The Abdominal Compartment Syndrome
|
|
|
- Kelly Tucker
- 5 years ago
- Views:
Transcription
1 The Abdominal Compartment Syndrome Andre R. Campbell, MD, FACS, FACP, FCCM Professor of Surgery, UCSF Endowed Chair of Surgical Education San Francisco General Hospital
2 Outline Case presentations Review literature Abdominal Compartment Syndrome and Intra-Abdominal Hypertension Suggest techniques that can be used to deal with these problems




3
4
5 Damage Control Principles Damage Control Surgery Abdominal Compartment Syndrome Closure of the Abdomen
6 Balogh Z et al. World J Surgery :
7 Balogh Z et al. World J Surgery :

8 Noosa Heads Australia December leaders from around the world Defined and updated the literature on this important clinical problem Consensus definition were developed Intraabdominal Hypertension occurred in 35% of ICU patients Approximately 5% developed ACS Sugrue Curr Opin Crit Care 2005:11:
9 Abdominal Compartment Syndrome Defined Normal IAP is 5mm Hg Can be non-pathological in the obese mm Hg is the way to express the pressure Measure at end expiration No abdominal contractions Gold standard intermittent indirect measurement is the bladder Abdominal Perfusion Pressure(APP)= MAP IAP Sugrue Curr Opin Crit Care 11: , 2005
10 Abdominal Compartment Syndrome Intra-Abdominal Hypertension: IAP of 12mm Hg recorded 4-6 hours apart on three different occasions A APP of 60 mm Hg or less recorded by a minimum standard measurements two times 1-6 hours apart
11 Abdominal Compartment Syndrome Pressure of 20 mm Hg or great with or without APP below 50 mm Hg recorded by minimum of three standard measurements 1-6 hours apart and single or MOF Primary Abdominal Compartment Syndrome: Associated with injury or disease of the abdominopelvic region that frequently requires early surgical or angio intervention or that develops after abdominal surgery(organ injury requiring damage control, secondary peritonitis, bleeding pelvis fracture, massive retroperitoneal hematoma liver transplantation. Sugrue Curr Opin Crit Care 2005:11:
12 Abdominal Compartment Syndrome Secondary ACS: Conditions that do not originate in the abdomen capillary leak, burns, and other conditions requiring massive resuscitation» 13 series reported in the literature Kirkpatrick et al JACS 2006 Apr;202(4): Tertiary ACS: Recurrent ACS develops after therapeutic surgical or medical treatment or primary or secondary ACS after decompressive laparotomy or after definitive closure
13 Grading of Intra-Abdominal Hypertension Grade I II III IV IAP(mm Hg) >25
14 Intra-Abdominal Hypertension Causes Trauma or hemorrhage Abdominal surgery Retroperitoneal bleed Peritonitis: secondary or tertiary Laparoscopy or pneumoperitoneum Repair of a large hernia Abdominal binding with postoperative velcro to prevent hernias Massive fluid resuscitation more than 5 liters in 24 hours Ileus: paralytic, pseudo obstructive Post operative rupture aneurysms
15 Pathogenesis- IAH Can occur in surgical and non-surgical patients Probably multifactorial in nature Capillary leak Shock with ischemia reperfusion injury release of vasoactive substances oxygen free radicals massive increase in extracellular volume occurs
16 Abdominal Compartment Syndrome Abdominal Wall Abnormalities: Reduced abdominal wall blood flow Local ischemia and edema»can reduce abdominal wall compliance»acs is exacerbated Wound complications can result»herniation, dehiscence, necrotizing faciitis Saggit et al, J Trauma, 45:3:
17 Abdominal Compartment Syndrome Pulmonary Dysfunction: High ventilatory pressures, hypoxia, hypercarbia Reduced static and dynamic lung compliance Increased peak pressures Reduced TLC, FRC, Residual volume V/Q abnormalities and hypoventilation»hypoxia and hypercarbia Saggit et al, J Trauma, 45:3:
18 Abdominal Compartment Syndrome Pulmonary Dysfunction (continued): PVR increases»reduced oxygen tension and increased intra-thoracic pressure Animal models show recent hemorrhage exacerbates cardiopulmonary effects Obesity hypoventilation syndrome»makes acute phase worst Saggit et al, J Trauma, 45:3:
19
20 Abdominal Compartment Syndrome Intracranial Derangement: Increased ICP reduces CPP»Shown in animal models and human studies Elevated ICP secondary to increased CVP, and intrathoracic pressure Surgical decompression reduces this affects Chronic elevations in ICP implicated in pseudotumor cerebri- obesity»responds to bariatric surgery Saggit et al, J Trauma, 45:3:
21 Abdominal Compartment Syndrome Measurements of IAP: Gastric Pressure Inferior Vena Cava Pressure Urinary Bladder Pressure» Gold Standard
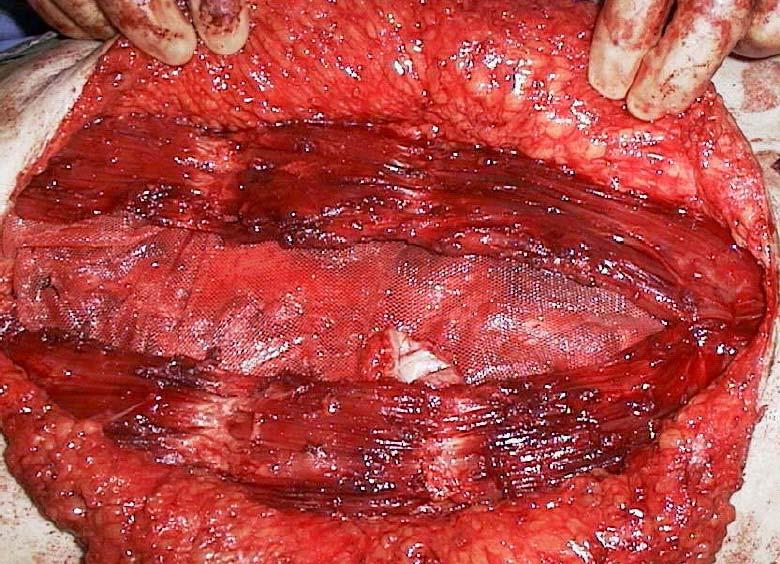
22 Techniques for closure of the Abdomen Skin approximation Bogota bag Vicryl mesh Dexon mesh Open-Steri-Drape Modified removal prosthesis-marlex with zipper or Wittman Patch Vacuum assisted closure Rutherford, EJ et al Cur Prob Surg 2004:41:
23 Comparison of Choices for Abdominal Closure Sugrue Curr Opin Crit Care 11: , 2005
24 Open Abdominal Cases Incidence estimated in the literature to be 10-23%» Retrospective studies in the literature New techniques allows fascial closure in 70-80% of cases Less morbidity and mortality if the fascia can be closed primarily- no need for a large second operation Technique of vacuum pack closure described by Barker using JPs for suction Argenta described use of wound vac on chronic wounds clinically subsequently applied to abdominal wound closure Barker DE et al. J Trauma 2000:48: Miller PR, et al J Trauma 2002:53: Argenta LC, Morykwas MJ Ann Plastic Surg 2000:45:3:332-4




