Lymphoid Neoplasms. Sylvie Freeman Department of Clinical Immunology, University of Birmingham
|
|
|
- George Fletcher
- 6 years ago
- Views:
Transcription
1 Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham
2 Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760 (2%) Non-Hodgkin s Lymphoma 9,280 (3%) Hodgkin s Disease 1,430 (<1%) Multiple Myeloma 3,570 (1%)
3 Overview of Lymphoma neoplasms of lymphoid origin, typically causing lymphadenopathy leukemia vs lymphoma lymphomas viewed as clonal expansions of lymphocyte arrested at a certain stage of development and transformed into a malignant cell types of non- Hodgkin s lymphoma reflect the developmental stages of lymphocytes. 85% of NHL are of B cell origin
4 B +TdT +HLA-DR Stem Cell T B cell T cell Precursor Pro B TdT+ CD19+ Pre B Bone Marrow Bone CD19+ Marrow CD22+ CD20+/- CD10+/- Thymus TdT+ CD4- CD8- TCR Pre thymic Cortical Thymocyte TCR Medullar Thymocyte T TdT+ CD4+ TdT+ CD4+ CD8+ TdT+ CD8+ Mature Mature B CD20+ CD22+ CD19+ CD10+/- Memory Naive Centroblast Centrocyte Plasma cell Peripheral Blood & 2ry Lymphoid Organs TdT+ CD4- CD8- CD4- CD8- Mature T cell T cell CD4+ Helper T CD8+ Cyto toxic T Fig. B and T cell MaturationPathway
5 Types of Lymphoid neoplasms Precursor B- and T- cell (lymphoblastic leukaemia/lymphoma) Mature B-cell neoplasms (includes NHLs, chronic leukaemias, plasma cell dyscrasias) Mature T-cell and NK-cell neoplasms (includes NHLs, chronic leukaemias) (Hodgkin lymphoma)
6 B-cell development stem cell lymphoid precursor progenitor-b LBL, ALL pre-b immature B-cell CLL MCL mature naive B-cell germinal center B-cell DLBCL, FL, BL, HL memory B-cell MZL CLL MM plasma cell


7 Mantle zone lymphoma Follicular lymphoma Burkitt s lymphoma Small lymphocytic lymphoma Waldenström s macroglobulinemia Sézary syndrome Mycosis fungoides Peripheral T cell lymphoma
8 The challenge of lymphoma classification Biologically rational classification Diseases that have distinct morphology immunophenotype genetic features clinical features Clinically useful classification Diseases that have distinct clinical features natural history prognosis treatment
9 WHO Classification (2001) B-cell neoplasms Precursor B-cell neoplasm Precursor B-lymphoblastic leukemia/lymphoma (precursor B-cell acute lymphoblastic leukemia) Mature (peripheral) B-cell neoplasms B-cell chronic lymphocytic leukemia/small lymphocytic lymphoma B-cell prolymphocytic leukemia Lymphoplasmacytic lymphoma Splenic marginal zone B-cell lymphoma (with or w/o villous lymphocyt es) Hairy cell leukemia Plasma cell myeloma/plasmacytoma Extranodal marginal zone B-cell lymphoma of mucosa- associated lymphoid tissue type Nodal marginal zone B-cell lymphoma (with or w/o monocytoid B cells) Follicular lymphoma Mantle cell lymphoma Diffuse large B-cell lymphoma Mediastinal large B-cell lymphoma Primary effusion lymphoma Burkitt's lymphoma/burkitt's cell leukemia T- and NK-cell neoplasms Precursor T-cell neoplasm Precursor T-lymphoblastic lymphoma/leukemia (precursor T- cell acute lymphoblastic leukemia) Mature (peripheral) T-cell neoplasms T-cell prolymphocytic leukemia T-cell granular lymphocytic leukemia Aggressive NK-cell leukemia Adult T-cell lymphoma/leukemia (human T-cell lymphotropic virus type I positive) Extranodal NK/T-cell lymphoma, nasal type Enteropathy type T-cell lymphoma Hepatosplenic gammadelta T-cell lymphoma Subcutaneous panniculitis-like T-cell lymphoma Mycosis fungoides/sezary syndrome Anaplastic large cell lymphoma, T/null-cell, primary cutaneous type Peripheral T-cell lymphoma, not otherwise characterized Angioimmunoblastic T-cell lymphoma Anaplastic large cell lymphoma, T/null-cell, primary systemic type
10 B-Cell Lymphoma Precursor lymphoblastic lymphoma/leukemia Mature Small lymphocytic lymphoma/leukemia Lymphoplasmacytic lymphoma Marginal Zone Lymphoma Follicular lymphoma Mantle cell lymphoma Diffuse large B cell Burkitt s lymphoma Hairy cell leukemia Plasma cell myeloma
