Abdominal pain in children. University of Warmia and Mazury in Olsztyn Faculty of Medical Sciences Department od Clinical Pediatrics
|
|
|
- Winifred Ray
- 5 years ago
- Views:
Transcription

1 Abdominal pain in children University of Warmia and Mazury in Olsztyn Faculty of Medical Sciences Department od Clinical Pediatrics
2 Abdominal pain in childhoodgeneral informations One of the most frequent complaint that brings children to a doctor Steps in reaching the diagnosis: a history, physical examination, laboratory testing, imaging studies, response to therapy Age- a key factor in evaluating the cause Poor sense of onset or location of pain, individual reaction to pain Can be caused by a wide range of surgical and non-surgical conditions
3 Abdominal pain in childhoodgeneral informations Repeated examination may be useful to look for the persistence or evolution of abdominal signs. Some children will have a cause found, however a significant number of children will be diagnosed with nonspecific abdominal pain. Neonates often present due to parental concern over perceived abdominal pain and broad differentials for presentation should be considered. Functional abdominal pain is very common but is a diagnosis of exclusion
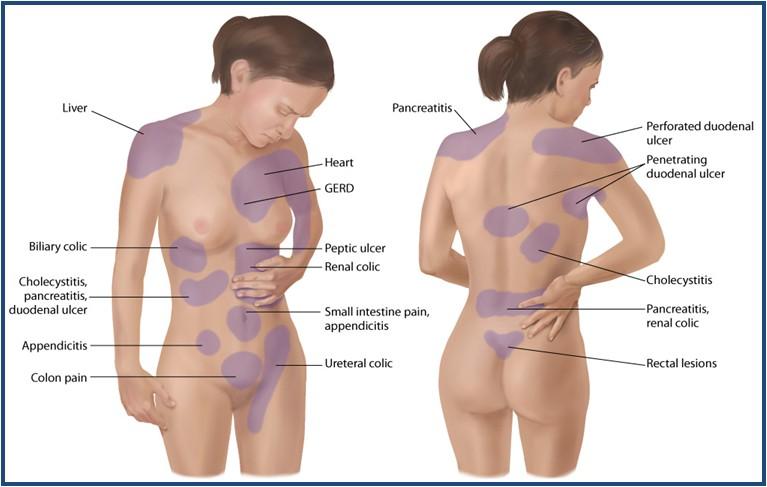
4 Abdominal pain in childhood- pathophysiology Visceral (splanchnic)- sensitization of nerve endings -tension, streching; ischaemia, inflammation *stomach, intestines - dull, poorly localised, *hepatobiliary, pancreatic, gastroduodenal disease- felt in epigastrium, *small and large bowel- periumbilically, *rectosigmoid colon, urinary tract, pelvic organs- suprapubic area Parietal (somatic)- stimulation of parietal peritoneum-sharp, intense, constant, localized, coughing and movement aggravate it Referred- felt in remote areas supplied by the same dermatome
, Character (hurt like needle? butterflies in stomach?, help to lie down? to poop?")
5 Abdominal pain in childhood- types of pain Acute (organic), Chronic (functional) - at least 2 weeks % of children persistent recurrent - 3 or more episodes occurring in 3 months Intensity (1-10 scale, smile to frown to tears face), Character (hurt like needle? butterflies in stomach?, help to lie down? to poop?), Duration of pain, time of day or night

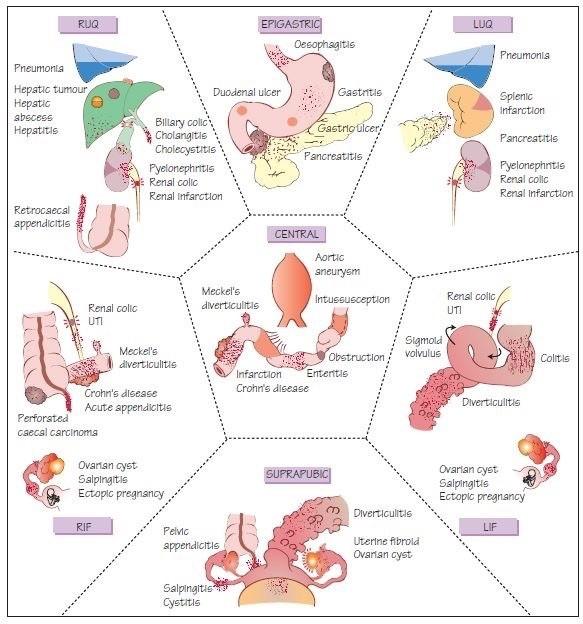
6 Common causes of Abdominal Pain Location- the further the pain from the umbilicus, the greater the likehood of organic disease,
7 Abdominal pain in childhood- differential diagnosis by age B irth to 1 yr: infantile colic, gastroenteritis, constipation, urinary tract infection, intussusception, volvulus, Hirschprung s disease, 2-5 yrs : gastroenteritis, appendicitis, constipation, urinary tract infection, intussusception, volvulus, trauma, pharyngitis, sickle cell crisis, Henoch-Schonlein purpura, mesenteric lymphadenitis, 6-11 yrs : gastroenteritis, appendicitis, constipation, functional pain, urinary tract infection, trauma, pharyngitis, pneumonia, sickle cell crisis, HenochSchonlein purpura, mesenteric lymphadenitis, yrs : appendicitis, gastroenteritis, constipation, dysmenorrhea, pelvic inflammatory disease, threatened abortion, ectopic pregnancy, ovarian/testicular torsion
8 Age- a key factor in evaluating the cause Neonates Infants and Preschool Hirschprung s enterocolitis Appendicitis Incarcerated hernia Intussuception Meckel s diverticulum UTI Volvulus School age child Appendicitis DKA Gastroenteriti Gastroenteritis s Henoch Schonlein Purpura Intussuscepti Mesenteric on adenitis Migraine Pneumonia Ovarian Pathology Pneumonia UTI Constipation Testicular torsion Volvulus UTI Viral Illness Constipation Highlighted in red=time critical illness Adolescents Appendicitis DKA Ectopic pregnancy Cholecystitis/ Cholelithiasis Gastroenteritis Inflammatory Bowel disease Ovarian cysttorsion or rupture Pancreatitis Pelvic Inflammatory Disease Renal calculi Testicular torsion UTI Viral illness

