Review Article Intersphincteric Resection for Low Rectal Cancer: An Overview
|
|
|
- Marjory Tucker
- 5 years ago
- Views:
Transcription
1 International Surgical Oncology Volume 2012, Article ID , 4 pages doi: /2012/ Review Article Intersphincteric Resection for Low Rectal Cancer: An Overview Constantine P. Spanos 1st Department of Surgery, Aristotelian University School of Medicine, Thessaloniki, Greece Correspondence should be addressed to Constantine P. Spanos, costasspanos@hotmail.com Received 8 February 2012; Accepted 5 March 2012 Academic Editor: Manousos-Georgios Pramateftakis Copyright 2012 Constantine P. Spanos. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The treatment of rectal cancer has evolved from being solely a surgical endeavor to a multidisciplinary practice. Despite the improvement in outcomes conferred by the addition of chemoradiation therapy to rectal cancer treatment, advances in surgical technique have significantly increased rates of sphincter preservation and the avoidance of a permanent stoma. In recent years, intersphincteric resection for low rectal cancer has been offered and performed in patients as an alternative to abdominoperineal resection. An overview of this procedure, including indications, oncological and functional results based on current literature, is presented herein. 1. Introduction There has been an evolution in the treatment of rectal cancer in recent times. A few decades ago, rectal cancer treatment was solely a surgical endeavour. Nowadays, it has evolved into therapy involving several disciplines. Nevertheless, surgery remains the cornerstone of curative treatment. The incorporation and widespread use of total mesorectal excision (TME) as the standard mode of surgical resection of adenocarcinoma of the rectum has been the most important surgical development in outcomes improvement for this disease [1, 2]. Supervised teaching of TME, as well as the detailed pathological audit of resected specimens, has also led to better oncological results [3]. Advances in surgical technique with the use of either advanced stapling or manual coloanal anastomoses have allowed for achieving continuity of the gastrointestinal tract at levels closer to the anal verge than those achieved historically. The advent of adjuvant and neoadjuvant chemoradiotherapy has also increased local control of disease [4] and in some instances has led to increased survival [5]. Surgery for rectal cancer in recent years has focused on anatomic and functional preservation of the sphincter without compromising oncological outcomes. Radical surgical treatment of cancers in lower third of the rectum has traditionally included low anterior resection (LAR) and coloanal anastomosis, and abdominoperineal resection (APR). Historically, the decision-making for sphinctersaving procedures has been related to the distance between the tumor and the anal sphincter complex [6]. In the 1980s, a distal margin of 5 cm was required. In the ensuing decades, the 2-cm-rule was accepted and adopted [6]. This rule has been challenged, however, and currently a distal margin of 1 cm is accepted as being appropriate for optimal oncologic outcome. This provides a greater proportion of rectal cancer patients with the possibility of sphincter preservation [7, 8]. Recently, adequacy of the circumferential resection margin is being considered of equal, if not greater, importance in the risk of local recurrence of rectal cancer [9]. In recent years, intersphincteric resection (ISR) has been proposed to offer sphincter preservation in patients with very low rectal lesions, as an alternative to APR. Of note, APR has consistently had higher rates of local recurrence rates (up to 22%) compared with LAR [10, 11]. 2. Materials and Methods A literature search for relevant articles in the English language associated with intersphincteric resection (ISR) between 2000 and 2012 was undertaken. All articles regarding intersphincteric resection were case series from single institutions or systematic reviews. Case reports were
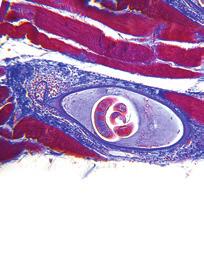
2 2 International Surgical Oncology excluded from this overview. Medline was the search engine utilized ISR: Definition. Schiessel and colleagues initially described the technique of ISR [12]. During ISR, a transanal division of the rectum, with removal of part or the entire internal anal sphincter (IAS) after TME, is performed, thus obtaining an adequate distal margin. Restoration of bowel continuity is achieved by performing a hand-sewn coloanal anastomosis. 3. Indications and Preoperative Evaluation When planning for proctectomy with ISR for rectal cancer, careful patient selection is paramount. Tumor height, its relationship to each component of the sphincter complex, and the presence or not of regional lymph node or distal metastases needs to be evaluated. For this reason, a combination of a careful physical exam and imaging modalities is utilized. Preoperative evaluation by the surgeon by means of digital rectal exam and rigid proctoscopy provides information regarding the level of the distal edge of tumour relative to the anal anatomic component of interest, which varies among experts in the literature [13, 14]. Anal anatomic components of interest include the anal verge, the dentate line and the anorectal ring. Specialized imaging is required to study the relationship of the IAS and external anal sphincter (EAS) with the tumour. Invasion of these structures by the lesion can also be depicted. Endorectal/endoanal ultrasound and magnetic resonance imaging (MRI) are performed for this reason. In addition, high-resolution MRI is accurate at estimating the circumferential margin; with an overall accuracy of 88% [15]. Additional cross-sectional imaging evaluates the presence of distal metastases. Inclusion criteria for performance of ISR include the following: (i) tumours located 30 mm from anal verge; (ii) tumours located 15 mm from dentate line; (iii) tumours located 1 cm from anorectal ring; (iv) local spread restricted to the rectal wall or the IAS; (v) adequate preoperative sphincter function and continence; (vi) absence of distant metastases. Contraindications to the performance of ISR are the presence of fecal incontinence, T4 lesions, undifferentiated tumors [10], as well as tumors invading the puborectalis and the external anal sphincter (EAS) [14]. A significant number of patients may require neoadjuvant chemoradiation therapy. In a systematic review of ISR involving 14 studies and 1289 patients who underwent ISR by Martin and colleagues, 44% of patients had stage III disease and 38% underwent preoperative chemoradiation overall [14]. Of note, in certain studies included in the review, preoperative radiation was a contraindication to performing ISR due to possible adverse functional effects. This is in contrast to a recent study by Denost and colleagues in which 93% of patients undergoing ISR received preoperative radiotherapy [16] Surgical Technique. The principle of the ISR technique is based on an anatomic dissection plane between the IAS and EAS [17]. The technique incorporates a combined abdominal and perineal approach. Initially, high ligation of the inferior mesenteric vessels is done. This is followed by TME down to the level of the pelvic floor. TME can be performed through a laparotomy or laparoscopically [6]. Subsequently, a per anal resection of the IAS is undertaken. The distal resection line may be at the intersphincteric groove (total ISR), between the dentate line and the intersphincteric groove (subtotal ISR), or at the dentate line (partial ISR). Additional maneuvers to reduce the risk of local tumor cell implantation include closure of the rectal stump, cytocidal washout, and pathological evaluation of the distal margin with frozen section analysis [18]. The specimen is usually delivered per anum. A handsewn coloanal anastomosis with construction of a colon J-pouch, transverse coloplasty, or straight anastomosis is performed. Certain groups, especially in Japan, perform lateral pelvic lymph node dissection for TNM stage III tumors [13]. A defunctioning temporary stoma is fashioned, which is closed 6 weeks to 12 months from the primary operation Short-Term Adverse Events. The overall operative mortality associated with ISR is 0.8% [14]. The cumulative morbidity rate is reported to be 25.8%. Anastomotic leak was experienced after a mean of 9.1%, and the rate of pelvic sepsis was 2.4% [14]. The rate of clinically apparent anastomotic leakage following stapled anastomosis following anterior resection is in the range of 3 15%. Rates of leakage rise significantly for more distally sited anastomoses [19]. Anastomotic leakage is associated with postoperative anastomotic stricture, cancer recurrence, poor postoperative function, as well as increased operative mortality [20]. In conclusion, ISR can be performed with acceptable rates of anastomotic leakage and low operative mortality Oncologic Outcomes. Radical surgical removal of the tumor is the only chance for permanent cure of rectal cancer, despite all progress in the development of oncologic therapy [10]. Rullier and colleagues [6] reported a local recurrence rate of 2% in a series of 92 patients undergoing ISR. Most patients (78%) had T3 lesions, and 88% underwent longcourse neoadjuvant radiochemotherapy. The overall 5-year survival rate was 81%, with a 5-year disease-free survival of 70%. Yamada et al. reported a similarly low 2.5% cumulative 5-year local recurrence rate, a 5-year disease-free survival rate of 83.5% for stage II patients and 72% for stage III patients [13].
3 International Surgical Oncology 3 Tilney and Tekkis performed a literature search to identify studies reporting outcomes following ISR. Twenty-one studies accumulating a total of 612 patients were identified [20]. The pooled rate of local recurrence was 9.5% with an average 5-year survival of 81.5%. Distant metastases occurred in 9.3%. In Martin s systematic review, the mean distal margin free from tumour was 17.1 mm, CRM-negative margins were achieved in 96% of patients, and the overall local recurrence rate was 6.7% (range : 0 23%). The 5-year overall and disease-free survival rate was 86.3% and 78.6%, respectively [14]. Rates of local recurrence following low anterior resection for the treatment of rectal cancer are commonly reported in the range of % following surgery alone [21].Preoperative chemoradiation therapy has led to local recurrence rates in the 6% range [4]. Therefore, the performance of ISR for treatment of very low rectal cancer affords similar oncologic outcomes to those of conventional resections. Moreover, Saito et al. [22] compared outcomes of patients undergoing ISR with patients undergoing APR. Similar local recurrence rates (ISR = 10.6%, APR = 15.7%, P = NS) and 5-year diseasefree survival (ISR = 69.1%, APR = 63.3%, P = NS) were reported. Patients undergoing ISR had significantly longer 5-year overall survival compared with patients undergoing APR (ISR = 80%, APR = 61.5%, P<0.05). In conclusion, local and distant oncologic outcomes are not comprised with ISR. It is considered that the risk of local recurrence may be a function of circumferential margin involvement rather than distal margin involvement. Risk factors for local and distant recurrence after ISR were reported by Akasu et al. [23]. Local recurrence rate was 6.7% and distant recurrence was 13%. In the multivariate analysis, risk factors for local recurrence included positive microscopic resection margins, focal d-differentiation of tumor (tumor budding), and elevated preoperative levels of CA 19-9 (>37U/mL). The identified risk factors for distant recurrence were pn1, pn2 disease, poor differentiation, and distance of tumor from anal verge, 2.5 cm Anorectal Physiology. An important goal of sphincterpreserving surgery is to reach acceptable quality of life levels by preserving fecal continence. The main concern of the ISR technique is functional outcome. Physiologic studies have shown that anal resting pressure is due to the IAS for 55%, the hemorrhoidal plexus for 15%, and to the EAS for 30% [24]. Total or partial excision of the IAS is bound to affect continence. Furthermore, preoperative radiation therapy may cause additional loss of sphincter function. Kohler et al. reported a 29% reduction in resting anal pressure following ISR. Squeeze pressure recovered to preoperative levels after 12 months [25]. Rullier et al. compared outcomes in patients undergoing partial or subtotal IAS resection. Subtotal excision of the sphincter was associated with significant reduction in resting but not squeeze pressure after ISR [26]. Of note, there have been no studies assessing anorectal physiology and continence after neoadjuvant radiation and prior to ISR Functional Outcomes and Quality of Life. As an antithesis to an aphorism by the famed architect Louis Sullivan, in rectal cancer surgery, function follows form (the type of operation performed). Loss of a part of the sphincter complex, loss of the rectal reservoir, and radiation is bound to have adverse effect on continence and defractory function. Bretagnol and colleagues reported that fecal continence measured by both the Kirwan and Wexner scores was significantly worse after ISR. In addition, the need for antidiarrheal medication was higher in patients undergoing ISR compared with patients that had undergone conventional coloanal anastomosis [27]. Frequency, urgency, the Wexner score, and the Fecal Incontinence Severity Index (FISI) were significantly improved following colonic J-pouch reconstruction compared with straight coloanal anastomosis [27]. Regarding quality of life (QOL), Bretagnol et al. used both the SF-36 and fecal incontinence quality of life (FIQL) to compare QOL between patients undergoing ISR and conventional coloanal anastomosis. There was no difference in the QOL scores between ISR patients and conventional coloanal anastomosis patients in the physical and mental subscales of the SF-36. In Martin s systematic review, the mean number of bowel movements per day was 2.7. Nearly half (51.2%) of patients reported perfect continence, about a third (29.1%) reported experienced fecal soiling, 23.8% had flatus incontinence, had 18.6% had urgency. In a large study assessing functional outcomes after ISR, Denost reported that half of the patients had a good functional result, 39% had minor fecal incontinence, and 11% had major incontinence [16].In the same study, the only independent predictors of good continence were a distance of tumour greater than 1 cm from the anorectal ring and anastomosis higher than 2 cm from the anal verge. Possible technical modifications when performing ISR may improve functional outcomes. These include partial ISR (when possible) and construction of a colon J-pouch. These are known to improve function in the first year after surgery. However, the effect is not sustained after 2 years [14]. 4. Conclusion In order to be successful in treating rectal cancer, good oncologic outcome is the first priority. Equally important is the achievement of an acceptable quality of life for the patient. The avoidance of a permanent stoma and all of the concomitant morbidity associated with it may be of greater importance to the patient. Low anterior resection with intersphincteric dissection and partial or total excision of the IAS may be offered an alternative to APR in selected patients. The functional outcomes after ISR are expected to be inferior to those of conventional low anterior resection; this information needs to be frankly communicated to the patient. The morbidity, mortality, and oncological outcomes
4 4 International Surgical Oncology after ISR are acceptable. Careful patient selection and sound operative technique, with emphasis on high-quality preoperative imaging and functional assessment, should lead to superior results. These principles have been closely examined at our own institution, and we have embarked on our first cases of intersphincteric resection in selected patients. References [1] R. J. Heald and R. D. H. Ryall, Recurrence and survival after total mesorectal excision for rectal cancer, The Lancet, vol. 1, no. 8496, pp , [2] J. K. MacFarlane, R. D. Ryall, and R. J. Heald, Mesorectal excision for rectal cancer, The Lancet, vol. 341, no. 8843, pp , [3] P. Quirke, R. Steele, J. Monson et al., Effect of the plane of surgery achievd on local recurrence in patients with operable rectal cancer: a prospective study using data from the MRC CR07 and NCIC-CTG C016 randomised clinical trial, The Lancet, vol. 373, no. 9666, pp , [4] R. Sauer, H. Becker, W. Hohenberger et al., Preoperative versus postoperative chemoradiotherapy for rectal cancer, The New England Medicine, vol. 351, no. 17, pp , [5] Swedish Rectal Cancer Trial, Improved survival with preoperative radiotherapy in resectable rectal cancer. Swedish Rectal Cancer Trial, The New England Medicine, vol. 336, pp , 1997, published correction appears in The New England Medicine, vol. 336, pp 1539, [6] E. Rullier, C. Laurent, F. Bretagnol, A. Rullier, V. Vendrely, and F. Zerbib, Sphincter-saving resection for all rectal carcinomas: the end of the 2-cm distal rule, Annals of Surgery, vol. 241, no. 3, pp , [7] H. Ueno, H. Mochizuki, Y. Hashiguchi et al., Preoperative parameters expanding the indication of sphincter preserving surgery in patients with advanced low rectal cancer, Annals of Surgery, vol. 239, no. 1, pp , [8] R.P.Kiran,L.Lian,andI.C.Lavery, Doesasubcentimeter distal resection margin adversely influence oncologic outcomes in patients with rectal cancer undergoing restorative proctectomy? Diseases of the Colon & Rectum, vol. 54, no. 2, pp , [9] P. Quirke, P. Durdey, M. F. Dixon, and N. S. Williams, Local recurrence of rectal adenocarcinoma due to inadequate surgical resection. Histopathological study of lateral tumour spread and surgical excision, The Lancet, vol. 2, no. 8514, pp , [10] R. Schiessel, J. Karner-Hanusch, F. Herbst, B. Teleky, and M. Wunderlich, Intersphincteric resection for low rectal tumours, British Surgery, vol. 81, no. 9, pp , [11] A. Wibe, A. Syse, F. Andersen et al., Oncological outcomes after total mesorectal excision for cure for cancer of the lower rectum: anterior vs abdominoperineal resection, Diseases of the Colon & Rectum, vol. 47, no. 1, pp , [12] R. Schiessel, J. Karner-Hanusch, F. Herbst, B. Teleky, and M. Wunderlich, Intersphincteric resection for low rectal tumours, British Surgery, vol. 81, no. 9, pp , [13] K. Yamada, S. Ogata, Y. Saiki, M. Fukunaga, Y. Tsuji, and M. Takano, Long-term results of intersphincteric resection for low rectal cancer, Diseases of the Colon & Rectum, vol. 52, no. 6, pp , [14] S. T. Martin, H. M. Heneghan, and D. C. Winter, Systematic review of outcomes after intersphincteric resection for low rectal cancer, British Surgery, vol. 99, no. 5, pp , [15] MERCURY Study Group, Diagnostic accuracy of preoperative magnetic resonance imaging in predicting curative resection of rectal cancer: prospective observational study, British Medical Journal, vol. 333, no. 7572, pp , [16] Q. Denost, C. Laurent, M. Capdepont, F. Zerbib, and E. Rullier, Risk factors for fecal incontinence after intersphincteric resection for rectal cancer, Diseases of the Colon & Rectum, vol. 54, no. 8, pp , [17] R. Chamlou, Y. Parc, T. Simon et al., Long-term results of intersphincteric resection for low rectal cancer, Annals of Surgery, vol. 246, no. 6, pp , [18] M. Ito, N. Saito, M. Sugito, A. Kobayashi, Y. Nishizawa, and Y. Tsunoda, Analysis of clinical factors associated with anal function after intersphincteric resection for very low rectal cancer, Diseases of the Colon & Rectum, vol. 52, no. 1, pp , [19] E. Rullier, C. Laurent, J. L. Garrelon, P. Michel, J. Saric, and M. Parneix, Risk factors for anastomotic leakage after resection of rectal cancer, British Surgery, vol. 85, no. 3, pp , [20] H. S. Tilney and P. P. Tekkis, Extending the horizons of restorative rectal surgery: intersphincteric resection for low rectal cancer, Colorectal Disease, vol. 10, no. 1, pp. 3 15, [21] A. G. Heriot, P. P. Tekkis, A. Darzi, and J. Mackay, Surgery for local recurrence of rectal cancer, Colorectal Disease, vol. 8, no. 9, pp , [22] N. Saito, M. Sugito, M. Ito et al., Oncologic outcome of intersphincteric resection for very low rectal cancer, World Surgery, vol. 33, no. 8, pp , [23] T. Akasu, M. Takawa, S. Yamamoto et al., Intersphincteric resection for very low rectal adenocarcinoma: univariate and multivariate analyses of risk factors for recurrence, Annals of Surgical Oncology, vol. 15, no. 10, pp , [24] Y. P. Sangwan and J. A. Solla, Internal anal sphincter: advances and insights, Diseases of the Colon & Rectum, vol. 41, no. 10, pp , [25] A. Köhler, S. Athanasiadis, A. Ommer, and E. Psarakis, Longterm results of low anterior resection with intersphincteric anastomosis in carcinoma of the lower one-third of the rectum: analysis of 31 patients, Diseases of the Colon & Rectum, vol. 43, no. 6, pp , [26] E. Rullier, F. Zerbib, C. Laurent et al., Intersphincteric resection with excision of internal anal sphincter for conservative treatment of very low rectal cancer, Diseases of the Colon & Rectum, vol. 42, no. 9, pp , [27] F. Bretagnol, E. Rullier, C. Laurent, F. Zerbib, R. Gontier, and J. Saric, Comparison of functional results and quality of life between intersphincteric resection and conventional coloanal anastomosis for low rectal cancer, Diseases of the Colon & Rectum, vol. 47, no. 6, pp , 2004.











5 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Analysis of the clinical factors associated with anal function after intersphincteric resection for very low rectal cancer
 Tokoro et al. World Journal of Surgical Oncology 2013, 11:24 WORLD JOURNAL OF SURGICAL ONCOLOGY RESEARCH Open Access Analysis of the clinical factors associated with anal function after intersphincteric
Tokoro et al. World Journal of Surgical Oncology 2013, 11:24 WORLD JOURNAL OF SURGICAL ONCOLOGY RESEARCH Open Access Analysis of the clinical factors associated with anal function after intersphincteric
Laparoscopic Resection Of Colon & Rectal Cancers. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Delayed anastomotic leakage following laparoscopic intersphincteric resection for lower rectal cancer: report of four cases and literature review
 Iwamoto et al. World Journal of Surgical Oncology (2017) 15:143 DOI 10.1186/s12957-017-1208-2 CASE REPORT Open Access Delayed anastomotic leakage following laparoscopic intersphincteric resection for lower
Iwamoto et al. World Journal of Surgical Oncology (2017) 15:143 DOI 10.1186/s12957-017-1208-2 CASE REPORT Open Access Delayed anastomotic leakage following laparoscopic intersphincteric resection for lower
Rectal Cancer. Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco
 Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
Index. Surg Oncol Clin N Am 14 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
Innovations in rectal cancer surgery TAMIS and transanal TME
 Innovations in rectal cancer surgery TAMIS and transanal TME A.D Hoore MD PhD, EBSQ CR Chair Departement of Abdominal Surgery University Hospitals Leuven, Belgium Actual treatment in rectal Early rectal
Innovations in rectal cancer surgery TAMIS and transanal TME A.D Hoore MD PhD, EBSQ CR Chair Departement of Abdominal Surgery University Hospitals Leuven, Belgium Actual treatment in rectal Early rectal
Long-term results of extended intersphincteric resection for very low rectal cancer: a retrospective study
 Kim et al. BMC Surgery (2016) 16:21 DOI 10.1186/s12893-016-0133-6 RESEARCH ARTICLE Open Access Long-term results of extended intersphincteric resection for very low rectal cancer: a retrospective study
Kim et al. BMC Surgery (2016) 16:21 DOI 10.1186/s12893-016-0133-6 RESEARCH ARTICLE Open Access Long-term results of extended intersphincteric resection for very low rectal cancer: a retrospective study
WHAT IS LARS? LOW ANTERIOR RESECTIONSYNDROME. Sophie Pilkington. Colorectal Surgeon University Hospital Southampton
 WHAT IS LARS? LOW ANTERIOR RESECTIONSYNDROME Sophie Pilkington Colorectal Surgeon University Hospital Southampton INTRODUCTION UK Bowel cancer 2013 41,100 new cases INTRODUCTION UK Bowel cancer 2013 41,100
WHAT IS LARS? LOW ANTERIOR RESECTIONSYNDROME Sophie Pilkington Colorectal Surgeon University Hospital Southampton INTRODUCTION UK Bowel cancer 2013 41,100 new cases INTRODUCTION UK Bowel cancer 2013 41,100
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
State-of-the-art of surgery for resectable primary tumors
 Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Ein Leben nach tiefer Rektumresektion: Was erwartet unsere Patienten im Langzeitverlauf?
 Ein Leben nach tiefer Rektumresektion: Was erwartet unsere Patienten im Langzeitverlauf? Dieter Hahnloser Klinik für Viszeral- und Transplantationschirurgie UniverstätsSpital Zürich Low Rectal Resection
Ein Leben nach tiefer Rektumresektion: Was erwartet unsere Patienten im Langzeitverlauf? Dieter Hahnloser Klinik für Viszeral- und Transplantationschirurgie UniverstätsSpital Zürich Low Rectal Resection
Innovations in Rectal Cancer Surgery
 Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
A Review of Rectal Cancer. Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center
 A Review of Rectal Cancer Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center No disclosures Disclosures About me.. Grew up in Southern Illinois
A Review of Rectal Cancer Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center No disclosures Disclosures About me.. Grew up in Southern Illinois
Rectal Cancer: Classic Hits
 Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
Rectal Cancer Update 2008 The Last 5 cm. Consensus Building
 Rectal Cancer Update 2008 The Last 5 cm Consensus Building Case Distal Rectal Cancer 65 male physician Rectal mass: 5cm from anal verge, 1cm above sphincter? Imaging choice: CT vs MR vs ERUS? Adjuvant
Rectal Cancer Update 2008 The Last 5 cm Consensus Building Case Distal Rectal Cancer 65 male physician Rectal mass: 5cm from anal verge, 1cm above sphincter? Imaging choice: CT vs MR vs ERUS? Adjuvant
COLON AND RECTAL CANCER
 COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
Pelvic Organ Functions: Urinary, Sexual and Bowel Dysfunction after Rectal Surgery
 Pelvic Organ Functions: Urinary, Sexual and Bowel Dysfunction after Rectal Surgery Disclosure M ADHULIKA G. V ARMA M D PROFESSOR AND CHIEF S E CTION O F COLORECTAL S U R G ERY U N I V ERS ITY O F CALIFORNIA,
Pelvic Organ Functions: Urinary, Sexual and Bowel Dysfunction after Rectal Surgery Disclosure M ADHULIKA G. V ARMA M D PROFESSOR AND CHIEF S E CTION O F COLORECTAL S U R G ERY U N I V ERS ITY O F CALIFORNIA,
Pathohistological Assessment of the Circular Margin of Resection During Total Mesorectal Excision, Conducted on The Malignant Formations of the Rectum
 International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment
International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment
COLON AND RECTAL CANCER
 No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
Incidence of Colorectal Cancers- Australia. Anterior Resection 5/23/2018. What spurs us to investigate?
 Incidence of Colorectal Cancers- Australia 17,000 Colorectal cancers in 2018 20% of Colorectal cancers are in the Rectum 12.3% of all new cancers Anterior Resection Syndrome (ARS) Lisa Wilson. Colorectal
Incidence of Colorectal Cancers- Australia 17,000 Colorectal cancers in 2018 20% of Colorectal cancers are in the Rectum 12.3% of all new cancers Anterior Resection Syndrome (ARS) Lisa Wilson. Colorectal
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
The effect of rectal washout on local recurrence following rectal cancer surgery
 COLORECTAL SURGERY Ann R Coll Surg Engl 208; 00: 46 5 doi 0.308/rcsann.207.0202 The effect of rectal washout on local recurrence following rectal cancer surgery SR Moosvi, K Manley, J Hernon Norfolk and
COLORECTAL SURGERY Ann R Coll Surg Engl 208; 00: 46 5 doi 0.308/rcsann.207.0202 The effect of rectal washout on local recurrence following rectal cancer surgery SR Moosvi, K Manley, J Hernon Norfolk and
PROCARE FINAL FEEDBACK Definitions
 1 PROCARE FINAL FEEDBACK 2006-2014 Definitions Version 0.2 29/10/2015 2 Table of Contents Introduction... 3 Part 1: PROCARE indicators 2006-2014... 4 1.1. Methods... 4 1.1.1. Descriptive numbers... 4 1.1.2.
1 PROCARE FINAL FEEDBACK 2006-2014 Definitions Version 0.2 29/10/2015 2 Table of Contents Introduction... 3 Part 1: PROCARE indicators 2006-2014... 4 1.1. Methods... 4 1.1.1. Descriptive numbers... 4 1.1.2.
Quality of life of patients after low anterior, intersphincteric, and abdominoperineal resection for rectal cancer a matched-pair analysis
 Int J Colorectal Dis (2013) 28:679 688 DOI 10.1007/s00384-013-1683-z ORIGINAL ARTICLE Quality of life of patients after low anterior, intersphincteric, and abdominoperineal resection for rectal cancer
Int J Colorectal Dis (2013) 28:679 688 DOI 10.1007/s00384-013-1683-z ORIGINAL ARTICLE Quality of life of patients after low anterior, intersphincteric, and abdominoperineal resection for rectal cancer
1. Background. increased sphincter preservation rate. Nonetheless, the 5- year disease-free survival and overall survival rates were
 Gastroenterology Research and Practice Volume 2016, Article ID 7870815, 5 pages http://dx.doi.org/10.1155/2016/7870815 Research Article Does Extending the Waiting Time of Low-Rectal Cancer Surgery after
Gastroenterology Research and Practice Volume 2016, Article ID 7870815, 5 pages http://dx.doi.org/10.1155/2016/7870815 Research Article Does Extending the Waiting Time of Low-Rectal Cancer Surgery after
NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES. Devon Paula Richardson
 NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES by Devon Paula Richardson Submitted in partial fulfilment of the requirements for the degree of Master
NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES by Devon Paula Richardson Submitted in partial fulfilment of the requirements for the degree of Master
Sphincter Sparing Procedures: Is it a standard for Management of Low Rectal Cancer
 Journal of the Egyptian Nat. Cancer Inst., Vol. 16, No. 4, December: 210-215, 2004 Sphincter Sparing Procedures: Is it a standard for Management of Low Rectal Cancer EL-SAYED ASHRAF KHALIL, M.D.FRCS; MOHAMAD
Journal of the Egyptian Nat. Cancer Inst., Vol. 16, No. 4, December: 210-215, 2004 Sphincter Sparing Procedures: Is it a standard for Management of Low Rectal Cancer EL-SAYED ASHRAF KHALIL, M.D.FRCS; MOHAMAD
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/38705 holds various files of this Leiden University dissertation. Author: Gijn, Willem van Title: Rectal cancer : developments in multidisciplinary treatment,
Cover Page The handle http://hdl.handle.net/1887/38705 holds various files of this Leiden University dissertation. Author: Gijn, Willem van Title: Rectal cancer : developments in multidisciplinary treatment,
CURRENT PRACTICE OF FOLLOW-UP MANAGEMENT AFTER POTENTIALLY CURATIVE RESECTION OF RECTAL CANCER
 CURRENT PRACTICE OF FOLLOW-UP MANAGEMENT AFTER POTENTIALLY CURATIVE RESECTION OF RECTAL CANCER 1. a. If you are retired, or do not perform such surgery, please check the box at the right, answer questions
CURRENT PRACTICE OF FOLLOW-UP MANAGEMENT AFTER POTENTIALLY CURATIVE RESECTION OF RECTAL CANCER 1. a. If you are retired, or do not perform such surgery, please check the box at the right, answer questions
Robotic versus Laparoscopic Intersphincteric Resection for Low Rectal Cancer: A Comparative Study of Short-term Outcomes
 ORIGINAL ARTICLE pissn 2234-778X eissn 2234-5248 J Minim Invasive Surg 2015;18(4):98-105 Journal of Minimally Invasive Surgery Robotic versus Laparoscopic Intersphincteric Resection for Low Rectal Cancer:
ORIGINAL ARTICLE pissn 2234-778X eissn 2234-5248 J Minim Invasive Surg 2015;18(4):98-105 Journal of Minimally Invasive Surgery Robotic versus Laparoscopic Intersphincteric Resection for Low Rectal Cancer:
Role of MRI for Staging Rectal Cancer
 Role of MRI for Staging Rectal Cancer High-resolution MRI has supplanted endoscopic ultrasound for staging rectal cancer. High-resolution MR images closely match histology and can show details such as
Role of MRI for Staging Rectal Cancer High-resolution MRI has supplanted endoscopic ultrasound for staging rectal cancer. High-resolution MR images closely match histology and can show details such as
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Outcome of rectal cancer after radiotherapy with a long or short waiting period before surgery, a descriptive clinical study
 Original Article Outcome of rectal cancer after radiotherapy with a long or short waiting period before surgery, a descriptive clinical study Elmer E. van Eeghen 1, Frank den Boer 2, Sandra D. Bakker 1,
Original Article Outcome of rectal cancer after radiotherapy with a long or short waiting period before surgery, a descriptive clinical study Elmer E. van Eeghen 1, Frank den Boer 2, Sandra D. Bakker 1,
RECTAL CARCINOMA: A DISTANCE APPROACH. Stephanie Nougaret
 RECTAL CARCINOMA: A DISTANCE APPROACH Stephanie Nougaret stephanienougaret@free.fr Despite the major improvements that have been made due to total mesorectal excision (TME) management of rectal cancer
RECTAL CARCINOMA: A DISTANCE APPROACH Stephanie Nougaret stephanienougaret@free.fr Despite the major improvements that have been made due to total mesorectal excision (TME) management of rectal cancer
Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach
 Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
Preoperative adjuvant radiotherapy
 Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
University of Groningen. Colorectal Anastomoses Bakker, Ilsalien
 University of Groningen Colorectal Anastomoses Bakker, Ilsalien IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
University of Groningen Colorectal Anastomoses Bakker, Ilsalien IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer
 SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
Clinical Study Laparoscopic versus Open Surgery for Colorectal Cancer: A Retrospective Analysis of 163 Patients in a Single Institution
 Minimally Invasive Surgery, Article ID 530314, 6 pages http://dx.doi.org/10.1155/2014/530314 Clinical Study Laparoscopic versus Open Surgery for Colorectal Cancer: A Retrospective Analysis of 163 Patients
Minimally Invasive Surgery, Article ID 530314, 6 pages http://dx.doi.org/10.1155/2014/530314 Clinical Study Laparoscopic versus Open Surgery for Colorectal Cancer: A Retrospective Analysis of 163 Patients
Neoadjuvant Therapy for Rectal Cancer is Overrated. Joon H. Lee, Research Resident University of Colorado 8/31/2009
 Neoadjuvant Therapy for Rectal Cancer is Overrated Joon H. Lee, Research Resident University of Colorado 8/31/2009 Objectives Brief overview of staging rectal cancer Current guidelines for evaluation and
Neoadjuvant Therapy for Rectal Cancer is Overrated Joon H. Lee, Research Resident University of Colorado 8/31/2009 Objectives Brief overview of staging rectal cancer Current guidelines for evaluation and
Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma?
 17 th Panhellenic IBD Congress Thessaloniki May 2018 Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma? Janindra Warusavitarne Consultant Colorectal Surgeon, St
17 th Panhellenic IBD Congress Thessaloniki May 2018 Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma? Janindra Warusavitarne Consultant Colorectal Surgeon, St
Colorectal Surgery. Patient Care. Goals and Objectives
 Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
CHAPTER 7 Concluding remarks and implications for further research
 CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference
 Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
Endoscopic Ultrasonography Assessment for Ampullary and Bile Duct Malignancy
 Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
MRI of Rectal Cancer
 MRI of Rectal Cancer Arnd-Oliver Schäfer Mathias Langer MRI of Rectal Cancer Clinical Atlas Prof. Dr. Arnd-Oliver Schäfer Department of Diagnostic Radiology Freiburg University Hospital Hugstetter Straße
MRI of Rectal Cancer Arnd-Oliver Schäfer Mathias Langer MRI of Rectal Cancer Clinical Atlas Prof. Dr. Arnd-Oliver Schäfer Department of Diagnostic Radiology Freiburg University Hospital Hugstetter Straße
Risk Factors of Permanent Stomas in Patients with Rectal Cancer after Low Anterior Resection with Temporary Stomas
 Original Article http://dx.doi.org/10.3349/ymj.2015.56.2.447 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 56(2):447-453, 2015 Risk Factors of Permanent Stomas in Patients with Rectal Cancer after Low
Original Article http://dx.doi.org/10.3349/ymj.2015.56.2.447 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 56(2):447-453, 2015 Risk Factors of Permanent Stomas in Patients with Rectal Cancer after Low
Colostomy & Ileostomy
 Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Comparison of Loop Ileostomy and Loop Colostomy as Defunctioning Stoma in Low Rectal Cancer Surgery NCI Experience
 Kasr El Aini Journal of Surgery VOL., 12, NO 1 January 2011 75 Comparison of Loop Ileostomy and Loop Colostomy as Defunctioning Stoma in Low Rectal Cancer Surgery NCI Experience Ahmed Abbas, MD MRCS General
Kasr El Aini Journal of Surgery VOL., 12, NO 1 January 2011 75 Comparison of Loop Ileostomy and Loop Colostomy as Defunctioning Stoma in Low Rectal Cancer Surgery NCI Experience Ahmed Abbas, MD MRCS General
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh
 Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
The main issues of the rectal resection for carcinoma
 The main issues of the rectal resection for carcinoma - Level of the vessels transection and mobilisation of the splenic flexure - Lymphadenectomy - Distal margin - Parietal invasion of rectal wall - Functional
The main issues of the rectal resection for carcinoma - Level of the vessels transection and mobilisation of the splenic flexure - Lymphadenectomy - Distal margin - Parietal invasion of rectal wall - Functional
Case Report 17-Week Delay Surgery after Chemoradiation in Rectal Cancer with Complete Pathological Response
 Case Reports in Surgery Volume 2015, Article ID 816491, 5 pages http://dx.doi.org/10.1155/2015/816491 Case Report 17-Week Delay Surgery after Chemoradiation in Rectal Cancer with Complete Pathological
Case Reports in Surgery Volume 2015, Article ID 816491, 5 pages http://dx.doi.org/10.1155/2015/816491 Case Report 17-Week Delay Surgery after Chemoradiation in Rectal Cancer with Complete Pathological
Colorectal Cancer. Nimalan Pathma-Nathan
 Colorectal Cancer Nimalan Pathma-Nathan Introduction Rooms at HSS and Westmead Private Outpatients at Westmead Multidisciplinary clinic Westmead Surgery and scopes HSS Westmead Public, Private and Children
Colorectal Cancer Nimalan Pathma-Nathan Introduction Rooms at HSS and Westmead Private Outpatients at Westmead Multidisciplinary clinic Westmead Surgery and scopes HSS Westmead Public, Private and Children
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 5, Issue 1 2015 Article 1 Ileal U Pouch Reconstruction Proximal To Straight Sublevator Ileoanal Anastomosis Following Total Proctocolectomy For Low Rectal Cancer
World Journal of Colorectal Surgery Volume 5, Issue 1 2015 Article 1 Ileal U Pouch Reconstruction Proximal To Straight Sublevator Ileoanal Anastomosis Following Total Proctocolectomy For Low Rectal Cancer
Staging of cancer patients is an important tool for the selection
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2007;5:997 1003 Improvement of Staging by Combining Tumor and Treatment Parameters: The Value for Prognostication in Rectal Cancer MARLEEN J. E. M. GOSENS,* J.
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2007;5:997 1003 Improvement of Staging by Combining Tumor and Treatment Parameters: The Value for Prognostication in Rectal Cancer MARLEEN J. E. M. GOSENS,* J.
The accuracy of the diagnostic pathway for staging of low-mid rectal tumours with endoscopic, MRI and Endorectal Ultrasound assessment.
 Carl Bradbury CoRIPS Research Award 130-9,963.00 The accuracy of the diagnostic pathway for staging of low-mid rectal tumours with endoscopic, MRI and Endorectal Ultrasound assessment. Lay Summary of Project
Carl Bradbury CoRIPS Research Award 130-9,963.00 The accuracy of the diagnostic pathway for staging of low-mid rectal tumours with endoscopic, MRI and Endorectal Ultrasound assessment. Lay Summary of Project
UCL. Rectum Adenocarcinoma. Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans
 Rectum Adenocarcinoma Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans Fifth Belgian Surgical Week May 6th, 2004, Oostende SOR rectum adenocarcinoma Indication of radiotherapy
Rectum Adenocarcinoma Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans Fifth Belgian Surgical Week May 6th, 2004, Oostende SOR rectum adenocarcinoma Indication of radiotherapy
Rectal Cancer Location: the Surgical Perspective
 Rectal Cancer Location: the Surgical Perspective September 5, 2014 W. Donald Buie MD,MSc, FRCSC Associate Professor of Surgery University of Calgary I have no disclosures 1 Outline Surgical Anatomy review
Rectal Cancer Location: the Surgical Perspective September 5, 2014 W. Donald Buie MD,MSc, FRCSC Associate Professor of Surgery University of Calgary I have no disclosures 1 Outline Surgical Anatomy review
Incidence and risk factors of anastomotic leaks. By: khaled Said Assistant professor of colorectal surgery Alexandria
 Incidence and risk factors of anastomotic leaks By: khaled Said Assistant professor of colorectal surgery Alexandria Anastomotic leakage after colorectal surgery is a major and potentially life-threatening
Incidence and risk factors of anastomotic leaks By: khaled Said Assistant professor of colorectal surgery Alexandria Anastomotic leakage after colorectal surgery is a major and potentially life-threatening
R. J. L. F. Loffeld, 1 P. E. P. Dekkers, 2 and M. Flens Introduction
 ISRN Gastroenterology Volume 213, Article ID 87138, 5 pages http://dx.doi.org/1.1155/213/87138 Research Article The Incidence of Colorectal Cancer Is Decreasing in the Older Age Cohorts in the Zaanstreek
ISRN Gastroenterology Volume 213, Article ID 87138, 5 pages http://dx.doi.org/1.1155/213/87138 Research Article The Incidence of Colorectal Cancer Is Decreasing in the Older Age Cohorts in the Zaanstreek
Citation for published version (APA): Bartels, S. A. L. (2013). Laparoscopic colorectal surgery: beyond the short-term effects
: Bartels, S. A. L. (2013). Laparoscopic colorectal surgery: beyond the short-term effects") UvA-DARE (Digital Academic Repository) Laparoscopic colorectal surgery: beyond the short-term effects Bartels, S.A.L. Link to publication Citation for published version (APA): Bartels, S. A. L. (2013).
UvA-DARE (Digital Academic Repository) Laparoscopic colorectal surgery: beyond the short-term effects Bartels, S.A.L. Link to publication Citation for published version (APA): Bartels, S. A. L. (2013).
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
Rectal Cancer. GI Practice Guideline
 Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
Staging of rectal cancer on MRI: What the surgeons want to know.
 Staging of rectal cancer on MRI: What the surgeons want to know. Poster No.: C-1108 Congress: ECR 2014 Type: Educational Exhibit Authors: G. Ayub, R. Chittal, A. Lowe, A. S. Punekar ; Leeds/, 1 2 1 2 2
Staging of rectal cancer on MRI: What the surgeons want to know. Poster No.: C-1108 Congress: ECR 2014 Type: Educational Exhibit Authors: G. Ayub, R. Chittal, A. Lowe, A. S. Punekar ; Leeds/, 1 2 1 2 2
Current innovations in colorectal surgery
 Current innovations in colorectal surgery KS Chapple Consultant Colorectal Surgeon Sheffield Teaching Hospitals NHS Trust Do we need more innovations? What innovations are there and are they worthwhile?
Current innovations in colorectal surgery KS Chapple Consultant Colorectal Surgeon Sheffield Teaching Hospitals NHS Trust Do we need more innovations? What innovations are there and are they worthwhile?
Case Report Uncommon Mixed Type I and II Choledochal Cyst: An Indonesian Experience
 Case Reports in Surgery Volume 2013, Article ID 821032, 4 pages http://dx.doi.org/10.1155/2013/821032 Case Report Uncommon Mixed Type I and II Choledochal Cyst: An Indonesian Experience Fransisca J. Siahaya,
Case Reports in Surgery Volume 2013, Article ID 821032, 4 pages http://dx.doi.org/10.1155/2013/821032 Case Report Uncommon Mixed Type I and II Choledochal Cyst: An Indonesian Experience Fransisca J. Siahaya,
Local Excision of Rectal Cancer Techniques and Outcomes
 Local Excision of Rectal Cancer Techniques and Outcomes Manoj J. Raval, MD, MSc, FRCSC Clinical Assistant Professor, UBC Rectal Cancer Update 2008 October 25, 2008 Overview Techniques & Description Patient
Local Excision of Rectal Cancer Techniques and Outcomes Manoj J. Raval, MD, MSc, FRCSC Clinical Assistant Professor, UBC Rectal Cancer Update 2008 October 25, 2008 Overview Techniques & Description Patient
Laparoscopic intersphincteric resection versus an open approach for low rectal cancer: a meta-analysis
 Chen et al. World Journal of Surgical Oncology (2017) 15:229 DOI 10.1186/s12957-017-1304-3 REVIEW Laparoscopic intersphincteric resection versus an open approach for low rectal cancer: a meta-analysis
Chen et al. World Journal of Surgical Oncology (2017) 15:229 DOI 10.1186/s12957-017-1304-3 REVIEW Laparoscopic intersphincteric resection versus an open approach for low rectal cancer: a meta-analysis
Postoperative Chemoradiotherapy for Rectal Carcinoma on Bowel Function
 ANNALS OF SURGERY Vol. 220, No. 5, 676-682 1994 J. B. Lippincott Company The Long-Term Effect of Adjuvant Postoperative Chemoradiotherapy for Rectal Carcinoma on Bowel Function C. F. Kollmorgen,* A. P.
ANNALS OF SURGERY Vol. 220, No. 5, 676-682 1994 J. B. Lippincott Company The Long-Term Effect of Adjuvant Postoperative Chemoradiotherapy for Rectal Carcinoma on Bowel Function C. F. Kollmorgen,* A. P.
Laparoscopic vs Robotic Rectal Cancer Surgery: Making it better!
 Laparoscopic vs Robotic Rectal Cancer Surgery: Making it better! Francis Seow- Choen Medical Director Seow-Choen Colorectal Centre Singapore In all situations: We have to use the right tool for the job
Laparoscopic vs Robotic Rectal Cancer Surgery: Making it better! Francis Seow- Choen Medical Director Seow-Choen Colorectal Centre Singapore In all situations: We have to use the right tool for the job
Operative Technique: Karen Horvath, MD, FACS. SCOAP Retreat June 17, 2011
 Operative Technique: Total Mesorectal Excision Karen Horvath, MD, FACS University it of Washington, Seattle SCOAP Retreat June 17, 2011 No Disclosures Purpose What is Total Mesorectal Excision (TME)? How
Operative Technique: Total Mesorectal Excision Karen Horvath, MD, FACS University it of Washington, Seattle SCOAP Retreat June 17, 2011 No Disclosures Purpose What is Total Mesorectal Excision (TME)? How
Safety and feasibility of laparoscopic intersphincteric resection for a lower rectal tumor
 4142 Safety and feasibility of laparoscopic intersphincteric resection for a lower rectal tumor NOBUHISA MATSUHASHI, TAKAO TAKAHASHI, TOSHIYUKI TANAHASHI, SATOSHI MATSUI, HISASHI IMAI, YOSHIHIRO TANAKA,
4142 Safety and feasibility of laparoscopic intersphincteric resection for a lower rectal tumor NOBUHISA MATSUHASHI, TAKAO TAKAHASHI, TOSHIYUKI TANAHASHI, SATOSHI MATSUI, HISASHI IMAI, YOSHIHIRO TANAKA,
Hester Cheung Memorial Lecture
 Hester Cheung Memorial Lecture STEVEN D WEXNER, MD, PHD (HON),FACS, FRCS, FRCS(ED) Director, Digestive Disease Center; Chairman, Department of Colorectal Surgery; Cleveland Clinic Florida Professor of
Hester Cheung Memorial Lecture STEVEN D WEXNER, MD, PHD (HON),FACS, FRCS, FRCS(ED) Director, Digestive Disease Center; Chairman, Department of Colorectal Surgery; Cleveland Clinic Florida Professor of
Original Article. Page 1 of 9
 Original Article Page 1 of 9 Clinical impact of laparoscopic intersphincteric resection following neoadjuvant chemoradiotherapy for locally advanced rectal cancer: case-controlled study Hajime Fujishima
Original Article Page 1 of 9 Clinical impact of laparoscopic intersphincteric resection following neoadjuvant chemoradiotherapy for locally advanced rectal cancer: case-controlled study Hajime Fujishima
Quality of life after minimally invasive surgery for rectal cancer
 Chen et al. Mini-invasive Surg 2018;2:42 DOI: 10.20517/2574-1225.2018.59 Mini-invasive Surgery Review Open Access Quality of life after minimally invasive surgery for rectal cancer Jason H. Chen 1, Jennifer
Chen et al. Mini-invasive Surg 2018;2:42 DOI: 10.20517/2574-1225.2018.59 Mini-invasive Surgery Review Open Access Quality of life after minimally invasive surgery for rectal cancer Jason H. Chen 1, Jennifer
Clinical Study Changing Trends in Use of Laparoscopy: A Clinical Audit
 Minimally Invasive Surgery, Article ID 562785, 4 pages http://dx.doi.org/10.1155/2014/562785 Clinical Study Changing Trends in Use of Laparoscopy: A Clinical Audit Ritu Khatuja, 1 Geetika Jain, 1 Sumita
Minimally Invasive Surgery, Article ID 562785, 4 pages http://dx.doi.org/10.1155/2014/562785 Clinical Study Changing Trends in Use of Laparoscopy: A Clinical Audit Ritu Khatuja, 1 Geetika Jain, 1 Sumita
Anastomotic Leakage Following Low Anterior Resection of Rectal Cancer Considering the Role of Protective Stoma
 Anastomotic Leakage Following Low Anterior Resection of Rectal Cancer Considering the Role of Protective Stoma Mozafar M 1, Sobhiyeh MR 1, Heibatollahi M 2 Original Article Abstract Background and aims:
Anastomotic Leakage Following Low Anterior Resection of Rectal Cancer Considering the Role of Protective Stoma Mozafar M 1, Sobhiyeh MR 1, Heibatollahi M 2 Original Article Abstract Background and aims:
Colorectal Cancer Dashboard
 Process Risk Assessment Presence or absence of cancer in first-degree blood relatives documented for patients with colorectal cancer Percent of patients with colorectal cancer for whom presence or absence
Process Risk Assessment Presence or absence of cancer in first-degree blood relatives documented for patients with colorectal cancer Percent of patients with colorectal cancer for whom presence or absence
PROCARE FINAL FEEDBACK
 1 PROCARE FINAL FEEDBACK General report 2006-2014 Version 2.1 08/12/2015 PROCARE indicators 2006-2014... 3 Demographic Data... 3 Diagnosis and staging... 4 Time to first treatment... 6 Neoadjuvant treatment...
1 PROCARE FINAL FEEDBACK General report 2006-2014 Version 2.1 08/12/2015 PROCARE indicators 2006-2014... 3 Demographic Data... 3 Diagnosis and staging... 4 Time to first treatment... 6 Neoadjuvant treatment...
Rectal Cancer. About the Colon and Rectum. Symptoms. Colorectal Cancer Screening
 Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Innovative Surgical Management in the Treatment of Rectal Cancer: MIS, Robotic, and Beyond
 Innovative Surgical Management in the Treatment of Rectal Cancer: MIS, Robotic, and Beyond Jonathan E. Efron, MD, FACS, FASCRS The Mark M Ravitch, MD Endowed Professorship in Surgery Chief of the Ravitch
Innovative Surgical Management in the Treatment of Rectal Cancer: MIS, Robotic, and Beyond Jonathan E. Efron, MD, FACS, FASCRS The Mark M Ravitch, MD Endowed Professorship in Surgery Chief of the Ravitch
L impatto dell imaging sulla definizione della strategia terapeutica
 GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
Transanal endoscopic microsurgery for early rectal cancer: single center experience
 Original paper Videosurgery Transanal endoscopic microsurgery for early rectal cancer: single center experience Narimantas Samalavicius 1,2, Marijus Ambrazevicius 1, Alfredas Kilius 1, Kestutis Petrulis
Original paper Videosurgery Transanal endoscopic microsurgery for early rectal cancer: single center experience Narimantas Samalavicius 1,2, Marijus Ambrazevicius 1, Alfredas Kilius 1, Kestutis Petrulis
Treatment of Locally Advanced Rectal Cancer: Current Concepts
 Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Х Anniversary International Conference "Russian School of Colorectal Surgery"
 Х Anniversary International Conference "Russian School of Colorectal Surgery" The most large-scale event for coloproctologists in the post-soviet states May, 29-30, 2017 Moscow, World Trade Center (WTC)
Х Anniversary International Conference "Russian School of Colorectal Surgery" The most large-scale event for coloproctologists in the post-soviet states May, 29-30, 2017 Moscow, World Trade Center (WTC)
Motility Disorders. Pelvic Floor. Colorectal Center for Functional Bowel Disorders (N = 701) January 2010 November 2011
 January 2010 November 2011") Motility Disorders Pelvic Floor Colorectal Center for Functional Bowel Disorders (N = 71) January 21 November 211 New Patients 35 3 25 2 15 1 5 Constipation Fecal Incontinence Rectal Prolapse Digestive-Genital
Motility Disorders Pelvic Floor Colorectal Center for Functional Bowel Disorders (N = 71) January 21 November 211 New Patients 35 3 25 2 15 1 5 Constipation Fecal Incontinence Rectal Prolapse Digestive-Genital
Synchronous Hepatic Cryotherapy and Resection
 HPB Surgery, 2000, Vol. 11, pp. 379-382 Reprints available directly from the publisher Photocopying permitted by license only (C) 2000 OPA (Overseas Publishers Association) N.V. Published by license under
HPB Surgery, 2000, Vol. 11, pp. 379-382 Reprints available directly from the publisher Photocopying permitted by license only (C) 2000 OPA (Overseas Publishers Association) N.V. Published by license under
Cover Page. Author: Wiltink, Lisette Title: Long-term effects and quality of life after treatment for rectal cancer Issue Date:
 Cover Page The handle http://hdl.handle.net/1887/46445 holds various files of this Leiden University dissertation Author: Wiltink, Lisette Title: Long-term effects and quality of life after treatment for
Cover Page The handle http://hdl.handle.net/1887/46445 holds various files of this Leiden University dissertation Author: Wiltink, Lisette Title: Long-term effects and quality of life after treatment for
!"#$ Oncology Outcomes Report
 !"#$ Oncology Outcomes Report The Cleveland Clinic Florida Cancer Institute is dedicated to the comprehensive care of patients with cancer. Oncologists collaborate with a variety of physicians across multiple
!"#$ Oncology Outcomes Report The Cleveland Clinic Florida Cancer Institute is dedicated to the comprehensive care of patients with cancer. Oncologists collaborate with a variety of physicians across multiple
The Laparoscopic Approach in the Treatment of Distal Colorectal Cancer
 The Open Colorectal Cancer Journal, 2011, 4, 13-17 13 Open Access The Laparoscopic Approach in the Treatment of Distal Colorectal Cancer Alexander Lebedyev 1, Damien Urban 2, Danny Rosin 1, Amram Ayalon
The Open Colorectal Cancer Journal, 2011, 4, 13-17 13 Open Access The Laparoscopic Approach in the Treatment of Distal Colorectal Cancer Alexander Lebedyev 1, Damien Urban 2, Danny Rosin 1, Amram Ayalon
Treatment strategy of metastatic rectal cancer
 35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 3, Issue 4 2013 Article 3 Sigmoidorectal Intussusception Presenting as Prolapse Per Anus in an Adult Venugopal Hg Hasmukh B. Vora Mahendra S. Bhavsar SMT.NHL
World Journal of Colorectal Surgery Volume 3, Issue 4 2013 Article 3 Sigmoidorectal Intussusception Presenting as Prolapse Per Anus in an Adult Venugopal Hg Hasmukh B. Vora Mahendra S. Bhavsar SMT.NHL
Lymph node harvest in rectal cancer surgery following neoadjuvant chemoradiotherapy
 Journal of Surgery 2014; 2(2): 27-1 Published online April 10, 2014 (http://www.sciencepublishinggroup.com/j/js) doi: 10.1148/j.js.20140202.1 Lymph node harvest in rectal cancer surgery following neoadjuvant
Journal of Surgery 2014; 2(2): 27-1 Published online April 10, 2014 (http://www.sciencepublishinggroup.com/j/js) doi: 10.1148/j.js.20140202.1 Lymph node harvest in rectal cancer surgery following neoadjuvant