11 T-Cell Lymphoma Precursor lymphoblastic lymphoma/leukemia Mature Peripheral T (unspecified) T-cell large granular lymphocytic leukaemia NK leukaemia Anaplastic large cell T/null Cutaneous anaplastic large cell T/null Mycosis Fungoides/Sezary syndrome Adult T-cell lymphoma/leukemia HTLV-1 + Enteropathy-type intestinal Hepatosplenic gamma delta Angioimmunoblastic
12 Non-Hodgkin lymphoma Incidence Diffuse large B-cell lymphoma Follicular NHL Other NHL
13 Pillars of WHO/REAL Classification Cell of origin Cell morphology Immunophenotyping Genotyping Clinical picture Abandon the use of indolent aggressive highly aggressive
14 Prognostic Indicators Histopathologic Type Grades within subtypes e.g. follicular lymphoma Variants within subtypes e.g. Blastoid mantle cell Biology Proliferation fraction Oncogenes, tumor suppressor genes, MDR Clinical Parameters Stage and bulk of disease International prognostic index
15 WHO Classification Indolent Aggressive Very Aggressive CLL/SLL Lymphoplasmacytoid/WM HCL Splenic marginal zone lymphoma Marginal zone lymphoma Extranodal (MALT) Nodal Follicular NHL (grade I-II) PLL Plasmacytoma/ multiple myeloma Mantle cell NHL Follicular NHL (grade III) DLBCL High-grade B-cell lymphoma/burkitt s-like PrecursorBlymphoblastic lymphoma/leukemia Burkitt s lymphoma/ B-cell acute leukemia Plasma cell leukemia
16 Category Survival of untreated patients Curability To treat or not to treat Non- Hodgkin lymphoma Indolent Years Generally not curable Aggressive Months Curable in some Generally defer Rx if asymptomatic Treat Very aggressive Weeks Curable in some Treat Hodgkin lymphoma All types Variable months to years Curable in most Treat
17 Risk factors for NHL Immune suppression Inherited immunodeficiencies organ transplant (cyclosporine) AIDS increasing age DNA repair defects ataxia telangiectasia xeroderma pigmentosum
18 Risk factors for NHL Chronic inflammation and antigenic stimulation Helicobacter pylori inflammation, stomach Chlamydia psittaci inflammation, ocular adnexal tissues Sjögren s syndrome Viral causes EBV and Burkitt s lymphoma HTLV-I and T cell leukemia-lymphoma Hepatitis C and SLVL
19 Clinical Features Variable severity: asymptomatic to extremely ill time course: evolution over weeks, months, or years Systemic manifestations (B symptoms) fever, night sweats, weight loss, anorexia, pruritis Local manifestations lymphadenopathy, splenomegaly most common, any tissue potentially can be infiltrated Cytopenias
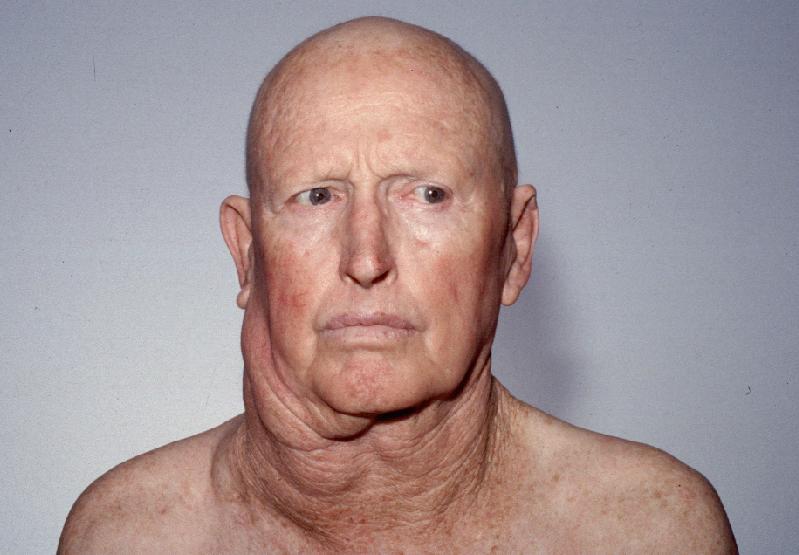
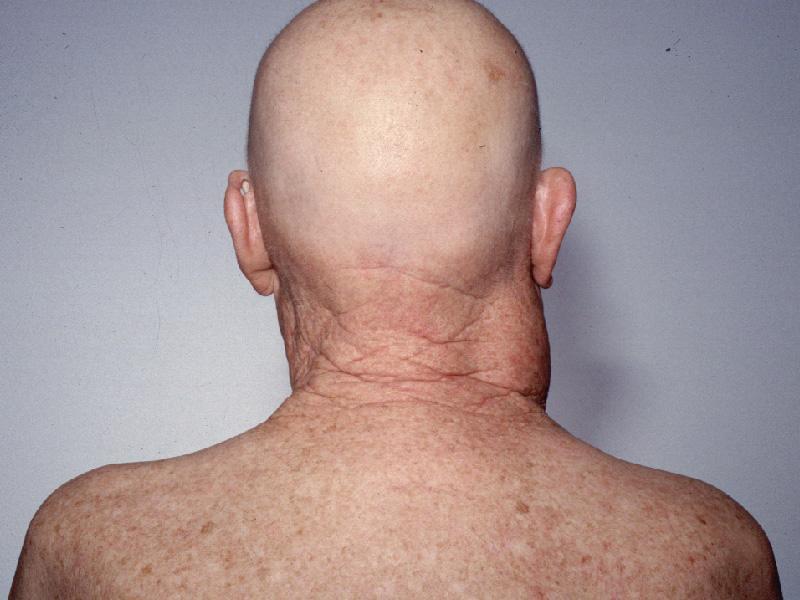
20
21
22 Clinical Features Extranodal primary - more common in high-grade lymphoma. Lymphadenopathy may fluctuate or spontaneously remit, especially in low-grade lymphomas. B symptoms more common in high-grade lymphomas. Haematogenous spread of disease, with no predictable pattern.
23 Other complications of lymphoma bone marrow failure (infiltration) CNS infiltration immune hemolysis or thrombocytopenia neutropenia in LGL leukaemias immunosuppression eg Igs (chronic LPDs), T cell (Hodgkin s or post fludarabine) compression of structures (eg spinal cord, ureters) by bulky disease pleural/pericardial effusions, ascites
24 Types of Lymphoma Indolent (low grade) Life expectancy in years, untreated 85-90% present in Stage III or IV Incurable (except? by allogenic SCT) Intermediate eg Mantle cell NHL Aggressive (high grade) Life expectancy in weeks, untreated Potentially curable
25 Epidemiology Indolent lymphomas are rare in young people and increase in incidence with age. High grade lymphoma is less age related, and is among most common cancers affecting the young. Burkitt s and lymphoblastic lymphoma are common in adolescents. AIDS patients develop aggressive, high grade lymphomas (Burkitt s, Burkitt s -like).
