Approach to Diagnosis of B-cell Lymphoproliferative Disorders. Eric Hsi, MD Department of Laboratory Medicine
|
|
|
- Kerry Charles
- 5 years ago
- Views:
Transcription
1 Approach to Diagnosis of B-cell Lymphoproliferative Disorders Eric Hsi, MD Department of Laboratory Medicine
2 No relevant financial disclosures
3 Outline The small B-cell lymphoproliferative disorders CLL MCL HCL and HCLv SMZL LPL B-PLL
4 B-CLL 90% of chronic leukemias in the West. 2-6 cases/100,000 people years Median age 65 M>F 2:1 Signs/Symptoms: Most asymptomatic Lymphocytosis (> 5x10 9 /L monoclonal B-cells with CLL phenotype) Fatigue, hemolytic anemia, infection, organomegaly/adenopathy M protein may be present
5 B-CLL Familial predisposition 5-10% have CLL in more than one family member 2-7x risk of CLL in 1 st degree relatives 1 st degree relatives have higher incidence of CLL-type MBL
6 B-CLL Morphology Small round lymphocytes Occasional prolymphocytes (usually <2%) Some cases may have irregular cells with nuclear clefting. Smudge cells
7 CLL Morphologic variation CLL with increased prolymphocytes CLL/PLL - Between 10 and 55% PL associated with worse prognosis. Atypical morphology Less condensed chromatin cleaved lymphocytes


8 CLL

9 CLL

10 CLL/PLL



11 CLL Bone marrow Involved by definition Patterns can be nodular, interstitial, diffuse Proliferation centers uncommon Diffuse pattern has been associated with higher stage and worse prognosis.
12 B-CLL Immunophenotype: CD19+, CD5+, CD20 dim+, CD23+, CD45+, CD200+, FMC7-, CD79b-/+, sig dim Genetics Rearranged Ig genes Del 13q14 (50%), trisomy 12 (20%), del 11q22-23 (20%), del 17p (10%), del 6q (5%) Trisomy 12 linked to atypical morphology Del 13q linked to typical morphology and favorable prognosis (isolated) Del 17p, del 11q22-23, and del 6q: unfavorable prognosis Del 17p in particular shows treatment resistance and short survival
13 B-CLL DDx: B-PLL, T-PLL, MCL, SMZL, FL, L-1 ALL



14 DDx FL L1-ALL MCL
15 B-CLL search for prognostic factors IgH somatic hypermutational status ( 2%) Mutated CLL better prognosis than unmutated CLL. Multiple studies have confirmed this finding. VH3-21 poor prognosis independent of mutational status FISH for recurrent abnormalities CD38 expression status predicts for OS Cutoff of 20% or 30% commonly used Associated with IGH mutational status Unmutated CLL associated with CD38 expression Mutated CLL associated with lack of CD38 expression ZAP-70 Gene expression profiling of mutated vs unmutated CLL identified ZAP-70 as differentially expressed. Hamblin et al 1999 Tobin et al Blood 2002 Damle et al 1999 Weistner et al 2003
16 IGH mutational status and CD38 predict outcome in CLL Survival by Mutational Status Survival by CD38 Status Damle et al 1999
17 Karyotypic abnormalities also predict outcome Several karyotypic abnormalities have been known to occur commonly CLL does not grow well in culture True incidence was not clear Interphase FISH allowed determination of the abnormalities Frequency and clinical significance Dohner H et al 2000
18 Genetic abnormalities in CLL Prognostic information Dohner et al NEJM 2000
19 CLL mutations and CNV Landau Cell 2013
20 Pathways for Driver Mutations Landau Cell 2013
21 CLL Median survival 7 yrs. Transformations PLL High grade (large cell) lymphoma - Richter s transformation HD-like LBL, MM (rare) Treatment: Watch/wait Nucleoside analog (fludarabine), cyclophosphamide +/- rituximab Newer targeted agents (NCCN 2017) BTK inhibitors ibrutinib (relapsed CLL, CLL with 17p/TP53 mutation) PI3K inhibitors idelalisib (relapsed CLL) BCL2 inhibitors venetoclax (relapsed CLL with 17p) Anti-CD20 mabs ofatumumab, obinutuzumab
22 Mantle Cell Lymphoma 3-10% of NHL Median age 60 yrs, M:F = 2:1 Poor prognosis - median survival 3-4 yrs. Lymphadenopathy common with presentation at high clinical stage (III or IV) extranodal sites can be involved: spleen, BM, GI tract (MLP), Waldeyer s ring
23 Mantle cell lymphoma Immunophenotype CD5+, CD10-, CD19+, CD20+, CD23-, sig+, FMC7+, CD79b+, Cyclin D1+, SOX11+ Molecular genetics t(11;14)(q13;q32) - CCND1/IGH present in vast majority of cases Blastoid variants associated with secondary changes such as tetraploid TP53 p16 deletion
24 Mantle Cell Lymphoma Diffuse, nodular, mantle zone pattern Monotonous proliferation of small cells with slight nuclear irregularity (centrocytes) Epithelioid histiocytes may be present Mitotic figures frequent (uncommon in low grade lymphomas) Aggressive cytology variants Blastoid Pleomorphic