25


26


27


28 Alien Physiology
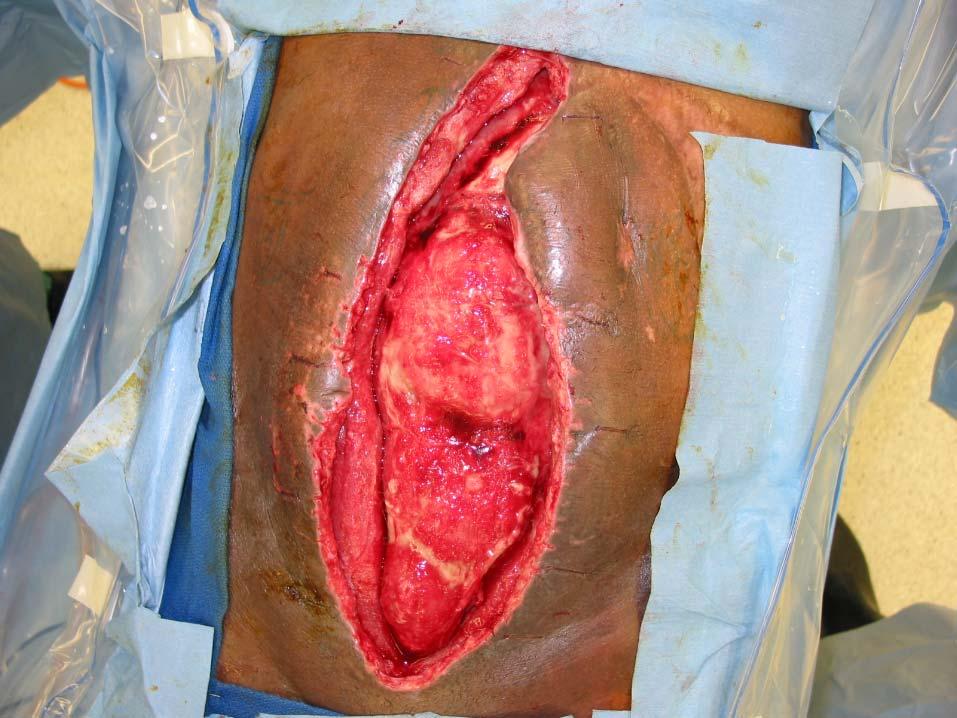
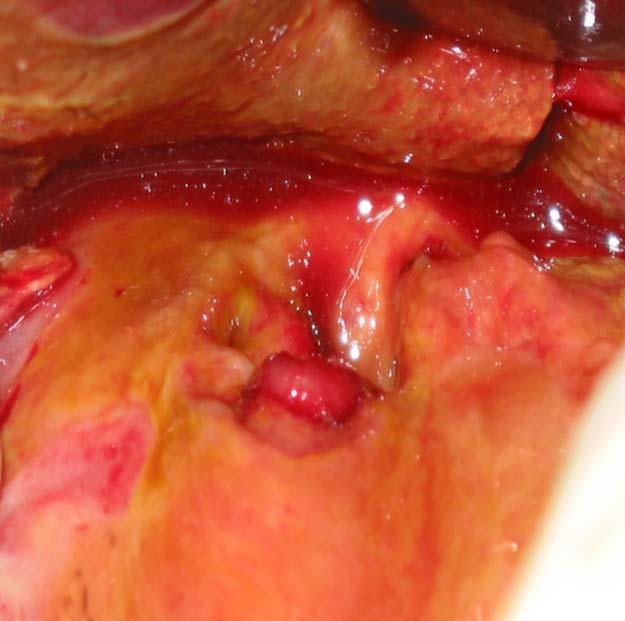
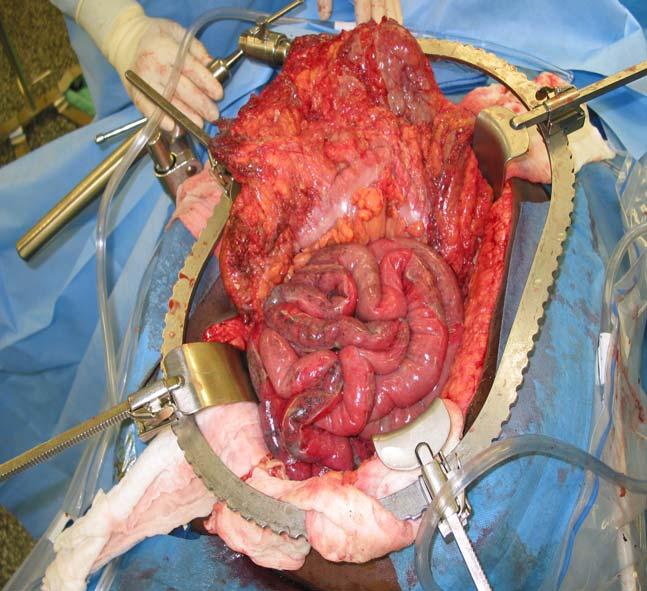
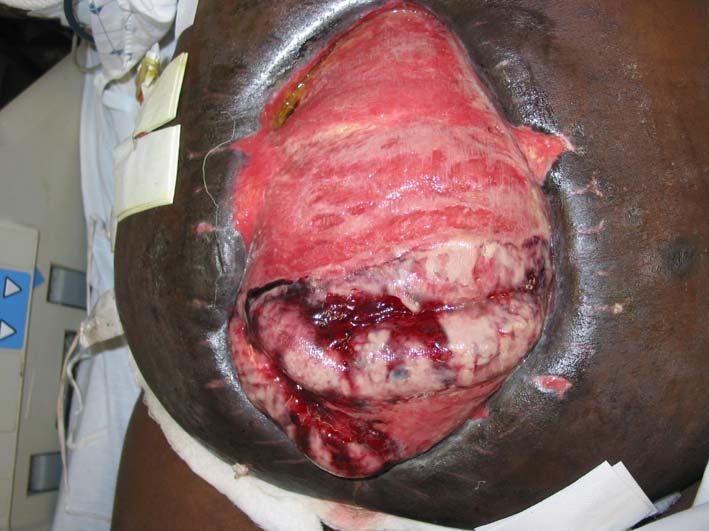
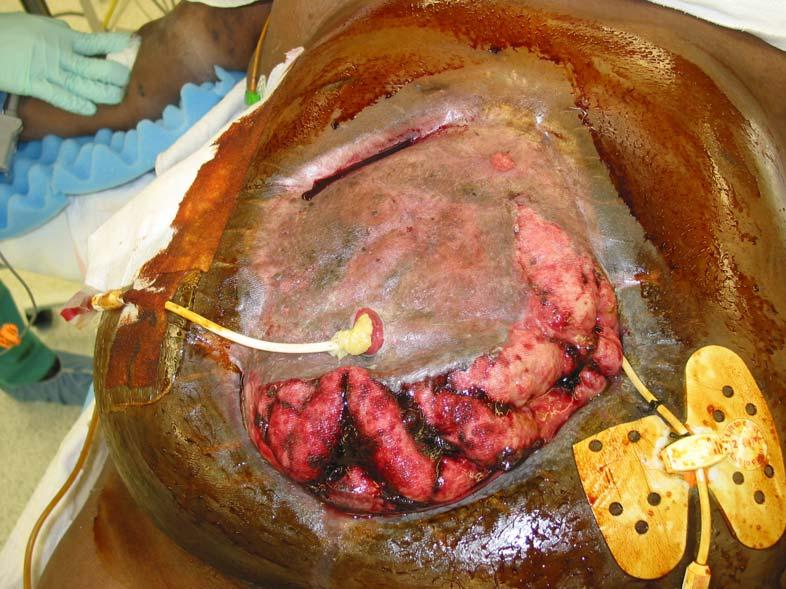
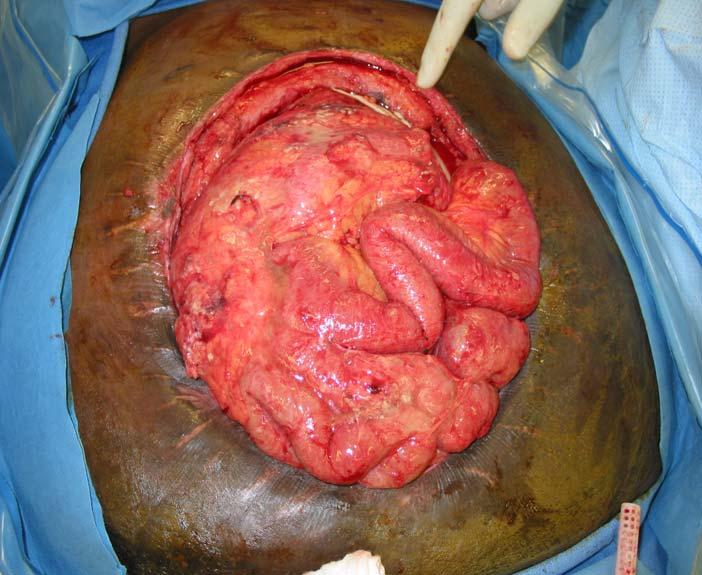
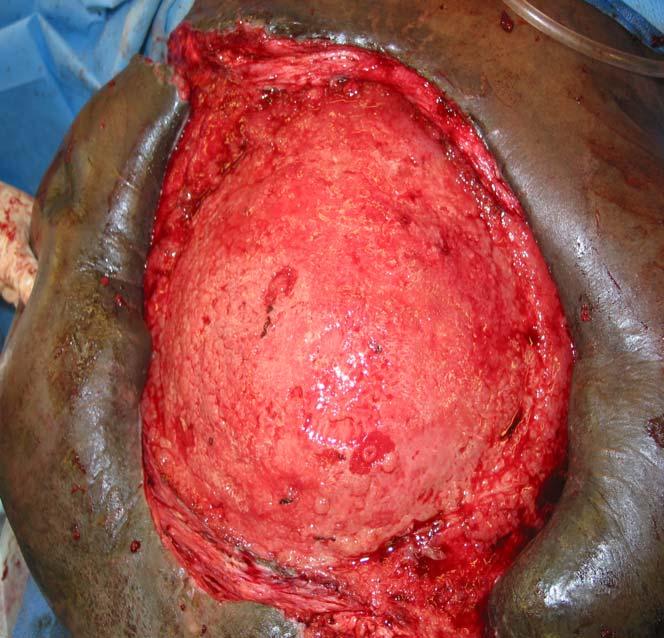
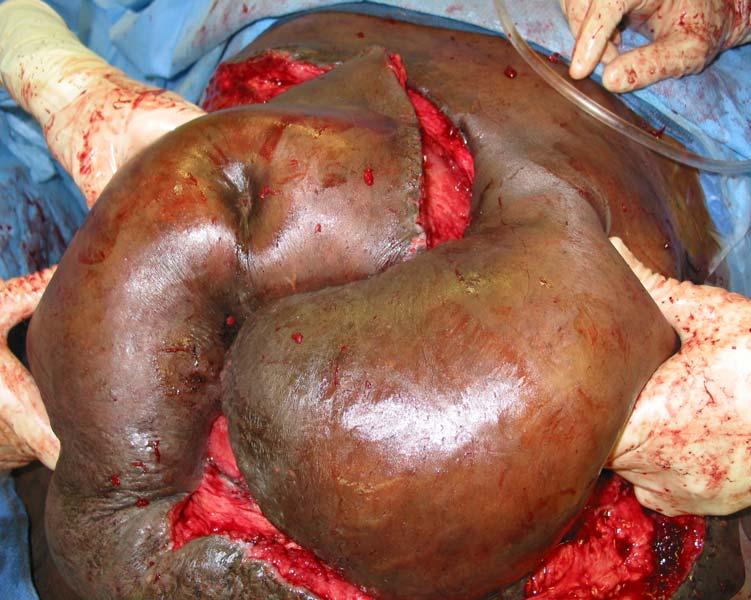
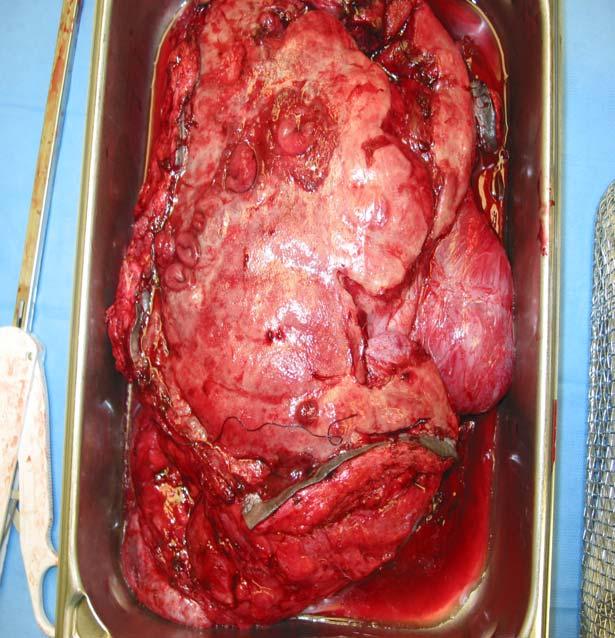
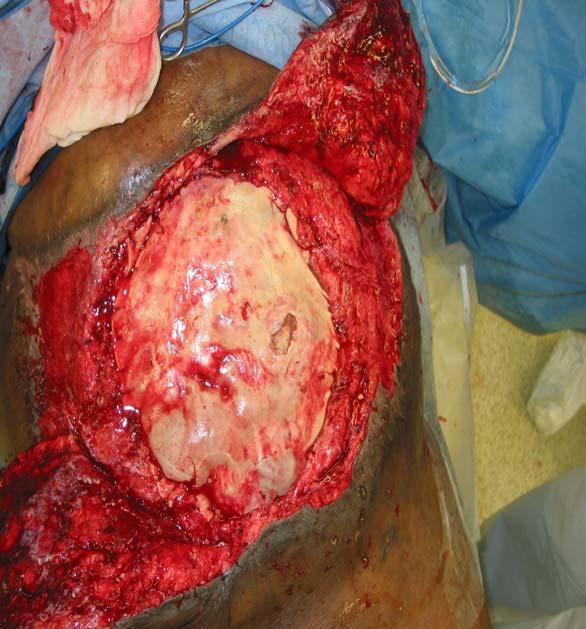
29 Case Presentation 46 yo obese man with abdominal pain One hour after arrival he had a cardiac arrest in the CT scanner BMI: 58 wt: 365 lbs Shock and hypotensive CT massive free air in the abdomen no PE Exp Lap 4/15/2005 A series of problems ensued with the patient Shock, renal failure, respiratory failure, 4 cardiac arrests on the night of admission 4 pressors Massive hemorrhage on Activated Protein C Developed Abdominal Compartment Syndrome

