Anaemia / SCD/ Bleeding disorders in Children
|
|
|
- Clifton Rich
- 6 years ago
- Views:
Transcription
1 Anaemia / SCD/ Bleeding disorders in Children Dr Neil Kennedy Handouts by Steve Graham
2 Learning Outcomes Describe mechanisms of anaemia in Malawian children Discuss important causes of anaemia Describe presentation and Rx of SCD and G6PD in Malawi Identify causes of anaemia from history and FBC/Film Discuss common causes of bleeding diathesis in children Prescribe blood for severe anaemia according to WHO guidelines HANDOUT
3 Mechanisms of Anaemia? Blood Loss Haemolysis Reduced red cell production: Nutrient deficiency Marrow suppression / failure
4 Causes of Anaemia Blood Loss Hookworm Schisto epistaxis Gastritis / Meckels / colitis Haemolysis / consumption Malaria Defective red cell: Membrane: Spherocytosis Enzymes: G6PD Haemoglobin: SCD, Thallassaemia Hypersplenism Reduced Red cell production Nutrient deficiency Iron B12 / Folate PEM Marrow suppression HIV Sepsis Malaria Miliary TB Renal Failure Leukaemia Parvovirus B19
5 Severe Anaemia Mechanisms in Malawian Children Red cell production failure 48%: Bacteraemia HIV Malaria Wasting Vit B12 def Vit A def Haemolysis 21.7%: Malaria G6PD in boys Blood Loss 7.2%: Hookworm Calis et al NEJM 2008;358(9):888-9
6 Severe Anaemia (Hb <5g/dL) Malawian Children Patients (%) Controls (%) Wasting 16 6 Iron Deficiency B12 deficiency Folate deficiency 0 0 Vit A deficiency HIV 13 6 Bacteraemia 15 4 Malaria Hookworm Schistosomiasis G6PD 14 9 Calis et al NEJM 2008;358(9):888-9
7 Severe Anaemia in Malawian Children Malaria major factor Bacteraemia with NTS common Due to dyserythropoeisis Consider antibiotics in febrile anaemic child, even if MPS +ve VIT A + B12 deficiency significant problems G6PD important cause severe anaemia HIV causing severe anaemia associated with high mortality 18 months after presentation with Hb <5g/dL, 65% of the HIV +ve had died, 10.7% of the HIV ve (pre-art study) Hookworm common in all anaemic > 1 year
8 What about Iron? Fe deficiency causing mild anaemia is common (PCV > 20%) and associated with hookworm May contribute to poor school performance Fe supplements reduce anaemia prevalence in community Fe supplements may increase mortality in areas with high malaria / sepsis burdern Iron deficiency may protect against severe anaemia, as?reduces bacteraemia risk Iron should not be given acutely to children with malaria / NTS sepsis / malnutrition Wait for child to recover then give for 3 months
9 Working out the cause of the anaemia Red cell production: Film: Microcytic hypochromic: Fe Macrocytic, hypersegmented neuts: B12 / folate Blasts: Leukaemia Malarial parasites Target cells, fragments, reticulocytes FBC:
 Malaria Heinz bodies (rare) Coombs test: autoimmune Blood loss: History Stool (HWA) urine")
10 Working out the cause of the anaemia Haemolysis / consumption Often enlarged spleen Urobilinogen / jaundice Film: Sickle targets (Thall) Malaria Heinz bodies (rare) Coombs test: autoimmune Blood loss: History Stool (HWA) urine (schisto)
 X linked Usually mild Favism")

11 Haemolytic anaemia G6PD Common in Malawi (10%) X linked Usually mild Favism induced by: ASA, SP, CTX Malaria / infections Diagnosis: Presumptive Enzyme, Heinz bodies
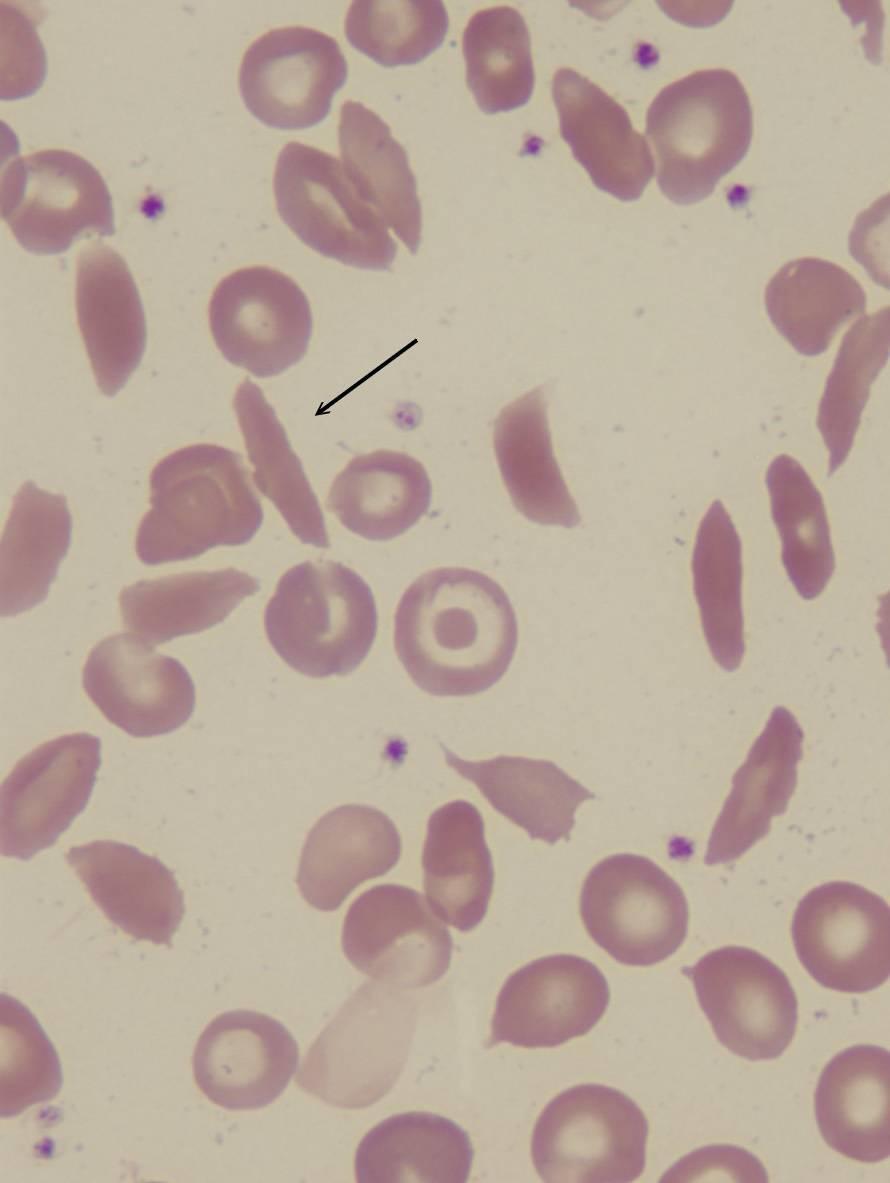
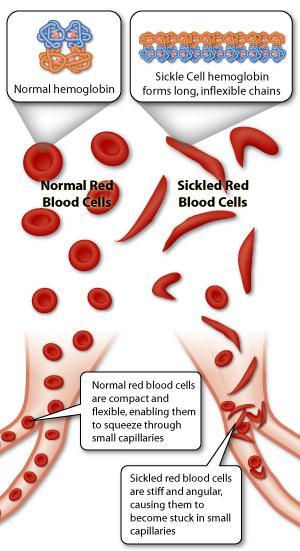
12 Haemolytic Anaemia - SCD Rarer (1.5%) but more significant Autosomal recessive Hb SS Glutamic acid valine substitution in chains HbS = 2 chains, 2 defective chains Low oxygen tension leads to: Polymerisation of HbS chains Distortion of red cell shape (sickle) Distorted red cells cause ischaemia
13
 Stroke")
14 Haemolytic Anaemia - SCD Symptoms > 6/12 Common problems: Hand / foot syndrome Anaemia repeat transfusions Jaundice Infections: Malaria, pneumococcus, NTS Limb / abdo pain Less common: Aplastic crisis (parvovirus) Stroke Diagnosis
15 SCD Treatment Regular: Benzathine prophylaxis / pneumovacc if avail Malaria prophylaxis (ITN / SP) Folic acid Education on treating GE / RTI Monitor Hb, transfuse needed Hydroxyurea Crisis: Analgesia (PCM, ibuprofen, morphine) Fluids ORS / IV
16 Case 1 18 months old girl, weight 10kg Febrile (temp 39.6C) dyspnoeic Hb 3g/dl