9 History
10 A s s es s m ent H is tory: O ns et o f pa in - sudden onset of pain, consider testicular or ovarian torsion intussusception a medical condition in which a part of the intestine folds into the section next to it, similar to the way the parts of a collapsible telescope retract, this can often result in an obstruction. perforated viscus An organ with an abnormal opening often is referred to as a perforated viscus. Viscus technically means a hollow organ found inside the body. Examples of these hollow organs mostly are found in the chest and abdomen such as the stomach, appendix, intestines, spleen, gallbladder, and urinary bladder.
11 A s s es s m ent H is tory : C ha ra c ter o f pa in- Episodic severe pain intussusception mesenteric adenitis Mesenteric adenitis means inflamed lymph glands in the abdomen, common cause of abdominal pain in children aged under 16 years, the name comes from mesentery- the part of the abdomen where the glands are located, adenitis which means inflamed lymph glands. It is sometimes called mesenteric lymphadenitis. gastroenteritis constipation Testicular torsion in patients with pain referred to the scrotum.
12 A s s es s m ent H is to ry : A s s o c ia ted S ym pto m s o o o o o o o Bilious vomiting implies volvulus or bowel obstruction and warrants surgical review. Pallor and lethargy during episodes of abdominal pain occurs in intussusception. Rash and purpura on extensor surface of lower limbs/buttocks: consider Henoch Schonlein Purpura Cough and fever with RUQ or LUQ pain- pneumonia Dysuria, and frequency - UTI. Polyuria, polydipsia, loss of weight - diabetic ketoacidosis Menstrual and sexual history in post-pubertal girls as ectopic pregnancy can be fatal.
13 A s s es s m ent H is to ry : A s s o c ia ted S ym pto m s o Diarrhea often is associated with gastroenteritis or food poisoning, but it also can occur with other conditions. o Bloody diarrhea is much more suggestive of inflammatory bowel disease or infectious enterocolitis. o The classic currant-jelly stool often is seen in patients with intussusception. o Failure to pass flatus or feces suggests intestinal obstruction o Polyuria and polydipsia suggest diabetes mellitus o Cough, shortness of breath, and chest pain point to a thoracic source.
14 A s s es s m ent H is to ry : stool pattern, consistency, completeness of evacuation, weight loss, growth, pubertal delay, fever, joint complaints, rush, chronic cough a past history of: ulcer disease, gallstone colic gastroesophageal reflux, diarrhea, constipation, jaundice, melena, mucus or blood in stool, hematuria, hematemesis medications family history- peptic disease, irritable colon, inflammatory bowel disease, pancreatitis, biliary disease, travels interference with school, family and peer relations, sexual issues
15 A s s es s m ent H is to ry : P a s t m edic a l his to ry: associated with rarer causes of abdominal pain Hirschprung s disease and Cystic Fibrosis - complicated by enterocolitis with sudden painful abdominal distension and bloody diarrhoea. These patients can rapidly deteriorate with dehydration, electrolyte disturbances and systemic toxicity and are at risk of colonic perforation. Primary bacterial peritonitis can occur in children with liver disease, nephrotic syndrome, splenectomy, ascites and those with VP shunts. Pancreatitis can be caused by drugs including chemotherapy and immunosuppressant agents. Inflammatory bowel disease- toxic megacolon

16 E x a m ina tio n:
17 E x a m ina tio n: Assess hydration status Children with peritonism: - will often not want to move in the bed - be unable to walk or hop comfortably - abdominal tenderness with percussion - internal rotation of the right hip can irritate an inflamed appendix.

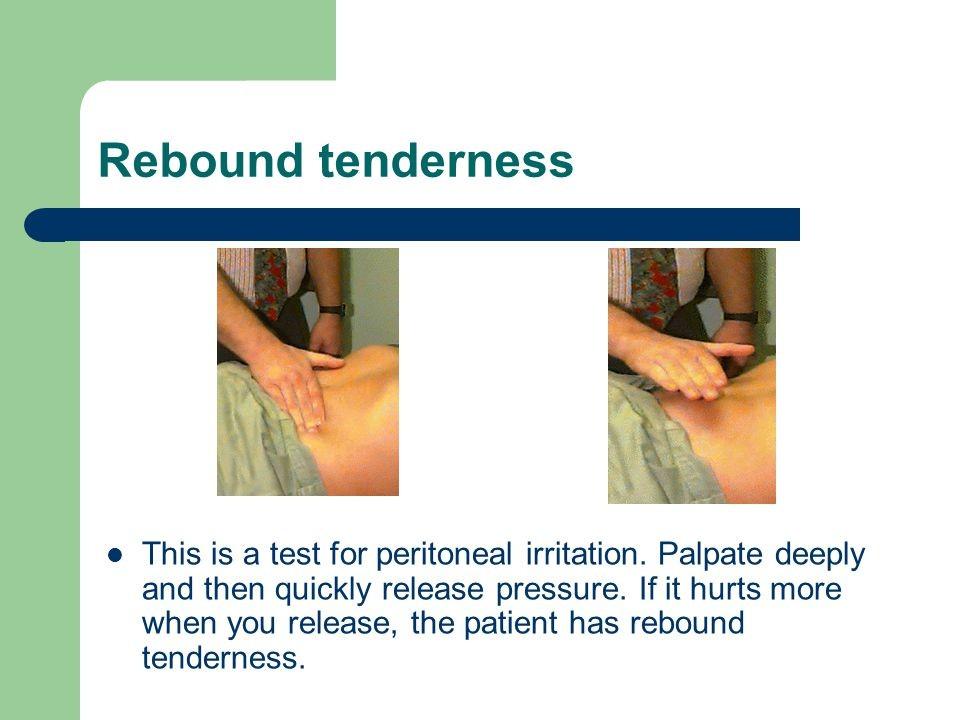
18 E x a m ina tio n: Examine abdomen focal vs generalised tenderness rebound tenderness guarding or rigidity abdominal masses distension palpable faeces Respiratory examination Inguinoscrotal examination including testes, look for hernia Rectal or vaginal exam ination is rarely indicated in a child and should only be perform ed by one person
19



20 I nves tig a tio ns : These will depend on differential diagnosis but may include the following B ut many children need no investigations
21 I nves tig a tio ns : urine blood sugar for DKA electrolytes +/- liver function tests Lipase (pancreatitis) urine pregnancy test/ quantitative beta hcg Coeliac serology and total IgA - consider for chronic abdominal pain Imaging AXR if obstruction suspected. Not helpful in diagnosing constipation. CXR if pneumonia suspected Ultrasound May be requested after discussion with senior staff Is not clinically indicated for testicular torsion.
22 Algorithm for evaluating acute abdominal pain in children.

23 M a na g em ent Treatment should be directed at the underlying cause In many patients, the key to diagnosis is repeated physical examination by the same physician over an extended time Indications for surgical consultations The use of analgesics

24
25 Acute abdominal pain Common- appendicitis, gastroenteritis, dietary indescretion, food poisoning Less common- incarcerated hernia, intussusception, Meckel's diverticulum, mesenteric lymphadenitis, peritonitis, pneumonia, Henoch-Schonlein purpura, viral gastroenteritis, abdominal trauma, rupture of spleen, intestinal obstruction, cholecystitis, cholelithiasis, splenic infarction, pancreatitis, urinary calculi, ectopic pregnancy, ovarian/testicular torsion, diabetic ketoacidosis, porphyria, acute adrenal insufficiency, sickle cell anaemia, hemolityc uremic syndrome
26
27 Acute abdominal pain in childhoodindications for surgical consultations Severe or increasing abdominal pain with progressive signs of deterioration Bile-stained or feculent vomitus Involuntary abdominal guarding/rigitidy Rebound abdominal tenderness Marked abdominal distension with diffuse tympany, no peristalsis Signs of acute fluid or blood loss into the abdomen Significant abdominal trauma Suspected surgical cause for the pain Abdominal pain without obvious etiology
28 Acute abdominal pain in childhoodsurgical emergency Appendicitis Intussusception Meconium peritonitis Intestinal obstruction from atresia Stenosis Esophageal webs Volvulus of a gut
29 Algorithmic approach to the children with acute abdominal pain requiring urgent management
30 Chronic and recurrent abdominal painterminology Chronic and recurrent abdominal pain are common symptoms in children and adolescents Chronic abdominal pain can be organic or nonorganic, depending on whether a specific etiology is identified Nonorganic abdominal pain or functional abdominal pain refers to pain without evidence of anatomic, inflammatory, metabolic, or neoplastic abnormalities Overlap between chronic and recurrent abdominal pain exists, and the terms are sometimes used synonymously.
31 Chronic abdominal pain in children Chronic abdominal pain (long-standing intermittent or constant abdominal pain) is common in children and adolescents In most children, chronic abdominal pain is functional, that is, without objective evidence of an underlying organic disorder Yet, an important part of the physician's job is to determine which children have an organic disorder Children with chronic abdominal pain are more likely than children without chronic abdominal pain to have headache, joint pain, anorexia, vomiting, nausea, excessive gas, and altered bowel symptoms

32 Chronic abdominal pain in children The physician must decide whether to order dia g nos tic tes ts and, if so, which tests. The presence of alarm symptoms or signs suggests a higher pretest probability or prevalence of organic disease and may justify the performance of diagnostic tests.

