University of Zurich. Normal valves. Zurich Open Repository and Archive. Bettex, D; Chassot, P G. Year: 2010
|
|
|
- Jeffery Daniel
- 5 years ago
- Views:
Transcription

1 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich Year: 2010 Normal valves Bettex, D; Chassot, P G Bettex, D; Chassot, P G (2010). Normal valves. In: Feneck, R; Kneeshaw, J; Ranucci, M. Core topics in transesophageal echocardiography. Cambridge, Postprint available at: Posted at the Zurich Open Repository and Archive, University of Zurich. Originally published at: Feneck, R; Kneeshaw, J; Ranucci, M Core topics in transesophageal echocardiography. Cambridge,
2 Normal Valves, TOE assessment Dominique A Bettex, M.D.; Pierre-Guy Chassot, M.D. Introduction Transoesophageal echocardiography (TOE) is a well known and accepted technique to assess valvular anatomy, function and pathology. A careful and complete assessment of the different valves of the heart should be part of routine TOE examination. The Council for intraoperative TOE 1 created guidelines for performing a comprehensive examination composed of a set of anatomically directed cross-sectional views. This document is the collective result of an effort that represents the consensus view of both anaesthesiologists and cardiologists who have extensive experience in perioperative echocardiography. We will be using mostly their standardized approach to assess the four valves of the heart. The mitral valve Anatomy Mitral valve (MV) anatomy is a complex entity constituted of 6 different parts: 2 leaflets, 120 chordae tendinae (20 on the edges), 2 papillary muscles, the annulus, the fibrous skeleton of the heart and the left ventricular walls. During diastole, the MV allows rapid filling of the left ventricle under low pressure and minimal gradient (smaller then 4
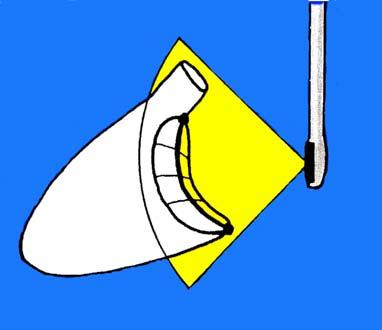
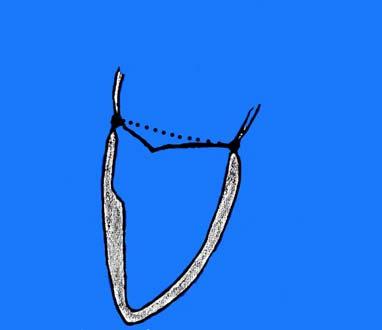
3 mmhg). The degree of opening of the leaflets reaches about 70 and the MV opening surface is 4 to 6 cm 2. During systole, the MV has to oppose resistance against the high left ventricular pressures (up to 200 mmhg). The intraventricular pressure applies the leaflets again each other on the coaptation surface called zona rugosa. The coaptation surface results from an active balance between closing and tethering forces (Figure 1). A dilatation of the annulus will lead to a diminution of this surface and to an imbalance of these forces; a mitral regurgitation (MR) will ensue. Normal MV function depends upon the complex interactions of all the different components of the valve. The anterior leaflet covers the 2/3 of the valve orifice but occupies 1/3 of the annulus circumference. The posterior leaflet occupies approximately 2/3 of the annulus circumference but covers only 1/3 of the valve orifice. The base of the anterior leaflet lies in closed proximity to the left and non-coronary cusps of the aortic valve. The combined surface area of the mitral leaflets is twice that of the mitral orifice, permitting large areas of coaptation. The two leaflets are joined at the anterolateral and posteromedial commissures, each of which is associated with a corresponding papillary muscle. Following Carpentier nomenclature (Figure 2), the posterior leaflet consists of three scallops: lateral (P1), middle (P2) and medial (P3); for descriptive purposes, the anterior leaflet is also divided into three parts: lateral third (A1), middle third (A2) and medial third (A3). The annulus is composed of fibroblastic tissue and completely encircles the orifice in a cone like shape. During systole, the annulus is a saddle-shaped ellipse, whereas it is almost round at end-diastole.this saddle-shape is particularly relevant for the diagnosis of a mitral valve prolapse as far as the level of the annulus will appear deeper in the
4 ventricular cavity in the transverse view (0 ) as in the longitudinal one (120 ) 2 (Figure 3). To avoid false positives, the diagnosis of mitral valve prolapse should be done exclusively in the longitudinal view. The mean mitral valve annular diameter for normal individuals varies between 20 and 38 mm at early diastole. It varies depending on the plan of visualisation due to its elliptic or D-shape (Figure 4). The annulus fibrosus of the mitral annulus becomes thinner and poorly defined as it extends posteriorly from the left and right trigones. This portion of the annulus is poorly supported and is prone to dilatation. The posterior leaflet of the mitral valve attaches to this portion of the annulus. Dilatation of the annular attachment of the posterior leaflet creates an increased tension on the middle scallop (P2) of the posterior leaflet explaining why 60% of chordal tears occur at the P2 scallop. The chordae tendinae are strong fibrous chords extending from the margins of the leaflets to the papillary muscles. They are divided into first order chordae if they insert into the free edge of the leaflets, second order if they insert into the ventricular side of the leaflets and third order if they insert into the basis of the leaflets. The chordae from both papillary muscles insert into both leaflets. The papillary muscles are large trabeculae carnae. Each papillary muscle has a consistent relationship with its respective commissural area (anterolateral and posteromedial). The antero-lateral one is more commonly supplied by 2 separate arteries, the left anterior descending and circumflex coronary arteries, while a single artery supplies the posterior papillary muscle: the posterior descending coronary artery arising most of the time from the right coronary artery. This explains the greater incidence of posterior papillary muscle dysfunction or rupture due to ischemia. The subvalvular apparatus pulls the annulus and base of the heart toward the ventricular
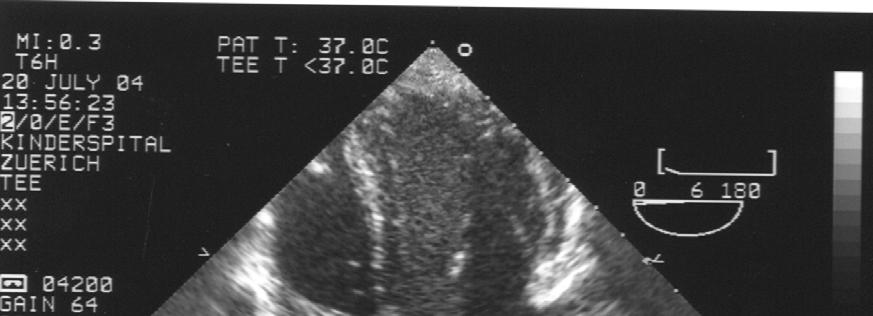
5 apex during systole thereby shortening the longitudinal axis of the left ventricle (LV). It provides support for the leaflets, facilitating coaptation and preventing prolapse. Bidimensional imaging Lambert et al 3 developed a systematic MV examination to improve intraoperative identification of mitral segments, precise localisation of the pathology, and determine the mechanism of MR. TOE correctly identified 96% of mitral segments as being normal or abnormal in the prospective group. In the retrospective study (non systematic assessment), 70% of segments only were correctly identified. They concluded that a systematic approach improves identification of mitral segments and of precise localisation of pathologies and may improve the diagnosis of the mechanism of MR. The MV is examined through four mid-oesophageal and two transgastric views. The mid oesophageal views are all developed by first positioning the transducer posterior to the mid level of the left atrium (LA), approximately 30 to 35 cm distal to the incisors, and directing the imaging plane through the mitral annulus parallel to the transmitral flow. Retroflexion of the probe is often necessary. The multiplane angle is then rotated forward to develop the mid oesophageal 4-chamber view (Figure 5). The posterior leaflet P1 is to the right of the image display, and the anterior mitral leaflet A3 is to the left. The multiplane angle is further rotated to 60 ; a transition in the image occurs beyond which the posterior leaflet is to the left of the display and the anterior to the right (Figure 6). At this transition angle, the imaging plane is parallel to the line that intersects the two commissures of the MV and forms the mid oesophageal mitral commissural view. P1 is to the right of the display, P3 is to the left, A2 or P2 is in the middle of the display,
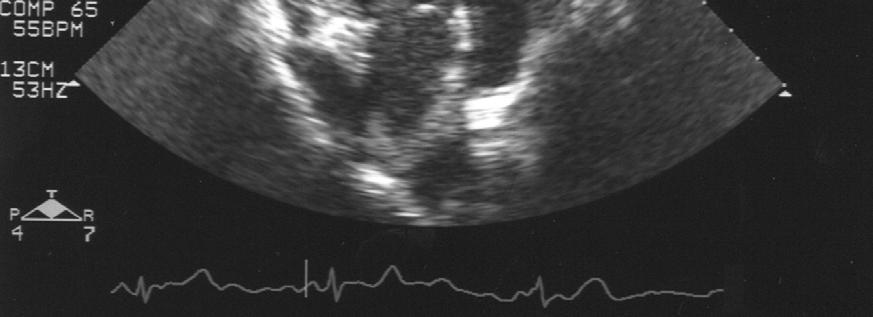
6 depending on the level of the cross-section. Further rotating the angle of the probe will gradually show the different part of the MV with the mid oesophageal 2-chamber view (Figure 7) and the mid oesophageal longitudinal view (Figure 8). In the 2-chamber view, P3 is to the left of the display and A1 is to the right; the longitudinal view shows P2 on the left of the display and A2 on the right. Transgastric views of the MV are developed by advancing the probe until the transducer is leveled with the base of the LV, approximately 35 to 40 cm distal to the incisors (Figure 9). An anteflexion of the tip of the probe and a slight withdrawing of the probe will be mostly required to obtain an orthogonal short-axis view of the MV; the posteromedial commissure is in the upper left of the display, the anterolateral commissure is to the lower right of the display, the posterior leaflet is to the right and the anterior one to the left of the display. A true orthogonal view of the MV is often difficult to obtain. In this case, the probe is withdrawn to get the posteromedial commissure, then further advanced in the stomach to get the anterolateral commissure. In the transgastric short-axis view, wall motion abnormalities should also be observed. The rotation forward of the multiplane angle to 90 will show the transgastric twochamber view (Figure 10); it will help us to assess the chordae tendinae (posterior chordae on the top of the screen, anterior on the bottom) and the papillary muscles. Doppler imaging Colour Doppler should be used in every cross-section to detect, localise and semiquantify MV flow abnormalities.
7 The transmitral Doppler spectral flow depends upon the instantaneous relationship between the left atrial and the left ventricular pressures (Figure 11). It will vary according to the pre- and afterload, ageing and heart rate. To assess accurately the maximal velocity of transmitral flow, the sample of the pulse wave Doppler (PWD) should be placed at the tip of the mitral leaflets (in case of CO assessment, the sample should be placed at the level of the annulus) and kept to a minimal size (3 to 5 mm)(figure 12). The Doppler beam should be aligned such that the angle between the beam and the direction of the flow is as close to zero as possible. The mitral flow is constituted of four different periods : the isovolumic relaxation time (IVRT), the rapid filling phase or E wave, the diastasis and the active filling phase or atrial contraction or A wave (Figure 11 and 12; Table 1). To assess exhaustively the function of the mitral valve as well as diastolic left ventricular function, the pulmonary venous flow should be interrogated (Figure 12; Table 1). The sample of the PWD should be placed 1 to 2 cm into the pulmonary vein, preferably into the upper left one. The pulmonary venous flow is constituted of four different waves: the systolic wave, divided in two parts: S1 depending upon the atrial relaxation and S2 depending upon the LV function, the diastolic passive wave or D and the diastolic retrograde wave during atrial systole or Apulm. The diastolic part of the pulmonary flow varies in accordance to the transmitral flow.
