secondary effects and sequelae of head trauma.
|
|
|
- Gillian Cobb
- 5 years ago
- Views:
Transcription

.")
1 Neuroimaging of vascular/secondary secondary effects and sequelae of head trauma. Andrès Server Alonso Department of Neuroradiology Division of Radiology Ullevål University Hospital Oslo, Norway. Guidelines for identifying trauma patients at high risk for blunt cerebrovascular injury Cervical spine fracture with Foramen transversarium involvement,, or 30% or more subluxation,, or Significant rotation or distraction mechanism Basillar skull fracture crossing carotid canal, foramen lacerum,, or cavernous sinus Severe facial fractures (LeFort II or III; naso-orbital orbital ethmoid complex, facial smash). Carotid or vertebral artery perivascular hematoma Horner`s syndrome GCS<6 at 24 h after initial assessment Neurologic examination incongruent with brain imaging Stroke or TIA Hanging atempt with cervical hematomas or cervical spine fractures From Sliker CW, Mirvis SE. Eur J Radiol 2007, 64(1):3-14.
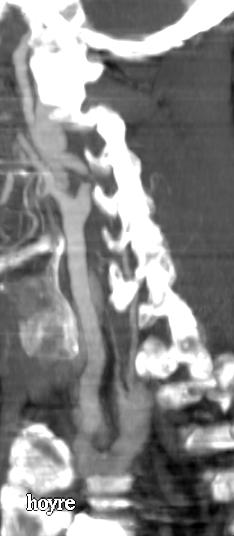
2 Primary vascular injuries Traumatic arterial dissection Extracranial carotid dissections Intracranial dissections or dissecting aneurysms Vertebral artery dissection Carotid-cavernous fistulas Traumatic intracranial aneurysms Traumatic venous thrombosis Traumatic carotid dissections 70% of carotid dissections involve both the cervical and petrous portions of the artery Dissections should be suspected if: Neurologic deficits Infarcts Evidence of significant skull trauma Aneurysms occur in 58% of traumatic dissections Intimal flap present in 20-35% of cases Carotid occlusion occur in 20% of dissections
3 Intracranial dissections or dissecting aneurysms Affect the supraclinoid carotid or middel cerebral arteries The location of the intramural hematoma is usually subintimal Dissecting aneurysms often present with a string-of-beads appearance Vertebral artery dissection 20% of all cervical vascular injuries A 24% to 46% incidence of vertebral artery injury associated with major blunt cervical spine trauma including fractures, subluxations or severe hyperextension or hyperflexion injury. The angiographic findings: stenosis, aneurysms and intimal flaps.







4 Day 0 Day 1 Day 3 Day 0 Day 8 Day 3













5



6 Traumatic intracranial aneurysms classification Proximal to the circle of Willis Infraclinoid carotid artery Supraclinoid carotid artery Vertebrobasilar Distal to the circle of Willis Subcortical cortical
7 TIA mechanisms of injury Infraclinoid carotid and basilar artery aneurysms are associated with: Basilar skull fractures Supraclinoid carotid artery aneurysms can be the result of : Either movement of the supraclinoid segment against the anterior clinoid process Or stretching of the carotid artery Distal subcortical aneurysms occurs along: The anterior cerebral artery and its branches Traumatic movement of the brain and vessels against the fixed falx cerebri Posterior cerebral artery aneurysms Result of trauma of the vessel against the tentorium TIA diagnosis Patients with history of trauma and recurrent epistaxis, visual loss, progressive cranial nerve palsy or an enlarging skull fracture MRI/MRA/CTA Arteriography Delayed formation of aneurysms








8 Pericallosal and callosomarginal arteries 29,7% 21,6% Peripheral MCA Anterior aspect of the cavernous ICA Petrous internal carotid artery ICA just below the skull base











9






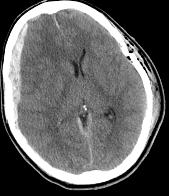
10 Secondary lesions The secondary effects of craniocerebral trauma may be more devastating than the primary injuries. Secondary lesions are those that develop subsequent to initial impact. They arise from Either sequelae of primary lesions Or the neurologic effects of systemic injuries Secondary lesions, are potentially preventable, provided that causative factors are quickly recognized and appropiate treatment promptly instituted.
11 BRAIN INJURY BRAIN INJURY Tissue damage Ischemia Cerebral swelling/edema Cell lesion Cytotoxic edema Ruptured BBB Vasogenic edema Cerebral vasoplegia Brain swelling hypoxia hypercapnia ischemia CBF CPP ICP Loss of autoregulation vasoparalysis hypotension Evaluation of relevant CT scan findings Status of the basal cisterns Midline shift Subarachnoid hemorrhage in the basal cisterns

 Midline shift The presence of midline shift is inversely related to prognosis.")
12 Status of the basal cisterns Compressed or absent basal cisterns indicate a threefold risk of raised intracranial pressure and the status of the basal cisterns is related to outcome. The degree of mass effect is evaluated at the level of midbrain: Open (all limbs open) Partially closed (one or two limbs obliterated) Completely closed (all limbs obliterated) Midline shift The presence of midline shift is inversely related to prognosis. Midline shift at the level of foramen of Monro should be determined by first measuring the width of the intracranial space (A); next the distance from the bone to the septum pellucidum is measured (B). Midline shift = (A/2)-B. B A

:217-228.")

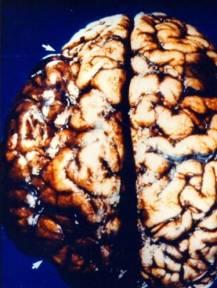
13 Subfalcine h. Transtentorial h. Lateral Different types of cerebral herniations Anterior=uncal Posterior=parahyppocampal Central Ascending Descending Transsphenoidal h. Descending Ascending Tonsillar h. External h. Johnson PL et al. Neuroimag Clin N Am 12(2002): Subfalcine herniation It is caused by unilateral frontal, parietal or temporal lobe mass effect or edema The ipsilateral cingulated gyrus is pushed down and under the rigid midline falx Owing to arterial compression: Focal necrosis of the cingulated gyrus Infarction involving the ACA territory

14 Transtentorial herniation Symptoms may result from displacement, compression and stretching of the brainstem and cranial nerves Hemorrhage and infarction caused by compression and tearing of arteries and veins Increasing edema and intracranial pressure caused by venous obstruction Hydrocephalus caused by obstruction of the aqueduct. Rhoton AJ. Neurosurgery 2000, 47:S







15 Day 0 Day 2 Day 2 Day 2 Day 2





16
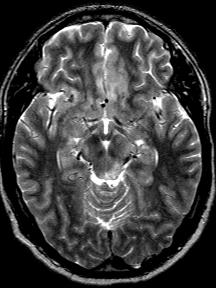
17 Post-traumatic traumatic cerebral infarction Mechanisms Direct vascular compression by mass effect (81-88%) 88%) Cerebral vasospasm Vascular injury Systemic hypoperfusion PTCI PTCI is most common in the PCA distribution PTCI is an indication of a poor clinical outcome, especially among patients with: Associated subdural hematoma Brain swelling/edema edema tsah

:254-260.")
18 DISTRIBUTION OF POSTTRAUMATIC CEREBRAL INFARCTION IN 16 PATIENTS vascular territory PCA 37,5% MCA 20,8% ACA 12,5% L-TT 8,3% VBT 12,5% CI 8,3 Server A et al. Acta radiologica 2001 (42): Day 0 Day 1






19







20 Outcome in patients with PTCI 6.2% 25% 12.5% 12,.5% 43.8% good recovery moderate disability severe disability vegetative state death Server A et al. Acta radiologica 2001 (42):
21 Traumatic cerebral edema/swelling Vasogenic due to blod-brain brain barrier disruption extracellular water accumulation Cytotoxic/cellular due to sustained intracellular water accumulation Osmotic caused by osmotic inbalances between brain and tissue Hydrocephalic edema/interstitial from edema related to an obstruction of CSF outflow Early Traumatic diffuse cerebral edema/swelling Gyral swelling, sulcal effacement,, loss of gray- white matter interface Late Diffuse low attenuation of the brain, generalized effacement of subarachnoid cisterns Pseudosubarachnoid hemorrhage White cerebellum sign The reversal sign








22 Day 1 Day 2 Day 3











23 4 months later









24










25





26 Sequelae of head trauma Early Delayed intracerebral hematoma Delayed subdural hematoma Delayed epidural hematoma CSF leak or fistula Late Cerebral atrophy Cerebellar atrophy Atrophy of the corpus callosum Acquired cephalocele Leptomeningeal cyst hypopituitarism




27 Leptomeningeal cyst When a skull fracture is accompanied by a tear of the dura, meninges and brain tissue may herniate into the fracture, preventing healing of the fractures and permiting cerebrospinal fluid pulsation to enlarge the fracture and extent into the subgaleal space. 90%< 3 years. The average time of diagnosis is 14 months after the initial fracture. 1 year later





28 Post-traumatic traumatic hydrocephalus PTH as low as 0,7% or as high as 20% PTH can present acutely, subacutely and syndrome of NPH PTH is to be distinguished from posttraumatic ventriculomegaly due to cerebral atrophy The appropiate management of these patients include: Study of CSF dynamics And/or ICP monitoring






