Seizure Management in End-of-Life Care: Fit for the Future? DR NICKY HARRIS PALLIATIVE CARE PAEDIATRICIAN PHD CANDIDATE, UWE
|
|
|
- Osborn Jefferson
- 5 years ago
- Views:
Transcription
1 Seizure Management in End-of-Life Care: Fit for the Future? DR NICKY HARRIS PALLIATIVE CARE PAEDIATRICIAN PHD CANDIDATE, UWE
2 Seizure/Fits/Convulsions Common in children with Life-limiting illness Neurological disease (static or progressive) Metabolic disease Malignant disease in CNS Not part of the image of a peaceful death
3 Challenges in Seizure management in End of Life Care Seizures may become more frequent, longer, and less responsive to treatment as underlying disease progresses Many drugs are not available in a form that is able to be easily administered or absorbed How to combine best practice in seizure management, with best practice in palliative care and respect patient choice Acceptable level of medical intervention place of care and place of death
4 Standard Seizure management Treatment options Wide range of oral medications, used alone or in combination Ketogenic diet Vagal nerve stimulation Surgical approaches Emergency management Buccal midazolam or rectal diazepam Rectal paraldehyde IV phenytoin or IV lorazepam Thiopentone, intubation and ventilation
5 End of Life Seizure management Treatment options Wide range of oral medications, used alone or in combination Ketogenic diet Vagal nerve stimulation Surgical approaches Emergency management Buccal midazolam or rectal diazepam Rectal paraldehyde IV phenytoin or lorazepam Thiopentone, intubation and ventilation
6 End-of-Life Seizure management Emergency management Buccal midazolam or rectal diazepam Rectal paraldehyde Subcutaneous midazolam infusion Subcutaneous phenobarbitone infusion
7 End-of-Life Seizure management Emergency management Buccal midazolam or rectal diazepam Rectal paraldehyde Subcutaneous midazolam infusion Subcutaneous phenobarbitone infusion When to use them? When not to use them? Practical issues: Availability Administration Dose Monitoring Any alternatives if these are unsuccessful?
8 Quality Improvement Methodology
9 Collaboration: SW CPCN, SWIPE, and SCN Project Leader: Dr Nicky Harris, Palliative Care Paediatrician and Postgraduate Researcher, UWE. Team members: Dr Megumi Baba, Medical Director, Children s Hospice South West Dr Antonia Beringer, Senior Research Associate, UWE Dr Charlotte Mellor, Consultant in Paediatric Palliative Care, Bristol Rebekah Rogers, Paediatric Pharmacist, Bristol Children s Hospital Dr Peta Sharples, Consultant Paediatric Neurologist, Bristol Kirsty Taylor, lead nurse, Devon Virgin Care Children s Palliative Care Team
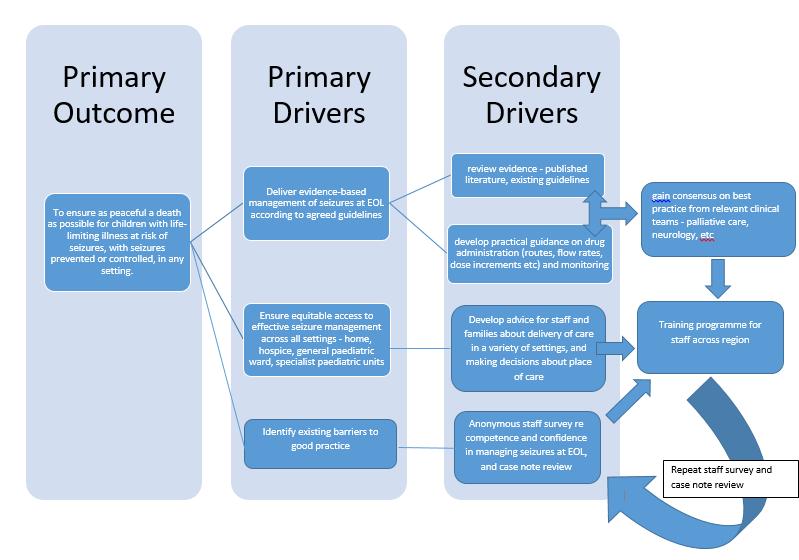
10 Primary Outcome To ensure as peaceful a death as possible for children with life-limiting illness at risk of seizures, with seizures prevented or controlled, in any setting.
11 Primary Drivers Deliver evidence-based management of seizures at EOL according to agreed guidelines Identify and address existing barriers to good practice Ensure equitable access to effective seizure management across all settings - home, hospice, general paediatric ward, specialist paediatric units
12 Secondary Drivers Review evidence - published literature, existing guidelines Anonymous staff survey re competence and confidence in managing seizures at EOL, and case note review Develop practical guidance on drug administration (routes, flow rates, dose increments etc) and monitoring Develop advice for staff and families about delivery of care in a variety of settings, and making decisions about place of care Gain consensus on best practice from relevant clinical teams - palliative care, neurology, etc Training programme for staff across region
13
14 What have we found?
15 Literature review + available guidance for management of seizures in EOL care Remarkably little published in peer-reviewed papers! Case reports and reflections No RCTs No Series reports in children
16 Literature review + available guidance for management of seizures in EOL care Grey literature guidelines, but limited evidence base Midazolam in Children 1 month 18 years: : Rainbows: start at 50mcg/kg/hr, increase to max 300mcg/kg/hour (max 100mg/24 hours, or 150mg/24 hours in specialist units) BNFC: start infusion at 1 mcg/kg/min, increase at min intervals to max 5 mcg/kg/min RCH Melbourne: 0.15mg/kg IV or SC stat, then 2 mcg/kg/min, increasing by 2mcg/kg/min until seizures cease, max 24 mcg/kg/min Adults: If seizures are mentioned (rare): Subcut midazolam 20-30mg/24 hours + prn 5-10mg s/c tds Increase dose as required; max 60mg/24 hours in community
17
18 Staff Survey 57/261 replies to survey monkey targeted at paediatric teams working in general paeds, epilepsy or neurology, or palliative care 78% had role in seizure management 93% had a role in supporting children who might die 80% had experience of managing seizures in children approaching the end of their lives 92% would anticipate that they would be asked to advise on seizure management in EOL situation
19
20
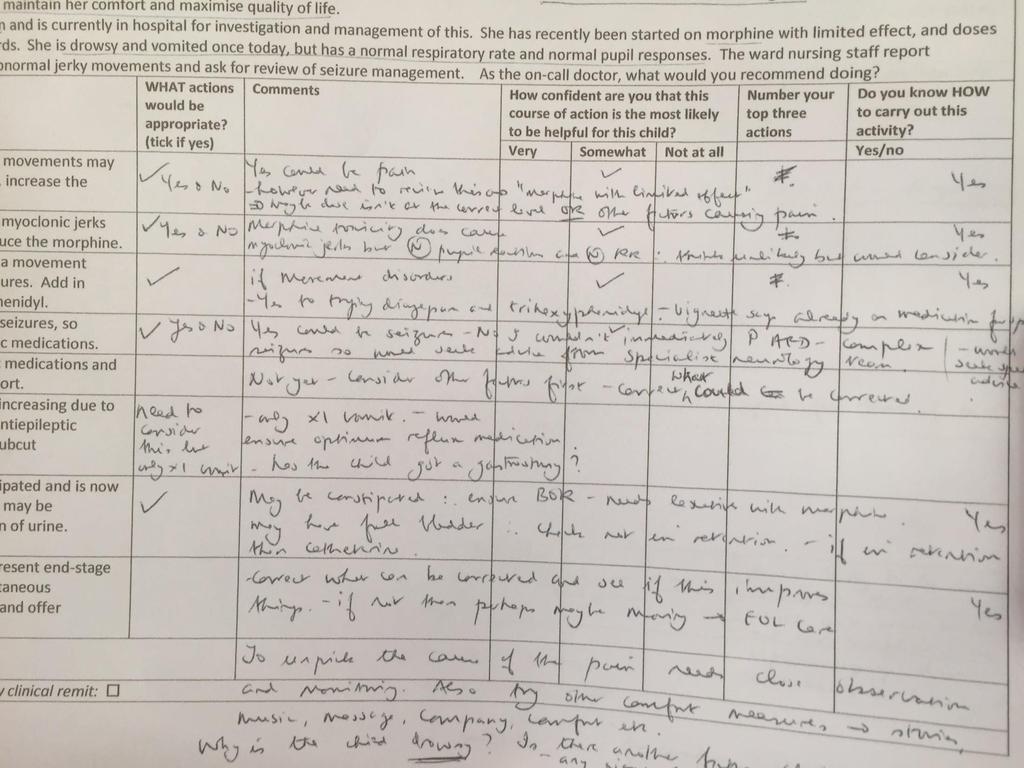
21 Clinical Vignettes 6 clinical scenarios about challenging seizure management in children s palliative care 17 yo CP, chest infection in hospice, not absorbing AEDs, how to control his fits? 9 yo, at home with brain tumour, fear of seizures,? Best prophylaxis 4 yo, neurodegenerative condition, twitching on ward? cause 6 yo, battens, high dose midazolam insufficient at home, what next? infant with HIE in A&E, apnoeas on midazolam, what options? 14 yo on PICU, fitting, unable to wean from ventilator, what can you do for him?
22
23
24
25 Summary of responses Wide range of potentially acceptable approaches to most scenarios General lack of consensus in therapeutic priorities Majority of responses were self-ranked as somewhat confident or not-at-all confident Level of detail in comments confirms complexity of decision-making, and a passion to explore all options to get the best solution.
26
27 Case note review: Remit for inclusion: age 0-25 receiving medical care in the south west known life-limiting illness where typical approach to the management of seizures or status epilepticus was limited by previous best-interests decisions time frame = preceding 10 years ( ) experienced difficult epilepsy management at EOL or when receiving palliative care
28 Identified Cases: 22 cases identified via survey monkey and targeted questioning of relevant staff and providers, and interrogation of CD register in hospice. 18 patients, (19 episodes of seizure management) met agreed criteria 4 patients excluded as although they fit the first 4 criteria, they died from other complications such as chest infections or planned extubation, without exacerbation/complications of epilepsy.
29 Key findings: 17 children received s/c or IV midazolam 9/17 on s/c midaz received doses larger than recommended in APPM guidelines. 4/6 children received phenobarbital doses above recommended guidelines General reluctance to escalate doses quickly to control symptoms Inconsistencies in rates of dose escalation, and identification of maximum doses
30 General Comments: Difficult area that causes significant clinical concern to staff In context of other simultaneous clinical concerns Impact of Family dynamics/circumstances on decision-making Practical delivery of care Emotional toll of supporting child, family and self Managing seizures was stressful, or labour-intensive or scary In 50% of cases, staff did not feel fully confident to diagnose or treat seizures
31
32
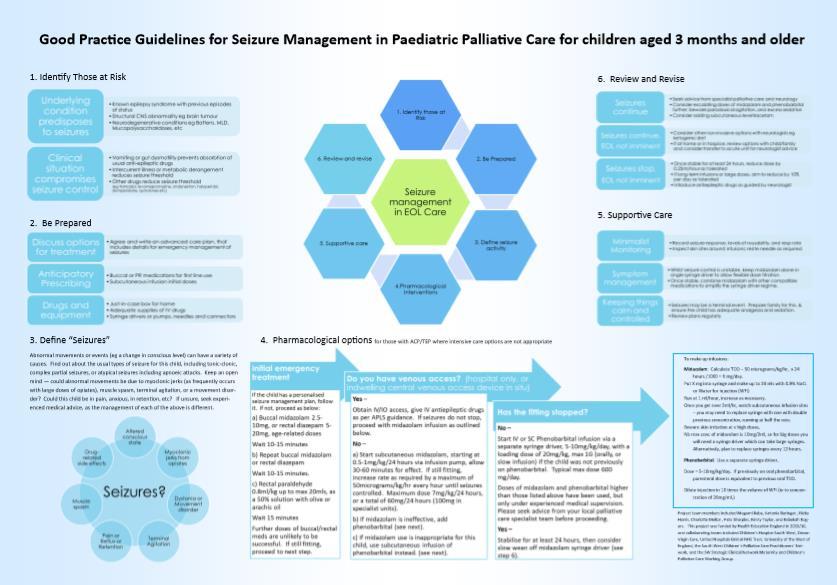
33 1. Identify those at Risk 6. Review and revise 2. Be Prepared Seizure management in EOL Care 5. Supportive care 3. Define seizure activity 4.Pharmacological interventions
34 1. Identify those at risk Underlying condition predisposes to seizures Known epilepsy syndrome with previous episodes of status Structural CNS abnormality eg brain tumour Neurodegenerative conditions eg Battens, MLD, Mucopolysaccharidoses, etc Clinical situation compromises seizure control Vomiting or gut dysmotility prevents absorbtion of usual anti-epileptic drugs Intercurrent illness or metabolic derangement reduces seizure threshold Other drugs reduce seizure threshold (eg tramadol, levomepromazine, ondansetron, haloperidol, domperidone, quinolones etc)
35 2. Be Prepared Discuss options for treatment Agree and write an advanced care plan, that includes details for emergency management of seizures Anticipatory Prescribing Buccal or PR medications for first line use Subcutaneous infusion initial doses Drugs and equipment Just-in-case box for home Adequate supplies of IV drugs Syringe drivers or pumps, needles and connectors
36 3. Is this Seizure Activity? abnormal movements or events have a variety of possible causes Drugrelated side effects Altered conscious state Myoclonic jerks from opiates Muscle spasm Seizures Dystonia or Movement disorder Pain or Reflux or Retention Terminal Agitation
37 4. Pharmacological Options for Seizure Management, for those with ACP/TEP where intensive care options are not appropriate Initial emergency treatment If the child has a personalised seizure management plan, follow it. If not, proceed as below: a) Buccal midazolam mg, or rectal diazepam 5-20mg, age-related doses Wait minutes b) Repeat buccal midazolam or rectal diazepam Wait minutes. c) Rectal paraldehyde 0.8ml/kg up to max 20mls, as a 50% solution with olive or arachis oil Wait 15 minutes Further doses of buccal/rectal meds are unlikely to be successful. If still fitting, proceed to next step. Do you have venous access? (hospital only, or indwelling central venous access device in situ) Yes Obtain IV/IO access, give IV phenytoin or IV lorazepam. If seizures do not stop, proceed with midazolam infusion as outlined below. No a) Start subcutaneous midazolam, starting at 50micrograms/kg/hour via infusion pump, allow minutes for effect. If still fitting, increase rate as required by 50micrograms/kg/hr every hour until seizures controlled, or you reach 200micrograms/kg/hour or a max 120mg/24 hours. b) If midazolam is ineffective, add phenobarbital (see next). c) If midazolam use is inappropriate for this child, use subcutaneous infusion of phenobarbital instead. (see next). Has the fitting stopped? No Start IV or SC Phenobarbital infusion via a separate syringe driver, 5-10mg/kg/day, with a loading dose of 20mg/kg, max 1G (orally, or slow infusion) if the child was not previously on phenobarbital. Typical max dose 600 mg/day. Doses of midazolam and phenobarbital higher than those listed above have been used, but only under experienced medical supervision. Please seek advice from your local palliative care specialist team before proceeding. Yes Stabilise for at least 24 hours, then consider slow wean off midazolam syringe driver (see step 6).
38 5. Supportive care Minimalist Monitoring Record seizure response, levels of rousability, and resp rate Inspect skin sites around infusions; resite needle as required Symptom management Whilst seizure control is unstable, keep midazolam alone in single syringe driver to allow flexible dose titration. Once stable, combine midazolam with other compatible medications to simplify the syringe driver regime. Keeping things calm and controlled Seizures may be a terminal event. Prepare family for this, & ensure the child has adequate analgesia and sedation. Review plans regularly


39 6. Review and Revise Seizures continue Seek advice from specialist palliative care and/or neurology Consider escalating doses of midazolam and phenobarbital further; beware paradoxical agitation, and excess sedation Consider adding subcutaneous levetiracetam Seizures continue, EOL not imminent Consider other non-invasive options with neurologists eg ketogenic diet If at home or in hospice, review options with child/family and consider transfer to acute unit for neurologist advice Seizures stop, EOL not imminent Once stable for at least 24 hours, reduce midazolam dose by 10-20% per hour as tolerated, and consider switching phenobarbital to enteral administration Introduce antiepileptic drugs as guided by neurologist
40 Addressing barriers to good practice Myth-busters: Drug administration Drug dosing Supportive Care Training programme Pharmacology of management of seizures Advanced care planning Practical guidance about syringe drivers
41 Gaining Consensus: Palliative Care Clinicians and Neurologists Best Practice guidance sent to eminent specialists in the field for comment: Neurology: Chair, British Paediatric Neurology Association Lead Clinicians, Paediatric Epilepsy Networks Paediatric Palliative Medicine: Association of Paediatric Palliative Medicine (APPM) Formulary Group Authors of Symptom Control Manual for Paediatric Palliative Care Regional Children s Palliative Care Clinical Networks
42 Next Steps External Peer Review Publication in BMJ Supportive and Palliative Care Harris N, Baba M, Mellor C et al: Seizure management in children requiring palliative care: a review of current practice BMJ Supportive & Palliative Care 2017 doi: / bmjspcare Accepted for presentation at International PPC Conference Rome November 2016 and National RCPCH Scientific Conference May 2017 Repeat survey, vignettes, case note review in another region NICE Guidance for EOL Care for Children and Young Adults 2016 identified seizure management as a research priority area Meeting of Expert Panel Group from Paediatric Neurology and PPC in autumn 2018.
43 Reflections on the process of Quality Improvement for rare EOL challenges: Funding opportunity was critical Protected time for staff Timeframe ensured no loss of momentum Pick your team to reflect real life challenges Clinical background/professions Relevant settings Academic partnership Rigorous methodology Collaboration and Peer Review essential Patient and Family Perspective
44 Seizure Management in End-of-Life Care: Fit for the Future? Thank you: Members of SW CPCN, SWIPE, SCN HEE for funding
In our patients the cause of seizures can be broadly divided into structural and systemic causes.
 Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
survey Parenteral anti-epileptics What is your experience? May July 2015
 Parenteral anti-epileptics What is your experience? May July 2015 Number of responses = 99 1a) In patients with pre-existing epilepsy controlled by PO medication that are imminently dying (prognosis
Parenteral anti-epileptics What is your experience? May July 2015 Number of responses = 99 1a) In patients with pre-existing epilepsy controlled by PO medication that are imminently dying (prognosis
[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]
![[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]](/thumbs/92/110296570.jpg "[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]") [Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text] Patients with egfr greater than 30mL/min Patients with egfr less than 30mL/min Symptom Drug Dose Symptom Drug Dose
[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text] Patients with egfr greater than 30mL/min Patients with egfr less than 30mL/min Symptom Drug Dose Symptom Drug Dose
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT
 PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
Renal Prescribing at End of Life Guidance for Anticipatory prescribing for patients in renal failure (egfr<30) at the end of life
 at the end of life") Guidance for Anticipatory prescribing for patients in renal failure (egfr
Guidance for Anticipatory prescribing for patients in renal failure (egfr
1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER
 1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER 1.1 GENERAL PRINCIPLES There are many causes of agitation in palliative care patients, which makes recommendations for treatment difficult.
1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER 1.1 GENERAL PRINCIPLES There are many causes of agitation in palliative care patients, which makes recommendations for treatment difficult.
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE
 PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
PAIN MANAGEMENT Patient established on oral morphine or opioid naive.
 PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Palliative Care Impact Survey
 September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
Care of the Dying Management in Severe Renal Failure
 Care of the Dying Management in Severe Renal Failure Clinical Guideline Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying Management in Severe Renal Failure Clinical Guideline Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying. For dosing in severe renal impairment see separate guidance for care of the dying in severe renal failure.
 Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
MORPHINE ADMINISTRATION
 Introduction Individualised Administration Drug of Choice Route of Administration & Doses Monitoring of Neonates & high risk patients Team Management Responsibility Morphine Protocol Flow Chart Introduction
Introduction Individualised Administration Drug of Choice Route of Administration & Doses Monitoring of Neonates & high risk patients Team Management Responsibility Morphine Protocol Flow Chart Introduction
On completion of this chapter you should be able to: list the most common types of childhood epilepsies and their symptoms
 9 Epilepsy The incidence of epilepsy is highest in the first two decades of life. It falls after that only to rise again in late life. Epilepsy is one of the most common chronic neurological condition
9 Epilepsy The incidence of epilepsy is highest in the first two decades of life. It falls after that only to rise again in late life. Epilepsy is one of the most common chronic neurological condition
Overview. 5% of paeds a+endances to ED
 Seizures Overview 5% of paeds a+endances to ED Status Epilepticus generalised convulsions las7ng 30 minutes or longer or failed to regain consciousness between fits over 30 minutes Why is SE important?
Seizures Overview 5% of paeds a+endances to ED Status Epilepticus generalised convulsions las7ng 30 minutes or longer or failed to regain consciousness between fits over 30 minutes Why is SE important?
Implementing the recommendation on medication management and symptom control
 Implementing the recommendation on medication management and symptom control Mike Grocott Professor of Anaesthesia and Critical Care Medicine University of Southampton Consultant in Critical Care Medicine
Implementing the recommendation on medication management and symptom control Mike Grocott Professor of Anaesthesia and Critical Care Medicine University of Southampton Consultant in Critical Care Medicine
Care of the Dying Management in Severe Renal Failure
 Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Syringe driver in Palliative Care
 Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
For patients and their carers this means smoother symptom control, better support in a crisis, and avoidance of admission if that is their choice.
 Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Care in the Last Days of Life
 Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL
 SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
PAIN MANAGEMENT Person established taking oral morphine or opioid naive.
 PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Algorithms for Symptom Management. In End of Life Care
 Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life
 MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
Antiepileptics Audit
 Antiepileptics Audit Dr Kate Marley Dr Lucy Potter Dr Melanie Brooks Dr Averil Fountain CNS Sue Croft External Reviewer: Dr A Nicolson Consultant Neurologist c CURRENT GUIDANCE 4.1 GENERAL PRINCIPLES Anti-epileptic
Antiepileptics Audit Dr Kate Marley Dr Lucy Potter Dr Melanie Brooks Dr Averil Fountain CNS Sue Croft External Reviewer: Dr A Nicolson Consultant Neurologist c CURRENT GUIDANCE 4.1 GENERAL PRINCIPLES Anti-epileptic
Use of Subcutaneous Levetiracetam at the end of life:
 Use of Subcutaneous Levetiracetam at the end of life: a literature review and audit Dr Anna Sutherland ST4 Palliative Medicine On behalf of the Health Education Thames Valley Registrars Research Network
Use of Subcutaneous Levetiracetam at the end of life: a literature review and audit Dr Anna Sutherland ST4 Palliative Medicine On behalf of the Health Education Thames Valley Registrars Research Network
Use of Subcutaneous Levetiracetam at the end of life:
 Use of Subcutaneous Levetiracetam at the end of life: a literature review and audit Dr Victoria Bradley ST4 Palliative Medicine On behalf of the Health Education Thames Valley Registrars Research Network
Use of Subcutaneous Levetiracetam at the end of life: a literature review and audit Dr Victoria Bradley ST4 Palliative Medicine On behalf of the Health Education Thames Valley Registrars Research Network
End of life prescribing guidance
 End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
Buccal Midazolam For the treatment of prolonged epileptic seizures, clusters of epileptic seizures and status epilepticus.
 Oxfordshire Clinical Commissioning Group, Oxford University Hospitals NHS Trust and Oxfordshire Health NHS Foundation Trust Shared Care Protocol and Information for GPs Buccal Midazolam For the treatment
Oxfordshire Clinical Commissioning Group, Oxford University Hospitals NHS Trust and Oxfordshire Health NHS Foundation Trust Shared Care Protocol and Information for GPs Buccal Midazolam For the treatment
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth)
") Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
Updated advice for nurses who care for patients with epilepsy
 NICE BULLETIN Updated advice for nurses who care for patients with epilepsy NICE provided the content for this booklet which is independent of any company or product advertised NICE BULLETIN Updated advice
NICE BULLETIN Updated advice for nurses who care for patients with epilepsy NICE provided the content for this booklet which is independent of any company or product advertised NICE BULLETIN Updated advice
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)
 Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)") Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
Supportive Care. End of Life Phase
 Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Antiepileptics Audit
 Antiepileptics Audit Dr Kate Marley Dr Lucy Potter Dr Melanie Brooks Dr Averil Fountain CNS Sue Croft External Reviewer: Dr A Nicolson Consultant Neurologist c CURRENT GUIDANCE 4.1 GENERAL PRINCIPLES Anti-epileptic
Antiepileptics Audit Dr Kate Marley Dr Lucy Potter Dr Melanie Brooks Dr Averil Fountain CNS Sue Croft External Reviewer: Dr A Nicolson Consultant Neurologist c CURRENT GUIDANCE 4.1 GENERAL PRINCIPLES Anti-epileptic
Symptom Management Guidelines for End of Life Care
 Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
Palliative care for patients with brain cancer
 Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
4. GUIDELINES FOR THE USE OF ANTI- EPILEPTICS IN PALLIATIVE CARE
 4. GUIDELINES FOR THE USE OF ANTI- EPILEPTICS IN PALLIATIVE CARE 4.1 GENERAL PRINCIPLES Anti-epileptic drugs should be considered in all patients with primary or secondary brain tumours who have a history
4. GUIDELINES FOR THE USE OF ANTI- EPILEPTICS IN PALLIATIVE CARE 4.1 GENERAL PRINCIPLES Anti-epileptic drugs should be considered in all patients with primary or secondary brain tumours who have a history
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT (estimated glomerular filtration rate<30)
") GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL IMPAIRMENT
 ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRESCRIPTION & ADMINISTRATION RECORD (SPAR) Name: Address: Postcode: Date of Birth: NHS Number:
 Name: Address: Postcode: Date of Birth: NHS Number:") FILE IN PATIENT S COMMUNITY HEALTH RECORD FOLDER : SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRERIPTION & ADMINISTRATION RECORD (SPAR) Abbreviations used in this document to be listed here with the full
FILE IN PATIENT S COMMUNITY HEALTH RECORD FOLDER : SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRERIPTION & ADMINISTRATION RECORD (SPAR) Abbreviations used in this document to be listed here with the full
Use of Subcutaneous Levetiracetam at the end of life:
 Use of Subcutaneous Levetiracetam at the end of life: a literature review and audit Dr Victoria Bradley ST4 Palliative Medicine On behalf of the Health Education Thames Valley Registrars Research Network
Use of Subcutaneous Levetiracetam at the end of life: a literature review and audit Dr Victoria Bradley ST4 Palliative Medicine On behalf of the Health Education Thames Valley Registrars Research Network
Supporting Last Days of Life Symptom Control Medication Guidance: Algorithm. Agitation & Anxiety
 Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
PALLIATIVE CARE PRESCRIBING FOR PATIENTS WHO ARE SUBSTANCE MISUSERS
 PALLIATIVE CARE PRESCRIBING FOR PATIENTS WHO ARE SUBSTANCE MISUSERS Background information Substance misusers who develop palliative care needs are likely to have psychological, social and existential
PALLIATIVE CARE PRESCRIBING FOR PATIENTS WHO ARE SUBSTANCE MISUSERS Background information Substance misusers who develop palliative care needs are likely to have psychological, social and existential
Lieven Lagae Department of Paediatric Neurology Leuven University Leuven, Belgium. Management of acute seizure settings from infancy to adolescence
 Lieven Lagae Department of Paediatric Neurology Leuven University Leuven, Belgium Management of acute seizure settings from infancy to adolescence Consequences of prolonged seizures Acute morbidity and
Lieven Lagae Department of Paediatric Neurology Leuven University Leuven, Belgium Management of acute seizure settings from infancy to adolescence Consequences of prolonged seizures Acute morbidity and
Mid Essex Locality Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care
 Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Sedation in Children
 CHILDREN S SERVICES Sedation in Children See text for full explanation and drug doses Patient for Sedation Appropriate staffing Resuscitation equipment available Monitoring equipment Patient suitability
CHILDREN S SERVICES Sedation in Children See text for full explanation and drug doses Patient for Sedation Appropriate staffing Resuscitation equipment available Monitoring equipment Patient suitability
Management of Seizures at the End of Life A new way forward?
 Management of Seizures at the End of Life A new way forward? Dr Victoria Bradley ST4 Palliative Medicine On behalf of the Health Education Thames Valley Registrars Research Network Dr Anna Sutherland,
Management of Seizures at the End of Life A new way forward? Dr Victoria Bradley ST4 Palliative Medicine On behalf of the Health Education Thames Valley Registrars Research Network Dr Anna Sutherland,
EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE
 EAST LANCASHIRE SPECIALIST PALLIATIVE CARE TEAM EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Reviewed and updated August 2009 Next review date August 2011 Approved
EAST LANCASHIRE SPECIALIST PALLIATIVE CARE TEAM EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Reviewed and updated August 2009 Next review date August 2011 Approved
Ventilation/End of Life Neuromuscular Disorders. Dr Emma Husbands Consultant Palliative Medicine
 Ventilation/End of Life Neuromuscular Disorders Dr Emma Husbands Consultant Palliative Medicine Emma.Husbands@glos.nhs.uk Contents Cases NIV and palliation and ethical bits APM guidelines Important bits
Ventilation/End of Life Neuromuscular Disorders Dr Emma Husbands Consultant Palliative Medicine Emma.Husbands@glos.nhs.uk Contents Cases NIV and palliation and ethical bits APM guidelines Important bits
Status Epilepticus And Prolonged Seizures: Guideline For Management In Adults. Contents
 Status Epilepticus And Prolonged Seizures: Guideline For Management In Adults Classification: Clinical guideline Lead Author: Rajiv Mohanraj, Consultant Neurologist Additional author(s): Matt Jones, Consultant
Status Epilepticus And Prolonged Seizures: Guideline For Management In Adults Classification: Clinical guideline Lead Author: Rajiv Mohanraj, Consultant Neurologist Additional author(s): Matt Jones, Consultant
patient group direction
 DIAZEPAM (RECTAL) v01 1/8 DIAZEPAM (RECTAL) PGD Details Version 1.0 Legal category Staff grades Approved by POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care
DIAZEPAM (RECTAL) v01 1/8 DIAZEPAM (RECTAL) PGD Details Version 1.0 Legal category Staff grades Approved by POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care
APPENDIX K Pharmacological Management
 1 2 3 4 APPENDIX K Pharmacological Management Table 1 AED options by seizure type Table 1 AED options by seizure type Seizure type First-line AEDs Adjunctive AEDs Generalised tonic clonic Lamotrigine Oxcarbazepine
1 2 3 4 APPENDIX K Pharmacological Management Table 1 AED options by seizure type Table 1 AED options by seizure type Seizure type First-line AEDs Adjunctive AEDs Generalised tonic clonic Lamotrigine Oxcarbazepine
Effective Shared Care Agreement for the treatment of severe motor complications in people with Parkinson Disease with apomorphine (APO-go )
") Effective Shared Care Agreement for the treatment of severe motor complications in people with Parkinson Disease with apomorphine (APO-go ) This shared care agreement outlines the ways in which the responsibilities
Effective Shared Care Agreement for the treatment of severe motor complications in people with Parkinson Disease with apomorphine (APO-go ) This shared care agreement outlines the ways in which the responsibilities
ALLERGIES/ SENSITIVITIES This section must be completed before prescribing/administering any drug
 COMMUNITY PRESCRIPTION CHART All entries should be in CAPITAL letters and in indelible black ink. If medications/ doses are stopped, cross through the relevant line clearly to avoid error. GP: PRESCRIBER
COMMUNITY PRESCRIPTION CHART All entries should be in CAPITAL letters and in indelible black ink. If medications/ doses are stopped, cross through the relevant line clearly to avoid error. GP: PRESCRIBER
Administering Rescue Medication into Children for Prolonged Seizures
 Standard Operating Procedure 10 (SOP 10) Administering Rescue Medication into Children for Prolonged Seizures Why we have a procedure? Black Country Partnership NHS Trust (hereafter referred to as the
Standard Operating Procedure 10 (SOP 10) Administering Rescue Medication into Children for Prolonged Seizures Why we have a procedure? Black Country Partnership NHS Trust (hereafter referred to as the
The last days of life in hospital and at home
 The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
Approach to symptom control near the end-of-life
 Approach to symptom control near the end-of-life 18 Sept 2011 Dr Alethea Yee Senior Consultant, Department of Palliative Medicine National Cancer Centre,Singapore What is end of life? No precise definition
Approach to symptom control near the end-of-life 18 Sept 2011 Dr Alethea Yee Senior Consultant, Department of Palliative Medicine National Cancer Centre,Singapore What is end of life? No precise definition
End of Life Care. Dr Anne Garry Consultant in Palliative Medicine
 End of Life Care Dr Anne Garry Consultant in Palliative Medicine Concerns voiced both by public and professionals.. Implementation and on-going training highly variable across country Decisions made by
End of Life Care Dr Anne Garry Consultant in Palliative Medicine Concerns voiced both by public and professionals.. Implementation and on-going training highly variable across country Decisions made by
PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE
 PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Originally produced: July 2006 First Review: August 2009 Second Review: November 2011 For review November 2013 Approved
PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Originally produced: July 2006 First Review: August 2009 Second Review: November 2011 For review November 2013 Approved
Management of Epilepsy in Primary Care and the Community. Carrie Burke, Epilepsy Specialist Nurse
 Management of Epilepsy in Primary Care and the Community Carrie Burke, Epilepsy Specialist Nurse Epilepsy & Seizures Epilepsy is a common neurological disorder characterised by recurring seizures (NICE,
Management of Epilepsy in Primary Care and the Community Carrie Burke, Epilepsy Specialist Nurse Epilepsy & Seizures Epilepsy is a common neurological disorder characterised by recurring seizures (NICE,
Surveillance report Published: 12 April 2018 nice.org.uk
 Surveillance report 2018 Epilepsies: diagnosis and management (2012) NICE guideline CG137 Surveillance report Published: 12 April 2018 nice.org.uk NICE 2018. All rights reserved. Subject to Notice of rights
Surveillance report 2018 Epilepsies: diagnosis and management (2012) NICE guideline CG137 Surveillance report Published: 12 April 2018 nice.org.uk NICE 2018. All rights reserved. Subject to Notice of rights
Medicines Protocol RECTAL DIAZEPAM
 Medicines Protocol RECTAL DIAZEPAM RECTAL DIAZEPAM v2.0 1/6 Protocol Details Version 2.0 Legal category Staff grades POM Registered Paramedic Registered Nurse Specialist Paramedic (Urgent and Emergency
Medicines Protocol RECTAL DIAZEPAM RECTAL DIAZEPAM v2.0 1/6 Protocol Details Version 2.0 Legal category Staff grades POM Registered Paramedic Registered Nurse Specialist Paramedic (Urgent and Emergency
Diamorphine 4 hour. alfentanil (500microgram/mL) Calculated by dividing 24 hour oral morphine dose by 30
 Calculated by dividing 24 hour oral morphine dose by 30") If more information is required please seek help from specialist palliative care pioid dose conversion chart, syringe driver doses, rescue/prn doses and opioid patches Use the conversion chart to work
If more information is required please seek help from specialist palliative care pioid dose conversion chart, syringe driver doses, rescue/prn doses and opioid patches Use the conversion chart to work
A Framework of Competences for Special Interest Module in Paediatric Epilepsies
 A Framework of Competences for Special Interest Module in Paediatric Epilepsies 2 Section 1 CONTENTS Introduction 5 Section 2 Specific Competences in Paediatric Epilepsies 7 Knowledge and Understanding
A Framework of Competences for Special Interest Module in Paediatric Epilepsies 2 Section 1 CONTENTS Introduction 5 Section 2 Specific Competences in Paediatric Epilepsies 7 Knowledge and Understanding
Shared Care Guideline. The Management of Epilepsies in Children
 THE SOUTH YORKSHIRE & BASSETLAW Shared Care Guideline For The Management of Epilepsies in Children Shared care guideline developed by: Sheffield Children's NHS Foundation Trust; Dr P Baxter Consultant
THE SOUTH YORKSHIRE & BASSETLAW Shared Care Guideline For The Management of Epilepsies in Children Shared care guideline developed by: Sheffield Children's NHS Foundation Trust; Dr P Baxter Consultant
Care of the dying in End Stage Kidney Disease (ESKD) - Conservative. Elizabeth Josland Renal Supportive Care CNC St George Hospital
 - Conservative. Elizabeth Josland Renal Supportive Care CNC St George Hospital") Care of the dying in End Stage Kidney Disease (ESKD) - Conservative Elizabeth Josland Renal Supportive Care CNC St George Hospital Introduction What does conservative management look like? How does the
Care of the dying in End Stage Kidney Disease (ESKD) - Conservative Elizabeth Josland Renal Supportive Care CNC St George Hospital Introduction What does conservative management look like? How does the
Conservative Management of Uraemia
 Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
BACKGROUND Measuring renal function :
 A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
Guidance for the Use of Subcutaneous Furosemide by Continuous Infusion for Heart Failure in Community Settings
 Guidance for the Use of Subcutaneous Furosemide by Continuous Infusion for Heart Failure in Community Settings NHS Highland Authorised by: Planning For Fairness: Yes/No (Formerly EQIA) Distribution Consultant
Guidance for the Use of Subcutaneous Furosemide by Continuous Infusion for Heart Failure in Community Settings NHS Highland Authorised by: Planning For Fairness: Yes/No (Formerly EQIA) Distribution Consultant
CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC
 CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC OBJECTIVES UNDERSTANDING OF: POTENTIAL COMPLEXITIES OF ESKD PATIENTS IMPORTANCE OF COMMUNICATION CONSIDERATIONS AT END-OF-LIFE END-OF-LIFE
CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC OBJECTIVES UNDERSTANDING OF: POTENTIAL COMPLEXITIES OF ESKD PATIENTS IMPORTANCE OF COMMUNICATION CONSIDERATIONS AT END-OF-LIFE END-OF-LIFE
Refractory Seizures. Dr James Edwards EMCORE May 30th 2014
 Refractory Seizures Dr James Edwards EMCORE May 30th 2014 Refractory Seizures Seizures are a common presentation to the ED and some patients will have multiple seizures or have a reduced level of consciousness
Refractory Seizures Dr James Edwards EMCORE May 30th 2014 Refractory Seizures Seizures are a common presentation to the ED and some patients will have multiple seizures or have a reduced level of consciousness
Anticipatory Medications for End of Life Patients. Doses must be proportional to the current analgesic medication YES NO YES NO
 Anticipatory Medications for End of Life Patients oses must be proportional to the current analgesic medication Please refer ALL patients on Methadone or Ketamine to palliative care team for advice. Patients
Anticipatory Medications for End of Life Patients oses must be proportional to the current analgesic medication Please refer ALL patients on Methadone or Ketamine to palliative care team for advice. Patients
Renal Palliative Care Last Days of Life
 Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
PHARMACOLOGY AND PHARMACOKINETICS
 DRUG GUIDELINE Insulin, human neutral (Actrapid ) Intravenous Infusion for SCOPE (Area): FOR USE IN: Critical Care Unit, Emergency Department and Operating Suite EXCLUSIONS: Paediatrics (seek Paediatrician
DRUG GUIDELINE Insulin, human neutral (Actrapid ) Intravenous Infusion for SCOPE (Area): FOR USE IN: Critical Care Unit, Emergency Department and Operating Suite EXCLUSIONS: Paediatrics (seek Paediatrician
APPENDIX T - Unit costs of anti-epileptic drugs for 2012 guideline
 Drug name APPENDIX T - Unit costs of anti-epileptic drugs for 2012 guideline Unit costs and weighted average unit costs for drug used in the treatment of focal and generalised epilepsies Prescription Cost
Drug name APPENDIX T - Unit costs of anti-epileptic drugs for 2012 guideline Unit costs and weighted average unit costs for drug used in the treatment of focal and generalised epilepsies Prescription Cost
SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA. [compatible with NICE guidance]
![SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA. [compatible with NICE guidance]](/thumbs/80/80440271.jpg "SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA. [compatible with NICE guidance]") SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA [compatible with NICE guidance] Medicines Management Committee August 2002 For review August 2003 Rationale The SiGMA algorithm
SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA [compatible with NICE guidance] Medicines Management Committee August 2002 For review August 2003 Rationale The SiGMA algorithm
NonConvulsive Seizure
 Sample Protocol #5: Management of status epilepticus and seizures in hospitalized patients nconvulsive Seizure Patient presents with alteration of consciousness unexplained by other etiologies AND suspicious
Sample Protocol #5: Management of status epilepticus and seizures in hospitalized patients nconvulsive Seizure Patient presents with alteration of consciousness unexplained by other etiologies AND suspicious
Guideline for use of Intramuscular Medication for Acutely Disturbed Behaviour in Mental Health and Associated Services
 NHS GGC Mental Health Service Guideline for use of Intramuscular Medication for Acutely Disturbed Behaviour in Mental Health and Associated Services Important Note: The Intranet version of this document
NHS GGC Mental Health Service Guideline for use of Intramuscular Medication for Acutely Disturbed Behaviour in Mental Health and Associated Services Important Note: The Intranet version of this document
Outline. What is a seizure? What is epilepsy? Updates in Seizure Management Terminology, Triage & Treatment
 Outline Updates in Seizure Management Terminology, Triage & Treatment Joseph Sullivan, MD! Terminology! Videos of different types of seizures! Diagnostic evaluation! Treatment options! Acute! Maintenance
Outline Updates in Seizure Management Terminology, Triage & Treatment Joseph Sullivan, MD! Terminology! Videos of different types of seizures! Diagnostic evaluation! Treatment options! Acute! Maintenance
Cardiac Catheter Labs Intravenous Drug Therapy Guide
 Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Cardiac Catheter Lab IV Medicines Guideline Helen Buxton ( Senior Cath Lab
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Cardiac Catheter Lab IV Medicines Guideline Helen Buxton ( Senior Cath Lab
Community Paediatric Policy for minimal sedation
 Community Paediatric Policy for minimal sedation Classification: Policy Lead Author: Amy Wilson Consultant Community Paediatrician Additional author(s): Trust Sedation Comittee Authors Division: Salford
Community Paediatric Policy for minimal sedation Classification: Policy Lead Author: Amy Wilson Consultant Community Paediatrician Additional author(s): Trust Sedation Comittee Authors Division: Salford
Care Coordination / Care Programme Approach Learning Disability PGN Management of Epilepsy in Learning Disability (LD) Planned and Urgent Care V03
 Planned and Urgent Care V03") Care Coordination / Care Programme Approach Learning Disability PGN Management of Epilepsy in Learning Disability (LD) Planned and Urgent Care V03 V03 issued Issue 1 Dec 14 Issue 2 Dec 17 Planned review
Care Coordination / Care Programme Approach Learning Disability PGN Management of Epilepsy in Learning Disability (LD) Planned and Urgent Care V03 V03 issued Issue 1 Dec 14 Issue 2 Dec 17 Planned review
SPAGG. Coversheet for Specialist Palliative Audit and Guideline Group Agreed Documentation
 SPAGG Coversheet for Specialist Palliative Audit and Guideline Group Agreed Documentation This sheet is to accompany all documentation agreed by SPAGG. This will assist maintenance of the guidelines as
SPAGG Coversheet for Specialist Palliative Audit and Guideline Group Agreed Documentation This sheet is to accompany all documentation agreed by SPAGG. This will assist maintenance of the guidelines as
MND Just in Case kit Information for GPs
 MND Just in Case kit Information for GPs What is the MND Just in Case kit? 2 Motor neurone disease (MND) is a progressive and terminal disease that results in degeneration of the motor neurones in the
MND Just in Case kit Information for GPs What is the MND Just in Case kit? 2 Motor neurone disease (MND) is a progressive and terminal disease that results in degeneration of the motor neurones in the
CrackCast Episode 18 Seizures
 CrackCast Episode 18 Seizures Episode overview: 1) Define status epilepticus 2) List the doses of common medications used for status epilepticus 3) List 10 differential diagnoses for seizures 4) List 10
CrackCast Episode 18 Seizures Episode overview: 1) Define status epilepticus 2) List the doses of common medications used for status epilepticus 3) List 10 differential diagnoses for seizures 4) List 10
patient group direction
 DIAZEPAM v01 1/9 DIAZEPAM PGD Details Version 1.0 Legal category Staff grades Approved by CD Benz POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care Practitioner
DIAZEPAM v01 1/9 DIAZEPAM PGD Details Version 1.0 Legal category Staff grades Approved by CD Benz POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care Practitioner
Refractory Status Epilepticus in Children: What are the Options?
 Refractory Status Epilepticus in Children: What are the Options? Weng Man Lam, PharmD, BCPS, BCPPS PICU Clinical Pharmacy Specialist Memorial Hermann Texas Medical Center November 11, 2017 Objectives 1.
Refractory Status Epilepticus in Children: What are the Options? Weng Man Lam, PharmD, BCPS, BCPPS PICU Clinical Pharmacy Specialist Memorial Hermann Texas Medical Center November 11, 2017 Objectives 1.
Anticipatory prescribing and end of life considerations. Dr Stephanie Lippett
 Anticipatory prescribing and end of life considerations Dr Stephanie Lippett contents Pain Restlessness/agitation Nausea/vomiting Secretions Syringe driver Anticipatory prescribing Important things to
Anticipatory prescribing and end of life considerations Dr Stephanie Lippett contents Pain Restlessness/agitation Nausea/vomiting Secretions Syringe driver Anticipatory prescribing Important things to
Coversheet for Network Site Specific Group Agreed Documentation
 Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
Essential Syringe Driver Training for T 34. Elaine Bird St Luke s Hospice
 Essential Syringe Driver Training for T 34 Elaine Bird St Luke s Hospice Aim For all practitioners to be accountable for their individual competence and capability when caring for a resident with a T34
Essential Syringe Driver Training for T 34 Elaine Bird St Luke s Hospice Aim For all practitioners to be accountable for their individual competence and capability when caring for a resident with a T34
BJF Acute Pain Team Formulary Group
 Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Prescribing and Monitoring Anti-Epileptic Drugs
 Prescribing and Monitoring Anti-Epileptic Drugs Mark Granner, MD Clinical Professor and Vice Chair for Clinical Programs Director, Iowa Comprehensive Epilepsy Program Department of Neurology University
Prescribing and Monitoring Anti-Epileptic Drugs Mark Granner, MD Clinical Professor and Vice Chair for Clinical Programs Director, Iowa Comprehensive Epilepsy Program Department of Neurology University
 The last days of life Linda Magann CNC Palliative Care St George Hospital I m not afraid of dying, I just don t want to be there when it happens Woody Allen Palliative Care is an approach that improves
The last days of life Linda Magann CNC Palliative Care St George Hospital I m not afraid of dying, I just don t want to be there when it happens Woody Allen Palliative Care is an approach that improves
** Medication exercises ** NICU Phase II
 ** Medication exercises ** NICU Phase II A) Baby A has had a bowel resection six hours ago. She weighs 3 kg. Post-op, she is quite agitated and she is on a fentanyl drip at 2 micrograms/kg/hr (#1). She
** Medication exercises ** NICU Phase II A) Baby A has had a bowel resection six hours ago. She weighs 3 kg. Post-op, she is quite agitated and she is on a fentanyl drip at 2 micrograms/kg/hr (#1). She
Children s palliative care is defined as an active and total approach to care, from the point of diagnosis or recognition, throughout the child s
 Level : a consultant paediatrician in PPM, or a small number of children s hospice medical leaders (mainly leaders in sub-specialty formation and development, and with roles beyond their local hospice),
Level : a consultant paediatrician in PPM, or a small number of children s hospice medical leaders (mainly leaders in sub-specialty formation and development, and with roles beyond their local hospice),
Guideline for the use of Clonidine for Sedation in Adult Intensive Care
 Guideline for the use of Clonidine for Sedation in Adult Intensive Care This guidance does not override the individual responsibility of health professionals to make appropriate decision according to the
Guideline for the use of Clonidine for Sedation in Adult Intensive Care This guidance does not override the individual responsibility of health professionals to make appropriate decision according to the
Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital.
 Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital. Things to consider: 1. Very common symptoms. 2. Can occur in any
Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital. Things to consider: 1. Very common symptoms. 2. Can occur in any
Doncaster & Bassetlaw Cancer Locality. Palliative Care Core Formulary
 Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
PRESCRIBING PRACTICE IN DELIRIUM. John Warburton Critical Care Pharmacist
 PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines