Perinatal Depression. Lauren Sacco DNP, ARNP Seattle Children s
|
|
|
- Joanna Barker
- 5 years ago
- Views:
Transcription
1 Perinatal Depression Lauren Sacco DNP, ARNP Seattle Children s
2 Birth Asphyxia May occur in utero, during labor/delivery or during the neonatal period Condition of impaired blood gas exchange that leads to progressive hypoxemia and hypercapnia with metabolic acidosis. ACOG and AAP discourage the term asphyxia as imprecise, prefer the term depression Death or severe neurological impairment following perinatal asphyxia in 0.5-1/1000 live births
3 Birth Asphyxia The term birth asphyxia should be reserved for infants with four characteristics: Profound metabolic or mixed acidemia (ph<7.0) on umbilical arterial blood sample Persistence of an APGAR score of 0-3 for over 5 minutes Neurologic manifestations in the immediate neonatal period including seizures, hypotonia, coma or HIE Evidence of multi-organ system dysfunction in the immediate neonatal period
4 Risk Factors maternal Hypertensive disorders Cardiac disease Pulmonary disease Diabetes Sickle cell disease Renal disease Premature rupture of membranes Vaginal bleeding Severe anemia Rh/ABO sensitization Uterine or pelvic anatomic abnormalities Previous fetal or neonatal death
5 Risk Factors fetal Multiple birth Post-dates IUGR Premature Polyhydramnios Meconium stained amniotic fluid
6 Risk Factors Intrapartum Abnormal presentations Forceps (other than low) C-section delivery Prolapsed cord Abnormal heart rate or rhythm Prolonged general anesthesia Anesthetic complications (hypotension, hypoxia) Nuchal cord Prolonged or precipitous labor Uterine hypertonus Infection
7 Pathophysiology Definitions Hypoxemia: low blood oxygen levels Hypoxia: lack of oxygen in the tissues of the body Ischemia: reduction or loss of blood flow to an organ The fetus and neonate are more resistant to asphyxia than adults good at redistributing preferentially, oxygenated blood to the heart, brain and adrenals
8 Pathophysiologic sequence Can occur at any time, well defined series of events Onset of asphyxia results in period of rapid breathing followed by primary apnea Primary apnea is followed by irregular gasping and secondary apnea by 10 minutes Heart rate initially increases during the rapid breathing then falls along with the ph, BP and cerebral, pulmonary and renal perfusion.
9 Pathophysiologic sequence The infant s response to resuscitation will depend on duration of the asphyxia Will respond to stimulation if born during primary apnea Will need PPV if delivered during gasping or secondary apnea
10 Pathophysiologic sequence As hypercapnia, hypoxemia and acidosis worsen, cerebral blood flow (CBF) becomes pressure passive which leaves the infant at risk of cerebral ischemia w/ systemic hypotension and cerebral hemorrhage with systemic hypertension. Prolonged asphyxia results in decreased cardiac output, hypotension and decreased CBF, risking cerebral ischemia and cell injury. As less oxygen is available anerobic metabolism ensues.
11 Aerobic vs Anaerobic Metabolism
12 Systems Affected by Asphyxia Neurologic Hypoxic ischemic encephalopathy (HIE) Seizures Cerebral edema or hemorrhage Cardiovascular Poor contractility failure Pulmonary Delayed onset of respirations!shunting!pphn risk Risk of MAS
13 Systems Affected by Asphyxia Renal GI Acute Tubular Necrosis (ATN)!risk of failure Syndrome of Inappropriate Antidiuretic Hormone (SIADH) Risk of necrotizing enterocolitis (NEC) Hematologic Disseminated intravascular coagulation (DIC) Metabolic Hypoglycemia, hypocalcemia, altered electrolytes Hepatic Abnormal liver function tests (LFTs), clotting factors
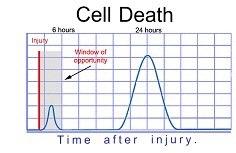
14 ! Hypoxic-Ischemic Encephalopathy caused by either placental, maternal, or fetal injury results in neonatal brain hypoxia neonatal brain responds by converting to anaerobic metabolism > depletion of adenosine triphosphate increased lactic acid production disturbance in normal metabolic activity this response disrupts intercellular pumps in the brain, causes a buildup of: sodium, calcium, and water > accumulation of fatty acids and oxygen-free radicals these events, together, cause cell apoptosis Preceding the initial injury to the neonatal brain, a second phase of injury will ensue if intervention is not initiated
15 ! Hypoxic-Ischemic Encephalopathy (HIE) The second phase of HIE is not well understood Includes accumulation of excitatory neurotransmitters and cell apoptosis Once the second phase begins, any brain injury that occurs in this phase is irreversible 15
16
17 Allen, K. A., & Brandon, D. H. (2011). Hypoxic Ischemic Encephalopathy: Pathophysiology and Experimental Treatments. Newborn and Infant Nursing Reviews : NAINR, 11(3),
18 Assessment for HIE No particular lab test to rule HIE in or out Clinical presentation is the best indicator Degree of other system involvement, electrolyte abnormalities are dependent on the severity of the insult EEG and MRI correlation have predictive value Sarnat and Sarnat s 3 Clinical Stages of Perinatal Hypoxic Ischemic Brain Injury (1976)
19 Sarnat Score! 19

20 EEG tracing ( ,en.png
21 Mild HIE Mildly increased muscle tone, brisk deep tendon reflexes during the first few days Transient behavioral abnormalities: poor feeding, irritability, irritated crying, sleepiness Normal CNS findings by 3-4 days of life
22 Moderate HIE Lethargic infant with significant hypotonia and decreased deep tendon reflexes Grasping, Moro and sucking reflexes sluggish or absent Occasional periods of apnea Seizures usually occur in the first 24hrs of life Full recovery in 1-2 weeks is possible and associated with a better long term outcome
23 Severe HIE Stupor or coma is typical Irregular breathing, generally requires vent support Hypotonia and depressed deep tendon reflexes Neonatal reflexes (sucking, Moro, etc) are absent Pupils can be dilated, fixed or poorly reactive to light Seizures occur early and often and may worsen over the initial hours of recovery secondary to reperfusion injury Fontanel may bulge with increasing cerebral edema HR and BP irregularities are common secondary to cardiorespiratory failure Multiple organ involvement common
24 HIE outcomes Dependent on severity Mild (Stage I) HIE generally normal neurological outcome Moderate (Stage II) HIE some with normal outcomes, resolution of neurological symptoms and normal nipple feeding by 1-2 wks is a good prognostic sign 30-50% with serious long term complications (CP, mental retardation) 10-20% with minor neurological morbidities
25 HIE Outcomes, cont Severe (Stage III) HIE Mortality rate of 50-75%, most during the first month 80% of the survivors develop serious complications: mental retardation, epilepsy, CP 10-20% with moderately serious disabilities Up to 10% are normal One study showed school age children with a history of moderate to severe HIE but neurologically normal, 15-20% had significant learning disabilities
26 Management First goal is always prevention identify infants at risk and be prepared Immediate resuscitation, NRP In the neonatal period: Maintenance of adequate ventilation hypercarbia can increase cerebral intracellular acidosis and impair cerebral vascular autoregulation Maintenance of adequate oxygenation PaO2>40 in preterm, >50 in term, avoid hyperoxia
27 Management, cont. In the neonatal period, cont. Cooling is the standard of care Maintenance of adequate perfusion maintain BP in the normal range for GA, volume and inotropes are often necessary, stable BP necessary with loss of cerebrovascular autoregulation Correct metabolic acidosis Maintain normal electrolytes and glucose often hyper then hypoglycemic, hyponatremia common
28 Management, cont. In the neonatal period, cont. Prevention of cerebral edema avoid fluid overload. Often have to restrict fluids to 60ml/kg/d, can decrease to 50ml/kg/d. Control of seizures Phenobarbital is the first choice: loading dose of 20mg/kg IV. If unresponsive, 5mg/kg doses up to 40mg/kg. If unable to control seizures with Phenobarbital start Ativan (lorazepam) 0.1mg/kg/dose repeat as necessary to control.
29 Seizures Can occur with HIE One of the most common signs of neurological dysfunction Can occur very early, even before the second phase postnatally Diagnosis can be challenging, as many as 80% of infants have clinical signs that are subtle or absent Must be distinguished from Jitteriness: usually normal eye movement, extremities are containable, fine movements Benign myoclonic activity: nonrepetitive, isolated jerky movements, generally occur during sleep Consider other causes: metabolic disturbances (hypoglycemia/ calcemia), inborn errors of metabolism, cerebral infarction, intracranial hemorrhage, infection (meningitis, TORCH, sepsis), neonatal drug withdrawal, developmental abnormalities
30 Seizures, cont. The earlier the onset the more ominous the prospects for recovery Important to recognize: Seizure activity can further damage the brain Suggestive of serious illness/injury which needs careful management Subtle seizure activity requires astute observation Obtain EEG as soon as practical Initiate aeeg immediately Seizures that occur as a result of HIE can be even more difficult to identify because many of these infants require intubation and paralytics > further mask clinical signs of seizure activity
31 Seizures-- Pathophysiology Neurons are depolarized by an inward migration of sodium They are repolarized by an efflux of potassium. Seizures occur due to excessive depolarization which results in excessive synchronous electrical discharge.
32 Seizures Pathophysiology, cont. Volpe (2001) proposed four possible reasons for the excessive depolarization Failure of the sodium-potassium pump secondary to a disturbance of energy production. Relative excess of excitatory vs inhibitory neurotransmitter. Relative lack of inhibitory vs excitatory neurotransmitter. Alteration in the neuronal membrane resulting in an inhibition of sodium movement

33 Seizure activity in 4 day old with HIE (ScienceDirect)
34 Seizures: Subtle & Clonic Subtle Apnea Staring, eyelid fluttering Sudden VS changes: BP fluctuations, tachycardia Cycling Most common type in preterm infants Clonic Multifocal: rhythmic, repetitive movement of one or two extremities that migrate to others in a non-orderly fashion Focal: rhythmic, repetitive movement of one extremity
35 Seizures: Tonic & Myoclonic Tonic Decerebrate or decorticate posturing Decerebrate: extremities are stiff and extended Decorticate: rigidly still with arms flexed, wrists clenched and legs extended Eye signs, occasional clonic movements Myoclonic Single or multiple jerky movements with flexion of upper or lower limbs Rare in neonates, but seen occasionally in metabolic problems

36
37 Management Assure adequate airway/ventilation Close CRM/oximetry monitoring Access for anticonvulsants Stat glucose, calcium, sodium and magnesium levels
38 Therapeutic Hypothermia! Research has shown that hypothermia can be neuroprotective May modify cells programmed for apoptosis, leading to their survival Reduced metabolic rate Decreased excitotoxicity Decreased edema Reduced alterations in ion flux 38
39 Therapeutic Hypothermia! Currently, two forms of cooling: selective head cooling total body cooling Protocols have been developed specific to each method and institution Infants who meet cooling criteria which is defined in each protocol cooled to C within 6 hours after birth maintained at that temperature for 72 hours followed by a slow rewarming process 39


40 Selective Head Cooling Study pictures from the Children s Hospital, Denver


41 Total Body Cooling
42 CoolCap Study Group 234 term infants with moderate to severe neonatal encephalopathy and abnormal EEG randomized to control or study group Head cooling was initiated within 6hrs and continued x 72hr when infant was gradually rewarmed Infants were cared for on a radiant warmer with temp adjusted to maintain rectal temp of degrees CoolCap water temp started at 8-12 degrees Outcomes no change in those with the most severe EEG changes, but beneficial to those less effected
43 Cochrane Review 2013 Systematic review of 11 randomized trials (n=1505) found that therapeutic hypothermia is beneficial in term and late preterm infants with HIE Found that cooling reduces mortality without increasing major disability in survivors and outweigh the short-term adverse effects Further trials should take place to determine the best techniques for cooling, patient selection, duration to help better understand this intervention
44 Seattle Children s Protocol Now encouraging cooling of eligible infants prior to and during transport Core/rectal temp goal 33.5C (check q15min) Passive cooling only Start prophylactic antibiotics Adequate sedation (avoid shivering) with morphine Phenobarbital for clinical seizures only Monitor electrolytes closely Avoid over ventilation and oxygenation
45 Seattle Children s cooling criteria Inclusion 36wk GA Perinatal depression based on one or more of the following: APGAR 5 at 10min need for resuscitation at 10 min cord ph <7 or arterial ph <7 within 1hr of birth Base deficit 12 in cord or blood gas within 1hr of birth Moderate to severe encephalopathy based on one of more of the following: Lethargy, stupor or coma, hypotonia Abnormal reflexes including oculomotor or pupillary abnormalities Absent or weak suck Clinical seizures or hyper-alert state
46 Seattle Children s cooling criteria, cont. Exclusion IUGR (BW < 1.8kg) Microcephaly (OFC <2SD for GA) Infant older than 6-12 hrs of age Infant likely to die or for whom withdrawal of care is being considered
47 Selected References Jacobs, S. E., Berg, M., Hunt, R., Tarnow-Mordi, W. O., Inder, T. E., & Davis, P. G. (January 01, 2013). Cooling for newborns with hypoxic ischaemic encephalopathy. The Cochrane Database of Systematic Reviews, 1.. Gluckman, et al Lancet 365: Gomella, T. Neonatology: management, procedures, on-call problems, diseases and drugs. McGraw-Hill Companies, Inc Fanaroff, A. & Martin, R. Neonatal-Perinatal Medicine: Diseases of the Fetus and Infant 7 th edition. Mosby, 2002.
Birth Asphyxia. Perinatal Depression. Birth Asphyxia. Risk Factors maternal. Risk Factors fetal. Risk Factors Intrapartum 2/12/2011
 Birth Asphyxia Perinatal Depression Sara Brown, ARNP Children s Hospital and Regional Medical Center May occur in utero, during labor/delivery or during the neonatal period Condition of impaired blood
Birth Asphyxia Perinatal Depression Sara Brown, ARNP Children s Hospital and Regional Medical Center May occur in utero, during labor/delivery or during the neonatal period Condition of impaired blood
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY
 ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY HYPOXIC-ISCHEMIC ENCEPHALOPATHY Hypoxic-İschemic Encephalopathy Encephalopathy due to hypoxic-ischemic injury [Hypoxic-ischemic encephalopathy
ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY HYPOXIC-ISCHEMIC ENCEPHALOPATHY Hypoxic-İschemic Encephalopathy Encephalopathy due to hypoxic-ischemic injury [Hypoxic-ischemic encephalopathy
Objectives. Birth Depression Management. Birth Depression Terms
 Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
Hypoxic-Ischemic Encephalopathy. TW de Witt University of Pretoria Department of Paediatrics Neonatology
 Hypoxic-Ischemic Encephalopathy TW de Witt University of Pretoria Department of Paediatrics Neonatology Background HIE remains a serious condition that causes significant mortality and longterm morbidity.
Hypoxic-Ischemic Encephalopathy TW de Witt University of Pretoria Department of Paediatrics Neonatology Background HIE remains a serious condition that causes significant mortality and longterm morbidity.
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara
 Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
NEONATAL SEIZURE. IAP UG Teaching slides
 NEONATAL SEIZURE 1 INTRODUCTION One of the important neonatal neurological emergencies requiring immediate medical care. Contribute to significant morbidity and mortality Incidence is around 0.5 to 0.8%
NEONATAL SEIZURE 1 INTRODUCTION One of the important neonatal neurological emergencies requiring immediate medical care. Contribute to significant morbidity and mortality Incidence is around 0.5 to 0.8%
Too Cool? Hypoxic Ischemic Encephalopathy and Therapeutic Hypothermia. Lauren Sacco DNP, ARNP, NNP-BC
 Too Cool? Hypoxic Ischemic Encephalopathy and Therapeutic Hypothermia Lauren Sacco DNP, ARNP, NNP-BC Pathophysiology of HIE Occurs in two energy failure phases: First phase happens during the initial insult
Too Cool? Hypoxic Ischemic Encephalopathy and Therapeutic Hypothermia Lauren Sacco DNP, ARNP, NNP-BC Pathophysiology of HIE Occurs in two energy failure phases: First phase happens during the initial insult
Neonatal Seizure. Dr.Nawar Yahya. Presented by: Sarah Khalil Zeina Shamil Zainab Waleed Zainab Qahtan. Supervised by:
 Neonatal Seizure Supervised by: Dr.Nawar Yahya Presented by: Sarah Khalil Zeina Shamil Zainab Waleed Zainab Qahtan Objectives: What is neonatal seizure Etiology Clinical presentation Differential diagnosis
Neonatal Seizure Supervised by: Dr.Nawar Yahya Presented by: Sarah Khalil Zeina Shamil Zainab Waleed Zainab Qahtan Objectives: What is neonatal seizure Etiology Clinical presentation Differential diagnosis
NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY
 & COOLING THERAPY") Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
TREATMENT OF HYPOXIC ISCHEMIC ENCEPHALOPATHY WITH COOLING Children s Hospital & Research Center Oakland Guideline Revised by P.
 TREATMENT OF HYPOXIC ISCHEMIC ENCEPHALOPATHY WITH COOLING Children s Hospital & Research Center Oakland Guideline Revised 05-13-13 by P. Joe SCREENING FOR POTENTIAL COOLING PATIENTS Patients who are >
TREATMENT OF HYPOXIC ISCHEMIC ENCEPHALOPATHY WITH COOLING Children s Hospital & Research Center Oakland Guideline Revised 05-13-13 by P. Joe SCREENING FOR POTENTIAL COOLING PATIENTS Patients who are >
Too or Too Cold. Too Cold...Too Hot...Just Right. Temperature Control in Newborns. Temperature Balance in Newborns. Basics in the Delivery Room
 Too or Too Cold Neonatology Rediscovers Temperature Control Advances and Controversies in Clinical Pediatrics May 31, 2007 Terri A. Slagle Neonatology, CPMC Too Cold...Too Hot...Just Right Too Cold = Issues
Too or Too Cold Neonatology Rediscovers Temperature Control Advances and Controversies in Clinical Pediatrics May 31, 2007 Terri A. Slagle Neonatology, CPMC Too Cold...Too Hot...Just Right Too Cold = Issues
These signs should lead to the administration of high concentrations of
 Hypoxic-ischemic encephalopathy (HIE); (cont.) Clinical manifestations; *Intrauterine; growth restriction and increased vascular resistances may be the st manifestation of fetal hypoxia. *During labor;
Hypoxic-ischemic encephalopathy (HIE); (cont.) Clinical manifestations; *Intrauterine; growth restriction and increased vascular resistances may be the st manifestation of fetal hypoxia. *During labor;
Running head: THERAPEUTIC HYPOTHERMIA AND TRANSPORT 1
 Running head: THERAPEUTIC HYPOTHERMIA AND TRANSPORT 1 Therapeutic Hypothermia for Neonatal Encephalopathy: Preparation for Transport to Cooling Center Teresa Z. Baker, DNP-S Annie L. Addison, FNP-S NURS
Running head: THERAPEUTIC HYPOTHERMIA AND TRANSPORT 1 Therapeutic Hypothermia for Neonatal Encephalopathy: Preparation for Transport to Cooling Center Teresa Z. Baker, DNP-S Annie L. Addison, FNP-S NURS
TLC March 27, Shawn Hollinger-Neonatal Fellow CHEO
 TLC March 27, 2013 Presented/Prepared by: Shawn Hollinger, PGY5 Neonatal-Perinatal Medicine Resident - University of Ottawa With slides/images from Dr. Brigitte Lemyre Associate Professor of Pediatrics
TLC March 27, 2013 Presented/Prepared by: Shawn Hollinger, PGY5 Neonatal-Perinatal Medicine Resident - University of Ottawa With slides/images from Dr. Brigitte Lemyre Associate Professor of Pediatrics
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Hypoxic Ischemic Encephalopathy. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Hypoxic Ischemic Encephalopathy. These podcasts are designed to give medical students an overview of key topics in pediatrics.
Case Presentations. Anamika B. Mukherjee, MD September 13, 2017
 Case Presentations Anamika B. Mukherjee, MD September 13, 2017 Nothing to disclose Disclosures Learning Objectives Use the CPQCC Toolkit for therapeutic hypothermia to apply the guidelines for screening
Case Presentations Anamika B. Mukherjee, MD September 13, 2017 Nothing to disclose Disclosures Learning Objectives Use the CPQCC Toolkit for therapeutic hypothermia to apply the guidelines for screening
Neonatal Therapeutic Hypothermia. A Wasunna Professor of Neonatal Medicine and Pediatrics School of Medicine, University of Nairobi
 Neonatal Therapeutic Hypothermia A Wasunna Professor of Neonatal Medicine and Pediatrics School of Medicine, University of Nairobi Definition of Perinatal Asphyxia *No agreed universal definition ACOG/AAP
Neonatal Therapeutic Hypothermia A Wasunna Professor of Neonatal Medicine and Pediatrics School of Medicine, University of Nairobi Definition of Perinatal Asphyxia *No agreed universal definition ACOG/AAP
Queen Charlotte Hospital
 Queen Charlotte Hospital Neuroprotection for neonatal encephalopathy Neonatal encephalopathy accounts for 1 million deaths worldwide and even greater numbers of disabled survivors In countries with
Queen Charlotte Hospital Neuroprotection for neonatal encephalopathy Neonatal encephalopathy accounts for 1 million deaths worldwide and even greater numbers of disabled survivors In countries with
State of Florida Hypothermia Protocol. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
PEDIATRIC BRAIN CARE
 PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
Birth Asphyxia - Summary of the previous meeting and protocol overview
 Birth Asphyxia - Summary of the previous meeting and protocol overview Dr Ornella Lincetto, WHO Geneve Milano, 11June 2007 Vilka är Personality egenskaper med den astrologiska Tvillingarna? Objective of
Birth Asphyxia - Summary of the previous meeting and protocol overview Dr Ornella Lincetto, WHO Geneve Milano, 11June 2007 Vilka är Personality egenskaper med den astrologiska Tvillingarna? Objective of
No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on Needed to be resuscitated at birth
 No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on 9-16-2011 Needed to be resuscitated at birth (included assisted vent) Had generalized edema and possible
No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on 9-16-2011 Needed to be resuscitated at birth (included assisted vent) Had generalized edema and possible
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO
 TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
NEONATAL SEIZURES-PGPYREXIA REVIEW
 NEONATAL SEIZURES-PGPYREXIA REVIEW This is a very important Postgraduate topics will few Q asked in undergraduation also. Lets see them in detail. References: 1.Volpe s Neurology of newborn 2.Nelson s
NEONATAL SEIZURES-PGPYREXIA REVIEW This is a very important Postgraduate topics will few Q asked in undergraduation also. Lets see them in detail. References: 1.Volpe s Neurology of newborn 2.Nelson s
COOLING FOR HYPOXIC ISCHEMIC ENCEPHALOPATHY
 COOLING FOR HYPOXIC ISCHEMIC ENCEPHALOPATHY Roger F. Soll H. Wallace Professor of Neonatology University of Vermont 19 th International Symposium on Neonatology Sao Paulo, Brazil DISCLOSURE Roger F. Soll
COOLING FOR HYPOXIC ISCHEMIC ENCEPHALOPATHY Roger F. Soll H. Wallace Professor of Neonatology University of Vermont 19 th International Symposium on Neonatology Sao Paulo, Brazil DISCLOSURE Roger F. Soll
The NeuroNICU From Concept to Clinical Service. MJ Harbert, MD Co-Director, NeuroNICU Service Rady Children s Hospital San Diego
 The NeuroNICU From Concept to Clinical Service MJ Harbert, MD Co-Director, NeuroNICU Service Rady Children s Hospital San Diego What is a NeuroNICU? Collaboration between Neonatology and Neurology Neonatal
The NeuroNICU From Concept to Clinical Service MJ Harbert, MD Co-Director, NeuroNICU Service Rady Children s Hospital San Diego What is a NeuroNICU? Collaboration between Neonatology and Neurology Neonatal
Wales Neonatal Network Guideline Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling.
 Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
Inclusion criteria for cooling: Babies should be assessed for 3 criteria: A, B and C. See Appendix 1 for a decision making flowchart.
 Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
This lecture will provide an overview of the neurologic exam of a neonate in the context of clinical cases.
 A11a Neuro Nuggets from the Trenches Michael D. Weiss, MD Associate Professor Department of Pediatrics, Division of Neonatology University of Florida, Gainesville, FL The speaker has signed a disclosure
A11a Neuro Nuggets from the Trenches Michael D. Weiss, MD Associate Professor Department of Pediatrics, Division of Neonatology University of Florida, Gainesville, FL The speaker has signed a disclosure
State of Florida Systemic Supportive Care Guidelines. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
Disclosures. Objectives. Definition: HIE. HIE: Incidence. Impact 9/10/2018. Hypoxic Ischemic Encephalopathy in the Neonate
 Disclosures Hypoxic Ischemic Encephalopathy in the Neonate No relevant financial relationships or conflicts of interest to disclose Franscesca Miquel-Verges MD 2018 Review therapies currently under research
Disclosures Hypoxic Ischemic Encephalopathy in the Neonate No relevant financial relationships or conflicts of interest to disclose Franscesca Miquel-Verges MD 2018 Review therapies currently under research
The high risk neonate
 The high risk neonate Infant classification by gestational (postmenstrual) age Preterm. Less than 37 completed weeks (259 days). Term. Thirty-seven to 416/7 weeks (260-294 days). Post-term. Forty-two weeks
The high risk neonate Infant classification by gestational (postmenstrual) age Preterm. Less than 37 completed weeks (259 days). Term. Thirty-seven to 416/7 weeks (260-294 days). Post-term. Forty-two weeks
Total Body Cooling & Hypoxic Ischemic Encephalopathy in the Neonate Kaleidoscope 2017
 Total Body Cooling & Hypoxic Ischemic Encephalopathy in the Neonate Kaleidoscope 2017 LEIGH ANN CATES PHD, APRN, NNP -BC, RRT-NPS, CHSE N E O N ATA L N U R S E P R A C T I T I O N E R - T E X A S C H I
Total Body Cooling & Hypoxic Ischemic Encephalopathy in the Neonate Kaleidoscope 2017 LEIGH ANN CATES PHD, APRN, NNP -BC, RRT-NPS, CHSE N E O N ATA L N U R S E P R A C T I T I O N E R - T E X A S C H I
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
Perinatal asphyxia: Pathophysiology and therapy
 Perinatal asphyxia: Pathophysiology and therapy Peter Davis Melbourne Australia With thanks to Dr Sue Jacobs Moderate or severe HIE Complicates ~1/1000 term live births: Mortality: >25% Major neurological
Perinatal asphyxia: Pathophysiology and therapy Peter Davis Melbourne Australia With thanks to Dr Sue Jacobs Moderate or severe HIE Complicates ~1/1000 term live births: Mortality: >25% Major neurological
Therapeutic Hypothermia for infants > 35 wks with moderate or severe Hypoxic Ischaemic Encephalopathy (HIE) Clinical Guideline Reference Number:
 Clinical Guideline Reference Number:") This is an official Northern Trust policy and should not be edited in any way Therapeutic Hypothermia for infants > 35 wks with moderate or severe Hypoxic Ischaemic Encephalopathy (HIE) Clinical Guideline
This is an official Northern Trust policy and should not be edited in any way Therapeutic Hypothermia for infants > 35 wks with moderate or severe Hypoxic Ischaemic Encephalopathy (HIE) Clinical Guideline
FHR Monitoring: Maternal Fetal Physiology
 FHR Monitoring: Maternal Fetal Physiology M. Sean Esplin, MD and Alexandra Eller, MD Maternal Fetal Medicine Intermountain Healthcare University of Utah Health Sciences Center Disclosures I have no financial
FHR Monitoring: Maternal Fetal Physiology M. Sean Esplin, MD and Alexandra Eller, MD Maternal Fetal Medicine Intermountain Healthcare University of Utah Health Sciences Center Disclosures I have no financial
Neonatal/Pediatric Cardiopulmonary Care
 Neonatal/Pediatric Cardiopulmonary Care Resuscitation 2 When To Resuscitate Need usually related Combination of Can occur in 3 Causes of Fetal Asphyxia 1 4 Apnea Hypoxia Stimulates chemoreceptors & baroreceptors
Neonatal/Pediatric Cardiopulmonary Care Resuscitation 2 When To Resuscitate Need usually related Combination of Can occur in 3 Causes of Fetal Asphyxia 1 4 Apnea Hypoxia Stimulates chemoreceptors & baroreceptors
Neonatal infections and neonatal seizures. Mohamed Waheed Elsharief Dept. of paediatrics Faculty of medicine Jazan University KSA
 Neonatal infections and neonatal seizures Mohamed Waheed Elsharief Dept. of paediatrics Faculty of medicine Jazan University KSA objectives By the end of this lecture the student should Define neonatal
Neonatal infections and neonatal seizures Mohamed Waheed Elsharief Dept. of paediatrics Faculty of medicine Jazan University KSA objectives By the end of this lecture the student should Define neonatal
8/20/12. Discuss the importance of thermoregulation in the neonate.
 Sharon Rush MSN NNP-BC Discuss the importance of thermoregulation in the neonate. To maintain correct body temperature range in order to: Reduce oxygen consumption Reduce calorie expenditure Maximize metabolic
Sharon Rush MSN NNP-BC Discuss the importance of thermoregulation in the neonate. To maintain correct body temperature range in order to: Reduce oxygen consumption Reduce calorie expenditure Maximize metabolic
Neurological and Neuromuscular Disorders. Elizabeth Papp, RN, MSN, CNS
 Neurological and Neuromuscular Disorders Elizabeth Papp, RN, MSN, CNS June, 2018 Neuromuscular Birth Injuries: Overview Nerve damage caused by trauma during delivery Prolonged labor LGA CPD Abnormal presentation
Neurological and Neuromuscular Disorders Elizabeth Papp, RN, MSN, CNS June, 2018 Neuromuscular Birth Injuries: Overview Nerve damage caused by trauma during delivery Prolonged labor LGA CPD Abnormal presentation
GUIDELINE PHYSIOLOGY OF BIRTH ASPHYXIA
 GUIDELINE PHYSIOLOGY OF BIRTH ASPHYXIA The newborn is not an adult, nor a child. In people of all ages, death can occur from a failure of breathing and / or circulation. The interventions required to aid
GUIDELINE PHYSIOLOGY OF BIRTH ASPHYXIA The newborn is not an adult, nor a child. In people of all ages, death can occur from a failure of breathing and / or circulation. The interventions required to aid
Admission/Discharge Form for Infants Born in Please DO NOT mail or fax this form to the CPQCC Data Center. This form is for internal use ONLY.
 Selection Criteria Admission/Discharge Form for Infants Born in 2016 To be eligible, you MUST answer YES to at least one of the possible criteria (A-C) A. 401 1500 grams o Yes B. GA range 22 0/7 31 6/7
Selection Criteria Admission/Discharge Form for Infants Born in 2016 To be eligible, you MUST answer YES to at least one of the possible criteria (A-C) A. 401 1500 grams o Yes B. GA range 22 0/7 31 6/7
COOLING FOR NEONATAL HYPOXIC ISCHAEMIC ENCEPHALOPATHY (HIE) - GUIDELINE
 - GUIDELINE") Background Objective Equipment Indications Contraindications When to initiate cooling in NPICU Procedure for therapeutic cooling NETS Transfer Issues Follow-up References Acknowledgements Related Documents
Background Objective Equipment Indications Contraindications When to initiate cooling in NPICU Procedure for therapeutic cooling NETS Transfer Issues Follow-up References Acknowledgements Related Documents
NEONATAL SEIZURES. Introduction
 Introduction NEONATAL SEIZURES Definition: Sudden, paroxysmal depolarisation of a group of neurones with transient alteration in neurological state. Possibly abnormal motor, sensory or autonomic activity
Introduction NEONATAL SEIZURES Definition: Sudden, paroxysmal depolarisation of a group of neurones with transient alteration in neurological state. Possibly abnormal motor, sensory or autonomic activity
D is for Disability Altered Mental Status in Children
 D is for Disability Altered Mental Status in Children Joshua Ross, MD, FAAP Pediatric Emergency Medicine Emergency Care and Trauma Symposium June 22, 2015 Objectives Describe a basic approach to evaluating
D is for Disability Altered Mental Status in Children Joshua Ross, MD, FAAP Pediatric Emergency Medicine Emergency Care and Trauma Symposium June 22, 2015 Objectives Describe a basic approach to evaluating
Brain injury and Resuscitation! Turning Back the Clock!
 Brain injury and Resuscitation! Turning Back the Clock! Dec 2008 Patrick J McNamara Learning Objectives Understand the benefits of Hypothermia and how it works? Identify patients who may benefit from treatment.
Brain injury and Resuscitation! Turning Back the Clock! Dec 2008 Patrick J McNamara Learning Objectives Understand the benefits of Hypothermia and how it works? Identify patients who may benefit from treatment.
The Pharmacokinetics of Antiepileptics Drugs in Neonates with Hypoxic Ischemic Encephalopathy
 The Pharmacokinetics of Antiepileptics Drugs in Neonates with Hypoxic Ischemic Encephalopathy KELIANA O MARA, PHARMD FLORIDA NEONATAL NEUROLOGIC NETWORK STATE MEETING Objectives Describe seizures in hypoxic
The Pharmacokinetics of Antiepileptics Drugs in Neonates with Hypoxic Ischemic Encephalopathy KELIANA O MARA, PHARMD FLORIDA NEONATAL NEUROLOGIC NETWORK STATE MEETING Objectives Describe seizures in hypoxic
Hyaline membrane disease. By : Dr. Ch Sarishma Peadiatric Pg
 Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Fetal Heart Rate Monitoring Myths and Misperceptions s: Electronic Fetal Heart Rate Monitoring (EFM): Baseline Assumptions.
: Baseline Assumptions.") Can FHR Monitoring Prevent Hypoxic-Ischemic Encephalopathy in the Newborn? Fetal Heart Rate Monitoring Myths and Misperceptions 1. Yes 2. No 72% Tekoa L. King CNM, MPH June 6, 2008 28% Yes No Objectives
Can FHR Monitoring Prevent Hypoxic-Ischemic Encephalopathy in the Newborn? Fetal Heart Rate Monitoring Myths and Misperceptions 1. Yes 2. No 72% Tekoa L. King CNM, MPH June 6, 2008 28% Yes No Objectives
Stabilization of the Newborn for Transport. Relevant Disclosure. Learning Objectives
 Stabilization of the Newborn for Transport Arlen Foulks, DO FAAP FACOP Medical Director, CCMH Level II NICU Medical Director, NeoFlight Assistant Professor of Pediatrics Neonatal Perinatal Medicine Section,
Stabilization of the Newborn for Transport Arlen Foulks, DO FAAP FACOP Medical Director, CCMH Level II NICU Medical Director, NeoFlight Assistant Professor of Pediatrics Neonatal Perinatal Medicine Section,
Neuro. Development. Judy Philbrook, NNP-BC. ! Primary neurulation! Prosencepahlic! Neuronal proliferation. ! 3-4 weeks! 2-3 months!
 Neuro Judy Philbrook, NNP-BC Microsoft clip art Development! Primary neurulation! Prosencepahlic! Neuronal proliferation! Neuronal migration! Organization! Myelination! 3-4 weeks! 2-3 months! 3-4 months!
Neuro Judy Philbrook, NNP-BC Microsoft clip art Development! Primary neurulation! Prosencepahlic! Neuronal proliferation! Neuronal migration! Organization! Myelination! 3-4 weeks! 2-3 months! 3-4 months!
Neonatal Resuscitation. Dustin Coyle, M.D. Anesthesiology
 Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
Current Management of the Infant Who Presents with Neonatal Encephalopathy
 Current Management of the Infant Who Presents with Neonatal Encephalopathy Elena V. Wachtel, MD, MPH, FAAP, and Karen D. Hendricks-Muñoz, MD, MPH, FAAP Neonatal encephalopathy after perinatal hypoxic-ischemic
Current Management of the Infant Who Presents with Neonatal Encephalopathy Elena V. Wachtel, MD, MPH, FAAP, and Karen D. Hendricks-Muñoz, MD, MPH, FAAP Neonatal encephalopathy after perinatal hypoxic-ischemic
ACoRN Workbook 2012 Update
 ACoRN Neonatal Society Société néonatale ACoRN www.acornprogram.net A Canadian non-profit Society Vancouver, British Columbia ACoRN Workbook 2012 Update Name: The ACoRN Process The Resuscitation Sequence
ACoRN Neonatal Society Société néonatale ACoRN www.acornprogram.net A Canadian non-profit Society Vancouver, British Columbia ACoRN Workbook 2012 Update Name: The ACoRN Process The Resuscitation Sequence
NEONATOLOGY Healthy newborn. Neonatal sequelaes
 NEONATOLOGY Healthy newborn. Neonatal sequelaes Ágnes Harmath M.D. Ph.D. senior lecturer 11. November 2016. Tasks of the neonatologist Prenatal diagnosed condition Inform parents, preparation of necessary
NEONATOLOGY Healthy newborn. Neonatal sequelaes Ágnes Harmath M.D. Ph.D. senior lecturer 11. November 2016. Tasks of the neonatologist Prenatal diagnosed condition Inform parents, preparation of necessary
Ashley Robson Canyon Creek Dr. Mckinney, TX 75070
 1 Ashley Robson 2212 Canyon Creek Dr. Mckinney, TX 75070 September 2 nd 2014 Debra Brandon PhD, RN, CCNS, FAAN Duke University School of Nursing Durham, NC Dear Mrs. Brandon- I would like the opportunity
1 Ashley Robson 2212 Canyon Creek Dr. Mckinney, TX 75070 September 2 nd 2014 Debra Brandon PhD, RN, CCNS, FAAN Duke University School of Nursing Durham, NC Dear Mrs. Brandon- I would like the opportunity
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
HYPOXIC ISCHEMIC ENCEPHALOPATHY AND THE OBSTETRICIAN
 HYPOXIC ISCHEMIC ENCEPHALOPATHY AND THE OBSTETRICIAN DISCLOSURE I have nothing to disclose and have no real or potential conflicts with this presentation and its content. Michael P. Nageotte, M.D. CASE:
HYPOXIC ISCHEMIC ENCEPHALOPATHY AND THE OBSTETRICIAN DISCLOSURE I have nothing to disclose and have no real or potential conflicts with this presentation and its content. Michael P. Nageotte, M.D. CASE:
Evidence-Based Update: Using Glucose Gel to Treat Neonatal Hypoglycemia
 Neonatal Nursing Education Brief: Evidence-Based Update: Using Glucose Gel to Treat Neonatal Hypoglycemia http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/
Neonatal Nursing Education Brief: Evidence-Based Update: Using Glucose Gel to Treat Neonatal Hypoglycemia http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/
Hypotension in the Neonate
 Neonatal Nursing Education Brief: Hypotension in the Neonate http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/ Neonatal
Neonatal Nursing Education Brief: Hypotension in the Neonate http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/ Neonatal
Neonatal Hypoglycemia. Presented By : Kamlah Olaimat 25\7\2010
 Neonatal Hypoglycemia Presented By : Kamlah Olaimat 25\7\2010 Definition The S.T.A.B.L.E. Program defines hypoglycemia as: Glucose delivery or availability is inadequate to meet glucose demand (Karlsen,
Neonatal Hypoglycemia Presented By : Kamlah Olaimat 25\7\2010 Definition The S.T.A.B.L.E. Program defines hypoglycemia as: Glucose delivery or availability is inadequate to meet glucose demand (Karlsen,
Resuscitating neonatal and infant organs and preserving function. GI Tract and Kidneys
 Resuscitating neonatal and infant organs and preserving function GI Tract and Kidneys Australian and New Zealand Resuscitation Council Joint Guidelines Outline Emphasis on the infant - PICU Kidney Gastrointestinal
Resuscitating neonatal and infant organs and preserving function GI Tract and Kidneys Australian and New Zealand Resuscitation Council Joint Guidelines Outline Emphasis on the infant - PICU Kidney Gastrointestinal
Pathophysiology Review. Hypoxic-Ischemic Encephalopathy & Therapeutic Hypothermia. Objectives. What is Hypoxic-Ischemic Encephalopathy?
 Hypoxic-Ischemic Encephalopathy & Therapeutic Hypothermia Nancy Couto Nurse Practitioner, NICU London Health Sciences Centre, Children s Hospital nancy.couto@lhsc.on.ca 2014 12 17 Objectives Review Pathophysiology
Hypoxic-Ischemic Encephalopathy & Therapeutic Hypothermia Nancy Couto Nurse Practitioner, NICU London Health Sciences Centre, Children s Hospital nancy.couto@lhsc.on.ca 2014 12 17 Objectives Review Pathophysiology
Status Epilepticus in Children
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Status Epilepticus in Children. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Status Epilepticus in Children. These podcasts are designed to give medical students an overview of key topics in pediatrics.
Hypoglycemia. Objectives. Glucose Metabolism
 Hypoglycemia Instructor: Janet Mendis, MSN, RNC-NIC, CNS Outline: Janet Mendis, MSN, RNC-NIC, CNS Summer Morgan, MSN, RNC-NIC, CPNP UC San Diego Health System Objectives State the blood glucose level at
Hypoglycemia Instructor: Janet Mendis, MSN, RNC-NIC, CNS Outline: Janet Mendis, MSN, RNC-NIC, CNS Summer Morgan, MSN, RNC-NIC, CPNP UC San Diego Health System Objectives State the blood glucose level at
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Difficulties at Birth: Long Term Developmental Outcomes
 Difficulties at Birth: Long Term Developmental Outcomes Alan D. Bedrick MD Division of Neonatology and Developmental Biology Department of Pediatrics University of Arizona Tucson, Arizona DISCLOSURE I
Difficulties at Birth: Long Term Developmental Outcomes Alan D. Bedrick MD Division of Neonatology and Developmental Biology Department of Pediatrics University of Arizona Tucson, Arizona DISCLOSURE I
Neonatal Hypoxic-Ischemic Injury: Ultrasound and Dynamic Color Doppler Sonography perfusion of the Brain and Abdomen with pathologic correlation.
 Neonatal Hypoxic-Ischemic Injury: Ultrasound and Dynamic Color Doppler Sonography perfusion of the Brain and Abdomen with pathologic correlation. Ricardo Faingold,MD Montreal Children s Hospital Medical
Neonatal Hypoxic-Ischemic Injury: Ultrasound and Dynamic Color Doppler Sonography perfusion of the Brain and Abdomen with pathologic correlation. Ricardo Faingold,MD Montreal Children s Hospital Medical
ADMISSION/DISCHARGE FORM FOR INFANTS BORN IN 2019 DO NOT mail or fax this form to the CPQCC Data Center. This form is for internal use ONLY.
 1 Any eligible inborn infant who dies in the delivery room or at any other location in your hospital within 12 hours after birth and prior to admission to the NICU is defined as a "Delivery Room Death."
1 Any eligible inborn infant who dies in the delivery room or at any other location in your hospital within 12 hours after birth and prior to admission to the NICU is defined as a "Delivery Room Death."
Study of role of MRI brain in evaluation of hypoxic ischemic encephalopathy
 Original article: Study of role of MRI brain in evaluation of hypoxic ischemic encephalopathy *Dr Harshad Bhagat, ** Dr Ravindra Kawade, ***Dr Y.P.Sachdev *Junior Resident, Department Of Radiodiagnosis,
Original article: Study of role of MRI brain in evaluation of hypoxic ischemic encephalopathy *Dr Harshad Bhagat, ** Dr Ravindra Kawade, ***Dr Y.P.Sachdev *Junior Resident, Department Of Radiodiagnosis,
Severity of Hypoxic Ischaemic Encephalopathy in Neonates with Birth Asphyxia
 Journal of Rawalpindi Medical College (JRMC); 2007; (): 8-22 Severity of Hypoxic Ischaemic Encephalopathy in Neonates with Birth Asphyxia Rubina Zulfiqar, Samiya Naeemullah Department of Paediatrics, Holy
Journal of Rawalpindi Medical College (JRMC); 2007; (): 8-22 Severity of Hypoxic Ischaemic Encephalopathy in Neonates with Birth Asphyxia Rubina Zulfiqar, Samiya Naeemullah Department of Paediatrics, Holy
Neurological outcome after perinatal asphyxia at term
 Section 1 Chapter 1 Scientific background Neurological outcome after perinatal asphyxia at term David Odd and Andrew Whitelaw Introduction It was nearly 150 years ago that an association between perinatal
Section 1 Chapter 1 Scientific background Neurological outcome after perinatal asphyxia at term David Odd and Andrew Whitelaw Introduction It was nearly 150 years ago that an association between perinatal
Objectives. Apnea Definition and Pitfalls. Pathophysiology of Apnea. Apnea of Prematurity and hypoxemia episodes 5/18/2015
 Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification
 Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) Diagnose and Procedures Codes 1. ICD-9-CM definition of
Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) Diagnose and Procedures Codes 1. ICD-9-CM definition of
Maternal and Fetal Physiology
 Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
What is symptomatic? Neonatal hypoglycemia: how low can you go? Hypoglycemia and MRI. Conflicts. What s the problem? Hypoglycemia and MRI
 Neonatal hypoglycemia: how low can you go? Kristi Watterberg, MD Professor of Pediatrics, UNM What is symptomatic? Jitteriness Cyanosis Poor feeding Weak, high-pitched cry Seizures Apnea Lethargy, low
Neonatal hypoglycemia: how low can you go? Kristi Watterberg, MD Professor of Pediatrics, UNM What is symptomatic? Jitteriness Cyanosis Poor feeding Weak, high-pitched cry Seizures Apnea Lethargy, low
Epilepsy CASE 1 Localization Differential Diagnosis
 2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 6.1 Define key terms introduced in this chapter. Slides 11, 15, 17, 26, 27, 31, 33, 37, 40 42, 44, 45, 51, 58 6.2 Describe the basic roles and structures
Introduction to Emergency Medical Care 1 OBJECTIVES 6.1 Define key terms introduced in this chapter. Slides 11, 15, 17, 26, 27, 31, 33, 37, 40 42, 44, 45, 51, 58 6.2 Describe the basic roles and structures
Therapeutic hypothermia for hypoxic ischemic encephalopathy using low-technology methods: A systematic review and meta-analysis
 Therapeutic hypothermia for hypoxic ischemic encephalopathy using low-technology methods: A systematic review and meta-analysis Rossouw G 1, Irlam J 2, Horn AR 1 1)Division of Neonatal Medicine, Department
Therapeutic hypothermia for hypoxic ischemic encephalopathy using low-technology methods: A systematic review and meta-analysis Rossouw G 1, Irlam J 2, Horn AR 1 1)Division of Neonatal Medicine, Department
Study of renal functions in neonatal asphyxia
 Original article: Study of renal functions in neonatal asphyxia *Dr. D.Y.Shrikhande, **Dr. Vivek Singh, **Dr. Amit Garg *Professor and Head, **Senior Resident Department of Pediatrics, Pravara Institute
Original article: Study of renal functions in neonatal asphyxia *Dr. D.Y.Shrikhande, **Dr. Vivek Singh, **Dr. Amit Garg *Professor and Head, **Senior Resident Department of Pediatrics, Pravara Institute
Figure removed due to copyright restrictions.
 Harvard-MIT Division of Health Sciences and Technology HST.071: Human Reproductive Biology Course Director: Professor Henry Klapholz IN SUMMARY HST 071 An Example of a Fetal Heart Rate Tracing Figure removed
Harvard-MIT Division of Health Sciences and Technology HST.071: Human Reproductive Biology Course Director: Professor Henry Klapholz IN SUMMARY HST 071 An Example of a Fetal Heart Rate Tracing Figure removed
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials
 Certification Preparatory Materials") Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Swiss neonatal network and Follow up Group
 Swiss neonatal network and Follow up Group March 2011 Barbara Brotschi and Cornelia Hagmann Hypoxic ischaemic encephalopathy Neonatal encephalopathy due to perinatal hypoxiaischaemia: clinically defined
Swiss neonatal network and Follow up Group March 2011 Barbara Brotschi and Cornelia Hagmann Hypoxic ischaemic encephalopathy Neonatal encephalopathy due to perinatal hypoxiaischaemia: clinically defined
Neurological and Neuromuscular Disorders. Elizabeth Papp, RN, MSN, CNS
 Neurological and Neuromuscular Disorders Elizabeth Papp, RN, MSN, CNS June, 2018 Neuromuscular Birth Injuries: Overview Nerve damage caused by trauma during delivery Abnormal labor time (long or short)
Neurological and Neuromuscular Disorders Elizabeth Papp, RN, MSN, CNS June, 2018 Neuromuscular Birth Injuries: Overview Nerve damage caused by trauma during delivery Abnormal labor time (long or short)
IJMB ABSTRACT INTRODUCTION /jp-journals
 Bhawna Bhimte, Amrita Vamne ORIGINAL ARTICLE 10.5005/jp-journals-10054-0027 Metabolic Derangement in Birth Asphyxia due to Cellular Injury with Reference to Mineral Metabolism in Different Stages of Hypoxic-ischemic
Bhawna Bhimte, Amrita Vamne ORIGINAL ARTICLE 10.5005/jp-journals-10054-0027 Metabolic Derangement in Birth Asphyxia due to Cellular Injury with Reference to Mineral Metabolism in Different Stages of Hypoxic-ischemic
BIRTH TRAUMA LITIGATION: PROVING THE CAUSE OF NEWBORN NEUROLOGIC INJURY 1 By Richard C. Halpern
 BIRTH TRAUMA LITIGATION: PROVING THE CAUSE OF NEWBORN NEUROLOGIC INJURY 1 By Richard C. Halpern Proving the cause of newborn neurologic injury in birth trauma litigation, an essential step to a successful
BIRTH TRAUMA LITIGATION: PROVING THE CAUSE OF NEWBORN NEUROLOGIC INJURY 1 By Richard C. Halpern Proving the cause of newborn neurologic injury in birth trauma litigation, an essential step to a successful
TREATMENT OF HYPOXIC ISCHEMIC ENCEPALOPATHY AND CEREBRAL HYPOTHERMIA
 TREATMENT OF HYPOXIC ISCHEMIC ENCEPALOPATHY AND CEREBRAL HYPOTHERMIA F. Emre CANPOLAT MD NICU, Ministry of Health, Zekai Tahir Burak Maternity and Teaching Hospital, Ankara, TURKEY Disclosure statement
TREATMENT OF HYPOXIC ISCHEMIC ENCEPALOPATHY AND CEREBRAL HYPOTHERMIA F. Emre CANPOLAT MD NICU, Ministry of Health, Zekai Tahir Burak Maternity and Teaching Hospital, Ankara, TURKEY Disclosure statement
Infection. Risk factor for infection ACoRN alerting sign with * Clinical deterioration. Problem List. Respiratory. Cardiovascular
 The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
INDUCED HYPOTHERMIA A Hot Topic. R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences
 INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
Pathophysiology and Cardiac Insights for Targeted Temperature Management in Emergency Medicine and Critical Care
 Pathophysiology and Cardiac Insights for Targeted Temperature Management in Emergency Medicine and Critical Care LINDSAY LEWIS BSN, RN, CCCC Faculty Disclosure I AM CURRENTLY EMPLOYED AS A CLINICAL MANAGER
Pathophysiology and Cardiac Insights for Targeted Temperature Management in Emergency Medicine and Critical Care LINDSAY LEWIS BSN, RN, CCCC Faculty Disclosure I AM CURRENTLY EMPLOYED AS A CLINICAL MANAGER
Col Rama Krishna Sanjeev Military Hospital Chennai Prof Shanmughasundaram Mehta Hospital, Chennai
 Col Rama Krishna Sanjeev Military Hospital Chennai Prof Shanmughasundaram Mehta Hospital, Chennai 11 day old male neonate admitted on 26/6 to our Hospital with c/olethargy -since day1 abnormal movements
Col Rama Krishna Sanjeev Military Hospital Chennai Prof Shanmughasundaram Mehta Hospital, Chennai 11 day old male neonate admitted on 26/6 to our Hospital with c/olethargy -since day1 abnormal movements
Correlation of Neurodevelopmental Outcome and brain MRI/EEG findings in term HIE infants
 Correlation of Neurodevelopmental Outcome and brain MRI/EEG findings in term HIE infants Ajou University School of Medicine Department of Pediatrics Moon Sung Park M.D. Hee Cheol Jo, M.D., Jang Hoon Lee,
Correlation of Neurodevelopmental Outcome and brain MRI/EEG findings in term HIE infants Ajou University School of Medicine Department of Pediatrics Moon Sung Park M.D. Hee Cheol Jo, M.D., Jang Hoon Lee,
SUBSTANCE EXPOSED INFANTS PRESENTED BY ECOLE J. BARROW-BROOKS M.ED & DARLENE D. OWENS MBA, LBSW, CADC, ADS
 SUBSTANCE EXPOSED INFANTS PRESENTED BY ECOLE J. BARROW-BROOKS M.ED & DARLENE D. OWENS MBA, LBSW, CADC, ADS 1 SUBSTANCE-EXPOSED INFANTS Refers to infants exposed to alcohol and or other substances ingested
SUBSTANCE EXPOSED INFANTS PRESENTED BY ECOLE J. BARROW-BROOKS M.ED & DARLENE D. OWENS MBA, LBSW, CADC, ADS 1 SUBSTANCE-EXPOSED INFANTS Refers to infants exposed to alcohol and or other substances ingested
Neuroprotection strategies in neonates with
 Neuroprotection strategies in neonates with encephalopathy Dr. Khorshid Mohammad, MD, MSc(Pediatrics), FABP, FRCP(Edin) NICU lead, Neuro-Critical Care Program, University of Calgary Disclosure I have no
Neuroprotection strategies in neonates with encephalopathy Dr. Khorshid Mohammad, MD, MSc(Pediatrics), FABP, FRCP(Edin) NICU lead, Neuro-Critical Care Program, University of Calgary Disclosure I have no
Early seizures indicate quality of perinatal care
 Archives of Disease in Childhood, 1985, 6, 89-813 Early seizures indicate quality of perinatal care R J DERHAM, T G MATTHEWS, AND T A CLARKE Rotunda Hospital, Dublin, Ireland SUMMARY An analysis of antepartum,
Archives of Disease in Childhood, 1985, 6, 89-813 Early seizures indicate quality of perinatal care R J DERHAM, T G MATTHEWS, AND T A CLARKE Rotunda Hospital, Dublin, Ireland SUMMARY An analysis of antepartum,
Lectures 4 Early fetal assessment, screening, ultrasound and treatment modalities during pregnancy. II. Asphyxia and Resuscitation (3 lectures)...
...") Outline of a 2 year Neonatology educational course (80 lectures) PLUS 2 graduate level courses (GENETICS and BIOSTATISTICS & EPIDEMIOLOGY Approximate Percent in Examination I. Maternal-Fetal Medicine (6
Outline of a 2 year Neonatology educational course (80 lectures) PLUS 2 graduate level courses (GENETICS and BIOSTATISTICS & EPIDEMIOLOGY Approximate Percent in Examination I. Maternal-Fetal Medicine (6
No Disclosures or Conflicts of Interest. Objectives. Overview. Therapeutic Hypothermia and other Potential Neuroprotective Strategies for HIE
 Therapeutic Hypothermia and other Potential Neuroprotective Strategies for HIE Alexis Davis, M.D. Medical Director, Neonatal Intensive Care Unit Lucile Packard Children s Hospital Clinical Associate Professor
Therapeutic Hypothermia and other Potential Neuroprotective Strategies for HIE Alexis Davis, M.D. Medical Director, Neonatal Intensive Care Unit Lucile Packard Children s Hospital Clinical Associate Professor