29 Day-0 Day-3 Day-18 Day-21 Day-30 Day-42 Traumatic cerebrospinal fluid leak Acute CSF fistulas occur in 2 to 11% of all patients with closed head trauma 70% occurs within 1 week CT-cisternography High-definition CT alone MRI-CISS







30

31 conclusion CTA has been shown to be a good non-invasive alternative tecnique to catheter angiography for the initial assessment of cerebrovascular trauma and vascular injuries of the neck. Neuroimaging is playing a crucial role in defining the mechanisms of secondary injury in traumatic brain injury and, in turn, potentially identifying targets of new therapy. CT is adequate in the evaluation for early onset of sequelae of head trauma.. MRI is the modality of choice for evaluation of subacute and later onset of delayed sequelae of head trauma. Radiology in traumatic brain injury has a bright future.
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
Principles Arteries & Veins of the CNS LO14
 Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD
 Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Multidetector CTA for Diagnosing Blunt Cerebrovascular Injuries
 Multidetector CTA for Diagnosing Blunt Cerebrovascular Injuries 4 th Nordic Trauma Course 2006 Stuart E. Mirvis, M.D., FACR Department of Diagnostic Radiology and Nuclear Medicine, University of Maryland
Multidetector CTA for Diagnosing Blunt Cerebrovascular Injuries 4 th Nordic Trauma Course 2006 Stuart E. Mirvis, M.D., FACR Department of Diagnostic Radiology and Nuclear Medicine, University of Maryland
Meninges and Ventricles
 Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
What Are We Going to Do? Fourth Year Meds Clinical Neuroanatomy. Hydrocephalus and Effects of Interruption of CSF Flow. Tube Blockage Doctrine
 Fourth Year Meds Clinical Neuroanatomy Ventricles, CSF, Brain Swelling etc. David A. Ramsay, Neuropathologist, LHSC What Are We Going to Do? Hydrocephalus and some effects of the interruption of CSF flow
Fourth Year Meds Clinical Neuroanatomy Ventricles, CSF, Brain Swelling etc. David A. Ramsay, Neuropathologist, LHSC What Are We Going to Do? Hydrocephalus and some effects of the interruption of CSF flow
Post traumatic vertebro basilar dissection: case report and review of literature
 Romanian Neurosurgery Volume XXXI Number 3 2017 July-September Article Post traumatic vertebro basilar dissection: case report and review of literature Karthikeyan Y.R., Sanjeev Chopra, Somnath Sharma,
Romanian Neurosurgery Volume XXXI Number 3 2017 July-September Article Post traumatic vertebro basilar dissection: case report and review of literature Karthikeyan Y.R., Sanjeev Chopra, Somnath Sharma,
HEAD AND NECK IMAGING. James Chen (MS IV)
") HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
For Emergency Doctors. Dr Suzanne Smallbane November 2011
 For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
Characteristic features of CNS pathology. By: Shifaa AlQa qa
 Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
ISCHEMIC STROKE IMAGING
 ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
PTA 106 Unit 1 Lecture 3
 PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
Pathological reaction to disease
 Chapter1 Pathological reaction to disease Normal anatomy Figures 1.1 1.6 2 4 Brain swelling and internal herniation Figures 1.7 1.15 5 9 Epilepsy Figures 1.16 1.18 9 10 Cerebellar atrophy Figures 1.19
Chapter1 Pathological reaction to disease Normal anatomy Figures 1.1 1.6 2 4 Brain swelling and internal herniation Figures 1.7 1.15 5 9 Epilepsy Figures 1.16 1.18 9 10 Cerebellar atrophy Figures 1.19
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases
 How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
NEURO IMAGING OF ACUTE STROKE
 1 1 NEURO IMAGING OF ACUTE STROKE ALICIA RICHARDSON, MSN, RN, ACCNS-AG, ANVP-BC WENDY SMITH, MA, RN, MBA, SCRN, FAHA LYNN HUNDLEY, APRN, CNRN, CCNS, ANVP-BC 2 2 1 DISCLOSURES Alicia Richardson: Stryker
1 1 NEURO IMAGING OF ACUTE STROKE ALICIA RICHARDSON, MSN, RN, ACCNS-AG, ANVP-BC WENDY SMITH, MA, RN, MBA, SCRN, FAHA LYNN HUNDLEY, APRN, CNRN, CCNS, ANVP-BC 2 2 1 DISCLOSURES Alicia Richardson: Stryker
Non-Traumatic Neuro Emergencies
 Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
CNS pathology Third year medical students,2019. Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Essentials of Clinical MR, 2 nd edition. 14. Ischemia and Infarction II
 14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
NEURORADIOLOGY DIL part 3
 NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
Case Conference: Neuroradiology. Case 1: Tumor Case 1: 22yo F w/ HA and prior Seizures
