Miyagawa-Hayashino, Aya; Matsumura, Author(s) Miyachi, Yoshiki; Manabe, Toshiaki. Citation Human Pathology (2009), 40(9): 1269
|
|
|
- Matilda Ray
- 5 years ago
- Views:
Transcription
 Fumi; Asada, Hideo; Tanioka, Miki; Mikami, Yoshiki; Kotani, Hirokazu; Miyachi,")

1 High ratio of IgG4-positive Titleplasmacytosis-is this a cutaneous plasma m disease? Miyagawa-Hayashino, Aya; Matsumura, Author(s) Fumi; Asada, Hideo; Tanioka, Miki; Mikami, Yoshiki; Kotani, Hirokazu; Miyachi, Yoshiki; Manabe, Toshiaki Citation Human Pathology (2009), 40(9): 1269 Issue Date URL c 2009 Elsevier Inc. All rights res Right でありません 引用の際には出版社版をご確認ご利用ください This is not the published versi published version. Type Journal Article Textversion author Kyoto University
2 1 TITLE PAGE High ratio of IgG4-positive plasma cell infiltration in cutaneous plasmacytosis - Is this a cutaneous manifestation of IgG4-related disease? Aya Miyagawa-Hayashino, MD, PhD 1, Yumi Matsumura, MD, PhD 2, Fumi Kawakami, MD1, Hideo Asada, MD, PhD 3, Miki Tanioka, MD, PhD 2, Akihiko Yoshizawa, MD 1, Yoshiki Mikami, MD, PhD1, Hirokazu Kotani, MD, PhD1, Yasuaki Nakashima, MD, PhD1, Yoshiki Miyachi, MD, PhD2, Toshiaki Manabe, MD, PhD1 1 Department of Diagnostic Pathology, Kyoto University Hospital, Kyoto, , Japan 2 Department of Dermatology, Kyoto University Graduate School of Medicine, , Kyoto, Japan 3 Department of Dermatology, Nara Medical University, Nara, , Japan. Keyword: systemic plasmacytosis, interstitial lung disease, IL-6, pemphigus Abbreviations: Ig, immunoglobulin; Th2, T helper 2; Dsg, desmoglein; HPF, high power fields; IL, interleukin Corresponding author Aya Miyagawa-Hayashino, MD, PhD Department of Diagnostic Pathology Kyoto University Hospital
3 2 54 Kawahara-Cho, Shogoin, Sakyo-ku Kyoto , JAPAN Tel : Fax: ayam@kuhp.kyoto-u.ac.jp Funding sources: Supported in part by a Grant-in-Aid for Young Scientists from the Japan Society for the Promotion of Science (A. M-H) Running title: cutaneous plasmacytosis as IgG4-related disease
4 3 Abstract Cutaneous plasmacytosis is a rare condition affecting middle-aged individuals, characterized by multiple red-brown papules and plaques over the trunk. It has been reported mainly in Japan. The condition is accompanied by polyclonal hypergammaglobulinemia and superficial lymphadenopathy. Lung or retroperitoneal involvement occurs rarely. In the present study, three consecutive cases of cutaneous plasmacytosis were observed histologically to have abundant infiltration of IgG4-bearing plasma cells. All three were associated with superficial lymphadenopathy, one with interstitial lung involvement showing ground-glass opacity on CT and the others with bone marrow plasmacytosis, showing histological evidence of an increased number of IgG4-positive plasma cells. All three had polyclonal hypergammaglobulinemia, one had high serum concentration of IgG4, and all had elevated serum IL-6. The ratios of IgG4+ to IgG+ plasma cells were assessed using skin biopsy specimens with pemphigus (n=7), discoid lupus erythematosus (n=5) and morphea (n=2) (mean ratios; 19%, 0%, and 0%, respectively); we noted the proportion of IgG4-positive plasma cells in cutaneous plasmacytosis (mean: 48%). IgG4-related sclerosing disease is a newly recognized systemic disorder characterized by lymphoplasmacytic infiltration and fibrosis, and by a high serum IgG4 level and increased IgG4-positive plasma cells in the tissues. Skin manifestations of this disorder have not been described. Although cutaneous plasmacytosis could be a chronic allergic hypersensitivity reaction, our findings raise the possibility of a relationship in pathogenesis between cutaneous plasmacytosis and IgG4-related sclerosing disease.
5 4 Introduction Cutaneous plasmacytosis is a rare skin disorder of unknown etiology. It manifests as brown to red papules containing polyclonal plasma cells, predominantly on the trunk. 1-3 This condition has been recognized principally in Asian patients, with a few cases in Caucasians. 4-7 The condition is accompanied by polyclonal hypergammaglobulinemia and superficial lymphadenopathy. Histology shows a dense perivascular and periadnexal infiltrate composed almost entirely of polyclonal plasma cells. Patients with cutaneous plasmacytosis often have systemic manifestations, including anemia, fever, hepatosplenomegaly and superficial lymphadenopathy. Lymphadenopathy occurs in more than 50% of patients The lung, breast 4 and retroperitoneum 13 are involved less frequently. In the lung, cutaneous plasmacytosis may present as lymphoid interstitial pneumonia 10 or as multiple tiny nodules. 11 In such cases, some investigators have called the disorder systemic plasmacytosis. 14 Most cases have followed a chronic and benign clinical course over a decade without spontaneous remission, suggesting that the condition is a benign reactive proliferation of plasma cells 1,9. A few cases have followed an aggressive clinical course as lymphoma 15, lymphoid interstitial pneumonia 10, or renal failure 8,9. Treatment has included topical and systemic corticosteroids 16, cyclophosphamide 4, topical tacrolimus, 17 PUVA and other chemotherapy. 6,9,18,19,20 Recent studies have shown that sclerosing pancreatitis is a unique immunoglobulin (Ig) G4-related disease. 21 Many IgG4-positive plasma cells are present in extrapancreatic organs in patients with sclerosing pancreatitis, and IgG4-related systemic disorder has been proposed as a distinct disease entity. 22 Four subclasses of IgG have been defined from the antigenic uniqueness of their heavy chains. The subclasses are designated
6 5 IgG1, IgG2, IgG3 and IgG4, in order of their serum concentrations, which are respectively ~60, 25, 10 and 5%. Each IgG subclass expresses a unique profile of effector activities. The IgG4 subclass, which is known to have poor complement- and leucocyte-activating properties, may be characteristic of chronic antigen stimulation. 23 Sclerosing pancreatitis is manifest as multifocal fibrosclerosis, 24 which in turn shows as various combinations of the following conditions: orbital pseudotumor, 25 sclerosing sialoadenitis, 26 hepatic inflammatory pseudotumor, sclerosing cholangitis, 27 mediastinal and retroperitoneal fibrosis, 28,29 inflammatory aortic aneurysm 30, lymphoid interstitial pneumonia 31 or inflammatory pseudotumor of the lung, 32 lymphadenopathy, 29,33 tubulointerstitial nephritis, 34 and hypophysitis. 35 Histological findings are similar in these diseases, and there is marked lymphoplasmacytic infiltration with sclerosis, obliterative phlebitis and occasional eosinophils. Serum assay for IgG4 is useful for diagnosis, and abundant IgG4-bearing plasma cells found histologically are a hallmark of these diseases. 24 No cutaneous manifestations of multifocal fibrosclerosis and/or autoimmune pancreatitis have been reported. IgG4-bearing plasma cells were assessed on skin biopsy specimens in these patients in order to investigate the association with IgG4-related systemic disorder, since cutaneous plasmacytosis is likely to be a skin manifestation of systemic disorder. Since autoantibodies belong mainly to the IgG4 and IgG1 subclasses in pemphigus, 23 the controls were pemphigus (n=7), discoid lupus erythematosus (n=5) and morphea (n=2).
7 6 Material and Methods Skin and serum samples were obtained from three patients having cutaneous plasmacytosis; two were treated at Kyoto University Hospital and the third at the Dermatology Department of Osaka University Hospital. We examined various tissues, including lymph node, lung, and bone marrow. We also obtained skin biopsies from 7 patients with pemphigus (pemphigus vulgaris, n=4; pemphigus foliaseus, n=3), 5 with discoid lupus erythematosus, and two with morphea, taken from the database of the Department of Diagnostic Pathology, Kyoto University Hospital; they were used as controls in IgG4 immunohistochemistry. Control subjects were included in this study according to the following criteria for pemphigus: (i) the clinical presence of intraepidermal blisters; (ii) the presence of squamous epithelial intercellular deposition of IgG and/or C3 according to direct immunofluorescence studies; (iii) the presence of antibodies against desmosomal cadherins desmoglein (Dsg) 1 for pemphigus foliaceus and/or Dsg 3 for pemphigus vulgaris on Enzyme-Linked ImmunoSorbent Assay; and (iv) histological findings consistent with pemphigus foliaceus: subcorneal blister with acantholytic keratinocytes and pemphigus vulgaris; suprabasal acantholysis with blister formation. 36 For discoid lupus erythematosus we required: (i) the presence of a well-demarcated red-purple macule or papule with a superficial scale; (ii) histological evidence of vacuolar interface dermatitis with dense perivascular, interstitial, and periadnexal inflammation, with occasional basement membrane thickening and dermal mucin deposition; or (iii) positive lupus band test. 37 For morphea (localized scleroderma), we required: (i) the thickening and fibrosis to be limited clinically to the skin; and (ii) histological findings of thickening and sclerosis of the reticular dermis, with increased width of collagen bundles, and a superficial and
8 7 deep perivascular lymphocytic infiltrate containing plasma cells. 38 All biopsy specimens were fixed in neutral buffered formalin, embedded in paraffin, and sliced into sections 4 μm thick. Morphological characteristics were assessed on standard HE sections. Immunohistochemistry was performed using an autoimmunostainer (Ventana XT System Benchmark; Ventana Medical System, Inc., Tucson, AZ, USA). The following antibodies were applied: anti-igg (polyclonal; Ventana), IgG4 (1:500, clone HP6025; Serotec, Oxford, UK), IgA (polyclonal; Ventana), IgM (polyclonal; Ventana), CD3 (2GV6; Ventana), CD20 (1:1000, L26; DakoCytomation, Denmark), CD79a (1:400, JCB117; DakoCytomation), and immunoglobulin κ and λ-light chins (polyclonal; Ventana). The number of IgG+ and IgG4+ plasma cells at three different high power fields (HPF) was counted in each section, and an average number of positive cells per HPF was calculated. The percentage of IgG4+/IgG+ plasma cells was determined. 33 To compare continuous variables we used the unpaired Student t test or Mann-Whitney s U test. Statistical analysis was performed using StataSE 9.0 (Stata corporation, TX). A p-value smaller than.05 was taken to be statistically significant.