8 The aortic valve Anatomy The aortic valve is a semilunar valve with 3 cusps of similar size. Each cusp is attached to the aortic root at its lower edge along a U-shaped line with its upper free edge protruding into the lumen of the aorta. Behind each cusp is a pocket-like dilatation of the aortic root called sinus of Valsalva. The three cusps are named according to their relationship with the coronary arteries: the left, right and noncoronary cusps. The adjacent portions of the left and noncoronary cusps are in continuity with the base of the anterior leaflet of the mitral valve. The anterior halves of the right and left cusps are in contact with the muscular interventricular septum. The region where the aortic valve joins the cylindrical portion of the ascending aorta is called the sino-tubular junction. The left ventricular outflow tract (LVOT) is situated just inferior to the aortic valve. The whole aortic root is generally considered during assessment of the aortic valve. It includes the aortic valve annulus, the cusps, the sinuses of Valsalva, the right and left coronary ostia, the sino-tubular junction and the proximal ascending aorta. Bidimensional imaging The aortic root is usually easy to visualise with TOE and needs 3 cross-sections for a complete evaluation. The mid oesophageal 5-chamber view (0 ) should initially be obtained, approximately 30 to 35 cm distal to the incisors. With the aorta brought in the middle of the display, the multiplane angle is rotated forward between 30 and 60 to
9 develop the mid oesophageal short-axis view of the valve (Figure 13). The left coronary cusp is then on the top of the screen (posterior), the right one on the bottom (anterior) and the non-coronary cusp is situated on the left of the display, facing the interatrial septum. A planimetry of the opening surface of the valve may be traced in this view (Figure 14A). The correct opening and closure of the aortic valve as well as the exclusion of a LVOT obstruction may also be assessed in this view, using TM-mode perpendicularly to the valve (Figure 14B). Colour flow Doppler is applied in this crosssection to assess the presence of aortic regurgitation and to estimate the size and location of the regurgitation orifice. The probe is withdrawn or anteflexed slightly to move the imaging plane superiorly through the sinuses of Valsalva to show the right and left coronary ostia and arteries. The probe is then advanced through and then inferiorly to the valve to produce a shortaxis view of the LVOT. As the multiplane angle is further rotated to 120 to 160, the long-axis of the aortic valve will be obtained with a good view of the LVOT, the sino-tubular junction and the proximal ascending aorta (Figure 15). The LVOT is on the left of the display and the ascending aorta on the right. The cusp on the bottom of the screen (anterior) is the right coronary cusp. The cusp situated superiorly is usually the noncoronary cusp, but may be the left one, depending upon the location of the imaging plane. In this view will be measured the dimensions of the aortic annulus, sino-tubular junction and proximal ascending aorta. The aortic annulus is measured during systole at the points of attachment of the aortic valve cusps to the LVOT (Figure 16). The normal aortic annulus dimension in systole is usually between 1.8 and 2.5 cm. Colour Doppler flow applied in this view will allow the detection and semi-quantification of an aortic regurgitation.
10 The transgastric long-axis view is obtained by advancing the probe in the stomach, approximately 35 to 40 cm distal to the incisors, to obtain the classical short-axis basal view of the LV. The multiplane angle is then rotated forward to 90 to 120 to visualise the aortic valve on the bottom right of the display (Figure 17). The LV outflow is directed away from the transducer in this view. Finally, a deep transgastric view may be obtained by advancing the probe deep into the stomach and positioning the probe adjacent to the LV apex at 0. The probe is then maximally anteflexed and slightly rotated to obtain the aortic valve in long-axis centred at the bottom of the display (Figure 18). The aortic valve is located in the far field at the bottom of the display with the LV outflow directed away from the transducer. These last 2 views offer the best alignment with the aortic flow for Doppler assessment. Detailed assessment of the anatomy of the valve is however difficult in these views because the LVOT and the aortic valve are located too far from the transducer. Peak outflow velocity at the aortic valve is obtained most easily with continuous wave Doppler, assuming there is no obstruction to outflow proximal to the valve such as a subaortic membrane or hypertrophic obstructive cardiomyopathy. Blood flow velocity in the LVOT is measured using the pulse wave Doppler sample positioned in the middle of the LVOT, just inferior to the aortic cusps. Normal LVOT and aortic outflow velocities are less than 1.5cm/sec (Figure 19; Table 1)
11 Tricuspid valve Anatomy The tricuspid valve is constituted of three leaflets (anterior, posterior and septal), multiple chordae tendinae and 3 small papillary muscles, a supporting annular ring and the RV myocardium. The septal insertion of the tricuspid valve is normally slightly (1 to 2 cm) more apical than the insertion of anterior mitral leaflet (Figure 5). Exceptions to this rule are: the atrioventricular canal in which case both valves are inserted at the same level and the Ebstein pathology where parts of the tricuspid valve is inserted much lower in the ventricular cavity. The tricuspid valve has chordae tendinae inserted on 3 papillary muscles, one of which is on the interventricular septum, which is another way to differentiate it from the mitral valve. Bidimensional imaging The tricuspid valve can be visualised with TOE from three main views. The probe should be positioned in the mid or low oesophagus to get a 4-chamber view (Figure 20). The septal and posterior leaflets will be visualised. The probe should be advanced and withdrawn to map the entire tricuspid annulus from its inferior to superior extent. The mutliplane angle is then rotated forward to 60 to obtain the right ventricular inflowoutflow view, with the anterior (closed to the aorta) and posterior (on the free wall of the right ventricle) leaflets of the tricuspid valve on the left of the screen as well as the
12 pulmonary valve on the right of the screen (Figure 21). The use of Colour Doppler will allow the detection of tricuspid flow abnormalities. The probe should then be pushed further down in transgastric position and rotated to 30 to obtain a short-axis of the valve with the anterior leaflet on the bottom of the screen and the posterior and septal ones on the top of the screen (Figure 22). Further rotating the multiplane angle to 110 will show the RV inflow long-axis view, with the posterior wall on the top of the screen, the anterior wall with the papillary muscles on the bottom of the screen and the posterior and anterior leaflet of the tricuspid valve (Figure 23). Doppler imaging The transtricuspidal Doppler flow will be optimally obtained in the deep oesophageal view between 0 and 60, using pulsed wave Doppler. Normal tricuspid blood flow is M- shaped, similar to that of transmitral blood flow, with the two characteristic waves, E and A, occuring in early diastole and during atrial systole (Table 1). Tricuspid blood flow velocities are usually lower than transmitral blood flow velocities and show a greater variation during ventilation, particularly during positive pressure ventilation. During mechanical ventilation, the E/A peak velocity ratio exhibits cyclic changes within the respiratory cycle so that an accurate analysis is difficult. During positive pressure inspiration, transmitral blood flow peak velocities will increase while tricuspid blood flow peak velocities will decrease. Reverse is true during expiration (Figure 24). Colour Doppler at the tricuspid level allows rapid detection of tricuspid regurgitation, which is a frequent and normal finding, particularly in mechanically ventilated patients.
13 Using continuous Doppler recording parallel to the regurgitant flow allows the determination of the maximal velocity of the backward flow (Vmax). Applying the Bernouilli equation, the gradient between right ventricle and atrium might be assessed: P = 4Vmax 2 In the absence of ventricular shunt, adding the central venous pressure value to this gradient will give a good estimation of the right ventricular systolic pressure. In the absence of any pathology of the RV outflow tract or of the pulmonary valve, the systolic ventricular pressure will be the same as the systolic pulmonary pressure (Figure 25). When the quality of the tricuspid regurgitant flow envelope is not good enough for an accurate measurement, it may be enhanced by saline or contrast medium injection through a peripheral or central venous line. Pulmonary Valve Anatomy The pulmonary valve is a semilunar valve constituted of 3 cusps and an annulus. The right ventricular infundibulum and the pulmonary valve are part of the right ventricular outflow tract (RVOT) that extends from the crista supraventricularis to the bifurcation of the main pulmonary artery.
14 Bidimensional imaging The pulmonary valve and the main pulmonary artery can be assessed with TEE in the basal view (Figure 26). The probe is placed in the upper-oesophagus 0 to plane, approximately 28 to 30 cm distal to the incisors. Pulmonary artery flow velocity can be assessed in this view, using pulsed Doppler. Other views to assess the pulmonary valve are the mid oesophageal inflow-outflow 60 view previously described (Figure 21 and 27) as well as the deep transgastric 120 view (Figure 28). This last view offers the best alignement for Doppler interrogation of the pulmonary valve. Transpulmonary flow is similar to transaortic flow with lower velocity (Table 1). Normally, RV ejection velocity increases more gradually, exhibits a peak occurring close to midejection, and decreases more slowly than LV ejection velocity (Figure 29). Pulmonary insufficiency or stenosis should be searched for applying colour Doppler in each of these views. Conclusion A systematic approach should be applied to assess the cardiac valves as well as for every TEE examination to avoid missing important diagnosis.
15 References 1: Shanewise JS, Cheung AT, Aronson S, Stewart WJ, Weiss RL, et al.: ASE/SCA guidelines for performing a comprehensive intraoperative multiplane transesophageal echocardiography examination: recommendations of the ASE Council for intraoperative echocardiography and the SCA Task Force for certification in perioperative transesophageal echocardiography. Anesth Analg 1999;89: : Levine RA, Triulzi MO, Harrigan P, Weyman AE. The relationship of mitral annular shape to the diagnosis of mitral valve prolapse. Circulation 1987;75: : Lambert AS, Miller JP, Merrick SH, Schiller NB, Foster E, Muhiudeen-Russell I, Cahalan MK. Improved evaluation of the location and mechanism of mitral valve regurgitation with a systematic TEE examination. Anesth Analg 1999;88:
16 Tabel 1: Normal Doppler values by adults Localisation Velocity and times Mitral flow E A E/A tde IVRT 0.6 to 1.3 m/sec 0.4 to 0.8 m/sec 1.2 to to 210 msec 75 to 90 msec Pulmonary venous flow S D A 0.5 m/sec 0.4 to 0.5 m/sec m/sec LVOT flow Aortic valve flow 0.8 to 1.3 m/sec 1 to 1.7 m/sec Tricuspidal flow E A Pulmonary artery flow 0.3 to 0.7 m/sec 0.3 m/sec 0.6 to 0.9 m/sec
17 Figure1: Mitral leaflets coaptation Active balance: Closing force Tethering force
18 Figure 2: Carpentier nomenclature: mitral valve viewed from the left ventricle as in a basal transgastric view, with the position of the different examination planes of a multiplane transesophageal probe.