26 Diagnosis of NHL Excisional biopsy needed to show nodal architecture (follicular vs diffuse). Immunophenotyping - immunohistochemistry of tissue sections) - flow cytometry (blood / BM / biopsy) Cytogenetics (inlcuding FISH, molecular studies) Ig / TCR gene rearrangement studies (clonality)
27 Mantle Cell Lymphoma Pax-5 t(9;14) B-CLL Small Lymphocytic p53? Bcl-1 t(11;14) Lymphoplasmacytic CD5- B Cells CD5+ B Cells Mantle Zone Germinal Center Marginal Zone Bcl-2 t(14;18) Follicular Lymphoma Bcl-6 t(2;3)? p53, c-myc, EBV t(8;14) t(8;22) t(2;8) p53 Diffuse Large Cell Lymphoma Burkitt s Lymphoma Richter s Syndrome Bcl-10 t(1;14) Marginal Zone Lymphoma (MALT) Molecular pathogenesis of B-cell lymphomas
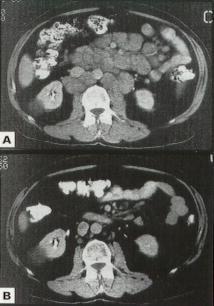
28 Staging Workup Requires CT scans of chest, abdomen and pelvis Bone marrow biopsy and aspirate (Lumbar puncture) eg AIDS lymphoma lymphoblastic lymphoma High grade lymphoma with positive marrow
29 Staging of lymphoma (Ann Arbor) Stage I Stage II Stage III Stage IV A: absence of B symptoms B: fever, night sweats, weight loss E: extranodal
30 International Prognostic Index (IPI) Patients of all ages Risk factors Age >60 years Performance status (PS) 2 4 Lactate dehydrogenase (LDH) level Elevated Extranodal involvement >1 site Stage (Ann Arbor) III IV Patients 60 years (age-adjusted) PS 2 4 LDH Elevated Stage III IV
31 Patients (%) Diffuse Large B-Cell Lymphoma (DLCL): OS IPI IPI P<0.001 IPI Year
32 Strategies for Improving Outcome for Aggressive NHL Monoclonal antibodies (MoAbs) Rituximab (anti-cd20) Combination with chemotherapy Dose intensification High-dose chemotherapy/asct Growth factor incorporation
33 Treatment for advanced indolent NHLs Deferred therapy Single alkylating agent Radiation therapy Combination chemotherapy Biological therapy MoAbs IFN Transplant autologous allogenic Purine analogues
34 MoAbs for Lymphoid malignancies MoAb Antigen Type Lymphoma rituximab CD20 Chimeric B cells epratuzumab CD22 Humanized B cells CD30 Humanized anaplastic / Hodgkin CD25 Humanized adult T-cell leukaemia campath CD52 Humanized CLL, T-PLL
35 Proposed Mechanisms of Action for MoAbs Immune Antibody-dependent cell-mediated cytotoxicity (ADCC) Complement-dependent cytotoxicity (CDC) Apoptosis +/- radioactive labels (eg Iodine, Yttrium)
36 Immunophenotyping Differentiation of normal and malignant haematological populations Uses antibody recognition of surface / intracellular antigens Important for - diagnosis / prognostic evaluation - monitoring treatment response (MRD) - identification of suitable targets for antibody therapy Flow cytometry v Immunohistochemistry of tissue sections
37 CD20 Expression in B-Cell Malignancies Hairy cell DLBCL Burkitt s lymphoma Marginal zone Follicular LP/Waldenström s Mantle cell CLL/PLL CLL Mean channel fluorescence
38 Immunophenotyping Flow cytometry Disadvantages (compared to immunohistochemistry) No visualisation of tissue architecture Poor yield of cells from sclerotic and some packed samples Misses rare neoplastic cells eg Hodgkins Sampling differences in patchy neoplastic infiltrates
39 Immunophenotyping Diagnosis Lineage classification myeloid v lymphoid (B or T or NK) Maturation classification
40 Immunophenotyping B cell LPD Light chain restriction (clonality) Aberrant pattern of antigens compared with normal subsets T cell LPD Subset restriction eg CD4 or CD8 ( but need TCR gene clonality) Aberrant pattern of antigens compared with normal subsets
41 Lymphoproliferative Panel Tube FITC PE PERCP/APC 1 IgG control IgG control IgG control 2 CD7 CD56 CD3 3 CD4 CD8 CD3 4 kappa lambda CD19APC 5 CD20 CD5 CD19APC 6 TCRgammadelta CD2 CD3 7 CD79b CD23 CD19APC 8 CD19 CD38 CD45 9 CD10 CD19 CD34 10 CD103 CD22 CD19APC
42 Notable Subtypes of Lymphoma
43 Follicular lymphoma most common type of indolent lymphoma usually widespread at presentation not curable (some exceptions) cell of origin: germinal center B-cell - centrocytes / centroblasts - expression of CD10 - IgV mutations (and signs of ongoing mutations) - BUT maintain high BCL-2 [t(14;18)]
44 Mantle cell NHL Intermediate usually widespread at presentation 20-30% longterm survival cell of origin: resemble follicle mantle cells (mature naïve B cells) - IgV either not mutated (90% of cases) or only very few mutations - positive for CD5 (like CLL) - but lack CD23 (unlike CLL) - t(11;14) - overexpression of cyclin D1
45 Lymphoplasmacytoid /Waldenstrom s Low grade Spleen, bone marrow, lymph nodes IgM paraprotein - hyperviscosity symptoms (10-30% of patients) - autoantibody or cryoglobulin activity cell of origin: may originate from B cells that have bypassed germinal centre - IgVH restricted, somatically mutated, predominantly CD27neg, IgM+IgD+ CD10neg CD5neg
46 Marginal zone lymphomas Usually localised extranodal (30% disseminated) Associated with 1) autoimmune diseases eg Sjorgen s, Hashimoto s 2) infections eg H Pylori - gastric MALT NHL Hep C - SLVL Can transform to DLBCL cell of origin: marginal zone (memory) B cell - IgM (absence of IgD) - typically have mutated IgV genes with ongoing mutations CD10neg CD5neg
47 Hairy cell Leukaemia low grade, rare Splenomegaly, pancytopenia, Hairy cells in spleen red pulp, blood, bone marrow (rarely LAD) Long-term survival with purine analogues Immune dysfunction, includes vasculitis cell of origin:? - has activation markers CD25, CD11c, CD103-40% of HCL express multiple surface Ig isotypes - on-going somatic mutation but lacks other features of germinal centre cells - gene profiling - more related to memory B cells
48 Chronic Lymphocytic Leukaemia /SLL Most prevalent leukaemia (30% of all leukaemias) Variable clinical course asymptomatic for many years v aggressive 5-10% transform to high grade (Richter s) - poor prognosis Hypogammaglobulinaemia Autoimmune cytopenias cell of origin:? - 50% CLLs - unmutated IgVH genes (poor prognosis) - (50% CLLs - mutated IgVH genes (better prognosis) however both types - common gene expression signature (but different from other lymphomas /leukaemias) - CD5+CD23+ weak surface Ig / BCR
49 Diffuse large B-cell lymphoma (DLBCL) most common type of aggressive lymphoma usually symptomatic extranodal involvement is common curable in ~ 40% cell of origin: - immunophenotypic and genetic features of B cells and B cell subsets but often incomplete / aberrant
50 AIDS Lymphoma Aggressive lymphomas of B cell origin. risk in HIV+ despite HAART Burkitt s, Burkitt s-like, and DLBCL. Primary CNS lymphoma/ Primary Effusion lymphoma Hodgkins Treatment often limited by immunocompromised status eg rituximab benefit offset by infections. Prognosis improved with HAART therapy.
51 Mycosis Fungoides / Sezary s Malignancy of helper T cells (Th2 response) CD4+ often CD7neg (CD25neg) Affinity for skin. Can be treated with electron beam therapy, PUVA, retinoids, IFN Sezary s when systemic (blood, lymph nodes)


52
53 Hodgkin lymphoma Lymphocyte predominant - B cell neoplasm (CD20+) with features of germinal centre origin (rearranged Ig, somatic mutations) Classical Hodgkin s neoplastic cells rearranged, mutated Ig genes no or little B cell immunphenotype, gained CD30, CD15 Reed-Sternberg cells (or RS variants) in the affected tissues most cells in affected lymph node are polyclonal reactive lymphoid cells, not neoplastic cells


")
54 RS cell and variants classic RS cell lacunar cell popcorn cell (mixed cellularity) (nodular sclerosis) (lymphocyte predominance)
55 A possible model of pathogenesis transforming event(s) loss of apoptosis EBV? germinal centre B cell RS cell cytokines inflammatory response
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
WHO Classification. B-cell chronic lymphocytic leukemia/small T-cell granular lymphocytic leukemia
 Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Lymphatic system component
 Introduction Lymphatic system component Statistics Overview Lymphoma Non Hodgkin s Lymphoma Non- Hodgkin's is a type of cancer that originates in the lymphatic system. It is estimated to be the sixth most
Introduction Lymphatic system component Statistics Overview Lymphoma Non Hodgkin s Lymphoma Non- Hodgkin's is a type of cancer that originates in the lymphatic system. It is estimated to be the sixth most
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Small B-cell (Histologically Low Grade) Lymphoma
 Lymphoma") Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
Classifications of lymphomas
 Classifications of lymphomas Lukes and Collins Kiel classification Working formulation REAL classification (1994) WHO classification (2000) WHO CLASSIFICATIONF OF NEOPLASMS HAEMATOPETIC AND LYMPHOID TISSUES
Classifications of lymphomas Lukes and Collins Kiel classification Working formulation REAL classification (1994) WHO classification (2000) WHO CLASSIFICATIONF OF NEOPLASMS HAEMATOPETIC AND LYMPHOID TISSUES
Lymphoma: The Basics. Dr. Douglas Stewart
 Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
LYMPHOMAS an overview of some subtypes of NHLs
 One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
The Lymphomas. An overview..
 The Lymphomas An overview.. Peter Anglin MD, FRCPC, MBA Stronach Regional Cancer Centre Newmarket, ON The lymphomas are an important part of the history of medicine 1666 Magpighi publishes first recorded
The Lymphomas An overview.. Peter Anglin MD, FRCPC, MBA Stronach Regional Cancer Centre Newmarket, ON The lymphomas are an important part of the history of medicine 1666 Magpighi publishes first recorded
FOLLICULARITY in LYMPHOMA
 FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
Immunopathology of Lymphoma
 Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
The spectrum of flow cytometry of the bone marrow
 The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
Clinical Policy: Bendamustine (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307
 Reference Number: PA.CP.PHAR.307") Clinical Policy: (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that
Clinical Policy: (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that
2010 Hematopoietic and Lymphoid ICD-O Codes - Alphabetical List THIS TABLE REPLACES ALL ICD-O-3 Codes
 Acute basophilic leukemia 9870/3 Acute biphenotypic leukemia [OBS] 9805/3 Acute erythroid leukemia 9840/3 Acute megakaryoblastic leukemia 9910/3 Acute monoblastic and monocytic leukemia 9891/3 Acute myeloid
Acute basophilic leukemia 9870/3 Acute biphenotypic leukemia [OBS] 9805/3 Acute erythroid leukemia 9840/3 Acute megakaryoblastic leukemia 9910/3 Acute monoblastic and monocytic leukemia 9891/3 Acute myeloid
2012 Hematopoietic and Lymphoid ICD-O Codes - Numerical List THIS TABLE REPLACES ALL ICD-O-3 Codes
 Malignant lymphoma, NOS 9590/3 Non-Hodgkin lymphoma, NOS 9591/3 B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma 9596/3 Primary
Malignant lymphoma, NOS 9590/3 Non-Hodgkin lymphoma, NOS 9591/3 B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma 9596/3 Primary
Hepatic Lymphoma Diagnosis An Algorithmic Approach
 Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Non-Hodgkin Lymphoma. Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract.
 Non-Hodgkin Lymphoma Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract. Protocol revision date: January 2005 No AJCC/UICC staging system Procedures Cytology
Non-Hodgkin Lymphoma Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract. Protocol revision date: January 2005 No AJCC/UICC staging system Procedures Cytology
During past decades, because of the lack of knowledge
 Staging and Classification of Lymphoma Ping Lu, MD In 2004, new cases of non-hodgkin s in the United States were estimated at 54,370, representing 4% of all cancers and resulting 4% of all cancer deaths,
Staging and Classification of Lymphoma Ping Lu, MD In 2004, new cases of non-hodgkin s in the United States were estimated at 54,370, representing 4% of all cancers and resulting 4% of all cancer deaths,
88-year-old Female with Lymphadenopathy. Faizi Ali, MD
 88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
Harmesh Naik, MD. GME Presentation to Family Practice Residents October 16, 2013.
 Harmesh Naik, MD. GME Presentation to Family Practice Residents October 16, 2013. Lymphoma: Lympho-proliferative disorders arising from lymphocytes Heterogeneous group of disorders Differing patterns of
Harmesh Naik, MD. GME Presentation to Family Practice Residents October 16, 2013. Lymphoma: Lympho-proliferative disorders arising from lymphocytes Heterogeneous group of disorders Differing patterns of
Bone Marrow. Procedures Blood Film Aspirate, Cell Block Trephine Biopsy, Touch Imprint
 Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Indolent Lymphomas. Dr. Melissa Toupin The Ottawa Hospital
 Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Parts 2 and 3
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Parts 2 and 3 NEOPLASTIC LYMPHOID DISEASES Introduction o The bone marrow is the source of all cells in the
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Parts 2 and 3 NEOPLASTIC LYMPHOID DISEASES Introduction o The bone marrow is the source of all cells in the
Indolent Lymphomas: Current. Dr. Laurie Sehn
 Indolent Lymphomas: Current Dr. Laurie Sehn Why does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with current standard
Indolent Lymphomas: Current Dr. Laurie Sehn Why does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with current standard
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU
 Rex K.H. Au-Yeung Department of Pathology, HKU") Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Combinations of morphology codes of haematological malignancies (HM) referring to the same tumour or to a potential transformation
 referring to the same tumour or to a potential transformation") Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
Non-Hodgkin lymphoma
 Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Pathology of the indolent B-cell lymphomas Elias Campo
 Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
Pathology #07. Hussein Al-Sa di. Dr. Sohaib Al-Khatib. Mature B-Cell Neoplasm. 0 P a g e
 Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Change Summary - Form 2018 (R3) 1 of 12
 1 of 12") Summary - Form 2018 (R3) 1 of 12 Form Question Number (r3) Type Description New Text Previous Text Today's date was removed 2018 N/A Today's Date Removed from Key Fields 2018 N/A HCT Type 2018 N/A Product
Summary - Form 2018 (R3) 1 of 12 Form Question Number (r3) Type Description New Text Previous Text Today's date was removed 2018 N/A Today's Date Removed from Key Fields 2018 N/A HCT Type 2018 N/A Product
Non-Hodgkin s Lymphomas Version
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
Integrated Hematopathology. Morphology and FCI with IHC
 Integrated Hematopathology Morphology and FCI with IHC FrontMatter.indd i 9/6/2009 9:30:12 PM FrontMatter.indd ii 9/6/2009 9:30:18 PM Integrated Hematopathology Morphology and FCI with IHC Cherie H Dunphy,
Integrated Hematopathology Morphology and FCI with IHC FrontMatter.indd i 9/6/2009 9:30:12 PM FrontMatter.indd ii 9/6/2009 9:30:18 PM Integrated Hematopathology Morphology and FCI with IHC Cherie H Dunphy,
Contents. vii. Preface... Acknowledgments... v xiii
 Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
HAEMATOLOGICAL MALIGNANCY
 HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
Common Problem Areas. WHO Classification. Defines separate diseases (entities) with their CLINICAL AGGRESSIVENESS LOW GRADE / HIGH GRADE
 with their CLINICAL AGGRESSIVENESS LOW GRADE / HIGH GRADE") WHO Classification Defines separate diseases (entities) with their CLINICAL AGGRESSIVENESS REVIEW OF MOST COMMON LYMPHOMA ENTITIES Dr Stefan Dojcinov LOW GRADE / HIGH GRADE (June 2014) The Non-Hodgkin
WHO Classification Defines separate diseases (entities) with their CLINICAL AGGRESSIVENESS REVIEW OF MOST COMMON LYMPHOMA ENTITIES Dr Stefan Dojcinov LOW GRADE / HIGH GRADE (June 2014) The Non-Hodgkin
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
LEUKAEMIA and LYMPHOMA. Dr Mubarak Abdelrahman Assistant Professor Jazan University
 LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
Patterns of Lymphoid Neoplasia in Peripheral Blood. Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure
 Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Aggressive Lymphomas - Current. Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre
 Aggressive Lymphomas - Current Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre Conflicts of interest I have no conflicts of interest to declare Outline What does aggressive lymphoma
Aggressive Lymphomas - Current Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre Conflicts of interest I have no conflicts of interest to declare Outline What does aggressive lymphoma
Clinical Policy: Bendamustine (Bendeka, Treanda) Reference Number: CP.PHAR.307
 Reference Number: CP.PHAR.307") Clinical Policy: (Bendeka, Treanda) Reference Number: CP.PHAR.307 Effective Date: 02/17 Last Review Date: 02/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Bendeka, Treanda) Reference Number: CP.PHAR.307 Effective Date: 02/17 Last Review Date: 02/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important
WBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
Flow cytometric analysis of B-cell lymphoproliferative disorders
 Flow cytometric analysis of B-cell lymphoproliferative disorders David M. Dorfman, M.D., Ph.D. Department of Pathology Brigham and Women s Hospital and Harvard Medical School Boston, MA Objectives Review
Flow cytometric analysis of B-cell lymphoproliferative disorders David M. Dorfman, M.D., Ph.D. Department of Pathology Brigham and Women s Hospital and Harvard Medical School Boston, MA Objectives Review
Pathology of Hematopoietic and Lymphoid tissue
 Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies
 Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Diagnosis of lymphoid neoplasms has been
 Iranian Journal of Pathology (2007)2 (1), 1-61 Review Article Mehdi Nassiri Dep. of Pathology, University of Miami Miller School of Medicine, Miami, USA Abstract Correct diagnosis and classification of
Iranian Journal of Pathology (2007)2 (1), 1-61 Review Article Mehdi Nassiri Dep. of Pathology, University of Miami Miller School of Medicine, Miami, USA Abstract Correct diagnosis and classification of
Plasma cell myeloma (multiple myeloma)
") Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
MANAGEMENT OF LYMPHOMAS
 MANAGEMENT OF LYMPHOMAS Challenges & Recommendations F. Chite Asirwa, MD. Internal Medicine Physician Medical Oncologist & Hematologist Director-AMPATH Oncology & Hematology @Kenya Physicians Association
MANAGEMENT OF LYMPHOMAS Challenges & Recommendations F. Chite Asirwa, MD. Internal Medicine Physician Medical Oncologist & Hematologist Director-AMPATH Oncology & Hematology @Kenya Physicians Association
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
Aggressive B-Cell Lymphomas
 Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Understanding your diagnosis. Dr Graham Collins Consultant Haemtologist Oxford University Hospitals
 Understanding your diagnosis Dr Graham Collins Consultant Haemtologist Oxford University Hospitals Common questions I get asked What is lymphoma? What subtype do I have and what does that mean? What are
Understanding your diagnosis Dr Graham Collins Consultant Haemtologist Oxford University Hospitals Common questions I get asked What is lymphoma? What subtype do I have and what does that mean? What are
Many of the hematolymphoid disorders are derived
 REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
Corporate Medical Policy
 Corporate Medical Policy Hematopoietic Stem-Cell Transplant for Non-Hodgkin Lymphomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplant_for_non_hodgkin_lymphomas
Corporate Medical Policy Hematopoietic Stem-Cell Transplant for Non-Hodgkin Lymphomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplant_for_non_hodgkin_lymphomas
Immunohistochemical classification of haematolymphoid tumours. Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital
 Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
Pathology of Hematopoietic and Lymphoid tissue
 CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
5000 International Clinical Cytometry Society: Practical Flow Cytometry in Hematopathology A Case-Based Approach
 5000 International Clinical Cytometry Society: Practical Flow Cytometry in Hematopathology A Case-Based Approach Joseph A DiGiuseppe, MD, PhD Hartford Hospital Disclosures In the past 12 months, I have
5000 International Clinical Cytometry Society: Practical Flow Cytometry in Hematopathology A Case-Based Approach Joseph A DiGiuseppe, MD, PhD Hartford Hospital Disclosures In the past 12 months, I have
Prepared by: Dr.Mansour Al-Yazji
 C L L CLL Prepared by: Abd El-Hakeem Abd El-Rahman Abu Naser Ahmed Khamis Abu Warda Ahmed Mohammed Abu Ghaben Bassel Ziad Abu Warda Nedal Mostafa El-Nahhal Dr.Mansour Al-Yazji LEUKEMIA Leukemia is a form
C L L CLL Prepared by: Abd El-Hakeem Abd El-Rahman Abu Naser Ahmed Khamis Abu Warda Ahmed Mohammed Abu Ghaben Bassel Ziad Abu Warda Nedal Mostafa El-Nahhal Dr.Mansour Al-Yazji LEUKEMIA Leukemia is a form
accumulation the blood, marrow, lymph nodes, and spleen.
 Chronic Lymphocytic Leukemia accumulation of mature-appearing appearing lymphocytes in the blood, marrow, lymph nodes, and spleen. CLL cells are: monoclonal l B lymphocytes that express CD19. CD5, and
Chronic Lymphocytic Leukemia accumulation of mature-appearing appearing lymphocytes in the blood, marrow, lymph nodes, and spleen. CLL cells are: monoclonal l B lymphocytes that express CD19. CD5, and
Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo
 Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas NAIVE -B LYMPHOCYTE MEMORY CELL CLL MCL FL MZL Small cell size Low proliferation
Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas NAIVE -B LYMPHOCYTE MEMORY CELL CLL MCL FL MZL Small cell size Low proliferation
Neoplastic proliferation arising from white blood cells. Introductory remarks. Classification
 Neoplastic proliferation arising from white blood cells Lymphoproliferative and myeloproliferative diseases and syndromes Oliver Rácz, 2012-2017 1 Introductory remarks Leukemia and lymphoma are old descriptive
Neoplastic proliferation arising from white blood cells Lymphoproliferative and myeloproliferative diseases and syndromes Oliver Rácz, 2012-2017 1 Introductory remarks Leukemia and lymphoma are old descriptive
3/23/2017. Disclosure of Relevant Financial Relationships. Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?!
 Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?! Judith A. Ferry Massachusetts General Hospital Disclosure of Relevant Financial Relationships USCAP requires that all
Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?! Judith A. Ferry Massachusetts General Hospital Disclosure of Relevant Financial Relationships USCAP requires that all
Lymphoma and Myeloma Kris3ne Kra4s, M.D.
 Lymphoma and Myeloma Kris3ne Kra4s, M.D. Hematologic Malignancies Leukemia Malignancy of hematopoie3c cells Starts in bone marrow, can spread to blood, nodes Myeloid or lymphoid Acute or chronic Lymphoma
Lymphoma and Myeloma Kris3ne Kra4s, M.D. Hematologic Malignancies Leukemia Malignancy of hematopoie3c cells Starts in bone marrow, can spread to blood, nodes Myeloid or lymphoid Acute or chronic Lymphoma
UNIVERSITÀ DI PISA FACOLTÀ DI MEDICINA E CHIRURGIA TESI DI LAUREA
 UNIVERSITÀ DI PISA FACOLTÀ DI MEDICINA E CHIRURGIA Corso di Laurea Specialistica in Medicina e Chirurgia TESI DI LAUREA How to treat Splenic Marginal Zone Lymphoma (SMZL) in patients unfit for surgery
UNIVERSITÀ DI PISA FACOLTÀ DI MEDICINA E CHIRURGIA Corso di Laurea Specialistica in Medicina e Chirurgia TESI DI LAUREA How to treat Splenic Marginal Zone Lymphoma (SMZL) in patients unfit for surgery
GENETIC MARKERS IN LYMPHOMA a practical overview. P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute
 GENETIC MARKERS IN LYMPHOMA a practical overview P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute B and T cell monoclonalities Rearrangement of immunoglobin and TCR genes may help
GENETIC MARKERS IN LYMPHOMA a practical overview P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute B and T cell monoclonalities Rearrangement of immunoglobin and TCR genes may help
Case 3. Ann T. Moriarty,MD
 Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
T CELL LYMPHOMA ANALYSIS
 T CELL LYMPHOMA ANALYSIS Charles Goolsby, Ph.D. Floyd E. Patterson Research Professor of Pathology Northwestern Feinberg School of Medicine c-goolsby@northwestern.edu 1 T CELL LYMPHOMA ANALYSIS Diverse
T CELL LYMPHOMA ANALYSIS Charles Goolsby, Ph.D. Floyd E. Patterson Research Professor of Pathology Northwestern Feinberg School of Medicine c-goolsby@northwestern.edu 1 T CELL LYMPHOMA ANALYSIS Diverse
Methods used to diagnose lymphomas
 Institut für Pathologie Institut für Pathologie Methods used to diagnose lymphomas Prof. Dr.Med. Leticia Quintanilla-Fend Molecular techniques NGS histology Cytology AS-PCR Sanger seq. MYC Immunohistochemistry
Institut für Pathologie Institut für Pathologie Methods used to diagnose lymphomas Prof. Dr.Med. Leticia Quintanilla-Fend Molecular techniques NGS histology Cytology AS-PCR Sanger seq. MYC Immunohistochemistry
Lymphoma Update: Lymphoma Update: What s Likely to be New in the New WHO. Patrick Treseler, MD, PhD University of California San Francisco
 Lymphoma Update: What s Likely to be New in the New WHO Blood 127:2375; 2016 Patrick Treseler, MD, PhD University of California San Francisco Lymphoma Update: What IS New in the New WHO! Patrick Treseler,
Lymphoma Update: What s Likely to be New in the New WHO Blood 127:2375; 2016 Patrick Treseler, MD, PhD University of California San Francisco Lymphoma Update: What IS New in the New WHO! Patrick Treseler,
Aggressive B-cell Lymphoma 2013
 Aggressive B-cell Lymphoma 2013 Diffuse Large B-Cell Lymphoma Burkitt Lymphoblastic lymphoma Gray zone Intermediate DLBCL/HL Intermediate BL/DLBCL Diffuse Large B-cell lymphoma Common morphology: diffuse
Aggressive B-cell Lymphoma 2013 Diffuse Large B-Cell Lymphoma Burkitt Lymphoblastic lymphoma Gray zone Intermediate DLBCL/HL Intermediate BL/DLBCL Diffuse Large B-cell lymphoma Common morphology: diffuse
Lymphoid Neoplasms Associated With IgM Paraprotein A Study of 382 Patients
 Hematopathology / LYMPHOMAS WITH IGM PARAPROTEIN Lymphoid Neoplasms Associated With IgM Paraprotein A Study of 382 Patients Pei Lin, MD, 1 Suyang Hao, MD, 1* Beverly C. Handy, MD, 2 Carlos E. Bueso-Ramos,
Hematopathology / LYMPHOMAS WITH IGM PARAPROTEIN Lymphoid Neoplasms Associated With IgM Paraprotein A Study of 382 Patients Pei Lin, MD, 1 Suyang Hao, MD, 1* Beverly C. Handy, MD, 2 Carlos E. Bueso-Ramos,
LYMPHOID MALIGNANCIES & NEW IDEAS
 LYMPHOID MALIGNANCIES & NEW IDEAS LEUKEMIAS AND LYMPHOMAS. Malignancies of B, T, or NK cells are lymphoid; of any other hematopoietic cells, myeloid. We ll only discuss lymphoid malignancies here, and
LYMPHOID MALIGNANCIES & NEW IDEAS LEUKEMIAS AND LYMPHOMAS. Malignancies of B, T, or NK cells are lymphoid; of any other hematopoietic cells, myeloid. We ll only discuss lymphoid malignancies here, and
A Practical Guide To Diagnose B-Cell Lymphomas on FNAs. Nancy P. Caraway, M.D.
 A Practical Guide To Diagnose B-Cell Lymphomas on FNAs Nancy P. Caraway, M.D. Major Factors Impacting Dx Lymphomas on Small Bxs Classification systems Immunophenotyping by multiprobe flow cytometry and
A Practical Guide To Diagnose B-Cell Lymphomas on FNAs Nancy P. Caraway, M.D. Major Factors Impacting Dx Lymphomas on Small Bxs Classification systems Immunophenotyping by multiprobe flow cytometry and
Aggressive B-cell Lymphomas
 Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
2012 by American Society of Hematology
 2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
Classification of Hematologic Malignancies. Patricia Aoun MD MPH
 Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Osteosclerotic Myeloma (POEMS Syndrome)
") Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
Michi Shinohara MD Associate Professor University of Washington/Seattle Cancer Care Alliance Dermatology, Dermatopathology
 Michi Shinohara MD Associate Professor University of Washington/Seattle Cancer Care Alliance Dermatology, Dermatopathology Agenda Overview of cutaneous T and B- cell lymphomas Diagnosis, Staging, Prognosis
Michi Shinohara MD Associate Professor University of Washington/Seattle Cancer Care Alliance Dermatology, Dermatopathology Agenda Overview of cutaneous T and B- cell lymphomas Diagnosis, Staging, Prognosis
HIGH GRADE B-CELL LYMPHOMA DAVID NOLTE, MD (PGY-2) HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD
 HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD") HIGH GRADE B-CELL LYMPHOMA DAVID NOLTE, MD (PGY-2) HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD OUTLINE High grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements Patient presentation 2008/2016
HIGH GRADE B-CELL LYMPHOMA DAVID NOLTE, MD (PGY-2) HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD OUTLINE High grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements Patient presentation 2008/2016
Corrigenda. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run
: corrections made in second print run") Corrigenda WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run In addition to corrections of minor typographical errors, corrections
Corrigenda WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run In addition to corrections of minor typographical errors, corrections
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113)
") Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
Hematologic Malignancies. Anna Schaal, RN, MSN, arnp Norris Cotton Cancer Center Lebanon, New Hampshire
 Hematologic Malignancies Anna Schaal, RN, MSN, arnp Norris Cotton Cancer Center Lebanon, New Hampshire Objectives At the end of the session, the oncology nurse will be able to: Explain the pathophysiology
Hematologic Malignancies Anna Schaal, RN, MSN, arnp Norris Cotton Cancer Center Lebanon, New Hampshire Objectives At the end of the session, the oncology nurse will be able to: Explain the pathophysiology
Lymphoma: What You Need to Know
 Lymphoma: What You Need to Know www.lymphoma.org.au Lymphoma What You Need to Know Whilst Lymphoma Australia (LA) has made every effort to confirm the accuracy of the information contained herein, it makes
Lymphoma: What You Need to Know www.lymphoma.org.au Lymphoma What You Need to Know Whilst Lymphoma Australia (LA) has made every effort to confirm the accuracy of the information contained herein, it makes
Lymphoma 101. Nathalie Johnson, MDPhD. Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University
 Lymphoma 101 Nathalie Johnson, MDPhD Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University Disclosures Consultant and Advisory boards for multiple companies
Lymphoma 101 Nathalie Johnson, MDPhD Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University Disclosures Consultant and Advisory boards for multiple companies
Immunophenotyping of lymphoproliferative disorders: state of the art
 Pathology (December 2005) 37(6), pp. 457 478 PRACTICAL ASPECTS OF DIAGNOSTIC HISTOPATHOLOGY Immunophenotyping of lymphoproliferative disorders: state of the art EMMA J. GUDGIN AND WENDY N. ERBER Haematology
Pathology (December 2005) 37(6), pp. 457 478 PRACTICAL ASPECTS OF DIAGNOSTIC HISTOPATHOLOGY Immunophenotyping of lymphoproliferative disorders: state of the art EMMA J. GUDGIN AND WENDY N. ERBER Haematology
Low grade High grade , immune suppression chronic persistent inflammation viruses B-symptoms
 We've one category for lymphoid neoplasm which is the lymphoma in contrast to that of myeloid which has three categories; acute myeloid leukemias, myeloproliferative & myelodysplastic disorders. Lymphoma
We've one category for lymphoid neoplasm which is the lymphoma in contrast to that of myeloid which has three categories; acute myeloid leukemias, myeloproliferative & myelodysplastic disorders. Lymphoma
C r h ist s op o h p e h r e R. R F l F ow o er e s, s M D, D M S
 1 Christopher R. Flowers, MD, MS Associate Professor of Hematology and Medical Oncology Winship Cancer Institute Emory University School of Medicine Atlanta, Georgia 2 1 Anyone can get blood cancer One
1 Christopher R. Flowers, MD, MS Associate Professor of Hematology and Medical Oncology Winship Cancer Institute Emory University School of Medicine Atlanta, Georgia 2 1 Anyone can get blood cancer One
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas. Original Policy Date
 MP 7.03.13 Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013
MP 7.03.13 Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013
The development of clonality testing for lymphomas in the Bristol Genetics Laboratory. Dr Paula Waits Bristol Genetics Laboratory
 The development of clonality testing for lymphomas in the Bristol Genetics Laboratory Dr Paula Waits Bristol Genetics Laboratory Introduction The majority of lymphoid malignancies belong to the B cell
The development of clonality testing for lymphomas in the Bristol Genetics Laboratory Dr Paula Waits Bristol Genetics Laboratory Introduction The majority of lymphoid malignancies belong to the B cell
Overview of Cutaneous Lymphomas: Diagnosis and Staging. Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology
 Overview of Cutaneous Lymphomas: Diagnosis and Staging Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology Definition of Lymphoma A cancer or malignancy that comes from
Overview of Cutaneous Lymphomas: Diagnosis and Staging Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology Definition of Lymphoma A cancer or malignancy that comes from
WBCs Disorders. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features and
WBCs Disorders Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features and
The patient had a mild splenomegaly but no obvious lymph node enlargement. The consensus phenotype obtained from part one of the exercise was:
 Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
Non-Hodgkin s Lymphoma
 Non-Hodgkin s Lympoma Non-Hodgkin s Lymphomas Janet H. Van Cleave MSN, ACNP-CS, CS, AOCN Acute Care Nurse Practitioner The Mount Sinai Medical Center of New York City Doctoral Student, Yale University
Non-Hodgkin s Lympoma Non-Hodgkin s Lymphomas Janet H. Van Cleave MSN, ACNP-CS, CS, AOCN Acute Care Nurse Practitioner The Mount Sinai Medical Center of New York City Doctoral Student, Yale University
BACKGROUND INFORMATION ON NON-HODGKIN S LYMPHOMA
 BACKGROUND INFORMATION ON NON-HODGKIN S LYMPHOMA General Non-Hodgkin s lymphomas (NHLs) encompass several unique malignant lymphoid disease entities that vary in clinical behavior, morphologic appearance,
BACKGROUND INFORMATION ON NON-HODGKIN S LYMPHOMA General Non-Hodgkin s lymphomas (NHLs) encompass several unique malignant lymphoid disease entities that vary in clinical behavior, morphologic appearance,
Hematology 101. Rachid Baz, M.D. 5/16/2014
 Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More