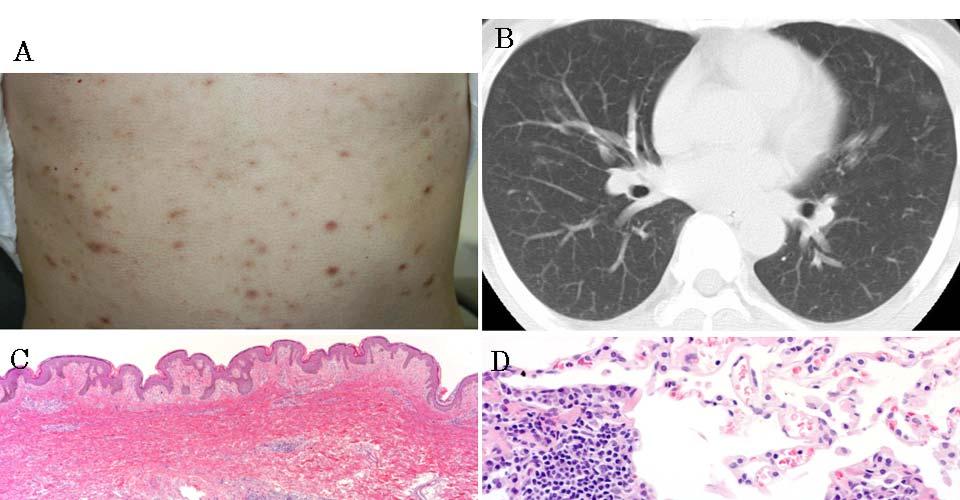
9 8 Results Clinical features Table 1 lists the clinical characteristics of patients with cutaneous plasmacytosis. All three were men, aged 54, 55 and 61 years. One case has been reported previously in detail. 17 All three patients came to our attention because of multiple reddish-brown papules over the trunk and face, which persisted for 5 (Pt 1), 3 (Pt 2) and 1.5 (Pt 3) years, respectively; see Fig. 1A. Their general conditions were relatively good, except that one had fatigue and one other had night sweat. All exhibited superficial lymphadenopathy. CT revealed diffuse lymphadenopathy, involving cervical, parotid, axillary, para-extrailiac, and inguinal locations. Chest CT revealed ground glass attenuation, with a slight reticular shadow in the middle and lower lobe bilaterally in one patient (Fig.1B). No honeycombing was noted. No fever or hepatosplenomegaly was found in any patient. All patients denied sicca syndrome and weight loss. Laboratory test results were as follows. Blood cell count with differential was normal. The erythrocyte sedimentation rate was raised in two of the patients tested (116 mm/h (Pt 1), 44 mm/h (Pt 3), normal 2-10 mm/h). C-reactive protein was raised in all three patients (2.1 mg/dl (Pt 1), 12.9 mg/dl (Pt 2), and 0.6 mg/dl (Pt 3); normal is <0.2 mg/dl). Total serum protein was elevated, and serum protein electrophoresis revealed polyclonal hypergammaglobulinemia with IgG (4637 mg/dl (Pt 1), 6480 mg/dl (Pt 2), and 2624 mg/dl (Pt 3); normal is mg/dl), IgA (475 mg/dl (Pt 1), 480 mg/dl (Pt 2), and 332 mg/dl (Pt 3); normal is mg/dl) and IgM (112 mg/dl (Pt1), 325 mg/dl (Pt 2), and 80 mg/dl (Pt 3); normal is mg/dl). One of the patients had an elevated serum IgG4 of 610 mg/dl (13.2% of total IgG, normal mg/dl) and a
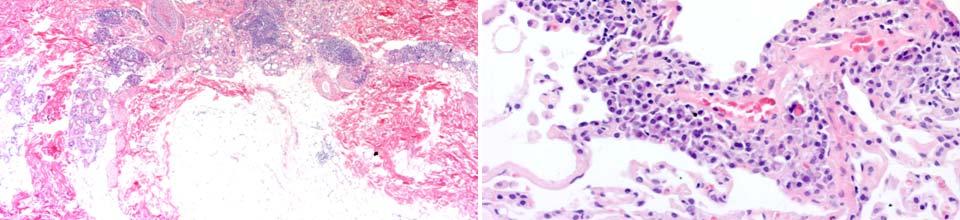
10 9 high serum IgE of 2600 IU/mL (normal IU/mL). Serum interleukin (IL)-6 level was raised (6.9 pg/ml (Pt 1), 74.5 pg/ml (Pt 2), and 4.6 pg/ml (Pt 3); normal is <4.0 pg/ml). Antinuclear antibody was positive in one patient (1:40). There was no measurable Bence-Jones protein in the urine. Flow cytometric evaluation on a lymph node in one patient revealed a polytypic lymphoplasmacytic infiltrate based on cell marker analysis. Predonisolone at low dosage (15 mg/day, 0.25 mg/kg) was started for cutaneous lesions in two patients, and tacrolimus ointment for the third. The third patient had severe plaques particularly on the face. Therefore, the tacrolimus ointment was applied to facial lesions. All patients were well at follow-up from 3 months to 3 years (Table 1). The treatment reduced the erythema and induration of the facial lesions for the third patient after 3 months. Therapeutic intervention via oral steroid had little effect in other two patients, and although not complete- a reduction in size of the skin lesions was observed. There was clinical response to predonisolone, with diminuation in size of lymph nodes and symptomatic improvement. Pathological findings Biopsy specimens of a papule on the trunk showed a moderately dense superficial and deep perivascular and periadnexal infiltrate, composed largely of plasma cells without atypia (Fig. 1C, 2A). None of the cases showed obliterative phlebitis or other vascular changes, or dermal sclerosis. An immunohistochemical study found that the infiltrating plasma cells were positive for IgG, IgA, IgM, κ, and λ-chains. There was no light chain restriction. A diagnosis of plasmacytosis was made. The number of IgG4+ plasma cells
11 10 was elevated (53 per HPF (Pt 1), 62 per HPF (Pt 2), and 72 per HPF (Pt 3)); see Figs. 2B, C. The proportion of IgG4+/IgG+ plasma cells was 42.2 % (Pt 1), 43.7% (Pt 2), and 58.1 % (Pt 3); see Table 2. Histology, obtained by transbronchial lung biopsy from segment 4 of the right lobe, showed thickening of the alveolar septum with marked infiltration of lymphoplamacytic cells, consistent with lymphocytic interstitial pneumonia (Fig. 1D). IgG4+ plasma cells were slightly increased in the interstitium (IgG4+/IgG+ plasma cells 15.4%). Lymph nodes from all three patients demonstrated interfollicular expansion, with variable sized follicles. The lymph node architecture was well preserved. The reactive follicle comprised a germinal center surrounded by a discrete mantle zone. The interfollicular region showed a mild increase in high endothelial venules, and large numbers of mature plasma cells (Fig. 3A, B). CD20+ B cells were confined to the follicles, and the CD3+ T cells resided mainly in the interfollicular regions. There was no immunoglobulin light chain restriction. The number of IgG4+ plasma cells was elevated (136 per HPF (Pt 1), 43 per HPF (Pt 2), and 94 per HPF (Pt 3)). The proportion of IgG4+/IgG+ plasma cells was 72.0% (Pt 1), 49.4% (Pt 2), and 53.4% (Pt 3); see Table 2, Fig. 3C, D. A bone marrow aspiration from one patient showed a normocellular marrow, with a normal myeloid to erythroid ratio, a normal number of megakaryocytes, and moderate plasmacytosis (12%). Discrete polyclonal plasmacytosis was found in the bone marrow aspiration. The mean number of IgG4+ plasma cells per HPF was 15, and the proportion of IgG4+/IgG+ plasma cells was 60.8 %.
12 11 Immunostaining of control skins Table 3 lists clinical features and the results of IgG4 and IgG immunostaining in controls. An increased proportion of IgG4+/IgG+ plasma cells was observed in pemphigus vulgaris and pemphigus foliaceus, ranging from 0 to 36.7% (mean 19.4%); in contrast there were none in discoid lupus erythematosus and morphea (vs pemphigus, P<.05). The inflammatory cells, including IgG4+ plasma cells, were more sparse in pemphigus than in cutaneous plasmacytosis. The lower number of IgG+ or IgG4+ plasma cells (pemphigus vs skin lesions of cutaneous plasmacytosis, P<.05), and the histology, are capable of distinguishing the pemphigus group with cutaneous plasmacytosis.
13 12 Discussion Since patients with sclerosing pancreatitis are recognized to have extrapancreatic lesions, and patients with extrapancreatic disease but with otherwise similar serological and histological features can have no pancreatic lesion, such lesions have been proposed as a manifestation of IgG4-related systemic disease. 29,39 This disorder commonly presents with a high serum IgG4 level and/or abundant IgG4+ plasma cells in the tissues involved. Skin lesions have not been described in patients with typical IgG4-related systemic disease, such as sclerosing pancreatitis or sclerosing cholangitis. Our cases showed marked IgG4-positive plasma cell infiltration in the skin; this is not known as a feature of cutaneous plasmacytosis. All of our patients with cutaneous plasmacytosis had associated extracutaneous lesions (lymph node, lung, and bone marrow), in which numerous IgG4-positive cells were found by immunohistochemistry. Systemic involvement has also included a peri-ureteric retroperitoneal mass causing hydronephrosis, 13 breast masses 4, hepatomegaly 10, and lymphoid interstitial pneumonia 10 in association with cutaneous plasmacytosis. Histology shows diffuse lymphoplasmacytic infiltration within fibrous tissue. Concomitant lymphadenopathy is common in IgG4-related systemic disease. Lymph node histology in IgG4-related systemic disease that is associated with autoimmune pancreatitis, sclerosing cholangitis, sclerosing decryoadenitis or sclerosing sialadenitis can be categorized into three patterns: Castleman disease-like, follicular hyperplasia, and interfollicular expansion by immunoblasts and plasma cells. 33 The lymph nodes in our cases showed reactive lymphoid follicles and marked distension of the interfollicular area by numerous plasma cells, and also a mild increase in thickened venules with a preserved nodal architecture. Histology of the lymph node in cutaneous plasmacytosis
14 13 was indistinguishable from lymph node lesions described in IgG4-related sclerosing disease; two of our cases fit best into the pattern of follicular hyperplasia, and one into the interfollicular expansion pattern specified in IgG4-related sclerosing disease. 33 Moreover, most patients are middle-aged to elderly ethnic Asians, with male predominance in both diseases. 40 The clinicopathological similarities between cutaneous plasmacytosis and IgG4-related sclerosing disease indicate a relation with cutaneous plasmacytosis as a manifestation of IgG4-related disease. Allergic symptoms and atopic dermatitis are associated with high serum levels of specific IgG subclass antibodies to allergens, particularly IgG4. In pemphigus, autoantibodies belong mainly to the IgG4 and IgG1 subclasses. IgG1 antibodies against desmoglein are present with equal frequency in individuals with and without pemphigus, but IgG4 antibodies are present almost exclusively in patients with active disease. 23,36 The present study finds increased IgG4+ plasma cells in patients with pemphigus group, although the significant increase in IgG4+ plasma cells (>40% IgG4+/IgG+ plasma cells) is likely to represent IgG4-related sclerosing disease, since all reactive lymph nodes not associated with IgG4-related systemic disease have a proportion below 30%. 33 Abundant IgG4-bearing plasma cell infiltration, exceeding 40% of IgG+ cells, is a characteristic histological finding for cutaneous plasmacytosis, and is not found in skin biopsies of control patients. The IgG4+/IgG+ plasma cell ratio in the lung biopsy specimen was lower than in skin or lymph node. This is probably because the specimen was small and unrepresentative of the whole lesion, although it might have been due to a different disease process. Involvement of the lung as a form of lymphoid interstitial pneumonia in cutaneous plasmacytosis has been recognized. 10
15 14 These is also some evidence that interstitial pneumonia occurs during the course of autoimmune pancreatitis. 31,41 Chest CT revealed diffuse ground-glass attenuation with honeycomb changes at the base of the lower lobe, or mild interstitial shadows. The histology in one case showed thickening of the lower lobe septum, with marked IgG4-positive plasma cells. 31 We suspect that there is a close relation between these pulmonary changes and cutaneous plasmacytosis, because of elevated serum IgG4 and the infiltration of IgG4-positive plasma cells in the lung tissue. Cutaneous plasmacytosis could be a type of chronic allergic/hypersensitivity reaction, since allergic and atopic dermatitis are both associated with elevated IgE and IgG4. Our data were limited because of a lack of serum level of IgE and IgG4 in two of the three patients. None of our cases showed obliterative phlebitis or tissue fibrosis characteristic of IgG4-related sclerosing disease. Although our cases exhibited lymphadenopathy, bone marrow involvement, and possible evidence of lung infiltrates in one case, the evidence for cutaneous plasmacytosis as a skin lesion of an IgG4-related sclerosing disease was not convincing, because of the lack of pancreatic involvement. Activation of T helper 2 (Th2) cells is believed to play a major role in allergic sensitization. The Th2 cytokines produce IL-4, IL-5 and IL-13, leading to the secretion of IgG4 and IgE by B cells. Allergic diseases are characterized by activation of the immune system and formation of IgE antibodies against specific allergens; IgG4 represents blocking antibody to IgE-coated mast cells. 42 A parallel increase in the serum IgE concentration was found in 20% of patients with sclerosing pancreatitis. 21 IgG4-related sclerosing disease is an immune reaction mediated by Th2 cells and T regulatory cells. 43, suggesting that cutaneous plasmacytosis and IgG4-related sclerosing disease have a common disease
16 15 process. Unknown environmental agents might trigger the production of IgG antibodies against unknown antigens, and trigger the subclass switching to IgG4 in B-cells. The geographical distribution of both cutaneous plasmacytosis and IgG4-related sclerosing disease has led to speculation that a HLA susceptibility gene is necessary for pathogenic activity of the disease. Another possibility is a primary infectious cause. Hyperproduction of IL-6 is also considered to be an important factor in the pathogenesis of cutaneous plasmacytosis. IL-6 induces B-cell proliferation and terminal differentiation, immunoglobulin secretion, and induces the acute inflammatory-phase response. An increase in IL-6 concentration has also been reported in cutaneous plasmacytosis. 13,16,44 Our cases were all associated with elevated serum IL-6. Further studies are needed to determine the role of IgG4 in the pathogenesis of this disease. Since cutaneous plasmacytosis and IgG4-related sclerosing disease are both extremely rare, to learn more it is necessary to investigate a large series of patients and to provide more evidence of systemic lesions for cutaneous plasmacytosis.
17 16 Acknowledgments The authors thank Mr. T Nishida of the Department of Dermatology, Osaka University Graduate School of Medicine, for providing tissue samples, and Ms. I Koyanagi, Ms. S Yamane, and Ms. C Tanaka, Kyoto University Hospital, for technical assistance.
18 17 References 1. Aso M, Shimao S. An unusual case of cutaneous plasmacytosis. J Dermatol 1982;9: Ishii N, Hayashi M, Nakajima H, et al. A case of cutaneous plasmacytosis. J Dermatol 1984;11: Kitamura K, Tamura N, Hatano H, et al. A case of plasmacytosis with multiple peculiar eruptions. J Dermatol 1980;7: Carey WP, Rico MJ, Nierodzik M, et al. Systemic plasmacytosis with cutaneous manifestations in a white man: successful therapy with cyclophosphamide/prednisone. J Am Acad Dermatol 1998;38: Cerottini JP, Guillod J, Vion B, et al. Cutaneous plasmacytosis: an unusual presentation sharing features with POEMS syndrome? Dermatology 2001;202: Hafner C, Hohenleutner U, Babilas P, et al. Targeting T cells to hit B cells: successful treatment of cutaneous plasmacytosis with topical pimecrolimus. Dermatology 2006;213: Lopez-Estebaranz JL, Rodriguez-Peralto JL, Ortiz Romero PL, et al. Cutaneous plasmacytosis: report of a case in a white man. J Am Acad Dermatol 1994;31: Shimizu S, Tanaka M, Shimizu H, et al.: Is cutaneous plasmacytosis a distinct clinical entity? J Am Acad Dermatol 1997;36: Uhara H, Saida T, Ikegawa S, et al. Primary cutaneous plasmacytosis: report of three cases and review of the literature. Dermatology 1994;189: Watanabe S, Ohara K, Kukita A, et al. Systemic plasmacytosis. A syndrome of peculiar multiple skin eruptions, generalized lymphadenopathy, and polyclonal
19 18 hypergammaglobulinemia. Arch Dermatol 1986;122: Amin HM, McLaughlin P, Rutherford CJ, et al. Cutaneous and systemic plasmacytosis in a patient of Asian descent living in the United States. Am J Dermatopathol 2002;24: Leonard AL, Meehan SA, Ramsey D, et al. Cutaneous and systemic plasmacytosis. J Am Acad Dermatol 2007;56:S38-S Kodama A, Tani M, Hori K, et al. Systemic and cutaneous plasmacytosis with multiple skin lesions and polyclonal hypergammaglobulinaemia: significant serum interleukin-6 levels. Br J Dermatol 1992;127: Tada Y, Komine M, Suzuki S, et al. Plasmacytosis: systemic or cutaneous, are they distinct? Acta Derm Venereol 2000;80: Nitta Y. Case of malignant lymphoma associated with primary systemic plasmacytosis with polyclonal hypergammaglobulinemia. Am J Dermatopathol 1997;19: Yamamoto T, Soejima K, Katayama I, et al. Intralesional steroid-therapy-induced reduction of plasma interleukin-6 and improvement of cutaneous plasmacytosis. Dermatology 1995;190: Miura H, Itami S, Yoshikawa K. Treatment of facial lesion of cutaneous plasmacytosis with tacrolimus ointment. J Am Acad Dermatol 2003;49: Kaneda M, Kuroda K, Fujita M, et al. Successful treatment with topical PUVA of nodular cutaneous plasmacytosis associated with alopecia of the scalp. Clin Exp Dermatol 1996;21: Lee DW, Choi SW, Park JW, et al. Systemic plasmacytosis: a case which improved with melphalan. J Dermatol 1995;22:205-9.
20 Tzung TY, Wu KH, Wu JC, et al. Primary cutaneous plasmacytosis successfully treated with topical photodynamic therapy. Acta Derm Venereol 2005;85: Hamano H, Kawa S, Horiuchi A, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med 2001;344: Kamisawa T, Funata N, Hayashi Y, et al. A new clinicopathological entity of IgG4-related autoimmune disease. J Gastroenterol 2003;38: Sitaru C, Mihai S, Zillikens D. The relevance of the IgG subclass of autoantibodies for blister induction in autoimmune bullous skin diseases. Arch Dermatol Res 2007;299: Hamano H, Arakura N, Muraki T, et al. Prevalence and distribution of extrapancreatic lesions complicating autoimmune pancreatitis. J Gastroenterol 2006;41: Sato Y, Ohshima K, Ichimura K, et al. Ocular adnexal IgG4-related disease has uniform clinicopathology. Pathol Int 2008;58: Kitagawa S, Zen Y, Harada K, et al. Abundant IgG4-positive plasma cell infiltration characterizes chronic sclerosing sialadenitis (Kuttner's tumor). Am J Surg Pathol 2005;29: Zen Y, Harada K, Sasaki M, et al. IgG4-related sclerosing cholangitis with and without hepatic inflammatory pseudotumor, and sclerosing pancreatitis-associated sclerosing cholangitis: do they belong to a spectrum of sclerosing pancreatitis? Am J Surg Pathol 2004;28: Hamano H, Kawa S, Ochi Y, et al. Hydronephrosis associated with retroperitoneal fibrosis and sclerosing pancreatitis. Lancet 2002;359: Kamisawa T, Funata N, Hayashi Y, et al. Close relationship between
21 20 autoimmune pancreatitis and multifocal fibrosclerosis. Gut 2003;52: Sakata N, Tashiro T, Uesugi N, et al. IgG4-positive plasma cells in inflammatory abdominal aortic aneurysm: the possibility of an aortic manifestation of IgG4-related sclerosing disease. Am J Surg Pathol 2008;32: Taniguchi T, Ko M, Seko S, et al. Interstitial pneumonia associated with autoimmune pancreatitis. Gut 2004;53: Zen Y, Kitagawa S, Minato H, et al. IgG4-positive plasma cells in inflammatory pseudotumor (plasma cell granuloma) of the lung. Hum Pathol 2005;36: Cheuk W, Yuen HK, Chu SY, et al. Lymphadenopathy of IgG4-related sclerosing disease. Am J Surg Pathol 2008;32: Takeda S, Haratake J, Kasai T, et al. IgG4-associated idiopathic tubulointerstitial nephritis complicating autoimmune pancreatitis. Nephrol Dial Transplant 2004;19: Wong S, Lam WY, Wong WK, et al. Hypophysitis presented as inflammatory pseudotumor in immunoglobulin G4-related systemic disease. Hum Pathol 2007;38: Bystryn JC, Rudolph JL. Pemphigus. Lancet 2005;366: Rothfield N, Sontheimer RD, Bernstein M: Lupus erythematosus: systemic and cutaneous manifestations. Clin Dermatol 2006;24: Laxer RM, Zulian F. Localized scleroderma. Curr Opin Rheumatol 2006;18: Zen Y, Sawazaki A, Miyayama S, et al. A case of retroperitoneal and mediastinal fibrosis exhibiting elevated levels of IgG4 in the absence of sclerosing pancreatitis (autoimmune pancreatitis). Hum Pathol 2006;37:
22 Jayaraman AG, Cesca C, Kohler S. Cutaneous plasmacytosis: A report of five cases with immunohistochemical evaluation for HHV-8 expression. Am J Dermatopathol 2006;28: Hirano K, Kawabe T, Komatsu Y, et al. High-rate pulmonary involvement in autoimmune pancreatitis. Intern Med J 2006; 36: Meiler F, Klunker S, Zimmermann M, Akdis CA, Akdis M. Distinct regulation of IgE, IgG4 and IgA by T regulatory cells and toll-like receptors. Allergy 2008;63: Zen Y, Fujii T, Harada K, et al. Th2 and regulatory immune reactions are increased in immunoglobulin G4-related sclerosing pancreatitis and cholangitis. Hepatology 2007;45: Kanbe N, Kurosawa M, Akimoto S, et al. Systemic plasmacytosis with deposition of interleukin (IL)-6 and elevated expression of IL-6 mrna in the skin lesions. Br J Dermatol 1998;138:721-3.
23 22 Figure legends Fig. 1 Skin and lung findings in patient 1 A: Diffuse red-brown papules on the chest and abdomen B: Chest CT showing ground-glass opacities and slight reticular shadows. C: Low-magnification photograph of cutaneous plasmacytosis showing dense perivascular and periadnexal infiltration of plasma cells in the deep dermis (HE, original magnification x20) D: Histological findings of lung biopsy specimen from the right middle lobe. Thickened alveolar septa due to lymphoplasmacytic infiltration (HE, x200) Fig. 2 Skin biopsy from patient 3 A: Numerous infiltration of plasma cells in the dermis (x100). B, C: Immunostaining for IgG (B) and IgG4 (C) in the corresponding field. Increased IgG4+ cells are seen (x100). Fig. 3 Lymph node from patient 1 A: Lymph node showing intact nodal architecture with reactive follicular hyperplasia (x200). B: The interfollicular zone is expanded and is densely populated by mature plasma cells accompanied by high endothelial venules (x200). C: Immunostaining for IgG. Numerous IgG+ cells are present between the follicles (x200). D: Immunostaining for IgG4. The number of IgG4+ cells is slightly higher than that of IgG4+ cells in the corresponding field. The IgG4+/IgG+ cell ratio exceeds 50% (x200).
24 Table 1: Clinical features of patients with cutaneous plasmacytosis Patient Age (yr) Gender Serum IgG Serum IgG4 γ-globulin IL-6 (mg/dl) (mg/dl) (%) (pg/ml) Associated disease 1 54 M (13.2%) lymphadenopathy, interstitial lung disease 2 55 M 6480 NA elevated 74.5 lymphadnopathy 3 61 M 2624 NA lymphadenopathy, bone marrow plasmacytosis Treatment Follow-up (yr) PSL 15mg 1.5 tacrolimus ointment 0.3 PSL 15mg 3 IgG, normal value mg/dL; IgG4, normal mg/dl; γ-globulin, normal %; IL-6, normal <4 pg/ml; NA, not available; PSL, prednisolone
25 Table 2: IgG4+/IgG+ plasma cell count and ratio in the various involved tissues of patients with cutaneous plasmacytosis Patient Location IgG4+/IgG+ plasma cells per HPF (%) 1 Skin 53/153 (42.2) Lymph node 136/189 (72.0) Lung 14/91 (15.4) 2 Skin 62/142 (43.7) Lymph node 43/87 (49.4) 3 Skin 72/124 (58.1) Lymph node 94/176 (53.4) Bone marrow 15/25 (60.8)
26 Table 3: IgG4+/IgG+ plasma cell count and ratio of control A. Patients with pemphigus vulgaris Patient Age Gender Dsg1 IgG Dsg3 IgG (normal <14) (normal <7) IgG4+/IgG+ Plasma Cells per HPF (%) 1 53 F 119 > /18 (36.7%) 2 73 F /6 (0) 3 47 F /11 (14.5%) 4 63 M /42 (20.5%) B. Patients with pemphigus foliaceus Patient Age Gender Dsg1 IgG Dsg3 IgG (normal <14) (normal <7) IgG4+/IgG+ Plasma Cells per HPF (%) 5 77 F /53.7 (20.5%) 6 64 F /65.7 (15.2%) 7 21 F /19.6 (28.6%) Dsg1, anti-desmoglein 1 antibody; Dsg3, anti-desmoglein 3 antibody
27 Table 3 (cond t) C. Patients with discoid lupus erythematosus Patient Age Gender IgG4+/IgG+ Plasma Cells per HPF (%) 8 46 F 0/327 (0) 9 32 F 0/13 (0) F 0/5 (0) F 0/5.3 (0) F 0/49 (0) D. Patients with morphea Patient Age Gender IgG4+/IgG+ Plasma Cells per HPF (%) M 0/3 (0) M 0/4 0)
28

29


30
Elsevier B.V.; この論文は出版社版でありま Right 引用の際には出版社版をご確認ご利用ください This is
 Title Refractory cutaneous lichenoid sarc tranilast. Author(s) Nakahigashi, Kyoko; Kabashima, Kenj Utani, Atsushi; Miyachi, Yoshiki Citation Journal of the American Academy of 63(1): 171-172 Issue Date
Title Refractory cutaneous lichenoid sarc tranilast. Author(s) Nakahigashi, Kyoko; Kabashima, Kenj Utani, Atsushi; Miyachi, Yoshiki Citation Journal of the American Academy of 63(1): 171-172 Issue Date
Case Report Cutaneous Plasmacytosis with Perineural Involvement
 Case Reports in Dermatological Medicine, Article ID 840845, 4 pages http://dx.doi.org/10.1155/2014/840845 Case Report Cutaneous Plasmacytosis with Perineural Involvement Elizabeth A. Brezinski, Maxwell
Case Reports in Dermatological Medicine, Article ID 840845, 4 pages http://dx.doi.org/10.1155/2014/840845 Case Report Cutaneous Plasmacytosis with Perineural Involvement Elizabeth A. Brezinski, Maxwell
IgG4-related sclerosing disease
 IgG4-related sclerosing disease TERUMI KAMISAWA, KENSUKE TAKUMA, NAOTO EGAWA Department of Internal Medicine Tokyo Metropolitan Komagome Hospital 3-18-22 Honkomagome, Bunkyo-ku, Tokyo 113-8677, Japan JAPAN
IgG4-related sclerosing disease TERUMI KAMISAWA, KENSUKE TAKUMA, NAOTO EGAWA Department of Internal Medicine Tokyo Metropolitan Komagome Hospital 3-18-22 Honkomagome, Bunkyo-ku, Tokyo 113-8677, Japan JAPAN
IgG4-related Kidney Disease in Which the Urinalysis, Kidney Function and Imaging Findings Were Normal
 CASE REPORT IgG4-related Kidney Disease in Which the Urinalysis, Kidney Function and Imaging Findings Were Normal Miho Otani 1, Masahiro Morinaga 1, Yoshihiko Nakajima 1, Hiromi Tomioka 2, Michiko Nishii
CASE REPORT IgG4-related Kidney Disease in Which the Urinalysis, Kidney Function and Imaging Findings Were Normal Miho Otani 1, Masahiro Morinaga 1, Yoshihiko Nakajima 1, Hiromi Tomioka 2, Michiko Nishii
Chronic Sclerosing Dacryoadenitis
 The Korean Journal of Pathology 2008; 42: 118-22 Chronic Sclerosing Dacryoadenitis - Report of 2 Cases - Ji Eun Kwon Sang Kyum Kim Sang-Ryul Lee 1 Woo-Ick Yang Haeryoung Kim 2 Department of Pathology and
The Korean Journal of Pathology 2008; 42: 118-22 Chronic Sclerosing Dacryoadenitis - Report of 2 Cases - Ji Eun Kwon Sang Kyum Kim Sang-Ryul Lee 1 Woo-Ick Yang Haeryoung Kim 2 Department of Pathology and
Key words: diagnosis, immunoglobulin G4, immunoglobulin G4-related diseases, immunohistochemistry, pseudolymphoma. CASE HISTORY
 doi: 10.1111/1346-8138.12301 Journal of Dermatology 2013; 40: 998 1003 ORIGINAL ARTICLE Case of immunoglobulin G4-related skin disease: Possible immunoglobulin G4-related skin disease cases in cutaneous
doi: 10.1111/1346-8138.12301 Journal of Dermatology 2013; 40: 998 1003 ORIGINAL ARTICLE Case of immunoglobulin G4-related skin disease: Possible immunoglobulin G4-related skin disease cases in cutaneous
Renal manifestations of IgG4-related systemic disease
 Renal manifestations of IgG4-related systemic disease Lynn D. Cornell, M.D. Mayo Clinic Rochester, MN While autoimmune pancreatitis (AIP) has been recognized since the first description by Sarles et al
Renal manifestations of IgG4-related systemic disease Lynn D. Cornell, M.D. Mayo Clinic Rochester, MN While autoimmune pancreatitis (AIP) has been recognized since the first description by Sarles et al
Immunoglobulin G4-Related Disease with Several Inflammatory Foci
 CASE REPORT Immunoglobulin G4-Related Disease with Several Inflammatory Foci Akira Sakamaki 1, Kenya Kamimura 1, Kazuhiko Shioji 1, Junko Sakurada 2, Takeshi Nakatsue 3, Yoko Wada 3, Michitaka Imai 1,
CASE REPORT Immunoglobulin G4-Related Disease with Several Inflammatory Foci Akira Sakamaki 1, Kenya Kamimura 1, Kazuhiko Shioji 1, Junko Sakurada 2, Takeshi Nakatsue 3, Yoko Wada 3, Michitaka Imai 1,
CME/SAM. Increased Immunoglobulin (Ig) G4 Positive Plasma Cell Density and IgG4/IgG Ratio Are Not Specific for IgG4- Related Disease in the Skin
 G4 Positive Plasma Cell Density and IgG4/IgG Ratio Are Not Specific for IgG4- Related Disease in the Skin") Increased Immunoglobulin (Ig) G4 Positive Plasma Cell Density and IgG4/IgG Ratio Are Not Specific for IgG4- Related Disease in the Skin Julia S. Lehman, MD, 1,2 Thomas C. Smyrk, MD, 1 and Mark R. Pittelkow,
Increased Immunoglobulin (Ig) G4 Positive Plasma Cell Density and IgG4/IgG Ratio Are Not Specific for IgG4- Related Disease in the Skin Julia S. Lehman, MD, 1,2 Thomas C. Smyrk, MD, 1 and Mark R. Pittelkow,
Review Article The Utility of Serum IgG4 Concentrations as a Biomarker
 International Rheumatology Volume 2012, Article ID 198314, 4 pages doi:10.1155/2012/198314 Review Article The Utility of Serum IgG4 Concentrations as a Biomarker Shigeyuki Kawa, 1 Tetsuya Ito, 2 Takayuki
International Rheumatology Volume 2012, Article ID 198314, 4 pages doi:10.1155/2012/198314 Review Article The Utility of Serum IgG4 Concentrations as a Biomarker Shigeyuki Kawa, 1 Tetsuya Ito, 2 Takayuki
Renal Pathology Case Conference. Case 2
 Renal Pathology Case Conference Case 2 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN cornell.lynn@mayo.edu March 2, 2008 Clinical presentation 68 year old woman, initially with normal renal function
Renal Pathology Case Conference Case 2 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN cornell.lynn@mayo.edu March 2, 2008 Clinical presentation 68 year old woman, initially with normal renal function
Hideaki Miura, Yasutaka Miyachi. Department of Internal Medicine, Social Insurance Central General Hospital. Tokyo, Japan
 CASE REPORT IgG4-Related Retroperitoneal Fibrosis and Sclerosing Cholangitis Independent of Autoimmune Pancreatitis. A Recurrent Case after a 5-Year History of Spontaneous Remission Hideaki Miura, Yasutaka
CASE REPORT IgG4-Related Retroperitoneal Fibrosis and Sclerosing Cholangitis Independent of Autoimmune Pancreatitis. A Recurrent Case after a 5-Year History of Spontaneous Remission Hideaki Miura, Yasutaka
この論文は出版社版でありません 引用の際には出版社版をご確認ご利用ください This is not the publis version. Please cite only the publi
 Title A case of progressive digital ische gemcitabine and S-1 in a patient wi Zaima, C; Kanai, M; Ishikawa, S; Ka Author(s) Mori, Y; Nishimura, T; Matsumoto, S T; Mimori, T Citation Japanese journal of
Title A case of progressive digital ische gemcitabine and S-1 in a patient wi Zaima, C; Kanai, M; Ishikawa, S; Ka Author(s) Mori, Y; Nishimura, T; Matsumoto, S T; Mimori, T Citation Japanese journal of
Case Report An IgG4-Related Salivary Gland Disorder: A Case Series Presenting with a Different Clinical Setting
 Case Reports in Immunology Volume 2011, Article ID 236079, 4 pages doi:10.1155/2011/236079 Case Report An IgG4-Related Salivary Gland Disorder: A Case Series Presenting with a Different Clinical Setting
Case Reports in Immunology Volume 2011, Article ID 236079, 4 pages doi:10.1155/2011/236079 Case Report An IgG4-Related Salivary Gland Disorder: A Case Series Presenting with a Different Clinical Setting
Plasma cells produce various immunoglobulins, ActaDV ActaDV
 506 CLINICAL REPORT Evaluation of IgG4 + Plasma Cell Infiltration in Patients with Systemic Plasmacytosis and Other Plasma Cell-infiltrating Skin Diseases Shintaro TAKEOKA 1, Masahiro KAMATA 1, Carren
506 CLINICAL REPORT Evaluation of IgG4 + Plasma Cell Infiltration in Patients with Systemic Plasmacytosis and Other Plasma Cell-infiltrating Skin Diseases Shintaro TAKEOKA 1, Masahiro KAMATA 1, Carren
Perifollicular granulomatous inflammation in reactive lymph nodes: a possible morphologic marker for IgG4 plasmacytosis
 J Hematopathol (2011) 4:207 214 DOI 10.1007/s12308-011-0117-5 ORIGINAL ARTICLE Perifollicular granulomatous inflammation in reactive lymph nodes: a possible morphologic marker for IgG4 plasmacytosis Imran
J Hematopathol (2011) 4:207 214 DOI 10.1007/s12308-011-0117-5 ORIGINAL ARTICLE Perifollicular granulomatous inflammation in reactive lymph nodes: a possible morphologic marker for IgG4 plasmacytosis Imran
IgG4-Related Tubulointerstitial Nephritis and Lymphadenopathy after Therapy for Malignant Lymphoma
 CASE REPORT IgG4-Related Tubulointerstitial Nephritis and Lymphadenopathy after Therapy for Malignant Lymphoma Yasuko Oshima 1, Ryosuke Usui 1, Shun Manabe 1, Naoki Hasegawa 2, Yukio Kakuta 2, Kosaku Nitta
CASE REPORT IgG4-Related Tubulointerstitial Nephritis and Lymphadenopathy after Therapy for Malignant Lymphoma Yasuko Oshima 1, Ryosuke Usui 1, Shun Manabe 1, Naoki Hasegawa 2, Yukio Kakuta 2, Kosaku Nitta
Citation The Journal of Dermatology, 37(8), available at
, available at") NAOSITE: Nagasaki University's Ac Title Two cases of blaschkitis with promi Author(s) Utani, Atsushi Citation The Journal of Dermatology, 37(8), Issue Date 2010-08 URL Right http://hdl.handle.net/10069/25634
NAOSITE: Nagasaki University's Ac Title Two cases of blaschkitis with promi Author(s) Utani, Atsushi Citation The Journal of Dermatology, 37(8), Issue Date 2010-08 URL Right http://hdl.handle.net/10069/25634
Mikulicz s Disease with Progressively Transformed Germinal Centers-type Immunoglobulin G4-related Lymphadenopathy Mimicking Sjögren s Syndrome
 Journal of Rheumatic Diseases Vol. 22, No. 6, December, 2015 http://dx.doi.org/10.4078/jrd.2015.22.6.395 Case Report Mikulicz s Disease with Progressively Transformed Germinal Centers-type Immunoglobulin
Journal of Rheumatic Diseases Vol. 22, No. 6, December, 2015 http://dx.doi.org/10.4078/jrd.2015.22.6.395 Case Report Mikulicz s Disease with Progressively Transformed Germinal Centers-type Immunoglobulin
Grover s disease: A case report.
 320 Case report Thai J Dermatol, October-December 2011 ABSTRACT: Grover s disease: A case report. Supicha Chavanich MD, Praneet Sajjachareonpong MD. CHAVANICH C, SAJJACHAREONPONG P. GROVER S DISEASE: A
320 Case report Thai J Dermatol, October-December 2011 ABSTRACT: Grover s disease: A case report. Supicha Chavanich MD, Praneet Sajjachareonpong MD. CHAVANICH C, SAJJACHAREONPONG P. GROVER S DISEASE: A
Ocular adnexal marginal zone B cell lymphoma infiltrated by IgG4-positive plasma cells
 JCP Online First, published on October 27, 2010 as 10.1136/jcp.2010.082156 1 Department of Ophthalmology, National Hospital Organization, Nagoya Medical Center, Nagoya, Japan 2 Department of Pathology,
JCP Online First, published on October 27, 2010 as 10.1136/jcp.2010.082156 1 Department of Ophthalmology, National Hospital Organization, Nagoya Medical Center, Nagoya, Japan 2 Department of Pathology,
CLINICAL SCIENCES. Ocular Adnexal IgG4-Related Lymphoplasmacytic Infiltrative Disorder
 CLINICAL SCIENCES Ocular Adnexal IgG4-Related Lymphoplasmacytic Infiltrative Disorder Toshinobu Kubota, MD; Suzuko Moritani, MD; Masao Katayama, MD; Hiroko Terasaki, MD, PhD Objective: To determine the
CLINICAL SCIENCES Ocular Adnexal IgG4-Related Lymphoplasmacytic Infiltrative Disorder Toshinobu Kubota, MD; Suzuko Moritani, MD; Masao Katayama, MD; Hiroko Terasaki, MD, PhD Objective: To determine the
IgG4-Negative Autoimmune Pancreatitis with Sclerosing Cholangitis and Colitis: Possible Association with Primary Sclerosing Cholangitis?