19 Figure 3: Saddle-shape of the mitral annulus 1 cm Right to left 0 to 20 Antero-posterior 90 to to 20 four-chamber 120 long-axis LV LV RV
20 Figure 4: Diameter of the mitral valve annulus: The diameter of the valve varies in function of the plane of the view due to the D-shape of the valve
 LA RA A3 P1 RV LV LA:")

21 Figure 5: Four-chamber view (0-20 ) LA RA A3 P1 RV LV LA: left atrium; LV: left ventricle; RA: right atrium; RV: right ventricle.
 P3 A2 (P2)")

22 Figure 6: Commissural view (60 ) P3 A2 (P2) P1 LA LV LA: left atrium; LV: left ventricle


23 Figure 7: Two-chamber view (90 ) P3 A1 LA LV LA: left atrium; LV: left ventricle

24 Figure 8: longitudinal view (120 ) P2 A2 LA Ao RV LV LA: left atrium; LV: left ventricle; RV: right ventricle; Ao: aorta
 PML")

25 Figure 9: Transgastric short-axis view (0 ) PML AML AML: anterior mitral leaflet; PML: posterior mitral leaflet;

 LV LA LA: left")
26 Figure 10: Transgastric two-chamber view (90 ) LV LA LA: left atrium; LV: left ventricle
27 Figure 11: Normal transmitral flow and transvalvular pressure gradient LVP LAP IVRT DT AVC A E 1: isovolumic relaxation time (IVRT) from the aortic valve closure (AVC) to the mitral valve opening 2: rapid filling phase (E wave); 3: diastasis; 4: atrial contraction (A wave); DT: deceleration time
28 Figure 12: Normal transmitral and transpulmonary venous flow LA: left atrium; LV: left ventricle; LSPV: left superior pulmonary vein; PV: pulmonary vein; MV: mitral valve

29 Figure 13: Short-axis view of the aortic valve and coronary arteries LA RA NC RCA LCA PA RA: right atrium; LA: left atrium; PA: pulmonary artery; LCA: left coronary artery; RCA: right coronary artery; NC: noncoronary cusp.

 and (B)")


30 Figure 14: (A) Aortic valve planimetry (1.88cm 2 ) and (B) TM-mode through the aortic valve showing a normal opening of the valve by a 14 yo patient A B


31 Figure 15: Long-axis of the aortic root LA Ao RVOT LA: left atrium; AO: aorta; RVOT: right ventricular outflow tract

32 Figure 16: Aortic valve annulus diameter: The diameter of the aortic valve annulus is 1.62 cm.


33 Figure 17: Transgastric long-axis 120 view LV LA Ao LA: left atrium; LV: left ventricle; Ao: aorta
34 Figure 18: Deep-transgastric long-axis 0 view


35 Figure 19: Pulsed wave Doppler through the LVOT (A) and continuous wave Doppler through the aortic valve (B) A B



36 Figure 20: Low-oesophageal view (0 ) LA CS RA STL LV ATL RV Anterolateral wall Posterior IVS LA: left atrium; LV: left ventricle; RA: right atrium; RV: right ventricle; STL: septal tricuspid leaflet, ATL: anterior tricuspid leaflet, CS: coronary sinus; IVS: interventricular septum.
37 Figure 21: RV inflow-outflow view (60 ) LA RA PTL ATL PV RV LA: left atrium; RA: right atrium; RV: right ventricle; PTL: posterior tricuspid leaflet; ATL: anterior tricuspid leaflet; PV: pulmonary valve.