33 Some causes of abdominal painmore information
, patomechanism: mesentery entrapped venous compression cessation of arterial circulation")
34 Intussusception- a surgical abdomen invagination of one part of intestine into itself age < 1 year, neonates seldom etiology: 90% idiopathic = unknown (2-7%)- viral infection with Peyer s patches enlarged, Meckel s diverticulum, polyps, enteric duplications, Henoch-Schonlein purpura, tumors (lymphoma), patomechanism: mesentery entrapped venous compression cessation of arterial circulation ischemia necrosis localisation: 75% ileocolic, 15% ileo-ileocolic, 10% ileoileal, colocolic
+ treatment (hydrostatic reduction)-5%")
35 Intussusception- a surgical abdomen symptoms: colicky abdominal pain with intervals of wellness, bloody stools- red jelly, projectile vomiting asymptomatic- altered states of consciousness physical examination: sausage shaped mass, intensic peristaltic movements ahead, silence behind the intussusception diagnosis: usg, barium enema (ileocecal junction)+ treatment (hydrostatic reduction)-5% reccurent surgical reduction-3% recurrence rate

36 Intussusception- radiology


37 Intussusception- barium enema
38 Pyloric Stenosis More common in boys than girls First born most commonly affected Family history in 10% patients Unexplained hypertrophy of the circular muscles of the pylorus develops Short history of vomiting in a baby of 2-8weeks of age Vomit may contain altered blood, non bile stained Upper abdo may be distended, visible gastric
39 Hirschprung's disease Etiology- congenital abnormality- inheritance pattern autosomal dominant with reduced penetrance (risk closer to 50%), mutations inactivating RET gene cause a susceptibility to HD, defective stem cells? Epidemiology: 1/5000 newborn Result- the absence of ganglion cells (parasympathetic ganglion cells) from the myenteric and submucosal plexuses of part of the large bowel due to changes in the proliferation, survival and migration of neural crest cells, narrow, contracted segment (75%-rectosigmoid, 10% entire colon), secondary dilatation of proximal colon
40 Hirschprung's disease Symptoms: first 24 hours of life- intestinal obstruction meconium ileus, abominal distention, bile-stained vomiting, constipation, fever, enterocolitis, dehydratation, death if not treated Rectal examination- narrow segment Treatment: surgery in 2 stages: colostomy with the creation of stoma, closure of stoma with remove of narrow part of bowel, perform a pull-through procedure to connect functional bowel to anus
, the localisation")
41 Hirschprung disease- abdomen distention (left), the localisation (right)


42 Hirschprung disease- megacolon



43 Hirschprung disease- dilatation of colon, narrow rectum
, 2 feet from ileocecal valve, 2 inches in length, 2 types of ectopic")

44 Meckel s diverticulum Most common congenital anomaly involving the small bowel and terminal ileum (2% of population), 2:1- male: female Remnant of omphalomesenteric duct (Vitelline duct), 2 feet from ileocecal valve, 2 inches in length, 2 types of ectopic tissue: gastric and pancreatic Symptoms: asymptomatic, (2% symptomatic)- most < 2 yrs of life, hemorrhage, intussusception, volvulus, diverticulitis 2 main complications: bleeding, obstruction Diagnosis: scintigraphy with 99Tc-pertechnetate, sensitivity and specificity is 85-95%.
45 Abdominal pain in childhoodmesenteric lymphadenitis Poorly defined symptoms MA is self limited inflammatory process that affects the mesenteric lymph nodes in RLQ Thought that inflammation of mesenteric lymph nodes leads to peritoneal reaction Site of tenderness may shift when child moves position active observation useful Leucocytosis is common Diagnosis is one of exclusion Ultrasound A persisting localized tenderness lasting more than 3-6hrs may warrant surgical exploration
")

46 Volvulus Malrotation of bowel may predispose infant to volvulus Bowel become twisted Up to 90% in children younger than 1yr ( up to 60% in 1st month of life) Male: female presentations 2:1 Babies who present in first week of life tend to have more severe obstruction Bilious vomiting, apnoeic episodes, bloody stool, abdo pain, shock