 Case Conference: Neuroradiology Case 1: 22yo F w/ HA and prior Seizures David E. Rex, MD, PhD Stanford University Hospital Department of Radiology Case 1: Tumor Most likely gangiloglioma, oligodendroglioma,
Case Conference: Neuroradiology Case 1: 22yo F w/ HA and prior Seizures David E. Rex, MD, PhD Stanford University Hospital Department of Radiology Case 1: Tumor Most likely gangiloglioma, oligodendroglioma,
STROKE - IMAGING. Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli.
 STROKE - IMAGING Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli. STROKE Describes a clinical event that consists of sudden onset of neurological symptoms Types Infarction - occlusion of
STROKE - IMAGING Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli. STROKE Describes a clinical event that consists of sudden onset of neurological symptoms Types Infarction - occlusion of
Brain Meninges, Ventricles and CSF
 Brain Meninges, Ventricles and CSF Lecture Objectives Describe the arrangement of the meninges and their relationship to brain and spinal cord. Explain the occurrence of epidural, subdural and subarachnoid
Brain Meninges, Ventricles and CSF Lecture Objectives Describe the arrangement of the meninges and their relationship to brain and spinal cord. Explain the occurrence of epidural, subdural and subarachnoid
CT INTERPRETATION COURSE
 CT INTERPRETATION COURSE Refresher Course ASTRACAT October 2012 Stroke is a Clinical Diagnosis A clinical syndrome characterised by rapidly developing clinical symptoms and/or signs of focal loss of cerebral
CT INTERPRETATION COURSE Refresher Course ASTRACAT October 2012 Stroke is a Clinical Diagnosis A clinical syndrome characterised by rapidly developing clinical symptoms and/or signs of focal loss of cerebral
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
NEURORADIOLOGY DIL part 4
 NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
Cerebro-vascular stroke
 Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
North Oaks Trauma Symposium Friday, November 3, 2017
 Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN
 CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
Cerebral aneurysms A case study
 August 2001 Cerebral aneurysms A case study Heather L. Hinds, Harvard Medical School Year III Our Patient 57yr old woman History of migraines Presents with persistent headache several months duration different
August 2001 Cerebral aneurysms A case study Heather L. Hinds, Harvard Medical School Year III Our Patient 57yr old woman History of migraines Presents with persistent headache several months duration different
HEAD/NECK VESSELS. Objectives
 Objectives Arterial Supply to Head and Neck Arteries to Head Surrounding Brain Common carotid arteries Arteries to Head Surrounding Brain External carotid arteries Arteries to Head Surrounding Brain External
Objectives Arterial Supply to Head and Neck Arteries to Head Surrounding Brain Common carotid arteries Arteries to Head Surrounding Brain External carotid arteries Arteries to Head Surrounding Brain External
Head trauma - interpreting CT scans
 Head trauma - interpreting CT scans Poster No.: C-2075 Congress: ECR 2014 Type: Educational Exhibit Authors: T. Rihtar; Zagreb/HR Keywords: Trauma, Hemorrhage, Edema, Diagnostic procedure, CT, Neuroradiology
Head trauma - interpreting CT scans Poster No.: C-2075 Congress: ECR 2014 Type: Educational Exhibit Authors: T. Rihtar; Zagreb/HR Keywords: Trauma, Hemorrhage, Edema, Diagnostic procedure, CT, Neuroradiology
Cerebral hemisphere. Parietal Frontal Occipital Temporal
 Cerebral hemisphere Sulcus / Fissure Central Precental gyrus Postcentral gyrus Lateral (cerebral) Parieto-occipital Cerebral cortex Frontal lobe Parietal lobe Temporal lobe Insula Amygdala Hippocampus
Cerebral hemisphere Sulcus / Fissure Central Precental gyrus Postcentral gyrus Lateral (cerebral) Parieto-occipital Cerebral cortex Frontal lobe Parietal lobe Temporal lobe Insula Amygdala Hippocampus
Index. aneurysm, 92 carotid occlusion, 94 ICA stenosis, 95 intracranial, 92 MCA, 94
 A ADC. See Apparent diffusion coefficient (ADC) Aneurysm cerebral artery aneurysm, 93 CT scan, 93 gadolinium, 93 Angiography, 13 Anoxic brain injury, 25 Apparent diffusion coefficient (ADC), 7 Arachnoid
A ADC. See Apparent diffusion coefficient (ADC) Aneurysm cerebral artery aneurysm, 93 CT scan, 93 gadolinium, 93 Angiography, 13 Anoxic brain injury, 25 Apparent diffusion coefficient (ADC), 7 Arachnoid
Neuroradiological Findings in Non- Accidental Trauma Educational Pictorial Review
