MANAGEMENT OF INTRACRANIAL. Moderator : Dr. A. Suri Dr. Deepak Agarwal Presented by: Dr Avijit Sarkari
|
|
|
- Logan Merritt
- 5 years ago
- Views:
Transcription

1 MANAGEMENT OF INTRACRANIAL ANEURYSMS Moderator : Dr. A. Suri Dr. Deepak Agarwal Presented by: Dr

2 Introduction Incidence of aneurysm difficult to estimate Prevalence % Half of the aneurysms ruptures The incidence of aneurysmal rupture is between 6 and 12 per 100, % present during childhood *van Gijn J, Rinkel GJ. Subarachnoid hemorrhage: diagnosis, causes and management. Brain 2001;124(Pt 2):
3 Introduction Overall mortality at 6 months: 40% - 50% 15% of patients expire before reaching the hospital 25% within 24 hours. Only one third of those who survive have functional independent lives. Hop JW, Rinkel GJ, Algra A, et al. Case-fatality rates and functional outcome after subarachnoid hemorrhage: h a systematic ti review. Stroke 1997;28: Rebleed has a catastrophic morbidity : 48% to 78%. Treatment of a ruptured aneurysm: imperative. Jane JA, Winn HR, Richardson AE. The natural history of intracranial aneurysms: rebleeding rates during the acute and long term period and implication for surgical management. Clin Neurosurg 1977; 24:
4 Etiology of intracranial aneurysm Congenital Atherosclerotic/ hypertensive Embolic Infectious Traumatic Associated with other conditions
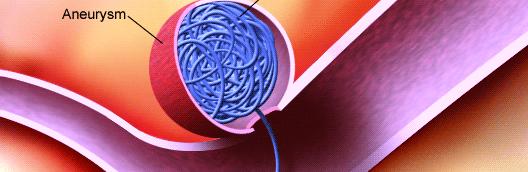
5 Major rupture SAH ICH IVH Subdural blood Presentation Mass effect- cranial nerve palsy: 3 rd nerve in PCOM Chiasmal syndrome - ophthalmic, Acom, Basilar top Cranial neuropathy- giant aneurysm compressing brainstem Endocrine disturbance: sellar and suprasellar
6 Presentation Minor hemorrhage/sentinel hemorrhage Small infarcts Seizures Prodromal /warning/ sentinel headache: minor blood leakage or aneurysmal expansion- reported in 30-60% of SAH Few hours to a few months before the rupture- median of 2 weeks Due to sentinel leaks/ mass effect of aneurysm expansion/ emboli Incidentally discoveredd
7 Decision making? Mode of presentation Ruptured aneurysm Un-ruptured aneurysm Patients related factors General condition Medical co-morbidities Aneurysm related factors Location Anatomy Size Availability of expertise Surgical Endovascular
8 Goals of aneurysm treatment Complete, permanent and safe occlusion of aneurysm. Less morbidity and mortality. Good quality of life.
9 Un-ruptured aneurysms Importance of treatment 1. Risk of SAH is % each year. 2. Around 50 % of these ruptures are fatal 3. Increase in size >1 cm increases the risk 11 fold (ISUIA trial. N Engl J Med 1998;339: )
10 Risks factors for SAH in un-ruptured aneurysms Increased aneurysm size on serial imaging Aneurysm size > 10 mm Aneurysm between 6-9 mm in middle and young age group Posterior circulation aneurysms: especially basilar apex Previous SAH from another aneurysm Symptomatic aneurysms Females Cigarette smoking Binge alcohol drinking
11 Factors affecting surgical outcome Aneurysm related factors Aneurysm size (>2.5 cm). Location (A-com, ICA bifurcation). Orientation Patient related factors Age Ischemic cerebro-vascular diseases Diabetes mellitus
12 Options for definitive treatment Surgery. Clipping Wrapping Wapp Parent vessel occlusion Revascularization procedures Endovascular methods. Endoscopy Conservative
13 Exclusive Indications for surgery SAH with ICH Hydrocephalus Signs of raised ICP Endovascular treatment is contraindicated
14 Clipping : Indications The choice of open surgical intervention is influenced by several factors: ---complexity of the aneurysm, ---size (too small or too large), --- geometry, ---unfavorable dome-to-neck ratio, ---access (inability to navigate delivery system to aneurysm site), --- anatomy (parent artery, branch artery, or perforator incorporation into neck).
15 Timing of surgery Anterior circulation: early surgery has good results Posterior circulations: Easy aneurysms: early surgery Difficult aneurysms : after two weeks (Haley EC jr et al the international cooperative study on the timing of aneurysm surgery; the north American experience. Stroke 23: ;1992) 214;1992)
16 Early surgery: Advantages Virtually eliminates re-bleed Facilitates treatment of vasospasm Removal of vasospasmogenic material Though operative mortality higher, but overall outcome is better Factors favoring early surgery: Good medical condition Good neurologic condition Large clot, blood Early rebleed, multiple episodes Imminent rebleed signs
17 Disadvantages of Early Surgery Inflammation and brain edema causes more difficult and traumatic retraction Acute clot makes dissection difficult Risk of intraoperative rupture is high Vessel injury may aggravate vasospasm Factors favoring late surgery: Poor medical and/or neurological condition Difficult aneurysms Significant edema on CT Active vasospasm
18 Surgery :Technical considerations Intraoperative objectives Prevent rupture Further enlargement Preserve normal vessels Minimize injury to the brain
19 Surgery :Technical considerations Clip too low- may occlude parent vessel Distal placement- aneurysmal rest Aneurysmal rest expand in future and may rebleed Surgical exposure: Avoid retraction ti Brain relaxation- hyperventilation, CSF drainage, lumbar spinal drainage, cisternal drainage Drugs
20 Surgery :Technical considerations Intra operative aneurysm rupture % Morbidity and mortality approach 30-35% When aneurysm can rupture Initial exposure- Reduce BP Temporary clip if possible Lobectomy if necessary for exposure Dissection of aneurysm- Blunt or sharp tears- tamponade, temporary clip If extends to parent vessel micro sutures may be taken Clip application- reapply clip or a second clip

21 Surgical technique The cornerstone of open surgical management -- microsurgical dissection of the subarachnoid planes --proximal and distal vascular control --direct visualization of clip application -- puncture verification of total aneurysm obliteration. Yasargil MG, Fox JL. The microsurgical approach to intracranial aneurysms. Surg Neurol 1975;3:7 14.
22 Advances in surgery Surgical innovations, such as cranial base approaches. Origitano TC, Anderson DE, Tarassoli Y, et al. Skull base approaches to complex cerebral aneurysms. Surg Neurol 1993;40: Intraoperative angiography: confirming parent or branch artery patency and aneurysm obliteration. Alexander TD, Macdonald RL, Weir B, et al. Intraoperative angiography in cerebral aneurysm surgery: a prospective study of 100 craniotomies. Neurosurgery 1996;39:10 7 [discussion: 17 8]. Origitano TC, Schwartz K, Anderson D, et al. Optimal clip application and intraoperative angiography for intracranial aneurysms. Surg Neurol 1999;51: [discussion: 124 8].
23 Wrapping Indications Aneurysm cannot be clipped Intraoperative rupture Materials used Muscle Muslin Plastic resin or polymer Artificial glue and muscle Fascia Teflon
24 Indications: Parent vessel ligation Large surgically difficult aneurysms Recurred after coiling Oh Other unclipable aneurysms Prerequisite: Good collateral l circulation i on balloon occlusion test or cross compression test Methods of parent vessel ligation Direct neck vessel ligation Gradual occlusion: Silverstone clamp
25 Indications: Revascularization procedures All those patients planned for ligation of parent vessel ligation but poor collateral circulation. Results: Good outcome 80% of anterior circulation 44% of posterior circulation Graft patency rate of 86% at 18 months Complications Acute graft occlusion Aneurysm rupture: d/t hemodynamic changes Ischemic deficits
26 Endovascular methods Exclusive Indications: Poor grade SAH Mdi Medical illness Surgically difficult aneurysms eg: proximal ICA basilar top giant aneurysm Patients preference
27 Endovascular methods Destructive ti procedures Balloon occlusion of parent vessel Reconstructive ti procedures GDC coils Bll Balloon remolding technique hi Stent coil technique
28 Balloon occlusion Generally used for proximal ICA and vertibro-basilar aneurysms Advantages Mass effect resolves Cranial neuropathies are known to improve Disadvantages: Recanalize, regrowth or rupture Ischemic symptoms Formation of de-novo aneurysms
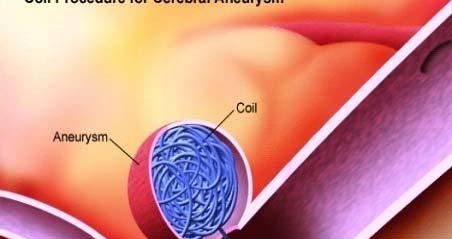
29 GDC coils Platinum spiral coils with circular memory Fit snugly in the aneurysm and induce thrombosis Disadvantages: Incomplete obliteration Recanalization Prolapse of coil and distal migration Parent artery thrombosis
30 Balloon remolding technique Introduced to overcome the problem of wide neck aneurysms Balloon is inflated in parent vessel against the neck and then coils are put in sac
31 Stent-coil technique Used in complex wide neck aneurysms Increases the density of coil packing
32 Limiting factors of coiling Dome to neck ratio < 2 Neck width > 4 mm Inadequate endovascular access Unstable intraluminal thrombus At Arterial il branch incorporated td in neck Middle cerebral artery aneurysms
33 Endoscopy Endoscope (fiberscope) to assist the microsurgical clipping of cerebral aneurysm- first reported by Fischer and Mustafa in 1994 Rigid endoscope: structures around the aneurysm can be detected with high quality imaging Supportive role in planning surgical manoeuvres and verifying whether clipping has been performed correctly Aneurysms of anterior circulation- esp. those of ICA and Acom artery. Many have the posterior communicating artery, choroidal artery or one of the distal cerebral arteries hidden behind the aneurysm dome
34 Special circumstances POOR GRADE SAH Rapid resuscitation Intracranial pressure monitoring Early aneurysm occlusion Prophylaxis py against delayed ischemia
35 Factors affecting outcome after definitive treatment 1. Diffuse SAH on NCCT head 2. Intraventricular bleed 3. Higher Fisher s Grade on NCCT head 4. Location of aneurysm (posterior circulation) 5. Rebleed before intervention 6. Post intervention infarct/hydrocephalus/meningitis 7. Acute renal failure 8. Septicemia A significant number of patients with poor grade SAH can have favorable outcome after aggressive definitive treatment. Patients who improve with resuscitation, merit intervention. Large craniotomy flaps / decompressive craniectomies are helpful in such patients. Ashish Suri,, Karanjit Singh Narang, B.S.Sharma. Sh Department of Neurosurgery. AIIMS
36 Advanced age?? Surgically g y treated patients do better than conservatively managed. Treatment of unruptured aneurysm is beneficial if life expectancy is more than 13 years. Treatment should not be denied only on the basis of age.
37 PREGNANCY?? Investigated and treated as same. Pregnancy can be continued Temporary clips than hypotension during surgery Mannitol and hyperventilation to be curtailed LSCS is preferred in unruptured cases Craniotomy and LSCS performed together Anticonvulsants and CCB to be avoided.
38 Infective aneurysms?? Streptococcus is most common cause Course of IV antibiotics for 4-6 wks. Surgical excision of aneurysm followed by bypass, anastomosis, or ligation of vessel.
39 Aneurysm >25 mm Mortality : 5-25% Giant aneurysm Good or excellent outcome in 70-80% Treatment options Clipping ( multiple clipping, fenestrated clips) Parent vessel ligation Revascularization with or without trapping Endovascular occlusion


40 CLIPPING V/S COILING
41 Clipping the mortality rate 1% -3.8% 38% the morbidity rate 4% - 12%. Clip vs coil: Safety King JT Jr, Berlin JA, et al. Morbidity and mortality from elective surgery for asymptomatic, unruptured, intracranial aneurysms: a meta-analysis. J Neurosurg 1994;81(6): Coiling the mortality rate 0.5% - 2% the morbidity rate is 4% to 5%. Johnston SC, Dudley RA, et al. Surgical and endovascular treatment of unruptured cerebral aneurysms at university hospitals. Neurology 1999;52(9):


42 Efficacy: Clip vs coil Clipping seems to be superior to coiling in achieving goals over the short and long term. Most series report a 92% to 96% exclusion rate of the aneurysm from the circulation with microsurgical clipping. David CA, Vishteh AG, et al. Late angiographic follow-up review of surgically treated aneurysms. J Neurosurg 1999;91(3): With respect to endovascular coiling, most series report 40% to 55% complete exclusion, 35.4% to 52% near-complete exclusion 3.5% to 8% incomplete exclusion of the aneurysms from the circulation. Murayama Y, Nien YL, et al. Guglielmi detachable coil embolization of cerebral aneurysms: 11 years experience. J Neurosurg 2003;98(5):
43 Clip vs coil Patient factors : Age Morbidity and mortality rate in those patients undergoing surgical clipping. 6.5% for patients less than 45 years old, 14.4% for patients 45 to 65 years old, 32% for patients greater than 64 years old Unruptured intracranial aneurysms :risk of rupture and risks of surgical intervention. N Engl J Med 1998;339: Similar finding have been reported with endovascular coiling, but the effects seem to be less significant with endovascular coiling in older patients. Barker FG II, Amin-Hanjani S, et al. Age-dependent differences in short-term outcome after surgical or endovascular treatment of unruptured intracranial aneurysms in the United States, Neurosurgery 2004;54(1):18 28 [discussion: 28 30].
44 Clip vs coil Aneurysm factors : size Increased size : increased risk with microsurgical treatment. Wirth et al : linear relation with regard to size and complication rate 3% for aneurysms less than 5 mm 7% for 6- to 15-mm aneurysms 14% for aneurysms of 16 to 24 mm. Wirth FP, Laws ER Jr, et al. Surgical treatment of incidental intracranial aneurysms. Neurosurgery 1983;12(5): Endovascular treatment : extremely large and small aneurysms having increased complications. Extremely small aneurysms : risk of intraprocedural rupture. Giant aneurysms: less favorable dome/neck ratio, Higher incidence of a branch vessel origin of the aneurysm neck, Often intra-aneurysmalaneurysmal thrombus.
45 Clip vs coil Aneurysm configuration Surgical complexity is increased Wide-necked Involving major neighboring artery : ensure complete exclusion of the aneurysm with preservation of the parent vessel and its associated branches. The most important factor :dome /neck ratio: large, intermediate, and small -the most favorable to least favorable configuration. Dense packing of the coils achieved with less risk of migration into the parent artery : small dome size, a small neck, and a large d/n ratio, (ideal for complete occlusion with fewer complications)
: 1531 8.")

46 Clip vs coil : Aneurysm location Posterior circulation aneurysms: higher complication rate with microsurgical treatment, most undergo endovascular therapy. Raaymakers TW, Rinkel GJ, et al. Mortality and morbidity of surgery for unruptured intracranial aneurysms: a meta-analysis. Stroke 1998;29(8): MCA aneurysms: often originate from one or both of the branching vessels often have an associated unfavorable d/n ratio. renders aneurysms unable to be coiled or migration of the coil into the parent vessel or a branch, resulting in a stroke. Clipping is still the most safe for most MCA aneurysms. Regli L, Uske A, et al. Endovascular coil placement compared with surgical clipping for the treatment of unruptured middle cerebral artery aneurysms: a consecutive series. J Neurosurg 1999;90(6):

47 The advantage of clipping: Clip vs coil Management: UA effective in changing the natural history of UIA in the short and long term. The disadvantage d of clipping: risk of treatment is higher h than that of coiling. The advantage of coiling: less invasive and safer than clipping, The major limitation: lack of durability in changing the natural history compared with clipping.
48 Clip vs coil Management: UA Anterior circulation aneurysms with a large d/n ratio, endovascular coiling should always be considered d as the first line of treatment in those patients with long, intermediate, and short estimated life expectancies, because this treatment provides the patient with relatively effective treatment that is safer than clipping. Posterior circulation aneurysms: patients with large and medium d/n ratios should undergo endovascular coiling regardless of the estimated life expectancy, because endovascular coiling provides a safer treatment that is relatively effective In some posterior circulation aneurysms with less favorable configurations, where the aneurysm sac involves one of the posterior cerebral branches, clipping may be the only alternative.
49 International Study of Unruptured Intracranial Aneurysms (ISUIA) 1998 report: retrospective data controversial- 0.05% yearly rupture rate identified ifi d for aneurysms <10 mm : considerably lower than the rate in earlier reports If true, the risks of treatment higher than the natural history risk. ISUIA: New prospective data Lancet 362: , 2003: results associated with endovascular or microsurgical repair.
50 ISUIA Patients in Group 2 (Patients who have had a ruptured aneurysm at another location that was isolated, trapped, clipped, or treated through endovascular obliteration) with unruptured intracranial aneurysms less than 7 mm had higher rupture rates than did those in Group 1 (p<0.0001). For both Group 1 and Group 2 patients the combined morbidity and mortality at 1 year was about 3% higher in the microsurgical group (12.6% for clipping vs. 9.8% for coiling in Group 1 patients t and 10.1% 1% vs. 7.1% in Group 2 patients).

51 Management: RA Preventing rebleed is top most priority Anterior circulation: clipping esp medium or small d/n ratios Except-short t life expectancy and/or a poor clinical i l grade Coiling: large d/n ratio Posterior circulation aneurysms: coiling the first choice Clipping: unfavorable d/n ratio, a long life expectancy, and a good clinical grade and is an option in those with a medium d/n ratio
52 ISAT trial (lancet 2005;360: ) Randomized study of 2143 patients ruptured intracranial aneurysms The safety of endovascular coiling compared with clipping. Prospective, randomized, d controlled trial Mortality or disability was 30.6 Vs 23.7 in surgical and endovascular gp at one year (p=0.0019) survival free of disability at 1 year is significantly better with coiling. Relative and absolute risk reduction in dependency or death is 22.6 vs 6.9 % in surgical and endovascular group. coiling is more likely to result in independent survival at 1 year than clipping; i the benefit continues for at least 7 years Risk of rebleed was higher in endovascular group at one year
53 Criticisms on ISAT trial Selection biases Premature analysis Only 22.4 % were randomized Outcome assessment Modified d Rankin Scale used for assessment Lack of angiographic data after surgery Lack of long term follow up Surgical outcome Post procedural rebleed and outcome
54 Worst headache of life. SAH Presentation Meningeal irritation (e.g.- neck stiffness, Kernig s/brudzinski s sign, low back pain, bilateral leg pain) : >75% of cases Take several (6-24 hrs) hours to develop LOC at the ictus: 45% of patients, often transient; 10% comatose for several days.-d/t d/t raised ICP, ICH, HCP, seizure, low CBF Seizures in acute phase:10-25% Focal neurologic abnormalities (25%) : hemiparesis, aphasia, hemineglect, cranial nerve palsies, memory loss
55 SAH Presentation Ocular hemorrhages (20-40%) : sub hyaloid pre-retinal/ intra-retinal surrounding fovea / intravitreous hemorrhage (Terson syndrome). Hypertension: 50% cases- often labile as ICP increases Temperature elevation: secondary to chemical meningitis from subarachnoid blood products- common after the 4 th day Tachycardia: often for several days.
56 SAH Grading: Hunt and Hess Grade 1 - Asymptomatic or mild headache Grade 2 - Moderate-to-severe headache, nuchal rigidity, and cranial nerve palsy Grade 3 - Mild alteration in mental status (confusion, lethargy) mild focal neurological deficit Grade 4 - Stupor and/or hemi paresis Grade 5 - Comatose and/or decerebrate rigidity idi Modified classification- Grade 0 Unruptured aneurysm Grade 1a no acute meningeal reaction but with fixed neuro deficit * Add one grade for HTN/DM/COPD/Severe Atherosclerosis/ angiographic vasospasm
57 SAH Grading: Fischer scale (based on CT scan ) To predict the likelihood lih of symptomatic cerebral vasospasm Group 1 - No blood detected Group 2 - Diffuse deposition of subarachnoid blood and no layers of blood greater than 1 mm Group 3 - Localized clots and/or vertical layers of blood 1 mm or greater in thickness Group 4 - Diffuse or no subarachnoid blood, but intracerebral or intraventricular clots are present
58 SAH WORK-UP : CT SCAN Sensitivity decreases with respect to increased time from ictus: 95% within the first 48 hours 80% at 72 hours 50% at 1 week Blood localized to the basal cisterns, the sylvian fissure, or the inter hemispheric fissure Helps rule out HCP. Falsely negative Small hemorrhages Severe anemia
59 SAH WORK-UP : DSA Gold standard: for evaluation of cerebral aneurysm (80-85% sensitivity) Can provide surgical information: Cerebrovascular anatomy, aneurysm location & source of bleeding, Aneurysm size/shape/orientation / of dome and neck Relation to the parent/perforating arteries If negative (10-20%): repeat test 3-4 weeks later May be useful to evaluate for possible cerebral vasospasm 3-D reconstruction: invaluable- dome-to-neck ratio parent artery or branch orientation to neck enhances surgical view for clip placement and vessel reconstruction
60 SAH WORK-UP : CTA Reported to detect aneurysms larger than 3 mm Sensitivity of 95% and 83% specificity. Provide sufficient anatomic detail esp relation to near by bony structure
61 Role is under evaluation SAH WORK-UP: MRA Limitations : to detect PICA and ACom aneurysm Risk/benefit ratio still favors conventional angiography Can detect aneurysms >3 mm with 86% sensitivity Useful Monitoring the status of small, unruptured aneurysms Evaluate the degree of intramural thrombus in giant aneurysms Screening high risk patients: including 1 st degree relative of patients with IC aneurysm False +ve in appox. 16%
62 SAH: MANAGEMENT ISSUES Rebleeding Hydrocephalus Delayed ischemic neurological deficit (DIND) Hyponatremia / hypovolemia DVT / Pulmonary embolism Seizures Determining the source of bleeding
63 SAH: ORDERS ON ADMISSION Admission in ICU with monitored bed Vital parameter and neurological status check 1 hrly Bed rest with head end elevated by30 degree, low external stimulation Nursing : strict I-O charting / daily weights / DVT pumps at LL /urinary catheterization/ NG tube IVF : Aggressive fluid therapy to head off cerebral salt wasting. NS + 20 meq 2 ml/kg/hr Avoid IM medication/ enema/ NSAID
64 SAH: ORDERS ON ADMISSION Prophylactic anticonvulsants : 3% have seizure- most authorities recommend for 1 week post-op p : Phenytoin mc. Leviteracetam now being increasing used Mild sedation (propofol/midazolam/lorazepam) Analgesic : fentanyl ( lower ICP and doesn t cause histamine release unlike morphine ) Steroid : effect on brain edema is controversial, usually given prior to craniotomy Stool softener / anti-emetics / antacids. Contraindicated for fear of impaired coagulation aspirin / dextran / heparin / repeated administration of hetastarch
65 SAH: NIMODEPINE Nimodipine 60 mg PO/NG/ IVq 4 hrs, initiated within 96hrs of SAH BRANT : British aneurysm nimodipine trial shown 22% vs. 33% incidence id of cerebral infarction i compared to placebo Blocks the slow channel of calcium influx Reduces the contraction of smooth muscles and may prevent vasospasm Possible beneficial effects are improved RBC rheology prevention of calcium entry in ischemic cells anti platelet aggregation dilatation of collateral lepto meningeal arteries Side effects are systemic hypotension renal failure pulmonary edema
66 SAH: PREVENTION OF REBLEED Early treatment (coiling/surgery). Bed rest does not prevent. Antifibrinolytic therapy Tranexamic acid reduces the risk Loading dosage of 1 gm bolus followed by 1 gm q 6 hrs until aneurysm is secured (max 72 hrs) Contraindicated: Epsilon aminocaproic acid (EACA) competitively blocks activation of plasminogen to plasmin. More incidence of HCP/DIND on prolonged use. Increased risk of cerebral infraction
67 Ventriculostomy Acute HCP or significant intraventricular blood. Allows drainage of CSF as well as ICP monitoring. May increase the risk of rebleed. Symptomatic improvement found in 30% immediately H&H grade >3 : if there is some improvement with ventriculostomy, ti t prognosis may be favourable Controversy: use of ventriculostomy in acute HCP increases or possibly decreases incidence of shunt dependency
68 SAH : VASOSPASM Non localizing finding New or increasing headache Alteration of level of consciousness Disorientation Meningismus Focal neurological sign Cranial nerve palsy Focal neurological deficit Anterior cerebral artery syndrome (mc)- frontal lobe findings predominate (abulia, grasp/suck reflex, urinary incontinence, drowsiness, slowness, delayed response, confusion Middle cerebral eb artery syndrome-hemiparesis, e es s, monoparesis, opa s, aphasia, ideomotor apraxia
69 VASOSPASM : TIME COURSE Onset is almost never before day 3 Max frequency on day 6-8 Clinical CVS usually resolves by day 12 post SAH Radiological CVS usually resolves slowly over 3-4 weeks Onset is usually insidious but in 10% may have abrupt and severe dt deterioration ti
70 VASOSPASM: DIAGNOSIS Clinical Criteria Delayed onset of persistent neuro deficit onset 4-20 days post SAH Deficit appropriate to involved arteries R/O other causes of deterioration Rebleeding HCP Cerebral edema Seizure Metabolic disturbances viz hyponatremia Hypoxia Sepsis


71 VASOSPASM Trans Cranial Doppler ( TCD ) Aaslid & colleague ( 1980 ) Principle : as an artery narrows, blood flow velocity within it increases May precede clinical symptoms by hrs Mean MCA MCA : ICA Interpretation t ti velocity (Lindegaard Ratio) < 120 cm/sec < 3 Normal cm/sec 3-6 Mild vasospasm > 200 cm/sec > 6 Severe vasospasm



72 VASOSPASM: IADSA Vasospasm appear as concentric narrowing which can be focal/segmental/diffuse. mild (<25%), moderate (25-50%) 50%) severe (>50%)
73 VASOSPASM: PREVENTION Preventing post SAH hypovolemia & anemia Smooth muscle relaxants :- CCB didn t succeed in counteracting vasospasm but may provide neuro-protectant effect Endothelin receptor antagonist, clazosentan ( ETa ) Direct mechanical arterial dilatation : balloon angioplasty ( 60-80% clinical improvement ) Indirect arterial dilatation : utilizing hyperdynamic y therapy
74 VASOSPASM : MANAGEMENT Removal of potential vasospasmogenic agents : blood clot mechanical removing during surgery subarachnoid irrigation with thrombolytic agents viz rt-pa at surgery or cisternal catheters or intrathecally (Findlay JM et al : RCT of intraoperative, intracisternal TPA for prevention of vasospasm) CSF drainage via serial LP/EVD/post op. cisternal catheter Sympatholytics / Cervical sympathectomy Intra-arterial or intra-thecal papaverine / verapamil Alpha ICAM 1 inhibition (Ab)
75 VASOSPASM : MANAGEMENT Protection of CNS from ischemic injury : - CCB - NMDA receptor antagonist ( selfotel / eliprodil / cerestat ) - Free radical scavengers ( tirilazad mesylate / nicaraven ) Improvement of rheological properties of intravascular blood to enhance perfusion - plasma / albumin / LMW dextran / PFC / mannitol - hematocrit: controversial 30-35% - good compromise between lowered viscosity without overlay reducing O2 carrying capacity Extracranial intracranial bypass around zone of vasospasm
: 895-902.")