30


31


32


33
34
35 Management of the Open Abdomen 21 patients(48%) were closed at > 9 days (range 9-21 days) 2 patients had a fascial dehiscence that was subsequently closed One patient developed a ventral hernia that was repaired Conclusion:»VAC assisted closures resulted in significantly higher fascial closure rates eliminating the need for hernia repair in most patients Miller PR et al. Ann Surg 2004:239:
36 Management of the Open Abdomen Early aggressive closure of the open abdomen Retrospective review of 37 patients Vacuum assisted closure and alloderm used Mean time with open abdomen was 21.7 days(6-45) Alloderm used if the abdominal wall could not be closed No fistulas, no intraabdominal complications or graft loss All survived to discharge No hernia formation noted Superficial wound infection occurred in 2 patients treated with wet to dry dressings Conclusions Early closure possible with vacuum pack, vacuum assisted wound closure and Alloderm Scott, BG et al, J of Trauma 2006:60:17-22
37 Other ways to close the abdomen Acellular cadaveric dermis(alloderm) Intact human skin Structural components of the dermal extracellular scaffold that enable it to recellularize and revascularize Integrates into surround tissue Mainly used in chronic hernia situation with failed mesh repairs Buinewicz et al, Ann Plast Surg 2004:52:


38





39

40 Retrospective review of one hospitals experience 26 months and 35 patients in the study Profoundly ill trauma patients Six died, 29 discharged 86% were closed using the vac at a mean of 7+1 day! No patients developed evisceration, abscess, or wound infection Four who failed closure 2 fistulas Suliburk et al, J of Trauma 2003;55:



41


42





43
44 Conclusions The Abdominal Compartment Syndrome is real! Difficult cases to manage Must be on a mission to close the patient ASAP Do not do it as the last case of the day Many options for management Some recommend dealing with fistulas or stomas before definitive repair Oblique releases can help reduce fascial tension
45 Conclusions Be prepared for problems to develop! Vacuum assisted closure allows can help close over 80% or more of these cases Geometry problem Get help when needed Some patients you will not be able to close
Difficult Abdominal Closure. Mark A. Carlson, MD
 Difficult Abdominal Closure Mark A. Carlson, MD Illustrative case 14 yo boy with delayed diagnosis of appendicitis POD9 Appendectomy 2 wk after onset of symptoms POD4: return to OR for midline laparotomy
Difficult Abdominal Closure Mark A. Carlson, MD Illustrative case 14 yo boy with delayed diagnosis of appendicitis POD9 Appendectomy 2 wk after onset of symptoms POD4: return to OR for midline laparotomy
Management of the Open Abdomen
 Management of the Open Abdomen Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Associate Professor of Surgery Denver Health Medical Center / University of Colorado The Open Abdomen
Management of the Open Abdomen Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Associate Professor of Surgery Denver Health Medical Center / University of Colorado The Open Abdomen
Bogota-VAC A Newly Modified Temporary Abdominal Closure Technique
 Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2008 Bogota-VAC A Newly Modified Temporary Abdominal Closure Technique von
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2008 Bogota-VAC A Newly Modified Temporary Abdominal Closure Technique von
Abdominal V.A.C. Therapy in Trauma
 Abdominal V.A.C. Therapy in Trauma Stefaan Nijs, M.D., Ph.D. Mathieu D Hondt, M.D. Dept Abdominal Surgery UZ Leuven 1 2 Damage control = naval technique Damage Control in Trauma 3 USS Nevada 4 In extremis
Abdominal V.A.C. Therapy in Trauma Stefaan Nijs, M.D., Ph.D. Mathieu D Hondt, M.D. Dept Abdominal Surgery UZ Leuven 1 2 Damage control = naval technique Damage Control in Trauma 3 USS Nevada 4 In extremis
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Abdominal Compartment Syndrome. Jeff Johnson, MD
 Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Open abdomen in trauma. Ari Leppäniemi Abdominal Center Meilahti hospital University of Helsinki Finland
 Open abdomen in trauma Ari Leppäniemi Abdominal Center Meilahti hospital University of Helsinki Finland Frequency and causes of open abdomen - in 23% (344/1531) after trauma laparotomies - damage control
Open abdomen in trauma Ari Leppäniemi Abdominal Center Meilahti hospital University of Helsinki Finland Frequency and causes of open abdomen - in 23% (344/1531) after trauma laparotomies - damage control
One hundred percent fascial approximation with sequential abdominal closure of the open abdomen
 The American Journal of Surgery 192 (2006) 238 242 HowIdoit One hundred percent fascial approximation with sequential abdominal closure of the open abdomen C. Clay Cothren, M.D. a,b, *, Ernest E. Moore,
The American Journal of Surgery 192 (2006) 238 242 HowIdoit One hundred percent fascial approximation with sequential abdominal closure of the open abdomen C. Clay Cothren, M.D. a,b, *, Ernest E. Moore,
INTRA-ABDOMINAL HYPERTENSION AND SECONDARY ABDOMINAL COMPARTMENT SYNDROME IN MEDICAL PATIENTS COMPLICATION WITH A HIGH MORTALITY
 Trakia Journal of Sciences, Vol. 12, Suppl. 1, pp 202-207, 2014 Copyright 2014 Trakia University Available online at: http://www.uni-sz.bg ISSN 1313-7050 (print) ISSN 1313-3551 (online) INTRA-ABDOMINAL
Trakia Journal of Sciences, Vol. 12, Suppl. 1, pp 202-207, 2014 Copyright 2014 Trakia University Available online at: http://www.uni-sz.bg ISSN 1313-7050 (print) ISSN 1313-3551 (online) INTRA-ABDOMINAL
MIST. Minimally invasive Infusion & Suction Therapy Device. Effective treatment for deadly abdominal trauma and sepsis
 MIST Minimally invasive Infusion & Suction Therapy Device Effective treatment for deadly abdominal trauma and sepsis Summary Medical device for treating condition that annually kills ~156k intensive care
MIST Minimally invasive Infusion & Suction Therapy Device Effective treatment for deadly abdominal trauma and sepsis Summary Medical device for treating condition that annually kills ~156k intensive care
Abdominal Compartment Syndrome. Jeff Johnson, MD
 Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Emergency Laparotomy. Open vs Closed Abdomen
 Emergency Laparotomy Open vs Closed Abdomen Disclosure Dr. McLean is a site primary investigator for XenMatrix AB Tissue Insert for Ventral Hernia repair. Sponsor: Bard Davol Learning Objectives: 1. The
Emergency Laparotomy Open vs Closed Abdomen Disclosure Dr. McLean is a site primary investigator for XenMatrix AB Tissue Insert for Ventral Hernia repair. Sponsor: Bard Davol Learning Objectives: 1. The
Modern Management of the Open Abdomen A Cautionary Tale. Grand Rounds December 16, 2010 SUNY, Downstate
 Modern Management of the Open Abdomen A Cautionary Tale Grand Rounds December 16, 2010 SUNY, Downstate Case HPI: 41 yo M BIBA; stabbed in left back while walking out of a shopping center. PMH/PSH: GSW
Modern Management of the Open Abdomen A Cautionary Tale Grand Rounds December 16, 2010 SUNY, Downstate Case HPI: 41 yo M BIBA; stabbed in left back while walking out of a shopping center. PMH/PSH: GSW
Intra-abdominal Hypertension and Abdominal Compartment Syndrome: A Potentially Fatal Mix. Daria C. Ruffolo
 Intra-abdominal Hypertension and Abdominal Compartment Syndrome: A Potentially Fatal Mix Daria C. Ruffolo No Conflict of Interest druffol@lumc.edu 708.216.4541 Objectives Differentiate between intra-abdominal
Intra-abdominal Hypertension and Abdominal Compartment Syndrome: A Potentially Fatal Mix Daria C. Ruffolo No Conflict of Interest druffol@lumc.edu 708.216.4541 Objectives Differentiate between intra-abdominal
In the early 1980s, Kron et al. 1 showed in an. Surgical management of abdominal compartment syndrome
 This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this
Oncology case of the week:
 Oncology case of the week: The Abdomen That Won t Close Anton Sharapov, R4 July 14, 2004 Case 56 yof in ER resident on call asked to assess stoma looks infected has been on antibiotics not settling PMH
Oncology case of the week: The Abdomen That Won t Close Anton Sharapov, R4 July 14, 2004 Case 56 yof in ER resident on call asked to assess stoma looks infected has been on antibiotics not settling PMH
Volume 16 - Issue 3, Cover Story
 Volume 16 - Issue 3, 2016 - Cover Story Update on Intra-Abdominal Hypertension Prof. Manu Malbrain, MD, PhD ******@***uzbrussel.be ICU Director - Intensive Care Unit, University Hospital Brussels (UZB)
Volume 16 - Issue 3, 2016 - Cover Story Update on Intra-Abdominal Hypertension Prof. Manu Malbrain, MD, PhD ******@***uzbrussel.be ICU Director - Intensive Care Unit, University Hospital Brussels (UZB)
ICU treatment of the trauma patient. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
PRACTICE GUIDELINES: INTRA-ABDOMINAL HYPERTENSION/ABDOMINAL COMPARTMENT SYNDROME
 PRACTICE GUIDELINES: INTRA-ABDOMINAL HYPERTENSION/ABDOMINAL COMPARTMENT SYNDROME OBJECTIVE: Provide guidelines describing the appropriate monitoring for adult and pediatric patients who are at risk for
PRACTICE GUIDELINES: INTRA-ABDOMINAL HYPERTENSION/ABDOMINAL COMPARTMENT SYNDROME OBJECTIVE: Provide guidelines describing the appropriate monitoring for adult and pediatric patients who are at risk for
