Insulin Regimens: Hitting Glycemia Targets
|
|
|
- Hester Arnold
- 5 years ago
- Views:
Transcription
1 Insulin Regimens: Hitting Glycemia Targets Grant Kelley MD March 1 st, 2018
2 Faculty Disclosure: Financial relationships with commercial interests None
3 Overview Mortality and Morbidity Insulin and Insulin analogs. Target Glucose Four steps to calculate insulin regimen 1. Total Daily Dose (TDD) 2. Basal Insulin 3. Nutritional Insulin 4. Correction Insulin New SQ Insulin Order Set Cases 70 kg DM2 outpatient Glyburide and Januvia with A1c kg DM2 outpatient 90U 70/30 am and 45U 70/30 hs with A1c kg DM2 outpatient 80U Lantus and Metformin with A1c10 70kg DM1 outpatient 21L and sliding scale with meals with A1c7 60kg DM1 insulin pump basal unconscious after CVA.
4 Diabetes Type 1 Type 2 Onset Sudden Gradual Age Onset Children/Adolescent Adult Body Habitus Thin/Normal Obese Ketoacidosis Risk Common Rare Autoantibody Usually present Absent Endogenous Insulin Low or absent Normal, decreased, increased Genetic concordance identical twins 50% 90% Prevalence 10% 90% Treatment Insulin Oral agents and Insulin 1) Basal Insulin Absolute Requirement in DM1 2) Stop Oral Agents in DM2
5 Morbidity and Mortality and Hypoglycemia Increase in inpatient mortality risk: mg/dl adjusted odds ratio (OR) 1.62 <40 mg/dl adjusted odds ratio (OR) 2.05 Increase LOS cw >70mg/dL group: mg/dl 1.51 fold <40 mg/dl 2.33 fold Diabetes Med. 12:e445-8, 2012
6 Morbidity and Hyperglycemia 1. Fluid and electrolyte abnormalities secondary to osmotic diuresis 2. Decreased WBC function 3. Delayed gastric emptying 4. Increased surgical complications including: Glc > 220 mg/dl - relative risk postop nosocomial infection 5.7 fold. Glc mg/dl - relative odds of wound infection to Glc >253 mg/dl - relative odds of wound infection to LOS with fluctuating (glucose <60 or >250 mg/dl) vs control (glucose mg/dl).

7 Insulin Signaling
8 Hyperglycemia and Poor Hospital Outcome Metabolic stress response stress hormones and peptides Glucose Insulin Reactive O2 species Immune dysfunction Infection dissemination FFA Ketones Lactate Cellular injury/apoptosis Inflammation Tissue damage Altered tissue wound repair Clement et al, Diabetes Care 27: , 2004 Prolonged hospital stay Disability / Death Transcription factors Secondary mediators

9 Target St Joseph s Hospital (80-200) mg/dl Outpatient Fasting mg/dl -SICU/MICU Ann Intern Med 154: , Intensive Insulin Therapy in Hospitalized Patients: A Systemic Review. Ann Intern Med 154: , Standards of Medical Care in Diabetes DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY
10 INSULINS



11 INSULIN HISTORICAL PERSPECTIVE Discovery: : Banting, Best, Macleod, Campbell, and Fletcher discovered insulin Nobel Prizes: 1923: Banting and Macleod Nobel Prize in Physiology or Medicine:. 1958: Frederick Sanger Nobel Prize sequencing insulin. 1969: Dorothy Hodgkin Nobel Prize tertiary structure X-Ray diffraction. 1977: Rosalyn Yalow Nobel Prize radioimmunoassay for insulin Davidson, Clinical Diabetes Mellitus; Kahn and Weir Joslin's Diabetes Mellitus


12 Insulin Beef and Pork Insulin: -1920s s insulin purified from beef or pork pancreata 1L insulin from pig pancreata shown Human Recombinant Insulin: -1980s recombinant DNA technology -produce human insulin in Saccharomyces cerevisiae or E coli. Human Insulin Analogs: -2000s recombinant DNA technology -development of human insulin analogs. -engineered to alter pharmacokinetics absorption from subcutaneous tissue binding to proteins. classroom.sdmesa.net/eschmid/lab7-biol210.htm

13 (Lantus) (Levemir) Degludec (Triceba) Des-B30 De Glu (deleted Glu) +16C diacid dec (hexadecanedioic acid added)
14
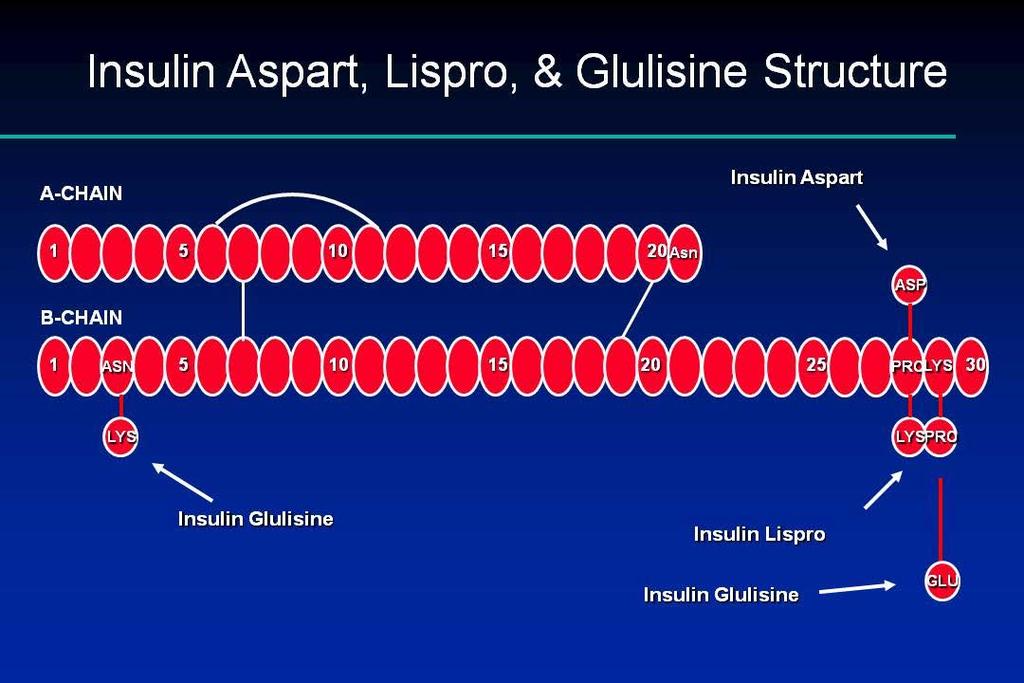
, glulisine (Apidra) and lispro (Humalog) modified to decrease heximer and dimer formation.")
15 Regular ( ) human, crystalline zinc insulins. Insulin preparations NPH (neutral protamine Hagedorn; 1936) protamine complex to delay absorption. Rapid acting analogs: aspart (Novolog), glulisine (Apidra) and lispro (Humalog) modified to decrease heximer and dimer formation. Long acting analogs: glargine (Lantus, Toujeo 300U/mL, Basaglar), detemir (Levemir) and degludec (Tiseba) modified to slow absorption kinectics: -glargine, degludec soluble at ph 4.0 but precipitates at physiologic ph upon SC injection. -detemir: binds albumin through its engineered fatty acid moiety. Mixtures: e.g. Humulin 70/30, Humalog 75/25
16 Insulin Profiles Toujeo (U300 glargine) Basaglar (glargine) Triseba (degludec )
17 Insulin Profiles: Best Insulin to Cover Glucose 1. Basal 2. Nutritional 3. Correction Insulin Effect NPH Detemir (Levemir) Glargine (Lantus) Regular Lispro (Humalog) Aspart (Novolog) Glulisine (Apidra) Inhaled insulin Time (hours) Society of Hospital Medicine
18 Insulin Profiles: Stacking Insulin given before a previous dose is gone will stack onto the previous dose Insulin Effect Time (hours) Society of Hospital Medicine


19 Insulin Profiles Avoid Mixtures In Hospital: 70/30; 75/25
20 INSULIN REGIMEN: TOTAL DAILY DOSE (TDD)
21 Basal Bolus Insulin Regimen Basal Insulin: Insulin to cover glucose produced by the liver/kidneys Bolus Insulin: Nutritional + Correction Nutritional: insulin to cover meal carbs. Correction: insulin to correct blood glucose to target.
22 Basal, Bolus, and Correction Insulin 400 Glucose and Insulin Profiles Breakfast Lunch Dinner Basal Insulin Nutritional Insulin Correction Insulin Glucose (mg/dl)
23 Physiologic Insulin Secretion: Basal/Bolus Concept Insulin (µu/ml) Nutritional (Prandial) Insulin Basal Insulin Breakfast Lunch Supper Glucose (mg/dl) Nutritional Glucose Basal Glucose A.M. P.M. Time of Day The 50/50 Rule
24 Four Steps to Calculate Basal Bolus Insulin Using Total Daily Dose 1. TDD (total daily dose): Daily insulin requirement. 2. Basal (~50% TDD): Insulin to cover glucose produced by the liver/kidneys. 3. Nutritional (~50% TDD): Insulin to cover meal carbs. 4. Correction (TDD dependent): Insulin to correct blood glucose to target.
25 Step 1) Calculate Total Daily Dose (TDD) 1) Preadmission Insulin: add insulin per day = TDD (best indication) beware of high doses of basal insulin (110 U Lantus no bolus) 2) Weight Based: Frail: Average: Resistant: U/kg/day (eg. thin, new DM1) (50kg=15U) U/kg/day (eg. new DM2) (70kg=35U) U/kg/day (eg. Obese DM2) (100kg=70U) 3) Insulin drip-based: add last 20h = TDD (careful with high rates) average rate last 4 hours x 20 = TDD ***Best educated guess use all available info! ***Average nondiabetic TDD ~30U.

26 Step 2) Calculate Basal Insulin 50/50 rule Basal insulin is ~ 50% of TDD. eg. TDD=36U/day then basal ~ 18U Lantus. Long acting insulin: Glargine (Lantus) (once a day) Detemir (Levemir) (once-twice a day) NPH (twice a day)
27 Advanced Calculation: Nutritional Calculate Nutritional Insulin Insulin Carbohydrate Ratio = 500 rule ~500/TDD = g Carb per U of insulin. e.g. TDD=180U/day 500/180 = 2.8 so 1U insulin required per 2.8 g Carb 60g Carbohydrate average ADA meal 60/2.8~20U Using Insulin, John Walsh et al, Torrey Pines Press

28 Step 3) Calculate Nutritional Insulin 50/50 rule Nutritional insulin is ~ 50% of TDD divided between 3 meals. eg. TDD=36U/day ~ 18/3=6U/meal. Rapid or Short acting insulin: Glulisine (Apidra) Aspart (Novolog) Lispro (Humalog) Regular (Novolin, Humulin)
29 Step 4) Calculate Correction Insulin Insulin required to correct hyperglycemia to target. Use Rapid or Short acting insulin. Dependent on sensitivity or TDD. Target Frail TDD<40 1U/50 Average U/ U/50 Obese >120 4U/ >420 MD
30 Advanced Calculation: Correction Step 4) Correction Insulin Sensitivity = 1800 rule ~1800/TDD = mg/dl glc change per U insulin. e.g. TDD=180U/day 1800/180=10 so 1U insulin will drop glc 10mg/dl. To correct 300mg/dl / 10 = 30U Using Insulin, John Walsh et al, Torrey Pines Press

31 Grid Nutritional and Correction Insulin (Bolus)
32 Ordering SQ Insulin NEW SQ Insulin order set

33 Medication Section of New SC Insulin Order Set

34 Medication Section of New SC Insulin Order Set

35 MAR: SC Insulin Order Target
36 Daily Adjustments Monitor glucose levels daily Consideration for changing sensitivity Steroids Improving condition (sepsis, etc.) Increase or decrease TDD by 10-20% TDD 36 x 1.2 ~ 42 TDD 36 x 0.8 ~ 28
37 Daily Adjustments Evaluate Glucose Measurements: basal: fasting changes reflect basal insulin. -if fasting hs to am need more long-acting insulin. -if fasting hs to am need less long-acting insulin. -if fasting hs to am good. bolus (nutrition + correction): next premeal should correct to target.

38 Review Patient Glycemia and Insulin Administration

39 Review Patient Glycemia and Insulin Administration
40 DISCHARGE TOOLS

41 Add Nutritional Scale to AVS
42 Nutritional Scale Added to AVS
43 CASES
44 Case 1: Four Step Calculation 70 kg DM2 outpatient Glyburide and Januvia with A1c 7 1. TDD: 2. Basal: 3. Nutritional: 4. Correction: (no hm ins) or (0.3U/kg=21U) 10U Lantus 3U Humalog ac Built into order set The patient is made NPO and POC Glc have been mg/dL. How should the insulin dosing be changed?
45 Medication Section of New SC Insulin Order Set X 10 Units Lantus X
46 Case 2: Four Step Calculation 140 kg DM2 outpatient 90U 70/30 am and 45U 70/30 hs with A1c 8 1. TDD: 2. Basal: 3. Nutritional: 4. Correction: 108U (135Ux.8) or (0.7U/kg=98U) 54U Lantus 18U Humalog ac Built into order set The patient is made NPO and POC Glc have been mg/dL. How should the insulin dosing be changed?
47 X 54 Units Lantus X
48 Case 3: Four Step Calculation 100 kg DM2 outpatient 80U Lantus and Metformin with A1c10 1. TDD: 64U (80Ux.8) or (0.7U/kg=70U) 2. Basal: 32U Lantus 3. Nutritional: 10U Humalog ac 4. Correction: Built into order set
49 X 32 Units Lantus X
50 Case 3 part b: Four Step Calculation 100 kg DM2 outpatient 80U Lantus and Metformin with A1c10 1. TDD: 64U (80Ux.8) or (0.7U/kg=70U) 2. Basal: 32U Lantus 3. Nutritional: 10U Humalog ac 4. Correction: Built into order set POC Glc range from mg/dl. What would you do? 1. TDD: 64x1.2=76; 64x1.1=70 2. Basal: 38U Lantus 3. Nutritional: 12U Humalog ac 4. Correction: Built into order set
51 X 38 Units Lantus X
52 Case 4: Four Step Calculation 70kg DM1 outpatient 21L and sliding scale with meals with A1c7 1. TDD: 2. Basal: 3. Nutritional: 4. Correction: 40U (21b+21nutr) or (0.5U/kg=35U) 18U Lantus 6U Humalog ac Built into order set The patient is made NPO, how should the insulin dosing be changed? Should a patient with DM1 ever not get basal insulin? Patients with DM1 absolutely require insulin or they will develop DKA.
53 X 18 Units Lantus X
54 Case 4 part b: Four Step Calculation 70kg DM1 outpatient 21L and sliding scale with meals with A1c7 1. TDD: 2. Basal: 3. Nutritional: 4. Correction: 40U (21b+21nutr) or (0.5U/kg=35U) 18U Lantus 6U Humalog ac Built into order set POC between and steroids tapered. What would you do? 1. TDD: 2. Basal: 3. Nutritional: 4. Correction: 36x0.8=28; 36x0.9=32 15U Lantus 5U Humalog ac Built into order set
55 X 15 Units Lantus X
56 Case 5: Four Step Calculation 60kg DM1 insulin pump basal 12 basal and 4 nutritional with A1c8 and unconscious after CVA 1. TDD: 24U (12+12) or (0.4U/kg=24U) 2. Basal: 12U Lantus 3. Nutritional: 4U Humalog ac 4. Correction: Built into order set
57 X 12 Units Lantus X
58 Summary Hyperglycemia and Hypoglycemia associated with increased morbidity, mortality, and LOS Four Steps to Calculate Basal Bolus Insulin 1. TDD (calculate: preadmission insulin, weight based, insulin gtt) 2. Basal (~50% TDD) 3. Nutritional (~50% TDD: 60g carb meal) 4. Correction (calculation intrinsic to Order Set)
Insulin Prior Authorization with optional Quantity Limit Program Summary
 Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols. Askiel Bruno, MD, MS Protocol PI
 Trial Treatment Protocols. Askiel Bruno, MD, MS Protocol PI") Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI SHINE Synopsis Acute ischemic stroke
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI SHINE Synopsis Acute ischemic stroke
Disclosure 1/16/2017. Michael R. Brennan D.O., M.S., F.A.C.E Director Beaumont Endocrine Center Chief of Endocrine Beaumont Grosse Pointe 1/16/2017 2
 Therapy For Diabetes Michigan Association of Osteopathic Family Physicians Mid-Winter Family Medicine Update Shanty Creek Resort, MI January 19-22nd 2017 Michael R. Brennan D.O., M.S., F.A.C.E Director
Therapy For Diabetes Michigan Association of Osteopathic Family Physicians Mid-Winter Family Medicine Update Shanty Creek Resort, MI January 19-22nd 2017 Michael R. Brennan D.O., M.S., F.A.C.E Director
Type I Type II Insulin Resistance
 Insulin An aqueous hormonal solution made in the pancreas. Affects metabolism by allowing glucose to leave the blood and enter the body cells, preventing hyperglycemia. It is measured in units, e.g. 100
Insulin An aqueous hormonal solution made in the pancreas. Affects metabolism by allowing glucose to leave the blood and enter the body cells, preventing hyperglycemia. It is measured in units, e.g. 100
Type 2 Diabetes Mellitus Insulin Therapy 2012
 Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Inpatient Diabetes Management: The Slippery Slope of Sliding Scale Insulin
 Inpatient Diabetes Management: The Slippery Slope of Sliding Scale Insulin David Newman, MD University of North Dakota School of Medicine Sanford Health Big Sky Conference 2017 Dr. David Newman, Personal/Professional
Inpatient Diabetes Management: The Slippery Slope of Sliding Scale Insulin David Newman, MD University of North Dakota School of Medicine Sanford Health Big Sky Conference 2017 Dr. David Newman, Personal/Professional
Adjusting Insulin Doses
 Adjusting Insulin Doses Everyone with diabetes, including you, will need to adjust your insulin doses at some time. There are several reasons why a person may need an insulin adjustment. These reasons
Adjusting Insulin Doses Everyone with diabetes, including you, will need to adjust your insulin doses at some time. There are several reasons why a person may need an insulin adjustment. These reasons
Nph insulin conversion to lantus
 Nph insulin conversion to lantus Search 26-2-2003 RESPONSE FROM AVENTIS. We appreciate the opportunity to respond to Dr. Grajower s request for information regarding Lantus ( insulin glargine [rdna origin.
Nph insulin conversion to lantus Search 26-2-2003 RESPONSE FROM AVENTIS. We appreciate the opportunity to respond to Dr. Grajower s request for information regarding Lantus ( insulin glargine [rdna origin.
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE
 INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
Learning Objectives. Perioperative SWEET Success
 Perioperative SWEET Success PERIOPERATIVE SWEET SUCCESS PRESENTED BY: KENDRA MARTIN, RN, BSN, CDE JENNIFER SIMPSON, RN, BC-ADM, MSN, CNS Disclosure to Participants Notice of Requirements For Successful
Perioperative SWEET Success PERIOPERATIVE SWEET SUCCESS PRESENTED BY: KENDRA MARTIN, RN, BSN, CDE JENNIFER SIMPSON, RN, BC-ADM, MSN, CNS Disclosure to Participants Notice of Requirements For Successful
8/21/2017 UNRAVELING THE CROWED INSULIN SCENE. A Practical Overview of Insulin Focusing on New Insulin Preparations
 UNRAVELING THE CROWED INSULIN SCENE A Practical Overview of Insulin Focusing on New Insulin Preparations Patricia Garnica MS, ANP-BC, CDE, CDTC North Shore University Hospital, Manhasset, N.Y. October
UNRAVELING THE CROWED INSULIN SCENE A Practical Overview of Insulin Focusing on New Insulin Preparations Patricia Garnica MS, ANP-BC, CDE, CDTC North Shore University Hospital, Manhasset, N.Y. October
Converting lantus to humalog 75 25
 P ford residence southampton, ny Converting lantus to humalog 75 25 This page includes the following topics and synonyms: Insulin Dosing in Type 2 Diabetes, Insulin Dosing in Type II Diabetes. Thiazide
P ford residence southampton, ny Converting lantus to humalog 75 25 This page includes the following topics and synonyms: Insulin Dosing in Type 2 Diabetes, Insulin Dosing in Type II Diabetes. Thiazide
Insulin Basics. Bryan Primary Care Conference May 21, 2016 Shannon Wakeley MD Complete Endocrinology
 Insulin Basics Bryan Primary Care Conference May 21, 2016 Shannon Wakeley MD Complete Endocrinology Disclosures Speakers Bureau for Sanofi, Astra Zeneca, Janssen, Boehringer-Ingelheim Objectives Discuss
Insulin Basics Bryan Primary Care Conference May 21, 2016 Shannon Wakeley MD Complete Endocrinology Disclosures Speakers Bureau for Sanofi, Astra Zeneca, Janssen, Boehringer-Ingelheim Objectives Discuss
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
4/16/2018. Flexible Intensive Insulin Therapy (FIIT) in People with Type 2 Diabetes: A Viable Option. Disclosures. Outline. No financial disclosures
 in People with Type 2 Diabetes: A Viable Option. Disclosures. Outline. No financial disclosures") Flexible Intensive Insulin Therapy (FIIT) in People with Type Diabetes: A Viable Option Kim Bisanz, MFCS, RDN, LDN, CDE Minnesota Academy of Nutrition & Dietetics Annual Meeting April 19, 18 18 MFMER slide-1
Flexible Intensive Insulin Therapy (FIIT) in People with Type Diabetes: A Viable Option Kim Bisanz, MFCS, RDN, LDN, CDE Minnesota Academy of Nutrition & Dietetics Annual Meeting April 19, 18 18 MFMER slide-1
ClinicalTrials.gov Identifier: sanofi-aventis. Sponsor/company:
 These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: sanofi-aventis ClinicalTrials.gov
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: sanofi-aventis ClinicalTrials.gov
INSULIN OVERVIEW. Type Brand Name Onset Peak Duration Role in glucose management Page Rapid-Acting lispro min. 3-5 hrs min.
 INSULIN OVERVIEW Type Brand Name Onset Peak Duration Role in glucose management Page Rapid-Acting lispro Humalog 15-30 min 30-90 min 3-5 hrs aspart glulisine Short-Acting Regular insulin NovoLog Apidra
INSULIN OVERVIEW Type Brand Name Onset Peak Duration Role in glucose management Page Rapid-Acting lispro Humalog 15-30 min 30-90 min 3-5 hrs aspart glulisine Short-Acting Regular insulin NovoLog Apidra
INSULIN 101: When, How and What
 INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
In-Hospital Management of Diabetes. Dr Benjamin Schiff Assistant Professor McGill University
 In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
Mixed Insulins Pick Me
 Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
Newer Insulins. Boca Raton Regional Hospital 15th Annual Internal Medicine Conference
 Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Insulin analogues Das PP, Datta PG
 The ORION Medical Journal 2007 Sep;28:497-500 Insulin analogues Das PP, Datta PG Introduction Diabetes mellitus is a very big challenge for our medical science. To overcome this problem we need newer generation
The ORION Medical Journal 2007 Sep;28:497-500 Insulin analogues Das PP, Datta PG Introduction Diabetes mellitus is a very big challenge for our medical science. To overcome this problem we need newer generation
APPENDIX American Diabetes Association. Published online at
 APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
Diabetes in Pregnancy
 Diabetes in Pregnancy Ebony Boyce Carter, MD, MPH Division of Maternal Fetal Medicine Washington University School of Medicine Disclosures I have no financial disclosures to report. Objectives Review the
Diabetes in Pregnancy Ebony Boyce Carter, MD, MPH Division of Maternal Fetal Medicine Washington University School of Medicine Disclosures I have no financial disclosures to report. Objectives Review the
ANNUAL MEETING 2 #FSHP2017
 FSHP Disclosure Strategies for Glycemic Management in the Inpatient Setting: Guidelines vs. Reality Melissa Marshall, PharmD, BCPS Jeffrey Ruff, PharmD We do not have (nor does any immediate family member
FSHP Disclosure Strategies for Glycemic Management in the Inpatient Setting: Guidelines vs. Reality Melissa Marshall, PharmD, BCPS Jeffrey Ruff, PharmD We do not have (nor does any immediate family member
Management of Diabetes New Concepts New Devices New Medications. Richard J. Comi, MD Professor of Medicine Geisel School of Medicine at Dartmouth
 Management of Diabetes New Concepts New Devices New Medications Richard J. Comi, MD Professor of Medicine Geisel School of Medicine at Dartmouth Objectives: At the end of this lecture, the learner will
Management of Diabetes New Concepts New Devices New Medications Richard J. Comi, MD Professor of Medicine Geisel School of Medicine at Dartmouth Objectives: At the end of this lecture, the learner will
Basal Bolus Insulin Therapy Frequently Asked Questions
 1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
Diabetes: Definition Pathophysiology Treatment Goals. By Scott Magee, MD, FACE
 Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Objectives. Navigating New Insulins. Disclosures. Diabetes: The Stats. Normal Insulin Release Individuals without diabetes. History of Insulin 5/23/17
 Objectives Compare and contrast currently available products. Navigating New s Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Diabetes Center Determine the factors
Objectives Compare and contrast currently available products. Navigating New s Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Diabetes Center Determine the factors
Lantus to levemir conversion
 Lantus to levemir conversion The Borg System is 100 % Lantus to levemir conversion 16-6-2005 Ask the Expert on... Lantus Conversion. Karen Shapiro, PharmD, BCPS. Disclosures. June 16, 2005. Question. Would