38 Figure 22: Short-axis transgastric tricuspid valve PTL ATL LVOT STL Ao Ao: aorta; LVOT: left ventricular outflow tract; PTL: posterior tricuspid leaflet; ATL: anterior tricuspid leaflet; STL: septal tricuspid leaflet.


39 Figure 23: RV inflow long-axis view transtgastric PTL ATL RA RV RA: right atrium; RV: right ventricle, ATL: anterior tricuspid leaflet; PTL: posterior tricuspid leaflet.
 and tricuspid")



40 Figure 24: Mitral (A) and tricuspid (B) Doppler flow variations during respiration. A B Positive pressure inspiration Positive pressure expiration

41 Figure 25: Pulmonary pressure assessment with continuous Doppler through the tricuspid regurgitation: The maximal velocity of the tricuspid regurgitation is 3.33 m/sec and gives a pressure gradient of 44 mmhg between the right ventricle and the right atrium. Considering a central venous pressure of 10 mmhg, the pulmonary systolic pressure in this case would be around 54 mmhg.


42 Figure 26: Basal view of the pulmonary valve PA SVC AO RVOT PA: pulmonary artery; RVOT: right ventricular outflow tract; Ao: aorta; SVC: superior vena cava

43 Figure 27: Mid oesophageal inflow-outflow view 60 centered on the pulmonary valve RA LA PTL ATL PV RV LA: left atrium; RA: right atrium; RV: right ventricle; PTL: posterior tricuspid leaflet; ATL: anterior tricuspid leaflet, PV: pulmonary valve.

44 Figure 28: Transgastric view of the RVOT and pulmonary valve (120 ) RA RV PA RA: right atrium; RV: right ventricle; PA: pulmonary artery; RVOT: right ventricular outflow tract; TV: tricuspid valve; AO: aorta; AV: aortic valve