 Neuroradiological Findings in Non- Accidental Trauma Educational Pictorial Review M B Moss, MD; L Lanier, MD; R Slater; C L Sistrom, MD; R G Quisling, MD; I M Schmalfuss, MD; and D Rajderkar, MD Contact:
Neuroradiological Findings in Non- Accidental Trauma Educational Pictorial Review M B Moss, MD; L Lanier, MD; R Slater; C L Sistrom, MD; R G Quisling, MD; I M Schmalfuss, MD; and D Rajderkar, MD Contact:
Neuroanatomy Dr. Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018
 Neuroanatomy Dr. Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018 Blood Supply of Brain and Spinal Cord Arterial Supply of Brain The brain receives blood
Neuroanatomy Dr. Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018 Blood Supply of Brain and Spinal Cord Arterial Supply of Brain The brain receives blood
OBJECTIVES. At the end of the lecture, students should be able to: List the cerebral arteries.
 DR JAMILA EL MEDANY OBJECTIVES At the end of the lecture, students should be able to: List the cerebral arteries. Describe the cerebral arterial supply regarding the origin, distribution and branches.
DR JAMILA EL MEDANY OBJECTIVES At the end of the lecture, students should be able to: List the cerebral arteries. Describe the cerebral arterial supply regarding the origin, distribution and branches.
INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU
 CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
The dura is sensitive to stretching, which produces the sensation of headache.
 Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
Screening and Management of Blunt Cereberovascular Injuries (BCVI)
") Grady Memorial Hospital Trauma Service Guidelines Screening and Management of Blunt Cereberovascular Injuries (BCVI) BACKGROUND Blunt injury to the carotid or vertebral vessels (blunt cerebrovascular injury
Grady Memorial Hospital Trauma Service Guidelines Screening and Management of Blunt Cereberovascular Injuries (BCVI) BACKGROUND Blunt injury to the carotid or vertebral vessels (blunt cerebrovascular injury
M555 Medical Neuroscience Blood Flow in CNS Meninges Blood Brain Barrier CSF
 M555 Medical Neuroscience Blood Flow in CNS Meninges Blood Brain Barrier CSF Arterial Blood Flow to CNS approximately % of what goes wrong within the skull that produces neurological deficits is vascular
M555 Medical Neuroscience Blood Flow in CNS Meninges Blood Brain Barrier CSF Arterial Blood Flow to CNS approximately % of what goes wrong within the skull that produces neurological deficits is vascular
Bilateral blunt carotid artery injury: A case report and review of the literature
 CASE REPORT Bilateral blunt carotid artery injury: A case report and review of the literature S Cheddie, 1 MMed (Surg), FCS (SA); B Pillay, 2 FCS (SA), Cert Vascular Surgery; R Goga, 2 FCS (SA) 1 Department
CASE REPORT Bilateral blunt carotid artery injury: A case report and review of the literature S Cheddie, 1 MMed (Surg), FCS (SA); B Pillay, 2 FCS (SA), Cert Vascular Surgery; R Goga, 2 FCS (SA) 1 Department
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Tutorials. By Dr Sharon Truter
 Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
Blood Supply. Allen Chung, class of 2013
 Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Applicable Neuroradiology
 For the Clinical Neurology Clerkship LSU Medical School New Orleans Amy W Voigt, MD Clerkship Director Introduction The field of Radiology first developed following the discovery of X-Rays by Wilhelm Roentgen
For the Clinical Neurology Clerkship LSU Medical School New Orleans Amy W Voigt, MD Clerkship Director Introduction The field of Radiology first developed following the discovery of X-Rays by Wilhelm Roentgen
2. Subarachnoid Hemorrhage
 Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Neuro Quiz 29 Transcranial Doppler Monitoring
 Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
The central nervous system
 Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Dural Arteriovenous Malformations and Fistulae (DAVM S DAVF S)
") Jorge Guedes Campos NEUROIMAGING DEPARTMENT HOSPITAL SANTA MARIA UNIVERSITY OF LISBON PORTUGAL DEFINITION region of arteriovenous shunting confined to a leaflet of packymeninges often adjacent to a major
Jorge Guedes Campos NEUROIMAGING DEPARTMENT HOSPITAL SANTA MARIA UNIVERSITY OF LISBON PORTUGAL DEFINITION region of arteriovenous shunting confined to a leaflet of packymeninges often adjacent to a major
Imaging of Acute Cerebral Trauma
 July, 2005 Imaging of Acute Cerebral Trauma Louis Rivera, Harvard Medical School, Year III 46 y/o Female s/p Trauma - Unrestrained? MVC requiring Med Flight - Facial bruising/swelling - DEEP COMA - SEIZURES
July, 2005 Imaging of Acute Cerebral Trauma Louis Rivera, Harvard Medical School, Year III 46 y/o Female s/p Trauma - Unrestrained? MVC requiring Med Flight - Facial bruising/swelling - DEEP COMA - SEIZURES
4The head basic anatomy and physiology
 Hene_Ch04.qxd 8/30/04 2:47 AM Page 108 108 THE HEAD BASIC ANATOMY AND PHYSIOLOGY 4The head basic anatomy and physiology The scalp Anatomists describe the SCALP as having five layers: Skin, Subcutaneous
Hene_Ch04.qxd 8/30/04 2:47 AM Page 108 108 THE HEAD BASIC ANATOMY AND PHYSIOLOGY 4The head basic anatomy and physiology The scalp Anatomists describe the SCALP as having five layers: Skin, Subcutaneous
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
TCD IN THE NICU, PICU AND OTHER APPLICATIONS. Dorothy Bulas M.D. Professor of Pediatrics & Radiology Children s National Washington D.C.
 TCD IN THE NICU, PICU AND OTHER APPLICATIONS Dorothy Bulas M.D. Professor of Pediatrics & Radiology Children s National Washington D.C. Objectives Recognize normal and abnormal cranial blood flow patterns
TCD IN THE NICU, PICU AND OTHER APPLICATIONS Dorothy Bulas M.D. Professor of Pediatrics & Radiology Children s National Washington D.C. Objectives Recognize normal and abnormal cranial blood flow patterns
An Introduction to Imaging the Brain. Dr Amy Davis
 An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN
 Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN History of Marshall scale Proposed by Marshall, et al in 1991 to classify head
Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN History of Marshall scale Proposed by Marshall, et al in 1991 to classify head
TRANSVERSE SECTION PLANE Scalp 2. Cranium. 13. Superior sagittal sinus
 TRANSVERSE SECTION PLANE 1 1. Scalp 2. Cranium 3. Superior sagittal sinus 4. Dura mater 5. Falx cerebri 6. Frontal lobes of the cerebrum 7. Middle meningeal artery 8. Cortex, grey matter 9. Cerebral vessels
TRANSVERSE SECTION PLANE 1 1. Scalp 2. Cranium 3. Superior sagittal sinus 4. Dura mater 5. Falx cerebri 6. Frontal lobes of the cerebrum 7. Middle meningeal artery 8. Cortex, grey matter 9. Cerebral vessels
Unit 18: Cranial Cavity and Contents
 Unit 18: Cranial Cavity and Contents Dissection Instructions: The calvaria is to be removed without damage to the dura mater which is attached to the inner surface of the calvaria. Cut through the outer
Unit 18: Cranial Cavity and Contents Dissection Instructions: The calvaria is to be removed without damage to the dura mater which is attached to the inner surface of the calvaria. Cut through the outer
Medical Neuroscience Tutorial Notes
 Medical Neuroscience Tutorial Notes Blood Supply to the Brain MAP TO NEUROSCIENCE CORE CONCEPTS 1 NCC1. The brain is the body's most complex organ. LEARNING OBJECTIVES After study of the assigned learning
Medical Neuroscience Tutorial Notes Blood Supply to the Brain MAP TO NEUROSCIENCE CORE CONCEPTS 1 NCC1. The brain is the body's most complex organ. LEARNING OBJECTIVES After study of the assigned learning
Neurosonography: State of the art
 Neurosonography: State of the art Lisa H Lowe, MD, FAAP Professor and Academic Chair, University MO-Kansas City Pediatric Radiologist, Children s Mercy Hospitals and Clinics Learning objectives After this
Neurosonography: State of the art Lisa H Lowe, MD, FAAP Professor and Academic Chair, University MO-Kansas City Pediatric Radiologist, Children s Mercy Hospitals and Clinics Learning objectives After this
The Skull, the Brain, the Meninges, and the Blood Supply of the Brain Relative to Trauma and Intracranial 14Hemorrhage
 The Nervous System The Skull, the Brain, the Meninges, and the Blood Supply of the Brain Relative to Trauma and Intracranial 14Hemorrhage Chapter Outline The Skull 213 The Thinnest Part of the Lateral
The Nervous System The Skull, the Brain, the Meninges, and the Blood Supply of the Brain Relative to Trauma and Intracranial 14Hemorrhage Chapter Outline The Skull 213 The Thinnest Part of the Lateral
Management of cervicocephalic arterial dissection. Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery
 Management of cervicocephalic arterial dissection Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery Definition Disruption of arterial wall, either at level of intima-media
Management of cervicocephalic arterial dissection Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery Definition Disruption of arterial wall, either at level of intima-media
Unusual Posttraumatic Vascular and Cerebral Injuries in Young Patients
 224 Marciuc et al - Unusual Posttraumatic Vascular and Cerebral Injuries in Young Patients DOI: 10.2478/romneu-2018-0029 Unusual Posttraumatic Vascular and Cerebral Injuries in Young Patients Emilia Marciuc