17 Case 2 15 months old girl Pallor Hb 4.5g/dl MCV 62 fl
18 Case 3 3 year old boy Persistent diarrhoea Failure to thrive Hepatosplenomegaly Axillary lymphadenopathy Hb 5g/dl MCV 104 fl
19 Case 4 20 months old female child Recurrent upper and lower limit pain Had one episode of jaundice recently Eats poorly Generally irritable unhappy and not thriving Chronically ill-looking, small for age Mild jaundice Swollen hands HB 6g/dl
20 Case 5 10 year old boy General malaise Weakness Bone pain Bruises easily Hb 6 g/dl WCC 45 x10 9 /L Platelets 23 x10 9 /L
21 Case 6 4 year old girl Generalised lymphadenopathy Oropharyngeal candidiasis Recurrent epistaxis Hb 7.5 g/dl WCC 17 Platelets 29

22 WHO treatment chronic anaemia Fe or FeFol daily x 14 days Review at 2/52 Continue Fe / FeFol x 3 months Deworm if > 2years Vit A and B12 deficiency may be more important Hookworm common in under 2s

23 WHO treatment severe anaemia Transfuse if: PCV < 12% or PCV 13-18% and: Clinically severe dehydration Shock Impaired consciousness CCF Deep / laboured breathing Parasitaemia > 10%
24 WHO treatment severe anaemia If NOT malnourished: 10mls/kg packed cells over 3-4 hours or 20mls/kg whole blood Frusemide only if signs of overload If malnourished: 10 mls/kg whole blood FLUID OVERLOAD COMMON give Frusemide
25 Things to think about in a child with Is it really just malaria? Is this the first transfusion? Have they got SCD or G6PD? Have they got HIV? Have they got septicaemia?
26 Bleeding diathesis Coagulation requires: Normal platelets (number and function) Normal clotting factors
27 Platelet disorders Present with mucosal bleeding / purpura Causes include: Infection and platelet destruction DIC Marrow infiltration (leukaemia) ITP / HIV autoimmune thrombocytopenia Hypersplenism Abnormal platelet function von Willebrands
28 Clotting cascade disorders Herdeditary Haemophilia Haem A Factor VIII x linked Spontaneous haemarthroses Rx Cryoprecipitate Acquired Vit K deficiency 1.Decreased absorption fat soluble vits (hepatic failure) 2.Haemorrhagic disease of the newborn Present with GI bleeds, bruising
29 Bleeding diathesis Ix FBC, coagulation screen, culture PT measures EXTRINSIC (PET) hepatic failure, warfarin PTTK measures INTRINSIC heamophilia (factor 8), heparin DIC PT, PTTK and platelets affected
30 Bleeding diathesis Rx Platelet problems: Platelet transfusion if < 20 (not ITP) Consider steroids Immunoglobulin for ITP Clotting factor deficiencies: Vit K for hepatic failure, HD Newborn Factor 8 cryo for haemophilia Fresh Frozen Plasma in emergency
31 Mafumbo ghalipo??
32 Learning Outcomes Describe mechanisms of anaemia in Malawian children Discuss important causes of anaemia Describe presentation and Rx of SCD and G6PD in Malawi Identify causes of anaemia from history and FBC/Film Discuss common causes of bleeding diathesis in children Prescribe blood for severe anaemia according to WHO guidelines HANDOUT
Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust
 Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust Regional Paediatric Specialty Trainees teaching 4 th July 2017 Scope
Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust Regional Paediatric Specialty Trainees teaching 4 th July 2017 Scope
Clinical & Laboratory Assessment
 Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
Anaemia in Pregnancy
 Anaemia in Pregnancy Definition :anaemia is a pathological condition in which the oxygen-carrying capacity of red blood cells is insufficient to meet the body needs. The WHO : haemoglobin concentration
Anaemia in Pregnancy Definition :anaemia is a pathological condition in which the oxygen-carrying capacity of red blood cells is insufficient to meet the body needs. The WHO : haemoglobin concentration
Haemorrhagic Disorders. Dr. Bashar Department of Pathology Mosul Medical College
 Haemorrhagic Disorders Dr. Bashar Department of Pathology Mosul Medical College Hemorrhagic Disorders These include Disorders of platelets. Disorders of blood vessels. Disorders of coagulation & fibrinolysis.
Haemorrhagic Disorders Dr. Bashar Department of Pathology Mosul Medical College Hemorrhagic Disorders These include Disorders of platelets. Disorders of blood vessels. Disorders of coagulation & fibrinolysis.