25

26

27


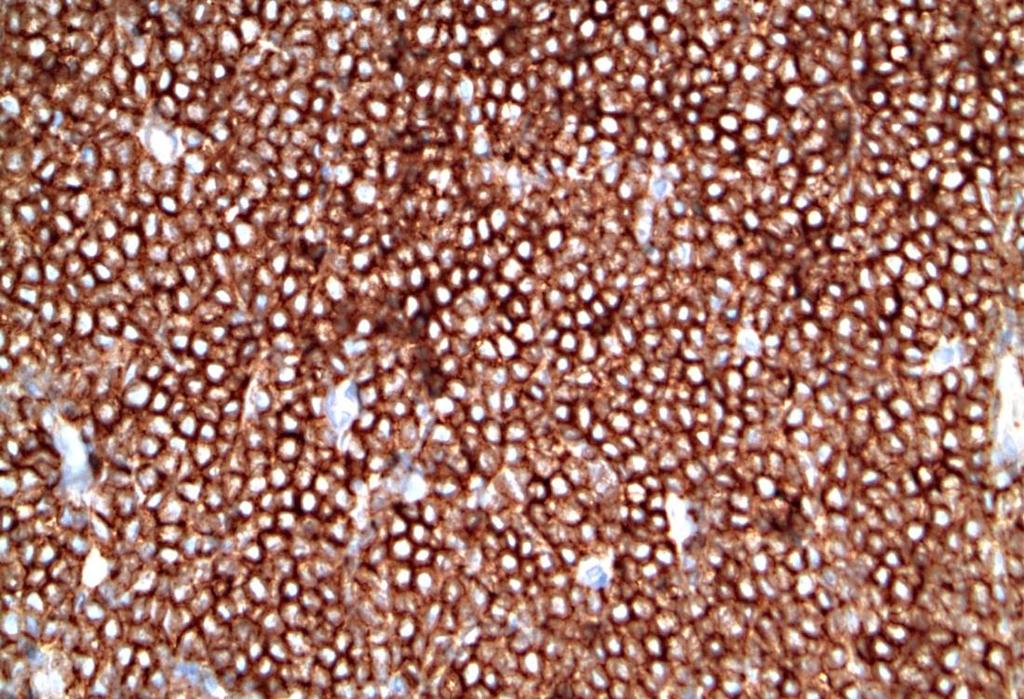


28 CD3 CD20 CD5 Cyclin D1

29 BMCL

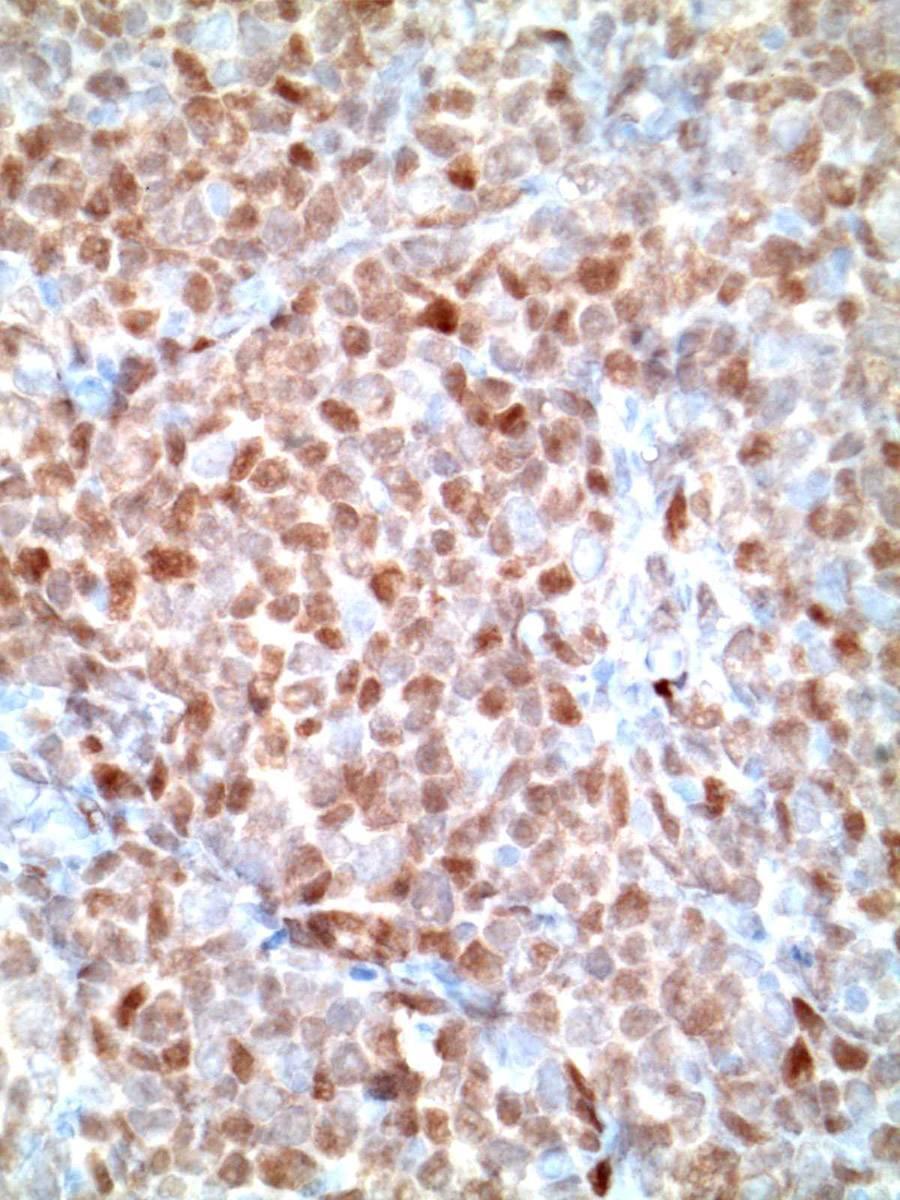
30 Cyclin D1
31 Mantle cell lymphoma Aggressive disease worst of low grade and high grade lymphomas Median survival 3-4 yrs but improving with newer therapies No plateau in survival curve Indolent variants Non-nodal presentation Spleen, PB involvement Often SOX11 negative High expression of SOX11, HDGFRP3 and DBN1 compared to classical MCL (suggesting a distinct biology) Orchard JA Blood 2003 Royo Leukemia 2012
32 Overall Survival: Nodal vs non-nodal Orchard JA Blood 2003
33 Indolent Leukemic MCL (without splenomegaly) Cases exist that are MBL or CLL-like Lymphocytosis without adenopathy or splenomegaly Ondrejka S Haematologica 2011
34 Indolent Leukemic MCL CD20 CyclinD1 CD20 CyclinD1 CyclinD1 Ondrejka et al Haematologica 2011 CyclinD1/SOX11
35 MCL Prognostic factors Proliferation signature has been shown by GEP studies to be of major importance in MCL Ki67 >30% associated with poor prognosis MIPI IGH mutational status Hypermutated (<97% homology) associated with favorable prognosis in MCL (59% vs 40% 5 year OS) 17p deletion (poor) NGS studies 25 significantly recurrently mutated genes Known drivers: ATM, CCND1 Tumor supressor genes: TP53 Antiapototic proteins (BIRC3) TLR2 Chromatin modifiers (MEF2B, MLL2, WHSC1) NOTCH1 and 2 Navarro et al Cancer Res 2012 Bea PNAS, 2013
36 Cyclin D1 negative MCL Approximately 5% of cases Similar GEP as typical MCL Overexpression of other D cyclin genes Morphology identical to typical MCL SOX11+ by IHC (marker for CCND1- MCL) CCND2 rearrangements in 55% of cases Usually immunoglobulin light gene partners Most often light chains (15 of 18 cases) Salaverria I et al Blood 2013 Fu K et al. Blood 2005 Nakashima M AIMM 2014

37 Enlarged Tonsil 82 yo man

38






39 CD20 CD5 Cyclin D1 LEF1 SOX11
40 Mantle Cell Lymphoma Differential Dx: SLL Mantle zone hyperplasia FCL LBL DLBCL B-PLL (blood)

41 B-PLL
42 In situ mantle cell neoplasia Uncommon (<<1% of reactive LNs) 100 reactive LNs screened by IHC none 1293 consecutive LNs from 132 patients screened by IHC none Can find in look back of patients with MCL 17 cases in largest series Adults (median age 66, M=F), incidental finding May have PB involvement by FC (CD5- or +) Can be found with other small B-cell lymphomas One case had treated MCL 4 years prior to ISMN, was followed for 1 year and developed classic MCL Typically indolent behavior with no treatment 1 of 12 patients with isolated ISMN developed MCL 4 years later (SOX11+) Carvajal-Cuenca Haematologica 2012 Adam et al Mod Pathol 2012

43 In situ mantle cell neoplasia Morphology Undistorted architecture, non-expanded mantle zones Cyclin D1+ cells in mantles, often inner portion, may find cells in GCs
44 Hairy Cell Leukemia Uncommon BCLPD - 2% of lymphoid leukemias Median age 55, M>F 5:1 Presents with splenomegaly, cytopenias, and characteristic monocytopenia.
45 HCL PB Morphology: Small lymphocyte Spongy chromatin Abundant lacy cytoplasm with peripheral cytoplasmic projections Absent or inconspicuous nucleoli Cytochemistry Strong TRAP positivity



46 HCL - PB TRAP
47 HCL Bone marrow morphology Variable infiltration Interstitial pattern is common Widely spaced cells with bean-shaped nuclei May have fried egg appearance Some cases may spindle, mimicking mast cell disease Reticulin fibrosis is common, often causing a dry tap Some cases can be hypocellular mimicking aplastic anemia Rare cases can present as a bone tumor.