 CASE REPORT IgG4-Negative Autoimmune Pancreatitis with Sclerosing Cholangitis and Colitis: Possible Association with Primary Sclerosing Cholangitis? Keita Saeki 1, Shigenari Hozawa 1, Naoteru Miyata 1,
CASE REPORT IgG4-Negative Autoimmune Pancreatitis with Sclerosing Cholangitis and Colitis: Possible Association with Primary Sclerosing Cholangitis? Keita Saeki 1, Shigenari Hozawa 1, Naoteru Miyata 1,
IgG4-related hypophysitis presenting as a pituitary adenoma with systemic disease
 Asian Journal of Surgery (2013) 36, 93e97 Available online at www.sciencedirect.com journal homepage: www.e-asianjournalsurgery.com CASE REPORT IgG4-related hypophysitis presenting as a pituitary adenoma
Asian Journal of Surgery (2013) 36, 93e97 Available online at www.sciencedirect.com journal homepage: www.e-asianjournalsurgery.com CASE REPORT IgG4-related hypophysitis presenting as a pituitary adenoma
Osteosclerotic Myeloma (POEMS Syndrome)
") Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
Clinical outcomes and pathological characteristics of immunoglobulin G4-related ophthalmic disease versus orbital inflammatory pseudotumor
 ORIGINAL ARTICLE Korean J Intern Med 2019;34:220-226 Clinical outcomes and pathological characteristics of immunoglobulin G4-related ophthalmic disease versus orbital inflammatory pseudotumor Hong Ki Min
ORIGINAL ARTICLE Korean J Intern Med 2019;34:220-226 Clinical outcomes and pathological characteristics of immunoglobulin G4-related ophthalmic disease versus orbital inflammatory pseudotumor Hong Ki Min
IgG4 Disease. General Principles of IgG4-related disease. EL Cluvar, AC Bateman
 IgG4 Disease General Principles of IgG4-related disease. EL Cluvar, AC Bateman Diagnostic Guidelines for IgG4-related disease with a focus on histopathological criteria. V Deshpande, A Khosroshahi Diagnostic
IgG4 Disease General Principles of IgG4-related disease. EL Cluvar, AC Bateman Diagnostic Guidelines for IgG4-related disease with a focus on histopathological criteria. V Deshpande, A Khosroshahi Diagnostic
88-year-old Female with Lymphadenopathy. Faizi Ali, MD
 88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
IgG4 ᛶ ᝈ䛸 ᶫᮏ ᕫච ᛶ ⅖ ḷᒣ Ꮫ య Ꮫ ぬ㐨
 IgG4 Autoimmune pancreatitis Histopathological features: Diffuse lymphoplasmacytic infiltration Stromal fibrosis Acinar atrophy Obliterative phlebitis 1. Hamano et al reported that serum IgG4 levels were
IgG4 Autoimmune pancreatitis Histopathological features: Diffuse lymphoplasmacytic infiltration Stromal fibrosis Acinar atrophy Obliterative phlebitis 1. Hamano et al reported that serum IgG4 levels were
Pulmonary Sarcoidosis - Radiological Evaluation
 Original Research Article Pulmonary Sarcoidosis - Radiological Evaluation Jayesh Shah 1, Darshan Shah 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident, 3 Professor and HOD Radiology Department,
Original Research Article Pulmonary Sarcoidosis - Radiological Evaluation Jayesh Shah 1, Darshan Shah 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident, 3 Professor and HOD Radiology Department,
Overlap of IgG4-related Disease and Multicentric Castleman s Disease in a Patient with Skin Lesions
 CASE REPORT Overlap of IgG4-related Disease and Multicentric Castleman s Disease in a Patient with Skin Lesions Hiroki Mochizuki 1, Manako Kato 1, Takakazu Higuchi 2, Ryosuke Koyamada 2, Satoru Arai 3,
CASE REPORT Overlap of IgG4-related Disease and Multicentric Castleman s Disease in a Patient with Skin Lesions Hiroki Mochizuki 1, Manako Kato 1, Takakazu Higuchi 2, Ryosuke Koyamada 2, Satoru Arai 3,
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU
 Rex K.H. Au-Yeung Department of Pathology, HKU") Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
CASE 01 LA Path Slide Seminar 13 March, 08. Deepti Dhall, MD Department of Pathology and Laboratory Medicine Cedars-Sinai Medical Center
 CASE 01 LA Path Slide Seminar 13 March, 08 Deepti Dhall, MD Department of Pathology and Laboratory Medicine Cedars-Sinai Medical Center Clinical History 60 year old male presented with obstructive jaundice
CASE 01 LA Path Slide Seminar 13 March, 08 Deepti Dhall, MD Department of Pathology and Laboratory Medicine Cedars-Sinai Medical Center Clinical History 60 year old male presented with obstructive jaundice
Value of Serum IgG4 in the Diagnosis of Autoimmune Pancreatitis and in Distinguishing it from Acute and Chronic Pancreatitis of Other Etiology
 94 Jul 2017 Vol 10 No.3 North American Journal of Medicine and Science Original Research Value of Serum IgG4 in the Diagnosis of Autoimmune Pancreatitis and in Distinguishing it from Acute and Chronic
94 Jul 2017 Vol 10 No.3 North American Journal of Medicine and Science Original Research Value of Serum IgG4 in the Diagnosis of Autoimmune Pancreatitis and in Distinguishing it from Acute and Chronic
Autoimmune Diseases with Oral Manifestations
 Autoimmune Diseases with Oral Manifestations Martin S. Greenberg DDS, FDS RCSEd Professor Emeritus Department of Oral Medicine University of Pennsylvania Disclosure Statement I have no actual or potential
Autoimmune Diseases with Oral Manifestations Martin S. Greenberg DDS, FDS RCSEd Professor Emeritus Department of Oral Medicine University of Pennsylvania Disclosure Statement I have no actual or potential
Sonographic findings of immunoglobulin G4-related sc. Author(s) Akihiro; Nakamaru, Yuji; Hatanaka, Kanako C.; Shimiz
 Akihiro; Nakamaru, Yuji; Hatanaka, Kanako C.; Shimiz") Title Sonographic findings of immunoglobulin G4-related sc Omotehara, Satomi; Nishida, Mutsumi; Satoh, Megumi; Author(s) Akihiro; Nakamaru, Yuji; Hatanaka, Kanako C.; Shimiz CitationJournal of medical
Title Sonographic findings of immunoglobulin G4-related sc Omotehara, Satomi; Nishida, Mutsumi; Satoh, Megumi; Author(s) Akihiro; Nakamaru, Yuji; Hatanaka, Kanako C.; Shimiz CitationJournal of medical
Department of Dermatology, Nippon Medical School, 1-1-5, Sendagi, Bunkyo-ku, Tokyo , Japan 2
 Dermatology Research and Practice Volume 2010, Article ID 931340, 5 pages doi:10.1155/2010/931340 Case Report Paraneoplastic Pemphigus Presenting as Mild Cutaneous Features of Pemphigus Foliaceus and Lichenoid
Dermatology Research and Practice Volume 2010, Article ID 931340, 5 pages doi:10.1155/2010/931340 Case Report Paraneoplastic Pemphigus Presenting as Mild Cutaneous Features of Pemphigus Foliaceus and Lichenoid
Dermatopathology. Dr. Rafael Botella Estrada. Hospital La Fe de Valencia
 Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia DERMATOPATHOLOGY CASE CHALLENGE: RECOGNIZING MIMIS AND MASQUERADERS Rosalie Elenitsas. University of Pennsylvania Spectrum Lupus
Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia DERMATOPATHOLOGY CASE CHALLENGE: RECOGNIZING MIMIS AND MASQUERADERS Rosalie Elenitsas. University of Pennsylvania Spectrum Lupus
ESIM Winter School 2014 Case Presentation
 ESIM Winter School 2014 Case Presentation Hacettepe University School of Medicine Ankara/Turkey Ozant Helvaci, M.D. Patient T.K., 59 years old, male, married with one child, unemployed, place of birth/
ESIM Winter School 2014 Case Presentation Hacettepe University School of Medicine Ankara/Turkey Ozant Helvaci, M.D. Patient T.K., 59 years old, male, married with one child, unemployed, place of birth/
Review Article Orbital IgG4-Related Disease: Clinical Features and Diagnosis
 International Scholarly Research Network Volume 2012, Article ID 412896, 5 pages doi:10.5402/2012/412896 Review Article Orbital IgG4-Related Disease: Clinical Features and Diagnosis Toshinobu Kubota 1
International Scholarly Research Network Volume 2012, Article ID 412896, 5 pages doi:10.5402/2012/412896 Review Article Orbital IgG4-Related Disease: Clinical Features and Diagnosis Toshinobu Kubota 1
University of Groningen. Acantholysis in pemphigus van der Wier, Gerda
 University of Groningen Acantholysis in pemphigus van der Wier, Gerda IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the
University of Groningen Acantholysis in pemphigus van der Wier, Gerda IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the
Autoimmune pancreatitis (AIP) was described more than a
 was described more than a") CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2007;5:1229 1234 The Use of Immunoglobulin G4 Immunostaining in Diagnosing Pancreatic and Extrapancreatic Involvement in Autoimmune Pancreatitis MAESHA G. DEHERAGODA,*
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2007;5:1229 1234 The Use of Immunoglobulin G4 Immunostaining in Diagnosing Pancreatic and Extrapancreatic Involvement in Autoimmune Pancreatitis MAESHA G. DEHERAGODA,*
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
A case of bullous pemphigoid following pemphigus foliaceus
 #2228 A case of bullous pemphigoid following pemphigus foliaceus Priyanka Vedak MD 1, Danielle Levine MD 1,3, Lyn Duncan MD 2,3, Hensin Tsao 1,3, Daniela Kroshinsky MD MPH 1,3 1. Department of Dermatology,
#2228 A case of bullous pemphigoid following pemphigus foliaceus Priyanka Vedak MD 1, Danielle Levine MD 1,3, Lyn Duncan MD 2,3, Hensin Tsao 1,3, Daniela Kroshinsky MD MPH 1,3 1. Department of Dermatology,
Isolated Mass-Forming IgG4-Related Cholangitis as an Initial Clinical Presentation of Systemic IgG4-Related Disease
 Journal of Pathology and Translational Medicine 2016; 50: 300-305 CASE STUDY Isolated Mass-Forming IgG4-Related Cholangitis as an Initial Clinical Presentation of Systemic IgG4-Related Disease Seokhwi
Journal of Pathology and Translational Medicine 2016; 50: 300-305 CASE STUDY Isolated Mass-Forming IgG4-Related Cholangitis as an Initial Clinical Presentation of Systemic IgG4-Related Disease Seokhwi
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Overview of the Immunoglobulin G4-related Disease Spectrum
 Review Article The Korean Journal of Pancreas and Biliary Tract 2015;20:124-129 http://dx.doi.org/10.15279/kpba.2015.20.3.124 pissn 1976-3573 eissn 2288-0941 면역글로불린 G4 연관질환의개요 1 한림대학교의과대학한림대학교성심병원내과, 2
Review Article The Korean Journal of Pancreas and Biliary Tract 2015;20:124-129 http://dx.doi.org/10.15279/kpba.2015.20.3.124 pissn 1976-3573 eissn 2288-0941 면역글로불린 G4 연관질환의개요 1 한림대학교의과대학한림대학교성심병원내과, 2
manifestations are uncommon. Initial descriptions of the disease (Rosai and Dorfman, 1969) specifically
 specifically") Postgraduate Medical Journal (July 1980) 56, 521-525 Diffuse cutaneous involvement and sinus histiocytosis with massive lymphadenopathy A. A. WOODCOCK B.Sc., M.B., Ch.B., M.R.C.P. Summary Severe skin involvement
Postgraduate Medical Journal (July 1980) 56, 521-525 Diffuse cutaneous involvement and sinus histiocytosis with massive lymphadenopathy A. A. WOODCOCK B.Sc., M.B., Ch.B., M.R.C.P. Summary Severe skin involvement
Early Detection and Intervention of Coronary Artery Involvement in Immunoglobulin G4-related Disease
 doi: 10.2169/internalmedicine.7816-16 http://internmed.jp CASE REPORT Early Detection and Intervention of Coronary Artery Involvement in Immunoglobulin G4-related Disease Yoji Komiya 1, Makoto Soejima
doi: 10.2169/internalmedicine.7816-16 http://internmed.jp CASE REPORT Early Detection and Intervention of Coronary Artery Involvement in Immunoglobulin G4-related Disease Yoji Komiya 1, Makoto Soejima
Plasma cell myeloma (multiple myeloma)
") Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Unusual Involvement of IgG4-Related Sclerosing Disease in Lacrimal and Submandibular Glands and Extraocular Muscles
 pissn: 1011-8942 eissn: 2092-9382 Korean J Ophthalmol 2012;26(3):216-221 http://dx.doi.org/10.3341/kjo.2012.26.3.216 Case Report Unusual Involvement of IgG4-Related Sclerosing Disease in Lacrimal and Submandibular
pissn: 1011-8942 eissn: 2092-9382 Korean J Ophthalmol 2012;26(3):216-221 http://dx.doi.org/10.3341/kjo.2012.26.3.216 Case Report Unusual Involvement of IgG4-Related Sclerosing Disease in Lacrimal and Submandibular
IgG4-related Sclerosing Disease of the Lung without Pancreas Involvement: Presentation on 18F-FDG PET/CT
 J Radiol Sci 2013; 38: 129-133 IgG4-related Sclerosing Disease of the Lung without Pancreas Involvement: Presentation on 18F-FDG PET/CT Han-Jui Lee 1 Yi-Chen Yeh 2,3 Chun-Ku Chen 1,3 Rheun-Chuan Lee 1,3
J Radiol Sci 2013; 38: 129-133 IgG4-related Sclerosing Disease of the Lung without Pancreas Involvement: Presentation on 18F-FDG PET/CT Han-Jui Lee 1 Yi-Chen Yeh 2,3 Chun-Ku Chen 1,3 Rheun-Chuan Lee 1,3
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA. April 16, 2008
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
FOLLICULARITY in LYMPHOMA
 FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
A subset of ocular adnexal marginal zone lymphomas may arise in association with
 A subset of ocular adnexal marginal zone lymphomas may arise in association with IgG4-related disease 1)*, Yasuharu Sato 1) 2)*, Koh-ichi Ohshima 3), Katsuyoshi Takata 1), Tomoko Miyata-Takata 1), Mai
A subset of ocular adnexal marginal zone lymphomas may arise in association with IgG4-related disease 1)*, Yasuharu Sato 1) 2)*, Koh-ichi Ohshima 3), Katsuyoshi Takata 1), Tomoko Miyata-Takata 1), Mai
Introduction to Immunopathology
 MICR2209 Introduction to Immunopathology Dr Allison Imrie 1 Allergy and Hypersensitivity Adaptive immune responses can sometimes be elicited by antigens not associated with infectious agents, and this
MICR2209 Introduction to Immunopathology Dr Allison Imrie 1 Allergy and Hypersensitivity Adaptive immune responses can sometimes be elicited by antigens not associated with infectious agents, and this
Common things are common, but not always the answer
 Kevin Conroy, Joe Mackenzie, Stephen Cowie kevin.conroy@nhs.net Respiratory Dept, Darlington Memorial Hospital, Darlington, UK. Common things are common, but not always the answer Case report Cite as:
Kevin Conroy, Joe Mackenzie, Stephen Cowie kevin.conroy@nhs.net Respiratory Dept, Darlington Memorial Hospital, Darlington, UK. Common things are common, but not always the answer Case report Cite as:
Figure 2: Lymph node Cortical follicular (F) and paracortical (PC) atrophy, with narrowing of the cortex relative to the medulla (M).
 and paracortical (PC) atrophy, with narrowing of the cortex relative to the medulla (M).") Figure 1: Lymph node Follicular hyperplasia, with expansion of the follicular germinal centres (F) by large blast cells. Paracortical hyperplasia, with expansion of the paracortex (PC) by small lymphocytes.
Figure 1: Lymph node Follicular hyperplasia, with expansion of the follicular germinal centres (F) by large blast cells. Paracortical hyperplasia, with expansion of the paracortex (PC) by small lymphocytes.
Long-term Outcome of Autoimmune Pancreatitis after Oral Prednisolone Therapy
 ORIGINAL ARTICLE Long-term Outcome of Autoimmune Pancreatitis after Oral Prednisolone Therapy Takayoshi Nishino 1, Fumitake Toki 2,HiroyasuOyama 3, Kyoko Shimizu 1 and Keiko Shiratori 1 Abstract Objective
ORIGINAL ARTICLE Long-term Outcome of Autoimmune Pancreatitis after Oral Prednisolone Therapy Takayoshi Nishino 1, Fumitake Toki 2,HiroyasuOyama 3, Kyoko Shimizu 1 and Keiko Shiratori 1 Abstract Objective
Case No. 5; Slide No. B13/8956/2
 Interface diseases Case No. 5; Slide No. B13/8956/2 Histological findings Severe hydropic vacuolation of epidermal and follicular basal cells/ interface dermatitis Multifocally apoptotic keratinocytes
Interface diseases Case No. 5; Slide No. B13/8956/2 Histological findings Severe hydropic vacuolation of epidermal and follicular basal cells/ interface dermatitis Multifocally apoptotic keratinocytes
22 year old QH mare with regionally extensive alopecia and scaling on one front limb and ventral chest (Figure 1 and 2).
.") 22 year old QH mare with regionally extensive alopecia and scaling on one front limb and ventral chest (Figure 1 and 2). Which of the following is the most likely disease? a. Sterile granuloma complex
22 year old QH mare with regionally extensive alopecia and scaling on one front limb and ventral chest (Figure 1 and 2). Which of the following is the most likely disease? a. Sterile granuloma complex
HYPERSENSITIVITY REACTIONS D R S H O AI B R AZ A
 HYPERSENSITIVITY REACTIONS D R S H O AI B R AZ A HYPERSENSITIVITY REACTIONS Are exaggerated immune response upon antigenic stimulation Individuals who have been previously exposed to an antigen are said
HYPERSENSITIVITY REACTIONS D R S H O AI B R AZ A HYPERSENSITIVITY REACTIONS Are exaggerated immune response upon antigenic stimulation Individuals who have been previously exposed to an antigen are said
Adaptive Immunity: Humoral Immune Responses
 MICR2209 Adaptive Immunity: Humoral Immune Responses Dr Allison Imrie 1 Synopsis: In this lecture we will review the different mechanisms which constitute the humoral immune response, and examine the antibody
MICR2209 Adaptive Immunity: Humoral Immune Responses Dr Allison Imrie 1 Synopsis: In this lecture we will review the different mechanisms which constitute the humoral immune response, and examine the antibody
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
Rameshwar Gutte and Uday Khopkar
 Extragenital unilateral lichen sclerosus et atrophicus in a child: a case report Rameshwar Gutte and Uday Khopkar Department of Dermatolgy, Seth GSMC and KEM Hospital, Parel, Mumbai-400012, India Egyptian
Extragenital unilateral lichen sclerosus et atrophicus in a child: a case report Rameshwar Gutte and Uday Khopkar Department of Dermatolgy, Seth GSMC and KEM Hospital, Parel, Mumbai-400012, India Egyptian
Case Report Thoracic Paravertebral Mass as an Infrequent Manifestation of IgG4-Related Disease
 Hindawi Case Reports in Rheumatology Volume 2017, Article ID 4716245, 4 pages https://doi.org/10.1155/2017/4716245 Case Report Thoracic Paravertebral Mass as an Infrequent Manifestation of IgG4-Related
Hindawi Case Reports in Rheumatology Volume 2017, Article ID 4716245, 4 pages https://doi.org/10.1155/2017/4716245 Case Report Thoracic Paravertebral Mass as an Infrequent Manifestation of IgG4-Related
B cell activation and antibody production. Abul K. Abbas UCSF
 1 B cell activation and antibody production Abul K. Abbas UCSF 2 Lecture outline B cell activation; the role of helper T cells in antibody production Therapeutic targeting of B cells 3 Principles of humoral
1 B cell activation and antibody production Abul K. Abbas UCSF 2 Lecture outline B cell activation; the role of helper T cells in antibody production Therapeutic targeting of B cells 3 Principles of humoral
Differential diagnosis
 Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
Update in deposition diseases
 Genoa, Italy Update in deposition diseases Prof. Franco Rongioletti, Section of Dermatology, Chair of Dermatopathology, University of Genoa,Italy Cutaneous deposition disorders Endogenous Exogenous Cutaneous
Genoa, Italy Update in deposition diseases Prof. Franco Rongioletti, Section of Dermatology, Chair of Dermatopathology, University of Genoa,Italy Cutaneous deposition disorders Endogenous Exogenous Cutaneous
Egyptian Dermatology Online Journal Vol. 6 No 1: 14, June 2010
 Wells Syndrome H. Gammaz, H. Amer, A. Adly and S. Mahmoud Egyptian Dermatology Online Journal 6 (1): 14 Al-Haud Al-Marsoud Hospital, Cairo, Egypt e-mail: hananderma@hotmail.com Submitted: April 15, 2010
Wells Syndrome H. Gammaz, H. Amer, A. Adly and S. Mahmoud Egyptian Dermatology Online Journal 6 (1): 14 Al-Haud Al-Marsoud Hospital, Cairo, Egypt e-mail: hananderma@hotmail.com Submitted: April 15, 2010
ITO, Yasuhiro ; FUJII, Mizue ; SHIBUYA, Takashi ; UEHARA, Jiro ; SATO, Katsuhiko ; IIZUKA, Hajime
 Journal of Dermatology (2011) 38(5):515-517. Granulocyte colony stimulating factor-producing squamous cell carcinoma of the skin ITO, Yasuhiro ; FUJII, Mizue ; SHIBUYA, Takashi ; UEHARA, Jiro ; SATO, Katsuhiko
Journal of Dermatology (2011) 38(5):515-517. Granulocyte colony stimulating factor-producing squamous cell carcinoma of the skin ITO, Yasuhiro ; FUJII, Mizue ; SHIBUYA, Takashi ; UEHARA, Jiro ; SATO, Katsuhiko
Introduction. Results. Discussion. Histopathologic and immunohistochemical findings. Results. conclusions,
 1/5 2/5 Carcinoma distinctive carcinoma. form erysipeloides (CE), metastasis. which clinically Itfrom has resembles been termed erysipelas, is an uncommon, but may extend It164 toclassically back, presents
1/5 2/5 Carcinoma distinctive carcinoma. form erysipeloides (CE), metastasis. which clinically Itfrom has resembles been termed erysipelas, is an uncommon, but may extend It164 toclassically back, presents
New lung lesion in a 55 year-old male treated with chemoradiation for non-small cell lung carcinoma
 July 2016 New lung lesion in a 55 year-old male treated with chemoradiation for non-small cell lung carcinoma Contributed by: Laurel Rose, MD, Resident Physician, Indiana University School of Medicine,
July 2016 New lung lesion in a 55 year-old male treated with chemoradiation for non-small cell lung carcinoma Contributed by: Laurel Rose, MD, Resident Physician, Indiana University School of Medicine,
Test Name Results Units Bio. Ref. Interval
 135091662 Age 45 Years Gender Male 29/8/2017 120000AM 29/8/2017 100215AM 29/8/2017 110825AM Ref By Final RHEUMATOID AUTOIMMUNE COMREHENSIVE ANEL ANTI NUCLEAR ANTIBODY / FACTOR (ANA/ANF), SERUM ----- 20-60
135091662 Age 45 Years Gender Male 29/8/2017 120000AM 29/8/2017 100215AM 29/8/2017 110825AM Ref By Final RHEUMATOID AUTOIMMUNE COMREHENSIVE ANEL ANTI NUCLEAR ANTIBODY / FACTOR (ANA/ANF), SERUM ----- 20-60
Department of Radiology, Korea University Anam Hospital, Korea University College of Medicine, Seoul, Korea 2
 Case Report pissn 1738-2637 / eissn 2288-2928 J Korean Soc Radiol 2018;79(5):276-281 https://doi.org/10.3348/jksr.2018.79.5.276 Sequential CT Findings in Two Cases of Immunoglobulin G4-Related Lung Disease:
Case Report pissn 1738-2637 / eissn 2288-2928 J Korean Soc Radiol 2018;79(5):276-281 https://doi.org/10.3348/jksr.2018.79.5.276 Sequential CT Findings in Two Cases of Immunoglobulin G4-Related Lung Disease:
Infections and nonmicrobial inflammatory stimuli can cause leukocytosis (as seen in Lab 1) as well as lymph node enlargement (lymphadenopathy).