General Surgery Service
 General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
4/30/2010. Options for abdominal wall reconstruction. Scott L. Hansen, MD
 Components Separation Scott L. Hansen, MD University of California, San Francisco Chief, Plastic and Reconstructive Surgery San Francisco General Hospital Overview Options for abdominal wall reconstruction
Components Separation Scott L. Hansen, MD University of California, San Francisco Chief, Plastic and Reconstructive Surgery San Francisco General Hospital Overview Options for abdominal wall reconstruction
Gastro-intestinal failure. ICU Fellowship Training Radboudumc
 Gastro-intestinal failure ICU Fellowship Training Radboudumc Case history (1) Male, 47 No previous medical history Mechanical ventilation for severe CAP Stable HD on NE 0.04 μg/kg/min Early enteral nutrition
Gastro-intestinal failure ICU Fellowship Training Radboudumc Case history (1) Male, 47 No previous medical history Mechanical ventilation for severe CAP Stable HD on NE 0.04 μg/kg/min Early enteral nutrition
IVC. Fig. ACS. 84/60mmHg. CT Fig. 2 AAA. 30 declamp. declamp. Tel:
 12 633 637 2003 IVC 3 4 5 3 12 633 637 2003 1 ACS ACS 1 6 3 ACS 3 Tel: 0566-75-2111 446-8602 28 2003 7 18 2003 10 15 Fig. 1 4 5 1 71 12 5 COPD 14 10 30 60 CT AAA 84/60mmHg 8.2g/dl6.6g/dl2.5mg/dl CT Fig.
12 633 637 2003 IVC 3 4 5 3 12 633 637 2003 1 ACS ACS 1 6 3 ACS 3 Tel: 0566-75-2111 446-8602 28 2003 7 18 2003 10 15 Fig. 1 4 5 1 71 12 5 COPD 14 10 30 60 CT AAA 84/60mmHg 8.2g/dl6.6g/dl2.5mg/dl CT Fig.
SURGICAL CRITICAL CARE REVIEW TRAUMA K. INABA, MD FACS LAC+USC MEDICAL CENTER
 SURGICAL CRITICAL CARE REVIEW TRAUMA K. INABA, MD FACS LAC+USC MEDICAL CENTER None DISCLOSURES OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY Abdominal Compartment
SURGICAL CRITICAL CARE REVIEW TRAUMA K. INABA, MD FACS LAC+USC MEDICAL CENTER None DISCLOSURES OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY Abdominal Compartment
Abdominal Wound Dehiscence. Presenter: T Mohammed Moderator: Dr H Pienaar
 Abdominal Wound Dehiscence Presenter: T Mohammed Moderator: Dr H Pienaar Introduction Wound Dehiscence is the premature "bursting" open of a wound along surgical suture. It is a surgical complication that
Abdominal Wound Dehiscence Presenter: T Mohammed Moderator: Dr H Pienaar Introduction Wound Dehiscence is the premature "bursting" open of a wound along surgical suture. It is a surgical complication that
DAMAGE CONTROL. Outline. Definition 5/29/2014. No Disclosures
 DAMAGE CONTROL No Disclosures Rochelle A. Dicker, MD Associate Professor of Surgery and Anesthesia University of California, San Francisco Definition Term used in the Merchant Marines and in Navies for
DAMAGE CONTROL No Disclosures Rochelle A. Dicker, MD Associate Professor of Surgery and Anesthesia University of California, San Francisco Definition Term used in the Merchant Marines and in Navies for
Management of the Open Abdomen Usefulness of the bilateral anterior rectus abdominis sheath turnover flap method for early fascial closure
 From the Japanese ssociation of Medical Sciences Japanese ssociation for cute Medicine Management of the Open bdomen Usefulness of the bilateral anterior rectus abdominis sheath turnover flap method for
From the Japanese ssociation of Medical Sciences Japanese ssociation for cute Medicine Management of the Open bdomen Usefulness of the bilateral anterior rectus abdominis sheath turnover flap method for
General Review: The open abdomen: Management with temporary abdomincal closure. The open abdomen
 The open abdomen Part 2: Management of the open abdomen using temporary abdominal closure Abstract Pretorius JP, MBChB, MMed (Surg), FCS (SA); Liebenberg C, MBChB; Piek D, MBChB; Smith M, MBChB Correspondence
The open abdomen Part 2: Management of the open abdomen using temporary abdominal closure Abstract Pretorius JP, MBChB, MMed (Surg), FCS (SA); Liebenberg C, MBChB; Piek D, MBChB; Smith M, MBChB Correspondence
Discussion of Complex Clinical Scenarios and Variable Review ACS NSQIP Clinical Support Team
 Discussion of Complex Clinical Scenarios and Variable Review CS NSQIP Clinical Support Team SCR Open Q& Calls The CS NSQIP Clinical Team is trialing Open format Q& calls for NSQIP SCRs Participation in
Discussion of Complex Clinical Scenarios and Variable Review CS NSQIP Clinical Support Team SCR Open Q& Calls The CS NSQIP Clinical Team is trialing Open format Q& calls for NSQIP SCRs Participation in
Masatoku Arai 1*, Shiei Kim 1, Hiromoto Ishii 1, Jun Hagiwara 1, Shigeki Kushimoto 2 and Hiroyuki Yokota 1
 Arai et al. World Journal of Emergency Surgery (2018) 1:9 https://doi.org/10.118/s1017-018-0200-7 RESEARCH ARTICLE Open Access The long-term outcomes of early abdominal wall reconstruction by bilateral
Arai et al. World Journal of Emergency Surgery (2018) 1:9 https://doi.org/10.118/s1017-018-0200-7 RESEARCH ARTICLE Open Access The long-term outcomes of early abdominal wall reconstruction by bilateral
Colostomy & Ileostomy
 Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Is the evolving management of intra-abdominal hypertension and abdominal compartment syndrome improving survival?*
 Continuing Medical Education Article Is the evolving management of intra-abdominal hypertension and abdominal compartment syndrome improving survival?* Michael L. Cheatham, MD, FCCM; Karen Safcsak, RN
Continuing Medical Education Article Is the evolving management of intra-abdominal hypertension and abdominal compartment syndrome improving survival?* Michael L. Cheatham, MD, FCCM; Karen Safcsak, RN
In any operation. Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications.
 In any operation Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications. Abdominal operation I position for operation Supine Abdominal operation I position for
In any operation Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications. Abdominal operation I position for operation Supine Abdominal operation I position for
Piotr W. Trzeciak, Joanna Porzeżyńska, Karolina Ptasińska,
 POLSKI PRZEGLĄD CHIRURGICZNY 2015, 87, 11, 592 597 10.1515/pjs-2016-0008 Abdominal cavity eventration treated by means of the open abdomen technique using the negative pressure therapy system case report
POLSKI PRZEGLĄD CHIRURGICZNY 2015, 87, 11, 592 597 10.1515/pjs-2016-0008 Abdominal cavity eventration treated by means of the open abdomen technique using the negative pressure therapy system case report
MESH REPAIR VERSUS PLANNED VENTRAL HERNIA STAGED REPAIR IN THE MANAGEMENT OF TRAUMA PATIENTS WITH ACUTE ABDOMINAL COMPARTMENT SYNDROME
 TOFIQ Journal of Medical Sciences, TJMS, Vol. 1, Issue 1, (2014), 47-61 ISSN: 2377-2808 MESH REPAIR VERSUS PLANNED VENTRAL HERNIA STAGED REPAIR IN THE MANAGEMENT OF TRAUMA PATIENTS WITH ACUTE ABDOMINAL
TOFIQ Journal of Medical Sciences, TJMS, Vol. 1, Issue 1, (2014), 47-61 ISSN: 2377-2808 MESH REPAIR VERSUS PLANNED VENTRAL HERNIA STAGED REPAIR IN THE MANAGEMENT OF TRAUMA PATIENTS WITH ACUTE ABDOMINAL
The Emergency Hernia or The call you don t want at 2:00 a.m.*
 or The call you don t want at 2:00 a.m.* *Or even at 8:00 a.m. Michael G. Sarr, MD Professor of Surgery Mayo Clinic South Canada WEST CANADA EAST CANADA Clinical talk Hernias Inguinal Umbilical Incisional
or The call you don t want at 2:00 a.m.* *Or even at 8:00 a.m. Michael G. Sarr, MD Professor of Surgery Mayo Clinic South Canada WEST CANADA EAST CANADA Clinical talk Hernias Inguinal Umbilical Incisional
Review Abdominal compartment syndrome Jeffrey Bailey and Marc J Shapiro
 http://ccforum.com/content/4/1/023 Review Abdominal compartment syndrome Jeffrey Bailey and Marc J Shapiro Saint Louis University, St Louis, Missouri, USA Received: 4 January 2000 Accepted: 5 January 2000
http://ccforum.com/content/4/1/023 Review Abdominal compartment syndrome Jeffrey Bailey and Marc J Shapiro Saint Louis University, St Louis, Missouri, USA Received: 4 January 2000 Accepted: 5 January 2000
Trauma Scenario. Abdominal Compartment Syndrome. Disclosure Statement of Financial Interest 8/17/2015
 Abdominal Compartment Syndrome Diane Cobble M.D., FACS Professor, ETSU Dept. of Surgery 7 th Annual Rural Trauma Symposium August 27, 2015 Disclosure Statement of Financial Interest I DO NOT have a financial
Abdominal Compartment Syndrome Diane Cobble M.D., FACS Professor, ETSU Dept. of Surgery 7 th Annual Rural Trauma Symposium August 27, 2015 Disclosure Statement of Financial Interest I DO NOT have a financial
V.A.C. Abdominal Dressing System
 European Journal of Trauma Original Article V.A.C. Abdominal Dressing System A Temporary Closure for Open Abdomen Ludwig Labler 1, Jörn Zwingmann 1, Dieter Mayer 2, Reto Stocker 1, Otmar Trentz 1, Marius
European Journal of Trauma Original Article V.A.C. Abdominal Dressing System A Temporary Closure for Open Abdomen Ludwig Labler 1, Jörn Zwingmann 1, Dieter Mayer 2, Reto Stocker 1, Otmar Trentz 1, Marius
Which Blunt Trauma Patients Should Be Studied by Abdominal CT?
 MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
Long Term Follow-up. 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown. Is the patient alive? Yes No
 Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
PEDIATRIC TRAUMA: Implications for Respiratory Care
 PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal compartment syndrome, as complication of fluid resuscitation, 331 338 abdominal perfusion pressure, 332 fluid restriction practice
Index Note: Page numbers of article titles are in boldface type. A Abdominal compartment syndrome, as complication of fluid resuscitation, 331 338 abdominal perfusion pressure, 332 fluid restriction practice
Ventral Hernia Repairs: 10 year Single Institution Review at Thomas Jefferson University Hospital
 Thomas Jefferson University Jefferson Digital Commons Department of Surgery Faculty Papers Department of Surgery 1-2011 Ventral Hernia Repairs: 10 year Single Institution Review at Thomas Jefferson University
Thomas Jefferson University Jefferson Digital Commons Department of Surgery Faculty Papers Department of Surgery 1-2011 Ventral Hernia Repairs: 10 year Single Institution Review at Thomas Jefferson University
Clinical Evidence Summary ACCURYN ADVANCED CRITICAL CARE MONITORING
 Clinical Evidence Summary ACCURYN ADVANCED CRITICAL CARE MONITORING Table of Contents Introduction: Urine Output 3 Intensive monitoring of urine output is associated with increased detection 4 of acute
Clinical Evidence Summary ACCURYN ADVANCED CRITICAL CARE MONITORING Table of Contents Introduction: Urine Output 3 Intensive monitoring of urine output is associated with increased detection 4 of acute
General'Surgery'Service'
 General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
Penetrating abdominal trauma clinical view. Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland
 Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
JKSS. Application of negative pressure wound therapy in patients with wound dehiscence after abdominal open surgery: a single center experience
 ORIGINAL ARTICLE pissn 2233-7903 eissn 2093-0488 Application of negative pressure wound therapy in patients with wound dehiscence after abdominal open surgery: a single center experience Ji Young Jang,
ORIGINAL ARTICLE pissn 2233-7903 eissn 2093-0488 Application of negative pressure wound therapy in patients with wound dehiscence after abdominal open surgery: a single center experience Ji Young Jang,
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 3, Issue 1 2013 Article 9 ISSUE 1 Perforation Of The Caecum Owing To Benign Rectal Obstruction: A Paradigm Of Damage Control In Emergency Colorectal Surgery DIMITRIOS
World Journal of Colorectal Surgery Volume 3, Issue 1 2013 Article 9 ISSUE 1 Perforation Of The Caecum Owing To Benign Rectal Obstruction: A Paradigm Of Damage Control In Emergency Colorectal Surgery DIMITRIOS
Management of Bleeding Pelvic Fractures
 Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Is Readmission a Good Quality Measure for Surgical Care? Examining the Underlying Reasons for Readmissions after Surgery at ACS NSQIP Hospitals
 Is Readmission a Good Quality Measure for Surgical Care? Examining the Underlying Reasons for Readmissions after Surgery at ACS NSQIP Hospitals Mila H. Ju, MD, MS Ryan P. Merkow, MD, MS Jeanette W. Chung,
Is Readmission a Good Quality Measure for Surgical Care? Examining the Underlying Reasons for Readmissions after Surgery at ACS NSQIP Hospitals Mila H. Ju, MD, MS Ryan P. Merkow, MD, MS Jeanette W. Chung,
Chapter 2 Damage Control
 Chapter 2 Damage Control Rona E. Altaras, Firas G. Madbak and Dale A. Dangleben History Originally a naval term, damage control (DC) is a simple and useful idea referring to the ability of a battleship
Chapter 2 Damage Control Rona E. Altaras, Firas G. Madbak and Dale A. Dangleben History Originally a naval term, damage control (DC) is a simple and useful idea referring to the ability of a battleship
Abdominal compartment syndrome
 Review Article Abdominal compartment syndrome Biswajit Mohapatra As per definition Abdominal Compartment Syndrome (ACS) is the sudden increase in the Intra-Abdominal pressure resulting in alteration in
Review Article Abdominal compartment syndrome Biswajit Mohapatra As per definition Abdominal Compartment Syndrome (ACS) is the sudden increase in the Intra-Abdominal pressure resulting in alteration in
Understanding Intra-Abdominal Pressures
 Understanding Intra-Abdominal Pressures 1 Contact Hour Course Expires: May 31, 2018 Course Updated: October 14, 2014 First Published: October 14, 2011 Copyright 2011 by RN.com All Rights Reserved Reproduction
Understanding Intra-Abdominal Pressures 1 Contact Hour Course Expires: May 31, 2018 Course Updated: October 14, 2014 First Published: October 14, 2011 Copyright 2011 by RN.com All Rights Reserved Reproduction
Teamwork radiology and surgery
 Catchment area Teamwork radiology and surgery Jigsaw TRAUMA Cholecystitis Perforation Appendicitis OP X-ray Abdominal wall Endoscopy GI bleeding Diverticulitis Pancreatitis Ileus Complex and timeconsuming
Catchment area Teamwork radiology and surgery Jigsaw TRAUMA Cholecystitis Perforation Appendicitis OP X-ray Abdominal wall Endoscopy GI bleeding Diverticulitis Pancreatitis Ileus Complex and timeconsuming
Vacuum-assisted close versus conventional treatment for postlaparotomy wound dehiscence
 ORIGINAL ARTICLE pissn 2288-6575 eissn 2288-6796 http://dx.doi.org/10.4174/astr.2014.87.5.260 Annals of Surgical Treatment and Research Vacuum-assisted close versus conventional treatment for postlaparotomy
ORIGINAL ARTICLE pissn 2288-6575 eissn 2288-6796 http://dx.doi.org/10.4174/astr.2014.87.5.260 Annals of Surgical Treatment and Research Vacuum-assisted close versus conventional treatment for postlaparotomy
Pneumoperitoneum. Laparoscopic instrumentation Access into the abdomen
 Basic Science in Laparoscopic Surgery Contents Pneumoperitoneum Patient positioning Laparoscopic instrumentation Access into the abdomen Laparoscopic Surgery Minimally Invasive Surgery (MIS) Keyhole Surgery
Basic Science in Laparoscopic Surgery Contents Pneumoperitoneum Patient positioning Laparoscopic instrumentation Access into the abdomen Laparoscopic Surgery Minimally Invasive Surgery (MIS) Keyhole Surgery
Early Results after Treatment of Open Abdomen after Aortic Surgery with Mesh Traction and Vacuum-Assisted Wound Closure
 Eur J Vasc Endovasc Surg (2010) 40, 60e64 Early Results after Treatment of Open Abdomen after Aortic Surgery with Mesh Traction and Vacuum-Assisted Wound Closure A. Seternes a, H.O. Myhre a,b, *, T. Dahl
Eur J Vasc Endovasc Surg (2010) 40, 60e64 Early Results after Treatment of Open Abdomen after Aortic Surgery with Mesh Traction and Vacuum-Assisted Wound Closure A. Seternes a, H.O. Myhre a,b, *, T. Dahl
Case Presentation Conference Ravi Dhanisetty, M.D. Kings County Hospital Center
 Case Presentation Morbidity and Mortality Conference Ravi Dhanisetty, M.D. Kings County Hospital Center 1 May 2009 Case Presentation 53 year old male bus driver had a syncopal episode and found down unresponsive.
Case Presentation Morbidity and Mortality Conference Ravi Dhanisetty, M.D. Kings County Hospital Center 1 May 2009 Case Presentation 53 year old male bus driver had a syncopal episode and found down unresponsive.
Mechanical Support in the Failing Fontan-Kreutzer
 Mechanical Support in the Failing Fontan-Kreutzer Stephanie Fuller MD, MS Thomas L. Spray Endowed Chair in Congenital Heart Surgery Associate Professor, The Perelman School of Medicine at the University
Mechanical Support in the Failing Fontan-Kreutzer Stephanie Fuller MD, MS Thomas L. Spray Endowed Chair in Congenital Heart Surgery Associate Professor, The Perelman School of Medicine at the University
Intra-abdominal Pressure as a Criterion for Abdominal Re-exploration INTRODUCTION
 Intra-abdominal Pressure as a Criterion for Abdominal Re-exploration Mohammed Moustafa, Mohammed Mokhtar, Gamal Saleh & Ahmed Moustafa Department of General Surgery Benha University Hospitals, Egypt ABSTRACT
Intra-abdominal Pressure as a Criterion for Abdominal Re-exploration Mohammed Moustafa, Mohammed Mokhtar, Gamal Saleh & Ahmed Moustafa Department of General Surgery Benha University Hospitals, Egypt ABSTRACT
Acute Diverticulitis. Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh
 Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
Renal Transplant Surgery
 Renal Transplant Surgery Mr Somaiah Aroori MS MD EBS in HPB FRCS Consultant HPB & Renal Transplant Surgeon SWTC, Derriford Hospital, Plymouth Over next few minutes Aim to cover Details of Transplant procedure
Renal Transplant Surgery Mr Somaiah Aroori MS MD EBS in HPB FRCS Consultant HPB & Renal Transplant Surgeon SWTC, Derriford Hospital, Plymouth Over next few minutes Aim to cover Details of Transplant procedure
Components separation technique is feasible for assisting delayed primary fascial closure of open abdomen
 https://helda.helsinki.fi Components separation technique is feasible for assisting delayed primary fascial closure of open abdomen Rasilainen, S. K. 2016-03 Rasilainen, S K, Mentula, P J & Leppaniemi,
https://helda.helsinki.fi Components separation technique is feasible for assisting delayed primary fascial closure of open abdomen Rasilainen, S. K. 2016-03 Rasilainen, S K, Mentula, P J & Leppaniemi,
COMPLICATIONS OF HERNIA REPAIR
 COMPLICATIONS OF HERNIA REPAIR Stanley Rogers, MD Associate Clinical Professor of Surgery University of Califronia, San Francisco Paré was respected as a hernia specialist, and was known to have elevated
COMPLICATIONS OF HERNIA REPAIR Stanley Rogers, MD Associate Clinical Professor of Surgery University of Califronia, San Francisco Paré was respected as a hernia specialist, and was known to have elevated
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Preoperative Optimization and Surgical Site Infection Reduction
 Preoperative Optimization and Surgical Site Infection Reduction David Evans, MD Medical Director of Trauma Services Associate Professor Department of Surgery Division of Trauma, Critical Care and Burn
Preoperative Optimization and Surgical Site Infection Reduction David Evans, MD Medical Director of Trauma Services Associate Professor Department of Surgery Division of Trauma, Critical Care and Burn
Preoperative Optimization and Surgical Site Infection Reduction
 Preoperative Optimization and Surgical Site Infection Reduction David Evans, MD Medical Director of Trauma Services Associate Professor Department of Surgery Division of Trauma, Critical Care and Burn
Preoperative Optimization and Surgical Site Infection Reduction David Evans, MD Medical Director of Trauma Services Associate Professor Department of Surgery Division of Trauma, Critical Care and Burn
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: ABDOMINAL WALL, RETROPERITONEUM, UROGENITAL 5-May-2013
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: ABDOMINAL WALL, RETROPERITONEUM, UROGENITAL 5-May-2013
Pulmonary Hypertension Perioperative Management
 Pulmonary Hypertension Perioperative Management Bruce J Leone, MD Professor of Anesthesiology Chief, Neuroanesthesiology Vice Chair for Academic Affairs Mayo Clinic Jacksonville, Florida Introduction Definition
Pulmonary Hypertension Perioperative Management Bruce J Leone, MD Professor of Anesthesiology Chief, Neuroanesthesiology Vice Chair for Academic Affairs Mayo Clinic Jacksonville, Florida Introduction Definition
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Policy No: FCHN.MP Page 1 of 6 Date Originated: Last Review Date Current Revision Date 7/10/07 06/2014 7/2/14
 Page 1 of 6 Date Originated: Last Review Date Current Revision Date 7/10/07 06/2014 7/2/14 SUBJECT: Abdominoplasty, Panniculectomy and Ventral/Incisional Hernia RELATED POLICIES/RELATED DESKTOP PROCEDURES:
Page 1 of 6 Date Originated: Last Review Date Current Revision Date 7/10/07 06/2014 7/2/14 SUBJECT: Abdominoplasty, Panniculectomy and Ventral/Incisional Hernia RELATED POLICIES/RELATED DESKTOP PROCEDURES:
Index. Note: Page numbers of article title are in boldface type.
 Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Demographics. MBSAQIP Case Number: *ACS NSQIP Case Number: *LMRN: *DOB: / / *Gender: Male Female
 Demographics MBSAQIP Case Number: *IDN: *ACS NSQIP Case Number: Name: *LMRN: *DOB: / / *Gender: Male Female *Race: White Black or African American American Indian or Alaska Native Native Hawaiian/Other
Demographics MBSAQIP Case Number: *IDN: *ACS NSQIP Case Number: Name: *LMRN: *DOB: / / *Gender: Male Female *Race: White Black or African American American Indian or Alaska Native Native Hawaiian/Other
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Canadian Trauma Trials Collaborative. Occult Pneumothorax in Critical Care (OPTICC): Standardized Data Collection Sheet
: Standardized Data Collection Sheet") Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Postoperative Surgical Site Infection after Incisional Hernia Repair: Link to Previous Surgical Site Infection? Zulfiqar Ali, AG Rehan
 Original Article Postoperative Surgical Site Infection after Incisional Hernia Repair: Link to Previous Surgical Site Infection? Zulfiqar Ali, AG Rehan ABSTRACT Objective: Aim of the study was to determine
Original Article Postoperative Surgical Site Infection after Incisional Hernia Repair: Link to Previous Surgical Site Infection? Zulfiqar Ali, AG Rehan ABSTRACT Objective: Aim of the study was to determine
Case Study. TRAM Flap Reconstruction with an Associated Complication. Repair using DermaMatrix Acellular Dermis.