48
49 Spleen and Liver in HCL Red pulp infiltration with white pulp atrophy. Red cell lakes can be seen collections of RBCs in spaces lined by hairy cells. Liver shows sinusoidal infiltrates.
50 HCL Immunophenotype CD11c+, CD19+, CD20+, CD22+, CD25+, CD103+ No marker is absolute diagnostic but constellation of bright coexpression of CD22 and CD11c is characteristic. Cyclin D1 is weakly expressed in >50% of cases Genetics Rearranged IgH No specific translocations BRAF V600E
51 Discovery of BRAF V600E in HCL Whole exome sequencing in 1 patient with HCL using CD19+ purified B-cells obtained at diagnosis and CD19- purified lymphocytes obtained after therapy. Sequence variants had to be >25% of reads to allow for heterozygous mutants that were present as a major proportion of the clonal population Mutations in BRAF, CSMD3, SLC5A1, CNTN6, and OR8J1 BRAF known to be mutated in many cancers and encodes for a protein kinase involved in MAPK signaling and was targeted for additional testing Sanger sequencing of additional 47 patients and BRAF V600E was found in 100% of cases Tiacci et al. NEJM 2011
52 Hairy cell leukemia and BRAF V600E HCL HCLv BLPD* SMZL Splen L/L, u 48/48 (100) 0/22 (0) 0/16 (0) 0/21 (0) CLL B-PLL LPL FL DLBL MCL BL Method Ref 0/35 (0) 0/71 (0) 0/18 (0) 0/12 (0) Sanger Tiacci /62 (100) 16/16 (100) 0/1 (0) 2/57 (3.5) 0/91 (0) ASPCR Arcaini /1 (0) Pyro Lennerz /136 (0.7) 1/4 (25) ASPCR Langabeer /23 (100) 0/1 (0) 0/11 (0) ASPCR Tiacci /11 0/1 0/8 0/5 1/6 0/2 0/3 0/6 ASPCR Warden 2013 *non CLL, MCL, FL,
53 Mutation Specific Ab Clone VE1 32/32 cases HCL positive All 20 non-hcl mimics cases negative Further screening >200 cases of mature B-cell neoplasms identified 1 CLL case (confirmed by sequencing) Andrulis M et al AJSP 2012
54 HCL Clinical Indolent course with good response to purine nucleoside analogs deoxycorformycin and 2-deoxyadenosine (2-CDA) DDx HCLv, SMZL, PLL
55 HCL Variant Prolymphocytic variant Cells have visible nucleoli, resembling prlymphocytes Chromatin is more condensed than typical HCL Patients present with higher WBC and often have a serum paraprotein. Immunophenotype: CD25-, CD103+ TRAP - Survival is shorter than HCL and it does not respond to HCL therapy (2CDA).


56 HCL v CD19+, CD20+, CD25-, CD22+, CD11c+, CD103+, TRAP- Spleen - red pulp predominant infiltrate
57 MAP2K1 (MEK1) mutation Recently, activating mutations in MAPK21 (exons 2-3) in HCLv and IGH V-34 expression classic HCL have been discovered. 6/15 IGHV4-34 negative HCLv 4/9 IGHV4-34 positive HCLv 5/7 IGHV4-34 negatiev chcl Waterfall et al. Nat Genetics 2014
58 Lymphoplasmacytic Lymphoma Uncommon type of lymphoma (1.5% of NHL) Disease of older adults (median age 63 yrs.), slight male predominance. Commonly involves LN, spleen, BM Often associated with Waldenstrom s macroglobulinemia (IgM paraprotein, >3 gm/dl) Paraprotein can cause cryoglobulinemia, autoimmune HA, neuropathy (myelin-associated glycoprotein)
59 LPL Morphology - LN Diffuse architecture Lymphoplasmacytic cells, Dutcher bodies Plasma cells may be present as admixed cells or in clusters Interfollicular pattern recognized Parcortical or perisinusoidal involvement with sparing of overall architecture and patent sinuses epithelioid histiocytes can mimic Lennert s lymphoma Small follicles or hyperplastic follicles Marginal zone/monocytoid B-cells absent
60 LPL - BM Interstitial or diffuse involvement Small lymphocytes, plasmacytoid lymphocytes, plasma cells Occasional centroblastic or immunoblastic cells Dutcher bodies often present Lymphoplasmacytoid, lymphoplasmacytic, and polymorphous types have been described
61 Lymphoplasmacytic Lymphoma Immunophenotype CD19+, CD20+, CD79a+, sig+, cig+ CD5-, CD10- Molecular genetics MYD88 L265P in >95% of cases 50% of IgM MGUS CXCR4 mutations in 27% (NS/FS mutations) Nonsense mutation assoc higher BM involvement and symptomatic disease requiring therapy Association with Hepatitis C infection and Type II mixed cyroglobulinemia Treon SP et al Blood 2014

62

63

64




65 CD20 CD5 Kappa Lambda

66 Peripheral Blood -55 yo man with anemia and high total protein -IgM kappa paraprotein


67

68




69 CD3 CD20 CD138 Cyclin D1


70 Kappa Lambda
71 Lymphoplasmacytic Lymphoma Differential Dx: SLL Plasmacytoma Marginal zone lymphoma Multiple myeloma Lymphoplasmacytic morphology, often with t(11;14)(q13;q32)

72 66 yo woman presented with anemia and leukopenia BM Aspirate 50x

73 BM Aspirate 100x

74






75 CD138 CD20 Cyclin D1 PAX5 Kappa Lambda
76 Additional Studies FISH positive for IGH/CCND1 MYD88 L265P negative Diagnosis: Plasma cell myeloma with IGH-CCND1 and CD20 expression
77 Splenic Marginal Zone Lymphoma Older adults (median age 66) presenting with splenomegaly +/- villous lymphocytes White pulp involvement with expanded marginal zones (perifollicular areas). Mantle zones infiltrated but GC can be intact sometimes. Red pulp also involved. Nodules have darker appearance in center with lighter outer rim (monocytoid B-cells) Hilar lymph nodes have nodular and diffuse infilrate Cytology varies from center of nodule to outer rim with larger cells collecting at outer edge.

78
79 SMZL Immunophenotype CD19+, CD20+, sig+ CD5-, CD10-, CD22-/+, CD11c-/+, CD25-/+ (30%+), CD103- IgD+ (may distinguish nodal and SMZL from MALT type MZL) Campo et al Am J Surg Pathol, Molecular genetic Loss of 7q22-36 in 30-40% (mirna 29a1 and mirna29b) NOTCH pathway gene mutations (40%) NOTCH2 activating mutation in 10-25% of cases. Others (SPEN, DTX1, NOTCH1) NFkB activation (50%) KLF2 inactivating mutations in 20-40% Loss of NFkB inhibitory activity Non-canonical, canonical pathways PTPRD 0% (contrast with NMZL) Chromatin modification genes (40%) KMT2D(MLL2), SIN3A, ARIDA1, EP300, CREBBP, TBL1XR1 Kiel MJ et al. J Exp Med 2012 Rossi D et al J Exp Med 2012 Clipson et al Leukemia 2015 Spina V et al Best Pract Res Clin Haaemtol 2017
80 Mutations and Pathways in MZL Spina V Best Pract Res Clinc Haematol 2017

81 De novo B-PLL An uncommon disease <1% of lymphocytic leukemias Clinical presentation Median age years at presentation Equal M:F Marked lymphocytosis, splenomegaly without lymphadenopathy, variable anemia/thrombocytopenia Morphology: >55% prolymphocytes Phenotype Mature B-cell markers: CD19, CD20, CD22, FMC7, CD79b, sig CD5 in 20-30% Cyclin D1 negative, SOX11 negative Exclude cases with t(11;14)(q13;q32)/igh-ccnd1 Dearden CE Hematology 2015 Swerdlow SH et al (Eds). WHO Classification of tumours of haematopoietic and lymphoid tissues, IARC 2008
82 B-PLL Generally poor prognosis but a minority (10-15%) may present with indolent/asymptomatic disease May persist for months years Treatment variable (no studies): Stable/indolent watchful waiting First line chemoimmunotherapy (FCR, BR) Relapse/refractory repeat chemoimmunotherapy, BCR inhibitor, trials, SCT. Dearden CE Hematology 2015
83 B-PLL Genetics MYC abnormalities (copy# and translocation) have been reported and appear relative frequently in B- PLL (>50%). Large series of well studied de novo B-PLL cases do not exist No association with Ki-67 index (translocated cases had <30% Ki67 staining) Most cases have a reported aggressive behavior Del(17p) or TP53 loss are also frequent (50%) May occur with MYC translocation Flately E et al. AJCP 2014 Lens D et al. Blood 1997 MYC/IGH Dual Fusion
84 History A 77 yo man with a history of prostate carcinoma (2000) s/p prostatectomy was noticed, at a routine check-up, to have mild thrombocytopenia CBC (Dec. 2003): WBC 6.42, Hgb 14.4, PLT 145K PMN 57%, Lymph 21%, Mono 3%, 9% abnormal lymphocytes. Flow cytometry was performed and showed 39% of lymphocytes were B-cells expressing CD5, CD19, CD20 (bright), CD23, CD79b (bright), FMC7, CD38, lambda (intermediate-bright). FISH studies for IGH-CCND1 were negative.