76 VASOSPASM MX: UNDER TRIAL Nicardipine prolonged release implants (NPRIs): Intra-op in cisterns where thick clots were located. Decreased incidence Kasuya H et al: Application of nicardipine proloned release inplants: Analysis of 7 consecutive patients with SAH. Neurosurgery 56 (5): Clazosentan: Selective endothelin Ia receptor antagonist. Reduces frequency and severity of vasospasm. Vajkoczy et al. J. Neurosurgery 03: 9-17, 2005 Statins: Simvastatin 80 mg/day, Pravastatin 40 mg/day Reduction in radiographic vasospasm, DIND and mortality. Silberg VAH et al: Do statins improve outcome and reduce incidence of vasospasm after anerysmal SAH: A meta-analysis. Stroke 39: , 2008
77 TRIPLE H THERAPY HYPERTENSION HYPERVOLEMIA 1. Dopamine : start at 2.5 mcg/kg/min and titrate up to mcg/kg/min 2. Dobutamine : start at 5 mcg/min titrate to 20 mcg/kg/min 3. Phenylephrine : start at 5 mcg/min titrate up to 10 mcg/kg 4. Norepinephrine : start at 1-2 mcg/min & then increase by 10 mcg/min 1. IVF : ml / hr 2. Albumin / plasma 3. DDAVP : antidiuretic, 2-4 mcg SQ q D in divided doses HEMODILUTION 1. Target hematocrit : < 33% 2. Blood transfusion for Hct < 25%
78 Complication of hyperdynamic therapy Intra cranial cerebral edema raised ICP hemorrhagic infarction in the area of ischemia Extra cranial pulmonary edema (17%) cardiac failure dilutional hyponatremia (3%) MI (2%) Complication related to catheter catheter related sepsis (13%) subclavian vein thrombosis (1.3%) pneumothorax (1%) hemothorax
79 Thank you
TREATMENT OF INTRACRANIAL ANEURYSMS
 TREATMENT OF INTRACRANIAL ANEURYSMS Presented by: Dr Nilesh S. Kurwale Introduction Incidence of aneurysm difficult to estimate Prevalence 0.2-7.9 % Half the aneurysms ruptures 2% present during childhood
TREATMENT OF INTRACRANIAL ANEURYSMS Presented by: Dr Nilesh S. Kurwale Introduction Incidence of aneurysm difficult to estimate Prevalence 0.2-7.9 % Half the aneurysms ruptures 2% present during childhood
Current State of the Art
 SAH Current State of the Art Thomas C. Steineke, M.D., Ph.D. Director of Neurovascular Surgery NJ Neuroscience Institute JFK Medical Center Introduction Signs and symptoms of a problem What are aneurysms
SAH Current State of the Art Thomas C. Steineke, M.D., Ph.D. Director of Neurovascular Surgery NJ Neuroscience Institute JFK Medical Center Introduction Signs and symptoms of a problem What are aneurysms
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Subarachnoid Hemorrhage (SAH) Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.
 Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.") Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
TCD AND VASOSPASM SAH
 CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage
 Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Subarachnoid Hemorrhage and Brain Aneurysm
 Subarachnoid Hemorrhage and Brain Aneurysm DIN Department of Interventional Neurology What is SAH? Subarachnoid Haemorrhage is the sudden leaking (haemorrhage) of blood from the blood vessels of brain.
Subarachnoid Hemorrhage and Brain Aneurysm DIN Department of Interventional Neurology What is SAH? Subarachnoid Haemorrhage is the sudden leaking (haemorrhage) of blood from the blood vessels of brain.
Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici
 Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici Nino Stocchetti Milan University Neuroscience ICU Ospedale Policlinico IRCCS Milano stocchet@policlinico.mi.it Macdonald RL et
Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici Nino Stocchetti Milan University Neuroscience ICU Ospedale Policlinico IRCCS Milano stocchet@policlinico.mi.it Macdonald RL et
Summary of some of the landmark articles:
 Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Ruptured Cerebral Aneurysm of the Anterior Circulation
 Original Articles * Division of Neurosurgery Department of Surgery Ruptured Cerebral Aneurysm of the Anterior Circulation Management and Microsurgical Treatment Ossama Al-Mefty, MD* ABSTRACT Based on the
Original Articles * Division of Neurosurgery Department of Surgery Ruptured Cerebral Aneurysm of the Anterior Circulation Management and Microsurgical Treatment Ossama Al-Mefty, MD* ABSTRACT Based on the
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
7/18/2018. Cerebral Vasospasm: Current and Emerging Therapies. Disclosures. Objectives
 Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
Sub-arachnoid haemorrhage
 Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Update in Diagnosis and Management of Intracranial Aneurysms for Primary Health Care Providers November 15, 2012 Boston, Massachusetts
 Update in Diagnosis and Management of Intracranial Aneurysms for Primary Health Care Providers November 15, 2012 Boston, Massachusetts Educational Partner: Session 1: Update in Diagnosis and Management
Update in Diagnosis and Management of Intracranial Aneurysms for Primary Health Care Providers November 15, 2012 Boston, Massachusetts Educational Partner: Session 1: Update in Diagnosis and Management
4/10/2018. The Surgical Treatment of Cerebral Aneurysms. Aneurysm Locations. Aneurysmal Subarachnoid Hemorrhage. Jerone Kennedy, M.D.
 The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications
 Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM. Vikram Jadhav MD, PhD. 04/12/2018 CentraCare Health St.
 ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
Case Report 1. CTA head. (c) Tele3D Advantage, LLC
 Tele3D Advantage, LLC") Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Multi-modality management of intracranial aneurysms
 Multi-modality management of intracranial aneurysms Christopher Koebbe, Maj, USAF, MC Staff Neurosurgeon San Antonio Military Medical Consortium Clinical Assistant Professor Department of Neurological
Multi-modality management of intracranial aneurysms Christopher Koebbe, Maj, USAF, MC Staff Neurosurgeon San Antonio Military Medical Consortium Clinical Assistant Professor Department of Neurological
Alessandro Della Puppa
 Intraoperative measurement of arterial blood flow in complex cerebral aneurysms surgery Studio flussimetrico intra-operatorio nel clipping degli aneurismi complessi Alessandro Della Puppa NEUROSURGERY
Intraoperative measurement of arterial blood flow in complex cerebral aneurysms surgery Studio flussimetrico intra-operatorio nel clipping degli aneurismi complessi Alessandro Della Puppa NEUROSURGERY
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Management of the Endovascular Patient and Acute Emergencies in the Angio Suite
 Management of the Endovascular Patient and Acute Emergencies in the Angio Suite June 9, 2015 Bridget Cantrell, APN, CNP Endovascular Neurosurgery Advocate Medical Group No Disclosures The human brain is
Management of the Endovascular Patient and Acute Emergencies in the Angio Suite June 9, 2015 Bridget Cantrell, APN, CNP Endovascular Neurosurgery Advocate Medical Group No Disclosures The human brain is
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease
 Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part B. Objectives Epidemiology of asah Concept: What is a brain
Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part B. Objectives Epidemiology of asah Concept: What is a brain
NIH Public Access Author Manuscript J Am Coll Radiol. Author manuscript; available in PMC 2013 June 24.
