Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
|
|
|
- Eleanore Sanders
- 5 years ago
- Views:
Transcription

1 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
2 Adenoma Low-grade appendiceal mucinous neoplasm High-grade appendiceal mucinous neoplasm Adenocarcinoma Serrated lesions or polyps Goblet cell tumors
3 Adenomatous proliferation resembling colorectal type (pencillate nuclei, pseudostratified, etc). Intact muscularis mucosae No tumor outside appendix Can be tubular, tubulovillous, or villous Dysplasia graded similar to other sites in GI tract Low Grade High Grade Defined in this way, an adenoma is benign.

4
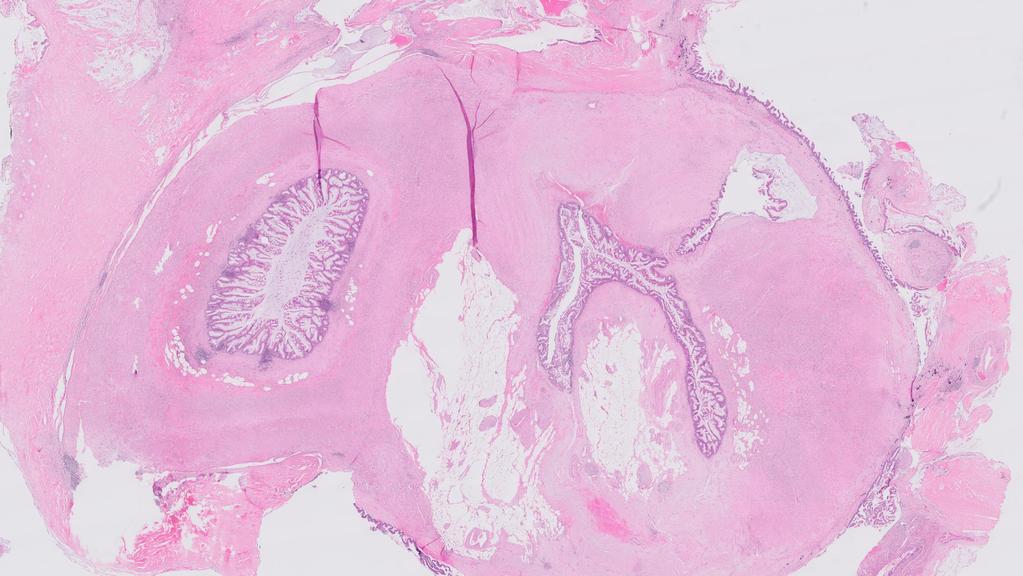
5 A low grade mucinous epithelial tumor characterized by villiform or undulating growth pattern and tall mucinous epithelial cells. Pushing invasion. Destruction of muscularis mucosae with fibrosis, diverticula, herniations, dissections, etc. with possible rupture.

6

7

8

9

10

11

12

13

14

15

16
17
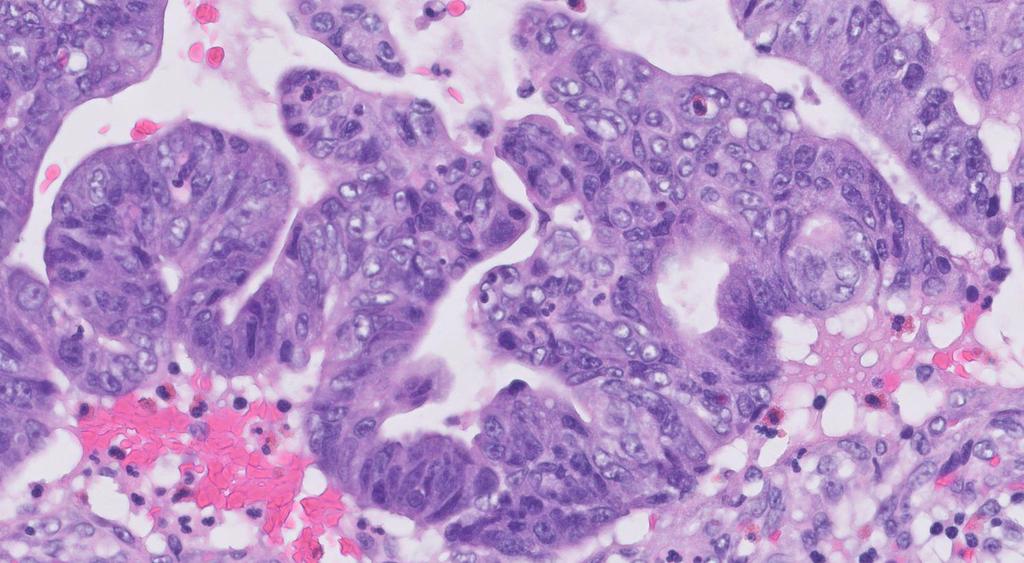
18 Pushing invasion but unequivocal high-grade cytology. May have complex architecture (micropapillary or cribriform). HAMNs are rare! Most tumors with high-grade cytology are invasive cancers; evaluate the entire tumor before concluding it is a HAMN. T stages the same as adenocarcinoma! Tis(HAMN) does not exist. Tumor into muscle is T2. But there is no data to support that HAMN is more likely than LAMN to disseminate.
19 Adenocarcinoma Adenocarcinoma, not otherwise specified Mucinous adenocarcinoma Adenocarcinoma, colonic type Signet ring cell adenocarcinoma Serrated adenocarcinoma

20

21 Mucinous adenocarcinoma

22
23 50 cases without cells in periappendiceal mucin 2 (4%) recurred as pseudomyxoma peritonei Neither was submitted entirely, raising the possibility that epithelial cells were unsampled 15 cases with cells in the periappendiceal mucin 5 (33%) recurred ( p=0.03); 1 died of disease
24
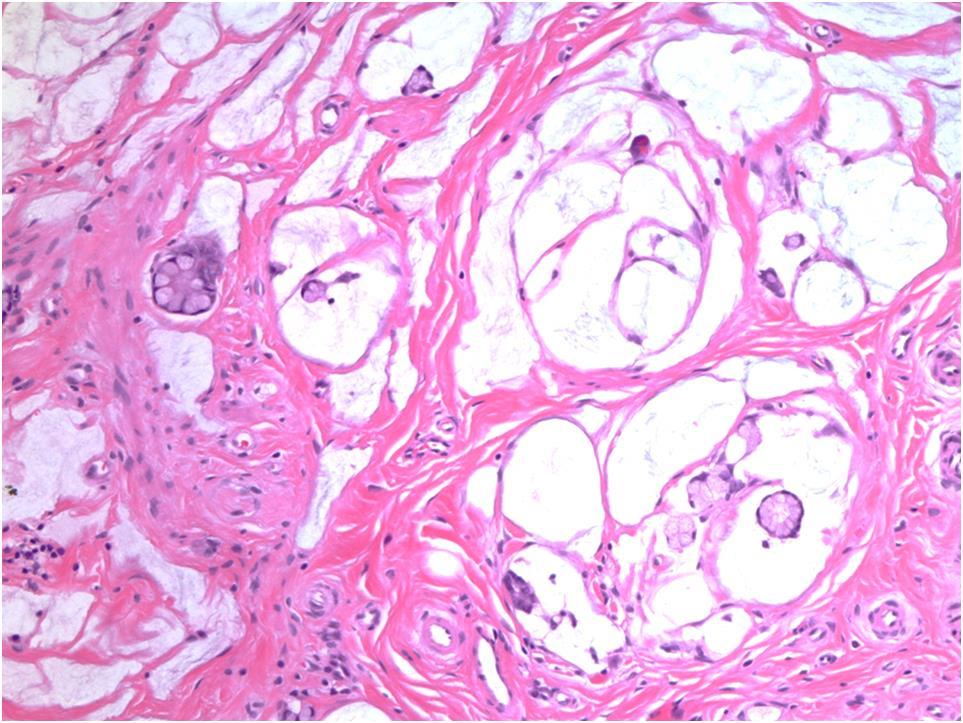
25 Low grade appendiceal mucinous neoplasm, ruptured, with extrusion of acellular mucin on the appendiceal serosa. In the comments: Clarify that there is mucin BUT NO mucinous epithelium on the surface of the appendix; Rupture of a mucinous neoplasm with extrusion of acellular mucin in the RLQ is associated with a low risk of recurrence as pseudomyxoma peritonei.

26

27

28 Low grade appendiceal mucinous neoplasm, ruptured, with involvement of the peri-appendiceal serosa (localized pseudomyxoma peritonei). Clarify that there is mucin AND low grade mucinous epithelium on the surface of the appendix; This is considered high risk of recurrence as PMP; Management varies. One paper reports that prognosis for low grade limited peritoneal disease was not affected by watching for radiologic progression (Ann Surg Oncol 2014)
29 Accumulation of mucin within the peritoneal cavity associated with mucinous tumor implants. Usually from a mucinous tumor of the appendix, but can arise from pancreas, gallbladder, colon, urachus, and teratoma of the ovary.

30 Classical low grade PMP

31 Classical low grade PMP Classic Pseudomyxoma Peritonei (Grade 1)

32 Peritoneal carcinoma
33 Ronnett et al. Am J Surg Pathol 1995 Ronnett et al. Cancer 2001
34 Am J Surg Pathol 2006;30:


35
36 3 grades of pseudomyxoma peritonei Grade 1: Abundant mucin, scant cells, low-grade cytology Grade 2: Distinguished from grade 1 by: High cytologic grade (>10% of tumor) High tumor cellularity Neoplastic epithelium in > 20% of mucin pools at 20X Destructive invasion Infiltrating jagged, irregular glands Expansile/confluent cribriform growth Small nests/glands within small mucin pools ( small mucin pool pattern ) Grade 3: Signet ring cells present Usual primary tumor LAMN, rarely HAMN Invasive adenocarcinoma, rarely HAMN Signet ring cell carcinoma or goblet cell adenocarcinoma

37 Small mucin pool pattern of grade 2 PMP
38 Tis(LAMN) LAMN confined by the muscularis propria No T1 or T2 for LAMN T3 LAMN that extends to subserosa. T4a - Tumor invades visceral peritoneum. 7 th edition: Tumor penetrates visceral peritoneum, including mucinous tumors within the right lower quadrant. M1a Intraperitoneal acellular mucin M1b Intraperitoneal metastasis only, including peritoneal mucinous deposits containing tumor cells M1c Metastasis to sites other than peritoneum
39 Extent of tumor spread in appendectomy TNM stages Prognosis Tumor is confined to the appendix: serosa intact, no mucin or tumor outside appendix Tumor perforates serosa with acellular mucin on the serosa or in the peritoneum Tumor perforates serosa with cellular mucin on the serosa Tis(LAMN) or T3 T4 T4 Almost certainly cured by appendectomy Low-risk of recurrence as pseudomyxoma High-risk of recurrence as pseudomyxoma Ultimately, it is critical to describe the extent of spread of tumor and mucin, emphasizing whether there is acellular or cellular mucin on the appendix serosa
40 LAMNs show frequent KRAS mutations (90%) and GNAS mutations (>50%). LAMNs express DNA mismatch repair proteins and are MSS. Mutations typical of colorectal carcinoma (APC, p53, and SMAD4) are not common in appendiceal mucinous neoplasms, but are more common in high-grade tumors. Misdraji J, Burgart LJ, Lauwers GY. Modern Pathology 2004;17: Zauber P, Berman E, Marotta S, et al. Scandinavian J Gastroenterol 2011;46: Nishikawa G, Sekine S, Ogawa R, et al. British J Cancer 2013;108: Hara K, Saito T, Hayashi T, et al. Pathology, Research and Practice. 2013;211:
41 Mucinous adenocarcinomas commonly have KRAS mutations and 35% have GNAS Occasional mucinous adenocarcinomas demonstrate mutations in TP53, PIK3CA, SMAD4, AKT1, and APC. Only 3% of appendix cancers show MSI (as opposed to 20% in the right colon and 15% of colon overall). MSI cancers may be more likely to show loss of MSH2/MSH6 expression than MLH1 promoter methylation. Kabbani W, Houlihan PS, Luthra R, et al. Modern Pathology 2002;15: Misdraji J, Burgart LJ, Lauwers GY. Modern Pathology 2004;17: Hara K, Saito T, Hayashi T, et al. Pathology, Research and Practice. 2013;211: Taggart MW, Galbincea J, Mansfield PF, et al. AJSP 2013;37:
42 Ruptured appendiceal diverticular disease Retention mucocele Endometriosis with intestinal metaplasia

43

44

45

46

47

48
49 Colon Hyperplastic polyp Sessile serrated adenoma/polyp SSA/P with dysplasia Traditional serrated adenoma Mixed polyp Appendix Hyperplastic polyp/mucosal hyperplasia Serrated polyp/lesion without dysplasia Serrated polyp/lesion with dysplasia

50

51

52

53

54
55
56 Appendix serrated polyps often have KRAS mutations (50%), particularly those with dysplasia. They infrequently have BRAF mutations (10-20%). KRAS may be more biologically important in the appendix than BRAF, and the serrated pathway of carcinogenesis may have less relevance in the appendix than in the colon. Yantiss RK, Panczykowski A, Misdraji J, et al. AJSP 2007;31: Pai RK, Hartman DJ, Gonzalo DH, et al. Human pathology. 2014;45:227-35
57 Appendiceal tumor with mucinous and neuroendocrine differentiation M = F; average 40s Present with appendicitis, incidentally, or as ovarian metastases ( Krukenberg ) Grossly, normal-appearing or somewhat thickened appendix Size difficult to determine in many cases Proximal margin must be identified
58 Keratin

59

60

61

62 Chromogranin
63
64 Developed a grading system that is based on identifying carcinomatous growth patterns Carcinomatous growth patterns Fused or cribriform glands Single file structures Diffusely infiltrating signet ring cells Sheets of tumor cells Compressed goblet cell nests with little or no stroma Extracellular mucin pools harboring epithelium demonstrating gland fusion or the absence of lumens
65 < 25% carcinomatous growth: Goblet cell carcinoid Confined to the appendix Benign behavior > 50% carcinomatous growth: Mixed carcinoidadenocarcinoma Highly likely to have spread beyond the appendix Aggressive biology
66 Classification of tumors with at least focal GCC Goblet cell carcinoid Adenocarcinoma ex GCC, signet ring cell type Adenocarcinoma ex GCC, poorly differentiated adenocarcinoma type
67 Goblet cell carcinoid Adenocarcinoma ex GCC, signet ring cell type. Partial or nearly complete loss of goblet cell clustered architecture. Signet cells as single cells, irregular clusters, or disordered arrangements but not sheets. Cytologic atypia.

68

69
70 Goblet cell carcinoid Adenocarcinoma ex GCC, signet ring cell type Adenocarcinoma ex GCC, poorly differentiated adenocarcinoma type At least 1 low power field or 1 mm 2 indistinguishable from poorly differentiated gland forming adenocarcinoma, signet ring cell adenocarcinoma, neuroendocrine carcinoma, or undifferentiated carcinoma.

71

72
73 Burke: 142 tumors classified by the proportion of adenocarcinoma (< 25%, 25-50%, > 50%, pure adenocarcinoma) Tang: Adenocarcinoma component classified as either signet ring cell or non-signet ring cell type
74 GCC, Mixed GCC-Adenocarcinoma, and Adenocarcinoma of the Appendix Taggart et al. Arch Pathol Lab Med 2015;139: Intermediate group (Group 2; 25-50%) does somewhat better than > 50% (group 3). Tumors with >50% adenocarcinoma (group 3) behave like adenocarcinoma (group 4)
75 GCC, Mixed GCC-Adenocarcinoma, and Adenocarcinoma of the Appendix Taggart et al. Arch Pathol Lab Med 2015;139: Group 2 Signet ring cell type and non-signet ring cell type behave similarly. 3 4
76 The term carcinoid misleads pathologists to inappropriately use neuroendocrine staging systems and oncologists to consider therapies for endocrine tumors. Adenocarcinoma ex GCC implies that an adenocarcinoma evolves from an endocrine tumor, which is confusing and untrue. Studies have noted inconsistent use of terminology for difficult or high-grade tumors, and only moderate interobserver agreement using Tang systems.
77 Mutations in chromatin remodeling genes (ARID2, ARID1A, KMT2D) occur in relatively high proportion of GCC (suggests epigenetic modification in the early stage of tumor formation). Mutations typical of CRC adenocarcinoma occur at low frequency (KRAS, P53, BRAF); usually in high-grade tumors. A subset have mutations that occur in signet ring cell gastric cancer (e-cadherin, RHOA). The overlap between GCC and adenoca-ex-gcc suggests a distinct tumor with a spectrum of grades. Johncilla M, Stachler M, Misdraji J, et al. Modern Pathology 2018;31: Jesinghaus M, Konukiewitz B, Foersch S, et al. Modern Pathology 2018;31:
78 126 tumors studied. Grading system with parallels in colorectal grading. Instead of % gland formation, we used % of tubular/clustered growth. Cut off values established by Burke and Taggart. Proposed nomenclature: Goblet cell adenocarcinoma, grade 1-3. G1: Tumors > 75% clustered or tubular growth. G2: Tumors with 50-75% clustered or tubular growth. G3: Tumors with < 50% tubular or clustered growth.

79 Low-grade pattern

80 Low-grade pattern

81 Low-grade pattern

82 Low-grade pattern

83 High-grade pattern

84 High-grade pattern

85 High-grade pattern

86 High-grade pattern

87 High-grade pattern

88 High-grade pattern

89 Goblet cell adenocarcinoma, Low grade: > 75% low grade patterns; < 25% high grade patterns Goblet cell adenocarcinoma, Intermediate grade: 50-75% low grade patterns; 25-50% high grade patterns Goblet cell adenocarcinoma, High grade: < 50% low grade patterns; > 50% high grade patterns Overall survival by grade

90
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Syllabus. Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix. Appendiceal tumors. Summary provided Complete presentation
 2016 Current Issues in Surgical Pathology Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix Syllabus Summary provided Complete presentation sanjay.kakar@ucsf.edu Sanjay Kakar, MD University
2016 Current Issues in Surgical Pathology Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix Syllabus Summary provided Complete presentation sanjay.kakar@ucsf.edu Sanjay Kakar, MD University
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Despite advances in our understanding of appendiceal. An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms
 REVIEW ARTICLE An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms Mark A. Valasek, MD, PhD* and Reetesh K. Pai, MD Abstract: Despite advances in our understanding of appendiceal
REVIEW ARTICLE An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms Mark A. Valasek, MD, PhD* and Reetesh K. Pai, MD Abstract: Despite advances in our understanding of appendiceal
Chapter 6 Frozen Section Evaluation of the Appendix
 Chapter 6 Frozen Section Evaluation of the Appendix Abstract Appendiceal tumors are rarely diagnosed preoperatively, and their classification is both challenging and controversial owing to their tendency
Chapter 6 Frozen Section Evaluation of the Appendix Abstract Appendiceal tumors are rarely diagnosed preoperatively, and their classification is both challenging and controversial owing to their tendency
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
Serrated Lesions in the Bowel Cancer Screening Programme
 Serrated Lesions in the Bowel Cancer Screening Programme Mark Arends Cambridge & Edinburgh Serrated Lesions of Large Bowel 1. Hyperplastic polyp 2. Serrated adenoma 3. Mixed polyp 4. Sessile serrated lesion
Serrated Lesions in the Bowel Cancer Screening Programme Mark Arends Cambridge & Edinburgh Serrated Lesions of Large Bowel 1. Hyperplastic polyp 2. Serrated adenoma 3. Mixed polyp 4. Sessile serrated lesion
A WHO update on Serrated Polyps
 A WHO update on Serrated Polyps Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Am J Gastroenterol. 2010 Nov 2. [Epub ahead of The Clinical Significance of Serrated Polyps.
A WHO update on Serrated Polyps Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Am J Gastroenterol. 2010 Nov 2. [Epub ahead of The Clinical Significance of Serrated Polyps.
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Defective mismatch repair in the pathogenesis of low-grade appendiceal mucinous neoplasms and adenocarcinomas
 & 2004 USCAP, Inc All rights reserved 0893-3952/04 $30.00 www.modernpathology.org Defective mismatch repair in the pathogenesis of low-grade appendiceal mucinous neoplasms and adenocarcinomas Joseph Misdraji
& 2004 USCAP, Inc All rights reserved 0893-3952/04 $30.00 www.modernpathology.org Defective mismatch repair in the pathogenesis of low-grade appendiceal mucinous neoplasms and adenocarcinomas Joseph Misdraji
Protocol for the Examination of Specimens From Patients With Carcinoma of the Appendix
 Protocol for the Examination of Specimens From Patients With Carcinoma of the Appendix Version: Appendix 4.0.0.1 Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC
Protocol for the Examination of Specimens From Patients With Carcinoma of the Appendix Version: Appendix 4.0.0.1 Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Part 3. Case #7 History:
 Part 3 Case #7 History: The patient is a 25 year old woman who had a colectomy for familial adenomatous polyposis 2 years ago. No carcinoma was found in her colectomy specimen. She presents now with 2
Part 3 Case #7 History: The patient is a 25 year old woman who had a colectomy for familial adenomatous polyposis 2 years ago. No carcinoma was found in her colectomy specimen. She presents now with 2
Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX
 Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX Appendix Occurrence of lesions (%) Acute appendicitis 72 Normal 16 Fibrosis 3 (Cyst-)Adenoma 3 Diverticulitis
Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX Appendix Occurrence of lesions (%) Acute appendicitis 72 Normal 16 Fibrosis 3 (Cyst-)Adenoma 3 Diverticulitis
Protocol for the Examination of Specimens From Patients With Carcinoma of the Appendix
 Protocol for the Examination of Specimens From Patients With Carcinoma of the Appendix Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For
Protocol for the Examination of Specimens From Patients With Carcinoma of the Appendix Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Low-grade serous neoplasia. Robert A. Soslow, MD
 Low-grade serous neoplasia Robert A. Soslow, MD soslowr@mskcc.org Outline Orientation Ovarian tumor overview Non serous borderline tumors Serous borderline tumors Clinical summary Morphologic description
Low-grade serous neoplasia Robert A. Soslow, MD soslowr@mskcc.org Outline Orientation Ovarian tumor overview Non serous borderline tumors Serous borderline tumors Clinical summary Morphologic description
Colon and Rectum: 2018 Solid Tumor Rules
 2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School
 Precursors of Colorectal Carcinoma Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Hyperplastic polyp Adenomatous polyp Colorectal carcinoma IBD-associated (1-2%) Sporadic
Precursors of Colorectal Carcinoma Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Hyperplastic polyp Adenomatous polyp Colorectal carcinoma IBD-associated (1-2%) Sporadic
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Appendiceal Pathology. Prof Ray McMahon Histopathology Department Manchester Royal Infirmary Bryan Warren School Sarajevo November 2016
 Appendiceal Pathology Prof Ray McMahon Histopathology Department Manchester Royal Infirmary Bryan Warren School Sarajevo November 2016 Appendicitis Appendicitis Appendicitis Scattered groups of neutrophils
Appendiceal Pathology Prof Ray McMahon Histopathology Department Manchester Royal Infirmary Bryan Warren School Sarajevo November 2016 Appendicitis Appendicitis Appendicitis Scattered groups of neutrophils
Update on Colonic Serrated (and Conventional) Adenomatous Polyps
 Adenomatous Polyps") Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING
 COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
3 cell types in the normal ovary
 Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors (neoplasms) 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal
Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors (neoplasms) 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal
Serrated Polyps and a Classification of Colorectal Cancer
 Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
Beyond the APC era Alternative pathways to CRC. Jeremy R Jass McGill University
 Beyond the APC era Alternative pathways to CRC Jeremy R Jass McGill University Outline Limitations of APC model KRAS and serrated polyps CRC and CpG island methylation Serrated pathway to CRC Fusion pathways
Beyond the APC era Alternative pathways to CRC Jeremy R Jass McGill University Outline Limitations of APC model KRAS and serrated polyps CRC and CpG island methylation Serrated pathway to CRC Fusion pathways
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer
 General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
Mucinous tumours of appendix and ovary: an overview and evaluation of current practice
 Department of Pathology, Laboratory Medicine Program, University Health Network, University of Toronto, Toronto, Canada Correspondence to Dr Marjan Rouzbahman, Department of Pathology, 11th floor, Eaton
Department of Pathology, Laboratory Medicine Program, University Health Network, University of Toronto, Toronto, Canada Correspondence to Dr Marjan Rouzbahman, Department of Pathology, 11th floor, Eaton
Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms
 Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms Dr. Claudia LY WONG, Department of Surgery, Kwong Wah Hospital Joint Hospital Surgical Grand Round Presentation,
Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms Dr. Claudia LY WONG, Department of Surgery, Kwong Wah Hospital Joint Hospital Surgical Grand Round Presentation,
Diagnostic Difficulties Encountered Among Colorectal Polyps
 Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
Polyps in general: is a descriptive term of forming a mass that is exophytic & polypoid.
 ميحرلا نمحرلا هللا مسب Gastric Tumors: Benign tumours & tumor-like conditions: -Mucosal: Gastric polyps (they are uncommon) -Mesenchymal tumours: Leiomyoma & Lipoma (can occur anywhere in the body) Malignant:
ميحرلا نمحرلا هللا مسب Gastric Tumors: Benign tumours & tumor-like conditions: -Mucosal: Gastric polyps (they are uncommon) -Mesenchymal tumours: Leiomyoma & Lipoma (can occur anywhere in the body) Malignant:
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
International Society of Gynecological Pathologists Symposium 2007
 International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neuroendocrine tumors of GI and Pancreatobiliary tracts. N. Volkan Adsay, MD
 Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 6, Issue 4 2016 Article 3 Laparoscopic Right Colectomy For Appendiceal Mucinous Cystadenoma: A Case Report Dion A. Putra Adianto Nugroho Ibrahim Basir University
World Journal of Colorectal Surgery Volume 6, Issue 4 2016 Article 3 Laparoscopic Right Colectomy For Appendiceal Mucinous Cystadenoma: A Case Report Dion A. Putra Adianto Nugroho Ibrahim Basir University
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Hereditary Gastric Cancer
 Hereditary Gastric Cancer Dr Bastiaan de Boer Consultant Pathologist Department of Anatomical Pathology PathWest Laboratory Medicine, QE II Medical Centre Clinical Associate Professor School of Pathology
Hereditary Gastric Cancer Dr Bastiaan de Boer Consultant Pathologist Department of Anatomical Pathology PathWest Laboratory Medicine, QE II Medical Centre Clinical Associate Professor School of Pathology
Protocol for the Examination of Specimens From Patients With Carcinoma of the Appendix
 Protocol for the Examination of Specimens From Patients With Carcinoma of the Appendix Protocol applies to all carcinomas arising in the vermiform appendix, including goblet cell carcinoid tumors. Other
Protocol for the Examination of Specimens From Patients With Carcinoma of the Appendix Protocol applies to all carcinomas arising in the vermiform appendix, including goblet cell carcinoid tumors. Other
3/30/2017. Disclosure of Relevant Financial Relationships. Case 5: Polypoid mass in ulcerative colitis. Case 5. TC Smyrk
 Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
Dysplastic intestinal-type metaplasia of appendiceal endometriosis: a mimic of low grade appendiceal mucinous neoplasm
 Mitchell et al. Diagnostic Pathology 2014, 9:39 CASE REPORT Open Access Dysplastic intestinal-type metaplasia of appendiceal endometriosis: a mimic of low grade appendiceal mucinous neoplasm Andrew Mitchell
Mitchell et al. Diagnostic Pathology 2014, 9:39 CASE REPORT Open Access Dysplastic intestinal-type metaplasia of appendiceal endometriosis: a mimic of low grade appendiceal mucinous neoplasm Andrew Mitchell
Basic Data. Birthday: Gender:Female Admission date:
 Basic Data Birthday:1951-07-02 Gender:Female Admission date:2004-06-28 Chief Complaint A protruding mass over RLQ abdomen for many years. Present Illness & Past History Pseudomyxoma peritonei s/p laparotomy
Basic Data Birthday:1951-07-02 Gender:Female Admission date:2004-06-28 Chief Complaint A protruding mass over RLQ abdomen for many years. Present Illness & Past History Pseudomyxoma peritonei s/p laparotomy
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Biliary tract tumors
 Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Update on the serrated pathway to colorectal carcinoma
 Human Pathology (2010) xx, xxx xxx www.elsevier.com/locate/humpath Progress in pathology Update on the serrated pathway to colorectal carcinoma Dale C. Snover MD Department of Pathology, Fairview Southdale
Human Pathology (2010) xx, xxx xxx www.elsevier.com/locate/humpath Progress in pathology Update on the serrated pathway to colorectal carcinoma Dale C. Snover MD Department of Pathology, Fairview Southdale
Large Colorectal Adenomas An Approach to Pathologic Evaluation
 Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
1. Esophageal diverticulum located above the upper esophageal sphincter is called
 Test Bank for Robbins Basic Pathology 9th Edition by Kumar Link full download: http://testbankair.com/download/test-bank-for-robbins-basic-pathology-9thedition-by-kumar/ Chapter 14: Oral Cavity and Gastrointestinal
Test Bank for Robbins Basic Pathology 9th Edition by Kumar Link full download: http://testbankair.com/download/test-bank-for-robbins-basic-pathology-9thedition-by-kumar/ Chapter 14: Oral Cavity and Gastrointestinal
Mucinous Tumors of the Ovary Beirut, Lebanon. Anaís Malpica, M.D. Professor Department of Pathology
 Mucinous Tumors of the Ovary Beirut, Lebanon Anaís Malpica, M.D. Professor Department of Pathology Primary Mucinous Tumors of the Ovary Cystadenoma Borderline (Tumor of Low Malignant Potential/Atypical
Mucinous Tumors of the Ovary Beirut, Lebanon Anaís Malpica, M.D. Professor Department of Pathology Primary Mucinous Tumors of the Ovary Cystadenoma Borderline (Tumor of Low Malignant Potential/Atypical
Serrated Colorectal Polyps New Challenges to Old Dogma. Kenneth Batts, M.D. Abbott Northwestern Hospital Minneapolis, MN
 Serrated Colorectal Polyps New Challenges to Old Dogma Kenneth Batts, M.D. Abbott Northwestern Hospital Minneapolis, MN A Sneak Preview.... This was in the good old days: Adenomas HPPs Mixed Polyps A Sneak
Serrated Colorectal Polyps New Challenges to Old Dogma Kenneth Batts, M.D. Abbott Northwestern Hospital Minneapolis, MN A Sneak Preview.... This was in the good old days: Adenomas HPPs Mixed Polyps A Sneak
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors
 Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Frédéric Bibeau, MD, PhD Pathology department Biopathology unit Institut du Cancer de Montpellier France Quality
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Frédéric Bibeau, MD, PhD Pathology department Biopathology unit Institut du Cancer de Montpellier France Quality
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci. Colon polyps. Colorectal cancer
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Section 1. Biology of gynaecological cancers: our current understanding
 Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
ONCOLOGY. Csaba Bödör. Department of Pathology and Experimental Cancer Research november 19., ÁOK, III.
 ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
5/21/2018. Prostate Adenocarcinoma vs. Urothelial Carcinoma. Common Differential Diagnoses in Urological Pathology. Jonathan I.
 Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Update of mixed tumours of the GI tract, the pancreas and the liver Introduction to the concept of mixed tumours and clinical implication Jean-Yves SCOAZEC Surgical
Enterprise Interest Nothing to declare Update of mixed tumours of the GI tract, the pancreas and the liver Introduction to the concept of mixed tumours and clinical implication Jean-Yves SCOAZEC Surgical
Mousa. Najat kayed &Renad Al-Awamleh. Nizar Alkhlaifat
 6 Mousa Najat kayed &Renad Al-Awamleh Nizar Alkhlaifat P a g e 1 This sheet written based on record 13 on website Cover slide( 95-117 ) No need to go back to slide FALLOPIAN TUBE PATHOLOGY In general fallopian
6 Mousa Najat kayed &Renad Al-Awamleh Nizar Alkhlaifat P a g e 1 This sheet written based on record 13 on website Cover slide( 95-117 ) No need to go back to slide FALLOPIAN TUBE PATHOLOGY In general fallopian
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
Neoplasia literally means "new growth.
 NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1)
") Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Specialised Services Policy: CP02 Hyperthermic Intraperitoneal Chemotherapy (HIPEC) and Cytoreductive Surgery for treatment of Pseudomyxoma Peritonei
 and Cytoreductive Surgery for treatment of Pseudomyxoma Peritonei") Specialised Services Policy: CP02 Hyperthermic Intraperitoneal Chemotherapy (HIPEC) of Pseudomyxoma Peritonei Document Author: Assistant Medical Director Executive Lead: Medical Director Approved by: Management
Specialised Services Policy: CP02 Hyperthermic Intraperitoneal Chemotherapy (HIPEC) of Pseudomyxoma Peritonei Document Author: Assistant Medical Director Executive Lead: Medical Director Approved by: Management
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Protocol for the Examination of Specimens from Patients with Carcinoma of the Appendix
 Protocol for the Examination of Specimens from Patients with Carcinoma of the Appendix Protocol applies to all carcinomas arising in the vermiform appendix, including goblet cell carcinoid tumors. Other
Protocol for the Examination of Specimens from Patients with Carcinoma of the Appendix Protocol applies to all carcinomas arising in the vermiform appendix, including goblet cell carcinoid tumors. Other
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
What Pathology can tell us in the approach of localized colorectal cancer
 What Pathology can tell us in the approach of localized colorectal cancer A/Prof Tony Lim Kiat Hon Department of Anatomical Pathology Singapore General Hospital ESMO 2017 Singapore Nov 1 2 Do we still
What Pathology can tell us in the approach of localized colorectal cancer A/Prof Tony Lim Kiat Hon Department of Anatomical Pathology Singapore General Hospital ESMO 2017 Singapore Nov 1 2 Do we still
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
General Surgery Grand Grounds
 General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
Gastrointestinal pathology 2018 lecture 4. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Overview. Collecting Cancer Data: Colon 11/5/2009. Collecting Cancer Data: NAACCR Webinar Series 1. Agenda NAACCR WEBINAR SERIES
 Collecting Cancer Data: Colon 11/5/2009 Collecting Cancer Data: Colon/Rectum/Appendix NAACCR 2009 2010 WEBINAR SERIES Agenda Overview Treatment MP/H Rules CSv2 2 Overview Colon/Rectum/Appendix 2009 2010
Collecting Cancer Data: Colon 11/5/2009 Collecting Cancer Data: Colon/Rectum/Appendix NAACCR 2009 2010 WEBINAR SERIES Agenda Overview Treatment MP/H Rules CSv2 2 Overview Colon/Rectum/Appendix 2009 2010
6/5/2010. Outline of Talk. Endometrial Alterations That Mimic Cancer & Vice Versa: Metaplastic / reactive changes. Problems in Biopsies/Curettages
 Outline of Talk Endometrial Alterations That Mimic Cancer & Vice Versa: Problems in Biopsies/Curettages Metaplastic / reactive changes Mucinous change Microglandular hyperplasia-like change Squamous metaplasia
Outline of Talk Endometrial Alterations That Mimic Cancer & Vice Versa: Problems in Biopsies/Curettages Metaplastic / reactive changes Mucinous change Microglandular hyperplasia-like change Squamous metaplasia
Disseminated Peritoneal Adenomucinosis Associated with a Panperitonitis-Like Onset: Report of a Case
 Surg Today (2001) 31:646 650 Disseminated Peritoneal Adenomucinosis Associated with a Panperitonitis-Like Onset: Report of a Case Yoshito Kuroki 1, Shunyou Otagiri 1, and Kazuhiro Tsukada 2 1 Department
Surg Today (2001) 31:646 650 Disseminated Peritoneal Adenomucinosis Associated with a Panperitonitis-Like Onset: Report of a Case Yoshito Kuroki 1, Shunyou Otagiri 1, and Kazuhiro Tsukada 2 1 Department
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER. Guidelines for the assessment of mismatch. Colorectal Cancer
 COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer January 2015 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer January 2015 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER. Guidelines for the assessment of mismatch. Colorectal Cancer
 COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer March 2017 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer March 2017 1 Background Mismatch repair (MMR) deficiency is seen in approximately
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING
 2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Eight Groups are Revised for 2018 Head & Neck Colon (includes rectosigmoid and rectum for cases diagnosed 1/1/2018 forward) Lung (2018 Draft not yet
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Eight Groups are Revised for 2018 Head & Neck Colon (includes rectosigmoid and rectum for cases diagnosed 1/1/2018 forward) Lung (2018 Draft not yet
A215- Urinary bladder cancer tissues
 A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
Disclaimer: I belong to the speakers bureau of the American Serrated Society, often referred to as the ASS
 An Exposé on Serrated Lesions of the Colorectum How do you know it is a hyperplastic polyp and not something else? How do you know it is something else and not a hyperplastic polyp? Disclaimer: I belong
An Exposé on Serrated Lesions of the Colorectum How do you know it is a hyperplastic polyp and not something else? How do you know it is something else and not a hyperplastic polyp? Disclaimer: I belong
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
The surface mucous cells and the cardiac and pyloric glands secrete mucus which protects the stomach from self-digestion.
 PATHOLOGY OF THE STOMACH Stomach mucosa Gastric mucosa is covered by a layer of mucus. The mucosal glands comprise the cardiac glands, the fundic glands in the fundus and body of the stomach, and the pyloric
PATHOLOGY OF THE STOMACH Stomach mucosa Gastric mucosa is covered by a layer of mucus. The mucosal glands comprise the cardiac glands, the fundic glands in the fundus and body of the stomach, and the pyloric
Neoplasia part I. Dr. Mohsen Dashti. Clinical Medicine & Pathology nd Lecture
 Neoplasia part I By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 2 nd Lecture Lecture outline Review of structure & function. Basic definitions. Classification of neoplasms. Morphologic features.
Neoplasia part I By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 2 nd Lecture Lecture outline Review of structure & function. Basic definitions. Classification of neoplasms. Morphologic features.
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Pathology Today American Society for Clinical Pathology Annual Meeting Workshop No: 1340 Gastrointestinal Pathology: New Approaches to Old Problems
 Pathology Today American Society for Clinical Pathology Annual Meeting Workshop No: 1340 Gastrointestinal Pathology: New Approaches to Old Problems ASCP Annual Meeting/WASPaLM XXVI World Congress Las Vegas,
Pathology Today American Society for Clinical Pathology Annual Meeting Workshop No: 1340 Gastrointestinal Pathology: New Approaches to Old Problems ASCP Annual Meeting/WASPaLM XXVI World Congress Las Vegas,
4/12/2018. MUSC Pathology Symposium Kiawah Island April 18, Jesse K. McKenney, MD
 MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
Stage 4 gastric adenocarcinoma icd 10
 > Stage 4 gastric adenocarcinoma icd 10 stage iii; Carcinoma of colon, stage iv; Colon cancer metastatic to unspecified site; Hereditary nonpolyposis colon cancer; Malignant tumor of colon; Metastasis.
> Stage 4 gastric adenocarcinoma icd 10 stage iii; Carcinoma of colon, stage iv; Colon cancer metastatic to unspecified site; Hereditary nonpolyposis colon cancer; Malignant tumor of colon; Metastasis.