Lantus to levemir conversion The Borg System is 100 % Lantus to levemir conversion 16-6-2005 Ask the Expert on... Lantus Conversion. Karen Shapiro, PharmD, BCPS. Disclosures. June 16, 2005. Question. Would
Inpatient Glycemic Management:
 Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Short-acting insulins. Biphasic insulins. Intermediate- and long-acting insulins
 Recommended Insulin Products This guideline states the Gloucestershire Joint Formulary recommended, first choice insulin products. The intention is to support the choice of treatment for new patients,
Recommended Insulin Products This guideline states the Gloucestershire Joint Formulary recommended, first choice insulin products. The intention is to support the choice of treatment for new patients,
Poll Question 2. Special Boot Camp Workshop Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services.
 Special Boot Camp Workshop Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Poll Question 1 Mary takes 6 units lispro (Humalog) before dinner. Which BG result reflects
Special Boot Camp Workshop Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Poll Question 1 Mary takes 6 units lispro (Humalog) before dinner. Which BG result reflects
Thursday School 2010 Management of Inpatient Diabetes and Hyperglycemia and Quality Improvement Efforts
 Thursday School 2010 Management of Inpatient Diabetes and Hyperglycemia and Quality Improvement Efforts Kendall Rogers, MD Using subcutaneous insulin to reliably achieve desired glycemic outcomes in non-critically
Thursday School 2010 Management of Inpatient Diabetes and Hyperglycemia and Quality Improvement Efforts Kendall Rogers, MD Using subcutaneous insulin to reliably achieve desired glycemic outcomes in non-critically
Pediatric Diabetes Update Fran R. Cogen, MD, CDE Professor of Pediatrics Director, Diabetes Services
 1.19.18 Pediatric Diabetes Update Fran R. Cogen, MD, CDE Professor of Pediatrics Director, Diabetes Services DISCLOSURES 1. No financial incentives 2. Volunteer Positions 1. National Certification Board
1.19.18 Pediatric Diabetes Update Fran R. Cogen, MD, CDE Professor of Pediatrics Director, Diabetes Services DISCLOSURES 1. No financial incentives 2. Volunteer Positions 1. National Certification Board
MANAGEMENT OF TYPE 1 DIABETES MELLITUS
 MANAGEMENT OF TYPE 1 DIABETES MELLITUS INVESTIGATIONS AND TREATMENT MANSI NAIK VII SEMESTER INVESTIGATIONS FASTING BLOOD SUGAR PLASMA GLUCOSE HEMOGLOBIN A 1c SYMPTOMS OF TYPE 1 DIABETES MELLITUS Polyuria
MANAGEMENT OF TYPE 1 DIABETES MELLITUS INVESTIGATIONS AND TREATMENT MANSI NAIK VII SEMESTER INVESTIGATIONS FASTING BLOOD SUGAR PLASMA GLUCOSE HEMOGLOBIN A 1c SYMPTOMS OF TYPE 1 DIABETES MELLITUS Polyuria
Diabetic Ketoacidosis
 October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
Lantus levemir conversion
 Lantus levemir conversion Search Learn about starting insulin-naïve patients with type 2 diabetes on Levemir. Read Important Safety & Prescribing Info on the HCP Website. Lantus and Levemir have a variety
Lantus levemir conversion Search Learn about starting insulin-naïve patients with type 2 diabetes on Levemir. Read Important Safety & Prescribing Info on the HCP Website. Lantus and Levemir have a variety
New Therapies for Diabetes Management: Hope or Headache?
 New Therapies for Diabetes Management: Hope or Headache? Elizabeth Stephens, MD, FACP PMG- Endocrinology Elizabeth.Stephens@providence.org November 2018 Disclosures None 1 Objectives Discussion of 3 rd
New Therapies for Diabetes Management: Hope or Headache? Elizabeth Stephens, MD, FACP PMG- Endocrinology Elizabeth.Stephens@providence.org November 2018 Disclosures None 1 Objectives Discussion of 3 rd
Exogenous Insulin in type 2 DM
 Exogenous Insulin in type 2 DM Russell Scott 2015 Part 1: Some basic biochemistry for Insulin absorption and action MY CHECK LIST Factors influencing insulin action: Forgets to inject Amount given Timing
Exogenous Insulin in type 2 DM Russell Scott 2015 Part 1: Some basic biochemistry for Insulin absorption and action MY CHECK LIST Factors influencing insulin action: Forgets to inject Amount given Timing
Background: Brief review of epidemiology, diagnosis, classification and pathophysiology of diabetes mellistus.
 Insulin Therapy in Diabetes Mellitus Part 1 Lekshmi T. Nair, MD, MHS Assistant Professor Department of Internal Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio State University Wexner
Insulin Therapy in Diabetes Mellitus Part 1 Lekshmi T. Nair, MD, MHS Assistant Professor Department of Internal Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio State University Wexner
Optimizing Care of the Inpatient with Hyperglycemia and Diabetes: Case Studies in Action
 Optimizing Care of the Inpatient with Hyperglycemia and Diabetes: Case Studies in Action Learning Objectives Identify patient situations where specific attention to glycemic control is warranted Determine
Optimizing Care of the Inpatient with Hyperglycemia and Diabetes: Case Studies in Action Learning Objectives Identify patient situations where specific attention to glycemic control is warranted Determine
Pharmacy Plan Guidance
 Pharmacy Plan Guidance The pharmacy plan is a tool used during the site readiness process to develop and document the site-specific procedures for study drug ordering, labeling and dispensing for the SHINE
Pharmacy Plan Guidance The pharmacy plan is a tool used during the site readiness process to develop and document the site-specific procedures for study drug ordering, labeling and dispensing for the SHINE
AACN PCCN Review. Endocrine
 AACN PCCN Review Endocrine Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com Endocrine I. INTRODUCTION Disorders
AACN PCCN Review Endocrine Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com Endocrine I. INTRODUCTION Disorders
Glycemic Control Insulin In The Hospital Setting
 Glycemic Control Insulin In The Hospital Setting Glycemic Control The Evidence For Insulin s s Benefit The Mechanism of Insulin s s Benefit The Achievement of Insulin s s Benefit A Few Cases Hyperglycemia
Glycemic Control Insulin In The Hospital Setting Glycemic Control The Evidence For Insulin s s Benefit The Mechanism of Insulin s s Benefit The Achievement of Insulin s s Benefit A Few Cases Hyperglycemia
Tips and Tricks for Starting and Adjusting Insulin. MC MacSween The Moncton Hospital
 Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Important Stuff. Basal Bolus What Adjustments? Pt weighs 80kg
 Diabetes Boot Camp Class 4 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Special Insulin and Pattern Management Diabetes Education Services 1998-2015. All rights
Diabetes Boot Camp Class 4 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Special Insulin and Pattern Management Diabetes Education Services 1998-2015. All rights
Type 1 Diabetes-Pathophysiology, Diagnosis, and Long-Term Complications. Alejandro J de la Torre Pediatric Endocrinology 10/17/2014
 Type 1 Diabetes-Pathophysiology, Diagnosis, and Long-Term Complications Alejandro J de la Torre Pediatric Endocrinology 10/17/2014 Objectives Understand the pathophysiology of Type 1 diabetes. Be familiar
Type 1 Diabetes-Pathophysiology, Diagnosis, and Long-Term Complications Alejandro J de la Torre Pediatric Endocrinology 10/17/2014 Objectives Understand the pathophysiology of Type 1 diabetes. Be familiar
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Initiation and Titration of Insulin in Diabetes Mellitus Type 2
 Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Diabetes: Inpatient Glucose control
 Diabetes: Inpatient Glucose control Leanne Current, PharmD, BCPS This activity is funded through the Medicaid section 1115(a) Demonstration Texas Healthcare Transformation and Quality Improvement Program
Diabetes: Inpatient Glucose control Leanne Current, PharmD, BCPS This activity is funded through the Medicaid section 1115(a) Demonstration Texas Healthcare Transformation and Quality Improvement Program
Objectives 2/13/2013. Figuring out the dose. Sub Optimal Glycemic Control: Moving to the Appropriate Treatment
 Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Glucose Management in Noncritical Hospitalized Patients
 Glucose Management in Noncritical Hospitalized Patients October 17, 2015 Archana R. Sadhu, MD., FACE Director of System Diabetes Program Director of Transplant Endocrinology Assistant Professor, Weill
Glucose Management in Noncritical Hospitalized Patients October 17, 2015 Archana R. Sadhu, MD., FACE Director of System Diabetes Program Director of Transplant Endocrinology Assistant Professor, Weill
These Aren t Your Average Rookies: A Primer on New and Emerging Insulins. Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP
 These Aren t Your Average Rookies: A Primer on New and Emerging Insulins Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP Disclosures Eli Lilly & Company: Advisory board member Boehringer Ingelheim: Advisory
These Aren t Your Average Rookies: A Primer on New and Emerging Insulins Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP Disclosures Eli Lilly & Company: Advisory board member Boehringer Ingelheim: Advisory
Glucose Management in the ICU: The Role of the Pharmacist
 Objectives Glucose Management in the ICU: The Role of the Pharmacist James Gilmore PharmD, BCPS Senior Pharmacist- Surgical Intensive Care Unit Brigham and Women s Hospital Boston, MA Evaluate primary
Objectives Glucose Management in the ICU: The Role of the Pharmacist James Gilmore PharmD, BCPS Senior Pharmacist- Surgical Intensive Care Unit Brigham and Women s Hospital Boston, MA Evaluate primary
Providing Stability to an Unstable Disease
 Basal Insulin Therapy Providing Stability to an Unstable Disease Thomas A. Hughes, M.D. Professor of Medicine - Retired Division of Endocrinology, Metabolism, and Diabetes University of Tennessee Health
Basal Insulin Therapy Providing Stability to an Unstable Disease Thomas A. Hughes, M.D. Professor of Medicine - Retired Division of Endocrinology, Metabolism, and Diabetes University of Tennessee Health
Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy
 Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy Jerry Meece, BPharm, CDE, FACA, FAADE Director of Clinical Services Plaza Pharmacy and Wellness Center Gainesville,
Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy Jerry Meece, BPharm, CDE, FACA, FAADE Director of Clinical Services Plaza Pharmacy and Wellness Center Gainesville,
Initiation and Adjustment of Insulin Regimens for Type 2 Diabetes
 Types of Insulin Rapid-acting insulin: lispro (Humalog), aspart (NovoRapid), glulisine (Apidra) Regular short-acting insulin: Humulin R, Novolin ge Toronto, Hypurin Regular Basal insulin: NPH (Humulin
Types of Insulin Rapid-acting insulin: lispro (Humalog), aspart (NovoRapid), glulisine (Apidra) Regular short-acting insulin: Humulin R, Novolin ge Toronto, Hypurin Regular Basal insulin: NPH (Humulin
Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes
 Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes Critically ill patients in the ICU Hospital Non-ICU Settings Home Guillermo E Umpierrez, MD, FACP, FACE Professor of Medicine
Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes Critically ill patients in the ICU Hospital Non-ICU Settings Home Guillermo E Umpierrez, MD, FACP, FACE Professor of Medicine
Basal-Bolus Insulin Therapy. Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January
 Basal-Bolus Insulin Therapy Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January 18 2018 Terminology No longer using the term diabetic. Diabetes does not define people. People with diabetes are individuals
Basal-Bolus Insulin Therapy Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January 18 2018 Terminology No longer using the term diabetic. Diabetes does not define people. People with diabetes are individuals
INSULIN THERAY دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد
 INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
Comparative Effectiveness, Safety, and Indications of Insulin Analogues in Premixed Formulations for Adults With Type 2 Diabetes Executive Summary
 Number 14 Effective Health Care Comparative Effectiveness, Safety, and Indications of Insulin Analogues in Premixed Formulations for Adults With Type 2 Diabetes Executive Summary Background and Key Questions
Number 14 Effective Health Care Comparative Effectiveness, Safety, and Indications of Insulin Analogues in Premixed Formulations for Adults With Type 2 Diabetes Executive Summary Background and Key Questions
January 7, 5:00 p.m. EST
 Study 3-151 Phase 2 Trial: Preliminary Results BIOD-531, a Concentrated Ultra-Rapid-Acting Prandial/Basal Insulin, Demonstrates Superior Post-Meal Glucose Control Compared to Marketed Prandial/Basal Insulins
Study 3-151 Phase 2 Trial: Preliminary Results BIOD-531, a Concentrated Ultra-Rapid-Acting Prandial/Basal Insulin, Demonstrates Superior Post-Meal Glucose Control Compared to Marketed Prandial/Basal Insulins
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Analogs & Premixed Insulin Analogs
 Rationale for the Development and Clinical Use of Insulin Analogs & Premixed Insulin Analogs A continuing education monograph for pharmacists, nurses, and dietitians this CE activity can also be completed
Rationale for the Development and Clinical Use of Insulin Analogs & Premixed Insulin Analogs A continuing education monograph for pharmacists, nurses, and dietitians this CE activity can also be completed
Update on Insulin-based Agents for T2D
 Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Insulin 10/11/17. Disclosures. Objectives. Speaker and Consultant for Jansen and Healthscripts Speaker and Consultant for Boehringer Ingelheim (BI)
") Insulin The What, When, Where, Who and Why Disclosures Speaker and Consultant for Jansen and Healthscripts Speaker and Consultant for Boehringer Ingelheim (BI) Objectives Define background and history
Insulin The What, When, Where, Who and Why Disclosures Speaker and Consultant for Jansen and Healthscripts Speaker and Consultant for Boehringer Ingelheim (BI) Objectives Define background and history
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Conversion from lantus to tresiba
 Conversion from lantus to tresiba Search dosages for Diabetes Type 2 and Diabetes Type 1; plus renal, liver and. Forecast your health care. Every time you have a symptom or are diagnosed of a condition,
Conversion from lantus to tresiba Search dosages for Diabetes Type 2 and Diabetes Type 1; plus renal, liver and. Forecast your health care. Every time you have a symptom or are diagnosed of a condition,
Module 5. Understanding Insulin Therapy
 Module 5. Understanding Insulin Therapy EDUCATIONAL OBJECTIVES Upon completion of this activity, participants will be better able to: 1. Define the basic physiologic concept of basal-bolus insulin; 2.
Module 5. Understanding Insulin Therapy EDUCATIONAL OBJECTIVES Upon completion of this activity, participants will be better able to: 1. Define the basic physiologic concept of basal-bolus insulin; 2.
Insulin Prior Authorization Criteria For Individuals who Purchased BlueCare / KS Solutions products
 Insulin Prior Authorization Criteria For Individuals who Purchased BlueCare / KS Solutions products FDA LABELED INDICATIONS 1-13,16-20 Rapid-Acting Indication Onset Peak Duration Insulins Fiasp (insulin
Insulin Prior Authorization Criteria For Individuals who Purchased BlueCare / KS Solutions products FDA LABELED INDICATIONS 1-13,16-20 Rapid-Acting Indication Onset Peak Duration Insulins Fiasp (insulin
Insulin Prior Authorization Criteria For Individuals Who Purchased BlueCare/KS Solutions/EPO Products
 Insulin Prior Authorization Criteria For Individuals Who Purchased BlueCare/KS Solutions/EPO Products FDA LABELED INDICATIONS 1-13,16-21 Rapid-Acting Indication Onset Peak Duration Insulins Admelog (insulin
Insulin Prior Authorization Criteria For Individuals Who Purchased BlueCare/KS Solutions/EPO Products FDA LABELED INDICATIONS 1-13,16-21 Rapid-Acting Indication Onset Peak Duration Insulins Admelog (insulin
第十五章. Diabetes Mellitus
 Diabetes-1/9 第十五章 Diabetes Mellitus 陳曉蓮醫師 2/9 - Diabetes 羅東博愛醫院 Management of Diabetes mellitus A. DEFINITION OF DIABETES MELLITUS Diabetes Mellitus is characterized by chronic hyperglycemia with disturbances
Diabetes-1/9 第十五章 Diabetes Mellitus 陳曉蓮醫師 2/9 - Diabetes 羅東博愛醫院 Management of Diabetes mellitus A. DEFINITION OF DIABETES MELLITUS Diabetes Mellitus is characterized by chronic hyperglycemia with disturbances
The ABCs of MDI: Gaining a working knowledge of Multiple Daily Injection insulin therapy. Today s Presenter
 FD Title Slide The ABCs of MDI: Gaining a working knowledge of Multiple Daily Injection insulin therapy learn.extension.org/events/3369 3 This material is based upon work supported by the National Institute
FD Title Slide The ABCs of MDI: Gaining a working knowledge of Multiple Daily Injection insulin therapy learn.extension.org/events/3369 3 This material is based upon work supported by the National Institute
Diabetic Emergencies DKA, HHS, Hypoglycemia. Disclosure. Learning Objectives
 Diabetic Emergencies DKA, HHS, Hypoglycemia October 2018 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Disclosure Michael McDermott has no conflict
Diabetic Emergencies DKA, HHS, Hypoglycemia October 2018 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Disclosure Michael McDermott has no conflict
Diabetes Head to Toe May 31, 2017
 Innovations in Insulin Joanne Reid RN CDE jmreid@gbhs.on.ca Danielle Benedict RPh Outline Setting the stage Insulin as pancreas replacement therapy Commonly used insulins New insulins Case Studies Dosing
Innovations in Insulin Joanne Reid RN CDE jmreid@gbhs.on.ca Danielle Benedict RPh Outline Setting the stage Insulin as pancreas replacement therapy Commonly used insulins New insulins Case Studies Dosing
4/10/2015. Foundations to Managing Inpatient Hyperglycemia. Learning Objectives
 Foundations to Managing Inpatient Hyperglycemia Module A 1 Learning Objectives Develop strategies to identify patients with hyperglycemia or diabetes in the inpatient setting Establish glycemic goals to
Foundations to Managing Inpatient Hyperglycemia Module A 1 Learning Objectives Develop strategies to identify patients with hyperglycemia or diabetes in the inpatient setting Establish glycemic goals to
9/16/2013. No Conflict of Interest to Disclose
 Catie Prinzing MSN, APRN, Clinical Nurse Specialist September 27, 2013 No Conflict of Interest to Disclose List key concepts to determining patient insulin doses during transitions in care Identify 5 points
Catie Prinzing MSN, APRN, Clinical Nurse Specialist September 27, 2013 No Conflict of Interest to Disclose List key concepts to determining patient insulin doses during transitions in care Identify 5 points
8/13/2016. Insulin Basics. Rapid-Acting Insulin Analogs. Current Insulin Products and Pens. Basal Insulin Analogs. History of Insulin Therapy
 Insulin Basics Anabolic hormone involved in metabolism Following carbohydrate ingestion insulin release is stimulated Suppresses hepatic glucose production Stimulates peripheral glucose uptake Commercially-available
Insulin Basics Anabolic hormone involved in metabolism Following carbohydrate ingestion insulin release is stimulated Suppresses hepatic glucose production Stimulates peripheral glucose uptake Commercially-available
Timely!Insulinization In!Type!2! Diabetes,!When!and!How
 Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Inpatient Management of Hyperglycemia Guillermo Umpierrez, MD, CDE Saturday, February 10, :30 a.m. 11:15 a.m.
 Inpatient Management of Hyperglycemia Guillermo Umpierrez, MD, CDE Saturday, February 1, 218 1:3 a.m. 11:15 a.m. There are over 7.5 million hospital admissions for patients with diabetes in the US. About
Inpatient Management of Hyperglycemia Guillermo Umpierrez, MD, CDE Saturday, February 1, 218 1:3 a.m. 11:15 a.m. There are over 7.5 million hospital admissions for patients with diabetes in the US. About
Degludec lantus conversion
 Degludec lantus conversion Search embarazadas con elevado riesgo de enfermedad tiroidea usando la. There are various possible causes of a high blood sugar level in the morning: The Dawn Phenomenon which
Degludec lantus conversion Search embarazadas con elevado riesgo de enfermedad tiroidea usando la. There are various possible causes of a high blood sugar level in the morning: The Dawn Phenomenon which
UKPDS: Over Time, Need for Exogenous Insulin Increases
 UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
Insulin Management. By Susan Henry Diabetes Specialist Nurse
 Insulin Management By Susan Henry Diabetes Specialist Nurse The Discovery of Insulin - 1921 - Banting & Best University Of Toronto Discovered hormone insulin in pancreatic extract of dog - Marjorie the
Insulin Management By Susan Henry Diabetes Specialist Nurse The Discovery of Insulin - 1921 - Banting & Best University Of Toronto Discovered hormone insulin in pancreatic extract of dog - Marjorie the
Inpatient Management of Hyperglycemia Guillermo Umpierrez, MD, CDE Saturday, February 10, :30 a.m. 11:15 a.m.
 Inpatient Management of Hyperglycemia Guillermo Umpierrez, MD, CDE Saturday, February 10, 2018 10:30 a.m. 11:15 a.m. There are over 7.5 million hospital admissions for patients with diabetes in the US.
Inpatient Management of Hyperglycemia Guillermo Umpierrez, MD, CDE Saturday, February 10, 2018 10:30 a.m. 11:15 a.m. There are over 7.5 million hospital admissions for patients with diabetes in the US.
Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς
 Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς Αναστασία Θανοπούλου Επίκουρη Καθηγήτρια Β Παθολογικής Κλινικής Πανεπιστημίου Αθηνών Διαβητολογικό Κέντρο, Ιπποκράτειο Νοσοκομείο
Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς Αναστασία Θανοπούλου Επίκουρη Καθηγήτρια Β Παθολογικής Κλινικής Πανεπιστημίου Αθηνών Διαβητολογικό Κέντρο, Ιπποκράτειο Νοσοκομείο
Martin J Stevens MD, FRCP, Endocrinologist and Professor of Medicine
 The Approach to Inpatient Hyperglycemia Martin J Stevens MD, FRCP, Endocrinologist and Professor of Medicine Great Lakes Hospital Medical Symposium May 7th 2010 Further Increases in the Prevalence of Diabetes
The Approach to Inpatient Hyperglycemia Martin J Stevens MD, FRCP, Endocrinologist and Professor of Medicine Great Lakes Hospital Medical Symposium May 7th 2010 Further Increases in the Prevalence of Diabetes
HYPERGLYCEMIA MANAGEMENT PROTOCOL A BASAL/BOLUS REGIMEN. Kacy Aderhold, MSN, APRN-CNS, CMSRN
 HYPERGLYCEMIA MANAGEMENT PROTOCOL A BASAL/BOLUS REGIMEN Kacy Aderhold, MSN, APRN-CNS, CMSRN Hyperglycemia Management Protocol Mimics the body s normal pancreas function, releasing a slow steady amount
HYPERGLYCEMIA MANAGEMENT PROTOCOL A BASAL/BOLUS REGIMEN Kacy Aderhold, MSN, APRN-CNS, CMSRN Hyperglycemia Management Protocol Mimics the body s normal pancreas function, releasing a slow steady amount
2018 Diabetes Summit Managing Diabetes: An Art and a Science
 2018 Diabetes Summit Managing Diabetes: An Art and a Science Natasha Petry, PharmD, BCACP NDSU College of Health Professions, School of Pharmacy, Department of Pharmacy Practice Patient-Centered Medical
2018 Diabetes Summit Managing Diabetes: An Art and a Science Natasha Petry, PharmD, BCACP NDSU College of Health Professions, School of Pharmacy, Department of Pharmacy Practice Patient-Centered Medical
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville
 Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
Insulin therapy in gestational diabetes mellitus
 Insulin therapy in gestational diabetes mellitus October 15, 2015 Kyung-Soo Kim Division of Endocrinology & Metabolism, Department of Internal Medicine, CHA Bundang Medical Center, CHA University Contents
Insulin therapy in gestational diabetes mellitus October 15, 2015 Kyung-Soo Kim Division of Endocrinology & Metabolism, Department of Internal Medicine, CHA Bundang Medical Center, CHA University Contents
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
INSULIN ALLERGY OBJECTIVES CASE OF DL
 INSULIN ALLERGY R E B E C C A C R E S P I R N M S N C P N P C D E C H I L D R E N S H O S P I T A L A T M O N T E F I O R E OBJECTIVES The learner will be able to define and identify the difference between
INSULIN ALLERGY R E B E C C A C R E S P I R N M S N C P N P C D E C H I L D R E N S H O S P I T A L A T M O N T E F I O R E OBJECTIVES The learner will be able to define and identify the difference between
DEMYSTIFYING INSULIN THERAPY
 DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
Diana McNeill MD, FACP Professor of Medicine Duke University Medical Center. Disclosures
 Insulin Therapy in Diabetes So Many Choices Diana McNeill MD, FACP Professor of Medicine Duke University Medical Center Disclosures Mytonomy-consultant Quantia webinars Acknowledgements: Dr. Sue Kirkman-UNC-
Insulin Therapy in Diabetes So Many Choices Diana McNeill MD, FACP Professor of Medicine Duke University Medical Center Disclosures Mytonomy-consultant Quantia webinars Acknowledgements: Dr. Sue Kirkman-UNC-
What the Pill Looks Like. How it Works. Slows carbohydrate absorption. Reduces amount of sugar made by the liver. Increases release of insulin
 Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
CANDY Camp Application
 CANDY Camp Application Please complete the following form and submit it by June 15, 2016. Please mail form to Bonnie Kruse, Diabetes Program Coordinator, HSHS St. Anthony s Memorial Hospital, 503 North
CANDY Camp Application Please complete the following form and submit it by June 15, 2016. Please mail form to Bonnie Kruse, Diabetes Program Coordinator, HSHS St. Anthony s Memorial Hospital, 503 North