 NIH Public Access Author Manuscript Published in final edited form as: J Am Coll Radiol. 2010 January ; 7(1): 73 76. doi:10.1016/j.jacr.2009.06.015. Cerebral Aneurysms Janet C. Miller, DPhil, Joshua A.
NIH Public Access Author Manuscript Published in final edited form as: J Am Coll Radiol. 2010 January ; 7(1): 73 76. doi:10.1016/j.jacr.2009.06.015. Cerebral Aneurysms Janet C. Miller, DPhil, Joshua A.
Small UIAs, <7 mm in diameter, uncommonly cause aneurysmal symptoms and are the most frequently detected incidentally.
 Research grant from Stryker Neurovascular Research grant from Covidien/ Medtronic Consultant and proctor for Stryker Neurovascular Consultant and proctor for Covidien/ Medtronic Consultant for Codman Neurovascular
Research grant from Stryker Neurovascular Research grant from Covidien/ Medtronic Consultant and proctor for Stryker Neurovascular Consultant and proctor for Covidien/ Medtronic Consultant for Codman Neurovascular
Interventions in the Management of Acute Stroke. Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital
 Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU
 CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Modern Management of ICH
 Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
SAH READMISSIONS TO NCCU
 SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
Moyamoya Syndrome with contra lateral DACA aneurysm: First Case report with review of literature
 Romanian Neurosurgery Volume XXXI Number 3 2017 July-September Article Moyamoya Syndrome with contra lateral DACA aneurysm: First Case report with review of literature Ashish Kumar Dwivedi, Pradeep Kumar,
Romanian Neurosurgery Volume XXXI Number 3 2017 July-September Article Moyamoya Syndrome with contra lateral DACA aneurysm: First Case report with review of literature Ashish Kumar Dwivedi, Pradeep Kumar,
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
DIAGNOSTIC AND THERAPEUTIC MANAGEMENT OF CEREBRAL VASOSPASM AFTER SAH
 DIAGNOSTIC AND THERAPEUTIC MANAGEMENT OF CEREBRAL VASOSPASM AFTER SAH Erich Schmutzhard Department of Neurology, NICU Medical University Hospital A-6020 Innsbruck, Austria Neurologie Intensiv Universitätskliniken
DIAGNOSTIC AND THERAPEUTIC MANAGEMENT OF CEREBRAL VASOSPASM AFTER SAH Erich Schmutzhard Department of Neurology, NICU Medical University Hospital A-6020 Innsbruck, Austria Neurologie Intensiv Universitätskliniken
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Management of Cerebral Aneurysms in Polycystic Kidney Disease. Dr H Stockley Consultant Neuroradiologist Greater Manchester Neuroscience Centre
 Management of Cerebral Aneurysms in Polycystic Kidney Disease Dr H Stockley Consultant Neuroradiologist Greater Manchester Neuroscience Centre What is a cerebral aneurysm? Developmental degenerative arterial
Management of Cerebral Aneurysms in Polycystic Kidney Disease Dr H Stockley Consultant Neuroradiologist Greater Manchester Neuroscience Centre What is a cerebral aneurysm? Developmental degenerative arterial
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Management of cerebral vasospasm
 Neurosurg Rev DOI 10.1007/s10143-005-0013-5 REVIEW R. Loch Macdonald Management of cerebral vasospasm Received: 5 August 2005 / Revised: 28 October 2005 / Accepted: 4 November 2005 # Springer-Verlag 2005
Neurosurg Rev DOI 10.1007/s10143-005-0013-5 REVIEW R. Loch Macdonald Management of cerebral vasospasm Received: 5 August 2005 / Revised: 28 October 2005 / Accepted: 4 November 2005 # Springer-Verlag 2005
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
(aneurysmal subarachnoid hemorrhage, 17%~60% :SAH. ,asah , 22%~49% : Willis. :1927 Moniz ;(3) 2. ischemic neurological deficit,dind) SAH) SAH ;(6)
 2. ischemic neurological deficit,dind) SAH) SAH ;(6)") ,, 2. : ;,, :(1), (delayed ;(2) ischemic neurological deficit,dind) ;(3) 2. :SAH ;(4) 5-10 10 HT -1-1 ;(5), 10 SAH ;(6) - - 27%~50%, ( cerebral vasospasm ) Glasgow (Glasgow Coma Scale,GCS), [1],, (aneurysmal
,, 2. : ;,, :(1), (delayed ;(2) ischemic neurological deficit,dind) ;(3) 2. :SAH ;(4) 5-10 10 HT -1-1 ;(5), 10 SAH ;(6) - - 27%~50%, ( cerebral vasospasm ) Glasgow (Glasgow Coma Scale,GCS), [1],, (aneurysmal
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
A Less Invasive Approach for Ruptured Aneurysm with Intracranial Hematoma: Coil Embolization Followed by Clot Evacuation
 A Less Invasive Approach for Ruptured Aneurysm with Intracranial Hematoma: Coil Embolization Followed by Clot Evacuation Je Hoon Jeong, MD 1 Jun Seok Koh, MD 1 Eui Jong Kim, MD 2 Index terms: Endovascular
A Less Invasive Approach for Ruptured Aneurysm with Intracranial Hematoma: Coil Embolization Followed by Clot Evacuation Je Hoon Jeong, MD 1 Jun Seok Koh, MD 1 Eui Jong Kim, MD 2 Index terms: Endovascular
Surgical techniques and procedures for cerebrovascular surgery. Surgery for the AVF at the cranio-cervical junction and high cervical spine
 VS-1 Surgery for the AVF at the cranio-cervical junction and high cervical spine Hiroyuki Kinouchi University of Yamanashi, Department of Neurosurgery Dural AVFs have been recognized as common type of
VS-1 Surgery for the AVF at the cranio-cervical junction and high cervical spine Hiroyuki Kinouchi University of Yamanashi, Department of Neurosurgery Dural AVFs have been recognized as common type of
History of revascularization
 History of revascularization Author (year) Kredel, 1942 Woringer& Kunlin, 1963 Donaghy& Yasargil, 1968 Loughheed 1971 Kikuchini & Karasawa1973 Karasawa, 1977 Story, 1978 Sundt, 1982 EC/IC bypass study
History of revascularization Author (year) Kredel, 1942 Woringer& Kunlin, 1963 Donaghy& Yasargil, 1968 Loughheed 1971 Kikuchini & Karasawa1973 Karasawa, 1977 Story, 1978 Sundt, 1982 EC/IC bypass study
ENDOVASCULAR THERAPIES FOR ACUTE STROKE
 ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Effect of clot removal on cerebral vasospasm TETSUJI INAGAWA, M.D., MITSUO YAMAMOTO, M.D., AND KAZUKO KAMIYA, M.D.
 J Neurosurg 72:224-230, 1990 Effect of clot removal on cerebral vasospasm TETSUJI INAGAWA, M.D., MITSUO YAMAMOTO, M.D., AND KAZUKO KAMIYA, M.D. Department of Neurosurgery, Shimane Prefectural Central Hospital,
J Neurosurg 72:224-230, 1990 Effect of clot removal on cerebral vasospasm TETSUJI INAGAWA, M.D., MITSUO YAMAMOTO, M.D., AND KAZUKO KAMIYA, M.D. Department of Neurosurgery, Shimane Prefectural Central Hospital,
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Neurosurgical Management of Aneurysmal Subarachnoid Hemorrhage
 Neurosurgical Management of Aneurysmal Subarachnoid Hemorrhage PVHMC STROKE SYMPOSIUM 2018 10/27/18 Srinath Samudrala MD, FACS Epidemiology of Subarachnoid Hemorrhage (SAH) Less than 10% of all stroke
Neurosurgical Management of Aneurysmal Subarachnoid Hemorrhage PVHMC STROKE SYMPOSIUM 2018 10/27/18 Srinath Samudrala MD, FACS Epidemiology of Subarachnoid Hemorrhage (SAH) Less than 10% of all stroke
The Worst Headache of My Life Hemorrhagic Stroke
 The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
Cerebral Aneurysms. U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health
 Cerebral Aneurysms U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health Cerebral Aneurysms What is a cerebral aneurysm? cerebral aneurysm (also known as an
Cerebral Aneurysms U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health Cerebral Aneurysms What is a cerebral aneurysm? cerebral aneurysm (also known as an
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Quality Metrics. Stroke Related Procedure Outcomes
 Quality Metrics Stroke Related Procedure Outcomes Below is a description of some of the stroke-related procedures performed at St. Dominic Hospital in Jackson, with quality information on the complication
Quality Metrics Stroke Related Procedure Outcomes Below is a description of some of the stroke-related procedures performed at St. Dominic Hospital in Jackson, with quality information on the complication
Cerebrovascular Disease
 Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
Coil Embolization for Intracranial Aneurysms
 Ontario Health Technology Assessment Series 2006; Vol. 6, No. 1 Coil Embolization for Intracranial Aneurysms An Evidence-Based Analysis January 2006 Medical Advisory Secretariat Ministry of Health and
Ontario Health Technology Assessment Series 2006; Vol. 6, No. 1 Coil Embolization for Intracranial Aneurysms An Evidence-Based Analysis January 2006 Medical Advisory Secretariat Ministry of Health and
Case 37 Clinical Presentation
 Case 37 73 Clinical Presentation The patient is a 62-year-old woman with gastrointestinal (GI) bleeding. 74 RadCases Interventional Radiology Imaging Findings () Image from a selective digital subtraction
Case 37 73 Clinical Presentation The patient is a 62-year-old woman with gastrointestinal (GI) bleeding. 74 RadCases Interventional Radiology Imaging Findings () Image from a selective digital subtraction
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service
 M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
TABLES. Table 1 Terminal vessel aneurysms. Table. Aneurysm location. Bypass flow** Symptoms Strategy Bypass recipient. Age/ Sex.
 Table TABLES Table 1 Terminal vessel aneurysms Age/ Sex Aneurysm location Symptoms Strategy Bypass recipient Recipient territory Recipient territory flow* Cut flow Bypass flow** Graft Patent postop F/U
Table TABLES Table 1 Terminal vessel aneurysms Age/ Sex Aneurysm location Symptoms Strategy Bypass recipient Recipient territory Recipient territory flow* Cut flow Bypass flow** Graft Patent postop F/U
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Aneurysms of the posterior inferior cerebellar artery
 ORIGINAL RESEARCH J.P. Peluso W.J. van Rooij M. Sluzewski G.N. Beute C.B. Majoie Posterior Inferior Cerebellar Artery Aneurysms: Incidence, Clinical Presentation, and Outcome of Endovascular Treatment
ORIGINAL RESEARCH J.P. Peluso W.J. van Rooij M. Sluzewski G.N. Beute C.B. Majoie Posterior Inferior Cerebellar Artery Aneurysms: Incidence, Clinical Presentation, and Outcome of Endovascular Treatment
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE
 MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
Coiling of ruptured and unruptured intracranial aneurysms
 ORIGINAL RESEARCH W.J. van Rooij G.J. Keeren J.P.P. Peluso M. Sluzewski Clinical and Angiographic Results of Coiling of 196 Very Small (< 3 mm) Intracranial Aneurysms BACKGROUND AND PURPOSE: Coiling of
ORIGINAL RESEARCH W.J. van Rooij G.J. Keeren J.P.P. Peluso M. Sluzewski Clinical and Angiographic Results of Coiling of 196 Very Small (< 3 mm) Intracranial Aneurysms BACKGROUND AND PURPOSE: Coiling of
 www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
Carotid Stenosis 1/24/2019. Review of Primary Studies. NASCET- Moderate stenosis. ACAS (Asymptomatic Carotid Atherosclerosis Study) NASCET
 NASCET") Review of Primary Studies Carotid Stenosis NINDS National Institute of Neurological Disorders and Stroke 2 large studies to determine who would benefit from surgery NASCET North American Symptomatic Carotid
Review of Primary Studies Carotid Stenosis NINDS National Institute of Neurological Disorders and Stroke 2 large studies to determine who would benefit from surgery NASCET North American Symptomatic Carotid
lek Magdalena Puławska-Stalmach
 lek Magdalena Puławska-Stalmach tytuł pracy: Kliniczne i radiologiczne aspekty tętniaków wewnątrzczaszkowych a wybór metody leczenia Summary An aneurysm is a localized, abnormal distended lumen of the
lek Magdalena Puławska-Stalmach tytuł pracy: Kliniczne i radiologiczne aspekty tętniaków wewnątrzczaszkowych a wybór metody leczenia Summary An aneurysm is a localized, abnormal distended lumen of the
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Extracranial to intracranial bypass for intracranial atherosclerosis
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Extracranial to intracranial bypass for intracranial atherosclerosis In cerebrovascular disease, blood vessels
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Extracranial to intracranial bypass for intracranial atherosclerosis In cerebrovascular disease, blood vessels
a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)).
).") 12.0 Outcomes 12.1 Definitions 12.1.1 Neurologic Outcome Events a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)). Criteria:
12.0 Outcomes 12.1 Definitions 12.1.1 Neurologic Outcome Events a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)). Criteria:
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Surgical Privileges Form: "Neurosurgery" Clinical Privileges Request. Requested (To be completed by the applicant) Not Recommended (For committee use)
 Not Recommended (For committee use)") Surgical Form: Clinical Request "Neurosurgery" Applicant s Name:. License No. (If Any):... Date:... Scope of Practice:. Facility:.. Place of Work:. the applicant) CATEGORY I: Core : 1. Interpretation of
Surgical Form: Clinical Request "Neurosurgery" Applicant s Name:. License No. (If Any):... Date:... Scope of Practice:. Facility:.. Place of Work:. the applicant) CATEGORY I: Core : 1. Interpretation of
What You Should Know About Cerebral Aneurysms
 American Society of Neuroradiology American Society of Interventional & Therapeutic Neuroradiology What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Intervention Committee
American Society of Neuroradiology American Society of Interventional & Therapeutic Neuroradiology What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Intervention Committee
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
Paul Gigante HMS IV Gillian Lieberman, MD. Sept Mr. T s T s Headache. Paul Gigante,, Harvard Medical School Year IV Gillian Lieberman, MD
 Sept 2005 Mr. T s T s Headache Paul Gigante,, Harvard Medical School Year IV Mr. T s T s Presentation 45 year-old welder complains of sudden severe headache and witnessed seizure with loss of consciousness
Sept 2005 Mr. T s T s Headache Paul Gigante,, Harvard Medical School Year IV Mr. T s T s Presentation 45 year-old welder complains of sudden severe headache and witnessed seizure with loss of consciousness
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Neuro Quiz 29 Transcranial Doppler Monitoring
 Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Long term follow-up of patients with coiled intracranial aneurysms Sprengers, M.E.S.
 UvA-DARE (Digital Academic Repository) Long term follow-up of patients with coiled intracranial aneurysms Sprengers, M.E.S. Link to publication Citation for published version (APA): Sprengers, M. E. S.
UvA-DARE (Digital Academic Repository) Long term follow-up of patients with coiled intracranial aneurysms Sprengers, M.E.S. Link to publication Citation for published version (APA): Sprengers, M. E. S.
Intracranial-to-intracranial vascular anastomosis created using a microanastomotic device for the treatment of distal middle cerebral artery aneurysms
 J Neurosurg 97:486 491, 2002 Intracranial-to-intracranial vascular anastomosis created using a microanastomotic device for the treatment of distal middle cerebral artery aneurysms Technical note DAVID
J Neurosurg 97:486 491, 2002 Intracranial-to-intracranial vascular anastomosis created using a microanastomotic device for the treatment of distal middle cerebral artery aneurysms Technical note DAVID
Definition พ.ญ.ส ธ ดา เย นจ นทร. Epidemiology. Definition 5/25/2016. Seizures after stroke Can we predict? Poststroke seizure
 Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Carotid Artery Stenting
 Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Development of Nicardipine Prolonged-Release Implants After Clipping for Preventing Cerebral Vasospasm: From Laboratory to Clinical Trial
 178 The Open Conference Proceedings Journal, 2010, 1, 178-182 Open Access Development of Nicardipine Prolonged-Release Implants After Clipping for Preventing Cerebral Vasospasm: From Laboratory to Clinical
178 The Open Conference Proceedings Journal, 2010, 1, 178-182 Open Access Development of Nicardipine Prolonged-Release Implants After Clipping for Preventing Cerebral Vasospasm: From Laboratory to Clinical
Treatment of Unruptured Vertebral Artery Dissecting Aneurysms
 33 Treatment of Unruptured Vertebral Artery Dissecting Aneurysms Isao NAITO, M.D., Shin TAKATAMA, M.D., Naoko MIYAMOTO, M.D., Hidetoshi SHIMAGUCHI, M.D., and Tomoyuki IWAI, M.D. Department of Neurosurgery,
33 Treatment of Unruptured Vertebral Artery Dissecting Aneurysms Isao NAITO, M.D., Shin TAKATAMA, M.D., Naoko MIYAMOTO, M.D., Hidetoshi SHIMAGUCHI, M.D., and Tomoyuki IWAI, M.D. Department of Neurosurgery,
Intracranial aneurysms are an important health problem
 ORIGINAL RESEARCH E.G. Klompenhouwer J.T.A. Dings R.J. van Oostenbrugge S. Oei J.T. Wilmink W.H. van Zwam Single-Center Experience of Surgical and Endovascular Treatment of Ruptured Intracranial Aneurysms
ORIGINAL RESEARCH E.G. Klompenhouwer J.T.A. Dings R.J. van Oostenbrugge S. Oei J.T. Wilmink W.H. van Zwam Single-Center Experience of Surgical and Endovascular Treatment of Ruptured Intracranial Aneurysms
The Endovascular Treatment of Cerebral Aneurysms
 The Endovascular Treatment of Cerebral Aneurysms George P. Teitelbaum, M.D., FSIR Regional Director, Neurointerventional Surgery Providence, California Types of Stroke and Their Causes Ischemic (87%):
The Endovascular Treatment of Cerebral Aneurysms George P. Teitelbaum, M.D., FSIR Regional Director, Neurointerventional Surgery Providence, California Types of Stroke and Their Causes Ischemic (87%):
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage. By: Shifaa AlQa qa
 CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
Disclosures. Anesthesia for Endovascular Treatment of Acute Ischemic Stroke. Acute Ischemic Stroke. Acute Stroke = Medical Emergency!
 Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Coiling of Very Large or Giant Cerebral Aneurysms: Long-Term Clinical and Serial Angiographic Results
 AJNR Am J Neuroradiol 24:257 262, February 2003 Coiling of Very Large or Giant Cerebral Aneurysms: Long-Term Clinical and Serial Angiographic Results Menno Sluzewski, Tomas Menovsky, Willem Jan van Rooij,
AJNR Am J Neuroradiol 24:257 262, February 2003 Coiling of Very Large or Giant Cerebral Aneurysms: Long-Term Clinical and Serial Angiographic Results Menno Sluzewski, Tomas Menovsky, Willem Jan van Rooij,
Disclosures. Objectives. Critical Care Management of Subarachnoid Hemorrhage. Nothing to disclose
 Critical Care Management of Subarachnoid Hemorrhage Nerissa U. Ko, MD, MAS UCSF Department of Neurology September 7, 2013 Nothing to disclose Disclosures Grant funding from American Heart Association,
Critical Care Management of Subarachnoid Hemorrhage Nerissa U. Ko, MD, MAS UCSF Department of Neurology September 7, 2013 Nothing to disclose Disclosures Grant funding from American Heart Association,
The current optimized approach for patients with a ruptured
 ORIGINAL RESEARCH I. Oran C. Cinar Continuous Intra-Arterial Infusion of Nimodipine During Embolization of Cerebral Aneurysms Associated With Vasospasm BACKGROUND AND PURPOSE: Despite rigorous efforts,
ORIGINAL RESEARCH I. Oran C. Cinar Continuous Intra-Arterial Infusion of Nimodipine During Embolization of Cerebral Aneurysms Associated With Vasospasm BACKGROUND AND PURPOSE: Despite rigorous efforts,
Brain Attack. Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship. Case Medical Center
 Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among
Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among