. The testicle becomes sore and extremely tender.")
47 Testicular Torsion Teenage boys May occur from strenuous exercise or injury, or no apparent cause Sudden and severe pain. Swelling and tenderness on the side of scrotum that is affected (more often on the right side). The testicle becomes sore and extremely tender. Associated nausea and vomiting The scrotum may also become red and inflamed Surgery needed within 6 hours
48 Clinical features Organic Site of pain Flanks, suprapubic, RUQ, Central, epigastric RLQ Family History- particularly of abdo pain, headache and depression Less likely, but take note Likely of IBS Psychological factors particularly anxiety Less likely Likely, especially anxiety Headache Less likely More likely Alarm symptoms Vomiting generally equally likely but beware persistent or significant vomiting. Chronic severe diarrhoea more likely. Unexplained fever. Gastrointestinal blood Present loss. Present Alarm symptoms less likely Expected Not found Abnormal signs Abnormal growth/ and or weight loss Abnormal investigations Non organic Absent Absent
49
50 a diagnostic dilemma! many cases of abdominal pain are benign, some require rapid diagnosis and treatment to minimize morbidity numerous disorders can cause abdominal pain the most common medical cause is gastroenteritis, and the most common surgical cause is appendicitis in most instances, abdominal pain can be diagnosed through the history and physical examination. age is a key factor in evaluating the cause in the acute surgical abdomen, pain generally precedes vomiting, while the reverse is true in medical conditions
51 diarrhea often is associated with gastroenteritis or food poisoning appendicitis should be suspected in any child with pain in the right lower quadrant signs that suggest an acute surgical abdomen include involuntary guarding or rigidity, marked abdominal distention, marked abdominal tenderness, and rebound abdominal tenderness. selected imaging studies also might be helpful surgical consultation is necessary if a surgical cause is suspected or the cause is not obvious after a thorough evaluation.
: Abdominal Emergencies
 INTRODUCTION Abdominal complaints are very common in emergency medicine. The specific cause of the abdominal pain can very rarely be determined in the pre-hospital environment, however performing a good
INTRODUCTION Abdominal complaints are very common in emergency medicine. The specific cause of the abdominal pain can very rarely be determined in the pre-hospital environment, however performing a good
Pathology of Intestinal Obstruction. Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College
 Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
Vomiting in children: The good coordination between radiologists and pediatricians is the key to success
 Vomiting in children: The good coordination between radiologists and pediatricians is the key to success C. Santos Montón 1, M. T. Garzon Guiteria 2, A. Hortal Benito-Sendín 1, K. El Karzazi 1, P. Sanchez
Vomiting in children: The good coordination between radiologists and pediatricians is the key to success C. Santos Montón 1, M. T. Garzon Guiteria 2, A. Hortal Benito-Sendín 1, K. El Karzazi 1, P. Sanchez
Good morning! July 24, 2014
 Good morning! July 24, 2014 Prep #1 A 2-year-old boy presents to your office with a 2-day history of swelling of the right eye. He has been otherwise well. There are scattered insect bites on his body,
Good morning! July 24, 2014 Prep #1 A 2-year-old boy presents to your office with a 2-day history of swelling of the right eye. He has been otherwise well. There are scattered insect bites on his body,
Chapter 24 - Abdominal_Emergencies
 Introduction to Emergency Medical Care 1 OBJECTIVES 24.1 Define key terms introduced in this chapter. 13, 15, 18, 20 22 24.2 Describe the location, structure, and function of the organs in the abdominal
Introduction to Emergency Medical Care 1 OBJECTIVES 24.1 Define key terms introduced in this chapter. 13, 15, 18, 20 22 24.2 Describe the location, structure, and function of the organs in the abdominal
Abdominal & scrotal pain
 Abdominal & scrotal pain Junior Teach Emergency Department 1 Created by SR Bruijns 03/11/2010 Objectives Understanding of, and emergency management of Acute abdominal pain Undifferentiated abdominal pain
Abdominal & scrotal pain Junior Teach Emergency Department 1 Created by SR Bruijns 03/11/2010 Objectives Understanding of, and emergency management of Acute abdominal pain Undifferentiated abdominal pain
Topics for discussion. Pediatric General Surgery. Physiology. Surgical Newborns. Neonatal Intestinal Obstruction
 Topics for discussion Pediatric General Surgery Professor General & Thoracic Surgery What makes Pediatric Surgery unique? Neonatal intestinal obstruction Abdominal wall defects Inguinal hernias Appendicitis
Topics for discussion Pediatric General Surgery Professor General & Thoracic Surgery What makes Pediatric Surgery unique? Neonatal intestinal obstruction Abdominal wall defects Inguinal hernias Appendicitis
Gastro- Intestinal Bleeding in Children
 Gastro- Intestinal Bleeding in Children Upper G1 Bleeding. Lower G1 Bleeding. Upper G1 Bleeding :- Presentation : Hematemesis Causes :- Neonate reflux esophagitis (dark, small amount) PyLoric stenosis
Gastro- Intestinal Bleeding in Children Upper G1 Bleeding. Lower G1 Bleeding. Upper G1 Bleeding :- Presentation : Hematemesis Causes :- Neonate reflux esophagitis (dark, small amount) PyLoric stenosis
VOMITING. Tan Lay Zye
 VOMITING Tan Lay Zye Vomiting is a common symptom. It is a complex reflex behavioural response involving forceful expulsion of the stomach contents through oral cavity. Contents Emetic reflex Causes of
VOMITING Tan Lay Zye Vomiting is a common symptom. It is a complex reflex behavioural response involving forceful expulsion of the stomach contents through oral cavity. Contents Emetic reflex Causes of
Causes of abdominal pain Doctors in the ED spend lots of time and money diagnosing abdominal pain. They still often do not know the exact cause
 1 2 3 What's Going On in There? EMS and Abdominal Pain Kevin McFarlane BSN,RN,CEN,CPEN,EMT Southwest Emergency Education and Consulting What is going on in there Acute Abdomen Sudden onset of pain within
1 2 3 What's Going On in There? EMS and Abdominal Pain Kevin McFarlane BSN,RN,CEN,CPEN,EMT Southwest Emergency Education and Consulting What is going on in there Acute Abdomen Sudden onset of pain within
Chapter Outline. Structural defects. Obstructive disorders. Preview from Notesale.co.uk Page 3 of 98. Cleft lip and cleft palate
 Structural defects Chapter Outline Cleft lip and cleft palate Page 3 of 98 Esophageal atresia and tracheoesophageal fistula Hernias Obstructive disorders Hypertrophic pyloric stenosis Intussusception Anorectal
Structural defects Chapter Outline Cleft lip and cleft palate Page 3 of 98 Esophageal atresia and tracheoesophageal fistula Hernias Obstructive disorders Hypertrophic pyloric stenosis Intussusception Anorectal
Intestinal Obstruction Clinical Presentation & Causes
 Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Abdominal Pain in Pediatric Patients Image Gently
 Abdominal Pain in Pediatric Patients Image Gently Susan D. John, M.D. Baptist Health Emergency Radiology 2017 Disclosure I have no financial relationships with a commercial entity producing healthcarerelated
Abdominal Pain in Pediatric Patients Image Gently Susan D. John, M.D. Baptist Health Emergency Radiology 2017 Disclosure I have no financial relationships with a commercial entity producing healthcarerelated
Interesting Pediatric ultrasound cases. Presented by: Falguni Patel (RDMS, RVT)
") Interesting Pediatric ultrasound cases Presented by: Falguni Patel (RDMS, RVT) Role of ultrasound to rule out Appendicitis Overview: Ultrasound is relatively inexpensive, safe and quick solution to rule
Interesting Pediatric ultrasound cases Presented by: Falguni Patel (RDMS, RVT) Role of ultrasound to rule out Appendicitis Overview: Ultrasound is relatively inexpensive, safe and quick solution to rule
Pediatric Surgical Emergencies Veronica Victorian, PA-C
 Pediatric Surgical Emergencies Veronica Victorian, PA-C Texas Children s Hospital Division of Pediatric General Surgery Assistant Professor, Baylor College of Medicine Objectives 1. Define Pediatric Surgical
