MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018
|
|
|
- Jocelin Snow
- 5 years ago
- Views:
Transcription

1 MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus
2 DISCLOSURES Supported by the U of Colorado DOM Outstanding Early Scholars Program Paul R O Hara II Endowed Chair in Esophageal Cancer Madeleine Kane NIH-NIDDK U01DK (SVI) Supported by the ASGE Endoscopy Research Award (2015, 2017), ACG Clinical Research Award Educational Grants Cook, Medtronic, Boston Scientific Consultant Medtronic, Boston Scientific


3 BARRETT S ESOPHAGUS


4 ESOPHAGEAL ADENOCARCINOMA
5 RISING INCIDENCE OF ESOPHAGEAL ADENOCARCINOMA Rate per 1,000, Adenocarcinoma Squamous Cell Carcinoma Not otherwise specified Pohl H et al, J Natl Cancer Inst 2005, Brown LM et al, J Natl Cancer Inst 2008
6 OBJECTIVES Role of confirmation of diagnosis by expert GI pathologists Review the goals of advanced imaging techniques? Role of EMR in BE patients What is the optimal management strategy for BE with dysplasia (LGD and HGD) and mucosal cancer Candidates for endoscopic eradication therapy Management of the post-ablation patient Quality indicators and updated guidelines

7
8
9 ASGE GUIDELINES FOR ENDOSCOPIC ERADICATION THERAPY In Barrett s esophagus patients with LGD AND HGD being considered for EET, we suggest confirmation of diagnosis by at least one expert GI pathologist or panel of pathologists compared to review by a single pathologist Strength of recommendation: Conditional Quality of evidence: Low Wani S et al. Gastrointest Endosc 2018 (in press)
10 INTEROBSERVER VARIABILITY AMONG PATHOLOGISTS Diagnosis Biopsy Kappa (95% CI) Strength of agreement NDBE 0.57 ( ) Moderate LGD/IND 0.22 ( ) Fair HGD 0.35 ( ) Fair EAC 0.71 ( ) Substantial EMR Kappa (95% CI) Strength of agreement 0.51 ( ) Moderate 0.33 ( ) Fair 0.43 ( ) Moderate 0.68 ( ) Substantial Wani S et al, CGH 2010
11 INTEROBSERVER VARIABILITY AMONG PATHOLOGISTS Diagnosis Biopsy Kappa (95% CI) Strength of agreement NDBE 0.57 ( ) Moderate LGD/IND 0.22 ( ) Fair HGD 0.35 ( ) Fair EAC 0.71 ( ) Substantial EMR Kappa (95% CI) Strength of agreement 0.51 ( ) Moderate 0.33 ( ) Fair 0.43 ( ) Moderate 0.68 ( ) Substantial Wani S et al, CGH 2010
12 CHANGE IN DIAGNOSIS BASED ON EXPERT PATHOLOGY REVIEW Expert pathology review results in a change in Study name Time point Statistics for each study Event rate and 95% CI Event Lower Upper rate limit limit p-value diagnosis (upstaging or downstaging) in 55% Cameron of patients Curvers Duits Majority Kerkhof of patients 0.15 are 0.13 downgraded to lower Mahindra Pech pathologic diagnosis Sangle Stolte Wani S et al. Gastrointest Endosc 2018 (in press)
13 IMPACT OF EXPERT PATHOLOGY REVIEW ON RISK OF PROGRESSION Duits et al patients with LGD - Number of pathologists associated with risk of progression to neoplasia (dose-response effect) - 3 pathologists agreed (OR 47.14) Qumseya et al - Increased cumulative risk and incidence of progression based on expert pathology review - Confirmed LGD based on expert pathology review associated with a higher rate of disease progression Duits et al. Gastroenterology 2017; Qumseya B et al. Am J Gastroenterol 2017
14 APPROPRIATE QUALITY INDICATORS PRE-PROCEDURE For patients in whom a diagnosis of dysplasia has been made, the rate at which the reading is made by a GI pathologist or confirmed by a 2 nd pathologist prior to EET Type of measure: Process Performance target: 90% Wani S et al. Am J Gastroenterol and Gastrointest Endosc 2017


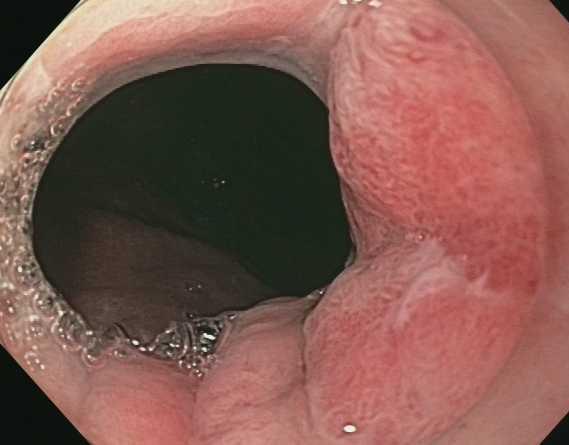
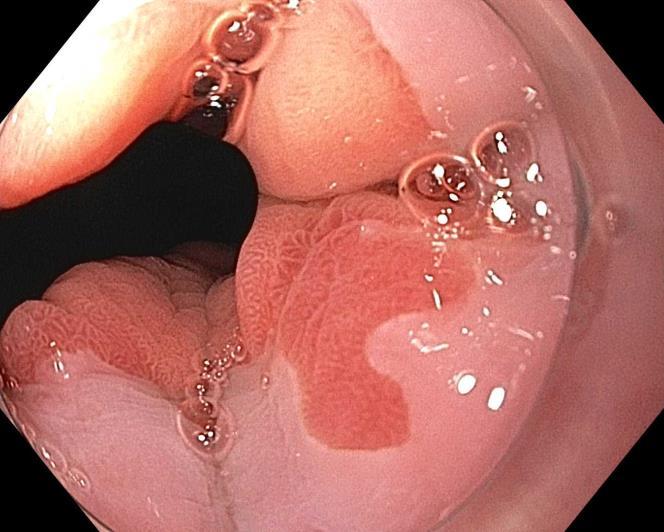
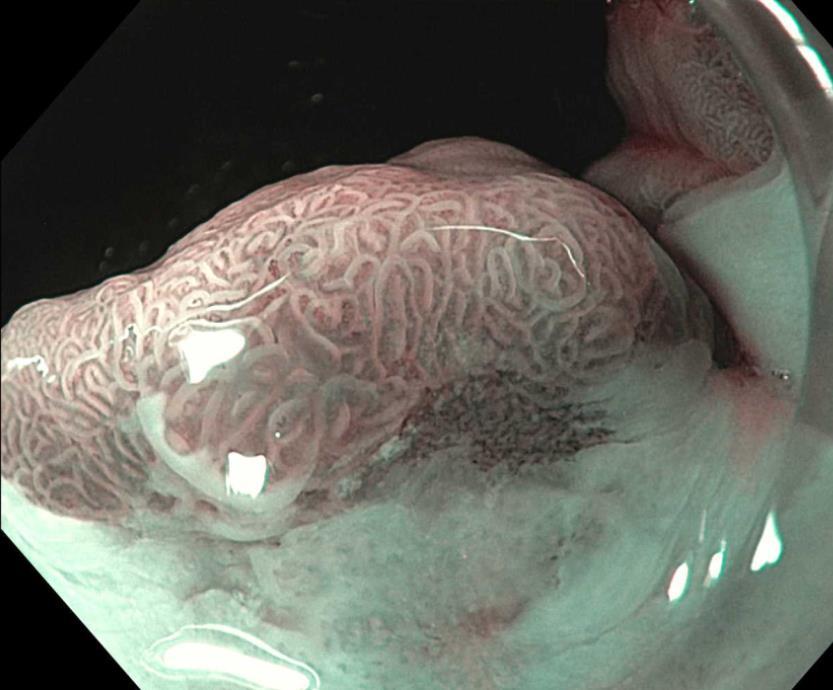
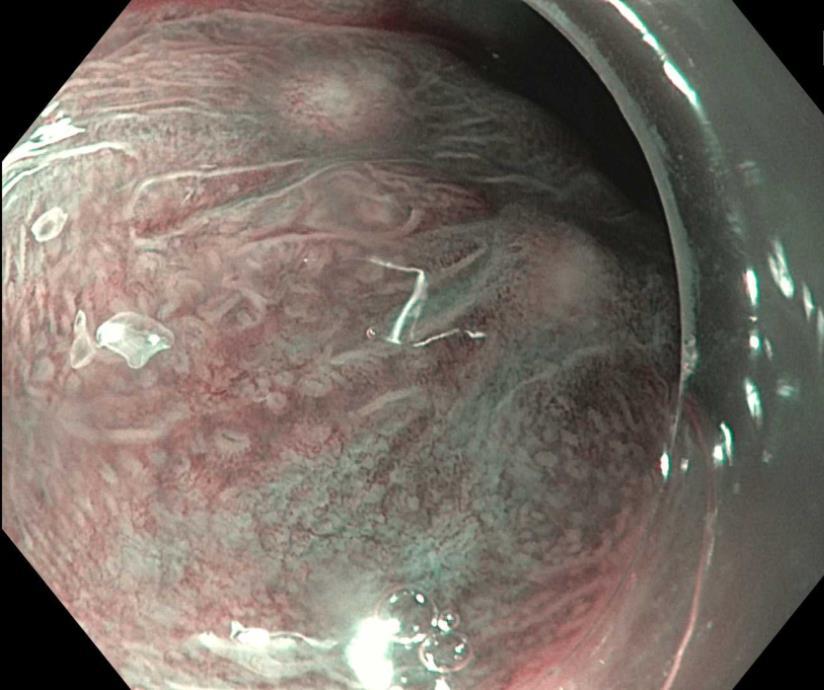
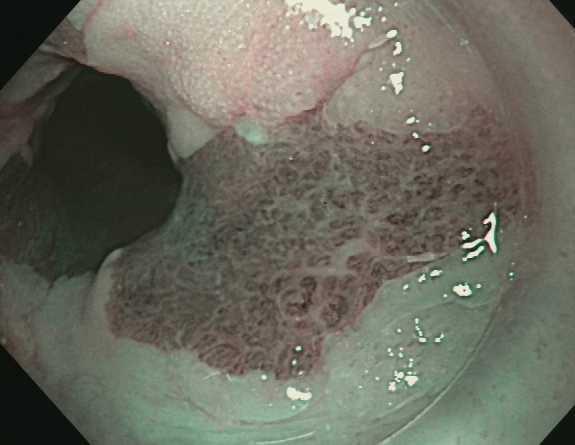
15 HIGH RESOLUTION ENDOSCOPY STANDARD OF CARE

16

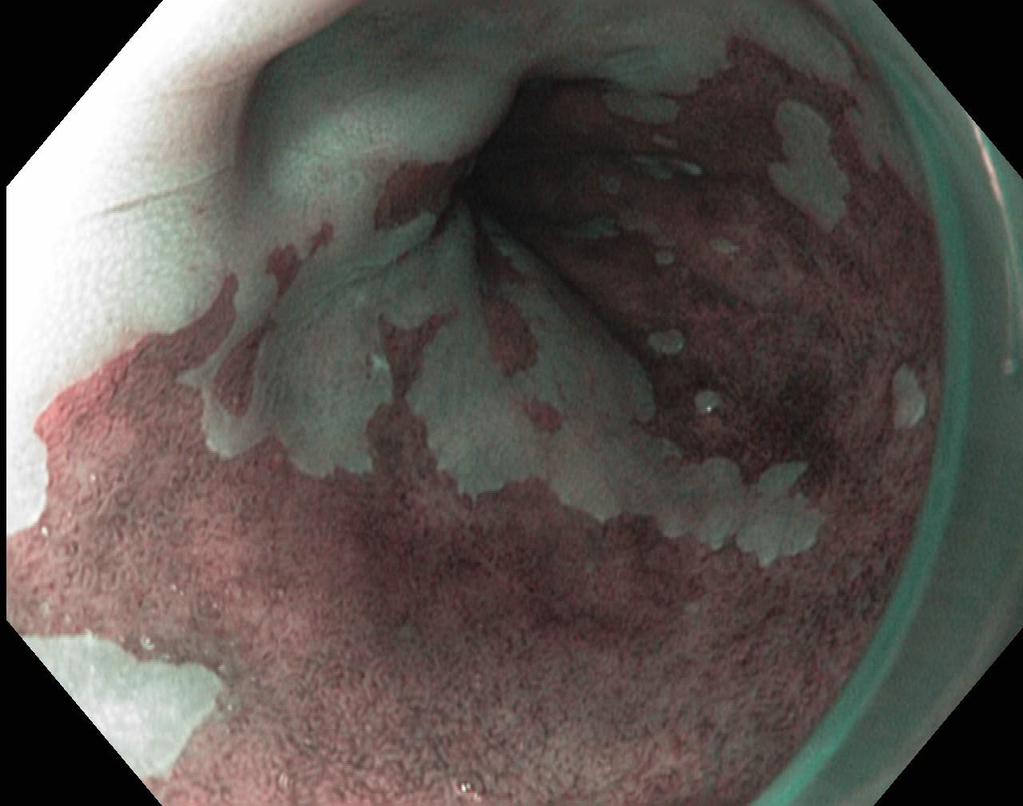
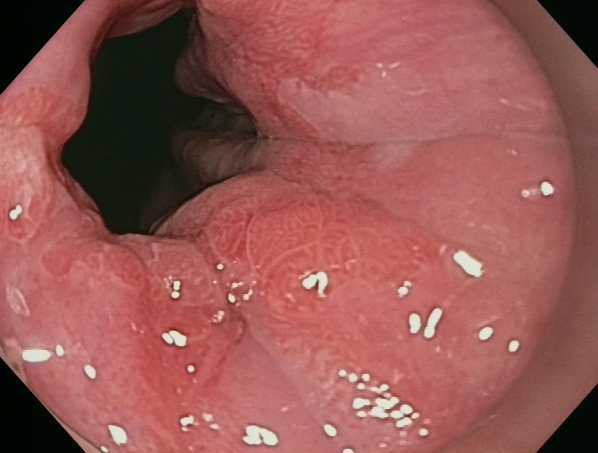
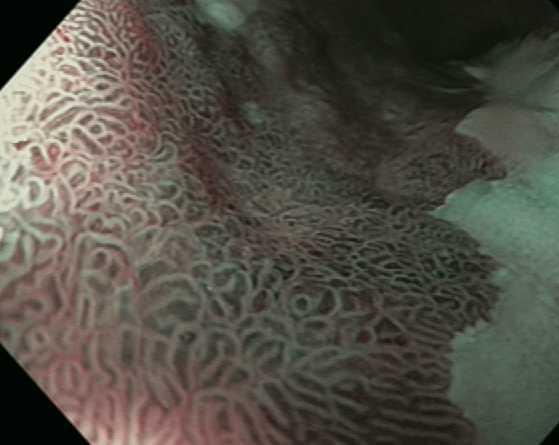
17 NARROW BAND IMAGING

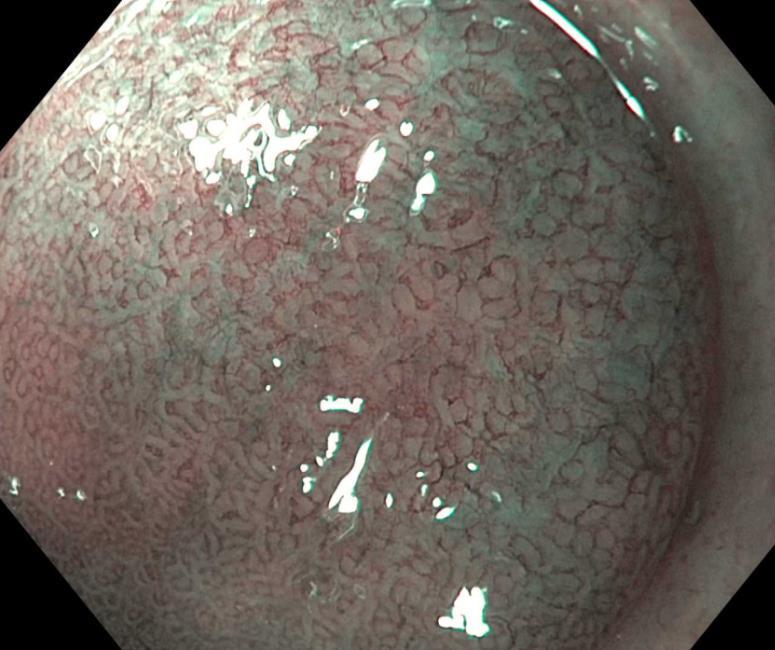
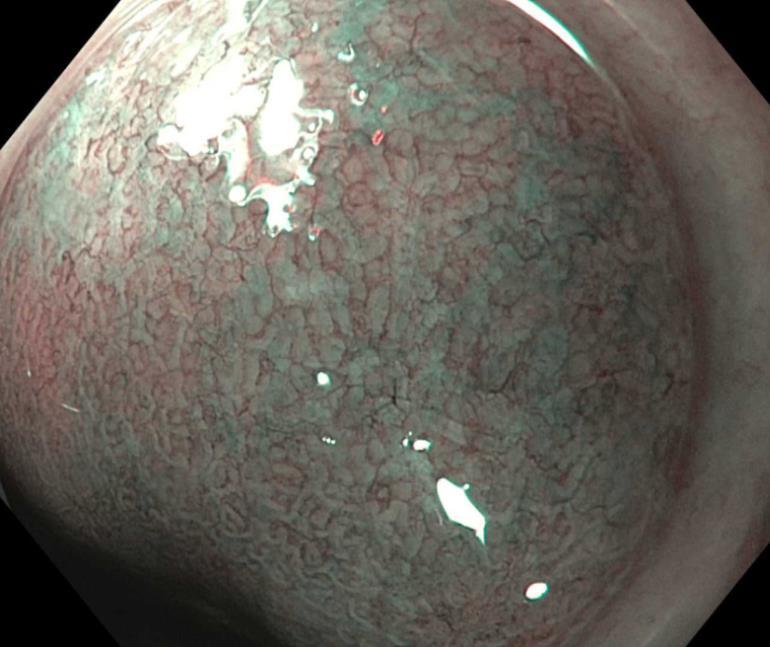
18
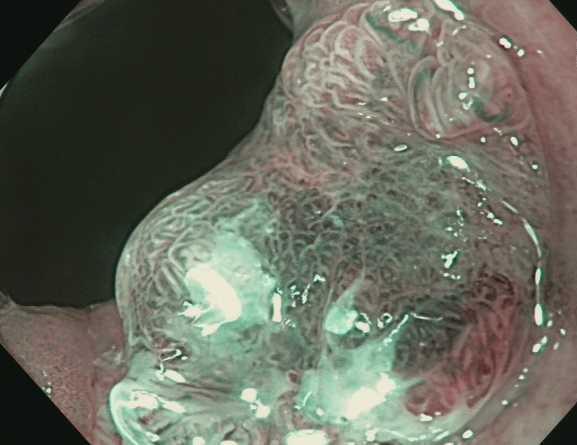
19 STANDARDIZED CONSENSUS DRIVEN CLASSIFICATION SYSTEM

20 ADVANCED IMAGING TO GUIDE EET Highest interest level Least amount of data NBI most widely used technique VLE based laser marking
21 APPROPRIATE QUALITY INDICATORS INTRA-PROCEDURE The rate at which landmarks and length of BE is documented using the Prague criteria and presence or absence of visible lesions is documented Type of measure: Process Performance target: 90% Wani S et al. Am J Gastroenterol and Gastrointest Endosc 2017
22 APPROPRIATE QUALITY INDICATORS INTRA-PROCEDURE The rate at which the BE segment is inspected using HD-WLE Type of measure: Process Performance target: 95% Wani S et al. Am J Gastroenterol and Gastrointest Endosc 2017

23 BASIS OF ENDOSCOPIC THERAPY Komanduri S, Muthusamy V, Wani S, Gastroenterology (in press)
24 ASGE GUIDELINES FOR ENDOSCOPIC ERADICATION THERAPY In Barrett s esophagus patients with confirmed HGD/IMC, we recommend against surgery compared with EET Strength of recommendation: Strong Quality of evidence: Very low Wani S et al. Gastrointest Endosc (in press)
25 ESOPHAGECTOMY vs. EET Study name Statistics for each study Risk ratio and 95% CI Risk Lower Upper ratio limit limit p-value Pech Prasad Prasad Wani Schmidt Meta Analysis No difference in 5-yr survival (RR 0.88, 95% CI ) EET group had significantly lower adverse events (RR 0.38, 95% CI ) Wani S et al. Gastrointest Endosc (in press)
26 ASGE GUIDELINES FOR ENDOSCOPIC ERADICATION THERAPY In Barrett s esophagus patients referred for EET, we recommend endoscopic resection of all visible lesions compared to no endoscopic resection of visible lesions Strength of recommendation: Strong Quality of evidence: Moderate Wani S et al. Gastrointest Endosc (in press)

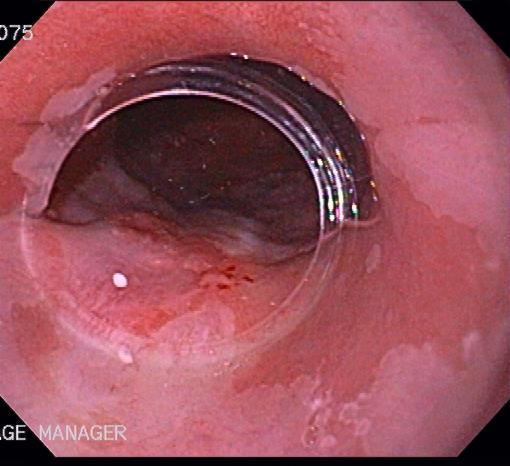
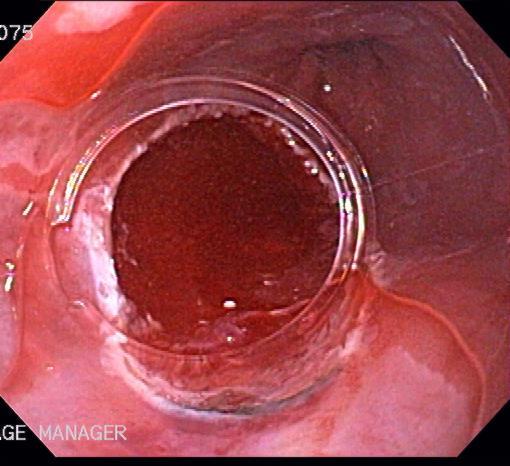

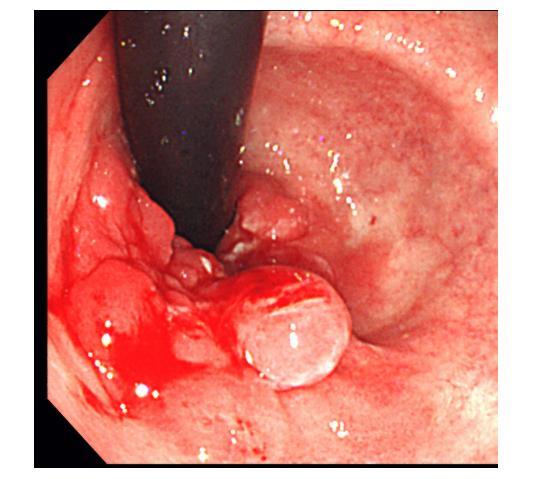
27 STAGING EMR
28 IMPACT OF EMR ON DIAGNOSIS Statistics for each study Event Lower Upper rate limit limit p-value Koutsampas Seewald Telakis Wani Westra Thota Ayers Elsadek Werbouck Conio Nijhawan Chennat Moss Konda Event rate and 95% CI EMR resulted in change in pathologic diagnosis in 39% (95% CI 34-45) of all patients Majority of patients were upgraded to a higher pathologic diagnosis

29

30
 Cancer Risk IM 0.598%/yr 0.516-0.7 Low LGD 1.70%/yr 1.")

31 Grade Grade of dysplasia & Cancer Risk Cancer Incidence (95% CI) Cancer Risk IM 0.598%/yr Low LGD 1.70%/yr Intermediate HGD 6.58%/yr High Rastogi et al. Gastrointest Endosc 2008 Wani S et al. Am J Gastroenterol 2009
32 PRINCIPLES OF ENDOSCOPIC ERADICATION THERAPIES Resection of neoplastic lesion lesion with highest dysplasia grade Eradication of remaining Barrett s esophagus (reduce the risk of metachronous neoplasia) Management of complications Enrollment in surveillance programs and address recurrences
33 Endoscopic Eradication Therapies: The Options Thermal techniques: - APC - MPEC - Lasers (Nd:YAG, KTP:YAG) - RFA Photochemical: - PDT Mechanical: - EMR Others: - Cryoablation - Ultrasonic ablation Multimodality therapies Wani S et al. Gastrointest Endosc 2010
34 AIM DYSPLASIA TRIAL 128 patients with BE and dysplasia (LGD/HGD) Mean BE length 5 cm; 12 month follow up %* 81%* 77%* Patients % % 19% SHAM RFA 10 0 p<0.001 LGD Eradication (n=64) HGD Eradication (n=63) 2% IM Eradication (n=127) Shaheen N et al. NEJM 2009
35 ASGE GUIDELINES FOR ENDOSCOPIC ERADICATION THERAPY In Barrett s esophagus patients with confirmed HGD, we recommend EET compared to surveillance Strength of recommendation: Strong Quality of evidence: Moderate Wani S et al. Gastrointest Endosc (in press)
36 Natural History of LGD Diagnosis Incident cases Incidence rate %/year (95% CI) HGD ( ) EAC ( ) HGD/EAC ( ) Mean time to development (years, SD) range 2.86 (4.22) 4.41 (1.49) 3.08 (2.57) Wani S et al, Gastroenterology 2011
37
38 SURVEILLANCE vs. ABLATION IN LGD Ablation reduced risk of progression to HGD/EAC by 25% - 1.5% ablation vs. 26.5% controls (95% CI %, p<0.001) Ablation reduced risk of progression to EAC by 7.4% - 1.5% ablation vs. 8.8% controls (95% CI %, p=0.03) Phoa et al, JAMA 2014
39 ASGE GUIDELINES FOR ENDOSCOPIC ERADICATION THERAPY In Barrett s esophagus patients with LGD, we suggest EET compared to surveillance; however, patients who place a high value on avoiding adverse events related to EET may choose surveillance as the preferred option Strength of recommendation: Conditional Quality of evidence: Moderate Wani S et al. Gastrointest Endosc (in press)
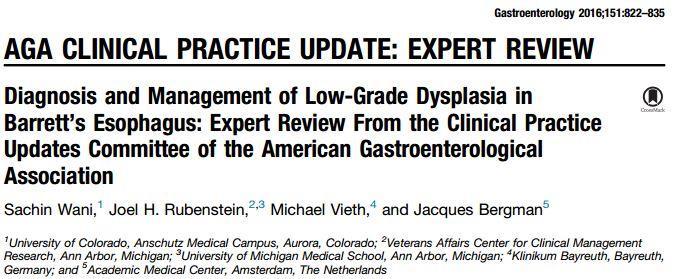
40 EFFECTIVENESS DATA
41 APPROPRIATE QUALITY INDICATORS INTRA-PROCEDURE The rate at which complete eradication of neoplasia is achieved by 18 months in patients with BE-related dysplasia or intramucosal cancer referred for EET Type of measure: Outcome Performance target: 80% Wani S et al. Am J Gastroenterol and Gastrointest Endosc 2017
42 APPROPRIATE QUALITY INDICATORS INTRA-PROCEDURE The rate at which complete eradication of intestinal metaplasia is achieved by 18 months in patients with BE-related dysplasia or intramucosal cancer referred for EET Type of measure: Outcome Performance target: 70% Wani S et al. Am J Gastroenterol and Gastrointest Endosc 2017
43 Adverse Events Meta-analysis 37 studies Pooled rate (RFA +/- EMR): 8.8% (95% CI ) Strictures: 5.6% (95% CI ) Bleeding: 1% (95% CI %) Perforation: 0.6% (95% CI ) Adverse events higher with EMR (RR 4.4) BE length and baseline histology predictors of adverse events Qumseya B, Wani S CGH 2016
44 APPROPRIATE QUALITY INDICATORS POST-PROCEDURE The rate at which adverse events are being tracked and documented in individuals post EET Type of measure: Process Performance target: 95% Wani S et al. Am J Gastroenterol and Gastrointest Endosc 2017
45 RECURRENCE OF INTESTINAL METAPLASIA AND NEOPLASIA Meta analysis 33 studies Pooled incidence any recurrence: 6.5 (95% CI )/100 patientyears Incidence of IM: 4.2 (95% CI )/100 patient-years Incidence of early neoplasia: 1.4 (95% CI )/100 patient-years Fuji et al, Endosc Int Open 2017
46 APPROPRIATE QUALITY INDICATORS POST-PROCEDURE During endoscopic surveillance after EET, the rate at which biopsies of any visible mucosal abnormalities are performed Type of measure: Process Performance target: 95% Wani S et al. Am J Gastroenterol and Gastrointest Endosc 2017
47 Approach to BE related neoplasia Patient with Barrett s esophagus related neoplasia Consider referral to tertiary care center Confirm diagnosis by expert GI pathologist Evaluation and discussion in clinic Accurate diagnosis and staging Repeat EGD using HD-WLE, advanced imaging and EUS Define extent by Prague C&M criteria and visible lesions by Paris classification Endoscopic resection of all visible lesions Highest histologic grade based on above evaluation Submuscosal Cancer High grade dysplasia or intramuscosal cancer Low grade dysplasia Surgical referral for esophagectomy (EET only in T1b cancer with favorable features and poor-surgical candidate) EET (resection or ablation) EET in confirmed LGD (expert GI pathologist, at least 2 EGDs with LGD) OR surveillance q6-12 months Enroll in surveillance program post complete eradication of intestinal metaplasia and neoplasia Wani et al, Gastro Clinics N Am 2015

48 Esophageal & Gastric Multidisciplinary Clinic Established August 2013


49 THANK YOU

50
Barrett s esophagus. Barrett s neoplasia treatment trends
 Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Management of Barrett s Esophagus. Case Presentation
 Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Endoscopic Management of Barrett s Esophagus
 Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Learning Objectives:
 Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD?
 Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Barrett s Esophagus: Ablate Everyone?
 Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Management of Barrett s: From Imaging to Resection
 Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Ablation for Barrett s Esophagus: Burn or Freeze
 Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus Policy Number: 2.01.80 Last Review: 6/2018 Origination: 6/2012 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus Policy Number: 2.01.80 Last Review: 6/2018 Origination: 6/2012 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Policy Number: Original Effective Date: MM.02.005 09/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Policy Number: Original Effective Date: MM.02.005 09/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Medicare Advantage Medical Policy
 Medicare Advantage Medical Policy Current Policy Effective Date: 1/1/18 Title: Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Description/Background Barrett Esophagus and the
Medicare Advantage Medical Policy Current Policy Effective Date: 1/1/18 Title: Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Description/Background Barrett Esophagus and the
Everything Esophagus: Barrett s Esophagus. Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina
 Everything Esophagus: Barrett s Esophagus Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina The Most Important Thing Stayed the Same Adenocarcinoma A
Everything Esophagus: Barrett s Esophagus Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina The Most Important Thing Stayed the Same Adenocarcinoma A
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus
 New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
Changes to the diagnosis and management of Barrett s Oesophagus
 Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
Barrett's Esophagus: Sorting Out the Controversy
 Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
Present Day Management of Barrett s Esophagus
 Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Gregory G. Ginsberg, M.D.
 Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Definition of GERD American College of Gastroenterology
 Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
How to remove BE cancer: EMR or ESD? Expected outcome
 How to remove BE cancer: EMR or ESD? Expected outcome Presented by Horst Neuhaus Institution Dpt. of Gastroenterology Evangelisches Krankenhaus Düsseldorf, Germany Indications for endoscopic resection
How to remove BE cancer: EMR or ESD? Expected outcome Presented by Horst Neuhaus Institution Dpt. of Gastroenterology Evangelisches Krankenhaus Düsseldorf, Germany Indications for endoscopic resection
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Follow this and additional works at:
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 217 Recurrence of intestinal metaplasia and early neoplasia after endoscopic eradication therapy for Barrett s esophagus:
Washington University School of Medicine Digital Commons@Becker Open Access Publications 217 Recurrence of intestinal metaplasia and early neoplasia after endoscopic eradication therapy for Barrett s esophagus:
RFA and Cyrotherapy for Esophageal Disease
 RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus. Original Policy Date
 MP 2.01.52 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Reviewed with literature
MP 2.01.52 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Reviewed with literature
Current Management of Low-Grade Dysplasia in Barrett Esophagus
 Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment Barrett s esophagus
 E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
Section: Medicine Effective Date: July 15, 2015 Subsection: Original Policy Date: December 7, 2011 Subject:
 Last Review Status/Date: June 2015 Page: 1 of 16 Cryoablation for Barrett s Esophagus Description Barrett s esophagus (BE) is a condition in which the normal squamous epithelium is replaced by specialized
Last Review Status/Date: June 2015 Page: 1 of 16 Cryoablation for Barrett s Esophagus Description Barrett s esophagus (BE) is a condition in which the normal squamous epithelium is replaced by specialized
Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series
 E17 Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series Authors Romy E. Verbeek 1, Frank P. Vleggaar 1, Fiebo J.
E17 Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series Authors Romy E. Verbeek 1, Frank P. Vleggaar 1, Fiebo J.
Populations Interventions Comparators Outcomes Individuals: With Barrett esophagus with high-grade dysplasia
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett (20180) Medical Benefit Effective Date: 01/01/16 Next Review Date: 09/19 Preauthorization No Review Dates: 05/09, 03/10, 03/11, 03/12, 07/12,
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett (20180) Medical Benefit Effective Date: 01/01/16 Next Review Date: 09/19 Preauthorization No Review Dates: 05/09, 03/10, 03/11, 03/12, 07/12,
Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia
: Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia") UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
Is Radiofrequency Ablation Effective In Treating Barrett s Esophagus Patients with High-Grade Dysplasia?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 12-2016 Is Radiofrequency Ablation Effective
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 12-2016 Is Radiofrequency Ablation Effective
Sixteen-year follow-up of Barrett s esophagus, endoscopically treated with argon plasma coagulation
 Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Recurrent intestinal metaplasia at the gastroesophageal junction following endoscopic eradication of dysplastic Barrett s esophagus may not be benign
 THIEME E849 Recurrent intestinal metaplasia at the gastroesophageal junction following endoscopic eradication of dysplastic Barrett s esophagus may not be benign Authors Georgina R. Cameron 1, 3, Paul
THIEME E849 Recurrent intestinal metaplasia at the gastroesophageal junction following endoscopic eradication of dysplastic Barrett s esophagus may not be benign Authors Georgina R. Cameron 1, 3, Paul
Review Article Outcomes of Radiofrequency Ablation for Dysplastic Barrett s Esophagus: A Comprehensive Review
 Gastroenterology Research and Practice Volume 2016, Article ID 4249510, 8 pages http://dx.doi.org/10.1155/2016/4249510 Review Article Outcomes of Radiofrequency Ablation for Dysplastic Barrett s Esophagus:
Gastroenterology Research and Practice Volume 2016, Article ID 4249510, 8 pages http://dx.doi.org/10.1155/2016/4249510 Review Article Outcomes of Radiofrequency Ablation for Dysplastic Barrett s Esophagus:
Opinion Statement. Esophagus (E Dellon, Section Editor)
") Curr Treat Options Gastro (2016) 14:1 18 DOI 10.1007/s11938-016-0080-4 Esophagus (E Dellon, Section Editor) Current Controversies in Radiofrequency Ablation Therapy for Barrett s Esophagus Kamar Belghazi,
Curr Treat Options Gastro (2016) 14:1 18 DOI 10.1007/s11938-016-0080-4 Esophagus (E Dellon, Section Editor) Current Controversies in Radiofrequency Ablation Therapy for Barrett s Esophagus Kamar Belghazi,
DISCLOSURES. This program meets the requirements for GI specific Category 1 contact hours. M
 DISCLOSURES Educational Dimensions is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center s Commission on Accreditation. Successful completion: Participants
DISCLOSURES Educational Dimensions is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center s Commission on Accreditation. Successful completion: Participants
Barrett esophagus. Bible class Inselspital
 Barrett esophagus Bible class Inselspital 2015.08.10 Guidelines Definition? BSG: ACG: Definition? BSG: ACG: What are the arguments for and against IM as prerequisite for the Dg? What are the arguments
Barrett esophagus Bible class Inselspital 2015.08.10 Guidelines Definition? BSG: ACG: Definition? BSG: ACG: What are the arguments for and against IM as prerequisite for the Dg? What are the arguments
Faculty Disclosure. Objectives. State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) 24/11/2014
 24/11/2014") State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
How to characterize dysplastic lesions in IBD?
 How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
History. Prevalence at Endoscopy. Prevalence and Reflux Sx. Prevalence at Endoscopy. Barrett s Esophagus: Controversy and Management
 Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
What s New in the Management of Esophageal Disease
 What s New in the Management of Esophageal Disease Philip O. Katz, MD Chairman, Division of Gastroenterology Einstein Medical Center Philadelphia Clinical Professor of Medicine Jefferson Medical College
What s New in the Management of Esophageal Disease Philip O. Katz, MD Chairman, Division of Gastroenterology Einstein Medical Center Philadelphia Clinical Professor of Medicine Jefferson Medical College
Slide 1. Slide 2. Slide 3 DISCLOSURES EXPECTED OUTCOMES DIAGNOSIS AND TREATMENT
 Slide 1 DIAGNOSIS AND TREATMENT 1 Slide 2 DISCLOSURES Successful completion: Participants must attend the entire program, including any resulting Q & A, and submit required documentation. Conflict of interest:
Slide 1 DIAGNOSIS AND TREATMENT 1 Slide 2 DISCLOSURES Successful completion: Participants must attend the entire program, including any resulting Q & A, and submit required documentation. Conflict of interest:
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery
 Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Ablation. See specific types, e.g., Thermal ablation Achalasia, 53 75 described, 53 features of, 53 management of past options, 54 POEM
Index Note: Page numbers of article titles are in boldface type. A Ablation. See specific types, e.g., Thermal ablation Achalasia, 53 75 described, 53 features of, 53 management of past options, 54 POEM
American Journal of Gastroenterology. Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma
 Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Barrett s Esophagus: State of the Art. Food Getting Stuck
 Barrett s Esophagus: State of the Art Nicholas J. Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina SOM Food Getting Stuck 73-year-old retired Wilmington police
Barrett s Esophagus: State of the Art Nicholas J. Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina SOM Food Getting Stuck 73-year-old retired Wilmington police
Barrett s Esophagus. Radiofrequency Ablation with the HALO Technology A Reference Book
 Radiofrequency Ablation with the HALO Technology A Reference Book 540 Oakmead Parkway, Sunnyvale, CA 94085 What is Barrett s esophagus? Barrett s esophagus is a change that occurs within the cellular lining
Radiofrequency Ablation with the HALO Technology A Reference Book 540 Oakmead Parkway, Sunnyvale, CA 94085 What is Barrett s esophagus? Barrett s esophagus is a change that occurs within the cellular lining
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions
 Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Dysplas'c Barre- s Esophagus: Cut, Burn, Freeze or Watch Very Very Closely
 Dysplas'c Barre- s Esophagus: Cut, Burn, Freeze or Watch Very Very Closely Felice Schnoll- Sussman, MD, FACG Director, Jay Monahan Center Associate Professor Clinical Medicine Weill Cornell Medical Center
Dysplas'c Barre- s Esophagus: Cut, Burn, Freeze or Watch Very Very Closely Felice Schnoll- Sussman, MD, FACG Director, Jay Monahan Center Associate Professor Clinical Medicine Weill Cornell Medical Center
Barrett s esophagus (BE) is a precancerous state
 is a precancerous state") CLINICAL ALIMENTARY TRACT Gastroenterology 2017;153:681 688 Late Recurrence of Barrett s Esophagus After Complete Eradication of Intestinal Metaplasia is Rare: Final Report From Ablation in Intestinal
CLINICAL ALIMENTARY TRACT Gastroenterology 2017;153:681 688 Late Recurrence of Barrett s Esophagus After Complete Eradication of Intestinal Metaplasia is Rare: Final Report From Ablation in Intestinal
Dysplasia 4/19/2017. How do I practice Chromoendoscopy for Surveillance of Colitis? SCENIC: Polypoid Dysplasia in UC. Background
 SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
Endoscopic diagnosis and therapies for Barrett esophagus. A review
 1130-0108/2014/106/2/103-119 Revista Española de Enfermedades Digestivas Copyright 2014 Arán Ediciones, S. L. Rev Esp Enferm Dig (Madrid Vol. 106, N.º 2, pp. 103-119, 2014 REVIEW Endoscopic diagnosis and
1130-0108/2014/106/2/103-119 Revista Española de Enfermedades Digestivas Copyright 2014 Arán Ediciones, S. L. Rev Esp Enferm Dig (Madrid Vol. 106, N.º 2, pp. 103-119, 2014 REVIEW Endoscopic diagnosis and
Barrett s esophagus: lessons from recent clinical trials
 INVITED REVIEW Annals of Gastroenterology (2016) 29, 1-7 Barrett s esophagus: lessons from recent clinical trials Daniela Golger, Andreas Probst, Helmut Messmann Klinikum Augsburg, Germany Abstract Data
INVITED REVIEW Annals of Gastroenterology (2016) 29, 1-7 Barrett s esophagus: lessons from recent clinical trials Daniela Golger, Andreas Probst, Helmut Messmann Klinikum Augsburg, Germany Abstract Data
Disclosures. Gastroesophageal Reflux Disease. Gastroesophageal Reflux Disease
 Kunal Jajoo, MD Brigham and Women s Hospital July 2012 Disclosures Spouse is a physician employed by Boston Scientific Corporation The content of this lecture equitably discusses products of multiple companies
Kunal Jajoo, MD Brigham and Women s Hospital July 2012 Disclosures Spouse is a physician employed by Boston Scientific Corporation The content of this lecture equitably discusses products of multiple companies
University Mainz. Early Gastric Cancer. Ralf Kiesslich. Johannes Gutenberg University Mainz, Germany. Early Gastric Cancer 15.6.
 Ralf Kiesslich Johannes Gutenberg University Mainz, Germany DIAGNOSIS Unmask lesions - Chromoendoscopy -NBI Red flag technology - Autofluorescence Surface and detail analysis - Magnifying endoscopy - High
Ralf Kiesslich Johannes Gutenberg University Mainz, Germany DIAGNOSIS Unmask lesions - Chromoendoscopy -NBI Red flag technology - Autofluorescence Surface and detail analysis - Magnifying endoscopy - High
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Research Article Diagnostic Accuracy of Mucosal Biopsy versus Endoscopic Mucosal Resection in Barrett s Esophagus and Related Superficial Lesions
 International Scholarly Research Notices Volume 2015, rticle ID 735807, 6 pages http://dx.doi.org/10.1155/2015/735807 Research rticle Diagnostic ccuracy of Mucosal iopsy versus Endoscopic Mucosal Resection
International Scholarly Research Notices Volume 2015, rticle ID 735807, 6 pages http://dx.doi.org/10.1155/2015/735807 Research rticle Diagnostic ccuracy of Mucosal iopsy versus Endoscopic Mucosal Resection
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Endoscopic therapy of Barrett s esophagus Oliver Pech and Christian Ell
 Endoscopic therapy of Barrett s esophagus Oliver Pech and Christian Ell Department of Internal Medicine 2, HSK Wiesbaden, Wiesbaden, Germany Correspondence to Oliver Pech, MD, PhD, Department of Gastroenterology,
Endoscopic therapy of Barrett s esophagus Oliver Pech and Christian Ell Department of Internal Medicine 2, HSK Wiesbaden, Wiesbaden, Germany Correspondence to Oliver Pech, MD, PhD, Department of Gastroenterology,
Barrett s Esophagus: State of the Art Management
 In the Name of God Barrett s Esophagus: State of the Art Management Siavosh Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Center, Shariati Hospital, TUMS IAGH
In the Name of God Barrett s Esophagus: State of the Art Management Siavosh Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Center, Shariati Hospital, TUMS IAGH
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
From reflux to esophageal cancer. Josh Boys, MD TCV 2 nd year indentured servant
 From reflux to esophageal cancer Josh Boys, MD TCV 2 nd year indentured servant The Pathway Esophageal Squamous epithelium+reflux Columnar lined esophagus (CLE) or Cardiac mucosa Intestinal Metaplasia
From reflux to esophageal cancer Josh Boys, MD TCV 2 nd year indentured servant The Pathway Esophageal Squamous epithelium+reflux Columnar lined esophagus (CLE) or Cardiac mucosa Intestinal Metaplasia
David Lewin MD Medical University of South Carolina
 Top 10 Advances in GI Pathology David Lewin MD Medical University of South Carolina No Disclosures Overview Top Articles/ presentations in the following areas Imaging (3) Molecular (2) Therapeutics (3)
Top 10 Advances in GI Pathology David Lewin MD Medical University of South Carolina No Disclosures Overview Top Articles/ presentations in the following areas Imaging (3) Molecular (2) Therapeutics (3)
Barrett s esophagus, reflux esophagitis, and eosinophilic esophagitis F. P. Vleggaar, P. D. Siersema Utrecht, the Netherlands
 DDW HIGHLIGHTS F. P. Vleggaar, P. D. Siersema Utrecht, the Netherlands Many new and exciting endoscopy-related studies on Barrett s esophagus, reflux esophagitis, and eosinophilic esophagitis were presented
DDW HIGHLIGHTS F. P. Vleggaar, P. D. Siersema Utrecht, the Netherlands Many new and exciting endoscopy-related studies on Barrett s esophagus, reflux esophagitis, and eosinophilic esophagitis were presented
Treatment of High-Grade Dysplasia and Early Stage Esophageal Adenocarcinoma with an Endoscope: The Ultimate in Minimally Invasive, Curative Therapy
 Curr Surg Rep (2014) 2:66 DOI 10.1007/s40137-014-0066-x ESOPHAGEAL/REFLUX SURGERY (SR DEMEESTER, SECTION EDITOR) Treatment of High-Grade Dysplasia and Early Stage Esophageal Adenocarcinoma with an Endoscope:
Curr Surg Rep (2014) 2:66 DOI 10.1007/s40137-014-0066-x ESOPHAGEAL/REFLUX SURGERY (SR DEMEESTER, SECTION EDITOR) Treatment of High-Grade Dysplasia and Early Stage Esophageal Adenocarcinoma with an Endoscope:
Current Management: Role of Radiofrequency Ablation
 Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Treat Barrett s, Remove the Risk. HALO System
 Treat Barrett s, Remove the Risk HALO System The HALO 360 System Advanced Ablation Technology for Barrett s Esophagus The HALO 360 System is designed to remove the Barrett s epithelium in a short, well-tolerated
Treat Barrett s, Remove the Risk HALO System The HALO 360 System Advanced Ablation Technology for Barrett s Esophagus The HALO 360 System is designed to remove the Barrett s epithelium in a short, well-tolerated
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Chapter 2 Complications of Gastroesophageal Reflux Disease
 Chapter 2 Complications of Gastroesophageal Reflux Disease Patrick Yachimski Acute esophageal exposure to gastric and/or duodenal refluxate can result in pyrosis and symptomatic gastroesophageal reflux
Chapter 2 Complications of Gastroesophageal Reflux Disease Patrick Yachimski Acute esophageal exposure to gastric and/or duodenal refluxate can result in pyrosis and symptomatic gastroesophageal reflux
Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading?
 Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading? Dr. Gaius Longcroft-Wheaton MB,BS, MD, MRCP(UK), MRCP(Gastro) Consultant gastroenterologist
Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading? Dr. Gaius Longcroft-Wheaton MB,BS, MD, MRCP(UK), MRCP(Gastro) Consultant gastroenterologist
What Is Barrett s Esophagus?
 What Is Barrett s Esophagus? Having Barrett s esophagus means the cells lining the esophagus (the tube that links the mouth and the stomach) have changed into types of intestinal cells that are not normal
What Is Barrett s Esophagus? Having Barrett s esophagus means the cells lining the esophagus (the tube that links the mouth and the stomach) have changed into types of intestinal cells that are not normal
Barrett s Esophagus. lining of the lower esophagus that bears his name (i.e., Barrett's esophagus). We now
. We now") Shamika Johnson Anatomy & Physiology 206 April 20, 2010 Barrett s Esophagus What is Barrett s Esophagus? Norman Barrett was a pathologist. In 1950, he described an abnormality in the lining of the lower
Shamika Johnson Anatomy & Physiology 206 April 20, 2010 Barrett s Esophagus What is Barrett s Esophagus? Norman Barrett was a pathologist. In 1950, he described an abnormality in the lining of the lower
The incidence of esophageal adenocarcinoma is rising in the ENDOSCOPY CORNER
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:843 847 ENDOSCOPY CORNER Acetic Acid Spray Is an Effective Tool for the Endoscopic Detection of Neoplasia in Patients With Barrett s Esophagus GAIUS LONGCROFT
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:843 847 ENDOSCOPY CORNER Acetic Acid Spray Is an Effective Tool for the Endoscopic Detection of Neoplasia in Patients With Barrett s Esophagus GAIUS LONGCROFT
Endoscopic management of Barrett s esophagus:european Society of Gastrointestinal Endoscopy (ESGE) Position Statement
 Position Statement") Endoscopic management of Barrett s esophagus:european Society of Gastrointestinal Endoscopy (ESGE) Position Statement Authors Bas Weusten 1, 2,RafBisschops 3,EmanuelCoron 4,MárioDinis- Ribeiro 5,Jean-MarcDumonceau
Endoscopic management of Barrett s esophagus:european Society of Gastrointestinal Endoscopy (ESGE) Position Statement Authors Bas Weusten 1, 2,RafBisschops 3,EmanuelCoron 4,MárioDinis- Ribeiro 5,Jean-MarcDumonceau
Achieving Clinically Proven Treatment Results With Photodynamic Therapy (PDT) and PHOTOFRIN (porfimer sodium) for Injection
 and PHOTOFRIN (porfimer sodium) for Injection") Achieving Clinically Proven Treatment Results With Photodynamic Therapy () and PHOTOFRIN (porfimer sodium) for Injection PHOTOFRIN (porfimer sodium) IS INDICATED FOR Palliation of patients with completely
Achieving Clinically Proven Treatment Results With Photodynamic Therapy () and PHOTOFRIN (porfimer sodium) for Injection PHOTOFRIN (porfimer sodium) IS INDICATED FOR Palliation of patients with completely
Barrett s Esophagus: Are We Making any Progress?
 3/22/217 arrett s Esophagus: re We Making any Progress? Stuart Jon Spechler, M.D. hief, Division of Gastroenterology, V North Texas Healthcare System; o-director, Esophageal Diseases enter, Professor of
3/22/217 arrett s Esophagus: re We Making any Progress? Stuart Jon Spechler, M.D. hief, Division of Gastroenterology, V North Texas Healthcare System; o-director, Esophageal Diseases enter, Professor of
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis
 Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
EVALUATION FORM WSGNA 2018 Fall Conference Endoscopy for Malignant and Premalignant Lesions of the GI Tract 10/27/2018
 EVALUATION FORM WSGNA 2018 Fall Conference Endoscopy for Malignant and Premalignant Lesions of the GI Tract 10/27/2018 Please respond to the following items on a scale from 5 (highest) to 1 (lowest). The
EVALUATION FORM WSGNA 2018 Fall Conference Endoscopy for Malignant and Premalignant Lesions of the GI Tract 10/27/2018 Please respond to the following items on a scale from 5 (highest) to 1 (lowest). The
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ
 - Project manual + FAQ") Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters.
 Real-Time Increased Detection of Neoplastic Tissue in Barrett s Esophagus with Probe-Based Confocal Laser Endomicroscopy: Final Results of an International Multicenter, Prospective, Randomized, Controlled
Real-Time Increased Detection of Neoplastic Tissue in Barrett s Esophagus with Probe-Based Confocal Laser Endomicroscopy: Final Results of an International Multicenter, Prospective, Randomized, Controlled
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool
 When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
Radiofrequency Ablation: Stepwise circumferential and focal RFA of Barrett s s esophagus using the HALO System
 Radiofrequency Ablation: Stepwise circumferential and focal RFA of Barrett s s esophagus using the HALO System Used abbreviations BE: Barrett s esophagus EC: Early cancer ER: Endoscopic resection HGD:
Radiofrequency Ablation: Stepwise circumferential and focal RFA of Barrett s s esophagus using the HALO System Used abbreviations BE: Barrett s esophagus EC: Early cancer ER: Endoscopic resection HGD:
Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia
 ...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
Endoscopic Submucosal Dissection ESD
 Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Chapter 12: Training in Pathology. DDSEP Chapter 13: Question 19
 DDSEP Chapter 13: Question 19 A 70 year-old male with a history of celiac disease diagnosed in his forties reports abdominal pain, dark stools, and 20-pound weight loss. He reports complete compliance
DDSEP Chapter 13: Question 19 A 70 year-old male with a history of celiac disease diagnosed in his forties reports abdominal pain, dark stools, and 20-pound weight loss. He reports complete compliance
Missed Lesions at Endoscopy. Dr Russell Walmsley, MD, FRCP, FRACP Gastroenterologist WDHB Chair Endoscopy Guidance Group for New Zealand
 Missed Lesions at Endoscopy Dr Russell Walmsley, MD, FRCP, FRACP Gastroenterologist WDHB Chair Endoscopy Guidance Group for New Zealand Missed Lesions at Endoscopy Is there a problem? With Gastroscopy
Missed Lesions at Endoscopy Dr Russell Walmsley, MD, FRCP, FRACP Gastroenterologist WDHB Chair Endoscopy Guidance Group for New Zealand Missed Lesions at Endoscopy Is there a problem? With Gastroscopy
This medical position statement considers a series of
 GASTROENTEROLOGY 2011;140:1084 1091 American Gastroenterological Association Medical Position Statement on the Management of Barrett s Esophagus The Institute Medical Position Panel consisted of the authors
GASTROENTEROLOGY 2011;140:1084 1091 American Gastroenterological Association Medical Position Statement on the Management of Barrett s Esophagus The Institute Medical Position Panel consisted of the authors
Confocal Laser Endomicroscopy
 Confocal Laser Endomicroscopy Policy Number: 2.01.87 Last Review: 3/2018 Origination: 3/2013 Next Review: 9/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage for
Confocal Laser Endomicroscopy Policy Number: 2.01.87 Last Review: 3/2018 Origination: 3/2013 Next Review: 9/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage for
Barrett s esophagus (BE), a known complication of chronic
, a known complication of chronic") CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:220 227 Patients With Nondysplastic Barrett s Esophagus Have Low Risks for Developing Dysplasia or Esophageal Adenocarcinoma SACHIN WANI,* GARY FALK, MATTHEW
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:220 227 Patients With Nondysplastic Barrett s Esophagus Have Low Risks for Developing Dysplasia or Esophageal Adenocarcinoma SACHIN WANI,* GARY FALK, MATTHEW
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Process
 MEASURE TYPE: Process") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Transfer of Health Information and Interoperability 2019 COLLECTION TYPE:
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Transfer of Health Information and Interoperability 2019 COLLECTION TYPE:
evidence note Radiofrequency ablation for Barrett s oesophagus with highgrade What is an evidence note Key points Literature search Introduction
 In response to an enquiry from the National Cancer Waiting Times Delivery Group What is an evidence note Evidence notes are rapid reviews of published secondary clinical and cost-effectiveness evidence
In response to an enquiry from the National Cancer Waiting Times Delivery Group What is an evidence note Evidence notes are rapid reviews of published secondary clinical and cost-effectiveness evidence
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD
 CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD Disclosure Statement NKC: No relevant conflicts to disclose. DTR: No relevant
CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD Disclosure Statement NKC: No relevant conflicts to disclose. DTR: No relevant
Long-term recurrence of neoplasia and Barrett s epithelium after complete endoscopic resection
 Editor s choice Scan to access more free content For numbered affiliations see end of article. Correspondence to Professor Thomas Rösch, Department of Interdisciplinary Endoscopy, University Hospital Hamburg-Eppendorf,
Editor s choice Scan to access more free content For numbered affiliations see end of article. Correspondence to Professor Thomas Rösch, Department of Interdisciplinary Endoscopy, University Hospital Hamburg-Eppendorf,
Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia
: Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia") UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
Barrett s Esophagus Burn, Resect, Freeze, or Just Watch Strategies for Evaluation and Surveillance of Barrett s Amitabh Chak, MD OBJECTIVES: NOTES:
 Speaker 1 Barrett s Esophagus Burn, Resect, Freeze, or Just Watch Strategies for Evaluation and Surveillance of Barrett s Amitabh Chak, MD 1. List the epidemiology of Barrett s esophagus. 2. Review the
Speaker 1 Barrett s Esophagus Burn, Resect, Freeze, or Just Watch Strategies for Evaluation and Surveillance of Barrett s Amitabh Chak, MD 1. List the epidemiology of Barrett s esophagus. 2. Review the
Long-term recurrence of neoplasia and Barrett s epithelium after complete endoscopic resection
 Editor s choice Scan to access more free content ORIGINAL ARTICLE Long-term recurrence of neoplasia and Barrett s epithelium after complete endoscopic resection Mario Anders, 1 Christina Bähr, 1 Muhammad
Editor s choice Scan to access more free content ORIGINAL ARTICLE Long-term recurrence of neoplasia and Barrett s epithelium after complete endoscopic resection Mario Anders, 1 Christina Bähr, 1 Muhammad