224 Marciuc et al - Unusual Posttraumatic Vascular and Cerebral Injuries in Young Patients DOI: 10.2478/romneu-2018-0029 Unusual Posttraumatic Vascular and Cerebral Injuries in Young Patients Emilia Marciuc
6th Nordic Trauma Radiology Course
 Imaging of the Injured Cervical Spine 6th Nordic Trauma Radiology Course Stuart E. Mirvis, MD, FACR University of Maryland School of Medicine #1 R/O Spinal Injury: Does radiography still have a role in
Imaging of the Injured Cervical Spine 6th Nordic Trauma Radiology Course Stuart E. Mirvis, MD, FACR University of Maryland School of Medicine #1 R/O Spinal Injury: Does radiography still have a role in
V. CENTRAL NERVOUS SYSTEM TRAUMA
 V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
+ Why screen? BCVI relatively rare- about 0.5-2%
 Kathleen R. Fink, MD University of Washington UW Medicine EMS & Trauma Conference September 27, 2016 Why screen? BCVI relatively rare- about 0.5-2% (0.075% 1.55%) Catastrophic potential (stroke) Aggressive
Kathleen R. Fink, MD University of Washington UW Medicine EMS & Trauma Conference September 27, 2016 Why screen? BCVI relatively rare- about 0.5-2% (0.075% 1.55%) Catastrophic potential (stroke) Aggressive
Role of the Radiologist
 Diagnosis and Treatment of Blunt Cerebrovascular Injuries NORDTER Consensus Conference October 22-24, 2007 Clint W. Sliker, M.D. University of Maryland Medical Center R Adams Cowley Shock Trauma Center
Diagnosis and Treatment of Blunt Cerebrovascular Injuries NORDTER Consensus Conference October 22-24, 2007 Clint W. Sliker, M.D. University of Maryland Medical Center R Adams Cowley Shock Trauma Center
Brain ميهاربا لض اف دمح ا د The Meninges 1- Dura Mater of the Brain endosteal layer does not extend meningeal layer falx cerebri tentorium cerebelli
 .احمد د فاضل ابراهيم Lecture 15 Brain The Meninges Three protective membranes or meninges surround the brain in the skull: the dura mater, the arachnoid mater, and the pia mater 1- Dura Mater of the Brain
.احمد د فاضل ابراهيم Lecture 15 Brain The Meninges Three protective membranes or meninges surround the brain in the skull: the dura mater, the arachnoid mater, and the pia mater 1- Dura Mater of the Brain
Internal Carotid Artery Dissection
 May 2011 Internal Carotid Artery Dissection Carolyn April, HMS IV Agenda Presentation of a clinical case Discussion of the clinical features of ICA dissection Discussion of the imaging modalities used
May 2011 Internal Carotid Artery Dissection Carolyn April, HMS IV Agenda Presentation of a clinical case Discussion of the clinical features of ICA dissection Discussion of the imaging modalities used
BRAIN HERNIATION S54 (1) Brain Herniation
 Brain Herniation") BRAIN HERNIATION S54 (1) Brain Herniation Last updated: September 5, 2017 PATHOPHYSIOLOGY... 1 TYPES OF HERNIATION... 2 SUPRATENTORIAL MASSES... 2 Central (s. downward transtentorial) herniation... 2 Uncal
BRAIN HERNIATION S54 (1) Brain Herniation Last updated: September 5, 2017 PATHOPHYSIOLOGY... 1 TYPES OF HERNIATION... 2 SUPRATENTORIAL MASSES... 2 Central (s. downward transtentorial) herniation... 2 Uncal
Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT
 Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT Val M. Runge, MD Wendy R. K. Smoker, MD Anton Valavanis, MD Control # 823 Purpose The focus of this educational
Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT Val M. Runge, MD Wendy R. K. Smoker, MD Anton Valavanis, MD Control # 823 Purpose The focus of this educational
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD
 Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
Medical Review Guidelines Magnetic Resonance Angiography
 Medical Review Guidelines Magnetic Resonance Angiography Medical Guideline Number: MRG2001-05 Effective Date: 2/13/01 Revised Date: 2/14/2006 OHCA Reference OAC 317:30-5-24. Radiology. (f) Magnetic Resonance
Medical Review Guidelines Magnetic Resonance Angiography Medical Guideline Number: MRG2001-05 Effective Date: 2/13/01 Revised Date: 2/14/2006 OHCA Reference OAC 317:30-5-24. Radiology. (f) Magnetic Resonance
Blood Supply of the CNS
 Blood Supply of the CNS Lecture Objectives Describe the four arteries supplying the CNS. Follow up each artery to its destination. Describe the circle of Willis and its branches. Discuss the principle
Blood Supply of the CNS Lecture Objectives Describe the four arteries supplying the CNS. Follow up each artery to its destination. Describe the circle of Willis and its branches. Discuss the principle
Benign brain lesions
 Benign brain lesions Diagnostic and Interventional Radiology Hung-Wen Kao Department of Radiology, Tri-Service General Hospital, National Defense Medical Center Computed tomography Hounsfield unit (HU)
Benign brain lesions Diagnostic and Interventional Radiology Hung-Wen Kao Department of Radiology, Tri-Service General Hospital, National Defense Medical Center Computed tomography Hounsfield unit (HU)
History of revascularization
 History of revascularization Author (year) Kredel, 1942 Woringer& Kunlin, 1963 Donaghy& Yasargil, 1968 Loughheed 1971 Kikuchini & Karasawa1973 Karasawa, 1977 Story, 1978 Sundt, 1982 EC/IC bypass study
History of revascularization Author (year) Kredel, 1942 Woringer& Kunlin, 1963 Donaghy& Yasargil, 1968 Loughheed 1971 Kikuchini & Karasawa1973 Karasawa, 1977 Story, 1978 Sundt, 1982 EC/IC bypass study
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage. By: Shifaa AlQa qa
 CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
Spasm of the extracranial internal carotid artery resulting from blunt trauma demonstrated by angiography
 Spasm of the extracranial internal carotid artery resulting from blunt trauma demonstrated by angiography Case report ELISHA S. GURDJIAN, M.D., BLAISE AUDET, M.D., RENATO W. SIBAYAN, M.D., AND LLYWELLYN
Spasm of the extracranial internal carotid artery resulting from blunt trauma demonstrated by angiography Case report ELISHA S. GURDJIAN, M.D., BLAISE AUDET, M.D., RENATO W. SIBAYAN, M.D., AND LLYWELLYN
Neurotrauma. Béla Faludi Dept.. of Neurology University of PécsP
 Neurotrauma Béla Faludi Dept.. of Neurology University of PécsP Emergency!!! Why here? Opened cranial injury visible: neurosurgery Closed injuries sometimes diagnosed by neurologist Masking situation:
Neurotrauma Béla Faludi Dept.. of Neurology University of PécsP Emergency!!! Why here? Opened cranial injury visible: neurosurgery Closed injuries sometimes diagnosed by neurologist Masking situation:
CEREBROVASCULAR DISEASES. By: Shifaa AlQa qa
 CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins
 ISPUB.COM The Internet Journal of Radiology Volume 18 Number 1 Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins K Kragha Citation K Kragha. Cryptogenic Enlargement Of Bilateral Superior Ophthalmic
ISPUB.COM The Internet Journal of Radiology Volume 18 Number 1 Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins K Kragha Citation K Kragha. Cryptogenic Enlargement Of Bilateral Superior Ophthalmic
Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage
 Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
intracranial anomalies
 Chapter 5: Fetal Central Nervous System 84 intracranial anomalies Hydrocephaly Dilatation of ventricular system secondary to an increase in the amount of CSF. Effects of hydrocephalus include flattening
Chapter 5: Fetal Central Nervous System 84 intracranial anomalies Hydrocephaly Dilatation of ventricular system secondary to an increase in the amount of CSF. Effects of hydrocephalus include flattening
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Attenuation value in HU From -500 To HU From -10 To HU From 60 To 90 HU. From 200 HU and above
 Brain Imaging Common CT attenuation values Structure Air Fat Water Brain tissue Recent hematoma Calcifications Bone Brain edema and infarction Normal liver parenchyma Attenuation value in HU From -500
Brain Imaging Common CT attenuation values Structure Air Fat Water Brain tissue Recent hematoma Calcifications Bone Brain edema and infarction Normal liver parenchyma Attenuation value in HU From -500
TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION
 TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION ---Rune Aaslid First TCD Publication 1982 WHAT IS TCD? Uses 2 MHz pulsed Doppler ultrasound Passes through cranial windows Provides information
TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION ---Rune Aaslid First TCD Publication 1982 WHAT IS TCD? Uses 2 MHz pulsed Doppler ultrasound Passes through cranial windows Provides information
Spontaneous Intracranial Hypotension Diagnosis and Treatment
 Spontaneous Intracranial Hypotension Diagnosis and Treatment John W. Engstrom MD, Philip R. Weinstein MD, and William P. Dillon M.D. University of California, San Francisco Spontaneous Intracranial Hypotension
Spontaneous Intracranial Hypotension Diagnosis and Treatment John W. Engstrom MD, Philip R. Weinstein MD, and William P. Dillon M.D. University of California, San Francisco Spontaneous Intracranial Hypotension
Interventions in the Management of Acute Stroke. Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital
 Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the