Pediatric Surgical Emergencies Veronica Victorian, PA-C Texas Children s Hospital Division of Pediatric General Surgery Assistant Professor, Baylor College of Medicine Objectives 1. Define Pediatric Surgical
PEDIATRIC GI EMERGENCIES. AGE-RELATED DIAGNOSIS Early Infancy EXAMINATION TIPS PEDIATRIC ABDOMINAL PAIN. How Common Is It?
 PEDIATRIC ABDOMINAL PAIN How Common Is It? PEDIATRIC GI EMERGENCIES Ghazala Q. Sharieff, MD 5% of unscheduled visits 2% of patients are admitted 1% need operative intervention EXAMINATION TIPS Palpate
PEDIATRIC ABDOMINAL PAIN How Common Is It? PEDIATRIC GI EMERGENCIES Ghazala Q. Sharieff, MD 5% of unscheduled visits 2% of patients are admitted 1% need operative intervention EXAMINATION TIPS Palpate
An Approach to Abdominal Pain
 An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
Gastrointestinal & Genitourinary Emergencies. Lesson Goal. Learning Objectives 9/10/2012
 Gastrointestinal & Genitourinary Emergencies Lesson Goal Recognize, assess & provide care to patients with abdominal cavity injuries Learning Objectives Discuss different causes of nontraumatic abdominal
Gastrointestinal & Genitourinary Emergencies Lesson Goal Recognize, assess & provide care to patients with abdominal cavity injuries Learning Objectives Discuss different causes of nontraumatic abdominal
Summary and conclusions
 Summary and conclusions 7 Chapter 7 68 Summary and conclusions Chapter 1 provides a general introduction to this thesis focused on the use of ultrasound (US) in children with abdominal problems. The literature
Summary and conclusions 7 Chapter 7 68 Summary and conclusions Chapter 1 provides a general introduction to this thesis focused on the use of ultrasound (US) in children with abdominal problems. The literature
Chapter Goal. Learning Objectives 9/12/2012. Chapter 29. Nontraumatic Abdominal Injuries
 Chapter 29 Nontraumatic Abdominal Injuries Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with nontraumatic abdominal pain Learning Objectives
Chapter 29 Nontraumatic Abdominal Injuries Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with nontraumatic abdominal pain Learning Objectives
Abdominal pain. Mohamed Ahmed Fouad Pediatric Lecturer Jazan Faculty of Medicine
 Abdominal pain Mohamed Ahmed Fouad Pediatric Lecturer Jazan Faculty of Medicine Objectives Understand the principal causes of acute abdominal pain in children. Describe the characteristics of visceral
Abdominal pain Mohamed Ahmed Fouad Pediatric Lecturer Jazan Faculty of Medicine Objectives Understand the principal causes of acute abdominal pain in children. Describe the characteristics of visceral
Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of Pediatrics UMDNJ RWJMS
 Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of Pediatrics UMDNJ RWJMS Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of
Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of Pediatrics UMDNJ RWJMS Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of
Objectives. Pediatric Mortality. Another belly pain. Gastroenteritis. Spewing & Pooing Child 4/18/16
 Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
Surgical Education Series
 Surgical Education Series The Acute Abdomen Ahmad kachooei, MD MPH Assistant Professor Division of General Surgery Department of Surgery University of Qom Outline Definitions What causes an acute abdomen
Surgical Education Series The Acute Abdomen Ahmad kachooei, MD MPH Assistant Professor Division of General Surgery Department of Surgery University of Qom Outline Definitions What causes an acute abdomen
Document Title: Non-Traumatic Abdominal Pain/Abdominal Emergencies. Author(s): Joseph House (University of Michigan), MD 2012
: Joseph House (University of Michigan), MD 2012") Project: Ghana Emergency Medicine Collaborative Document Title: Non-Traumatic Abdominal Pain/Abdominal Emergencies Author(s): Joseph House (University of Michigan), MD 2012 License: Unless otherwise noted,
Project: Ghana Emergency Medicine Collaborative Document Title: Non-Traumatic Abdominal Pain/Abdominal Emergencies Author(s): Joseph House (University of Michigan), MD 2012 License: Unless otherwise noted,
Emergent Pediatric Ultrasound. Katharine Dennis, RDMS/RVT Tiffany Schultz, RDMS UNC Health Care Dept of General Ultrasound
 Emergent Pediatric Ultrasound Katharine Dennis, RDMS/RVT Tiffany Schultz, RDMS UNC Health Care Dept of General Ultrasound Introduction Learning Objectives Review common pediatric emergent ultrasound exams
Emergent Pediatric Ultrasound Katharine Dennis, RDMS/RVT Tiffany Schultz, RDMS UNC Health Care Dept of General Ultrasound Introduction Learning Objectives Review common pediatric emergent ultrasound exams
DR JAIKISHOR JOTHIRAJ MD POST GRADUATE DEPT OF RADIODIAGNOSIS
 DR JAIKISHOR JOTHIRAJ MD POST GRADUATE DEPT OF RADIODIAGNOSIS YASHODAMMAL 70 YRS OD LADY had C/o diffuse lower abdominal pain 20 days h/o blood in stools 4 days h/o vomiting 2 days h/o burning micturation
DR JAIKISHOR JOTHIRAJ MD POST GRADUATE DEPT OF RADIODIAGNOSIS YASHODAMMAL 70 YRS OD LADY had C/o diffuse lower abdominal pain 20 days h/o blood in stools 4 days h/o vomiting 2 days h/o burning micturation
Pediatric Bowel Obstruction
 Pediatric Bowel Obstruction Matt Zerden, Harvard Medical School III Patient 1 16 year old presents with severe, episodic abdominal pain, nausea and vomiting. Questionable abdominal mass in RLQ Previous
Pediatric Bowel Obstruction Matt Zerden, Harvard Medical School III Patient 1 16 year old presents with severe, episodic abdominal pain, nausea and vomiting. Questionable abdominal mass in RLQ Previous
PEDIATRIC EMERGENCY DEPARTMENT CLINICAL GUIDELINE: GI SURGICAL EMERGENCIES: VOMITING
 GI SURGICAL EMERGENCIES: VOMITING PYLORIC STENOSIS Population: Infants: onset between 2-5 weeks of age 1 in 250 births Male: female ratio 4:1 Familial incidence History: No vomiting in the first few weeks
GI SURGICAL EMERGENCIES: VOMITING PYLORIC STENOSIS Population: Infants: onset between 2-5 weeks of age 1 in 250 births Male: female ratio 4:1 Familial incidence History: No vomiting in the first few weeks
SAEMS ABDOMINAL PAIN STANDING ORDER Self-Learning Module
 SAEMS ABDOMINAL PAIN STANDING ORDER Self-Learning Module Dawn Daniels Tucson Medical Center January 2016 PURPOSE This SAEMS Standing Order Training Module has been developed to serve as a template for
SAEMS ABDOMINAL PAIN STANDING ORDER Self-Learning Module Dawn Daniels Tucson Medical Center January 2016 PURPOSE This SAEMS Standing Order Training Module has been developed to serve as a template for
ACUTE ABDOMEN. Dr. M Asadi. Surgical Oncology Research Center MUMS. Assistant Professor of General Surgery
 ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
ACUTE ABDOMEN IN OLDER CHILDREN. Carlos J. Sivit M.D.
 ACUTE ABDOMEN IN OLDER CHILDREN Carlos J. Sivit M.D. ACUTE ABDOMEN Clinical condition characterized by severe abdominal pain developing over several hours ACUTE ABDOMINAL PAIN Common childhood complaint
ACUTE ABDOMEN IN OLDER CHILDREN Carlos J. Sivit M.D. ACUTE ABDOMEN Clinical condition characterized by severe abdominal pain developing over several hours ACUTE ABDOMINAL PAIN Common childhood complaint
Sonographic Appearances of Common Gut Pathology in Paediatric Patients: Comparison with Plain Abdominal Radiography
 3668 Radiographer Text 1/4/04 2:57 PM Page 11 The Radiographer vol. 51: 11-17 Sonographic Appearances of Common Gut Pathology in Paediatric Patients: Comparison with Plain Abdominal Radiography Lino Piotto
3668 Radiographer Text 1/4/04 2:57 PM Page 11 The Radiographer vol. 51: 11-17 Sonographic Appearances of Common Gut Pathology in Paediatric Patients: Comparison with Plain Abdominal Radiography Lino Piotto
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
Spleen indications of splenectomy complications OPSI
 Intestinal obstruction Differences between adynamic ileus and mechanical obstruction Aetiology Pathophysiology (Cluster contractions- bowel proximal to the obstruction dilate- wall of obstructed gut is
Intestinal obstruction Differences between adynamic ileus and mechanical obstruction Aetiology Pathophysiology (Cluster contractions- bowel proximal to the obstruction dilate- wall of obstructed gut is
Hirschprung s. Meconium plug R/S >1 R/S <1
