Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference
|
|
|
- Alexander Kristian Barnett
- 5 years ago
- Views:
Transcription
1 Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
2 Disclosures I have no disclosures
3 Outline Background Role of radiology in rectal cancer care MRI ERUS Multidisciplinary Conference

4 Coming together is a beginning Keeping together is progress Working together is success Henry Ford

5 Courtesy of Dr. Robert Madoff, U of Minnesota
6 Rectal Cancer Care Multidisciplinary Surgery Radiology Interdisciplinary Pathology Radiation Oncology Medical oncology Multidisciplinary conference

7 Rectal Cancer Care Problem: Variable practice Variable reporting Variable outcomes
8 Local regional staging Improve outcomes by standardizing practice and standardizing reporting MRI All rectal cancers should get an MRI All rectal MRIs should use a standardized report ERUS ERUS should be used for early lesions prior to local excision
9 MRI is essential for planning optimal treatment for rectal cancer Identification of CRM (negative, at risk, positive) Relationship of tumour to levators and sphincter complex Identification of locally confined tumour for primary surgery Identification of locally advanced requiring neoadjuvant therapy Extrarectal involvement T3, T4 Extramural vessel invasion (EMVI) Nodal disease Assessment of response to neoadjuvant therapy Planning low rectal cancer surgery (dissection planes, reconstruction)

 Risk for positive CRM increases with violation of the mesorectum")
10 Circumferential resection margin (CRM) Surgically created plane produced during the dissection of the mesorectum from the surrounding tissues Importance A positive CRM is an independent predictor of local recurrence and survival (Quirke, Adam) Risk for positive CRM increases with more advanced T and N stage (Nategaal/ Quirke) Risk for positive CRM increases with violation of the mesorectum (Quirke)
11 CRM+ is associated with increased local recurrence No neoadjuvant therapy Neoadjuvant therapy Quirke, Nagtegal, J Clin Oncol 2008;26:303-12
12 CRM+ is associated with poorer survival No neoadjuvant therapy Neoadjuvant therapy Quirke, Nagtegal, J Clin Oncol 2008;26:303-12


13 Prediction of involved CRM Beets-Tan 2004
14 MRI is most accurate for CRM
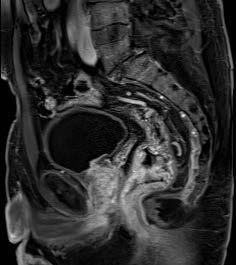
15 Case #1 Good risk tumour A 65 year old male presents with bright red rectal bleeding for 6 months. Comorbidities include hypertension. Colonoscopy demonstrates a large anterior polypoid tumour at 5 cm. CT scan does not demonstrate any metastases and MRI was ordered.
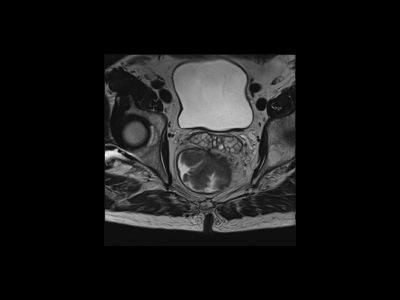


16
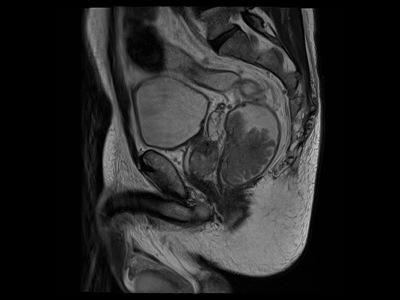
17 Case # 2 56 year old male 3-5 months history of altering bowel habits Circumferential rectal tumor 2-3 cm above the dentate; 6 cm from verge CT no mets, incidental finding of liver cirrhosis
18
19

20
21 Do all T3s need to be treated with neoadjuvant therapy? Can we save function without compromising cure?


22 T2 Low Rectal Tumor Preservation of the T2 hypointense outer muscularis propria wall layer = T2 disease

23 T2 or early T3?

24
25 pt3a (< 5mm invasion) tumours have a good 5 year survival T3a T3b Merkel et al IJCR Dis 2001;16: pt3a < 5 mm; pt3b > 5 mm
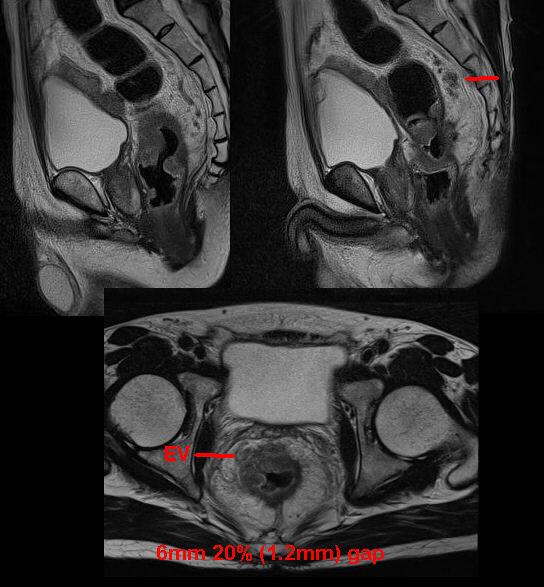
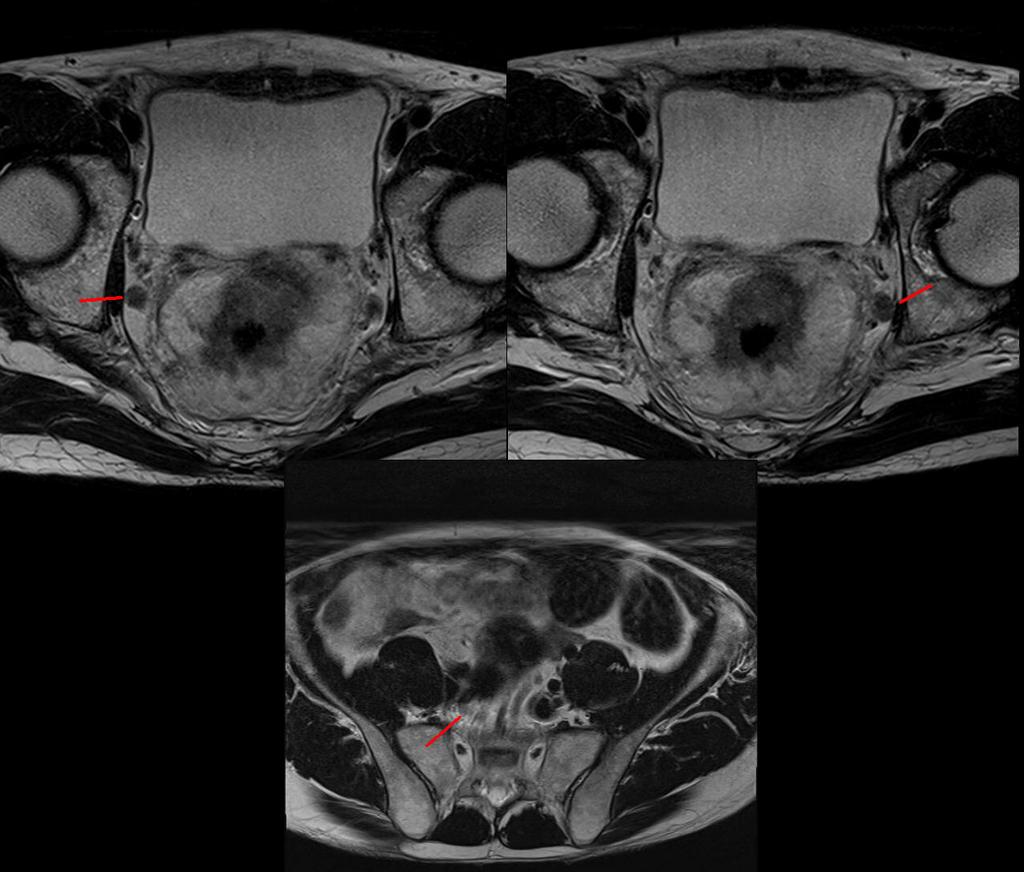
26 Minimally invasive T3 without extramural vascular invasion (EMVI) T2 and T3 tumour < 5 mm without EMVI have an 85-90% 5 yr cancer specific survival Mercury trial suggests that MRI can reliably identify EMVI preoperatively At the present time these patient should be discussed at Multidisciplinary Tumour Conference prior to a decision to omit neoadjuvant therapy

27 ct4 invading the levator ani and the sphincter
28 Does MRI usage affect the uptake of neoadjuvant therapy?
29 Use of Neoadjuvant chemoradiation/radiation in locally advanced rectal cancer Alberta (2015) 325 patients radical resection for rectal cancer; complete data in 321 MRI obtained in 246 (76.6%); 170 were classified as Stage II or III* 135 (79.4%) received ncrt (114) or nrt (21) 35 (20.6%) did not receive 19 (54%) patient factors, 3 (8.6%) system factors 13 (37%) unknown A large proportion of patients who did not receive ncrt/rt did so because of patient factors *20 (8%) were understaged
30 Use of Neoadjuvant chemoradiation in locally advanced rectal cancer Alberta (2015) No MRI in 75 (23.4%) patients; 15 (20%) tumours above peritoneal reflection 8 (13.3%) of the remaining 60 received neoadjuvant treatment 26 (43.3%) were stage II or III on final pathology; should have been offered/received ncrt/nrt A significant proportion of those that did not get properly staged missed out on neoadjuvant therapy
31 Measuring the response to neoadjuvant therapy Mercury study group, Patel Am J Roentgenol. 2012

32 Mass et al. Ann Surg Oncol (2015)22: A. Complete response B. Equivocal response C. Residual tumour D. Smooth scar E. Small ulcer F. Residual tumour
33 What are the limitations of MRI? Technique dependent planning; reader dependent Susceptible to motion artifact Nodal status based on size homogeneity, shape Micro-metastases may be missed T2 T3 interface sometimes difficult (experienced radiologist, good rapport) Contraindicated in patients with some cardiac pacemakers, orthopedic hardware
34 Synoptic reporting of MRI Improves completeness of reporting Ensures that all important information required for decisions is gathered Alberta Provincial plan for synoptic reporting for all rectal MRI Standardizing technique as much as possible Standardized outcome measures Provide feedback to radiologists based on pathologic evaluation
35 Synoptic report

36 Use of Staging MRI and Completeness of MRI reports Use of preoperative staging MRI has increased from 53% to 67% to 75% Tumour height Relationship to Anal sphincter Relationship to anterior Extramural vascular invasion Distance to mesorectal fascia % complete
37 MRI - Meticulous attention to technique (Mercury trial) MR definitive sequence high resolution small FOV 3 mm thick non fat suppressed T2 sections orthogonal to lumen and no gap. Failure to image perpendicular to lumen attributed to 11/22 overestimation errors on review of data. All 18 interpreting GI radiologists went to workshops on technique and reporting.

38 Same case slightly different angles There are no publications demonstrating superiority of Endorectal in staging
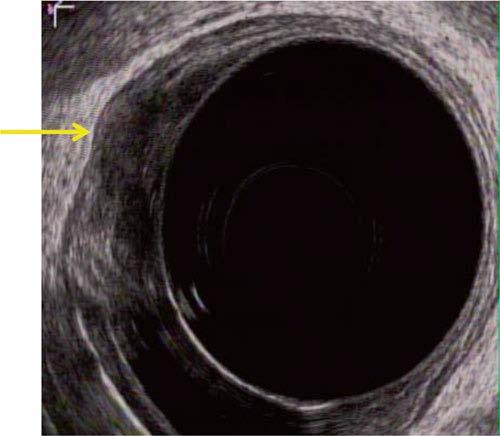
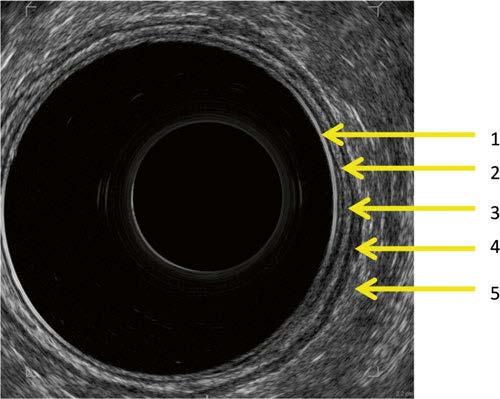
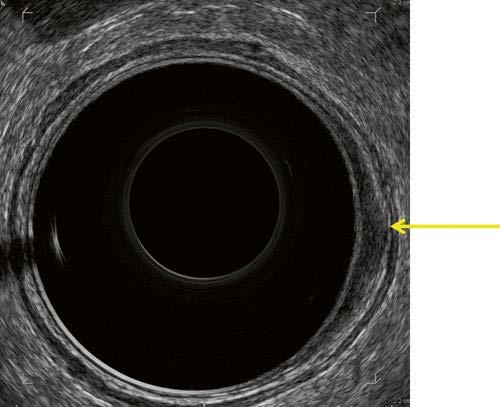
39 Endorectal Ultrasound
40 ERUS Useful for staging prior to local excision Advantages Simple to perform Inexpensive compared to MRI Accurate for T stage not for N stage Disadvantages Inaccurate with obstructing lesions Operator dependent Experience dependent Better with staging locally advanced lesions Prior to local excision I will obtain an MRI and an ERUS

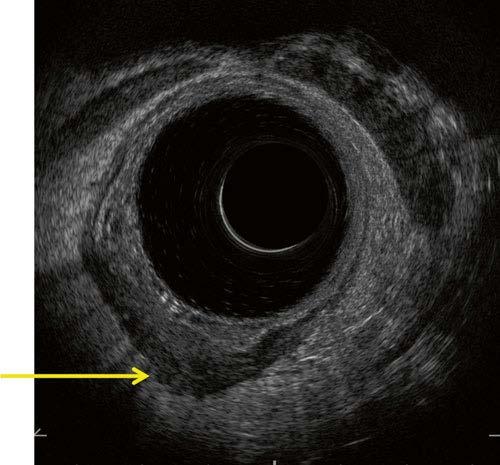
41 ut0 ut1 ut2 ut3
42 ERUS accuracy Higher sensitivity for locally advanced cancer 95% Lower accuracy for detecting T2 tumours compared to T1 T3 T4
43 ERUS N stage N-stage Accuracy ~ 75% (64-83%) Problem areas: Blood vessel vs. lymph node (use Doppler) Overstaging (5-22%) secondary to inflammation Understaging (2-25%) nodes too small or beyond the range of the probe 50-75% of + ve nodes are normal size (<5mm) 43
44 Overstaging and understaging UK study, multicenter 91 T1 cancers Understaged as T0 24% Correctly staged as T1-57% Overstaged as T2-16%, and as T3 in 2% Ashraf et.al. Colorectal Disease.2012;14:

45 Summary: Role of Radiology Treatment planning depends on accurate preoperative staging Accurate staging predicts surgical and pathologic findings MRI plays a central role in assessing response to neoadjuvant therapy Quality reporting is essential

46 Multidisciplinary Conference (MDC)


47 Rectal Cancer Care Multidisciplinary Surgery Radiology Pathology Interdisciplinary Radiation Oncology Medical oncology Multidisciplinary conference
48 Advantages of Multidisciplinary conference (MDC) Multidisciplinary team management is associated with improved clinical decision making Superior outcomes Better patient experience Improved communication More timely Consensus decisions Multiple viewpoints; ownership Education from other specialties (i.e.) MRI Surgical margins Tumour location Chemoradiation risk and benefit for the individual
49 Structure, Membership of MDC Structure Meeting time that everyone can attend Thursday at 4:30 pm TBCC/FMC Cases are identified in advance and sent out on a locked to the members Radiology and pathology are notified of the cases for review in advance The essential specialty must be represented for a case to be discussed ( i.e. if the question is primarily surgical then at least one surgeon must be present) Membership Surgeons (CR SO HPB), med oncologists, rad oncologists, radiologists, pathologists (case specific) Open to physicians and surgeons from Calgary, Lethbridge, Medicine Hat and Red Deer Attendance credit for MAINPORT
50 MDC Process Chair is at TBCC/FMC All other sites are linked by Telehealth Individuals can attend by phone Case presented by the primary physician/surgeon Films are reviewed by radiology Discussion regarding question at hand Consensus is reached Treatment plan set; consults are booked (surgery, chemo, rads) Report is generated immediately and distributed the next day to the physicians and surgeons involved with the case
51 Referral Anyone who participates in rectal cancer care can refer a patient to MDC for discussion Appropriate referrals: Re-reading MRI and other modalities Surgical management Organizing a second opinion (surgical or medical) Use of neoadjuvant therapy; SCRT vs LCCRT Use of adjuvant chemotherapy Recurrent disease treatment or palliation Assessment for enrollment in current trials Our goal is to have all rectal cancer cases discussed
52 The Value of Multidisciplinary Teams ( Mercury study) Rectal cancer MDT 2% ( 4/182) CRM positive rate in resected patients discussed at MDT 8% ( 16/194) CRM positive rate in all discussed patients including unresectable disease 28% ( 16/162) CRM positive rate in patients not discussed CRM positive rate in all cases discussed by MDT was significantly lower than in cases not discussed ( p< 0.001) Burton et al Br J Cancer 2006;94: Following this paper the Royal Marsden Hospital made MDT and MRI mandatory for all rectal cancers There was a reduction of the overall CRM+ to 3%!!

53 Team effort
54 Summary Cross sectional imaging is an essential component of comprehensive care of rectal cancer patients Accurate local regional staging guides treatment decision MRI should be performed for all rectal cancers ERUS prior to local excision MDC is essential to support multidisciplinary and interdisciplinary care It is the foundation for good decision making and excellent comphensive care
55
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015
: Imaging Guidelines September 2015") Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
RECTAL CARCINOMA: A DISTANCE APPROACH. Stephanie Nougaret
 RECTAL CARCINOMA: A DISTANCE APPROACH Stephanie Nougaret stephanienougaret@free.fr Despite the major improvements that have been made due to total mesorectal excision (TME) management of rectal cancer
RECTAL CARCINOMA: A DISTANCE APPROACH Stephanie Nougaret stephanienougaret@free.fr Despite the major improvements that have been made due to total mesorectal excision (TME) management of rectal cancer
Role of MRI for Staging Rectal Cancer
 Role of MRI for Staging Rectal Cancer High-resolution MRI has supplanted endoscopic ultrasound for staging rectal cancer. High-resolution MR images closely match histology and can show details such as
Role of MRI for Staging Rectal Cancer High-resolution MRI has supplanted endoscopic ultrasound for staging rectal cancer. High-resolution MR images closely match histology and can show details such as
11/09/2014. Update Management of Rectal Cancer. Outline. I have no disclosures
 Update Management of Rectal Cancer June 7, 2014 W. Donald Buie MD,MSc, FRCSC Associate Professor of Surgery University of Calgary I have no disclosures Outline Pre-operative staging Who needs neoadjuvant
Update Management of Rectal Cancer June 7, 2014 W. Donald Buie MD,MSc, FRCSC Associate Professor of Surgery University of Calgary I have no disclosures Outline Pre-operative staging Who needs neoadjuvant
Rectal Cancer Location: the Surgical Perspective
 Rectal Cancer Location: the Surgical Perspective September 5, 2014 W. Donald Buie MD,MSc, FRCSC Associate Professor of Surgery University of Calgary I have no disclosures 1 Outline Surgical Anatomy review
Rectal Cancer Location: the Surgical Perspective September 5, 2014 W. Donald Buie MD,MSc, FRCSC Associate Professor of Surgery University of Calgary I have no disclosures 1 Outline Surgical Anatomy review
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
L impatto dell imaging sulla definizione della strategia terapeutica
 GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
COLORECTAL CANCER STAGING in 2010
 COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
Rectal Cancer Update 2008 The Last 5 cm. Consensus Building
 Rectal Cancer Update 2008 The Last 5 cm Consensus Building Case Distal Rectal Cancer 65 male physician Rectal mass: 5cm from anal verge, 1cm above sphincter? Imaging choice: CT vs MR vs ERUS? Adjuvant
Rectal Cancer Update 2008 The Last 5 cm Consensus Building Case Distal Rectal Cancer 65 male physician Rectal mass: 5cm from anal verge, 1cm above sphincter? Imaging choice: CT vs MR vs ERUS? Adjuvant
Dr. Anat Ravid Surgical Oncology Lead Erie St. Clair Regional Cancer Program May 1, 2014
 Preoperative Staging MRI in Rectal Cancer: Where Are We Going in the Pelvis? Dr. Anat Ravid Surgical Oncology Lead Erie St. Clair Regional Cancer Program May 1, 2014 Objectives: How are we looking? Who
Preoperative Staging MRI in Rectal Cancer: Where Are We Going in the Pelvis? Dr. Anat Ravid Surgical Oncology Lead Erie St. Clair Regional Cancer Program May 1, 2014 Objectives: How are we looking? Who
Rectal Cancer. Rectal Cancer: The CCF perspective 16/11/2017. Meagan Costedio, MD, FACS, FASCRS. 38,220 new cases estimated in
 Rectal Cancer: The CCF perspective Meagan Costedio, MD, FACS, FASCRS Medical Director Colorectal Surgery University Hospitals Ahuja Medical Center Associate Professor - Division of Colorectal Surgery Rectal
Rectal Cancer: The CCF perspective Meagan Costedio, MD, FACS, FASCRS Medical Director Colorectal Surgery University Hospitals Ahuja Medical Center Associate Professor - Division of Colorectal Surgery Rectal
RECTAL CANCER CLINICAL CASE PRESENTATION
 RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
Rectal Cancer: Classic Hits
 Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
Carcinoma del retto: Highlights
 Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
Local Excision of Rectal Cancer Techniques and Outcomes
 Local Excision of Rectal Cancer Techniques and Outcomes Manoj J. Raval, MD, MSc, FRCSC Clinical Assistant Professor, UBC Rectal Cancer Update 2008 October 25, 2008 Overview Techniques & Description Patient
Local Excision of Rectal Cancer Techniques and Outcomes Manoj J. Raval, MD, MSc, FRCSC Clinical Assistant Professor, UBC Rectal Cancer Update 2008 October 25, 2008 Overview Techniques & Description Patient
MRI in staging of rectal carcinoma
 MRI in staging of rectal carcinoma Poster No.: C-0152 Congress: ECR 2015 Type: Scientific Exhibit Authors: J. R. Ramos Rodriguez, M. Atencia Ballesteros, M. D. M. Muñoz Ruiz, A. J. Márquez Moreno, M. D.
MRI in staging of rectal carcinoma Poster No.: C-0152 Congress: ECR 2015 Type: Scientific Exhibit Authors: J. R. Ramos Rodriguez, M. Atencia Ballesteros, M. D. M. Muñoz Ruiz, A. J. Márquez Moreno, M. D.
Staging Colorectal Cancer
 Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
COLON AND RECTAL CANCER
 COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh
 Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Current Issues and Controversies in the Management of Rectal Cancer
 Current Issues and Controversies in the Management of Rectal Cancer Ghazi M. Nsouli MD 11 th Annual Congress of the Lebanese Society of Gastroenterology November 16, 2012 GMN 20121116 1 Staging of rectal
Current Issues and Controversies in the Management of Rectal Cancer Ghazi M. Nsouli MD 11 th Annual Congress of the Lebanese Society of Gastroenterology November 16, 2012 GMN 20121116 1 Staging of rectal
Staging of rectal cancer on MRI: What the surgeons want to know.
 Staging of rectal cancer on MRI: What the surgeons want to know. Poster No.: C-1108 Congress: ECR 2014 Type: Educational Exhibit Authors: G. Ayub, R. Chittal, A. Lowe, A. S. Punekar ; Leeds/, 1 2 1 2 2
Staging of rectal cancer on MRI: What the surgeons want to know. Poster No.: C-1108 Congress: ECR 2014 Type: Educational Exhibit Authors: G. Ayub, R. Chittal, A. Lowe, A. S. Punekar ; Leeds/, 1 2 1 2 2
Oncology Review article High-Resolution MRI in Rectal Cancer
 Oncology Review article High-Resolution MRI in Rectal Cancer Adriana Dieguez Department Of Magnetic Resonance And Computed Tomography In Oncologic Diseases, Diagnóstico Médico Junín 1023, C1113AAE. Buenos
Oncology Review article High-Resolution MRI in Rectal Cancer Adriana Dieguez Department Of Magnetic Resonance And Computed Tomography In Oncologic Diseases, Diagnóstico Médico Junín 1023, C1113AAE. Buenos
Rectal cancer with synchroneous liver mets: A challenging clinical case
 ESMO Preceptorship Programme Rectal cancer Singapur November 2017 Rectal cancer with synchroneous liver mets: A challenging clinical case Andrés Cervantes Disclosures Consulting and advisory services,
ESMO Preceptorship Programme Rectal cancer Singapur November 2017 Rectal cancer with synchroneous liver mets: A challenging clinical case Andrés Cervantes Disclosures Consulting and advisory services,
COLON AND RECTAL CANCER
 No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
RECTAL CANCER APPARENT COMPLETE RESPONSE (acr) AFTER LONG COURSE CHEMORADIOTHERAPY
 AFTER LONG COURSE CHEMORADIOTHERAPY") COLORECTAL CLINICAL SUBGROUP RECTAL CANCER APPARENT COMPLETE RESPONSE (acr) AFTER LONG COURSE CHEMORADIOTHERAPY Finalised by: Dr Simon Gollins Mr Andrew Renehan Dr Mark Saunders Mr Nigel Scott Dr Shabbir
COLORECTAL CLINICAL SUBGROUP RECTAL CANCER APPARENT COMPLETE RESPONSE (acr) AFTER LONG COURSE CHEMORADIOTHERAPY Finalised by: Dr Simon Gollins Mr Andrew Renehan Dr Mark Saunders Mr Nigel Scott Dr Shabbir
CRC Surgery Educational Slide Deck. Dr. Andy Smith Sunnybrook Surgical Oncology Research Group Department of Surgery University of Toronto
 CRC Surgery Educational Slide Deck Dr. Andy Smith Sunnybrook Surgical Oncology Research Group Department of Surgery University of Toronto Staging Our group has made a major contribution re N-issues We
CRC Surgery Educational Slide Deck Dr. Andy Smith Sunnybrook Surgical Oncology Research Group Department of Surgery University of Toronto Staging Our group has made a major contribution re N-issues We
Disclosures. Personalized Approaches to Gastrointestinal Cancers. Objectives. What is personalized cancer care. Go through some genomic studies
 Personalized Approaches to Gastrointestinal Cancers Emily Groves, MD Colorectal Surgery Assistant Professor, Division of Surgical Oncology Disclosures None Objectives What is personalized medicine and
Personalized Approaches to Gastrointestinal Cancers Emily Groves, MD Colorectal Surgery Assistant Professor, Division of Surgical Oncology Disclosures None Objectives What is personalized medicine and
CREATE Trial Proposal: Survey of current practice and potential trial participation
 CREATE Trial Proposal: Survey of current practice and potential trial participation Approximately a quarter of newly diagnosed rectal cancer patients have features on pre-treatment pelvic MRI indicating
CREATE Trial Proposal: Survey of current practice and potential trial participation Approximately a quarter of newly diagnosed rectal cancer patients have features on pre-treatment pelvic MRI indicating
Advances in Imaging Technology In The Management of Colorectal Cancer
 Advances in Imaging Technology In The Management of Colorectal Cancer Dushyant Sahani, M.D Director of CT Associate Professor Department of Radiology Massachusetts General Hospital Harvard Medical School
Advances in Imaging Technology In The Management of Colorectal Cancer Dushyant Sahani, M.D Director of CT Associate Professor Department of Radiology Massachusetts General Hospital Harvard Medical School
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Rectal Cancer. Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco
 Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
Alison Douglass Gillian Lieberman, MD. November. Colon Cancer. Alison Douglass, Harvard Medical School Year III Gillian Lieberman, MD
 November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
The Role Of The Post-CRT MRI In Assessing Response
 Low Rectal Cancer: Is It Safe To Change The Plane Of Surgery? The Role Of The Post-CRT MRI In Assessing Response Nick Battersby, Mit Dattani, Nick West, Graham Branagan, Mark Gudgeon, Phil Quirke, Paris
Low Rectal Cancer: Is It Safe To Change The Plane Of Surgery? The Role Of The Post-CRT MRI In Assessing Response Nick Battersby, Mit Dattani, Nick West, Graham Branagan, Mark Gudgeon, Phil Quirke, Paris
Rectal Cancer : Curative treatment without surgery
 Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Large polyps: EMR, ESD, TEM and segmental resection. Terry Phang 2017 SON fall update
 Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Appendix 4 Urology Care Pathways
 Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
State-of-the-art of surgery for resectable primary tumors
 Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
Handling & Grossing of Colo-rectal Specimens for Tumours. for Medical Officers in Pathology
 Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Pathohistological Assessment of the Circular Margin of Resection During Total Mesorectal Excision, Conducted on The Malignant Formations of the Rectum
 International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment
International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment
Guideline for the Management of Vulval Cancer
 Version History Guideline for the Management of Vulval Cancer Version Date Brief Summary of Change Issued 2.0 20.02.08 Endorsed by the Governance Committee 2.1 19.11.10 Circulated at NSSG meeting 2.2 13.04.11
Version History Guideline for the Management of Vulval Cancer Version Date Brief Summary of Change Issued 2.0 20.02.08 Endorsed by the Governance Committee 2.1 19.11.10 Circulated at NSSG meeting 2.2 13.04.11
Index. Surg Oncol Clin N Am 14 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
THE ROLE OF HIGH RESOLUTION MAGNETIC RESONANCE IMAGING (MRI) IN DETECTING CIRCUMFERENTIAL RESECTION MARGIN (CRM) FOR THE PROGNOSIS OF RECTAL CANCER
 IN DETECTING CIRCUMFERENTIAL RESECTION MARGIN (CRM) FOR THE PROGNOSIS OF RECTAL CANCER") THE ROLE OF HIGH RESOLUTION MAGNETIC RESONANCE IMAGING (MRI) IN DETECTING CIRCUMFERENTIAL RESECTION MARGIN (CRM) FOR THE PROGNOSIS OF RECTAL CANCER Arpana Shrestha, Fu Tian and Jin-jian Xiang Department
THE ROLE OF HIGH RESOLUTION MAGNETIC RESONANCE IMAGING (MRI) IN DETECTING CIRCUMFERENTIAL RESECTION MARGIN (CRM) FOR THE PROGNOSIS OF RECTAL CANCER Arpana Shrestha, Fu Tian and Jin-jian Xiang Department
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer
 SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
Preoperative adjuvant radiotherapy
 Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS
 PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
The accuracy of the diagnostic pathway for staging of low-mid rectal tumours with endoscopic, MRI and Endorectal Ultrasound assessment.
 Carl Bradbury CoRIPS Research Award 130-9,963.00 The accuracy of the diagnostic pathway for staging of low-mid rectal tumours with endoscopic, MRI and Endorectal Ultrasound assessment. Lay Summary of Project
Carl Bradbury CoRIPS Research Award 130-9,963.00 The accuracy of the diagnostic pathway for staging of low-mid rectal tumours with endoscopic, MRI and Endorectal Ultrasound assessment. Lay Summary of Project
Treatment strategy of metastatic rectal cancer
 35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
State of the art: Standard(s) of radio/chemotherapy for rectal cancer
 of radio/chemotherapy for rectal cancer") State of the art: Standard(s) of radio/chemotherapy for rectal cancer Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Disclosure Advisory Board: Sanofi Oncology, Eli-
State of the art: Standard(s) of radio/chemotherapy for rectal cancer Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Disclosure Advisory Board: Sanofi Oncology, Eli-
Rectal Cancer. GI Practice Guideline
 Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES. Devon Paula Richardson
 NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES by Devon Paula Richardson Submitted in partial fulfilment of the requirements for the degree of Master
NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES by Devon Paula Richardson Submitted in partial fulfilment of the requirements for the degree of Master
How can surgeons help the Radiation Oncologists?
 How can surgeons help the Radiation Oncologists? Lorna Weir BC Surgical Oncology fall breast cancer update Oct 24, 2009 Disclosure no conflict of interest Outline Introduction OR reports Marking of surgical
How can surgeons help the Radiation Oncologists? Lorna Weir BC Surgical Oncology fall breast cancer update Oct 24, 2009 Disclosure no conflict of interest Outline Introduction OR reports Marking of surgical
Navigators Lead the Way
 RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
Rectal Cancer Cookbook Update. A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux
 Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
CHAPTER 7 Concluding remarks and implications for further research
 CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
A Review of Rectal Cancer. Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center
 A Review of Rectal Cancer Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center No disclosures Disclosures About me.. Grew up in Southern Illinois
A Review of Rectal Cancer Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center No disclosures Disclosures About me.. Grew up in Southern Illinois
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Ontario s Initiatives in Surgical Quality- The Successes & Where We are Going
 Ontario s Initiatives in Surgical Quality- The Successes & Where We are Going Robin S. McLeod Professor of Surgery and Health Policy, Management and Evaluation University of Toronto Lead, Quality Improvement
Ontario s Initiatives in Surgical Quality- The Successes & Where We are Going Robin S. McLeod Professor of Surgery and Health Policy, Management and Evaluation University of Toronto Lead, Quality Improvement
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
Audit Report. Colorectal Cancer Quality Performance Indicators. Patients diagnosed April 2016 March Published: March 2018
 Colorectal Cancer Managed Clinical Network Audit Report Colorectal Cancer Quality Performance Indicators Patients diagnosed April 2016 March 2017 Published: March 2018 Mr Michael Walker NOSCAN MCN Clinical
Colorectal Cancer Managed Clinical Network Audit Report Colorectal Cancer Quality Performance Indicators Patients diagnosed April 2016 March 2017 Published: March 2018 Mr Michael Walker NOSCAN MCN Clinical
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Colorectal cancer: pathology
 UK NEQAS for Molecular Pathology Colorectal cancer: pathology Nick West Pathology & Tumour Biology May 2013 Colorectal cancer (CRC) 40,695 new cases in 2010 15,708 deaths Management of CRC Surgery Main
UK NEQAS for Molecular Pathology Colorectal cancer: pathology Nick West Pathology & Tumour Biology May 2013 Colorectal cancer (CRC) 40,695 new cases in 2010 15,708 deaths Management of CRC Surgery Main
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Cancer Surgery OR Checklists The Foundation of Synoptic Reporting Elaine Mckevitt, MD, MEd FRCSC Carl J. Brown, MD MSc FRCSC
 Cancer Surgery OR Checklists The Foundation of Synoptic Reporting Elaine Mckevitt, MD, MEd FRCSC Carl J. Brown, MD MSc FRCSC Surgical Oncology Network, BCCA October 21, 2011 Synoptic Reporting Synoptic
Cancer Surgery OR Checklists The Foundation of Synoptic Reporting Elaine Mckevitt, MD, MEd FRCSC Carl J. Brown, MD MSc FRCSC Surgical Oncology Network, BCCA October 21, 2011 Synoptic Reporting Synoptic
Where are we at with organ preservation for rectal cancer? Simon Bach Queen Elizabeth Hospital Birmingham ACPGBI Edinburgh 2016
 Where are we at with organ preservation for rectal cancer? Simon Bach Queen Elizabeth Hospital Birmingham ACPGBI Edinburgh 2016 Disclosures Consultant for Johnson and Johnson (Ethicon Inc) Encompasses
Where are we at with organ preservation for rectal cancer? Simon Bach Queen Elizabeth Hospital Birmingham ACPGBI Edinburgh 2016 Disclosures Consultant for Johnson and Johnson (Ethicon Inc) Encompasses
Effective Health Care Program
 Comparative Effectiveness Review Number 142 Effective Health Care Program Imaging Tests for the Staging of Colorectal Cancer Executive Summary Background Colorectal Cancer In the United States each year
Comparative Effectiveness Review Number 142 Effective Health Care Program Imaging Tests for the Staging of Colorectal Cancer Executive Summary Background Colorectal Cancer In the United States each year
Guideline for the Management of Patients Suitable for Immediate Breast Reconstruction
 Version History Guideline for the Management of Patients Suitable for Immediate Breast Reconstruction Version Summary of change Date Issued 2.0 Endorsed by the Governance Committee 20.02.08 2.1 Circulated
Version History Guideline for the Management of Patients Suitable for Immediate Breast Reconstruction Version Summary of change Date Issued 2.0 Endorsed by the Governance Committee 20.02.08 2.1 Circulated
Clinical guideline Published: 1 November 2011 nice.org.uk/guidance/cg131
 Colorectal cancer: diagnosis and management Clinical guideline Published: 1 November 2011 nice.org.uk/guidance/cg131 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Colorectal cancer: diagnosis and management Clinical guideline Published: 1 November 2011 nice.org.uk/guidance/cg131 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
MRI Rectal Staging Template Revision Summary
 MRI Rectal Staging Template 2015 Revision Summary The following changes have been made since the June 2012 release. Formatting Standardized headings were added to the template. These headings are: Clinical
MRI Rectal Staging Template 2015 Revision Summary The following changes have been made since the June 2012 release. Formatting Standardized headings were added to the template. These headings are: Clinical
MRI: IMPACT ON RECTAL CANCER CARE AND STANDARDISATION
 MRI: IMPACT ON RECTAL CANCER CARE AND STANDARDISATION Professor Gina Brown Consultant Radiologist and Professor of Gastrointestinal Cancer Imaging, The Royal Marsden Hospital and Imperial College, London,
MRI: IMPACT ON RECTAL CANCER CARE AND STANDARDISATION Professor Gina Brown Consultant Radiologist and Professor of Gastrointestinal Cancer Imaging, The Royal Marsden Hospital and Imperial College, London,
Outcome of rectal cancer after radiotherapy with a long or short waiting period before surgery, a descriptive clinical study
 Original Article Outcome of rectal cancer after radiotherapy with a long or short waiting period before surgery, a descriptive clinical study Elmer E. van Eeghen 1, Frank den Boer 2, Sandra D. Bakker 1,
Original Article Outcome of rectal cancer after radiotherapy with a long or short waiting period before surgery, a descriptive clinical study Elmer E. van Eeghen 1, Frank den Boer 2, Sandra D. Bakker 1,
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Colorectal Surgery. Patient Care. Goals and Objectives
 Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/887/22038 holds various files of this Leiden University dissertation. Author: Swellengrebel, H.A.M. Title: Challenges in the multimodality treatment of rectal
Cover Page The handle http://hdl.handle.net/887/22038 holds various files of this Leiden University dissertation. Author: Swellengrebel, H.A.M. Title: Challenges in the multimodality treatment of rectal
Breast Surgery When Less is More and More is Less. E MacIntosh, MD June 6, 2015
 Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Radiotherapy for rectal cancer. Karin Haustermans Department of Radiation Oncology
 Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
BC CRC Update Unusual Colorectal Tumors
 BC CRC Update Unusual Colorectal Tumors Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary I
BC CRC Update Unusual Colorectal Tumors Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary I
AJCC 7 th Edition Staging Disease Site Webinar Colorectum
 AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310
AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310
7 th Edition Staging. AJCC 7 th Edition Staging. Disease Site Webinar. Colorectum. Overview. This webinar is sponsored by
 AJCC 7 th Edition Staging Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers
AJCC 7 th Edition Staging Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers
Follow up The way ahead. John Griffith
 Follow up The way ahead John Griffith Key Emerging Principles Risk stratified pathways of care Personalised care plan and treatment summary with a hand held record Information and education Remote monitoring
Follow up The way ahead John Griffith Key Emerging Principles Risk stratified pathways of care Personalised care plan and treatment summary with a hand held record Information and education Remote monitoring
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
TME and autonomic nerve preservation techniques: based on Video and Cadaveric anatomy
 TME and autonomic nerve preservation techniques: based on Video and Cadaveric anatomy Nam Kyu Kim M.D., Ph.D., FACS, FRCS, FASCRS Professor Department of Surgery Yonsei University College of Medicine Seoul,
TME and autonomic nerve preservation techniques: based on Video and Cadaveric anatomy Nam Kyu Kim M.D., Ph.D., FACS, FRCS, FASCRS Professor Department of Surgery Yonsei University College of Medicine Seoul,
Treatment of Locally Advanced Rectal Cancer: Current Concepts
 Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases
 Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Optimal Imaging Strategies for Rectal Cancer Staging and Ongoing Management
 Curr. Treat. Options in Oncol. (2016) 17: 32 DOI 10.1007/s11864-016-0403-7 Lower Gastrointestinal Cancers (AB Benson, Section Editor) Optimal Imaging Strategies for Rectal Cancer Staging and Ongoing Management
Curr. Treat. Options in Oncol. (2016) 17: 32 DOI 10.1007/s11864-016-0403-7 Lower Gastrointestinal Cancers (AB Benson, Section Editor) Optimal Imaging Strategies for Rectal Cancer Staging and Ongoing Management