45 Figure 29: Transpulmonary pulsed wave Doppler flow (basal view 0 )
Since the introduction of transesophageal echocardiography
 ASE/SCA Guidelines for Performing a Comprehensive Intraoperative Multiplane Transesophageal Echocardiography Examination: Recommendations of the American Society of Echocardiography Council for Intraoperative
ASE/SCA Guidelines for Performing a Comprehensive Intraoperative Multiplane Transesophageal Echocardiography Examination: Recommendations of the American Society of Echocardiography Council for Intraoperative
Comprehensive Transoesophageal Echocardiography Examination
 IJUTPC PICTORIAL REVIEW Comprehensive Transoesophageal Echocardiography Examination Comprehensive Transoesophageal Echocardiography Examination 1 Ravi Hebballi, 2 Ann Ngui 1 Consultant in Cardiothoracic
IJUTPC PICTORIAL REVIEW Comprehensive Transoesophageal Echocardiography Examination Comprehensive Transoesophageal Echocardiography Examination 1 Ravi Hebballi, 2 Ann Ngui 1 Consultant in Cardiothoracic
JOINT MEETING 2 Tricuspid club Chairpersons: G. Athanassopoulos, A. Avgeropoulou, M. Khoury, G. Stavridis
 JOINT MEETING 2 Tricuspid club Chairpersons: G. Athanassopoulos, A. Avgeropoulou, M. Khoury, G. Stavridis Similarities and differences in Tricuspid vs. Mitral Valve Anatomy and Imaging. Echo evaluation
JOINT MEETING 2 Tricuspid club Chairpersons: G. Athanassopoulos, A. Avgeropoulou, M. Khoury, G. Stavridis Similarities and differences in Tricuspid vs. Mitral Valve Anatomy and Imaging. Echo evaluation
Breakout Session: Transesophageal Echocardiography
 Breakout Session: Transesophageal Echocardiography Doris Ockert, MD Andrew Schroeder, MD University of Wisconsin School of Medicine and Public Health Jutta Novalija, MD, PhD Medical College of Wisconsin
Breakout Session: Transesophageal Echocardiography Doris Ockert, MD Andrew Schroeder, MD University of Wisconsin School of Medicine and Public Health Jutta Novalija, MD, PhD Medical College of Wisconsin
Cardiac ultrasound protocols
 Cardiac ultrasound protocols IDEXX Telemedicine Consultants Two-dimensional and M-mode imaging planes Right parasternal long axis four chamber Obtained from the right side Displays the relative proportions
Cardiac ultrasound protocols IDEXX Telemedicine Consultants Two-dimensional and M-mode imaging planes Right parasternal long axis four chamber Obtained from the right side Displays the relative proportions
Introduction. Aortic Valve. Outflow Tract and Aortic Valve Annulus
 Chapter 1: Surgical anatomy of the aortic and mitral valves Jordan RH Hoffman MD, David A. Fullerton MD, FACC University of Colorado School of Medicine, Department of Surgery, Division of Cardiothoracic
Chapter 1: Surgical anatomy of the aortic and mitral valves Jordan RH Hoffman MD, David A. Fullerton MD, FACC University of Colorado School of Medicine, Department of Surgery, Division of Cardiothoracic
Appendix II: ECHOCARDIOGRAPHY ANALYSIS
 Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Two semilunar valves. Two atrioventricular valves. Valves of the heart. Left atrioventricular or bicuspid valve Mitral valve
 The Heart 3 Valves of the heart Two atrioventricular valves Two semilunar valves Right atrioventricular or tricuspid valve Left atrioventricular or bicuspid valve Mitral valve Aortic valve Pulmonary valve
The Heart 3 Valves of the heart Two atrioventricular valves Two semilunar valves Right atrioventricular or tricuspid valve Left atrioventricular or bicuspid valve Mitral valve Aortic valve Pulmonary valve
British Society of Echocardiography
 British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital
 Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
Normal TTE/TEE Examinations
 Normal TTE/TEE Examinations Geoffrey A. Rose, MD FACC FASE Sanger Heart & Vascular Institute Before you begin imaging... Obtain the patient s Height Weight BP PLAX View PLAX View Is apex @ 9-10 o clock?
Normal TTE/TEE Examinations Geoffrey A. Rose, MD FACC FASE Sanger Heart & Vascular Institute Before you begin imaging... Obtain the patient s Height Weight BP PLAX View PLAX View Is apex @ 9-10 o clock?
Transoesophageal Echocardiographic Evaluation of the Mitral Valve
 10.5005/jp-journals-10027-1018 REVIEW ARTICLE IJPUT Transoesophageal Echocardiographic Evaluation of the Mitral Valve Gary Lau, Ravi Hebballi ABSTRACT Transoesophageal echocardiography allows the precise
10.5005/jp-journals-10027-1018 REVIEW ARTICLE IJPUT Transoesophageal Echocardiographic Evaluation of the Mitral Valve Gary Lau, Ravi Hebballi ABSTRACT Transoesophageal echocardiography allows the precise
MITRAL STENOSIS. Joanne Cusack
 MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
Adel Hasanin Ahmed 1
 Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
the Cardiovascular System I
 the Cardiovascular System I By: Dr. Nabil A Khouri MD, MsC, Ph.D MEDIASTINUM 1. Superior Mediastinum 2. inferior Mediastinum Anterior mediastinum. Middle mediastinum. Posterior mediastinum Anatomy of
the Cardiovascular System I By: Dr. Nabil A Khouri MD, MsC, Ph.D MEDIASTINUM 1. Superior Mediastinum 2. inferior Mediastinum Anterior mediastinum. Middle mediastinum. Posterior mediastinum Anatomy of
ECHOCARDIOGRAPHY DATA REPORT FORM
 Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function
 Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Ch.15 Cardiovascular System Pgs {15-12} {15-13}
 Ch.15 Cardiovascular System Pgs {15-12} {15-13} E. Skeleton of the Heart 1. The skeleton of the heart is composed of rings of dense connective tissue and other masses of connective tissue in the interventricular
Ch.15 Cardiovascular System Pgs {15-12} {15-13} E. Skeleton of the Heart 1. The skeleton of the heart is composed of rings of dense connective tissue and other masses of connective tissue in the interventricular
Certificate in Clinician Performed Ultrasound (CCPU) Syllabus. Rapid Cardiac Echo (RCE)
 Syllabus. Rapid Cardiac Echo (RCE)") Certificate in Clinician Performed Ultrasound (CCPU) Syllabus Rapid Cardiac Echo (RCE) Purpose: Rapid Cardiac Echocardiography (RCE) This unit is designed to cover the theoretical and practical curriculum
Certificate in Clinician Performed Ultrasound (CCPU) Syllabus Rapid Cardiac Echo (RCE) Purpose: Rapid Cardiac Echocardiography (RCE) This unit is designed to cover the theoretical and practical curriculum
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Anatomy of left ventricular outflow tract'
 Anatomy of left ventricular outflow tract' ROBERT WALMSLEY British Heart Journal, 1979, 41, 263-267 From the Department of Anatomy and Experimental Pathology, The University, St Andrews, Scotland SUMMARY
Anatomy of left ventricular outflow tract' ROBERT WALMSLEY British Heart Journal, 1979, 41, 263-267 From the Department of Anatomy and Experimental Pathology, The University, St Andrews, Scotland SUMMARY
Atrial Septal Defects
 Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
The Doppler Examination. Katie Twomley, MD Wake Forest Baptist Health - Lexington
 The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
Blood supply of the Heart & Conduction System. Dr. Nabil Khouri
 Blood supply of the Heart & Conduction System Dr. Nabil Khouri Arterial supply of Heart Right coronary artery Left coronary artery 3 Introduction: Coronary arteries - VASAVASORUM arising from aortic sinuses
Blood supply of the Heart & Conduction System Dr. Nabil Khouri Arterial supply of Heart Right coronary artery Left coronary artery 3 Introduction: Coronary arteries - VASAVASORUM arising from aortic sinuses
Right Heart Evaluation ASE Guidelines Review. Chris Mann RDCS, RCS, FASE Faculty, Echocardiography Pitt Community College Greenville, NC
 Right Heart Evaluation ASE Guidelines Review Chris Mann RDCS, RCS, FASE Faculty, Echocardiography Pitt Community College Greenville, NC Objectives Briefly review right atrial and right ventricular anatomy
Right Heart Evaluation ASE Guidelines Review Chris Mann RDCS, RCS, FASE Faculty, Echocardiography Pitt Community College Greenville, NC Objectives Briefly review right atrial and right ventricular anatomy
LECTURE 5. Anatomy of the heart
 LECTURE 5. Anatomy of the heart Main components of the CVS: Heart Blood circulatory system arterial compartment haemomicrocirculatory (=microvascular) compartment venous compartment Lymphatic circulatory
LECTURE 5. Anatomy of the heart Main components of the CVS: Heart Blood circulatory system arterial compartment haemomicrocirculatory (=microvascular) compartment venous compartment Lymphatic circulatory
Lab Activity 23. Cardiac Anatomy. Portland Community College BI 232
 Lab Activity 23 Cardiac Anatomy Portland Community College BI 232 Cardiac Muscle Histology Branching cells Intercalated disc: contains many gap junctions connecting the adjacent cell cytoplasm, creates