85 Bone Marrow

86

87




88 CD20 PAX5 CD3 CD5





89 LEF1 SOX11 CD138 k l


90 BCL2 MYC
91 Karyotype 47-53, XY, +der(1;3)(q10;q10)x2, +4, +7, t(8;14)(q24.1;q32), +9, +der(14)t(8;14), +15, add(17)(q21), i(18)(q10)[cp20]
92 History (2) The patient was asymptomatic. Physical exam showed no adenopathy or organomegaly. CT scans of the chest/abdomen showed no adenopathy or mass. Decision was made to watch and wait. He did well with no therapy for 51 months Age 82 Pathologic fracture of the left humerus while playing golf (April 2008)

93 Humerus Biopsy
94 Humerus Biopsy Areas of necrosis were present 2 distinct infiltrates of mononuclear cells Lymphoid cells with features similar to the B-cell lymphoproliferative process originally present in the initial bone marrow biopsy (B-PLL) Immunoblastic component with features of plasmablastic lymphoma (PBL) Lambda restricted CD20 CD5 PAX5 CD138 BCL2 MYC PLL PBL Following images: PLL on left/pbl on right


95 400x original magnification B-PLL PBL




96 CD20 CD20 CD5 CD5




97 CD138 CD138 PAX5 PAX5




98 BCL2 BCL2 MYC MYC


99 PBL: Kappa PBL: Lambda
100 Additional Studies Additional IHC PBL component Cyclin D1-, HHV8-, BCL6-, MYC+, BCL2- VS38c+, Ki67 20% EBER negative Flow cytometry showed: Small B-cell component similar to prior study (CD5+/Lambda+ B-cells) IGH FR3 PCR Single peak Serum/urine protein electrophoresis negative for paraprotein The patient was treated with RCHOP x 5
101 Additional History The patient did well for 1 year and relapsed with multiple bone, soft tissue, lung mases and lymphadenopathy. He began bortezomib therapy but progressed within one month. He suffered a right hip fracture and internal fixation and biopsy was performed (next slide) demonstrating a similar plasmablastic lymphoma IHC/ISH studies showed expression of CD138, MUM1 and cytoplasmic lambda. The cells were negative for EBER, PAX5, cytoplasmic kappa. FISH for MYC rearrangement (break apart probes) was positive The patient elected hospice and died 3 months later (approx. 6 years and 2 mo. after initial diagnosis).
102 Diagnosis B-prolymphocytic leukemia with prolonged indolent phase (51 months) and subsequent transformation to plasmablastic lymphoma. Educational features: The B-PLL, despite the complex karyotype and t(8;14)(q24;q32) followed an asymptomatic indolent course Termination in a plasmablastic lymphoma that was aggressive but associated with loss of BCL2 protein.
103 Reference Age/Sex WBC Current case 77 M 6.42 Y 51 Iioka J Clin Exp Hematopat M 17.1 Y 9 Merchant Arch Pathol Lab Med F 91.8 N 0 Indolent? TFT Karyotype FISH del17p TP , XY, +der(1;3)(q10;q10)x2, +4, +7, t(8;14)(q24.1;q32), +9, +der(14)t(8;14), +15, add(17)(q21), i(18)(q10)[cp20] N NA 47, XY, +der(3)t(3;8)(p13;q13),-8,t(8;14)(q24;q32)+18[cp5]/48, XY,+add(3)(p13),t(8;14)(q24;q32)+18[2]/46,XY[4] N NA 40 45,XX,add(5)(p15),-6,+7,der(8)add(8)(p23), t(8;14)(q24;q32),add(14)(q32),der(14)t(8;14),-17[cp19]/ 46,XX[1] Y NA Put N Ann Hematol M NA N ,XY,t(8;14)(q24;q32)[13]/45,sl, 9,add(10)(q24)[6]/46,XY[4] N NL 65 M NA N ,XY,t(8;14)(q24;q32),+12,del(15)(q?15q?22),+3mar[16]/46,XY[4] N NL 68 F NA NA NA 73 M NA N ,XX,t(8;14)(q24;q32),+12,del(13)(q13q22),+18[9]/47,sl, X[8]/47,sdl1,t(1;6)(q43;q11), t(11;14)(q13;q32)[3] N NL 48,XY,t(8;14)(q24;q32),del(11)(p1?2p14),+12,del(13)(q14q22),add(16)(p13), 17,+2mar [9]/46,XY[1] Y NL 68 M NA N F NA N ,add(X)(p21)[12], Y[12],add(1)(q42)[6],add(3)(p21)[2],45 46,add(X)(p21)[12], Y[12],add(1)(q42)[6],add(3)(p21)[2],add(12)(q24)[3],der(14)t(?,8,14)(?;q24;q32)[12], 17[8],+mar[5][cp12] Y Y 45,XX,t(2;8)(p12;q24),del(3)(p12),+add(3)(q11),der(8)t(8;9)(p12;q?21), 9, 17,der(19)t( 9;19)(?p;q13)[20] Y Y 33 M NA N 5 46,XY,t(8;22)(q24;q11)[20] N N 63 M NA N ,X, Y,t(8;22)(q24;q11), 17, 20[20] Y Y 68 M NA Y 12 46,XY,t(8;22)(q24;q11),der(8)add(8)(p2?3)t(8;22)(q24;q11)[12]/92,slx2[4] N Y Crisotomo RH Leuk Res F 156 N 0 45,X,-X,add(8)(p11.2),t(8;14)(q24;q32),add(20)ql3[8]/46,XX[12] N NA Kuriakose P Cancer Genet Cytogenet F 31.2 Y > 6 46,XX,t(8;14)(q24.1;q32)[10]/46,XX[1] N NA Lens D Leukemia F 60 N 1 44,XX,der(1)t(1;17)(q42;q11),t(2;8)(p12;q24)?dic(14;17)(p11;?q11),-17, - 18,+mar[19]/46,XX[5] Y Y Flately E Am J Clin Pathol F 37.2 N 0 46,XX,t(8;14)(q24.1;q32)[2]/46,XX[19] N NA 78 M 27.8 N 0 45,XY,add(6)(q27),add(7)(q32),del(7)(q32),t(8;14)(q24.1;q32), 10,add(11)(q25),der(12),add(12)(p13),(q11.2), +1-3mar[4]/46,XY[16] hsr(12)(p13), 13,add(14)(p10), 17, 18,del(20) Y NA


104
Pathology of the indolent B-cell lymphomas Elias Campo
 Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
Outlines. Disclosures. Updates on B-cell Chronic Lymphoproliferative Disorders of the Blood and Bone Marrow
 Updates on B-cell Chronic Lymphoproliferative Disorders of the Blood and Bone Marrow Sa A, Wang MD Jeffrey L. Jorgensen, MD, PhD Department of Hematopathology, UT M.D. Anderson Cancer Center, Houston,
Updates on B-cell Chronic Lymphoproliferative Disorders of the Blood and Bone Marrow Sa A, Wang MD Jeffrey L. Jorgensen, MD, PhD Department of Hematopathology, UT M.D. Anderson Cancer Center, Houston,
Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo
 Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas NAIVE -B LYMPHOCYTE MEMORY CELL CLL MCL FL MZL Small cell size Low proliferation
Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas NAIVE -B LYMPHOCYTE MEMORY CELL CLL MCL FL MZL Small cell size Low proliferation
Patterns of Lymphoid Neoplasia in Peripheral Blood. Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure
 Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
B-cell Chronic Lymphoproliferative Disorders of the Blood and Bone Marrow
 B-cell Chronic Lymphoproliferative Disorders of the Blood and Bone Marrow Sanam Loghavi, MD Department of Hematopathology University of Texas MD Anderson Cancer Center Houston, TX Disclosures I have no
B-cell Chronic Lymphoproliferative Disorders of the Blood and Bone Marrow Sanam Loghavi, MD Department of Hematopathology University of Texas MD Anderson Cancer Center Houston, TX Disclosures I have no
9/28/2017. Follicular Lymphoma and Nodal Marginal Zone Lymphoma. Follicular Lymphoma Definition. Low-Grade B-Cell Lymphomas in WHO Classification
 and L. Jeffrey Medeiros, MD DISCLOSURES I do not have anything to disclose Low-Grade B-Cell Lymphomas in WHO Classification Lymphoma Type Frequency Follicular lymphoma 22.1 % Extranodal MALT-lymphoma 7.6
and L. Jeffrey Medeiros, MD DISCLOSURES I do not have anything to disclose Low-Grade B-Cell Lymphomas in WHO Classification Lymphoma Type Frequency Follicular lymphoma 22.1 % Extranodal MALT-lymphoma 7.6
Small, mature-appearing appearing
 B-cell Chronic Lymphoproliferative Disorders of the Blood and Bone Marrow Disclosures I have nothing to disclose. Jeffrey L. Jorgensen, MD, PhD Department of Hematopathology, UT M.D. Anderson Cancer Center,
B-cell Chronic Lymphoproliferative Disorders of the Blood and Bone Marrow Disclosures I have nothing to disclose. Jeffrey L. Jorgensen, MD, PhD Department of Hematopathology, UT M.D. Anderson Cancer Center,
Low-grade B-cell lymphoma
 Low-grade B-cell lymphoma Patho-Basic 11. September 2018 Stephan Dirnhofer Pathology Outline Definition LPL, MBL/CLL/SLL, MCL FL Subtypes & variants Diagnosis including Grading Transformation Summary Be
Low-grade B-cell lymphoma Patho-Basic 11. September 2018 Stephan Dirnhofer Pathology Outline Definition LPL, MBL/CLL/SLL, MCL FL Subtypes & variants Diagnosis including Grading Transformation Summary Be
Small B-cell (Histologically Low Grade) Lymphoma
 Lymphoma") Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
FOLLICULARITY in LYMPHOMA
 FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
Low-Grade B-Cell Lymphomas in WHO Classification. Follicular Lymphoma Definition. Follicular Lymphoma Clinical Features 11/7/2017 DISCLOSURES
 Low-Grade B-Cell Lymphomas in WHO Classification DISCLOSURES I do not have anything to disclose Lymphoma Type Frequency Follicular lymphoma 22.1 % Extranodal MALT-lymphoma 7.6 % Small lymphocytic lymphoma/cll
Low-Grade B-Cell Lymphomas in WHO Classification DISCLOSURES I do not have anything to disclose Lymphoma Type Frequency Follicular lymphoma 22.1 % Extranodal MALT-lymphoma 7.6 % Small lymphocytic lymphoma/cll
Case 3. Ann T. Moriarty,MD
 Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Flow cytometric analysis of B-cell lymphoproliferative disorders
 Flow cytometric analysis of B-cell lymphoproliferative disorders David M. Dorfman, M.D., Ph.D. Department of Pathology Brigham and Women s Hospital and Harvard Medical School Boston, MA Objectives Review
Flow cytometric analysis of B-cell lymphoproliferative disorders David M. Dorfman, M.D., Ph.D. Department of Pathology Brigham and Women s Hospital and Harvard Medical School Boston, MA Objectives Review
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
PhenoPath. Diagnoses you can count on B CELL NON-HODGKIN LYMPHOMA
 PhenoPath Diagnoses you can count on B CELL NON-HODGKIN LYMPHOMA C urrent diagnosis of B cell non-hodgkin lymphoma (B-NHL) is based on the 2008 WHO Classification of Tumours of Haematopoietic and Lymphoid
PhenoPath Diagnoses you can count on B CELL NON-HODGKIN LYMPHOMA C urrent diagnosis of B cell non-hodgkin lymphoma (B-NHL) is based on the 2008 WHO Classification of Tumours of Haematopoietic and Lymphoid
Immunopathology of Lymphoma
 Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
A Practical Guide To Diagnose B-Cell Lymphomas on FNAs. Nancy P. Caraway, M.D.
 A Practical Guide To Diagnose B-Cell Lymphomas on FNAs Nancy P. Caraway, M.D. Major Factors Impacting Dx Lymphomas on Small Bxs Classification systems Immunophenotyping by multiprobe flow cytometry and
A Practical Guide To Diagnose B-Cell Lymphomas on FNAs Nancy P. Caraway, M.D. Major Factors Impacting Dx Lymphomas on Small Bxs Classification systems Immunophenotyping by multiprobe flow cytometry and
The patient had a mild splenomegaly but no obvious lymph node enlargement. The consensus phenotype obtained from part one of the exercise was:
 Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo
 Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
3/23/2017. Disclosure of Relevant Financial Relationships. Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?!
 Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?! Judith A. Ferry Massachusetts General Hospital Disclosure of Relevant Financial Relationships USCAP requires that all
Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?! Judith A. Ferry Massachusetts General Hospital Disclosure of Relevant Financial Relationships USCAP requires that all
CCND1-IGH Fusion-Amplification and MYC Copy Number Gain in a Case of Pleomorphic Variant Mantle Cell Lymphoma
 AJCP /CASE REPORT CCND1-IGH Fusion-Amplification and MYC Copy Number Gain in a Case of Pleomorphic Variant Mantle Cell Lymphoma Yuan Miao, MD, 1,2 Pei Lin, MD, 1 Wei Wang, MD, 1 L. Jeffrey Medeiros, MD,
AJCP /CASE REPORT CCND1-IGH Fusion-Amplification and MYC Copy Number Gain in a Case of Pleomorphic Variant Mantle Cell Lymphoma Yuan Miao, MD, 1,2 Pei Lin, MD, 1 Wei Wang, MD, 1 L. Jeffrey Medeiros, MD,
Diagnosis of lymphoid neoplasms has been
 Iranian Journal of Pathology (2007)2 (1), 1-61 Review Article Mehdi Nassiri Dep. of Pathology, University of Miami Miller School of Medicine, Miami, USA Abstract Correct diagnosis and classification of
Iranian Journal of Pathology (2007)2 (1), 1-61 Review Article Mehdi Nassiri Dep. of Pathology, University of Miami Miller School of Medicine, Miami, USA Abstract Correct diagnosis and classification of
CLL what do I need to know as an Internist in Taimur Sher MD Associate Professor of Medicine Mayo Clinic
 CLL what do I need to know as an Internist in 218 Taimur Sher MD Associate Professor of Medicine Mayo Clinic Case 1 7 y/o white male for yearly medical evaluation Doing well and healthy Past medical history
CLL what do I need to know as an Internist in 218 Taimur Sher MD Associate Professor of Medicine Mayo Clinic Case 1 7 y/o white male for yearly medical evaluation Doing well and healthy Past medical history
Methods used to diagnose lymphomas
 Institut für Pathologie Institut für Pathologie Methods used to diagnose lymphomas Prof. Dr.Med. Leticia Quintanilla-Fend Molecular techniques NGS histology Cytology AS-PCR Sanger seq. MYC Immunohistochemistry
Institut für Pathologie Institut für Pathologie Methods used to diagnose lymphomas Prof. Dr.Med. Leticia Quintanilla-Fend Molecular techniques NGS histology Cytology AS-PCR Sanger seq. MYC Immunohistochemistry
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Test Utilization: Chronic Lymphocytic Leukemia
 Test Utilization: Chronic Lymphocytic Leukemia Initial Evaluation Diagnostic Criteria Selection of Tests for Prognosis Response to Therapy Challenges Assessment for persistent disease Paul J. Kurtin, M.D.
Test Utilization: Chronic Lymphocytic Leukemia Initial Evaluation Diagnostic Criteria Selection of Tests for Prognosis Response to Therapy Challenges Assessment for persistent disease Paul J. Kurtin, M.D.
2013 AAIM Pathology Workshop
 2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
Initial Diagnosis and Treatment 81 Male
 Case SH2017-0359 Shiraz Fidai 1, Sandeep Gurbuxani 1, Girish Venkataraman 1, Gordana Raca 2, Madina Sukhanova 3, Michelle M Le Beau 3, Y. Lynn Wang 4, Mir Alikhan 4, Megan M.McNerney 4, Yuri Kobzev 4,
Case SH2017-0359 Shiraz Fidai 1, Sandeep Gurbuxani 1, Girish Venkataraman 1, Gordana Raca 2, Madina Sukhanova 3, Michelle M Le Beau 3, Y. Lynn Wang 4, Mir Alikhan 4, Megan M.McNerney 4, Yuri Kobzev 4,
Hematology 101. Rachid Baz, M.D. 5/16/2014
 Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
accumulation the blood, marrow, lymph nodes, and spleen.
 Chronic Lymphocytic Leukemia accumulation of mature-appearing appearing lymphocytes in the blood, marrow, lymph nodes, and spleen. CLL cells are: monoclonal l B lymphocytes that express CD19. CD5, and
Chronic Lymphocytic Leukemia accumulation of mature-appearing appearing lymphocytes in the blood, marrow, lymph nodes, and spleen. CLL cells are: monoclonal l B lymphocytes that express CD19. CD5, and
Aggressive B-cell Lymphomas
 Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
Molecular Advances in Hematopathology
 Molecular Advances in Hematopathology HOW MOLECULAR METHODS HAVE CHANGED MY PRACTICE Objectives Understand the importance of cytogenetic/molecular studies in hematolymphoid diseases Know some of the important
Molecular Advances in Hematopathology HOW MOLECULAR METHODS HAVE CHANGED MY PRACTICE Objectives Understand the importance of cytogenetic/molecular studies in hematolymphoid diseases Know some of the important
CLL & SLL: Current Management & Treatment. Dr. Isabelle Bence-Bruckler
 CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
LYMPHOMAS an overview of some subtypes of NHLs
 One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
Case Report Primary Hairy Cell Leukemia/Lymphoma of the Breast: A Case Report and Review of the Literature
 Hindawi Publishing Corporation Volume 2014, Article ID 497027, 5 pages http://dx.doi.org/10.1155/2014/497027 Case Report Primary Hairy Cell Leukemia/Lymphoma of the Breast: A Case Report and Review of
Hindawi Publishing Corporation Volume 2014, Article ID 497027, 5 pages http://dx.doi.org/10.1155/2014/497027 Case Report Primary Hairy Cell Leukemia/Lymphoma of the Breast: A Case Report and Review of
Lymphoma Update: Lymphoma Update: What s Likely to be New in the New WHO. Patrick Treseler, MD, PhD University of California San Francisco
 Lymphoma Update: What s Likely to be New in the New WHO Blood 127:2375; 2016 Patrick Treseler, MD, PhD University of California San Francisco Lymphoma Update: What IS New in the New WHO! Patrick Treseler,
Lymphoma Update: What s Likely to be New in the New WHO Blood 127:2375; 2016 Patrick Treseler, MD, PhD University of California San Francisco Lymphoma Update: What IS New in the New WHO! Patrick Treseler,
CLL: disease specific biology and current treatment. Dr. Nathalie Johnson
 CLL: disease specific biology and current treatment Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck
CLL: disease specific biology and current treatment Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck
Investigation and Management of Chronic Lymphocytic Leukemia. James Johnston
 Investigation and Management of Chronic Lymphocytic Leukemia James Johnston Site Specific Clinics CLL Clinic (787-4454) Erin Elphee BN James Johnston Rajat Kumar Matt Seftel (transplant) Myeloma Clinic
Investigation and Management of Chronic Lymphocytic Leukemia James Johnston Site Specific Clinics CLL Clinic (787-4454) Erin Elphee BN James Johnston Rajat Kumar Matt Seftel (transplant) Myeloma Clinic
Gray Zones and Double Hits Distinguishing True Burkitt Lymphoma from Other High-Grade B-NHLs Burkitt Lymphoma Burkitt-Like Lymphoma DLBCL Patrick Tres
 Gray Zones and Double Hits Distinguishing True Burkitt Lymphoma from Other High-Grade B-NHLs Burkitt Lymphoma Burkitt-Like Lymphoma DLBCL Patrick Treseler, MD, PhD University of California San Francisco
Gray Zones and Double Hits Distinguishing True Burkitt Lymphoma from Other High-Grade B-NHLs Burkitt Lymphoma Burkitt-Like Lymphoma DLBCL Patrick Treseler, MD, PhD University of California San Francisco
CLL & SLL: Current Management & Treatment. Dr. Peter Anglin
 CLL & SLL: Current Management & Treatment Dr. Peter Anglin Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of blood cell B lymphocyte Lymphocytic Cancer of white blood
CLL & SLL: Current Management & Treatment Dr. Peter Anglin Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of blood cell B lymphocyte Lymphocytic Cancer of white blood
Aggressive B-Cell Lymphomas
 Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
HIGH GRADE B-CELL LYMPHOMA DAVID NOLTE, MD (PGY-2) HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD
 HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD") HIGH GRADE B-CELL LYMPHOMA DAVID NOLTE, MD (PGY-2) HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD OUTLINE High grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements Patient presentation 2008/2016
HIGH GRADE B-CELL LYMPHOMA DAVID NOLTE, MD (PGY-2) HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD OUTLINE High grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements Patient presentation 2008/2016
Plasma cell myeloma (multiple myeloma)
") Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
11/8/2018 DISCLOSURES. I have NO Conflicts of Interest to Disclose. UTILTY OF DETECTING PATTERNS
 Bharat N. Nathwani, M.D. City of Hope Medical Center Professor, Director of Pathology Consultation Services, 1500 East Duarte Road, Duarte, California, 91010 DISCLOSURES -------------------------------------------------------
Bharat N. Nathwani, M.D. City of Hope Medical Center Professor, Director of Pathology Consultation Services, 1500 East Duarte Road, Duarte, California, 91010 DISCLOSURES -------------------------------------------------------
Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent
 Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Follicular Lymphoma: the WHO
 Follicular Lymphoma: the WHO and the WHERE? Yuri Fedoriw, MD Associate Professor of Pathology and Laboratory Medicine Director of Hematopathology University of North Carolina Chapel Hill, NC Disclosure
Follicular Lymphoma: the WHO and the WHERE? Yuri Fedoriw, MD Associate Professor of Pathology and Laboratory Medicine Director of Hematopathology University of North Carolina Chapel Hill, NC Disclosure
5000 International Clinical Cytometry Society: Practical Flow Cytometry in Hematopathology A Case-Based Approach
 5000 International Clinical Cytometry Society: Practical Flow Cytometry in Hematopathology A Case-Based Approach Joseph A DiGiuseppe, MD, PhD Hartford Hospital Disclosures In the past 12 months, I have
5000 International Clinical Cytometry Society: Practical Flow Cytometry in Hematopathology A Case-Based Approach Joseph A DiGiuseppe, MD, PhD Hartford Hospital Disclosures In the past 12 months, I have
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Osteosclerotic Myeloma (POEMS Syndrome)
") Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
Non-Hodgkin s Lymphomas Version
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
CLL Biology and Initial Management. Gordon D. Ginder, MD Director, Massey Cancer Center Lipman Chair in Oncology