 as well as lymph node enlargement (lymphadenopathy).") LAB 5: LYMPHOID TISSUE AND SKIN The focus of this week s lab will be pathology of the lymphoid tissue and skin. The lymphoid organs include the thymus, spleen, and lymph nodes. Abnormalities in the lymph
LAB 5: LYMPHOID TISSUE AND SKIN The focus of this week s lab will be pathology of the lymphoid tissue and skin. The lymphoid organs include the thymus, spleen, and lymph nodes. Abnormalities in the lymph
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
CLINCOPATHOLOGICAL CASE
 CLINCOPATHOLOGICAL CASE Generalized vesiculo-bullous and pustular eruption in an adult man Hassab El-Naby H, MD, El-Khalawany M, MD Department of Dermatology, Al-Azhar University, Cairo, Egypt CLINICAL
CLINCOPATHOLOGICAL CASE Generalized vesiculo-bullous and pustular eruption in an adult man Hassab El-Naby H, MD, El-Khalawany M, MD Department of Dermatology, Al-Azhar University, Cairo, Egypt CLINICAL
Among the benign intraepithelial melanocytic proliferations, Inflamed Conjunctival Nevi. Histopathological Criteria. Resident Short Reviews
 Resident Short Reviews Inflamed conjunctival nevi (ICN) may suggest malignancy because of their rapid growth and atypical histology. The objective of this study was to characterize the diagnostic features
Resident Short Reviews Inflamed conjunctival nevi (ICN) may suggest malignancy because of their rapid growth and atypical histology. The objective of this study was to characterize the diagnostic features
Kidney disease associated with autoimmune disease
 Kidney disease associated with autoimmune disease Masaomi Nangaku Division of Nephrology and Endocrinology the University of Tokyo Graduate School of Medicine, Japan M-type Phospholipase A2 Receptor as
Kidney disease associated with autoimmune disease Masaomi Nangaku Division of Nephrology and Endocrinology the University of Tokyo Graduate School of Medicine, Japan M-type Phospholipase A2 Receptor as
Annular elastolytic giant cell granuloma presented with annular erythematous patches over the face and cheek in a Chinese lady
 Hong Kong J. Dermatol. Venereol. (2009) 17, 151-155 Case Report Annular elastolytic giant cell granuloma presented with annular erythematous patches over the face and cheek in a Chinese lady SKF Loo, LY
Hong Kong J. Dermatol. Venereol. (2009) 17, 151-155 Case Report Annular elastolytic giant cell granuloma presented with annular erythematous patches over the face and cheek in a Chinese lady SKF Loo, LY
Case Report IgG4-Related Nasal Pseudotumor
 Case Reports in Otolaryngology Volume 2015, Article ID 749890, 4 pages http://dx.doi.org/10.1155/2015/749890 Case Report IgG4-Related Nasal Pseudotumor L. K. Døsen, 1 P. Jebsen, 2 B. Dingsør, 3 and R.
Case Reports in Otolaryngology Volume 2015, Article ID 749890, 4 pages http://dx.doi.org/10.1155/2015/749890 Case Report IgG4-Related Nasal Pseudotumor L. K. Døsen, 1 P. Jebsen, 2 B. Dingsør, 3 and R.
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated inflammation
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated inflammation
Lymphocytoma Cutis. Cynthia M. Magro MD. Director of Dermatopathology Weill Medical College of Cornell University New York, New York
 Lymphocytoma Cutis Cynthia M. Magro MD Professor of Pathology Director of Dermatopathology Weill Medical College of Cornell University New York, New York Lymphocytoma Cutis Falls under other designations
Lymphocytoma Cutis Cynthia M. Magro MD Professor of Pathology Director of Dermatopathology Weill Medical College of Cornell University New York, New York Lymphocytoma Cutis Falls under other designations
CHEST. Postgraduate Education Corner. Adenopathy and Pulmonary Infiltrates in a Japanese Emigrant in Brazil
 CHEST Postgraduate Education Corner CHEST IMAGING AND PATHOLOGY FOR CLINICIANS Adenopathy and Pulmonary Infiltrates in a Japanese Emigrant in Brazil Alexandre M. Kawassaki, MD ; Hironori Haga, MD ; Thiago
CHEST Postgraduate Education Corner CHEST IMAGING AND PATHOLOGY FOR CLINICIANS Adenopathy and Pulmonary Infiltrates in a Japanese Emigrant in Brazil Alexandre M. Kawassaki, MD ; Hironori Haga, MD ; Thiago
CPC. Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand
 CPC Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand A 53 year-old woman with fever, facial swelling and rashes on face, trunk and upper extremities for 3
CPC Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand A 53 year-old woman with fever, facial swelling and rashes on face, trunk and upper extremities for 3
Autoimmune pancreatitis (AIP) can be defined as a
 can be defined as a") CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:1010 1016 Diagnosis of Autoimmune Pancreatitis: The Mayo Clinic Experience SURESH T. CHARI,* THOMAS C. SMYRK, MICHAEL J. LEVY,* MARK D. TOPAZIAN,* NAOKI
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:1010 1016 Diagnosis of Autoimmune Pancreatitis: The Mayo Clinic Experience SURESH T. CHARI,* THOMAS C. SMYRK, MICHAEL J. LEVY,* MARK D. TOPAZIAN,* NAOKI
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
B. Autoimmune blistering diseases
 Go Back to the Top To Order, Visit the Purchasing Page for Details formation immediately above the basal layer. The dermal papillae, which are covered by basal cells in the single layer that is left in
Go Back to the Top To Order, Visit the Purchasing Page for Details formation immediately above the basal layer. The dermal papillae, which are covered by basal cells in the single layer that is left in
Title: Erythema annulare centrifugum associated with chronic lymphocytic leukaemia. Authors: Helbling I, Walewska R, Dyer MJS, Bamford M, Harman KE
 Title: Erythema annulare centrifugum associated with chronic lymphocytic leukaemia Authors: Helbling I, Walewska R, Dyer MJS, Bamford M, Harman KE Sir, A wide range of conditions have been described as
Title: Erythema annulare centrifugum associated with chronic lymphocytic leukaemia Authors: Helbling I, Walewska R, Dyer MJS, Bamford M, Harman KE Sir, A wide range of conditions have been described as
Case Rep Dermatol 2009;1:66 70 DOI: / Key Words Coma Blister Barbiturate Overdose Meningoencephalitis
 66 Coma Blisters Joana Rocha a Teresa Pereira a Filipa Ventura a Fernando Pardal b Celeste Brito a Departments of a Dermatology and b Pathology, Hospital de São Marcos, Braga, Portugal Key Words Coma Blister
66 Coma Blisters Joana Rocha a Teresa Pereira a Filipa Ventura a Fernando Pardal b Celeste Brito a Departments of a Dermatology and b Pathology, Hospital de São Marcos, Braga, Portugal Key Words Coma Blister
HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT
 HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT Nirmala Ponnuthurai, Sabeera Begum, Lee Bang Rom Paediatric Dermatology Unit, Institute of Paediatric, Hospital Kuala Lumpur, Malaysia Abstract
HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT Nirmala Ponnuthurai, Sabeera Begum, Lee Bang Rom Paediatric Dermatology Unit, Institute of Paediatric, Hospital Kuala Lumpur, Malaysia Abstract
How 5 Diseases Became One. Moez Tajdin R3 McGill University
 How 5 Diseases Became One Moez Tajdin R3 McGill University Conflicts of Interest None! Mr. M. ID: 65 M PMH Benign prostatic hyperplasia Prostate cancer Awaiting biopsy Skin rash Dyslipidemia Hypertension
How 5 Diseases Became One Moez Tajdin R3 McGill University Conflicts of Interest None! Mr. M. ID: 65 M PMH Benign prostatic hyperplasia Prostate cancer Awaiting biopsy Skin rash Dyslipidemia Hypertension
Refractory bilateral scrotal ulcers with numerous IgG4-positive plasma cells: Another skin location for IgG4-related sclerosing disease
 www.edoriumjournals.com CASE REPORT OPEN ACCESS Refractory bilateral scrotal ulcers with numerous IgG4-positive plasma cells: Another skin location for IgG4-related sclerosing disease Jaclyn L Jerz, Jae
www.edoriumjournals.com CASE REPORT OPEN ACCESS Refractory bilateral scrotal ulcers with numerous IgG4-positive plasma cells: Another skin location for IgG4-related sclerosing disease Jaclyn L Jerz, Jae
Case Reports in Clinical Pathology, 2015, Vol. 2, No. 1
 CASE REPORT A case of IgG4-related interstitial lung disease showing usual interstitial pneumonia pattern: Unusual case for histological features with pathological proof Seidai Sato 1, Masaki Hanibuchi
CASE REPORT A case of IgG4-related interstitial lung disease showing usual interstitial pneumonia pattern: Unusual case for histological features with pathological proof Seidai Sato 1, Masaki Hanibuchi
Pulmonary function tests findings and their diagnostic value in patients with IgG4-related disease
 Original Article Pulmonary function tests findings and their diagnostic value in patients with IgG4-related disease Lu Cao, Yi-Bing Chen, Da-Hui Zhao, Wen-Fang Shi, Song Meng, Li-Xin Xie Department of
Original Article Pulmonary function tests findings and their diagnostic value in patients with IgG4-related disease Lu Cao, Yi-Bing Chen, Da-Hui Zhao, Wen-Fang Shi, Song Meng, Li-Xin Xie Department of
Summary. lymphoma/myeloma, regulatory T cells (T reg) Introduction. Clinical and Experimental Immunology ORIGINAL ARTICLE doi: /cei.
 Introduction. Clinical and Experimental Immunology ORIGINAL ARTICLE doi: /cei.") bs_bs_banner Clinical and Experimental Immunology ORIGINAL ARTICLE doi:1.1111/cei.1273 Increased frequency of skin-infiltrating FoxP3 + regulatory T cells as a diagnostic indicator of severe atopic dermatitis
bs_bs_banner Clinical and Experimental Immunology ORIGINAL ARTICLE doi:1.1111/cei.1273 Increased frequency of skin-infiltrating FoxP3 + regulatory T cells as a diagnostic indicator of severe atopic dermatitis
Case Report A Retrospectively Diagnosed Case of IgG4-Related Tubulointerstitial Nephritis Showing Good Renal Outcome and Pathological Progress
 Hindawi Publishing Corporation Volume 213, Article ID 953214, 7 pages http://dx.doi.org/1.1155/213/953214 Case Report A Retrospectively Diagnosed Case of IgG4-Related Tubulointerstitial Nephritis Showing
Hindawi Publishing Corporation Volume 213, Article ID 953214, 7 pages http://dx.doi.org/1.1155/213/953214 Case Report A Retrospectively Diagnosed Case of IgG4-Related Tubulointerstitial Nephritis Showing