Lab Activity 23 Cardiac Anatomy Portland Community College BI 232 Cardiac Muscle Histology Branching cells Intercalated disc: contains many gap junctions connecting the adjacent cell cytoplasm, creates
Diastolic Function: What the Sonographer Needs to Know. Echocardiographic Assessment of Diastolic Function: Basic Concepts 2/8/2012
 Diastolic Function: What the Sonographer Needs to Know Pat Bailey, RDCS, FASE Technical Director Beaumont Health System Echocardiographic Assessment of Diastolic Function: Basic Concepts Practical Hints
Diastolic Function: What the Sonographer Needs to Know Pat Bailey, RDCS, FASE Technical Director Beaumont Health System Echocardiographic Assessment of Diastolic Function: Basic Concepts Practical Hints
ΔΙΑΔΕΡΜΙΚΗ ΑΝΤΙΜΕΤΩΠΙΣΗ ΔΟΜΙΚΩΝ ΠΑΘΗΣΕΩΝ: Ο ΡΟΛΟΣ ΤΗΣ ΑΠΕΙΚΟΝΙΣΗΣ ΣΤΟ ΑΙΜΟΔΥΝΑΜΙΚΟ ΕΡΓΑΣΤΗΡΙΟ ΣΤΗΝ ΤΟΠΟΘΕΤΗΣΗ MITRACLIP
 ΔΙΑΔΕΡΜΙΚΗ ΑΝΤΙΜΕΤΩΠΙΣΗ ΔΟΜΙΚΩΝ ΠΑΘΗΣΕΩΝ: Ο ΡΟΛΟΣ ΤΗΣ ΑΠΕΙΚΟΝΙΣΗΣ ΣΤΟ ΑΙΜΟΔΥΝΑΜΙΚΟ ΕΡΓΑΣΤΗΡΙΟ ΣΤΗΝ ΤΟΠΟΘΕΤΗΣΗ MITRACLIP ΒΛΑΣΗΣ ΝΙΝΙΟΣ MD MRCP ΚΛΙΝΙΚΗ ΑΓΙΟΣ ΛΟΥΚΑΣ ΘΕΣΣΑΛΟΝΙΚΗ CONFLICT OF INTEREST PROCTOR
ΔΙΑΔΕΡΜΙΚΗ ΑΝΤΙΜΕΤΩΠΙΣΗ ΔΟΜΙΚΩΝ ΠΑΘΗΣΕΩΝ: Ο ΡΟΛΟΣ ΤΗΣ ΑΠΕΙΚΟΝΙΣΗΣ ΣΤΟ ΑΙΜΟΔΥΝΑΜΙΚΟ ΕΡΓΑΣΤΗΡΙΟ ΣΤΗΝ ΤΟΠΟΘΕΤΗΣΗ MITRACLIP ΒΛΑΣΗΣ ΝΙΝΙΟΣ MD MRCP ΚΛΙΝΙΚΗ ΑΓΙΟΣ ΛΟΥΚΑΣ ΘΕΣΣΑΛΟΝΙΚΗ CONFLICT OF INTEREST PROCTOR
Assessment of LV systolic function
 Tutorial 5 - Assessment of LV systolic function Assessment of LV systolic function A knowledge of the LV systolic function is crucial in the undertanding of and management of unstable hemodynamics or a
Tutorial 5 - Assessment of LV systolic function Assessment of LV systolic function A knowledge of the LV systolic function is crucial in the undertanding of and management of unstable hemodynamics or a
8/31/2016. Mitraclip in Matthew Johnson, MD
 Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
Revealing new insights. irotate electronic rotation and xplane adjustable biplane imaging. Ultrasound cardiology. irotate and xplane
 Ultrasound cardiology irotate and xplane Revealing new insights irotate electronic rotation and xplane adjustable biplane imaging Annemien van den Bosch and Jackie McGhie Department of Cardiology, Erasmus
Ultrasound cardiology irotate and xplane Revealing new insights irotate electronic rotation and xplane adjustable biplane imaging Annemien van den Bosch and Jackie McGhie Department of Cardiology, Erasmus
The Heart. Happy Friday! #takeoutyournotes #testnotgradedyet
 The Heart Happy Friday! #takeoutyournotes #testnotgradedyet Introduction Cardiovascular system distributes blood Pump (heart) Distribution areas (capillaries) Heart has 4 compartments 2 receive blood (atria)
The Heart Happy Friday! #takeoutyournotes #testnotgradedyet Introduction Cardiovascular system distributes blood Pump (heart) Distribution areas (capillaries) Heart has 4 compartments 2 receive blood (atria)
LAB 12-1 HEART DISSECTION GROSS ANATOMY OF THE HEART
 LAB 12-1 HEART DISSECTION GROSS ANATOMY OF THE HEART Because mammals are warm-blooded and generally very active animals, they require high metabolic rates. One major requirement of a high metabolism is
LAB 12-1 HEART DISSECTION GROSS ANATOMY OF THE HEART Because mammals are warm-blooded and generally very active animals, they require high metabolic rates. One major requirement of a high metabolism is
Chapter 20 (1) The Heart
 The Heart") Chapter 20 (1) The Heart Learning Objectives Describe the location and structure of the heart Describe the path of a drop of blood from the superior vena cava or inferior vena cava through the heart out
Chapter 20 (1) The Heart Learning Objectives Describe the location and structure of the heart Describe the path of a drop of blood from the superior vena cava or inferior vena cava through the heart out
PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING
 PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING STANDARD - Primary Instrumentation 1.1 Cardiac Ultrasound Systems SECTION 1 Instrumentation Ultrasound instruments
PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING STANDARD - Primary Instrumentation 1.1 Cardiac Ultrasound Systems SECTION 1 Instrumentation Ultrasound instruments
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Anatomy of the Heart. Figure 20 2c
 Anatomy of the Heart Figure 20 2c Pericardium & Myocardium Remember, the heart sits in it s own cavity, known as the mediastinum. The heart is surrounded by the Pericardium, a double lining of the pericardial
Anatomy of the Heart Figure 20 2c Pericardium & Myocardium Remember, the heart sits in it s own cavity, known as the mediastinum. The heart is surrounded by the Pericardium, a double lining of the pericardial
Imaging Guide Echocardiography
 Imaging Guide Guide to Small Animal Echocardiography using the Vevo Imaging Systems System Compatibility: This guide contains instructions and suggestions for work on the Vevo2100, VevoLAZR, Vevo 3100
Imaging Guide Guide to Small Animal Echocardiography using the Vevo Imaging Systems System Compatibility: This guide contains instructions and suggestions for work on the Vevo2100, VevoLAZR, Vevo 3100
THE CARDIOVASCULAR SYSTEM. Part 1
 THE CARDIOVASCULAR SYSTEM Part 1 CARDIOVASCULAR SYSTEM Blood Heart Blood vessels What is the function of this system? What other systems does it affect? CARDIOVASCULAR SYSTEM Functions Transport gases,
THE CARDIOVASCULAR SYSTEM Part 1 CARDIOVASCULAR SYSTEM Blood Heart Blood vessels What is the function of this system? What other systems does it affect? CARDIOVASCULAR SYSTEM Functions Transport gases,
What are the best diagnostic tools to quantify aortic regurgitation?
 What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
Danil Hammoudi.MD 1/12/2009
 Danil Hammoudi.MD Aorta the biggest and longest artery (a blood vessel carrying blood away from the heart) in the body. It carries oxygen rich blood from the left ventricle of the heart to the body.inferior
Danil Hammoudi.MD Aorta the biggest and longest artery (a blood vessel carrying blood away from the heart) in the body. It carries oxygen rich blood from the left ventricle of the heart to the body.inferior
Coronary Anomalies & Hemodynamic Identification
 Coronary Anomalies & Hemodynamic Identification David Stultz, MD Cardiology Fellow, PGY 6 May 2, 2006 Anomaly #1 Anomaly #2 Anomaly #3 Figure 18-27 Anomalous origin of the left circumflex artery.
Coronary Anomalies & Hemodynamic Identification David Stultz, MD Cardiology Fellow, PGY 6 May 2, 2006 Anomaly #1 Anomaly #2 Anomaly #3 Figure 18-27 Anomalous origin of the left circumflex artery.
Introduction to TEE using Heartworks Echocardiography Simulator
 Introduction to TEE using Heartworks Echocardiography Simulator Steven M. Ewer, MD Assistant Professor Division of Cardiovascular Medicine University of Wisconsin School of Medicine & Public Health Version
Introduction to TEE using Heartworks Echocardiography Simulator Steven M. Ewer, MD Assistant Professor Division of Cardiovascular Medicine University of Wisconsin School of Medicine & Public Health Version
Doppler Basic & Hemodynamic Calculations
 Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
THE HEART. A. The Pericardium - a double sac of serous membrane surrounding the heart
 THE HEART I. Size and Location: A. Fist-size weighing less than a pound (250 to 350 grams). B. Located in the mediastinum between the 2 nd rib and the 5 th intercostal space. 1. Tipped to the left, resting
THE HEART I. Size and Location: A. Fist-size weighing less than a pound (250 to 350 grams). B. Located in the mediastinum between the 2 nd rib and the 5 th intercostal space. 1. Tipped to the left, resting
human anatomy 2016 lecture thirteen Dr meethak ali ahmed neurosurgeon
 Heart The heart is a hollow muscular organ that is somewhat pyramid shaped and lies within the pericardium in the mediastinum. It is connected at its base to the great blood vessels but otherwise lies
Heart The heart is a hollow muscular organ that is somewhat pyramid shaped and lies within the pericardium in the mediastinum. It is connected at its base to the great blood vessels but otherwise lies
B-Mode measurements protocols:
 Application Note How to Perform the Most Commonly Used Measurements from the Cardiac Measurements Package associated with Calculations of Cardiac Function using the Vevo Lab Objective The Vevo LAB offline
Application Note How to Perform the Most Commonly Used Measurements from the Cardiac Measurements Package associated with Calculations of Cardiac Function using the Vevo Lab Objective The Vevo LAB offline
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
ICE: Echo Core Lab-CRF
 APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
 QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES") THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
MITRAL REGURGITATION ECHO PARAMETERS TOOL
 Comprehensive assessment of qualitative and quantitative parameters, along with the use of standardized nomenclature when reporting echocardiographic findings, helps to better define a patient s MR and
Comprehensive assessment of qualitative and quantitative parameters, along with the use of standardized nomenclature when reporting echocardiographic findings, helps to better define a patient s MR and
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD
 COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
Regurgitant Lesions. Bicol Hospital, Legazpi City, Philippines July Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA
 Regurgitant Lesions Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Aortic Insufficiency Valve anatomy and function LVOT and
Regurgitant Lesions Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Aortic Insufficiency Valve anatomy and function LVOT and
Ch 19: Cardiovascular System - The Heart -
 Ch 19: Cardiovascular System - The Heart - Give a detailed description of the superficial and internal anatomy of the heart, including the pericardium, the myocardium, and the cardiac muscle. Trace the
Ch 19: Cardiovascular System - The Heart - Give a detailed description of the superficial and internal anatomy of the heart, including the pericardium, the myocardium, and the cardiac muscle. Trace the
Valve Analysis and Pathoanatomy: THE MITRAL VALVE
 : THE MITRAL VALVE Marc R. Moon, M.D. John M. Shoenberg Chair in CV Disease Chief, Cardiac Surgery Washington University School of Medicine, St. Louis, MO Secretary, American Association for Thoracic Surgery
: THE MITRAL VALVE Marc R. Moon, M.D. John M. Shoenberg Chair in CV Disease Chief, Cardiac Surgery Washington University School of Medicine, St. Louis, MO Secretary, American Association for Thoracic Surgery
Back to Basics: Common Errors In Quantitation In Everyday Practice
 Back to Basics: Common Errors In Quantitation In Everyday Practice Deborah Agler, ACS, RDCS, FASE October 9, 2017 ASE: Echo Florida Rebecca T. Hahn, MD Director of Interventional Echocardiography Professor
Back to Basics: Common Errors In Quantitation In Everyday Practice Deborah Agler, ACS, RDCS, FASE October 9, 2017 ASE: Echo Florida Rebecca T. Hahn, MD Director of Interventional Echocardiography Professor
Normal TTE Examination, Doppler Echocardiography and Normal Antegrade Flow Patterns
 Normal TTE Examination, Doppler Echocardiography and Normal Antegrade Flow Patterns Pravin Patil, MD FACC FASE Associate Professor of Medicine Director, Cardiovascular Disease Training Program Lewis Katz
Normal TTE Examination, Doppler Echocardiography and Normal Antegrade Flow Patterns Pravin Patil, MD FACC FASE Associate Professor of Medicine Director, Cardiovascular Disease Training Program Lewis Katz
THE HEART OBJECTIVES: LOCATION OF THE HEART IN THE THORACIC CAVITY CARDIOVASCULAR SYSTEM
 BIOLOGY II CARDIOVASCULAR SYSTEM ACTIVITY #3 NAME DATE HOUR THE HEART OBJECTIVES: Describe the anatomy of the heart and identify and give the functions of all parts. (pp. 356 363) Trace the flow of blood
BIOLOGY II CARDIOVASCULAR SYSTEM ACTIVITY #3 NAME DATE HOUR THE HEART OBJECTIVES: Describe the anatomy of the heart and identify and give the functions of all parts. (pp. 356 363) Trace the flow of blood
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION
 LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
Chapter 18 - Heart. I. Heart Anatomy: size of your fist; located in mediastinum (medial cavity)
") Chapter 18 - Heart I. Heart Anatomy: size of your fist; located in mediastinum (medial cavity) A. Coverings: heart enclosed in double walled sac called the pericardium 1. Fibrous pericardium: dense connective
Chapter 18 - Heart I. Heart Anatomy: size of your fist; located in mediastinum (medial cavity) A. Coverings: heart enclosed in double walled sac called the pericardium 1. Fibrous pericardium: dense connective
AP2 Lab 3 Coronary Vessels, Valves, Sounds, and Dissection
 AP2 Lab 3 Coronary Vessels, Valves, Sounds, and Dissection Project 1 - BLOOD Supply to the Myocardium (Figs. 18.5 &18.10) The myocardium is not nourished by the blood while it is being pumped through the
AP2 Lab 3 Coronary Vessels, Valves, Sounds, and Dissection Project 1 - BLOOD Supply to the Myocardium (Figs. 18.5 &18.10) The myocardium is not nourished by the blood while it is being pumped through the
P = 4V 2. IVC Dimensions 10/20/2014. Comprehensive Hemodynamic Evaluation by Doppler Echocardiography. The Simplified Bernoulli Equation
 Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE. Sampling Rate M-Mode: 1800 / sec 2D: 30 / sec
 M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE Honoraria: Philips Classical M-mode Echocardiography M-Mode offers better time and image resolution. Sampling Rate M-Mode: 1800 / sec
M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE Honoraria: Philips Classical M-mode Echocardiography M-Mode offers better time and image resolution. Sampling Rate M-Mode: 1800 / sec
CARDIAC AND CORONARY ARTERY ANATOMY NO DISCLOSURES. Axial Anatomy of Heart. Axial Anatomy of Heart. Axial Anatomy of Heart
 CARDIAC AND CORONARY ARTERY ANATOMY NO DISCLOSURES NASCI MEETING, ORLANDO FLORIDA 2009 KOSTAKI G. BIS, MD, FACR DEPARTMENT OF RADIOLOGY WILLIAM BEAUMONT HOSPITAL Royal Oak, Michigan OBJECTIVES CARDIAC
CARDIAC AND CORONARY ARTERY ANATOMY NO DISCLOSURES NASCI MEETING, ORLANDO FLORIDA 2009 KOSTAKI G. BIS, MD, FACR DEPARTMENT OF RADIOLOGY WILLIAM BEAUMONT HOSPITAL Royal Oak, Michigan OBJECTIVES CARDIAC
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
During the last few decades, the utility of intraoperative
 ASE POSITION PAPER Guidelines for Performing a Comprehensive Epicardial Echocardiography Examination: Recommendations of the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists
ASE POSITION PAPER Guidelines for Performing a Comprehensive Epicardial Echocardiography Examination: Recommendations of the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists
Introduction to Anatomy. Dr. Maher Hadidi. Bayan Yanes. April/9 th /2013
 Introduction to Anatomy Dr. Maher Hadidi Bayan Yanes 27 April/9 th /2013 KEY POINTS: 1) Right side of the heart 2) Papillary muscles 3) Left side of the heart 4) Comparison between right and left sides
Introduction to Anatomy Dr. Maher Hadidi Bayan Yanes 27 April/9 th /2013 KEY POINTS: 1) Right side of the heart 2) Papillary muscles 3) Left side of the heart 4) Comparison between right and left sides
14 Valvular Stenosis
 14 Valvular Stenosis 14-1. Valvular Stenosis unicuspid valve FIGUE 14-1. This photograph shows severe valvular stenosis as it occurs in a newborn. There is a unicuspid, horseshoe-shaped leaflet with a
14 Valvular Stenosis 14-1. Valvular Stenosis unicuspid valve FIGUE 14-1. This photograph shows severe valvular stenosis as it occurs in a newborn. There is a unicuspid, horseshoe-shaped leaflet with a
Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency
 Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency Rahul R. Jhaveri, MD, Muhamed Saric, MD, PhD, FASE, and Itzhak Kronzon, MD, FASE, New York, New York Background: Two-dimensional
Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency Rahul R. Jhaveri, MD, Muhamed Saric, MD, PhD, FASE, and Itzhak Kronzon, MD, FASE, New York, New York Background: Two-dimensional
CV Anatomy Quiz. Dr Ella Kim Dr Pip Green
 CV Anatomy Quiz Dr Ella Kim Dr Pip Green Q1 The location of the heart is correctly described as A) lateral to the lungs. B) medial to the sternum. C) superior to the diaphragm. D) posterior to the spinal
CV Anatomy Quiz Dr Ella Kim Dr Pip Green Q1 The location of the heart is correctly described as A) lateral to the lungs. B) medial to the sternum. C) superior to the diaphragm. D) posterior to the spinal
Heart Dissection. 5. Locate the tip of the heart or the apex. Only the left ventricle extends all the way to the apex.
 Heart Dissection Page 1 of 6 Background: The heart is a four-chambered, hollow organ composed primarily of cardiac muscle tissue. It is located in the center of the chest in between the lungs. It is the
Heart Dissection Page 1 of 6 Background: The heart is a four-chambered, hollow organ composed primarily of cardiac muscle tissue. It is located in the center of the chest in between the lungs. It is the
Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension
 ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
The Cardiac Cycle Clive M. Baumgarten, Ph.D.
 The Cardiac Cycle Clive M. Baumgarten, Ph.D. OBJECTIVES: 1. Describe periods comprising cardiac cycle and events within each period 2. Describe the temporal relationships between pressure, blood flow,
The Cardiac Cycle Clive M. Baumgarten, Ph.D. OBJECTIVES: 1. Describe periods comprising cardiac cycle and events within each period 2. Describe the temporal relationships between pressure, blood flow,
ISUOG Basic Training. Obtaining & Interpreting Heart Views Correctly Alfred Abuhamad, USA. Basic training. Editable text here
 ISUOG Basic Training Obtaining & Interpreting Heart Views Correctly Alfred Abuhamad, USA Learning Objectives 6, 7 & 8 At the end of the lecture you will be able to: describe how to assess cardiac situs
ISUOG Basic Training Obtaining & Interpreting Heart Views Correctly Alfred Abuhamad, USA Learning Objectives 6, 7 & 8 At the end of the lecture you will be able to: describe how to assess cardiac situs
Congenital Heart Defects
 Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
2. right heart = pulmonary pump takes blood to lungs to pick up oxygen and get rid of carbon dioxide
 A. location in thorax, in inferior mediastinum posterior to sternum medial to lungs superior to diaphragm anterior to vertebrae orientation - oblique apex points down and to the left 2/3 of mass on left
A. location in thorax, in inferior mediastinum posterior to sternum medial to lungs superior to diaphragm anterior to vertebrae orientation - oblique apex points down and to the left 2/3 of mass on left
5 Working With Measurements
 5 Working With Measurements Measurement Overview Measurements accompanying ultrasound images supplement other clinical procedures available to the attending physician. Accuracy of the measurements is determined
5 Working With Measurements Measurement Overview Measurements accompanying ultrasound images supplement other clinical procedures available to the attending physician. Accuracy of the measurements is determined
What is Ebstein Anomaly?
 Echocardiograpnhic Evaluation of : Definition, Detection and Determinants of Outcome P. W. O Leary, M.D. Division of Pediatric Cardiology Mayo Clinic No Conflicts to Disclose What is? Failure of the TV
Echocardiograpnhic Evaluation of : Definition, Detection and Determinants of Outcome P. W. O Leary, M.D. Division of Pediatric Cardiology Mayo Clinic No Conflicts to Disclose What is? Failure of the TV
CARDIOVASCULAR SYSTEM
 CARDIOVASCULAR SYSTEM Overview Heart and Vessels 2 Major Divisions Pulmonary Circuit Systemic Circuit Closed and Continuous Loop Location Aorta Superior vena cava Right lung Pulmonary trunk Base of heart
CARDIOVASCULAR SYSTEM Overview Heart and Vessels 2 Major Divisions Pulmonary Circuit Systemic Circuit Closed and Continuous Loop Location Aorta Superior vena cava Right lung Pulmonary trunk Base of heart
Outline. EuroScore II. Society of Thoracic Surgeons Score. EuroScore II
 SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
List of Videos. Video 1.1
 Video 1.1 Video 1.2 Video 1.3 Video 1.4 Video 1.5 Video 1.6 Video 1.7 Video 1.8 The parasternal long-axis view of the left ventricle shows the left ventricular inflow and outflow tract. The left atrium
Video 1.1 Video 1.2 Video 1.3 Video 1.4 Video 1.5 Video 1.6 Video 1.7 Video 1.8 The parasternal long-axis view of the left ventricle shows the left ventricular inflow and outflow tract. The left atrium
Chapter 14. Circulatory System Images. VT-122 Anatomy & Physiology II
 Chapter 14 Circulatory System Images VT-122 Anatomy & Physiology II The mediastinum Dog heart Dog heart Cat heart Dog heart ultrasound Can see pericardium as distinct bright line Pericardial effusion Fluid
Chapter 14 Circulatory System Images VT-122 Anatomy & Physiology II The mediastinum Dog heart Dog heart Cat heart Dog heart ultrasound Can see pericardium as distinct bright line Pericardial effusion Fluid
cardiac imaging planes planning basic cardiac & aortic views for MR
 cardiac imaging planes planning basic cardiac & aortic views for MR Dianna M. E. Bardo, M. D. Assistant Professor of Radiology & Cardiovascular Medicine Director of Cardiac Imaging cardiac imaging planes
cardiac imaging planes planning basic cardiac & aortic views for MR Dianna M. E. Bardo, M. D. Assistant Professor of Radiology & Cardiovascular Medicine Director of Cardiac Imaging cardiac imaging planes
Case # 1. Page: 8. DUKE: Adams
 Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease
 Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
Anatomy of the Heart
 Biology 212: Anatomy and Physiology II Anatomy of the Heart References: Saladin, KS: Anatomy and Physiology, The Unity of Form and Function 8 th (2018). Required reading before beginning this lab: Chapter
Biology 212: Anatomy and Physiology II Anatomy of the Heart References: Saladin, KS: Anatomy and Physiology, The Unity of Form and Function 8 th (2018). Required reading before beginning this lab: Chapter
The Normal Echocardiogram
 The Normal Echocardiogram Pravin V. Patil, MD FACC Lewis Katz School of Medicine at Temple University Acknowledgments Dr. Susan Wiegers Dr. Martin Keane Temple Cardiac Sonographers Disclosures No relevant
The Normal Echocardiogram Pravin V. Patil, MD FACC Lewis Katz School of Medicine at Temple University Acknowledgments Dr. Susan Wiegers Dr. Martin Keane Temple Cardiac Sonographers Disclosures No relevant
Chapter 20: Cardiovascular System: The Heart
 Chapter 20: Cardiovascular System: The Heart I. Functions of the Heart A. List and describe the four functions of the heart: 1. 2. 3. 4. II. Size, Shape, and Location of the Heart A. Size and Shape 1.
Chapter 20: Cardiovascular System: The Heart I. Functions of the Heart A. List and describe the four functions of the heart: 1. 2. 3. 4. II. Size, Shape, and Location of the Heart A. Size and Shape 1.
Fetal Echocardiography and the Routine Obstetric Sonogram
 JDMS 23:143 149 May/June 2007 143 Fetal Echocardiography and the Routine Obstetric Sonogram SHELLY ZIMBELMAN, RT(R)(CT), RDMS, RDCS ASAD SHEIKH, MD, RDCS Congenital heart disease (CHD) is the most common
JDMS 23:143 149 May/June 2007 143 Fetal Echocardiography and the Routine Obstetric Sonogram SHELLY ZIMBELMAN, RT(R)(CT), RDMS, RDCS ASAD SHEIKH, MD, RDCS Congenital heart disease (CHD) is the most common
ULTRASOUND OF THE FETAL HEART
 ULTRASOUND OF THE FETAL HEART Cameron A. Manbeian, MD Disclosure Statement Today s faculty: Cameron Manbeian, MD does not have any relevant financial relationships with commercial interests or affiliations
ULTRASOUND OF THE FETAL HEART Cameron A. Manbeian, MD Disclosure Statement Today s faculty: Cameron Manbeian, MD does not have any relevant financial relationships with commercial interests or affiliations
Case 47 Clinical Presentation
 93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
Heart Anatomy. 7/5/02 Stephen G Davenport 1
 Heart Anatomy Copyright 1999, Stephen G. Davenport, No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form without prior written permission. 7/5/02 Stephen
Heart Anatomy Copyright 1999, Stephen G. Davenport, No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form without prior written permission. 7/5/02 Stephen
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
ECHOCARDIOGRAPHY SERVICE OBJECTIVES FOR ECHOCARDIOGRAPHY IN THE McGILL CARDIOLOGY TRAINING PROGRAM
 ECHOCARDIOGRAPHY SERVICE OBJECTIVES FOR ECHOCARDIOGRAPHY IN THE McGILL CARDIOLOGY TRAINING PROGRAM As stipulated by Royal College training requirements, residents undergo a minimum of 6 months of training
ECHOCARDIOGRAPHY SERVICE OBJECTIVES FOR ECHOCARDIOGRAPHY IN THE McGILL CARDIOLOGY TRAINING PROGRAM As stipulated by Royal College training requirements, residents undergo a minimum of 6 months of training
Functional anatomy of the aortic root. ΔΡΟΣΟΣ ΓΕΩΡΓΙΟΣ Διεσθσνηής Καρδιοθωρακοτειροσργικής Κλινικής Γ.Ν. «Γ. Παπανικολάοσ» Θεζζαλονίκη
 Functional anatomy of the aortic root ΔΡΟΣΟΣ ΓΕΩΡΓΙΟΣ Διεσθσνηής Καρδιοθωρακοτειροσργικής Κλινικής Γ.Ν. «Γ. Παπανικολάοσ» Θεζζαλονίκη What is the aortic root? represents the outflow tract from the LV provides
Functional anatomy of the aortic root ΔΡΟΣΟΣ ΓΕΩΡΓΙΟΣ Διεσθσνηής Καρδιοθωρακοτειροσργικής Κλινικής Γ.Ν. «Γ. Παπανικολάοσ» Θεζζαλονίκη What is the aortic root? represents the outflow tract from the LV provides
Middle mediastinum---- heart & pericardium. Dep. of Human Anatomy Zhou Hongying
 Middle mediastinum---- heart & pericardium Dep. of Human Anatomy Zhou Hongying eaglezhyxzy@163.com Subdivisions of the mediastinum Contents of Middle mediastinum Heart Pericardium: a serous sac enclosing
Middle mediastinum---- heart & pericardium Dep. of Human Anatomy Zhou Hongying eaglezhyxzy@163.com Subdivisions of the mediastinum Contents of Middle mediastinum Heart Pericardium: a serous sac enclosing
RIGHT VENTRICULAR SIZE AND FUNCTION
 RIGHT VENTRICULAR SIZE AND FUNCTION Edwin S. Tucay, MD, FPCC, FPCC, FPSE Philippine Society of Echocardiography Quezon City, Philippines Echo Mission, BRTTH, Legaspi City, July 1-2, 2016 NO DISCLOSURE
RIGHT VENTRICULAR SIZE AND FUNCTION Edwin S. Tucay, MD, FPCC, FPCC, FPSE Philippine Society of Echocardiography Quezon City, Philippines Echo Mission, BRTTH, Legaspi City, July 1-2, 2016 NO DISCLOSURE