 NEONATAL ABDOMINAL EMERGENCIES LOW OBSTRUCTION HIGH OBSTRUCTION INTESTINAL OBSTRUCTION High obstruction - proximal to mid-ileumileum Few dilated, air filled bowel loops Complete obstruction diagnosed by
NEONATAL ABDOMINAL EMERGENCIES LOW OBSTRUCTION HIGH OBSTRUCTION INTESTINAL OBSTRUCTION High obstruction - proximal to mid-ileumileum Few dilated, air filled bowel loops Complete obstruction diagnosed by
Objectives: Resources:
 Objectives: Realize the impact of Age : - Where/who are the history sources Recognize and interpret the : - Important symptoms - Important signs Resources: Davidson s. Slides Surgical recall. Raslan s
Objectives: Realize the impact of Age : - Where/who are the history sources Recognize and interpret the : - Important symptoms - Important signs Resources: Davidson s. Slides Surgical recall. Raslan s
Evidence Process for Abdominal Pain Guideline Research 11/16/2017. Guideline Review using ADAPTE method and AGREE II instrument 11/16/2017
 Evidence Process for Abdominal Pain Guideline Research Guideline Review using ADAPTE method and AGREE II instrument Approximately 139 Potentially relevant guidelines identified in various resources* 59
Evidence Process for Abdominal Pain Guideline Research Guideline Review using ADAPTE method and AGREE II instrument Approximately 139 Potentially relevant guidelines identified in various resources* 59
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Always keep it in the differential
 Acute Appendicitis Lissa C. Sakata and Lindsey Perea 2 Always keep it in the differential Learning Objectives 1. The learner should be able to describe the etiology of acute appendicitis. 2. The learner
Acute Appendicitis Lissa C. Sakata and Lindsey Perea 2 Always keep it in the differential Learning Objectives 1. The learner should be able to describe the etiology of acute appendicitis. 2. The learner
GI POTPOURRI. What is the best diagnostic test? Presentation #1: Vomiting. I have no disclosures
 I have no disclosures GI POTPOURRI Andi Marmor, MD Associate Professor, Pediatrics UCSF, San Francisco General Hospital Presentation #1: Vomiting Caraway, a 3 week old boy, is brought to your walk-in clinic
I have no disclosures GI POTPOURRI Andi Marmor, MD Associate Professor, Pediatrics UCSF, San Francisco General Hospital Presentation #1: Vomiting Caraway, a 3 week old boy, is brought to your walk-in clinic
HCPCS Codes (Alphanumeric, CPT AMA) ICD-9-CM Codes Covered by Medicare Program
 ICD-9-CM Codes Covered by Medicare Program") HCPCS s (Alphanumeric, CPT AMA) 82272 Blood, occult, by peroxidase activity (e.g., guaiac), qualitative, feces, 1-3 simultaneous determinations, performed for other than colorectal neoplasm screening ICD-9-CM
HCPCS s (Alphanumeric, CPT AMA) 82272 Blood, occult, by peroxidase activity (e.g., guaiac), qualitative, feces, 1-3 simultaneous determinations, performed for other than colorectal neoplasm screening ICD-9-CM
USMLE and COMLEX II. CE / CK Review. General Surgery. 1. Northwestern Medical Review
 USMLE and COMLEX II CE / CK Review General Surgery 1. Northwestern Medical Review Northwestern Medical Review www.northwesternmedicalreview.com Lansing, Michigan 2014-2015 Acute Abdomen 1. Your patient
USMLE and COMLEX II CE / CK Review General Surgery 1. Northwestern Medical Review Northwestern Medical Review www.northwesternmedicalreview.com Lansing, Michigan 2014-2015 Acute Abdomen 1. Your patient
Abdominal Assessment
 Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
Small Bowel and Colon Surgery
 Small Bowel and Colon Surgery Why Do I Need a Small Bowel Resection? A variety of conditions can damage your small bowel. In severe cases, your doctor may recommend removing part of your small bowel. Conditions
Small Bowel and Colon Surgery Why Do I Need a Small Bowel Resection? A variety of conditions can damage your small bowel. In severe cases, your doctor may recommend removing part of your small bowel. Conditions
Gastrointestinal Disorders. Disorders of the Esophagus 3/7/2013. Congenital Abnormalities. Achalasia. Not an easy repair. Types
 Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Abdo Pain rules & regulations. Mark Hartnell 2010
 Abdo Pain rules & regulations Mark Hartnell 2010 Aims Simple rules which might help in patients with abdominal pain Talk about some myths and realities Discuss some practical how to s in day to day treatment
Abdo Pain rules & regulations Mark Hartnell 2010 Aims Simple rules which might help in patients with abdominal pain Talk about some myths and realities Discuss some practical how to s in day to day treatment
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC
 Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Abdominal Examination Benchmarks
 Abdominal Examination Benchmarks Preparation and Positioning: Stand on the right side of the patient. The patient should be supine and double draped so only the abdomen is exposed o To relax the abdominal
Abdominal Examination Benchmarks Preparation and Positioning: Stand on the right side of the patient. The patient should be supine and double draped so only the abdomen is exposed o To relax the abdominal
Chapter 18 - Gastrointestinal & Urologic Emergencies
 1 2 3 4 5 6 7 8 Chapter 18 Gastrointestinal and Urologic National EMS Education Standard Competencies (1 of 4) Medicine Applies fundamental knowledge to provide basic emergency care and transportation
1 2 3 4 5 6 7 8 Chapter 18 Gastrointestinal and Urologic National EMS Education Standard Competencies (1 of 4) Medicine Applies fundamental knowledge to provide basic emergency care and transportation
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal pain, abdominal considerations in, 183 184 antiemetics in, 182 auscultation in, 170 C-reactive protein in, 174 175 character
Index Note: Page numbers of article titles are in boldface type. A Abdominal pain, abdominal considerations in, 183 184 antiemetics in, 182 auscultation in, 170 C-reactive protein in, 174 175 character
12 Blueprints Q&A Step 2 Surgery
 12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 20 Caring for Clients with Bowel Disorders Diarrhea Pathophysiology Result from impaired water absorption
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 20 Caring for Clients with Bowel Disorders Diarrhea Pathophysiology Result from impaired water absorption
Episode 19 part 2 Pediatric Abdominal Pain Prepared by Dr. Lucas Chartier
 Episode 19 part 2 Pediatric Abdominal Pain Prepared by Dr. Lucas Chartier GASTROENTERITIS History: Common diagnosis but may hide sinister pathology, so consider it a diagnosis of exclusion In cases of
Episode 19 part 2 Pediatric Abdominal Pain Prepared by Dr. Lucas Chartier GASTROENTERITIS History: Common diagnosis but may hide sinister pathology, so consider it a diagnosis of exclusion In cases of
Pediatric abdominal emergencies In the first year of life
 Common Pediatric abdominal emergencies In the first year of life Kristian Stien Thomassen Section of Pediatric Radiology Dept. of Radiology and Nuclear Medicine Oslo University Hospital Understand the
Common Pediatric abdominal emergencies In the first year of life Kristian Stien Thomassen Section of Pediatric Radiology Dept. of Radiology and Nuclear Medicine Oslo University Hospital Understand the
F A M N O P R S ! D !
 A B C D E F A M N O P Q G H I J R S T U V 595 W http://www.encognitive.com/images/digestive-system-2.jpg K L M A N B C O P D E F G D Q R H S I J K http://apbrwww5.apsu.edu/thompsonj/anatomy%20&%20physiology/2020/2020%20exam%20reviews/exam%203/colon%20diagram.jpgd
A B C D E F A M N O P Q G H I J R S T U V 595 W http://www.encognitive.com/images/digestive-system-2.jpg K L M A N B C O P D E F G D Q R H S I J K http://apbrwww5.apsu.edu/thompsonj/anatomy%20&%20physiology/2020/2020%20exam%20reviews/exam%203/colon%20diagram.jpgd
Department of Pediatrics, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea
 pissn: 2234-8646 eissn: 2234-8840 http://dx.doi.org/10.5223/pghn.2013.16.4.219 Pediatr Gastroenterol Hepatol Nutr 2013 December 16(4):219-224 Review Article PGHN Acute Abdominal Pain in Children Joon Sung
pissn: 2234-8646 eissn: 2234-8840 http://dx.doi.org/10.5223/pghn.2013.16.4.219 Pediatr Gastroenterol Hepatol Nutr 2013 December 16(4):219-224 Review Article PGHN Acute Abdominal Pain in Children Joon Sung
Adult Intussusception: A Complication of Metastatic Melanoma or Primary Malignancy?
 January 2013 Adult Intussusception: A Complication of Metastatic Melanoma or Primary Malignancy? Johanna Sheu, Harvard Medical School Year III 1 Agenda Menu of tests Definition/anatomy/classification Pediatrics
January 2013 Adult Intussusception: A Complication of Metastatic Melanoma or Primary Malignancy? Johanna Sheu, Harvard Medical School Year III 1 Agenda Menu of tests Definition/anatomy/classification Pediatrics
NCD for Fecal Occult Blood Test
 NCD for Fecal Occult Blood Test Applicable CPT Code(s): 82272 Blood, occult, by peroxidase activity (e.g., guaiac), qualitative, feces, 1-3 simultaneous determinations, performed for other than colorectal
NCD for Fecal Occult Blood Test Applicable CPT Code(s): 82272 Blood, occult, by peroxidase activity (e.g., guaiac), qualitative, feces, 1-3 simultaneous determinations, performed for other than colorectal
Health Center Krusevac, Department of Surgery, Krusevac, Serbia
 Health Center Krusevac, Department of Surgery, Krusevac, Serbia SURGICAL TREATMENT OF MECKEL S DIVERTICULUM Milan Jovanovic, R. Zdravkovic, S. Zajic, M. Smiljkovic, V. Kulic, A. Kitanovic, G. Filipovic,
Health Center Krusevac, Department of Surgery, Krusevac, Serbia SURGICAL TREATMENT OF MECKEL S DIVERTICULUM Milan Jovanovic, R. Zdravkovic, S. Zajic, M. Smiljkovic, V. Kulic, A. Kitanovic, G. Filipovic,
Abdominal Pain. Luke Donnelly, MD Emergency Medicine
 Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Scrotal pain and Swelling
 Scrotal pain and Swelling Color index : Important Further explanation Done By: Nada Alamri Editing link Acute Scrotal Pain DDx: 1) Testicular torsion : Twisting and strangulation of the testicle on the
Scrotal pain and Swelling Color index : Important Further explanation Done By: Nada Alamri Editing link Acute Scrotal Pain DDx: 1) Testicular torsion : Twisting and strangulation of the testicle on the
Sick or not sick? Objectives. Bilious vomiting. Deadly Misdiagnoses: Kids with GI Complaints. Ronald Dieckmann, MD. Problems in assessment
 Deadly Misdiagnoses: Kids with GI Complaints Objectives Understand key assessment techniques for recognition of serious illness in children. Ronald Dieckmann, MD Professor of Clinical Pediatrics and Emergency
Deadly Misdiagnoses: Kids with GI Complaints Objectives Understand key assessment techniques for recognition of serious illness in children. Ronald Dieckmann, MD Professor of Clinical Pediatrics and Emergency
OBJECTIVES VISCERAL PAIN RECEPTORS LOCATION & NATURE OF THE PAIN LOCATION OF VISCERAL PAIN RECEPTORS 4/12/2018. Nancy Brown, APRN, CPNP April 18, 2018
 Nancy Brown, APRN, CPNP April 18, 2018 OBJECTIVES 1. Understand the principle causes of acute abdominal pain in children. 2. Make symptom based diagnoses of functional abdominal pain in children. 3. Recognize
Nancy Brown, APRN, CPNP April 18, 2018 OBJECTIVES 1. Understand the principle causes of acute abdominal pain in children. 2. Make symptom based diagnoses of functional abdominal pain in children. 3. Recognize
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients).
.") Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
Cecal Volvulus: Case Presentation and Review of CT Findings
 August 2011 Cecal Volvulus: Case Presentation and Review of CT Findings Omar Pardesi, Harvard Medical School Year III Our Patient LD: History & Physical HPI: 28 y.o. female presents with diffuse abdominal
August 2011 Cecal Volvulus: Case Presentation and Review of CT Findings Omar Pardesi, Harvard Medical School Year III Our Patient LD: History & Physical HPI: 28 y.o. female presents with diffuse abdominal
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Approach to Abdominal Mass Part 1. These podcasts are designed to give medical students an overview of key topics in
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Approach to Abdominal Mass Part 1. These podcasts are designed to give medical students an overview of key topics in
Suspected Foreign Body Ingestion
 Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdomen, surgery of, abdominal pain and, 163 vascular anatomy of, 253 255 Abdominal aortic aneurysm, 264 266 Abdominal emergencies, vascular,
Note: Page numbers of article titles are in boldface type. A Abdomen, surgery of, abdominal pain and, 163 vascular anatomy of, 253 255 Abdominal aortic aneurysm, 264 266 Abdominal emergencies, vascular,
Pediatric Surgery MUHC MCH Siste. Objectives of Training
 Preamble A rotation in Pediatric Surgery must give residents the opportunity to become familiar with the unique needs of infants and children as surgical patients. Some of the surgical diseases encountered
Preamble A rotation in Pediatric Surgery must give residents the opportunity to become familiar with the unique needs of infants and children as surgical patients. Some of the surgical diseases encountered
GENI Program: GI and Abdominal Chief Complaints. Kim Macfarlane Clinical Nurse Specialist, Critical Care February 2008
 GENI Program: GI and Abdominal Chief Complaints Kim Macfarlane Clinical Nurse Specialist, Critical Care February 2008 Dehydration Common acute and chronic problem Recognition is critically important to
GENI Program: GI and Abdominal Chief Complaints Kim Macfarlane Clinical Nurse Specialist, Critical Care February 2008 Dehydration Common acute and chronic problem Recognition is critically important to
Esophageal Disorders. Gastrointestinal Diseases. Peptic Ulcer Disease. Wireless capsule endoscopy. Diseases of the Small Intestine 7/24/2010
 Esophageal Disorders Gastrointestinal Diseases Fernando Vega, MD HIHIM 409 Dysphagia Difficulty Swallowing and passing food from mouth via the esophagus Diagnostic aids: Endoscopy, Barium x ray, Cineradiology,
Esophageal Disorders Gastrointestinal Diseases Fernando Vega, MD HIHIM 409 Dysphagia Difficulty Swallowing and passing food from mouth via the esophagus Diagnostic aids: Endoscopy, Barium x ray, Cineradiology,
Pediatric Surgery: core knowledge for Pediatric residents Part 1 of 2 [updated June 2016]
![Pediatric Surgery: core knowledge for Pediatric residents Part 1 of 2 [updated June 2016]](/thumbs/77/74797014.jpg "Pediatric Surgery: core knowledge for Pediatric residents Part 1 of 2 [updated June 2016]") Pediatric Surgery: core knowledge for Pediatric residents Part 1 of 2 [updated June 2016] MCMASTER DIVISION OF PEDIATRIC SURGERY: DR. KAREN BAILEY DR. BRIAN CAMERON DR. PETER FITZGERALD DR. HELENE FLAGEOLE
Pediatric Surgery: core knowledge for Pediatric residents Part 1 of 2 [updated June 2016] MCMASTER DIVISION OF PEDIATRIC SURGERY: DR. KAREN BAILEY DR. BRIAN CAMERON DR. PETER FITZGERALD DR. HELENE FLAGEOLE
Case 1. Case Discussion. History. Present Illness. Impression. Physical Examination
 Case 1 Case Discussion R1 林吉倡 2013 / 01 / 02 13-yo Male BW: 45 kg DAY1 16:35 pm C/C: Epigastric pain since this morning TPR: 36.5/94/18 BP:133/83 SpO2: 100% GCS: 15 Triage: 2 Present Illness Sudden-onset
Case 1 Case Discussion R1 林吉倡 2013 / 01 / 02 13-yo Male BW: 45 kg DAY1 16:35 pm C/C: Epigastric pain since this morning TPR: 36.5/94/18 BP:133/83 SpO2: 100% GCS: 15 Triage: 2 Present Illness Sudden-onset
A Perf-ect Differential
 A Perf-ect Differential Carolyn Marcus, MD Disclosure of Financial Relationships Husband works as in-house legal counsel at Sanofi Case Presentation 6 year old boy with a history of constipation presents
A Perf-ect Differential Carolyn Marcus, MD Disclosure of Financial Relationships Husband works as in-house legal counsel at Sanofi Case Presentation 6 year old boy with a history of constipation presents
Development of pancreas and Small Intestine. ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama
 Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
3/22/2011. Inflammatory Bowel Disease. Inflammatory Bowel Disease Objectives: Appendicitis. Lemone and Burke Chapter 26
 Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
DOMINATE THE CLERKSHIP REVIEW PACKET. What are the electrolyte compositions of NS, LR, Plasmalyte A? Na Cl K HCO3 Ca Mg ph NS LR Plasmalyte A
 DOMINATE THE CLERKSHIP REVIEW PACKET POST OP CARE Fluids What percent of total body water does each compartment (extracellular, intracellular, interstitial, intravascular) make up? What are the electrolyte
DOMINATE THE CLERKSHIP REVIEW PACKET POST OP CARE Fluids What percent of total body water does each compartment (extracellular, intracellular, interstitial, intravascular) make up? What are the electrolyte
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint
 Examination Blueprint") GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
Diagnostic Imaging of Pediatric Gastrointestinal Abnormalities. Learning Objectives
 Diagnostic Imaging of Pediatric Gastrointestinal Abnormalities Tess Chapman, MD Associate Professor of Radiology, University of Washington School of Medicine Staff Radiologist, Seattle Children s Hospital
Diagnostic Imaging of Pediatric Gastrointestinal Abnormalities Tess Chapman, MD Associate Professor of Radiology, University of Washington School of Medicine Staff Radiologist, Seattle Children s Hospital
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
The Acute Abdomen New Mexico Nurse Practitioner Council Annual Conference, 2012
 The Acute Abdomen New Mexico Nurse Practitioner Council Annual Conference, 2012 Darra D. Kingsley, MD Associate Professor, Surgery, University of New Mexico School of Medicine Associate Chief of Staff,
The Acute Abdomen New Mexico Nurse Practitioner Council Annual Conference, 2012 Darra D. Kingsley, MD Associate Professor, Surgery, University of New Mexico School of Medicine Associate Chief of Staff,
Neonatal intestinal obstruction: how to make etiological diagnosis?
 Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. Mnari, M. Zguidi, A. Zrig, M. Maatouk, B. Hmida, R. Salem,
Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. Mnari, M. Zguidi, A. Zrig, M. Maatouk, B. Hmida, R. Salem,
In children 3 months to 3 years of age intussusception is
 Baird Mallory, MD, 1 and Yale Popowich, MD 2 In children 3 months to 3 years of age intussusception is one of the most common causes of a distal small bowel obstruction. It is often associated with intermittent
Baird Mallory, MD, 1 and Yale Popowich, MD 2 In children 3 months to 3 years of age intussusception is one of the most common causes of a distal small bowel obstruction. It is often associated with intermittent
Neonatal intestinal obstruction: how to make etiological diagnosis?
 Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. MNARI, M. Zguidi, A. Zrig, M. MAATOUK, B. Hmida, R. Salem,
Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. MNARI, M. Zguidi, A. Zrig, M. MAATOUK, B. Hmida, R. Salem,
8/29/2016 DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW. LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES
 DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES Define Diverticular Disease Discuss Epidemiology and Pathophysiology of Diverticular disease
DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES Define Diverticular Disease Discuss Epidemiology and Pathophysiology of Diverticular disease
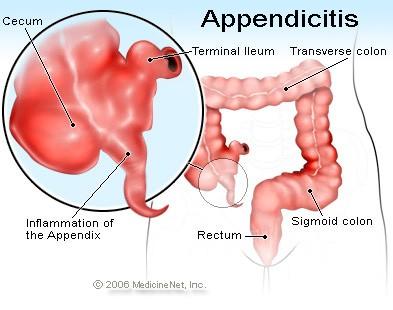
The appendix is a small, tube-like structure attached to the first part of the large intestine, also called the colon. The appendix.
 The appendix is a small, tube-like structure attached to the first part of the large intestine, also called the colon. The appendix is located in the lower right portion of the abdomen. It has no known
The appendix is a small, tube-like structure attached to the first part of the large intestine, also called the colon. The appendix is located in the lower right portion of the abdomen. It has no known
EVALUATION OF A SICK CHILD WITH FEVER
 EVALUATION OF A SICK CHILD WITH FEVER Learning objectives At the conclusion of this learning activity, participants should be able to; Discuss the different etiologies of acute illness in a child Identify
EVALUATION OF A SICK CHILD WITH FEVER Learning objectives At the conclusion of this learning activity, participants should be able to; Discuss the different etiologies of acute illness in a child Identify
FACE THE EXAMINER. Hirschsprung s Disease in Newborns. (This section is meant for residents to check their understanding regarding a particular topic)
") Journal of Neonatal Surgery 2013;2(4):51 FACE THE EXAMINER Hirschsprung s Disease in Newborns (This section is meant for residents to check their understanding regarding a particular topic) QUESTIONS 1.
Journal of Neonatal Surgery 2013;2(4):51 FACE THE EXAMINER Hirschsprung s Disease in Newborns (This section is meant for residents to check their understanding regarding a particular topic) QUESTIONS 1.
Acute Abdomen. Nirav Patel MD, FACS Banner University Medical Center - Phoenix
 Acute Abdomen Nirav Patel MD, FACS Banner University Medical Center - Phoenix ? Diffuse periumbilical with localization to RLQ + Nausea, anorexia, fevers - Diarrhea, emesis Exacerbated by movement, bumps
Acute Abdomen Nirav Patel MD, FACS Banner University Medical Center - Phoenix ? Diffuse periumbilical with localization to RLQ + Nausea, anorexia, fevers - Diarrhea, emesis Exacerbated by movement, bumps
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT
 GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT Name & Title Of Author: Dr Linda Jewes, Consultant Microbiologist Date Amended: December 2016 Approved by Committee/Group: Drugs & Therapeutics
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT Name & Title Of Author: Dr Linda Jewes, Consultant Microbiologist Date Amended: December 2016 Approved by Committee/Group: Drugs & Therapeutics
Muscle spasm Diminished bowel sounds Nausea/vomiting
 3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
Management of Common Paediatric Surgical G.I. Problems
 Management of Common Paediatric Surgical G.I. Problems Dr. Loh Ser Kheng Dale Lincoln Senior Consultant Department of Paediatric Surgery National University Hospital National University Health System Tongue
Management of Common Paediatric Surgical G.I. Problems Dr. Loh Ser Kheng Dale Lincoln Senior Consultant Department of Paediatric Surgery National University Hospital National University Health System Tongue
Update on Paediatric Surgical Emergencies March 2017
 Update on Paediatric Surgical Emergencies March 2017 Michael Stanton MBBS, MD, FRCS (Paed Surg) Consultant Paediatric & Neonatal Surgeon Southampton Children s Hospital & Spire Hospital Southampton Paediatric
Update on Paediatric Surgical Emergencies March 2017 Michael Stanton MBBS, MD, FRCS (Paed Surg) Consultant Paediatric & Neonatal Surgeon Southampton Children s Hospital & Spire Hospital Southampton Paediatric
Introduction and Definitions
 Bowel obstruction Introduction and Definitions Accounts for 5% of all acute surgical admissions Patients are often extremely ill requiring prompt assessment, resuscitation and intensive monitoring Obstruction
Bowel obstruction Introduction and Definitions Accounts for 5% of all acute surgical admissions Patients are often extremely ill requiring prompt assessment, resuscitation and intensive monitoring Obstruction
Problem. A 34-year. year-old woman admitted for control of diabetes develops acute abdominal pain that increases in severity over several hours.
 Immediate Questions Problem. A 34-year year-old woman admitted for control of diabetes develops acute abdominal pain that increases in severity over several hours. A. What are the patient's vital signs?
Immediate Questions Problem. A 34-year year-old woman admitted for control of diabetes develops acute abdominal pain that increases in severity over several hours. A. What are the patient's vital signs?
Digestion. Intake and assimilation of nutrients Elimination of waste Eating Required physically Pleasurable Social Emotional
 Digestive System 1 Digestion Intake and assimilation of nutrients Elimination of waste Eating Required physically Pleasurable Social Emotional Food behaviors can become just as addictive as any other pleasurable
Digestive System 1 Digestion Intake and assimilation of nutrients Elimination of waste Eating Required physically Pleasurable Social Emotional Food behaviors can become just as addictive as any other pleasurable
Intussusception Secondary to a Meckel Diverticulum in an Adolescent
 48) Intussusception Secondary to a Meckel Diverticulum in an Adolescent Yener O., Demir M., Yigitbaşı R. Department of Surgery, Göztepe Training and Research Hospital, Istanbul, Turkey Received March 28,
48) Intussusception Secondary to a Meckel Diverticulum in an Adolescent Yener O., Demir M., Yigitbaşı R. Department of Surgery, Göztepe Training and Research Hospital, Istanbul, Turkey Received March 28,