 CLL Biology and Initial Management Gordon D. Ginder, MD Director, Massey Cancer Center Lipman Chair in Oncology CLL- Epidemiology Most common adult leukemia 25-30% in western world Incidence in US 4.5
CLL Biology and Initial Management Gordon D. Ginder, MD Director, Massey Cancer Center Lipman Chair in Oncology CLL- Epidemiology Most common adult leukemia 25-30% in western world Incidence in US 4.5
High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li,
: Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li,") High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li, M.D., Ph.D. Fudan University Shanghai Cancer Center
High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li, M.D., Ph.D. Fudan University Shanghai Cancer Center
5003 Immunohistochemistry in hematopathology, what's in, what's out, what's useful
 www.ascp.org/ascp2014 5003 Immunohistochemistry in hematopathology, what's in, what's out, what's useful Kathryn Rizzo, DO, PhD VIRGINIA COMMONWEALTH UNIVERSITY Department of Pathology School of Medicine
www.ascp.org/ascp2014 5003 Immunohistochemistry in hematopathology, what's in, what's out, what's useful Kathryn Rizzo, DO, PhD VIRGINIA COMMONWEALTH UNIVERSITY Department of Pathology School of Medicine
Society for Hematopathology 2017
 Society for Hematopathology 2017 Session 2 Genetic Testing in the Diagnosis of Lymphoid Neoplasms Summary of the cases Session Chairs: Rebecca King and Miguel Piris September 7, 2017 Lymphoma diseases/variants
Society for Hematopathology 2017 Session 2 Genetic Testing in the Diagnosis of Lymphoid Neoplasms Summary of the cases Session Chairs: Rebecca King and Miguel Piris September 7, 2017 Lymphoma diseases/variants
Clinicopathologic features of 112 cases with mantle cell lymphoma
 Cancer Biol Med 2015;12:46-52. doi: 10.7497/j.issn.2095-3941.2015.0007 ORIGINAL ARTICLE Clinicopathologic features of 112 cases with mantle cell lymphoma Dong-Mei Zhou, Gang Chen, Xiong-Wei Zheng, Wei-Feng
Cancer Biol Med 2015;12:46-52. doi: 10.7497/j.issn.2095-3941.2015.0007 ORIGINAL ARTICLE Clinicopathologic features of 112 cases with mantle cell lymphoma Dong-Mei Zhou, Gang Chen, Xiong-Wei Zheng, Wei-Feng
Lymphoid Neoplasms. Sylvie Freeman Department of Clinical Immunology, University of Birmingham
 Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
Pathology #07. Hussein Al-Sa di. Dr. Sohaib Al-Khatib. Mature B-Cell Neoplasm. 0 P a g e
 Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
The History of Lymphoma Classification and the 2017 Revision
 The History of Lymphoma Classification and the 2017 Revision ESMO Perceptorship on Lymphoma, Lugano 2018 German Ott Department of Clinical Pathology, Robert-Bosch-Krankenhaus and Dr. Margarete Fischer-Bosch
The History of Lymphoma Classification and the 2017 Revision ESMO Perceptorship on Lymphoma, Lugano 2018 German Ott Department of Clinical Pathology, Robert-Bosch-Krankenhaus and Dr. Margarete Fischer-Bosch
Many of the hematolymphoid disorders are derived
 REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
WHO 2016 update lymphoid neoplasms. Dr Sue Morgan Alfred Hospital, Melbourne
 WHO 2016 update lymphoid neoplasms Dr Sue Morgan Alfred Hospital, Melbourne WHO 4 th edition 2008 Established guideline worldwide for diagnosis of haematological malignancy for the last 9 years Significant
WHO 2016 update lymphoid neoplasms Dr Sue Morgan Alfred Hospital, Melbourne WHO 4 th edition 2008 Established guideline worldwide for diagnosis of haematological malignancy for the last 9 years Significant
PRECURSOR LYMHPOID NEOPLASMS. B lymphoblastic leukaemia/lymphoma T lymphoblastic leukaemia/lymphoma
 PRECURSOR LYMHPOID NEOPLASMS B lymphoblastic leukaemia/lymphoma T lymphoblastic leukaemia/lymphoma B lymphoblastic leukaemia/lymphoma Definition: B lymphoblastic leukaemia/lymphoma is a neoplasm of precursor
PRECURSOR LYMHPOID NEOPLASMS B lymphoblastic leukaemia/lymphoma T lymphoblastic leukaemia/lymphoma B lymphoblastic leukaemia/lymphoma Definition: B lymphoblastic leukaemia/lymphoma is a neoplasm of precursor
What can a «solid-tumour» expert learn from lymphomas and myeloma management
 What can a «solid-tumour» expert learn from lymphomas and myeloma management Franco Cavalli M.D., F.R.C.P. Scientific Director Oncology Institute of Southern Switzerland (IOSI) A bit of history (I) CT
What can a «solid-tumour» expert learn from lymphomas and myeloma management Franco Cavalli M.D., F.R.C.P. Scientific Director Oncology Institute of Southern Switzerland (IOSI) A bit of history (I) CT
CLL Ireland Information Day Presentation
 CLL Ireland Information Day Presentation 5 May 2018 Professor Patrick Thornton Consultant Haematologist, Senior Lecturer RCSI, and Clinical Director Hermitage Medical Clinic Laboratory Chronic Lymphocytic
CLL Ireland Information Day Presentation 5 May 2018 Professor Patrick Thornton Consultant Haematologist, Senior Lecturer RCSI, and Clinical Director Hermitage Medical Clinic Laboratory Chronic Lymphocytic
ACCME/Disclosures 4/13/2016. Clinical History
 ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
The development of clonality testing for lymphomas in the Bristol Genetics Laboratory. Dr Paula Waits Bristol Genetics Laboratory
 The development of clonality testing for lymphomas in the Bristol Genetics Laboratory Dr Paula Waits Bristol Genetics Laboratory Introduction The majority of lymphoid malignancies belong to the B cell
The development of clonality testing for lymphomas in the Bristol Genetics Laboratory Dr Paula Waits Bristol Genetics Laboratory Introduction The majority of lymphoid malignancies belong to the B cell
Aggressive B cell Lymphomas
 Aggressive B cell Lymphomas I have nothing to disclose. Disclosures Raju K. Pillai City of Hope National Medical Center Outline WHO 2016 Classification Large B cell Lymphomas New entities and changes in
Aggressive B cell Lymphomas I have nothing to disclose. Disclosures Raju K. Pillai City of Hope National Medical Center Outline WHO 2016 Classification Large B cell Lymphomas New entities and changes in
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Parts 2 and 3
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Parts 2 and 3 NEOPLASTIC LYMPHOID DISEASES Introduction o The bone marrow is the source of all cells in the
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Parts 2 and 3 NEOPLASTIC LYMPHOID DISEASES Introduction o The bone marrow is the source of all cells in the
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Immunohistochemical classification of haematolymphoid tumours. Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital
 Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
The next lymphoma classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno
 Evolution of classification The next classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno The Lymphoma Forum of Excellence, Bellinzona, January 2011 Rappaport Lukes and Collins (immunophenotype)
Evolution of classification The next classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno The Lymphoma Forum of Excellence, Bellinzona, January 2011 Rappaport Lukes and Collins (immunophenotype)
DETERMINATION OF A LYMPHOID PROCESS
 Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
LES CAHIERS CERBA. Recommendations for the diagnosis and interpretation of blood lymphocytosis
 LES CAHIERS CERBA Recommendations for the diagnosis and interpretation of blood lymphocytosis written by B. Caron Servan, S. Defasque, C. Hémar, H. Mossafa Clinical pathologists, Laboratoire CERBA LES
LES CAHIERS CERBA Recommendations for the diagnosis and interpretation of blood lymphocytosis written by B. Caron Servan, S. Defasque, C. Hémar, H. Mossafa Clinical pathologists, Laboratoire CERBA LES
Mantle Cell Lymphoma
 Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
WHO Classification. B-cell chronic lymphocytic leukemia/small T-cell granular lymphocytic leukemia
 Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
NORTH CAROLINA SOCIETY OF PATHOLOGISTS
 NORTH CAROLINA SOCIETY OF PATHOLOGISTS 2018 Annual Meeting and Shelley Lecture April 13-14, 2018 The Ballantyne Hotel Charlotte, NC FOCUS ON HEMATOPATHOLOGY SATURDAY HANDOUTS This continuing medical education
NORTH CAROLINA SOCIETY OF PATHOLOGISTS 2018 Annual Meeting and Shelley Lecture April 13-14, 2018 The Ballantyne Hotel Charlotte, NC FOCUS ON HEMATOPATHOLOGY SATURDAY HANDOUTS This continuing medical education
Diagnostic Molecular Pathology of Lymphoid Neoplasms
 Diagnostic Molecular Pathology of Lymphoid Neoplasms (Part II) Rational use of molecular testing in lymphomas Beirut, Lebanon Friday December 2, 2011: Hematopathology Session Adam Bagg University of Pennsylvania
Diagnostic Molecular Pathology of Lymphoid Neoplasms (Part II) Rational use of molecular testing in lymphomas Beirut, Lebanon Friday December 2, 2011: Hematopathology Session Adam Bagg University of Pennsylvania
WHO UPDATE ON LYMPHOMAS. Dr Priya Mary Jacob Asst Professor, Pathology.
 WHO UPDATE ON LYMPHOMAS Dr Priya Mary Jacob Asst Professor, Pathology 3 rd 4 th 4 th revised 2001 2008 2017 The Change The Significance of the Change- Diagnostic, Prognostic The Rationale behind the change.
WHO UPDATE ON LYMPHOMAS Dr Priya Mary Jacob Asst Professor, Pathology 3 rd 4 th 4 th revised 2001 2008 2017 The Change The Significance of the Change- Diagnostic, Prognostic The Rationale behind the change.
Participants Identification No. % Evaluation
 BMD-02 Cell Identification Participants Identification No. % Evaluation Erythrocyte precursor, normal 228 95.8 Educational Erythrocyte, normal 7 3.0 Educational Erythrocyte precursor with megaloblastic
BMD-02 Cell Identification Participants Identification No. % Evaluation Erythrocyte precursor, normal 228 95.8 Educational Erythrocyte, normal 7 3.0 Educational Erythrocyte precursor with megaloblastic
The ABCs of Waldenström s Macroglobulinemia (WM)
") The ABCs of Waldenström s Macroglobulinemia (WM) Jeffrey V. Matous MD Colorado Blood Cancer Institute IWMF Ed Forum May 2017 Objectives Describe the roots underneath WM Review incidence, possible risk
The ABCs of Waldenström s Macroglobulinemia (WM) Jeffrey V. Matous MD Colorado Blood Cancer Institute IWMF Ed Forum May 2017 Objectives Describe the roots underneath WM Review incidence, possible risk
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies
 Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Commentary on the WHO Classification of Tumors of Lymphoid Tissues (2008): Indolent B Cell Lymphomas
: Indolent B Cell Lymphomas") Commentary on the WHO Classification of Tumors of Lymphoid Tissues (2008): Indolent B Cell Lymphomas The Harvard community has made this article openly available. Please share how this access benefits
Commentary on the WHO Classification of Tumors of Lymphoid Tissues (2008): Indolent B Cell Lymphomas The Harvard community has made this article openly available. Please share how this access benefits
Aggressive B-cell Lymphoma 2013
 Aggressive B-cell Lymphoma 2013 Diffuse Large B-Cell Lymphoma Burkitt Lymphoblastic lymphoma Gray zone Intermediate DLBCL/HL Intermediate BL/DLBCL Diffuse Large B-cell lymphoma Common morphology: diffuse
Aggressive B-cell Lymphoma 2013 Diffuse Large B-Cell Lymphoma Burkitt Lymphoblastic lymphoma Gray zone Intermediate DLBCL/HL Intermediate BL/DLBCL Diffuse Large B-cell lymphoma Common morphology: diffuse
Workshop Case # 8 (H 4205/07)
") Workshop Case # 8 (H 4205/07) 53 y old male patient had a history of gastrectomy 15 years earlier for gastric carcinoma.on routine sonographic and CT control an enlarged lymph node was detected in the
Workshop Case # 8 (H 4205/07) 53 y old male patient had a history of gastrectomy 15 years earlier for gastric carcinoma.on routine sonographic and CT control an enlarged lymph node was detected in the
Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma
 Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma Nancy Lee Harris, M. D. Massachusetts General Hospital Harvard Medical School Aggressive B-cell Lymphomas WHO 4 th Edition
Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma Nancy Lee Harris, M. D. Massachusetts General Hospital Harvard Medical School Aggressive B-cell Lymphomas WHO 4 th Edition
Defined lymphoma entities in the current WHO classification
 Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
GENETIC MARKERS IN LYMPHOMA a practical overview. P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute
 GENETIC MARKERS IN LYMPHOMA a practical overview P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute B and T cell monoclonalities Rearrangement of immunoglobin and TCR genes may help
GENETIC MARKERS IN LYMPHOMA a practical overview P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute B and T cell monoclonalities Rearrangement of immunoglobin and TCR genes may help
Hepatic Lymphoma Diagnosis An Algorithmic Approach
 Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Prepared by: Dr.Mansour Al-Yazji
 C L L CLL Prepared by: Abd El-Hakeem Abd El-Rahman Abu Naser Ahmed Khamis Abu Warda Ahmed Mohammed Abu Ghaben Bassel Ziad Abu Warda Nedal Mostafa El-Nahhal Dr.Mansour Al-Yazji LEUKEMIA Leukemia is a form
C L L CLL Prepared by: Abd El-Hakeem Abd El-Rahman Abu Naser Ahmed Khamis Abu Warda Ahmed Mohammed Abu Ghaben Bassel Ziad Abu Warda Nedal Mostafa El-Nahhal Dr.Mansour Al-Yazji LEUKEMIA Leukemia is a form
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU
 Rex K.H. Au-Yeung Department of Pathology, HKU") Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Clinical Policy: Bendamustine (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307
 Reference Number: PA.CP.PHAR.307") Clinical Policy: (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that
Clinical Policy: (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that
Lymphoid Neoplasms Associated With IgM Paraprotein A Study of 382 Patients
 Hematopathology / LYMPHOMAS WITH IGM PARAPROTEIN Lymphoid Neoplasms Associated With IgM Paraprotein A Study of 382 Patients Pei Lin, MD, 1 Suyang Hao, MD, 1* Beverly C. Handy, MD, 2 Carlos E. Bueso-Ramos,
Hematopathology / LYMPHOMAS WITH IGM PARAPROTEIN Lymphoid Neoplasms Associated With IgM Paraprotein A Study of 382 Patients Pei Lin, MD, 1 Suyang Hao, MD, 1* Beverly C. Handy, MD, 2 Carlos E. Bueso-Ramos,
WBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
Welcome & Introductions
 Living with Chronic Lymphocytic Leukemia (CLL) Welcome & Introductions Dr. Brander s slides are available for download at www.lls.org/programs Wednesday, July 12, 2017 1 Living with Chronic Lymphocytic
Living with Chronic Lymphocytic Leukemia (CLL) Welcome & Introductions Dr. Brander s slides are available for download at www.lls.org/programs Wednesday, July 12, 2017 1 Living with Chronic Lymphocytic
The spectrum of flow cytometry of the bone marrow
 The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
Update on Waldenström Macroglobulinemia (WM)
") Update on Waldenström Macroglobulinemia (WM) Stephen M. Ansell, MD, PhD Professor of Medicine Division of Hematology Mayo Clinic Rochester, MN Update on Waldenström Macroglobulinemia (WM) Disclosures Stephen
Update on Waldenström Macroglobulinemia (WM) Stephen M. Ansell, MD, PhD Professor of Medicine Division of Hematology Mayo Clinic Rochester, MN Update on Waldenström Macroglobulinemia (WM) Disclosures Stephen
Case Workshop of Society for Hematopathology and European Association for Haematopathology
 Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Aggressive B cell Lymphomas
 Aggressive B cell Lymphomas Raju K. Pillai City of Hope National Medical Center I have no disclosures Outline What is new in the WHO 2016 classification Insights from genomic studies Double Hit Lymphoma
Aggressive B cell Lymphomas Raju K. Pillai City of Hope National Medical Center I have no disclosures Outline What is new in the WHO 2016 classification Insights from genomic studies Double Hit Lymphoma