Interpreting Blood Tests Part 1. Dr Andrew Smith
 Interpreting Blood Tests Part 1 Dr Andrew Smith Outline Part 1 (This Week) Introduction Which Tube!?! FBCs U+Es Part 2 (Next Week): More Electrolytes LFTs Clotting Extras Introduction Bloods are a core
Interpreting Blood Tests Part 1 Dr Andrew Smith Outline Part 1 (This Week) Introduction Which Tube!?! FBCs U+Es Part 2 (Next Week): More Electrolytes LFTs Clotting Extras Introduction Bloods are a core
There are two main causes of a low platelet count
 Thrombocytopenia Thrombocytopenia is a condition in which a person's blood has an unusually low level of platelets Platelets, also called thrombocytes, are found in a person's blood along with red blood
Thrombocytopenia Thrombocytopenia is a condition in which a person's blood has an unusually low level of platelets Platelets, also called thrombocytes, are found in a person's blood along with red blood
Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN
 Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN The student should be able:» To identify the mechanism of homeostasis and the role of vessels, platelets
Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN The student should be able:» To identify the mechanism of homeostasis and the role of vessels, platelets
PCCN Review Hematology
 PCCN Review Hematology Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Anemia Definition reduction in RBC concentration Causes iron deficiency
PCCN Review Hematology Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Anemia Definition reduction in RBC concentration Causes iron deficiency
Sickle Cell Disease. Edward Malters, MD
 Sickle Cell Disease Edward Malters, MD Introduction Vaso-occlusive phenomena and hemolysis are the clinical hallmarks of Sickle Cell Disease (SCD) Inherited disorder due to homozygosity for the abnormal
Sickle Cell Disease Edward Malters, MD Introduction Vaso-occlusive phenomena and hemolysis are the clinical hallmarks of Sickle Cell Disease (SCD) Inherited disorder due to homozygosity for the abnormal
Blood Transfusion. Dr William Dooley
 Blood Transfusion Dr William Dooley Plan Cases Blood groups / Indications Procedure Monitoring / Reactions Cases For following cases: - Would you give them a blood transfusion? - How many units you would
Blood Transfusion Dr William Dooley Plan Cases Blood groups / Indications Procedure Monitoring / Reactions Cases For following cases: - Would you give them a blood transfusion? - How many units you would
Approach to a pale child
 Approach to a pale child Dr. Dafalla Ahmed Babiker Jazan university objectives Definition of anemia Classification and causes Important points in history and physical examination Investigations. Definition
Approach to a pale child Dr. Dafalla Ahmed Babiker Jazan university objectives Definition of anemia Classification and causes Important points in history and physical examination Investigations. Definition
Paediatric Haematology and Oncology. All in One hour! Dr Nigel Coad
 Paediatric Haematology and Oncology All in One hour! Dr Nigel Coad Anaemia Normal Ranges Physiological Anaemia Causes Normal babies, more marked in Prematures Impaired Production Reduced Haematinics (IRON(
Paediatric Haematology and Oncology All in One hour! Dr Nigel Coad Anaemia Normal Ranges Physiological Anaemia Causes Normal babies, more marked in Prematures Impaired Production Reduced Haematinics (IRON(
Hematologic changes in systemic diseases. Chittima Sirijerachai
 Hematologic changes in systemic diseases Chittima Sirijerachai Systemic diseases Infection Renal diseases Liver diseases Connective tissue diseases Malignancy Anemia of chronic disease (ACD) Chronic infections:
Hematologic changes in systemic diseases Chittima Sirijerachai Systemic diseases Infection Renal diseases Liver diseases Connective tissue diseases Malignancy Anemia of chronic disease (ACD) Chronic infections:
Disorders of Blood Cells & Blood Coagulation
 Disorders of Blood Cells & Blood Coagulation HIHIM 409 WBC count RBC count WBC differential Hemoglobin (HGB) Hematocrit (HCT) % of volume occupied by RBCs CBC Red cell indices Mean cell volume (MCV) average
Disorders of Blood Cells & Blood Coagulation HIHIM 409 WBC count RBC count WBC differential Hemoglobin (HGB) Hematocrit (HCT) % of volume occupied by RBCs CBC Red cell indices Mean cell volume (MCV) average
The Child with a Hematologic Alteration
 47 The Child with a Hematologic Alteration HELPFUL HINT Review the anatomy and physiology of the hematologic system in an anatomy and physiology textbook. MATCHING KEY TERMS Match the term with the correct
47 The Child with a Hematologic Alteration HELPFUL HINT Review the anatomy and physiology of the hematologic system in an anatomy and physiology textbook. MATCHING KEY TERMS Match the term with the correct
Candidates must answer ALL questions
 Time allowed: Three hours. Part 1 examination Haematology: First paper Tuesday 22 March 2016 Candidates must answer ALL questions Question 1: General Haematology A 16 year old non-european is referred
Time allowed: Three hours. Part 1 examination Haematology: First paper Tuesday 22 March 2016 Candidates must answer ALL questions Question 1: General Haematology A 16 year old non-european is referred
General Characterisctics
 Anemia General Characterisctics Definition: anemia is a decrease in red blood cells. Happens due to underproduction, increased destruction or loss of red cells. Diagnosis of anemia: Hgb < 135 (men) Hgb
Anemia General Characterisctics Definition: anemia is a decrease in red blood cells. Happens due to underproduction, increased destruction or loss of red cells. Diagnosis of anemia: Hgb < 135 (men) Hgb
Dr Banu Kaya Consultant Haematologist Barts Health NHS Trust Royal London Hospital, London, UK SICKLE CELL AND THALASSAEMIA OVERVIEW
 Dr Banu Kaya Consultant Haematologist Barts Health NHS Trust Royal London Hospital, London, UK SICKLE CELL AND THALASSAEMIA OVERVIEW Objectives Gain awareness of haemoglobinopathy inheritance, pathophysiology
Dr Banu Kaya Consultant Haematologist Barts Health NHS Trust Royal London Hospital, London, UK SICKLE CELL AND THALASSAEMIA OVERVIEW Objectives Gain awareness of haemoglobinopathy inheritance, pathophysiology
PATHOLOGY & PATHOPHYSIOLOGY
 PATHOLOGY & PATHOPHYSIOLOGY DISORDERS OF BLOOD DISORDERS OF BLOOD Disorders of Blood Infections Tumours Nutritional disorders Coagulation disorders Congenital disorders Septicaemia Leukemia Iron deficiency
PATHOLOGY & PATHOPHYSIOLOGY DISORDERS OF BLOOD DISORDERS OF BLOOD Disorders of Blood Infections Tumours Nutritional disorders Coagulation disorders Congenital disorders Septicaemia Leukemia Iron deficiency
DIC. Disseminated intravascular coagulation, is a life threatening pathological process in which clotting factors are abnormally activated.
 Miss. kamlah 1 DIC Disseminated intravascular coagulation, is a life threatening pathological process in which clotting factors are abnormally activated. Resulting in wide spread of clot formation in the
Miss. kamlah 1 DIC Disseminated intravascular coagulation, is a life threatening pathological process in which clotting factors are abnormally activated. Resulting in wide spread of clot formation in the
Rory McCulloch. Specialty Trainee Haematology Royal Devon & Exeter Hospital
 Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
Haematology dilemma s to refer or not to refer?
 Haematology dilemma s to refer or not to refer? NWL Pathology GP Study Day Dr Fatts Chowdhury Consultant Haematologist in Transfusion Medicine NHS Blood and Transplant Senior Honorary Clinical Lecturer
Haematology dilemma s to refer or not to refer? NWL Pathology GP Study Day Dr Fatts Chowdhury Consultant Haematologist in Transfusion Medicine NHS Blood and Transplant Senior Honorary Clinical Lecturer
Blood transfusion. Dr. J. Potgieter Dept. of Haematology NHLS - TAD
 Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
Classification of Anaemia
 Classification of Anaemia Dr Roger Pool Department of Haematology NHLS & University of Pretoria MEASUREMENT OF HAEMATOCRIT The haematocrit ratio (Hct) is the proportion of blood made up of cells - mainly
Classification of Anaemia Dr Roger Pool Department of Haematology NHLS & University of Pretoria MEASUREMENT OF HAEMATOCRIT The haematocrit ratio (Hct) is the proportion of blood made up of cells - mainly
THE KENYA POLYTECHNIC UNIVERSITY COLLEGE
 THE KENYA POLYTECHNIC UNIVERSITY COLLEGE SCHOOL OF HEALTH SCIENCES AND TECHNOLOGY DEPARTMENT OF BIOMEDICAL LABORATORY SCIENCES AND TECHNOLOGY DIPLOMA IN MEDICAL LABORATORY SCIENCES FINAL YEAR EXAMINATION
THE KENYA POLYTECHNIC UNIVERSITY COLLEGE SCHOOL OF HEALTH SCIENCES AND TECHNOLOGY DEPARTMENT OF BIOMEDICAL LABORATORY SCIENCES AND TECHNOLOGY DIPLOMA IN MEDICAL LABORATORY SCIENCES FINAL YEAR EXAMINATION
BLOOD TRANSFUSION. Dr Lumka Ntabeni
 BLOOD TRANSFUSION Dr Lumka Ntabeni Blood transfusion definition SAFE transfer of BLOOD COMPONENTS from a DONOR to a RECEPIENT CONTENT Brief history of blood transfusion How is safety guaranteed? How do
BLOOD TRANSFUSION Dr Lumka Ntabeni Blood transfusion definition SAFE transfer of BLOOD COMPONENTS from a DONOR to a RECEPIENT CONTENT Brief history of blood transfusion How is safety guaranteed? How do
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Symptoms and Signs in Hematology (2)/ 2013
/ 2013") Symptoms and Signs in Hematology (2)/ 2013 Abdallah Abbadi.MD.FRCP Professor of Medicine,Hematology & Oncology University of Jordan & JUH Email: abdalla.awidi@gmail.com Case one: A 24 yr old female complains
Symptoms and Signs in Hematology (2)/ 2013 Abdallah Abbadi.MD.FRCP Professor of Medicine,Hematology & Oncology University of Jordan & JUH Email: abdalla.awidi@gmail.com Case one: A 24 yr old female complains
Evaluation of Anemia. Md. Shafiqul Bari Associate professor (Medicine) SOMC
 SOMC") Evaluation of Anemia Md. Shafiqul Bari Associate professor (Medicine) SOMC Definition Anemia is operationally defined as a reduction in one or more of the major RBC measurements Hemoglobin concentration
Evaluation of Anemia Md. Shafiqul Bari Associate professor (Medicine) SOMC Definition Anemia is operationally defined as a reduction in one or more of the major RBC measurements Hemoglobin concentration
Haemostasis & Coagulation disorders Objectives:
 Haematology Lec. 1 د.ميسم مؤيد علوش Haemostasis & Coagulation disorders Objectives: - Define haemostasis and what are the major components involved in haemostasis? - How to assess the coagulation status?
Haematology Lec. 1 د.ميسم مؤيد علوش Haemostasis & Coagulation disorders Objectives: - Define haemostasis and what are the major components involved in haemostasis? - How to assess the coagulation status?
Bleeding and Thrombotic Disorders. Kristine Krafts, M.D.
 Bleeding and Thrombotic Disorders Kristine Krafts, M.D. Bleeding and Thrombotic Disorders Bleeding disorders von Willebrand disease Hemophilia A and B DIC TTP/HUS ITP Thrombotic disorders Factor V Leiden
Bleeding and Thrombotic Disorders Kristine Krafts, M.D. Bleeding and Thrombotic Disorders Bleeding disorders von Willebrand disease Hemophilia A and B DIC TTP/HUS ITP Thrombotic disorders Factor V Leiden
Hematology Revision. By Dr.AboRashad . Mob
 1 1- Hb A2 is consisting of: a) 3 ά chains and 2 γ chains b) 2 ά chains and 2 β chains c) 2 ά chains and 2 δ chains** d) 2 ά chains and 3 δ chains e) 3 ά chains and 2 δ chains 2- The main (most) Hb found
1 1- Hb A2 is consisting of: a) 3 ά chains and 2 γ chains b) 2 ά chains and 2 β chains c) 2 ά chains and 2 δ chains** d) 2 ά chains and 3 δ chains e) 3 ά chains and 2 δ chains 2- The main (most) Hb found
Anaemia due to a red blood cell membrane defect
 Anaemia due to a red blood cell membrane defect BHS training course 2013 1 Red blood cell membrane defect Pathologies Clinical signs Diagnostic criteria Treatment (HS) 2 The pathologies Structural organisation
Anaemia due to a red blood cell membrane defect BHS training course 2013 1 Red blood cell membrane defect Pathologies Clinical signs Diagnostic criteria Treatment (HS) 2 The pathologies Structural organisation
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Hematology
 Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Hematology - Anemia: It is a reduction in number of RBCs or Hb concentration > 2 SD below the mean for a corresponding
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Hematology - Anemia: It is a reduction in number of RBCs or Hb concentration > 2 SD below the mean for a corresponding
Platelet Disorders. By : Saja Al-Oran
 Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
Approach to the child with anemia. Nittaya Wisanuyothin,MD. Pediatrics Department, Maharat Nakhonratchasima Hospital
 Approach to the child with anemia Nittaya Wisanuyothin,MD. Pediatrics Department, Maharat Nakhonratchasima Hospital Definition of anemia Hb< 2 SD or P2.5 below the mean for a healthy of the same gender
Approach to the child with anemia Nittaya Wisanuyothin,MD. Pediatrics Department, Maharat Nakhonratchasima Hospital Definition of anemia Hb< 2 SD or P2.5 below the mean for a healthy of the same gender
Types of Anaemias and their Management. S. Moncrieffe, Pharm.D., MPH, Dip.Ed., RPh. PSJ CE Mandeville Hotel April 27, 2014
 Types of Anaemias and their Management S. Moncrieffe, Pharm.D., MPH, Dip.Ed., RPh. PSJ CE Mandeville Hotel April 27, 2014 Objectives At the end of the presentations participants should be able to: 1. Define
Types of Anaemias and their Management S. Moncrieffe, Pharm.D., MPH, Dip.Ed., RPh. PSJ CE Mandeville Hotel April 27, 2014 Objectives At the end of the presentations participants should be able to: 1. Define
Congenital Haemoglobinopathies
 Congenital Haemoglobinopathies L. DEDEKEN, MD H O P I T A L U N I V E R S I T A I R E D E S E N F A N T S R E I N E F A B I O L A U N I V E R S I T E L I B R E DE B R U X E L L E S Red Blood Cell Disorders
Congenital Haemoglobinopathies L. DEDEKEN, MD H O P I T A L U N I V E R S I T A I R E D E S E N F A N T S R E I N E F A B I O L A U N I V E R S I T E L I B R E DE B R U X E L L E S Red Blood Cell Disorders
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College
 Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
COAGULATIONS. Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin)
, FRCP(Edin)") COAGULATIONS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin) Haemostasis-blood must be maintained in a fluid state in order to function as a transport system, but must be able to solidify to form a clot following
COAGULATIONS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin) Haemostasis-blood must be maintained in a fluid state in order to function as a transport system, but must be able to solidify to form a clot following
Year 2002 Paper two: Questions supplied by Jo 1
 Year 2002 Paper two: Questions supplied by Jo 1 Question 70 A 25 year old previously well male student presents with recent exertional dyspnoea, epistaxis and bruising. There is no history of medication,
Year 2002 Paper two: Questions supplied by Jo 1 Question 70 A 25 year old previously well male student presents with recent exertional dyspnoea, epistaxis and bruising. There is no history of medication,
HAEMOLYTIC ANAEMIA. Dr. Hasan Fahmawi, MRCP(London), FRCP(Edin) Consultant Physician
, FRCP(Edin) Consultant Physician") HAEMOLYTIC ANAEMIA Dr. Hasan Fahmawi, MRCP(London), FRCP(Edin) Consultant Physician Haemolysis Definition shortening of the normal red blood lifespan of 120 days Increase in unconjugated bilirubin, increased
HAEMOLYTIC ANAEMIA Dr. Hasan Fahmawi, MRCP(London), FRCP(Edin) Consultant Physician Haemolysis Definition shortening of the normal red blood lifespan of 120 days Increase in unconjugated bilirubin, increased
Coagulation Disorders. Dr. Muhammad Shamim Assistant Professor, BMU
 Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Dairion Gatot, Soegiarto Ganie, Savita Handayani. Divisi Hematologi & Onkologi Medik Departemen Ilmu Penyakit Dalam FK-USU/RS H.Adam Malik Medan 2009
 HAEMOLYTIC ANAEMIA Dairion Gatot, Soegiarto Ganie, Savita Handayani. Divisi Hematologi & Onkologi Medik Departemen Ilmu Penyakit Dalam FK-USU/RS H.Adam Malik Medan 2009 WHEN BY THEN Hb 9 g% transfusion
HAEMOLYTIC ANAEMIA Dairion Gatot, Soegiarto Ganie, Savita Handayani. Divisi Hematologi & Onkologi Medik Departemen Ilmu Penyakit Dalam FK-USU/RS H.Adam Malik Medan 2009 WHEN BY THEN Hb 9 g% transfusion
C. treatment with Desferal (deferoxamine mesylate USP, iron-chelating agent)
") HEMOLYTIC ANEMIAS Single choice tests 1. Select the clinical manifestation that is not characteristic for the hemolytic crisis: A. decrease of the red blood cell count B. reticulocytosis C. jaundice D.
HEMOLYTIC ANEMIAS Single choice tests 1. Select the clinical manifestation that is not characteristic for the hemolytic crisis: A. decrease of the red blood cell count B. reticulocytosis C. jaundice D.
Borderline cytopenias. Dr Taku Sugai Consultant Haematologist
 Borderline cytopenias Dr Taku Sugai Consultant Haematologist Borderline cytopenias Neutropenia Thrombocytopenia Anaemia with normal haematinics Two recent cases of cytopenias Neutropenia ANC of more than
Borderline cytopenias Dr Taku Sugai Consultant Haematologist Borderline cytopenias Neutropenia Thrombocytopenia Anaemia with normal haematinics Two recent cases of cytopenias Neutropenia ANC of more than
Approach to Hemolysis
 Objectives: Approach to Hemolysis To know the function of platelets and the relationship between the platelet count in peripheral blood and the extent of abnormal bleeding. To know about the diseases associated
Objectives: Approach to Hemolysis To know the function of platelets and the relationship between the platelet count in peripheral blood and the extent of abnormal bleeding. To know about the diseases associated
HEME 10 Bleeding Disorders
 HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin
 Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin Version: 6 Date: 2 nd March 2010 Authors: Responsible committee or Director: Review date: Target audience: Stakeholders/
Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin Version: 6 Date: 2 nd March 2010 Authors: Responsible committee or Director: Review date: Target audience: Stakeholders/
The importance of thrombocytopenia and its causes
 SYSMEX EDUCATIONAL ENHANCEMENT AND DEVELOPMENT NO 4 2017 SEED HAEMATOLOGY The importance of thrombocytopenia and its causes Key words: Thrombocytopenia, thrombocytopenic, low levels of platelets What is
SYSMEX EDUCATIONAL ENHANCEMENT AND DEVELOPMENT NO 4 2017 SEED HAEMATOLOGY The importance of thrombocytopenia and its causes Key words: Thrombocytopenia, thrombocytopenic, low levels of platelets What is
Laboratory Empowerment. Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance
 Laboratory Empowerment Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance Why? Electronic ICE requesting was in use for requesting red cells NBTC Indication Codes were
Laboratory Empowerment Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance Why? Electronic ICE requesting was in use for requesting red cells NBTC Indication Codes were
Drop of Blood Unravels Mysteries. Prof. Salma Afrose Department of Hematology Dhaka Medical College
 Drop of Blood Unravels Mysteries Prof. Salma Afrose Department of Hematology Dhaka Medical College Peripheral Blood Film (PBF) PBF is a laboratory workup that involves cytology of Peripheral blood cell
Drop of Blood Unravels Mysteries Prof. Salma Afrose Department of Hematology Dhaka Medical College Peripheral Blood Film (PBF) PBF is a laboratory workup that involves cytology of Peripheral blood cell
Chapter 3 MAKING THE DECISION TO TRANSFUSE
 Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Dr. Joyce Regi M.D (Path),D.P.B. Holy Family Hospital & Research Centre
,D.P.B. Holy Family Hospital & Research Centre") Dr. Joyce Regi M.D (Path),D.P.B. Holy Family Hospital & Research Centre Autoimmune haemolytic anaemia is charaterised by shortened red cell survival & the presence of antibodies directed against autologous
Dr. Joyce Regi M.D (Path),D.P.B. Holy Family Hospital & Research Centre Autoimmune haemolytic anaemia is charaterised by shortened red cell survival & the presence of antibodies directed against autologous
Bleeding Disorders. Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph
 Bleeding Disorders Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph Normal hemostasis The normal hemostatic response involves interactions among: The blood vessel wall (endothelium)
Bleeding Disorders Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph Normal hemostasis The normal hemostatic response involves interactions among: The blood vessel wall (endothelium)
Part 1 examination. Haematology: First paper. Tuesday 20 March Candidates must answer all questions. Each question is worth a total of 25 marks.
 Part 1 examination Haematology: First paper Tuesday 20 March 2018 Candidates must answer all questions. Each question is worth a total of 25 marks. Time allowed: 3 hours Question 1: General Haematology
Part 1 examination Haematology: First paper Tuesday 20 March 2018 Candidates must answer all questions. Each question is worth a total of 25 marks. Time allowed: 3 hours Question 1: General Haematology
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi
.ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi") Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
Blood is serious business
 Transfusion at RCH BLOOD TRANSFUSION Anthea Greenway Dept of Clinical Haematology >10000 fresh blood products per year Supports craniofacial and cardiac surgery Support bone marrow, liver transplant and
Transfusion at RCH BLOOD TRANSFUSION Anthea Greenway Dept of Clinical Haematology >10000 fresh blood products per year Supports craniofacial and cardiac surgery Support bone marrow, liver transplant and
BLEEDING DISORDERS. JC Opperman 2012
 BLEEDING DISORDERS JC Opperman 2012 Primary and Secondary Clotting Laboratory Tests Routine screening tests Prothrombin time (PT) (INR) increased in neonates (12-18 sec) Partial thromboplastin time (PTT)
BLEEDING DISORDERS JC Opperman 2012 Primary and Secondary Clotting Laboratory Tests Routine screening tests Prothrombin time (PT) (INR) increased in neonates (12-18 sec) Partial thromboplastin time (PTT)
Prof. Mahmoud Rushdi Faculty of Veterinary Medicine Assiut University Egypt. RBCs counts. Anaemia.
 By Prof. Mahmoud Rushdi Faculty of Veterinary Medicine Assiut University Egypt ١ RBCs counts Normal Anaemia Polycythaemia Morphological Etiological Relative Absolute Size Stain Shape Inclusion Hemorrhagic
By Prof. Mahmoud Rushdi Faculty of Veterinary Medicine Assiut University Egypt ١ RBCs counts Normal Anaemia Polycythaemia Morphological Etiological Relative Absolute Size Stain Shape Inclusion Hemorrhagic
Cytopaenias in HIV. Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH
 Cytopaenias in HIV Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH Introduction Cytopaenias in HIV are common Anaemias multifactorial causes Thrombocytopaenias may be the first
Cytopaenias in HIV Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH Introduction Cytopaenias in HIV are common Anaemias multifactorial causes Thrombocytopaenias may be the first
Maresce Bizaare AWACC 2013
 Maresce Bizaare AWACC 2013 Cytopaenias in HIV Most common complication of HIV Anaemia is most common cytopaenia ITP occurs in 30%, may be first manifestation of HIV Laboratory approach to cytopaenia FBC,
Maresce Bizaare AWACC 2013 Cytopaenias in HIV Most common complication of HIV Anaemia is most common cytopaenia ITP occurs in 30%, may be first manifestation of HIV Laboratory approach to cytopaenia FBC,
Miss. kamlah ahmed 1
 Miss. kamlah ahmed 1 Anatomy & Physiology Blood has two compartments: 1- a fluid portion called plasma. 2- a cellular portion known as the formed elements of the blood. Which are RBC (erythrocytes), WBC
Miss. kamlah ahmed 1 Anatomy & Physiology Blood has two compartments: 1- a fluid portion called plasma. 2- a cellular portion known as the formed elements of the blood. Which are RBC (erythrocytes), WBC
Pathology Service User Guide Haematology
 Pathology Service User Guide Haematology Worthing This section of the Pathology Service User Guide includes: Routine haematology Immunology Haematinic investigations Haemoglobinopathy screening Bone marrow
Pathology Service User Guide Haematology Worthing This section of the Pathology Service User Guide includes: Routine haematology Immunology Haematinic investigations Haemoglobinopathy screening Bone marrow
11. An acute leukemia causing. 12. An adult patient presents with acute. 13. Anemia due to renal failure may be
 Hematology Study online at 1. A 23 year old white female has weakness, fatigue and has developed a habit of chewing ice. What are the expected findings in regard to TIBC and Ferritin? 2. A 25 year old
Hematology Study online at 1. A 23 year old white female has weakness, fatigue and has developed a habit of chewing ice. What are the expected findings in regard to TIBC and Ferritin? 2. A 25 year old
Normal Development. Normal Development 10/16/2012. Hematopoietic and Lymph Node Pathology. Red Blood Cell Maturation & Anemias
 Hematopoietic and Lymph Node Pathology Normal Development Red Blood Cell Maturation & Anemias Normal Development Differentiation of Hematopoietic Cells 1 Bone Marrow Bone Marrow Bone Marrow, RBC Precursors
Hematopoietic and Lymph Node Pathology Normal Development Red Blood Cell Maturation & Anemias Normal Development Differentiation of Hematopoietic Cells 1 Bone Marrow Bone Marrow Bone Marrow, RBC Precursors
namib la UnIVERSITY OF SCIEnCE AnD TECHnOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES
 namib la UnIVERSITY OF SCIEnCE AnD TECHnOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF BIOMEDICAL SCIENCES QUALIFICATION CODE: SOBBMS LEVEL: 6 COURSE
namib la UnIVERSITY OF SCIEnCE AnD TECHnOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF BIOMEDICAL SCIENCES QUALIFICATION CODE: SOBBMS LEVEL: 6 COURSE
Guidelines for Shared Care Centres and Community Staff
 Reference: CG1410 Written by: Dr Jeanette Payne Peer reviewer Dr Jenny Welch Approved: February 2016 Approved by D&TC: 8th January 2016 Review Due: February 2019 Intended Audience This document contains
Reference: CG1410 Written by: Dr Jeanette Payne Peer reviewer Dr Jenny Welch Approved: February 2016 Approved by D&TC: 8th January 2016 Review Due: February 2019 Intended Audience This document contains
IRON DEFICIENCY / ANAEMIA ANTHONY BEETON
 IRON DEFICIENCY / ANAEMIA ANTHONY BEETON HYPOXIA 1-2 mg IRON Labile iron Body iron ± 3 4 g Liver and the reticuloendothelial system and spleen (approximately 200 300 mg in adult women and 1 g in adult
IRON DEFICIENCY / ANAEMIA ANTHONY BEETON HYPOXIA 1-2 mg IRON Labile iron Body iron ± 3 4 g Liver and the reticuloendothelial system and spleen (approximately 200 300 mg in adult women and 1 g in adult
Nutritional anaemia. Dr J Potgieter Dept of Haematology NHLS - TAD
 Nutritional anaemia Dr J Potgieter Dept of Haematology NHLS - TAD Classification of anaemia Microcytic, hypochromic MCV < 80fl MCH > 27pg Iron deficiency Anaemia of chronic disease Thalassaemia Lead poisoning
Nutritional anaemia Dr J Potgieter Dept of Haematology NHLS - TAD Classification of anaemia Microcytic, hypochromic MCV < 80fl MCH > 27pg Iron deficiency Anaemia of chronic disease Thalassaemia Lead poisoning
Iron Deficiency in Athletes. Dr Dan Bates (B.Med, BSc(HONS) Sports Medicine Registrar
 Sports Medicine Registrar") Iron Deficiency in Athletes Dr Dan Bates (B.Med, BSc(HONS) Sports Medicine Registrar Stages of Iron deficiency Iron Storage depletion Depletion suggested by Decrease in ferritin Functional Iron depletion
Iron Deficiency in Athletes Dr Dan Bates (B.Med, BSc(HONS) Sports Medicine Registrar Stages of Iron deficiency Iron Storage depletion Depletion suggested by Decrease in ferritin Functional Iron depletion
Haemopoiesis. Matthew Hazell Consultant Clinical Scientist Trainee
 Haemopoiesis Matthew Hazell Consultant Clinical Scientist Trainee Learning objectives Describe haemopoiesis and the development of blood cells from stem cells to mature cells Explain the roles of the different
Haemopoiesis Matthew Hazell Consultant Clinical Scientist Trainee Learning objectives Describe haemopoiesis and the development of blood cells from stem cells to mature cells Explain the roles of the different
Approach to Anemia PG CME
 Approach to Anemia PG CME 2014 2017 Vikram Mathews Haematology Department Christian Medical College Vellore Definition of Anemia Beutler et al. Blood 2006. Definition of Anemia WHO definition of anemia
Approach to Anemia PG CME 2014 2017 Vikram Mathews Haematology Department Christian Medical College Vellore Definition of Anemia Beutler et al. Blood 2006. Definition of Anemia WHO definition of anemia
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89
 Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
In adults, the predominant Hb (HbA) molecule has four chains: two α and two β chains. In thalassemias, the synthesis of either the α or the β chains
 molecule has four chains: two α and two β chains. In thalassemias, the synthesis of either the α or the β chains") Thalassaemias Thalassemia Thalassemia is an inherited autosomal recessive blood disease. Associated with absence or reduction in a or b globin chains. Reduced synthesis of one of the globin chains can
Thalassaemias Thalassemia Thalassemia is an inherited autosomal recessive blood disease. Associated with absence or reduction in a or b globin chains. Reduced synthesis of one of the globin chains can
Contents SECTION 1: PHYSIOLOGY OF BLOOD
 Contents SECTION 1: PHYSIOLOGY OF BLOOD Chapter 1: Overview of Physiology of Blood 1 Normal Haematopoiesis 1 Red Blood Cells 6 White Blood Cells 15 Immune System 27 Megakaryopoiesis 32 Normal Haemostasis
Contents SECTION 1: PHYSIOLOGY OF BLOOD Chapter 1: Overview of Physiology of Blood 1 Normal Haematopoiesis 1 Red Blood Cells 6 White Blood Cells 15 Immune System 27 Megakaryopoiesis 32 Normal Haemostasis
Origins of the Cellular Elements.
 Blood Life-sustaining fluid Circulates through heart and vessels Delivers oxygen and nutrients to tissues Removes waste to the lungs, kidneys and liver Clots outside the body Origins of the Cellular Elements.
Blood Life-sustaining fluid Circulates through heart and vessels Delivers oxygen and nutrients to tissues Removes waste to the lungs, kidneys and liver Clots outside the body Origins of the Cellular Elements.
Session 11 Disorders of Red cells. B.M.C.Randika Wimalasiri Lecturer(Probationary) Department of Medical Laboratory Sciences
 Department of Medical Laboratory Sciences") Session 11 Disorders of Red cells B.M.C.Randika Wimalasiri Lecturer(Probationary) Department of Medical Laboratory Sciences Red cells Biconcave cells carry oxygen to the peripheral tissues red colour-
Session 11 Disorders of Red cells B.M.C.Randika Wimalasiri Lecturer(Probationary) Department of Medical Laboratory Sciences Red cells Biconcave cells carry oxygen to the peripheral tissues red colour-
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne
 John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
QUESTIONS OF HEMATOLOGY AND THEIR ANSWERS
 QUESTIONS OF HEMATOLOGY AND THEIR ANSWERS WHAT IS TRUE AND WHAT IS FALSE? Questions 1 Iron deficiency anemia a) Is usually associated with a raised MCV. b) The MCH is usually low. c) Is most commonly due
QUESTIONS OF HEMATOLOGY AND THEIR ANSWERS WHAT IS TRUE AND WHAT IS FALSE? Questions 1 Iron deficiency anemia a) Is usually associated with a raised MCV. b) The MCH is usually low. c) Is most commonly due
Definition Aetiology
 Definition Anaemia is a fall in haemoglobin below the reference ranges for age and sex (adult female
Definition Anaemia is a fall in haemoglobin below the reference ranges for age and sex (adult female
Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin
 Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin Document Information Version: 2 Date: 28 th December 2013 Authors (incl. job title): Professor David Rees (Consultant
Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin Document Information Version: 2 Date: 28 th December 2013 Authors (incl. job title): Professor David Rees (Consultant
Non-immune acquired haemolytic anaemias. Dr.Maysem
 Non-immune acquired haemolytic anaemias Dr.Maysem Causes of Non-immune acquired haemolytic anaemias. Infections Infections can cause haemolysis in a variety of ways: -They may precipitate an acute haemolytic
Non-immune acquired haemolytic anaemias Dr.Maysem Causes of Non-immune acquired haemolytic anaemias. Infections Infections can cause haemolysis in a variety of ways: -They may precipitate an acute haemolytic
RBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 RBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Discuss the classification of anemia into hypochromic-microcytic, normochromicnormocytic and macrocytic. Categorize laboratory test procedures used in the
RBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Discuss the classification of anemia into hypochromic-microcytic, normochromicnormocytic and macrocytic. Categorize laboratory test procedures used in the
Interpreting the CBC. Robert Miller PA Assistant Professor of Clinical Pediatrics and Family Medicine USC Keck School of Medicine Retired
 Interpreting the CBC Robert Miller PA Assistant Professor of Clinical Pediatrics and Family Medicine USC Keck School of Medicine Retired The CBC 3 Cell Lines RBCs WBCs Platelets Assess general health Make
Interpreting the CBC Robert Miller PA Assistant Professor of Clinical Pediatrics and Family Medicine USC Keck School of Medicine Retired The CBC 3 Cell Lines RBCs WBCs Platelets Assess general health Make
Glucose-6-P-dehydrogenase deficiency. Béatrice GULBIS, M.D., PhD
 Glucose-6-P-dehydrogenase deficiency Béatrice GULBIS, M.D., PhD SCD day 18/02/2016 1 1. Yes 2. No SCD woman has to be tested for G6PD deficiency? 3. I don t know SCD day 18/02/2016 2 Haemolytic crisis
Glucose-6-P-dehydrogenase deficiency Béatrice GULBIS, M.D., PhD SCD day 18/02/2016 1 1. Yes 2. No SCD woman has to be tested for G6PD deficiency? 3. I don t know SCD day 18/02/2016 2 Haemolytic crisis
Blood Transfusion. Dr Will Dooley
 Blood Transfusion Dr Will Dooley Plan Cases OSCE practice scenario Blood groups Monitoring / Reactions Miss Irene Bleede, 23yo Asymptomatic, healthy woman with menorrhagia Hb 78 g/l, MCV 73fl Would you
Blood Transfusion Dr Will Dooley Plan Cases OSCE practice scenario Blood groups Monitoring / Reactions Miss Irene Bleede, 23yo Asymptomatic, healthy woman with menorrhagia Hb 78 g/l, MCV 73fl Would you
Clinical Guidance. Neonatal Manual Chapter 8: Haematology
 Clinical Guidance Neonatal Manual Chapter 8: Haematology Summary This manual contains clinical guidelines developed by the Neonatal Unit multidisciplinary team over recent years. This chapter contains
Clinical Guidance Neonatal Manual Chapter 8: Haematology Summary This manual contains clinical guidelines developed by the Neonatal Unit multidisciplinary team over recent years. This chapter contains
Haematological Cancer Suspected (Adults & Children)
") Haematological Cancer Suspected (Adults & Children) Link to NICE guidelines: https://www.nice.org.uk/guidance/ng47 Patient of any age presents with symptoms of possible haematological cancer If 60 years
Haematological Cancer Suspected (Adults & Children) Link to NICE guidelines: https://www.nice.org.uk/guidance/ng47 Patient of any age presents with symptoms of possible haematological cancer If 60 years
Year 2003 Paper two: Questions supplied by Tricia
 QUESTION 65 A 36-year-old man presents in a post-ictal state after an observed generalised seizure. Full blood investigation shows: haemoglobin 0 g/l [128-175] mean corpuscular volume (MCV) 106 fl [80-7]
QUESTION 65 A 36-year-old man presents in a post-ictal state after an observed generalised seizure. Full blood investigation shows: haemoglobin 0 g/l [128-175] mean corpuscular volume (MCV) 106 fl [80-7]
GUIDELINE: ASSESSMENT OF BRUISING & BLEEDING IN CHILDREN. All children in whom there is concern regarding bruising / bleeding
 GUIDELINE: ASSESSMENT OF BRUISING & BLEEDING IN CHILDREN Reference: Bruising / Bleeding / NAI Version No: 1 Applicable to All children in whom there is concern regarding bruising / bleeding Classification
GUIDELINE: ASSESSMENT OF BRUISING & BLEEDING IN CHILDREN Reference: Bruising / Bleeding / NAI Version No: 1 Applicable to All children in whom there is concern regarding bruising / bleeding Classification
GP Referral Guidelines. for. South Wales Cancer Network. Document Control Sheet. Specialty/Project Haematological Site Specific Group
 GP Referral Guidelines for South Wales Cancer Network Document Control Sheet Organisation South Wales Cancer Network Specialty/Project Haematological Site Specific Group Document Title GP Referral Guidelines
GP Referral Guidelines for South Wales Cancer Network Document Control Sheet Organisation South Wales Cancer Network Specialty/Project Haematological Site Specific Group Document Title GP Referral Guidelines
Haemolytic anaemias. Dr. J Potgieter Department of Haematology NHLS Tshwane Academic Division
 Haemolytic anaemias Dr. J Potgieter Department of Haematology NHLS Tshwane Academic Division Red Cell Destruction Extravascular in macrophages of RES (BM, liver, spleen) Haem to iron and protoporphyrin
Haemolytic anaemias Dr. J Potgieter Department of Haematology NHLS Tshwane Academic Division Red Cell Destruction Extravascular in macrophages of RES (BM, liver, spleen) Haem to iron and protoporphyrin
TECHNICAL UNIVERSITY OF MOMBASA
 TECHNICAL UNIVERSITY OF MOMBASA Faculty of Applied and Health Sciences DEPARTMENT OF MEDICAL SCIENCES DIPLOMA IN MEDICAL LABORATORY SCIENCES (DMLS ) AML 2301 : HAEMATOLOGY II SPECIAL/SUPPLEMENTARY : EXAMINATIONS
TECHNICAL UNIVERSITY OF MOMBASA Faculty of Applied and Health Sciences DEPARTMENT OF MEDICAL SCIENCES DIPLOMA IN MEDICAL LABORATORY SCIENCES (DMLS ) AML 2301 : HAEMATOLOGY II SPECIAL/SUPPLEMENTARY : EXAMINATIONS
Approach to bleeding disorders &treatment. by RAJESH.N General medicine post graduate
 Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Sickle cell disease. Fareed Omar 10 March 2018
 Sickle cell disease Fareed Omar 10 March 2018 Physiology Haemoglobin structure HbA2: 2α and 2δ chains (2-3%) HbF: 2α and 2γ chains (
Sickle cell disease Fareed Omar 10 March 2018 Physiology Haemoglobin structure HbA2: 2α and 2δ chains (2-3%) HbF: 2α and 2γ chains (
REVIEW OF THE HEMATOPOIETIC SYSTEM
 REVIEW OF THE HEMATOPOIETIC SYSTEM BLOOD BLOOD = Plasma + Formed Elements PLASMA = 91% Water + 7-8% Proteins + 1-2% small molecules SERUM = Plasma Clotting Factors PLASMA PROTEINS Together, the plasma
REVIEW OF THE HEMATOPOIETIC SYSTEM BLOOD BLOOD = Plasma + Formed Elements PLASMA = 91% Water + 7-8% Proteins + 1-2% small molecules SERUM = Plasma Clotting Factors PLASMA PROTEINS Together, the plasma
HLS Midterm ( )
") HLS Midterm (2012-2013) 1. Which of the following cells increase in level during allergic reactions? (a) Neutrophils (b) Basophils (c) Eosinophils (d) Lymphocytes (e) Monocytes 2. Which of the following
HLS Midterm (2012-2013) 1. Which of the following cells increase in level during allergic reactions? (a) Neutrophils (b) Basophils (c) Eosinophils (d) Lymphocytes (e) Monocytes 2. Which of the following
Haematology and Transfusion
 Haematology and Transfusion dr.w.engelhardt@gmail.com Wolfram Engelhardt Offenburg, Germany James Blundell 1828 Diameter 6-8 µm Erythrocytes Women: Men: 4-5 x 10 6 /µl 5-6 x 10 6 /µl live 100-120 days
Haematology and Transfusion dr.w.engelhardt@gmail.com Wolfram Engelhardt Offenburg, Germany James Blundell 1828 Diameter 6-8 µm Erythrocytes Women: Men: 4-5 x 10 6 /µl 5-6 x 10 6 /µl live 100-120 days
CrackCast Episode 7 Blood and Blood Components
 CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic