Oncology 2013, 8:290 RESEARCH Open Access Is adjuvant radiotherapy warranted in resected pt1-2 node-positive rectal cancer? Junjie Peng 1,2, Xinxiang Li 1,2, Ying Ding 3, Debing Shi
Peng et al. Radiation Oncology 2013, 8:290 RESEARCH Open Access Is adjuvant radiotherapy warranted in resected pt1-2 node-positive rectal cancer? Junjie Peng 1,2, Xinxiang Li 1,2, Ying Ding 3, Debing Shi
Ein Leben nach tiefer Rektumresektion: Was erwartet unsere Patienten im Langzeitverlauf?
 Ein Leben nach tiefer Rektumresektion: Was erwartet unsere Patienten im Langzeitverlauf? Dieter Hahnloser Klinik für Viszeral- und Transplantationschirurgie UniverstätsSpital Zürich Low Rectal Resection
Ein Leben nach tiefer Rektumresektion: Was erwartet unsere Patienten im Langzeitverlauf? Dieter Hahnloser Klinik für Viszeral- und Transplantationschirurgie UniverstätsSpital Zürich Low Rectal Resection
Staging Colorectal Cancer
 Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Colorectal Surgery. Patient Care. Goals and Objectives
 Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Case Report 17-Week Delay Surgery after Chemoradiation in Rectal Cancer with Complete Pathological Response
 Case Reports in Surgery Volume 2015, Article ID 816491, 5 pages http://dx.doi.org/10.1155/2015/816491 Case Report 17-Week Delay Surgery after Chemoradiation in Rectal Cancer with Complete Pathological
Case Reports in Surgery Volume 2015, Article ID 816491, 5 pages http://dx.doi.org/10.1155/2015/816491 Case Report 17-Week Delay Surgery after Chemoradiation in Rectal Cancer with Complete Pathological
BC CRC Update Unusual Colorectal Tumors
 BC CRC Update Unusual Colorectal Tumors Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary I
BC CRC Update Unusual Colorectal Tumors Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary I
Terminology: anal canal cancer. Terminology: Anal margin cancer. Treatment Epidermoid
 Terminology: anal canal cancer Epidermoid Below dentate line squamous CC At and above dentate line «basaloid», «cloacogenic», or «transi6onal» = non kera6nizing types of squamous cell carcinoma same =t
Terminology: anal canal cancer Epidermoid Below dentate line squamous CC At and above dentate line «basaloid», «cloacogenic», or «transi6onal» = non kera6nizing types of squamous cell carcinoma same =t
Audit Report. Colorectal Cancer Quality Performance Indicators. Patients diagnosed April 2016 March Published: March 2018
 Colorectal Cancer Managed Clinical Network Audit Report Colorectal Cancer Quality Performance Indicators Patients diagnosed April 2016 March 2017 Published: March 2018 Mr Michael Walker NOSCAN MCN Clinical
Colorectal Cancer Managed Clinical Network Audit Report Colorectal Cancer Quality Performance Indicators Patients diagnosed April 2016 March 2017 Published: March 2018 Mr Michael Walker NOSCAN MCN Clinical
The Role Of The Post-CRT MRI In Assessing Response
 Low Rectal Cancer: Is It Safe To Change The Plane Of Surgery? The Role Of The Post-CRT MRI In Assessing Response Nick Battersby, Mit Dattani, Nick West, Graham Branagan, Mark Gudgeon, Phil Quirke, Paris
Low Rectal Cancer: Is It Safe To Change The Plane Of Surgery? The Role Of The Post-CRT MRI In Assessing Response Nick Battersby, Mit Dattani, Nick West, Graham Branagan, Mark Gudgeon, Phil Quirke, Paris
editoriale Optimal lymph node dissection for T3-T4 lower rectal cancer, the so-called high risk group: the Japanese experience Introduction
 G Chir Vol. 30 - n. 10 - pp. 393-399 Ottobre 2009 editoriale Optimal lymph node dissection for T3-T4 lower rectal cancer, the so-called high risk group: the Japanese experience M. YASUNO Introduction The
G Chir Vol. 30 - n. 10 - pp. 393-399 Ottobre 2009 editoriale Optimal lymph node dissection for T3-T4 lower rectal cancer, the so-called high risk group: the Japanese experience M. YASUNO Introduction The