 Case Study TRAM Flap Reconstruction with an Associated Complication. Repair using DermaMatrix Acellular Dermis. TRAM Flap Reconstruction with an Associated Complication Challenge Insulin-dependent diabetes
Case Study TRAM Flap Reconstruction with an Associated Complication. Repair using DermaMatrix Acellular Dermis. TRAM Flap Reconstruction with an Associated Complication Challenge Insulin-dependent diabetes
Vacuumed Assisted Closure
 Vacuumed Assisted Closure Louise Morris Lead Nurse in Tissue Viability Jackie Stephen-Haynes Consultant Nurse and senior Lecturer in Tissue Viability 2009 Aims and Objectives To develop an awareness of
Vacuumed Assisted Closure Louise Morris Lead Nurse in Tissue Viability Jackie Stephen-Haynes Consultant Nurse and senior Lecturer in Tissue Viability 2009 Aims and Objectives To develop an awareness of
SUPPLEMENTAL DIGITAL CONTENT 2 : SURGERY SUBGROUPS DEFINITONS AND DISTRIBUTION
 mortality 24h in ICU mortality 24h in ICU 1 SUPPLEMETAL DIGITAL COTET 2 : SURGERY SUBGROUPS DEFIITOS AD DISTRIBUTIO =2,717,902 GHM codes* Surgery description CARDIAC SURGERY 05C021 to 05C034 Cardiac valve(s)
mortality 24h in ICU mortality 24h in ICU 1 SUPPLEMETAL DIGITAL COTET 2 : SURGERY SUBGROUPS DEFIITOS AD DISTRIBUTIO =2,717,902 GHM codes* Surgery description CARDIAC SURGERY 05C021 to 05C034 Cardiac valve(s)
DO NOT DUPLICATE. Negative pressure wound therapy (NPWT) has revolutionized the
 has revolutionized the") Original research WOUNDS 2013;25(4):89 93 From the Aesthetic and Plastic Surgery Institute, University of California Irvine, Orange, CA and Long Beach Memorial Medical Center, Long Beach, CA Address correspondence
Original research WOUNDS 2013;25(4):89 93 From the Aesthetic and Plastic Surgery Institute, University of California Irvine, Orange, CA and Long Beach Memorial Medical Center, Long Beach, CA Address correspondence
EVALUATION OF SELF LEARNING BASED ON WHO MANUAL SURGICAL CARE AT THE DISTRICT HOSPITAL (SCDH)
") EVALUATION OF SELF LEARNING BASED ON WHO MANUAL SURGICAL CARE AT THE DISTRICT HOSPITAL (SCDH) Note: For the answers, refer to the SCDH Manual. The pages listed below each question will contain the answers,
EVALUATION OF SELF LEARNING BASED ON WHO MANUAL SURGICAL CARE AT THE DISTRICT HOSPITAL (SCDH) Note: For the answers, refer to the SCDH Manual. The pages listed below each question will contain the answers,
Management of Traumatic Brain Injury (and other neurosurgical emergencies)
") Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
Historical perspective
 Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
ABDOMINAL COMPARTMENT SYNDROME
 REVIEW ARTICLE ABDOMINAL COMPARTMENT SYNDROME Muhammad Saaiq Department of Surgery, Pakistan Institute of Medical Sciences (PIMS), Islamabad INTRODUCTION AND HISTORICAL BACKGROUND 5 6 cnacer, use of pneumatic
REVIEW ARTICLE ABDOMINAL COMPARTMENT SYNDROME Muhammad Saaiq Department of Surgery, Pakistan Institute of Medical Sciences (PIMS), Islamabad INTRODUCTION AND HISTORICAL BACKGROUND 5 6 cnacer, use of pneumatic
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006.
 Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006 Introduction Laparoscopic surgery started in the mid 1950s. In recent
Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006 Introduction Laparoscopic surgery started in the mid 1950s. In recent
The abdominal compliance measurement to optimize laparoscopy. 2014
 The abdominal compliance measurement to optimize laparoscopy. 2014 J P Mulier Laparoscopic surgery requires most of the time the insufflation of carbon dioxide in the peritoneal cavity under pressure to
The abdominal compliance measurement to optimize laparoscopy. 2014 J P Mulier Laparoscopic surgery requires most of the time the insufflation of carbon dioxide in the peritoneal cavity under pressure to
Conflicts of Interest
 Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
Open abdomen therapy with vacuum-assisted wound closure and mesh-mediated fascial traction
 Open abdomen therapy with vacuum-assisted wound closure and mesh-mediated fascial traction Bjarnason, Thordur 2014 Link to publication Citation for published version (APA): Bjarnason, T. (2014). Open abdomen
Open abdomen therapy with vacuum-assisted wound closure and mesh-mediated fascial traction Bjarnason, Thordur 2014 Link to publication Citation for published version (APA): Bjarnason, T. (2014). Open abdomen
Albumina nel paziente critico. Savona 18 aprile 2007
 Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
3/21/2011. Advances in laparoscopic ventral hernia repair. Laparoscopic approach well-suited for simple hernias:
 Advances in laparoscopic ventral hernia repair Topics Technique of laparoscopic ventral hernia repair Patient selection Is laparoscopic any better than open? Recent advances (or, should we say, advances?)
Advances in laparoscopic ventral hernia repair Topics Technique of laparoscopic ventral hernia repair Patient selection Is laparoscopic any better than open? Recent advances (or, should we say, advances?)
REINFORCED BIOSCAFFOLDS
 REINFORCED BIOSCAFFOLDS Midline Incisional Open OviTex 1S Resorbable Clinical Case Study: Open Abdomen Incisional Herniorrhaphy in Contaminated (CDC Class IV) Operative Field Performed by Dr. Michael Sawyer,
REINFORCED BIOSCAFFOLDS Midline Incisional Open OviTex 1S Resorbable Clinical Case Study: Open Abdomen Incisional Herniorrhaphy in Contaminated (CDC Class IV) Operative Field Performed by Dr. Michael Sawyer,
ANZ Emergency Laparotomy Audit Quality Improvement (ANZELA-QI) Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM
 Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM") ANZ Emergency Laparotomy Audit Quality Improvement (ANZELA-QI) Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM DATA COLLECTION FORM Most Australian hospitals contribute data
ANZ Emergency Laparotomy Audit Quality Improvement (ANZELA-QI) Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM DATA COLLECTION FORM Most Australian hospitals contribute data
Colorectal non-inflammatory emergencies
 Colorectal non-inflammatory emergencies Prof. Hesham Amer Professor of general surgery, Kasr Alainy hospital, Cairo university Dr. Doaa Mansour Dr. Ahmed Nabil Dr. Ahmed Abdel-Salam Lecturers of general
Colorectal non-inflammatory emergencies Prof. Hesham Amer Professor of general surgery, Kasr Alainy hospital, Cairo university Dr. Doaa Mansour Dr. Ahmed Nabil Dr. Ahmed Abdel-Salam Lecturers of general
Management of Complex Wounds with Vacuum Assisted Closure
 Management of Complex Wounds with Vacuum Assisted Closure Wendy McInnes Vascular / Wound Nurse Practitioner The Queen Elizabeth Hospital, Adelaide, South Australia Treasurer ANZSVN wendy.mcinnes@health.sa.gov.au
Management of Complex Wounds with Vacuum Assisted Closure Wendy McInnes Vascular / Wound Nurse Practitioner The Queen Elizabeth Hospital, Adelaide, South Australia Treasurer ANZSVN wendy.mcinnes@health.sa.gov.au
34 yo M presented in ER of KCH at 7/06/10 Painful lump lt groin + vomiting Pain started 2 hrs before presentation. PMH known left inguinal hernia PSH
 Case Presentation 34 yo M presented in ER of KCH at 7/06/10 Painful lump lt groin + vomiting Pain started 2 hrs before presentation. PMH known left inguinal hernia PSH negative NKDA Case Presentation VS:
Case Presentation 34 yo M presented in ER of KCH at 7/06/10 Painful lump lt groin + vomiting Pain started 2 hrs before presentation. PMH known left inguinal hernia PSH negative NKDA Case Presentation VS: