Anesthetic Management of Child with Moyamoya Disease for Pial Synangiosis
|
|
|
- Kory Sharleen Owen
- 5 years ago
- Views:
Transcription
1 Anesthetic Management of Child with Moyamoya Disease for Pial Synangiosis Craig D. McClain, MD, MPH Boston Children s Hospital and Harvard Medical School
2 Case Presentation 14 year old male with bilateral moyamoya disease is referred from an outside hospital and presents for bilateral pial synangiosis H/o multiple TIAs Old, completed stroke in right hemisphere Mild left sided weakness, but otherwise neurologically intact
3 Pt. has history of craniopharyngioma treated with surgery and radiation Patient also has pan-hypopituitarism secondary to resection of craniopharyngioma Other medical history is non-contributory
4 What blood vessels are involved with moyamoya disease? A. Internal carotid arteries B. Vertebral arteries C. Remnants of the Vein of Galen D. External carotid arteries E. All of the above

5 Sorry I disagree Try again
6 CORRECT!!
7 PATHOPHYSIOLOGY OF MOYAMOYA DISEASE
8 Moyamoya Disease Bilateral narrowing of the terminal internal carotid arteries in the supraclinoid area Results in long term progressive cerebral ischemia Secondary development of abnormal, weak, thin collateral arteries in Basal Ganglia/Circle of Willis area These collaterals are what gives rise to the name moyamoya, meaning like a puff of smoke in Japanese The following slide shows the circle of Willis and the internal carotid arteries NEJM 2009; 360:
9 Moyamoya Disease Moyamoya disease is a neurovascular disorder that has a bimodal peak of presentation. In the first decade of life, the disease tends to present with strokes or TIAs In the 5 th decade of life, presentation tends to be with hemorrhage and the consequences of intracranial bleeding NEJM 2009; 360:
10 Natural History The natural history of moyamoya disease is quite variable. Progression can be slow with infrequent events, or progress can be fulminant resulting in a rapid decline with permanent neurologic impairment.
11 Anesthetic Goals Maintenance of adequate cerebral blood flow is the primary goal of anesthesia when managing these patients. The anesthetic and surgical management can sound fairly straight forward on paper. However, putting these plans into practice can be fraught with pitfalls. Anesth Analg 1993; 77:
12 Autoregulation It is unclear what degree of autoregulation these patients possess. They do appear to have some degree of autoregulation, but it is unclear what the limits are. It would appear that the limits of autoregulation in moyamoya patients are somewhat individualized and narrower than the general population.
13 CMRO 2 /CBF Physiology Healthy children typically have a higher Cerebral Metabolic Rate of Oxygen consumption (CMRO 2 ) Moyamoya vessels and normal cerebral collaterals are maximally dilated at baseline Blood flow typically just meets oxygen demand in the awake moyamoya patient As mentioned above, cerebrovascular autoregulation is impaired
14 This graph shows the normal cerebral autoregulatory limits for healthy adult patients

15 In a normal, healthy brain, there is a relative luxury of blood flow for cerebral oxygen demand
16 In a brain with moyamoya, the CBF is just meeting the oxygen demand. Thus, these patients are extremely sensitive to any decrease in CBF. Even minor decreases in CBF may lead to ischemia and stroke.
17 RADIOGRAPHIC FEATURES

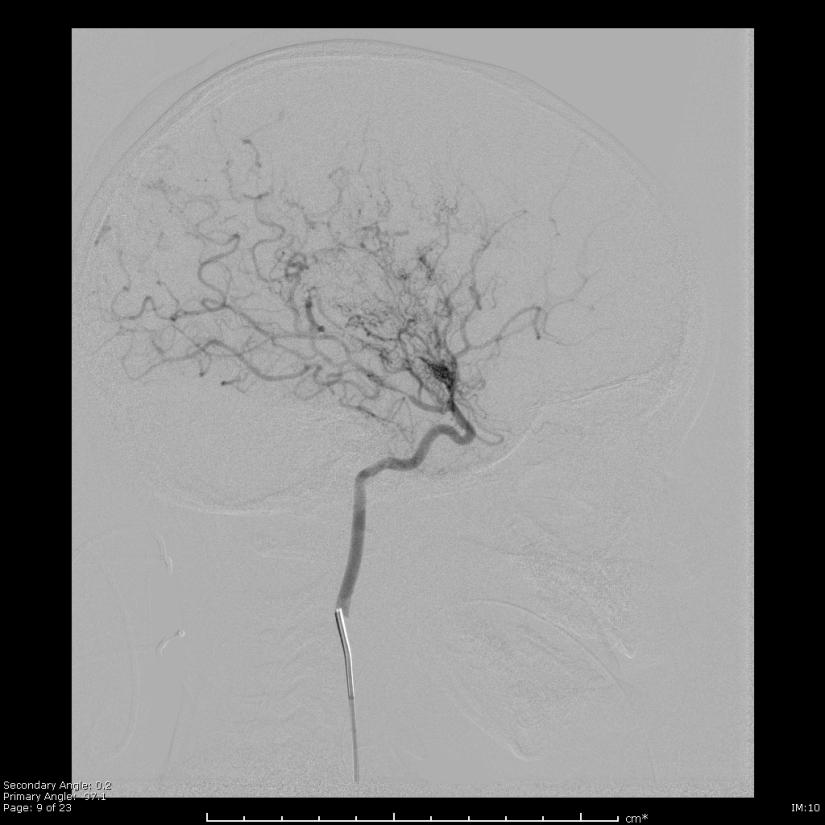
18 What is the Suzuki grade of this angiogram? A. Grade I B. Grade II-III C. Grade III-IV
19 Sorry I disagree Try again
20 CORRECT!!
21 Suzuki Grade Disease severity classified into stages based on description of Suzuki, et al in The presence of the classic puff of smoke appearance of collaterals on angiogram corresponds to the intermediate stages of the Suzuki grading system Arch Neurol 1969; 20:
22 Suzuki Grade Grade I narrowing of ICA apex Grade II initiation of moyamoya collaterals Grade III progressive ICA stenosis with intensification of moyamoya collaterals Grade IV development of ECA collaterals Grade V intensification of ECA collaterals and reduction of moyamoya collaterals Grade VI total occlusion of ICA and disappearance of moyamoya collaterals Arch Neurol 1969; 20:
23 The following images are simply examples and not meant to be this patient s images


24 Clockwise Suzuki I, II-III and III-IV
 Normal flow (green arrow, black")
25 MRI Axial flair MR with ivy sign (red arrow, bright signal in sulci for slow flow) Normal flow (green arrow, black sulci).
26 Our Patient Pt has undergone MRI/MRA that showed bilateral moyamoya disease with Ivy sign Pt then had a cerebral angiogram that showed bilateral moyamoya disease with Suzuki grade IV on right and Suzuki grade II on left
27 ASSOCIATED CONDITIONS
28 Please select the single best answer that describes pathologies associated with moyamoya disease. A. Down s syndrome B. Neurofibromatosis C. History of intracranial radiation D. Hemoglobinopathies E. All of the above
29 Sorry I disagree Try again
30 CORRECT!!
31 A number of other pathologies are associated with moyamoya disease including Down s syndrome, various hemoglobinopathies (namely sickle cell disease), neurofibromatosis, and patients who have have intracranial radiation (specifically for sellar masses). Neurosurg Focus 2009; 26(4): E10.
32 Associated Conditions Common 50-75% Moyamoya disease without other disease Asian ethnicity Less common (moyamoya syndrome) 10-20% Sickle cell disease Neurofibromatosis type I History of intracranial radiation Down s syndrome Rare (moyamoya syndrome) - <10% Congenital cardiac disease Renal artery stenosis Hyperthyroidism Giant cervicofacial hemangiomas NEJM 2009; 360:
33 Associated Conditions It is crucial to understand that these associations occur frequently and to plan care with consideration of the comorbidities (e.g. congenital cardiac disease with Down s and endocrinopathies with a history of sellar tumors)
34 OUTCOMES WITH TYPE OF MANAGEMENT
35 Outcomes with surgical management are superior to medical management alone. True False
36 Sorry I disagree Try again
37 CORRECT!!
38 Medical Management Medical management is limited to drugs that either decrease the headaches associated with moyamoya (calcium channel blockers, may also decrease TIAs) and antiplatelet agents such as aspirin. Agents such as calcium channel blockers must be used cautiously as they may cause hypotension Other aspects of medical management include encouraging aggressive hydration and avoidance of activities that may cause excessive perspiration or hyperventilation. NEJM 2009; 360:
39 Surgical vs. Medical Management Although more work needs to be done to answer this question definitively, a metaanalysis performed in 2005 indicated that the estimated rate of symptomatic progression in patients who have had surgery for moyamoya is 2.6% (1156 patients). That same year, a paper reported that the rate of disease progression with medical management alone is high. Childs Nerv Syst 2005; 21:
40 Surgical vs. Medical Management Up to 2/3 of patients with moyamoya will have symptomatic disease progression over a 5 year period In the majority of patients, even asymptomatic ones, moyamoya will progress without intervention. The current evidence indicates that while there is real risk to surgery, patients who have undergone surgical procedures to correct cerebral blood flow issues for moyamoya will have a much lower rate of symptomatic disease progression. Further, anecdotal evidence would indicate that this improvement is long lasting (at least for decades). Neurosurg 1997; 99: Suppl 2: S11-S18.
41 SURGICAL APPROACHES
42 What is involved with pial synangiosis? Please select the single best answer. A. Ligation of the superficial temporal artery and anastomosis to the ICA B. A direct surgical approach that involves EC-IC bypass C. An indirect surgical approach approximating a target EC branch to the surface of the brain D. Suturing a target vessel on to the dura. E. A, B and C F. A and C G. All of the above
43 Sorry I disagree Try again
44 CORRECT!!
45 Surgical Approaches Broadly speaking, surgical approaches to treatment of moyamoya disease can be divided into direct and indirect approaches. There is no clear cut superior approach and a variety of centers have their own biases for why they prefer one over the other. Surgical treatment generally utilizes the external carotid to provide a new source of blood flow to the affected hemisphere A complete discussion of the relative merits of direct and indirect approaches is beyond the scope of this presentation. There is a volume of literature addressing this controversy that interested readers should pursue. Please see the SNACC bibliography for moyamoya disease. Mayo Clin Proc 1994; 69:
46 Direct Surgical Approaches With direct approaches, a branch of the external carotid (often the superficial temporal artery) is directly anastomosed to a cortical artery. This is also called an EC-IC bypass. Historically, the direct approach has been more common in adults where an immediate increase in cerebral blood flow is crucial. Direct techniques can be difficult in children because of the small size of the vessels involved. NEJM 2009; 360:
47 Indirect Surgical Approaches Indirect approaches involve the placement of vascularized tissue (such as the temporalis muscle or the superficial temporal artery, supplied by the EC) in direct contact with the brain which leads to ingrowth of new vessels that ultimately will provide increased CBF to the affected hemisphere. Skull Base 2005; 15:
48 Indirect Surgical Approach The indirect approach takes advantage of the fact that chronically ischemic cortical tissue expresses a variety of angiogenic factors including metalloproteinases, transforming growth factor β-1 and vascular endothelial growth factor. These factors will encourage angiogenesis when there is a source of blood flow in close proximity NEJM 2009; 360:
49 Indirect Surgical Approach Indirect approaches include encephaloduroarteriosynangiosis, encephalomyoarteriosynangiosis, drilling of burr holes, pial synagiosis A report of 143 patients treated with pial synangiosis showed significant reduction of stroke after the surgical procedure 67% of patients had strokes preoperatively, 7.7% had strokes in the perioperative periods and only 3.2% had strokes at at least one year follow-up The long term risk of stroke appears to be about 4% as measured in a group of patients with at least 5 year followup Skull Base 2005; 15:
50 Pial Synangiosis The pial synangiosis procedure consists of Identification and mapping of the target vessel (often the STA) Dissection and skeletonization of the target vessel Opening a craniotomy under the vessel Opening the dura in a stellate fashion Opening the arachnoid Suturing the target vessel to the pia mater Closing Pediatr Neurosurg 1995; 23: J. Neurosurg: Pediatrics 2004; 100:

51 STA Dissection This photograph shows the target vessel dissected out with the dura open underneath. Note the stellate fashion of dural opening which is designed to provide more area of dural edge to help further encourage vessel ingrowth.

52 STA-Pia Mater Attachment In this photograph, the target vessel is being sutured to the pia mater.
53 INTRAOPERATIVE ANESTHETIC MANAGEMENT
54 Which of the following would be useful monitors for assessing adequacy of cerebral blood flow? Please select the single best answer. A. Invasive blood pressure B. EEG C. ET CO2 D. All of the above
55 Sorry I disagree Try again
56 CORRECT!!
57 Monitoring During Revascularization The most important aspect of a safe anesthetic in these patients is maintenance of adequate cerebral blood flow. A variety of methods can help estimate the adequacy of CBF including ETCO 2, invasive blood pressure monitoring and EEG.
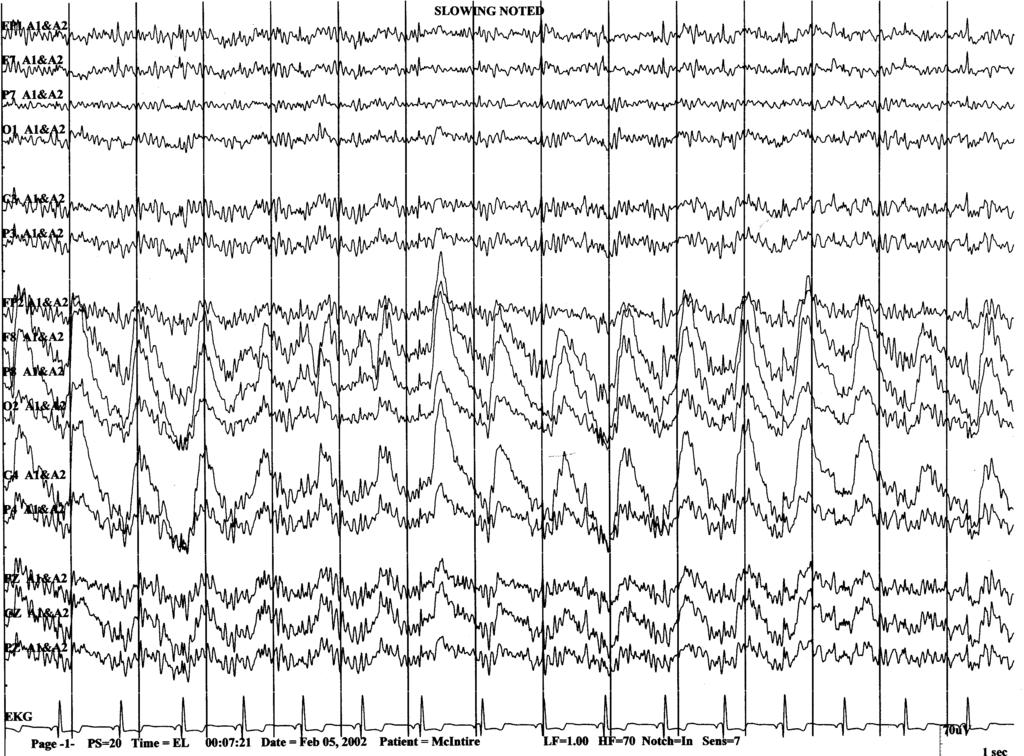

58 Intraoperative Electroencephalography
59 Intraoperative EEG Monitoring It is difficult to obtain a practical direct measurement of cerebral blood flow intraoperatively. MAP and ETCO 2 are surrogates for CBF and cerebral perfusion in the setting of intact autoregulation. Moyamoya patients may have some degree of autoregulation, but the limits would appear to be much narrower than patients with normal brains.
60 Intraoperative EEG Monitoring Much experience with intraoperative EEG for monitoring for cerebral ischemia during carotid surgery (CEA) Slowing on EEG has been associated with acute changes in CBF (i.e. hyperventilation) in pts with moyamoya Arch Neurol 1979; 36:
61 EEG Monitored by EEG tech from neurology Concerned about slowing Can indicate decrease in CBF and parenchyma at risk of ischemia Interventions Will depend on milieu of situation May involve adjusting ventilation or interventions to attempt to normalize systemic BP to improve CBF Propofol decreases CMRO 2 Neurosurg Clin North Am 1996; 7:
62 EEG Monitoring A 2011 retrospective study looked at one hospital s experience with EEG monitoring during pial synangiosis, total of 220 patients. Slowing occurred in 100 cases Correlated with specific operative manipulations Suturing vessel to pia Closure of craniotomy Generally occurred bilaterally, independent of side of intervention Pediatr Neurol 2011; 44:
63 Anesthetic Approach This procedure will invariably be performed under general anesthesia. The patients should be admitted to the hospital the night before surgery for preoperative hydration with 1.5x maintenance fluids until they go into the OR. This minimizes the hypotensive effects of the vasodilatory agents we utilize. The morning of surgery, the patients have a modified array EEG placed in the preoperative area if they are old enough to tolerate it when awake. In very young patients, EEG leads are placed after induction of anesthesia. Anesth Analg 1993; 77:
64 Anesthetic Approach Patients may be premedicated with IV midazolam and brought to the OR. A baseline EEG obtained and monitored prior to IV induction. General anesthesia may be maintained with a combination of an opioid infusion (fentanyl, sufentanil, or remifentanil) and inhaled agent. The cocktail of drugs is really a matter of semantics. Practitioners must simply be aware of the pitfalls of maneuvers that decrease CBF and plan accordingly. The patients are placed in head pins or a gel head ring (at the surgeon s discretion).
65 Anesthetic Approach It is appropriate to be aggressive with fluids, which is somewhat the opposite of classic fluid management approaches taught for intracranial surgery. The most severely affected side is generally operated upon first. If everything has been stable and there are no concerns, it is fine to proceed to the second side in order to accomplish synangiosis bilaterally in a single anesthetic.
66 Anesthetic Approach If slowing occurs, it is imperative to immediately ensure that cerebral blood flow is optimized. Ensure the patient s ventilation is appropriate and inadvertant hyperventilation (even very mild) has not occurred. Optimize blood pressure. This may require fluid bolus or use of vasoactive agents. If these maneuvers fail, small ( mg/kg) doses of propofol may help alleviate the slowing without decreasing blood pressure. Electroencephalography and Clinical Neurophysiology 1980; 49:
67 Anesthetic Approach Care must be taken on awakening to ensure a lucid patient that can follow commands while still having adequate pain control. Early and frequent neurologic exams are crucial in this patient population Anesth Analg 1997; 85;
68 POSTOPERATIVE CARE
69 Postoperative Period Is the patient cured at the end of the procedure if things have gone well? Yes No
70 Sorry I disagree Try again
71 CORRECT!!
72 Postoperative Care After an indirect surgical approach, the patient is fundamentally the same as they were preoperatively. However, because of the surgery, they are now set up for success. Vessel ingrowth can take months to accomplish so the same concerns of aggressively maintaining adequate cerebral blood flow apply in the immediate postoperative period.
73 Postoperative Care These patients should go to the ICU postoperatively for close neuromonitoring. Pain control and aggressive treatment of postoperative vomiting is crucial. There are reports of children stroking and dying in the immediate postoperative period from excessive crying due to poor pain control. Journal of Neurosurgical Anesthesiology 1998; 10:
74 The following three slides illustrate this concept
75 This is the preoperative relationship of vessels, bone and cortex.

76 The only change in the immediate postoperative period is the vessel has been sutured to the pia. The brain does not have any new source of cortical blood flow, yet.
77 This picture illustrates the ingrowth of new vessels as a result of the angiogenic factors in the CSF encouraging angiogenesis due to proximity of the target vessel.
Anaesthesia recommendations for patients suffering from. Moyamoya disease
 orphananesthesia Anaesthesia recommendations for patients suffering from Disease name: Moyamoya disease ICD 10: I67.5 Moyamoya disease Synonyms: Moyamoya means something hazy, like a puff of cigarette
orphananesthesia Anaesthesia recommendations for patients suffering from Disease name: Moyamoya disease ICD 10: I67.5 Moyamoya disease Synonyms: Moyamoya means something hazy, like a puff of cigarette
INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU
 CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
Neurosurg Focus 5 (5):Article 4, 1998
:Article 4, 1998") Neurosurg Focus 5 (5):Article 4, 1998 Multiple combined indirect procedure for the surgical treatment of children with moyamoya disease. A comparison with single indirect anastomosis with direct anastomosis
Neurosurg Focus 5 (5):Article 4, 1998 Multiple combined indirect procedure for the surgical treatment of children with moyamoya disease. A comparison with single indirect anastomosis with direct anastomosis
Moyamoya. Moyamoya Disease Double Trouble. Epidemiology 1/16/2015
 Moyamoya Moyamoya Disease Double Trouble Jan Boerke, ACNP AACN Brunch January 24, 2015 Moyamoya - puff of smoke in Japanese Describes the look of the tangle of tiny vessels formed to compensate for the
Moyamoya Moyamoya Disease Double Trouble Jan Boerke, ACNP AACN Brunch January 24, 2015 Moyamoya - puff of smoke in Japanese Describes the look of the tangle of tiny vessels formed to compensate for the
Overview Blood supply of the brain What is moyamoya disease? > 1
 Moyamoya Disease Overview Moyamoya disease is caused by blocked arteries at the base of the brain. The name "moyamoya" means "puff of smoke" in Japanese and describes the appearance of tiny vessels that
Moyamoya Disease Overview Moyamoya disease is caused by blocked arteries at the base of the brain. The name "moyamoya" means "puff of smoke" in Japanese and describes the appearance of tiny vessels that
Moyamoya syndrome associated with cocaine abuse Case report
 Neurosurg Focus 5 (5):Article 7, 1998 Moyamoya syndrome associated with cocaine abuse Case report Marc S. Schwartz, M.D., and R. Michael Scott, M.D. Division of Neurosurgery, Albany Medical College, Albany,
Neurosurg Focus 5 (5):Article 7, 1998 Moyamoya syndrome associated with cocaine abuse Case report Marc S. Schwartz, M.D., and R. Michael Scott, M.D. Division of Neurosurgery, Albany Medical College, Albany,
Moyamoya disease is a progressive cerebrovascular. Pial synangiosis in patients with moyamoya younger than 2 years of age.
 J Neurosurg Pediatrics 13:420 425, 2014 AANS, 2014 Pial synangiosis in patients with moyamoya younger than 2 years of age Clinical article Eric M. Jackson, M.D., Ning Lin, M.D., Sunil Manjila, M.D., R.
J Neurosurg Pediatrics 13:420 425, 2014 AANS, 2014 Pial synangiosis in patients with moyamoya younger than 2 years of age Clinical article Eric M. Jackson, M.D., Ning Lin, M.D., Sunil Manjila, M.D., R.
History of revascularization
 History of revascularization Author (year) Kredel, 1942 Woringer& Kunlin, 1963 Donaghy& Yasargil, 1968 Loughheed 1971 Kikuchini & Karasawa1973 Karasawa, 1977 Story, 1978 Sundt, 1982 EC/IC bypass study
History of revascularization Author (year) Kredel, 1942 Woringer& Kunlin, 1963 Donaghy& Yasargil, 1968 Loughheed 1971 Kikuchini & Karasawa1973 Karasawa, 1977 Story, 1978 Sundt, 1982 EC/IC bypass study
This quiz is being published on behalf of the Education Committee of the SNACC.
 Quiz 48 Cerebrovascular Atherosclerotic Disease Shobana Rajan, M.D. Associate Director of Neuroanesthesia, Vice Chair of Education, Allegheny Health Network. Quiz team; Suneeta Gollapudy M.D, Angele Marie
Quiz 48 Cerebrovascular Atherosclerotic Disease Shobana Rajan, M.D. Associate Director of Neuroanesthesia, Vice Chair of Education, Allegheny Health Network. Quiz team; Suneeta Gollapudy M.D, Angele Marie
Neuro Quiz 29 Transcranial Doppler Monitoring
 Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
MOYA Moya disease is a rare idiopathic
 Research Papers Moya Moya Cases Treated with Encephaloduroarteriosynangiosis Parimal Tripathi, Varsha Tripathi, Ronak J. Naik and Jaimin M. Patel From Gujarat Cancer & Research Institute, Ahmedabad; Sterling
Research Papers Moya Moya Cases Treated with Encephaloduroarteriosynangiosis Parimal Tripathi, Varsha Tripathi, Ronak J. Naik and Jaimin M. Patel From Gujarat Cancer & Research Institute, Ahmedabad; Sterling
Neurosurgical Treatment of Moyamoya Disease: Bypass Surgery for the Brain
 Neurosurgical Treatment of Moyamoya Disease: Bypass Surgery for the Brain Christopher Payne Currently, no medical treatment exists to prevent the progression of moyamoya disease, and neurosurgical treatment
Neurosurgical Treatment of Moyamoya Disease: Bypass Surgery for the Brain Christopher Payne Currently, no medical treatment exists to prevent the progression of moyamoya disease, and neurosurgical treatment
PTA 106 Unit 1 Lecture 3
 PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
Imaging of Moya Moya Disease
 Abstract Imaging of Moya Moya Disease Pages with reference to book, From 181 To 185 Rashid Ahmed, Hurnera Ahsan ( Liaquat National Hospital, Karachi. ) Moya Moya disease is a rare disease causing occlusion
Abstract Imaging of Moya Moya Disease Pages with reference to book, From 181 To 185 Rashid Ahmed, Hurnera Ahsan ( Liaquat National Hospital, Karachi. ) Moya Moya disease is a rare disease causing occlusion
Moyamoya disease in the midwestern United States
 Neurosurg Focus 5 (5):Article 1, 1998 Moyamoya disease in the midwestern United States Nicholas M. Wetjen, B.S., P. Charles Garell, M.D., Nicholas V. Stence, and Christopher M. Loftus, M.D. Division of
Neurosurg Focus 5 (5):Article 1, 1998 Moyamoya disease in the midwestern United States Nicholas M. Wetjen, B.S., P. Charles Garell, M.D., Nicholas V. Stence, and Christopher M. Loftus, M.D. Division of
Neuroscience. Journal. Moyamoya disease a review and case illustration. P A L M E T T O H E A L T H Vol. 2 Issue 3 Summer 2016
 Neuroscience P A L M E T T O H E A L T H Vol. 2 Issue 3 Summer 2016 Journal Moyamoya disease a review and case illustration pg. 5 Choroid Plexus Papilloma in adults pg. 8 As physician co-leaders of Palmetto
Neuroscience P A L M E T T O H E A L T H Vol. 2 Issue 3 Summer 2016 Journal Moyamoya disease a review and case illustration pg. 5 Choroid Plexus Papilloma in adults pg. 8 As physician co-leaders of Palmetto
Moyamoya Syndrome with contra lateral DACA aneurysm: First Case report with review of literature
 Romanian Neurosurgery Volume XXXI Number 3 2017 July-September Article Moyamoya Syndrome with contra lateral DACA aneurysm: First Case report with review of literature Ashish Kumar Dwivedi, Pradeep Kumar,
Romanian Neurosurgery Volume XXXI Number 3 2017 July-September Article Moyamoya Syndrome with contra lateral DACA aneurysm: First Case report with review of literature Ashish Kumar Dwivedi, Pradeep Kumar,
Direct Bypass Techniques for the Treatment of Pediatric Moyamoya Disease
 Direct Bypass Techniques for the Treatment of Pediatric Moyamoya Disease Raphael Guzman, MD a, Gary K. Steinberg, MD, PhD b, * KEYWORDS Moyamoya disease Pediatric Direct bypass INDICATIONS Moyamoya disease
Direct Bypass Techniques for the Treatment of Pediatric Moyamoya Disease Raphael Guzman, MD a, Gary K. Steinberg, MD, PhD b, * KEYWORDS Moyamoya disease Pediatric Direct bypass INDICATIONS Moyamoya disease
A CASE OF RECURRENT ALTERNATING TRANSIENT HEMIPARESIS Dr. Shunmuga Arumugasamy.S DNB Resident Railway Hospital, Perambur.
 A CASE OF RECURRENT ALTERNATING TRANSIENT HEMIPARESIS Dr. Shunmuga Arumugasamy.S DNB Resident Railway Hospital, Perambur. 6 year old school going child. Apparently normal till 3 yrs when she developed
A CASE OF RECURRENT ALTERNATING TRANSIENT HEMIPARESIS Dr. Shunmuga Arumugasamy.S DNB Resident Railway Hospital, Perambur. 6 year old school going child. Apparently normal till 3 yrs when she developed
Extracranial-to-Intracranial Bypass Using Radial Artery Grafting for Complex Skull Base Tumors: Technical Note
 Extracranial-to-Intracranial Bypass Using Radial Artery Grafting for Complex Skull Base Tumors: Technical Note Saleem I. Abdulrauf, M.D., F.A.C.S. 1 ABSTRACT The management of complex skull base tumors
Extracranial-to-Intracranial Bypass Using Radial Artery Grafting for Complex Skull Base Tumors: Technical Note Saleem I. Abdulrauf, M.D., F.A.C.S. 1 ABSTRACT The management of complex skull base tumors
Carotid Artery Stenting
 Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Disclosures. CREST Trial: Summary. Lecture Outline 4/16/2015. Cervical Atherosclerotic Disease
 Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Recent Advances in Neurology Difficult Cases
 Patient X: History Part 1 Recent Advances in Neurology Difficult Cases Heather J. Fullerton, MD, MAS Professor of Neurology & Pediatrics Director, Pediatric Brain Center Previously healthy 14-year old
Patient X: History Part 1 Recent Advances in Neurology Difficult Cases Heather J. Fullerton, MD, MAS Professor of Neurology & Pediatrics Director, Pediatric Brain Center Previously healthy 14-year old
Moyamoya disease: An unusual presentation of stroke. Sheena Chew, HMS III Dr. Gillian Lieberman. Image from
 Moyamoya disease: An unusual presentation of stroke Sheena Chew, HMS III Dr. Gillian Lieberman Image from http://www.sensitivelight.com/smoke2/ Agenda 1. Index patient: we will follow a patient with an
Moyamoya disease: An unusual presentation of stroke Sheena Chew, HMS III Dr. Gillian Lieberman Image from http://www.sensitivelight.com/smoke2/ Agenda 1. Index patient: we will follow a patient with an
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery
 2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
Extracranial to intracranial bypass for intracranial atherosclerosis
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Extracranial to intracranial bypass for intracranial atherosclerosis In cerebrovascular disease, blood vessels
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Extracranial to intracranial bypass for intracranial atherosclerosis In cerebrovascular disease, blood vessels
Intracranial vascular anastomosis using the microanastomotic system
 J Neurosurg 89:676 681, 1998 Intracranial vascular anastomosis using the microanastomotic system Technical note DAVID W. NEWELL, M.D., ANDREW T. DAILEY, M.D., AND STEPHEN L. SKIRBOLL, M.D. Department of
J Neurosurg 89:676 681, 1998 Intracranial vascular anastomosis using the microanastomotic system Technical note DAVID W. NEWELL, M.D., ANDREW T. DAILEY, M.D., AND STEPHEN L. SKIRBOLL, M.D. Department of
5. COMMON APPROACHES. Each of the described approaches is also demonstrated on supplementary videos, please see Appendix 2.
 5. COMMON APPROACHES Each of the described approaches is also demonstrated on supplementary videos, please see Appendix 2. 5.1. LATERAL SUPRAORBITAL APPROACH The most common craniotomy approach used in
5. COMMON APPROACHES Each of the described approaches is also demonstrated on supplementary videos, please see Appendix 2. 5.1. LATERAL SUPRAORBITAL APPROACH The most common craniotomy approach used in
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Double STA-MCA Anatomosis for Bilateral Carotid Occlusion
 Double STA-MCA Anatomosis for Bilateral Carotid Occlusion -Case Report and Literature Review- Sandra vuignier 1, Kenji Kanamaru 2, Tomohiro Araki 2 1 Department of Neurosurgery, Nagoya University School
Double STA-MCA Anatomosis for Bilateral Carotid Occlusion -Case Report and Literature Review- Sandra vuignier 1, Kenji Kanamaru 2, Tomohiro Araki 2 1 Department of Neurosurgery, Nagoya University School
Title. CitationWorld Neurosurgery, 80(5): Issue Date Doc URL. Rights. Rights(URL)
: Issue Date Doc URL. Rights. Rights(URL)") Title Effective Surgical Revascularization Improves Cerebr Moyamoya Disease Kawabori, Masahito; Kuroda, Satoshi; Nakayama, Naoki Author(s) Nagara CitationWorld Neurosurgery, 80(5): 612-619 Issue Date 2013-11
Title Effective Surgical Revascularization Improves Cerebr Moyamoya Disease Kawabori, Masahito; Kuroda, Satoshi; Nakayama, Naoki Author(s) Nagara CitationWorld Neurosurgery, 80(5): 612-619 Issue Date 2013-11
CEA and cerebral protection Volodymyr labinskyy, MD
 CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None
CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None
7/18/2018. Cerebral Vasospasm: Current and Emerging Therapies. Disclosures. Objectives
 Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
GUIDELINE FOR RECOVERY ROOM MANAGEMENT OF PATIENTS AFTER CAROTID ENDARTERECTOMY
 GUIDELINE FOR RECOVERY ROOM MANAGEMENT OF PATIENTS AFTER CAROTID ENDARTERECTOMY Full Title of Guideline: Author (include email and role): Guideline for Recovery Room Management of Patients after Carotid
GUIDELINE FOR RECOVERY ROOM MANAGEMENT OF PATIENTS AFTER CAROTID ENDARTERECTOMY Full Title of Guideline: Author (include email and role): Guideline for Recovery Room Management of Patients after Carotid
Slide 1. Slide 2 Conflict of Interest Disclosure. Slide 3 Stroke Facts. The Treatment of Intracranial Stenosis. Disclosure
 Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Role of IONM in reducing the incidence and severity in pediatric patients with AIS
 Role of IONM in reducing the incidence and severity in pediatric patients with AIS Mohamed Nassef M.D PGY 2 ANESTHESIA McMaster University DEC 9, 2015 Objectives: Literature Review on neurological complications
Role of IONM in reducing the incidence and severity in pediatric patients with AIS Mohamed Nassef M.D PGY 2 ANESTHESIA McMaster University DEC 9, 2015 Objectives: Literature Review on neurological complications
Anesthetic Techniques in Endoscopic Sinus and Skull Base Surgery
 Anesthetic Techniques in Endoscopic Sinus and Skull Base Surgery Martha Cordoba Amorocho, MD Iuliu Fat, MD Supplement to Cordoba Amorocho M, Fat I. Anesthetic techniques in endoscopic sinus and skull base
Anesthetic Techniques in Endoscopic Sinus and Skull Base Surgery Martha Cordoba Amorocho, MD Iuliu Fat, MD Supplement to Cordoba Amorocho M, Fat I. Anesthetic techniques in endoscopic sinus and skull base
In patients with moyamoya the clinical significance of. Preoperative transdural collateral vessels in moyamoya as radiographic biomarkers of disease
 CLINICAL ARTICLE J Neurosurg Pediatr 19:289 295, 2017 Preoperative transdural collateral vessels in moyamoya as radiographic biomarkers of disease Armide Storey, BS, 1 R. Michael Scott, MD, 1 Richard Robertson,
CLINICAL ARTICLE J Neurosurg Pediatr 19:289 295, 2017 Preoperative transdural collateral vessels in moyamoya as radiographic biomarkers of disease Armide Storey, BS, 1 R. Michael Scott, MD, 1 Richard Robertson,
Spasm of the extracranial internal carotid artery resulting from blunt trauma demonstrated by angiography
 Spasm of the extracranial internal carotid artery resulting from blunt trauma demonstrated by angiography Case report ELISHA S. GURDJIAN, M.D., BLAISE AUDET, M.D., RENATO W. SIBAYAN, M.D., AND LLYWELLYN
Spasm of the extracranial internal carotid artery resulting from blunt trauma demonstrated by angiography Case report ELISHA S. GURDJIAN, M.D., BLAISE AUDET, M.D., RENATO W. SIBAYAN, M.D., AND LLYWELLYN
Emergency EC-IC bypass for symptomatic atherosclerotic ischemic stroke
 Emergency EC-IC bypass for symptomatic atherosclerotic ischemic stroke Tetsuyoshi Horiuchi, Junpei Nitta, Shigetoshi Ishizaka, Kohei Kanaya, Takao Yanagawa, and Kazuhiro Hongo. Department of Neurosurgery,
Emergency EC-IC bypass for symptomatic atherosclerotic ischemic stroke Tetsuyoshi Horiuchi, Junpei Nitta, Shigetoshi Ishizaka, Kohei Kanaya, Takao Yanagawa, and Kazuhiro Hongo. Department of Neurosurgery,
IOM at University of. Training for physicians. art of IOM. neurologic. injury during surgery. surgery on by IOM. that rate is.
 Topics covered: Overview of science and art of IOM IOM at University of Michigan Hospital and Health Systems What is the purpose of Intraoperative monitoring? Training for physicians Overview of science
Topics covered: Overview of science and art of IOM IOM at University of Michigan Hospital and Health Systems What is the purpose of Intraoperative monitoring? Training for physicians Overview of science
Longitudinal anterior-to-posterior shift of collateral channels in patients with moyamoya disease: an implication for its hemorrhagic onset
 CLINICAL ARTICLE Longitudinal anterior-to-posterior shift of collateral channels in patients with moyamoya disease: an implication for its hemorrhagic onset Shusuke Yamamoto, MD, Satoshi Hori, MD, PhD,
CLINICAL ARTICLE Longitudinal anterior-to-posterior shift of collateral channels in patients with moyamoya disease: an implication for its hemorrhagic onset Shusuke Yamamoto, MD, Satoshi Hori, MD, PhD,
Moyamoya disease (MMD), an idiopathic disease. Direct versus indirect revascularization in the treatment of moyamoya disease
, an idiopathic disease. Direct versus indirect revascularization in the treatment of moyamoya disease") CLINICAL ARTICLE J Neurosurg 129:480 489, 2018 Direct versus indirect revascularization in the treatment of moyamoya disease *Seong-eun Park, BSc, Ju-seong Kim, MD, Eun Kyung Park, MD, Kyu-Won Shim, MD,
CLINICAL ARTICLE J Neurosurg 129:480 489, 2018 Direct versus indirect revascularization in the treatment of moyamoya disease *Seong-eun Park, BSc, Ju-seong Kim, MD, Eun Kyung Park, MD, Kyu-Won Shim, MD,
11/6/2013. Vanderbilt University Institute of Imaging Science (VUIIS) 7 Tesla Vascular Imaging. Evaluating stroke risk
 7 Tesla Vascular Imaging. Evaluating stroke risk") Vanderbilt University Institute of Imaging Science (VUIIS) New MI Techniques for Imaging Cerebrovascular Disease Manus J. Donahue Depts. of adiology, Physics, Neurology and Physics Vanderbilt University
Vanderbilt University Institute of Imaging Science (VUIIS) New MI Techniques for Imaging Cerebrovascular Disease Manus J. Donahue Depts. of adiology, Physics, Neurology and Physics Vanderbilt University
Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage
 Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Managing Hypertension in the Perioperative Arena
 Managing Hypertension in the Perioperative Arena Optimizing Perioperative Management Strategies for Hypertension in the Cardiac Surgical Patient Objectives: Treatment of hypertensive emergencies. ALBERT
Managing Hypertension in the Perioperative Arena Optimizing Perioperative Management Strategies for Hypertension in the Cardiac Surgical Patient Objectives: Treatment of hypertensive emergencies. ALBERT
NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES
 NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section
NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section
Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS
 Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS 11-8-18 Outline 1. Background 2. Anatomy of patent foramen ovale (PFO) 3. Relationship between PFO and
Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS 11-8-18 Outline 1. Background 2. Anatomy of patent foramen ovale (PFO) 3. Relationship between PFO and
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Lecture Outline: 1/5/14
 John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
Head Trauma Inservice (October)
") John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
9/18/16. Setting: Community ED, 30k admissions per year Time: Friday night, 11pm. CC: Syncope
 William A. Knight IV MD, FACEP Associate Professor Emergency Medicine & Neurosurgery University of Cincinnati September 21, 2016 (William.knight@uc.edu) ED as the Front Door Spectrum of care with Endovascular
William A. Knight IV MD, FACEP Associate Professor Emergency Medicine & Neurosurgery University of Cincinnati September 21, 2016 (William.knight@uc.edu) ED as the Front Door Spectrum of care with Endovascular
Blunt Carotid Injury- CT Angiography is Adequate For Screening. Kelly Knudson, M.D. UCHSC April 3, 2006
 Blunt Carotid Injury- CT Angiography is Adequate For Screening Kelly Knudson, M.D. UCHSC April 3, 2006 CT Angiography vs Digital Subtraction Angiography Blunt carotid injury screening is one of the very
Blunt Carotid Injury- CT Angiography is Adequate For Screening Kelly Knudson, M.D. UCHSC April 3, 2006 CT Angiography vs Digital Subtraction Angiography Blunt carotid injury screening is one of the very
SURGICAL MANAGEMENT OF MOYAMOYA DISEASE- RETROSPECTIVE ANALYSIS OF A SINGLE INSTITUTION SERIES
 SURGICAL MANAGEMENT OF MOYAMOYA DISEASE- RETROSPECTIVE ANALYSIS OF A SINGLE INSTITUTION SERIES Submitted for M.Ch Neurosurgery By Dr. Ranjit Devidas Rangnekar October 2016 Department of Neurosurgery Sree
SURGICAL MANAGEMENT OF MOYAMOYA DISEASE- RETROSPECTIVE ANALYSIS OF A SINGLE INSTITUTION SERIES Submitted for M.Ch Neurosurgery By Dr. Ranjit Devidas Rangnekar October 2016 Department of Neurosurgery Sree
Moyamoya disease. Critical Role of PDGFR-α in Angiogenesis through Indirect Bypass in Mouse Model of Moyamoya Disease.
 FPⅢ- Critical Role of PDGFR-α in Angiogenesis through Indirect Bypass in Mouse Model of Moyamoya Disease Tomohide Hayashi Departments of Neurosurgery, University of Toyama Background - is a unique cerebrovascular
FPⅢ- Critical Role of PDGFR-α in Angiogenesis through Indirect Bypass in Mouse Model of Moyamoya Disease Tomohide Hayashi Departments of Neurosurgery, University of Toyama Background - is a unique cerebrovascular
TABLES. Table 1 Terminal vessel aneurysms. Table. Aneurysm location. Bypass flow** Symptoms Strategy Bypass recipient. Age/ Sex.
 Table TABLES Table 1 Terminal vessel aneurysms Age/ Sex Aneurysm location Symptoms Strategy Bypass recipient Recipient territory Recipient territory flow* Cut flow Bypass flow** Graft Patent postop F/U
Table TABLES Table 1 Terminal vessel aneurysms Age/ Sex Aneurysm location Symptoms Strategy Bypass recipient Recipient territory Recipient territory flow* Cut flow Bypass flow** Graft Patent postop F/U
Dural Arteriovenous Malformations and Fistulae (DAVM S DAVF S)
") Jorge Guedes Campos NEUROIMAGING DEPARTMENT HOSPITAL SANTA MARIA UNIVERSITY OF LISBON PORTUGAL DEFINITION region of arteriovenous shunting confined to a leaflet of packymeninges often adjacent to a major
Jorge Guedes Campos NEUROIMAGING DEPARTMENT HOSPITAL SANTA MARIA UNIVERSITY OF LISBON PORTUGAL DEFINITION region of arteriovenous shunting confined to a leaflet of packymeninges often adjacent to a major
Moyamoya Disease A Vasculopathy and an Uncommon Cause of Recurrent Cerebrovascular Accidents
 Moyamoya Disease A Vasculopathy and an Uncommon Cause of Recurrent Cerebrovascular Accidents Yasmin S. Hamirani, Md 1 *, Mohammad Valikhani, Md 2, Allison Sweney, Ms Iii 2, Hafsa Khan, Md 2, Mohammad Pathan,
Moyamoya Disease A Vasculopathy and an Uncommon Cause of Recurrent Cerebrovascular Accidents Yasmin S. Hamirani, Md 1 *, Mohammad Valikhani, Md 2, Allison Sweney, Ms Iii 2, Hafsa Khan, Md 2, Mohammad Pathan,
Internal Carotid Artery Dissection
 May 2011 Internal Carotid Artery Dissection Carolyn April, HMS IV Agenda Presentation of a clinical case Discussion of the clinical features of ICA dissection Discussion of the imaging modalities used
May 2011 Internal Carotid Artery Dissection Carolyn April, HMS IV Agenda Presentation of a clinical case Discussion of the clinical features of ICA dissection Discussion of the imaging modalities used
Carotid Stenosis 1/24/2019. Review of Primary Studies. NASCET- Moderate stenosis. ACAS (Asymptomatic Carotid Atherosclerosis Study) NASCET
 NASCET") Review of Primary Studies Carotid Stenosis NINDS National Institute of Neurological Disorders and Stroke 2 large studies to determine who would benefit from surgery NASCET North American Symptomatic Carotid
Review of Primary Studies Carotid Stenosis NINDS National Institute of Neurological Disorders and Stroke 2 large studies to determine who would benefit from surgery NASCET North American Symptomatic Carotid
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Management of Traumatic Brain Injury (and other neurosurgical emergencies)
") Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Management of cervicocephalic arterial dissection. Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery
 Management of cervicocephalic arterial dissection Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery Definition Disruption of arterial wall, either at level of intima-media
Management of cervicocephalic arterial dissection Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery Definition Disruption of arterial wall, either at level of intima-media
Summary of some of the landmark articles:
 Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Intracranial-to-intracranial vascular anastomosis created using a microanastomotic device for the treatment of distal middle cerebral artery aneurysms
 J Neurosurg 97:486 491, 2002 Intracranial-to-intracranial vascular anastomosis created using a microanastomotic device for the treatment of distal middle cerebral artery aneurysms Technical note DAVID
J Neurosurg 97:486 491, 2002 Intracranial-to-intracranial vascular anastomosis created using a microanastomotic device for the treatment of distal middle cerebral artery aneurysms Technical note DAVID
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Alessandro Della Puppa
 Intraoperative measurement of arterial blood flow in complex cerebral aneurysms surgery Studio flussimetrico intra-operatorio nel clipping degli aneurismi complessi Alessandro Della Puppa NEUROSURGERY
Intraoperative measurement of arterial blood flow in complex cerebral aneurysms surgery Studio flussimetrico intra-operatorio nel clipping degli aneurismi complessi Alessandro Della Puppa NEUROSURGERY
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Interventions in the Management of Acute Stroke. Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital
 Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Title. Author(s) 黒田, 敏 ; 川堀, 真人 ; 宮本, 倫行 ; 笹森, 徹 ; 遠藤, 将吾 ; 中山, 若樹 ; 石川, 達哉. Citation 脳卒中の外科, 37(5): Issue Date Doc URL.
 黒田, 敏 ; 川堀, 真人 ; 宮本, 倫行 ; 笹森, 徹 ; 遠藤, 将吾 ; 中山, 若樹 ; 石川, 達哉. Citation 脳卒中の外科, 37(5): Issue Date Doc URL.") Title 側頭葉から後頭葉にかけて高度の虚血を有するもやもや病に対する脳血行再建術 Author(s) 黒田, 敏 ; 川堀, 真人 ; 宮本, 倫行 ; 笹森, 徹 ; 遠藤, 将吾 ; 中山, 若樹 ; 石川, 達哉 Citation 脳卒中の外科, 37(5): 345-349 Issue Date 2009 Doc URL http://hdl.handle.net/2115/70929
Title 側頭葉から後頭葉にかけて高度の虚血を有するもやもや病に対する脳血行再建術 Author(s) 黒田, 敏 ; 川堀, 真人 ; 宮本, 倫行 ; 笹森, 徹 ; 遠藤, 将吾 ; 中山, 若樹 ; 石川, 達哉 Citation 脳卒中の外科, 37(5): 345-349 Issue Date 2009 Doc URL http://hdl.handle.net/2115/70929
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion
 Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Spontaneous Recanalization after Complete Occlusion of the Common Carotid Artery with Subsequent Embolic Ischemic Stroke
 Original Contribution Spontaneous Recanalization after Complete Occlusion of the Common Carotid Artery with Subsequent Embolic Ischemic Stroke Abstract Introduction: Acute carotid artery occlusion carries
Original Contribution Spontaneous Recanalization after Complete Occlusion of the Common Carotid Artery with Subsequent Embolic Ischemic Stroke Abstract Introduction: Acute carotid artery occlusion carries
Occlusive cerebrovascular disease. A Novel Chronic Cerebral Hypoperfusion Model with Cognitive Impairment and Low Mortality Rate in Rats
 FPⅧ-1 A Novel Chronic Cerebral Hypoperfusion Model with Cognitive Impairment and Low Mortality Rate in Rats Ahmed Said Mansour 1, Kuniyasu Niizuma 2, Sherif Rashad 2, Hidenori Endo 2, Toshiki Endo 3, Kenichi
FPⅧ-1 A Novel Chronic Cerebral Hypoperfusion Model with Cognitive Impairment and Low Mortality Rate in Rats Ahmed Said Mansour 1, Kuniyasu Niizuma 2, Sherif Rashad 2, Hidenori Endo 2, Toshiki Endo 3, Kenichi
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
Marc Norman, Ph.D. - Do Not Use without Permission 1. Cerebrovascular Accidents. Marc Norman, Ph.D. Department of Psychiatry
 Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cerebral Bypass Surgery
 Cerebral Bypass Surgery Overview Cerebral bypass surgery is performed to restore, or revascularize, blood flow to the brain. A cerebral bypass is the brain's equivalent of a coronary bypass in the heart.
Cerebral Bypass Surgery Overview Cerebral bypass surgery is performed to restore, or revascularize, blood flow to the brain. A cerebral bypass is the brain's equivalent of a coronary bypass in the heart.
Quality Metrics. Stroke Related Procedure Outcomes
 Quality Metrics Stroke Related Procedure Outcomes Below is a description of some of the stroke-related procedures performed at St. Dominic Hospital in Jackson, with quality information on the complication
Quality Metrics Stroke Related Procedure Outcomes Below is a description of some of the stroke-related procedures performed at St. Dominic Hospital in Jackson, with quality information on the complication
2/7/
 Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Anastomosis of the superficial temporal artery to the distal anterior cerebral artery with interposed cephalic vein graft
 J Neurosurg 58~25-429, 1983 Anastomosis of the superficial temporal artery to the distal anterior cerebral artery with interposed cephalic vein graft Case report RYOJI ISHII, M.D., TETSUO KOIKE, M.D.,
J Neurosurg 58~25-429, 1983 Anastomosis of the superficial temporal artery to the distal anterior cerebral artery with interposed cephalic vein graft Case report RYOJI ISHII, M.D., TETSUO KOIKE, M.D.,
Carotid Artery Stenting (CAS) Pathophysiology. Technical Considerations. Plaque characteristics: relevant concepts. CAS and CEA
 Pathophysiology. Technical Considerations. Plaque characteristics: relevant concepts. CAS and CEA") Carotid Artery Stenting (CAS) Carotid Artery Stenting for Stroke Risk Reduction Matthew A. Corriere MD, MS, RPVI Assistant Professor of Surgery Department of Vascular and Endovascular Surgery Rationale:
Carotid Artery Stenting (CAS) Carotid Artery Stenting for Stroke Risk Reduction Matthew A. Corriere MD, MS, RPVI Assistant Professor of Surgery Department of Vascular and Endovascular Surgery Rationale:
Identifying Cerebrovascular Disorders. Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine
 Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
TCD in Subclavian Steal Syndrome
 ISSN 2005-7881 Journal of Neurosonology 2(Suppl. 1):25-30, 2010 TCD in Subclavian Steal Syndrome Soon-Tae Lee, M.D., Ph.D. Department of Neurology, Seoul National University Hospital, Seoul, South Korea
ISSN 2005-7881 Journal of Neurosonology 2(Suppl. 1):25-30, 2010 TCD in Subclavian Steal Syndrome Soon-Tae Lee, M.D., Ph.D. Department of Neurology, Seoul National University Hospital, Seoul, South Korea
Blood Supply. Allen Chung, class of 2013
 Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio
 Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
TCD AND VASOSPASM SAH
 CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
TCD IN THE NICU, PICU AND OTHER APPLICATIONS. Dorothy Bulas M.D. Professor of Pediatrics & Radiology Children s National Washington D.C.
 TCD IN THE NICU, PICU AND OTHER APPLICATIONS Dorothy Bulas M.D. Professor of Pediatrics & Radiology Children s National Washington D.C. Objectives Recognize normal and abnormal cranial blood flow patterns
TCD IN THE NICU, PICU AND OTHER APPLICATIONS Dorothy Bulas M.D. Professor of Pediatrics & Radiology Children s National Washington D.C. Objectives Recognize normal and abnormal cranial blood flow patterns
Title in Children. Issue Date Copyright 2011 S. Karger AG, Base.
 NAOSITE: Nagasaki University's Ac Title Author(s) Clinical Features and Long-Term Fol in Children. Hayashi, Kentaro; Horie, Nobutaka; Citation Pediatric Neurosurgery, 47(1), pp.1 Issue Date 2011-09 URL
NAOSITE: Nagasaki University's Ac Title Author(s) Clinical Features and Long-Term Fol in Children. Hayashi, Kentaro; Horie, Nobutaka; Citation Pediatric Neurosurgery, 47(1), pp.1 Issue Date 2011-09 URL
Carotid artery stenting for long CTO and pseudo occlusion of carotid artery -2 case reports-
 Carotid artery stenting for long CTO and pseudo occlusion of carotid artery -2 case reports- Katsutoshi Takayama, MD, Ph.D Department of Radiology and Interventional Neuroradiology Ishinkai Yao General
Carotid artery stenting for long CTO and pseudo occlusion of carotid artery -2 case reports- Katsutoshi Takayama, MD, Ph.D Department of Radiology and Interventional Neuroradiology Ishinkai Yao General
CEREBRAL PHYSIOLOGY CEREBRAL PHYSIOLOGY REGULATION OF CBF REGULATION OF CBF REGULATION OF CBF. Cerebral Blood Flow (CBF)
") NEUROANESTHESIA: THE FAST-TRACK APPROACH Bruce Weiner, CRNA, MS Moffitt Cancer Center Tampa, FL LEARNER OUTCOMES Discuss the interaction between intracranial pathophysiology, cerebral perfusion and general
NEUROANESTHESIA: THE FAST-TRACK APPROACH Bruce Weiner, CRNA, MS Moffitt Cancer Center Tampa, FL LEARNER OUTCOMES Discuss the interaction between intracranial pathophysiology, cerebral perfusion and general
Moyamoya disease in children
 Childs Nerv Syst (2010) 26:1297 1308 DOI 10.1007/s00381-010-1209-8 SPECIAL ANNUAL ISSUE Moyamoya disease in children David M. Ibrahimi & Rafael J. Tamargo & Edward S. Ahn Received: 8 June 2010 /Accepted:
Childs Nerv Syst (2010) 26:1297 1308 DOI 10.1007/s00381-010-1209-8 SPECIAL ANNUAL ISSUE Moyamoya disease in children David M. Ibrahimi & Rafael J. Tamargo & Edward S. Ahn Received: 8 June 2010 /Accepted:
Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease
 2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
R Adams Cowley Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland.
 R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
Surgical techniques and procedures for cerebrovascular surgery. Surgery for the AVF at the cranio-cervical junction and high cervical spine
 VS-1 Surgery for the AVF at the cranio-cervical junction and high cervical spine Hiroyuki Kinouchi University of Yamanashi, Department of Neurosurgery Dural AVFs have been recognized as common type of
VS-1 Surgery for the AVF at the cranio-cervical junction and high cervical spine Hiroyuki Kinouchi University of Yamanashi, Department of Neurosurgery Dural AVFs have been recognized as common type of
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available