Two Years Living with the EHRA/HRS Consensus Document of VT Ablation: Need for an Update?
|
|
|
- Preston Bradley
- 5 years ago
- Views:
Transcription

1 Two Years Living with the EHRA/HRS Consensus Document of VT Ablation: Need for an Update? David Wilber MD Loyola University of Chicago Disclosures: Biosense / Webster: Consultant, Investigator; Boston Scientific: Consultant, Investigator,; CardioInsight: consultant, investigator, Medtronic: Consultant, Investigator; St Jude: Investigator; Siemens: Consultant, Investigator
2 OVERVIEW Idiopathic VT PVC ablation spectrum of sites of origin for idiopathic VA Role of imaging and ancillary mapping techniques Scar Related VT Evolving role of substrate ablation Mortality associated with VT and ICD shocks, role of early intervention New insights on nonischemic myopathy substrates and mechanisms
3 PVC-MEDIATED MYOPATHY Subtle hemodynamic abnormalities in pts with frequent PVCs and normal LV function Increased LVEDD Diastolic dysfunction Increased BNP Normalization of LV function in pts with frequent PVCs and reduced ejection fraction of unknown etiology in small series following pharmacologic suppression (Duffee et al, MCP 1998) or catheter ablation (Takemoto et al, JACC 2005; Yarlaggadda et al, Circulation 2005; Bogun et al, Heart Rhythm 2007; Taieb et al, JICE 2007). PVC frequency in reported cases typically > 10,000/24 hr; can occur with any site of origin
4 PVC-MEDIATED MYOPATHY Mechanism unknown Not tachycardia mediated myopathy (normal heart rates) Single PVCs associated with complex transient alternation in intracellular calcium and membrane ionic currents, heart rate dynamics, and myocardial and peripheral autonomic stimulation and inhibition; cumulative effects with frequent ectopy unknown Dysynchronous myocardial activation Prevalence, individual risk, and time course of development poorly understood Differentiation from primary cardiomyopathy problematic (? role for MRI) Similar phenomenon may occur in patients with scar related ventricular ectopy, further impairing LV function
 had LVEF < 50% Mean PVC burden LV")
 had reduction of")
 or improvement > 15% (n=1) Baman, Bogun, Heart Rhythm")
5 PVC BURDEN AND LV FUNCTION 174 pts referred for ablation of PVCs 57 pts (33%) had LVEF < 50% Mean PVC burden LV dysfunction 33+13% Normal function, dilated LV 22+11% Normal function, normal LV 13+12% 146 pts (84%) had reduction of PVCs >80% 46/57 (81%) pts with LVD, normalization of function (n=45) or improvement > 15% (n=1) Baman, Bogun, Heart Rhythm 2010; 7:
6 LONG-TERM FOLLOW-UP OF FREQUENT PVCS 281 pts with frequent PVCs (>1000/24 hr) and no other heart disease 42 pts (15%) had LVD at baseline and underwent ablation Remaining 239 pts followed for 4-8 yrs (mean 5.6 yrs), baseline EF 64+7% Overall PVC frequency stable over time; changes in LV function noted after 4 years, primarily in pts with high baseline frequency (> 20,000/ 24 hr) 5% of study cohort developed > 6% decline in EF by end of study (20% of pts with > 20,000/24 hr Niwano et al, Heart 2009
7 SPECTRUM OF IDIOPATHIC VA (n=314) RV TACHYCARDIAS (54%) RVOT Pulmonary Artery PeriHis Tricuspid Annulus Other RV EPICARDIAL VT (10%) Anterior Interventricular vein Great cardiac vein Middle cardiac vein LV TACHYCARDIAS (34%) Fascicular Aortic Sinus of Valsalva LVOT endocardium / intramural Mitral Annulus Papillary muscle Other LV BUNDLE BRANCH REENRY (2%) LUMC 8/10



8 THE LEFT VENTRICULAR OSTIUM



9 ICE IMAGING OF OUTFLOW TRACT LCC





10 SOV VT: 3-D ICE IMAGING OF AORTA






11 RVOT septum LVOT septum RSOV LSOV AIV-GCV junction -30 ms -30 ms -52 ms -35 ms -10 ms PA SUPERIOR
 Intramural foci had similar EPI / ENDO activation times (within 20 ms) and had larger total RF applications to effect ablation Green et al, HRS Scientific Sessions 2010")
12 VT adjacent to LFT 25 pts underwent ablation of focal peri-left fibrous trigone (LFT) tachycardia in the following distribution: Distal Great Cardiac Vein 4 pts Endocardial Peri-LFT 16 pts Intramural Peri-LFT 5 pts (3/5 via GCV) Intramural foci had similar EPI / ENDO activation times (within 20 ms) and had larger total RF applications to effect ablation Green et al, HRS Scientific Sessions 2010 The electrocardiogram did not easily discriminate site of successful ablation.





13 SUPERIOR VT ORIGINATING ADJACENT TO LFT PA AO LV RAO LAO PA AO PA AO PA PA AO LV LV

14 IDIOPATHIC PVCs FROM PAPILLARY MUSCLES Anterolateral 200 ms Posterior


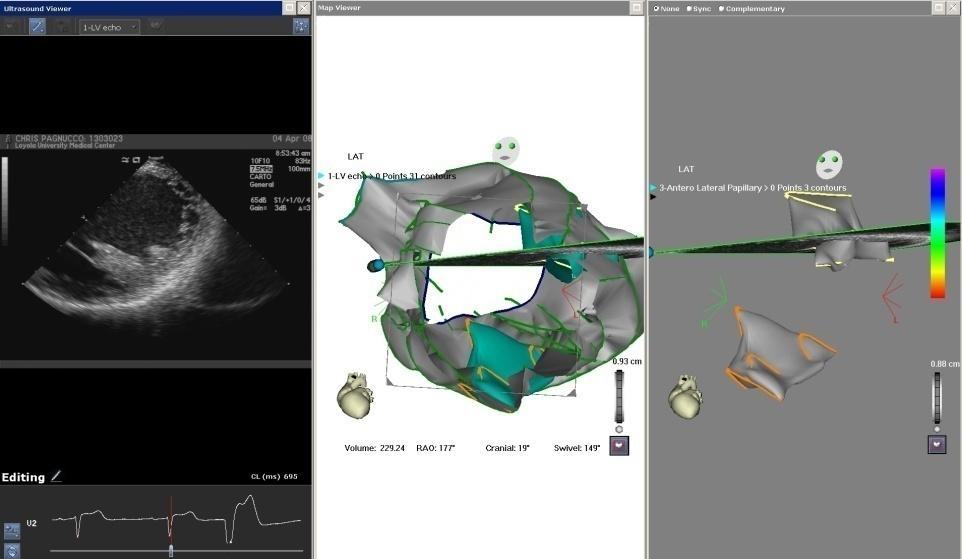
15 IMAGING THE PAPILLARY MUSCLES



16 ABLATION OF PVCS FROM ANTEROLATERAL PM A-L PM LPO

17 EPI ENDO ABLATION AT THE BASE OF THE ALPM
18 IDIOPATHIC EPICARDIAL LVVT - perivascular sites of origin - catecholamine enhanced, adenosine sensitive - may account for 5-10% of idiopathic VT Anterior GCV Posterior CS AIV MCV Daniels et al, Circulation 2006

19 DETECTION OF EPICARDIAL ILVT ON SURFACE ECG MDI > % sensitivity, 93% specificity for epicardial origin (N=240, 2009)
20 Baseline VT Induction RB-SA 380 ms RB-SA 430 ms RB-SA 430 ms LB-SA 500 ms
21 Other induced VTs RB-SA CL 350? RB-RIA CL 310
22 CHALLENGES Frequent spontaneous shifts in VT morphology spontaneous or catheter induced terminations (during mapping or entrainment attempts) As procedure progressed, low dose isoproterenol needed to sustain VT

23 Sinus Rhythm Mapping LVV = 390 cc Scar Area = 165 cm2 RAO LAO INFERIOR

24 Widespread Diastolic Potentials


25 Pacemapping in sinus VT4: LBBB VT3:RBBB


26 RF DEPLOYMENT Total 28 min RF application
27 Outcome Programmed stimulation with 3VES to refractioriness from the RV septum and LV apex on isoproterenol resulted in only 3-5 beats of polymorphic VT No further VT in subsequent month on low dose amiodarone 200 mg alone



28 DE-MRI for Substrate Identification Wijnmaalen et al, Eur Heart J 2011; 32:


29 Is activation mapping with hemodynamic support preferable to substrate mapping for unstable VT? Preliminary data confirm feasibility and reasonable safety Cost, case complexity are issues No data as yet to suggest superior outcomes; need for randomized studies
30 ISSUES WITH CURRENT APPROACHES TO MANAGEMENT OF ICD SHOCKS Device programming may decrease number of overall appropriate shocks, but much less often eliminates them completely; inappropriate shocks remain problematic Shocks, particularly when frequent, decrease QOL Limitations of AAD Associated with significant risk of adverse events requiring discontinuation; may be associated with increased noncardiac mortality when used at higher doses. Slow VT rate and may increase DFT and pacing thresholds Little information on efficacy in setting of prior drug failure Little or no role in setting of incessant slow VT or electrical storm
31 AAD SUPPRESSION OF ICD SHOCKS 412 pts, secondary prevention ICD within 21 days Amiodarone discontinued 18% Sotalol discontinued 23% 302 pts, secondary prevention ICD within 3 mo Sotalol discontinued 23% Connolly et al. JAMA 2006; Pacifico et al. NEJM 1999; 340:
32 ADVERSE OUTCOME AFTER ICD THERAPY 20% isolated VT/VF 4% electrical storm HR for death (storm) First 3 mo: 18 (8-40) > 3 mo: 3.5 ( HR for death (isolated) 2.5 (1.5-4) Predictors of storm (MVA) Isolated VT/VF: 9 (4-21) Predictors of HF events ICD shock 1.9 ( ) Moss, Circulation 2004; 110: Sesselberg, Heart Rhythm 2007;4: Goldenberg, Circulation 2006: 113:
33 ICD SHOCKS AND MORTALITY 269/811 pts received at least 1 ICD shock (128 appropriate only, 87 inappropriate only, 54 both) 18% mortality in first year post shock, majority from HF 30% of deaths within 24 hours of shock Exclude deaths within 24 hrs Poole et al, NEJM 2008; 359:
; 3934 VA episodes 20% increased risk of death / shocked episode VT frequency increased risk of death ATP treated VT or fast VT: 3% / episode Shocked fast VT: 31% / episode")
34 ICD THERAPY TYPE AND MORTALITY 2135 pts in 4 studies evaluating ATP (PainFREE I and II, EMPIRIC, PREPARE) Mean EF 32%, CAD 71%, BB 68%, Class I or II 82%, primary prevention 67% 24% of pts received therapy (50% ATP only); 3934 VA episodes 20% increased risk of death / shocked episode VT frequency increased risk of death ATP treated VT or fast VT: 3% / episode Shocked fast VT: 31% / episode Shocked VF: 15% / episode Sweeney et al, Heart Rhythm 2010; 7:
 Ablation may have favorable impact on outcome 95 pts with ES CAD 76%, NIDCM 10% hypotension, shock 50 pts Acute outcome 68 (72%) no")
35 ELECTRICAL STORM 10-40% of secondary prevention ICD patients, 3-5% of primary prevention, often on a background of chronic AAD therapy Cardiac mortality 30-50% at 2-3 yrs (Bansch JACC 2000, Exner Circulation 2001, Verma JCVE 2004, Gatzoulis Europace 2005) Ablation may have favorable impact on outcome 95 pts with ES CAD 76%, NIDCM 10% hypotension, shock 50 pts Acute outcome 68 (72%) no inducible VT 17 (18%) no clinical VT 10 (11%) clinical VTs induced Overall cardiac death 12% at mean 22 mo follow-up Carbucicchio et al, Circulation 2008; 117:

36 OUTCOME OF POSTMI VT ABLATION VT frequency reduced by 75% in 2/3 of pts The Multicenter Thermocool VT Ablation Trial One year mortality 18% Stevenson, Wilber, Natale et al, Circulation 2008, 118:
37 Substrate Mapping & Ablation in Sinus Rhythm to Halt Ventricular Tachycardia (SMASH VT) Trial Patients with recent ICD (within 6 mo) for secondary prevention (cardiac arrest, VT, syncope with inducible VT) and history of myocardial infarction Randomization to substrate ablation (N=64) or standard medical therapy (N=64) All pts received ACEI or ARB, ASA, and beta blockers Mean age 67+10, LVEF 32+9, FC III, IV 19% No procedure related deaths, major complications 5% No AAD permitted unless pt already receiving for supraventricular arrhythmia Reddy et al, NEJM 2007; 357:
38 Substrate Mapping & Ablation in Sinus Rhythm to Halt Ventricular Tachycardia (SMASH VT) Trial P = ICD Events (shocks+atp) All Cause Mortality Reddy et al, NEJM 2007; 357:
39 We need to consider earlier scar related VT ablation because. AAD have modest efficacy, particularly if shocks occur on preexisting drug therapy, and are associated with significant risk of adverse events Even a single or limited number of shocks predict increase risk of adverse cardiac events, including HF, electrical storm, and death Current techniques are applicable to all presentations, dramatically decrease the risk of therapies, and may completely eliminate VT in > 50% of pts Initial data suggest a more favorable response to ablation, with lower risk, when applied at an earlier stage of the disease BUT we need randomized trials to convince many
40 FREQUENCY OF EPICARDIAL SITES OF VT ORIGIN Structural heart disease Chagas Disease (30-40%) NIDCM (25-50%) Hypertrophic cardiomyopathy (up to 50%) ARVD (~ 30%) Post infarction VT (10%) Other ( Idiopathic LV aneurysm, sarcoid, noncompaction) Idiopathic ventricular tachycardia (5-10%)
 Correlated with voltage maps, and sites of successful VT ablation for endo and epi")

41 IMAGING OF NIDCM SUBSTRATE 14/29 pts with NIDCM and VA had scar (endo 7, mid 5, epi 2) Correlated with voltage maps, and sites of successful VT ablation for endo and epi scar; arrhythmias associated with predominantly intramural scar not successfully ablated Absence of scar more common in pts with PVCs only Bogun et al, JACC 2009; 53:


42 Superior View INTRAMURAL ORIGIN OF VT IN NIDCM MVA Endo Sinus Voltage Endo VT Activation EGM at earliest site MVA Epi Sinus Voltage Epi VT Activation

43 Ablation at earliest endocardial site terminated VT after 15 sec, but could be easily reinduced Ablation at earliest epicardial site terminated VT within 5 sec. No further inducible VT
44 Epicardial Ablation in ARVC 13 pts with failed endocardial ablation LVA more extensive on epicardium (< 1 mv, cm2) than endocardium (<1.5 mv, cm2) Basal RV thickness > 10 mm in 6/13 pts 27 epicardial VTs targeted Epicardial VTs opposite normal myocardium in 10 pts (77%), opposite ineffective endocardial sites 11 pts (85%, closest distance between sites 4-16 mm) 11/13 (85%) had no inducible VT at the end of the procedure During mean follow-up of mo, 77% no recurrent VT Garcia et al, Circulation 2009; 120:



45 Garcia et al, Circulation 2009; 120:
46 COMBINED EPI/ENDO APPROACH LUMC Experience 8 pts (5 prior failed endo ablation) Mean age 39 (20-62), 4 F 2 pts with mildly abnormal LV function All pts with ICDs, multiple sks despite AAD, incessant in 3 RV endo and epicardial mapping in all, LV mapping in 2 RV epicardial LVA exceeded endo LVA in 7/8 No LV LVA Ablation with 3.5 mm IT, max power 50 W 20 VTs induced 7 eliminated by endocardial ablation alone 11 required epicardial ablation (7/8 pts required epi ablation) 1 VT (CL 240) could not be localized





47 27 year old woman with ARVD and multiple VTs, prior ICD, and incompletely successful endocardial VT ablation Endo Endo Epi VT Epi RAO Sinus LAO
48 Reddy VY, d Avila A, Dukkipati S, Neuzil P, Doshi SK, Dauber K, Wilber D Long-term outcome after combined epi-endo ablation of ventricular tachycardia related to arrhythmogenic right ventricular cardiomyopathy. HRS pts (71% prior failed endo ablation) meeting ITF criteria 40 VTs induced at baseline (mean CL ms) 38/40 VTs (95%) eliminated acutely Mean follow-up mo Single procedure success rate 88% (15/17 pts)


49 EPICARDIAL ABLATION IN HOCM 10 pts with HOCM and SMVT 80% epicardial scar, 60% endocardial scar, 10% no scar 3/5 pts with ablation during SMVT had termination on endocardium (1 surgical cryo) 4 additional pts had both endocardial and epicardial substrate ablation During mean f/u mo, 7/9 pts free of recurrent VT Dukkipati S R et al. Circ A and E 2011;4:
50


51 Dickfeld T et al. Circ Arrhythm Electrophysiol 2011;4:


52 Tian J et al. Circ Arrhythm Electrophysiol 2010;3:
Antiarrhythmic Drugs and Ablation in Patients with ICD and Shocks
 Antiarrhythmic Drugs and Ablation in Patients with ICD and Shocks Alireza Ghorbani Sharif, MD Interventional Electrophysiologist Tehran Arrhythmia Clinic January 2016 Recurrent ICD shocks are associated
Antiarrhythmic Drugs and Ablation in Patients with ICD and Shocks Alireza Ghorbani Sharif, MD Interventional Electrophysiologist Tehran Arrhythmia Clinic January 2016 Recurrent ICD shocks are associated
The implantable cardioverter defibrillator is not enough: Ventricular Tachycardia Catheter Ablation in Patients with Structural Heart Disease
 The implantable cardioverter defibrillator is not enough: Ventricular Tachycardia Catheter Ablation in Patients with Structural Heart Disease Paolo Della Bella, MD Arrhythmia Department and Clinical Electrophysiology
The implantable cardioverter defibrillator is not enough: Ventricular Tachycardia Catheter Ablation in Patients with Structural Heart Disease Paolo Della Bella, MD Arrhythmia Department and Clinical Electrophysiology
Ablation of Ventricular Tachycardia in Non-Ischemic Cardiomyopathy
 Ablation of Ventricular Tachycardia in Non-Ischemic Cardiomyopathy Fermin C Garcia, MD University of Pennsylvania Cardiac Electrophysiology Philadelphia, PA Nothing to disclose No conflict of interest
Ablation of Ventricular Tachycardia in Non-Ischemic Cardiomyopathy Fermin C Garcia, MD University of Pennsylvania Cardiac Electrophysiology Philadelphia, PA Nothing to disclose No conflict of interest
Ablative Therapy for Ventricular Tachycardia
 Ablative Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS 2 nd Annual UC Davis Heart and Vascular Center Cardiovascular Nurse / Technologist Symposium May 5, 2012 Disclosures Research
Ablative Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS 2 nd Annual UC Davis Heart and Vascular Center Cardiovascular Nurse / Technologist Symposium May 5, 2012 Disclosures Research
ΔΠΔΜΒΑΣΙΚΗ ΘΔΡΑΠΔΙΑ ΚΟΙΛΙΑΚΩΝ ΑΡΡΤΘΜΙΩΝ
 ΔΠΔΜΒΑΣΙΚΗ ΘΔΡΑΠΔΙΑ ΚΟΙΛΙΑΚΩΝ ΑΡΡΤΘΜΙΩΝ ΣΔΛΙΟ ΠΑΡΑΚΔΤΑÏΓΗ ΓΙΔΤΘΤΝΣΗ ΔΤ Α Καρδιολογική Κλινική ΑΠΘ, Νοζοκομείο ΑΧΕΠΑ, Θεζζαλονίκη NO CONFLICT OF INTEREST INTRODUCTION Sustained VT is an important cause
ΔΠΔΜΒΑΣΙΚΗ ΘΔΡΑΠΔΙΑ ΚΟΙΛΙΑΚΩΝ ΑΡΡΤΘΜΙΩΝ ΣΔΛΙΟ ΠΑΡΑΚΔΤΑÏΓΗ ΓΙΔΤΘΤΝΣΗ ΔΤ Α Καρδιολογική Κλινική ΑΠΘ, Νοζοκομείο ΑΧΕΠΑ, Θεζζαλονίκη NO CONFLICT OF INTEREST INTRODUCTION Sustained VT is an important cause
Catheter ablation of monomorphic ventricular tachycardia. Department of Cardiology, IKEM, Prague, Czech Republic
 Catheter ablation of monomorphic ventricular tachycardia Department of Cardiology, IKEM, Prague, Czech Republic DECLARATION OF CONFLICT OF INTEREST None Ventricular tachycardia ablation in IKEM, Prague
Catheter ablation of monomorphic ventricular tachycardia Department of Cardiology, IKEM, Prague, Czech Republic DECLARATION OF CONFLICT OF INTEREST None Ventricular tachycardia ablation in IKEM, Prague
Map-Guided Ablation of Non-ischemic VT. Takashi Nitta Cardiovascular Surgery, Nippon Medical School Tokyo, JAPAN
 Map-Guided Ablation of Non-ischemic VT Takashi Nitta Cardiovascular Surgery, Nippon Medical School Tokyo, JAPAN nothing Declaration of Interest Catheter Ablation of Non-ischemic VT Sarcoidosis, 13, 6%
Map-Guided Ablation of Non-ischemic VT Takashi Nitta Cardiovascular Surgery, Nippon Medical School Tokyo, JAPAN nothing Declaration of Interest Catheter Ablation of Non-ischemic VT Sarcoidosis, 13, 6%
Advances in Ablation Therapy for Ventricular Tachycardia
 Advances in Ablation Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS Director, Cardiac Electrophysiology Training Program University of California, San Francisco For those of you who
Advances in Ablation Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS Director, Cardiac Electrophysiology Training Program University of California, San Francisco For those of you who
Prophylactic ablation
 Ventricular tachycardia in ischaemic heart disease. Update on electrical therapy 29 august 2010 Prophylactic ablation Pasquale Notarstefano Cardiovacular Department S. Donato Hospital, Arezzo (IT) Prophylactic
Ventricular tachycardia in ischaemic heart disease. Update on electrical therapy 29 august 2010 Prophylactic ablation Pasquale Notarstefano Cardiovacular Department S. Donato Hospital, Arezzo (IT) Prophylactic
Recurrent Implantable Defibrillator Discharges (ICD) Discharges ICD Storm
 Discharges ICD Storm") Recurrent Implantable Defibrillator Discharges (ICD) Discharges ICD Storm Guy Amit, MD, MPH Soroka University Medical Center Ben-Gurion University of the Negev Beer-Sheva, Israel Disclosures Consultant:
Recurrent Implantable Defibrillator Discharges (ICD) Discharges ICD Storm Guy Amit, MD, MPH Soroka University Medical Center Ben-Gurion University of the Negev Beer-Sheva, Israel Disclosures Consultant:
The patient with electric storm
 The complex patient in the cardiac care unit: The patient with electric storm Helmut U. Klein University of Rochester Medical Center Heart Research Follow-up Program and Isar Heart Center Muenchen Presenter
The complex patient in the cardiac care unit: The patient with electric storm Helmut U. Klein University of Rochester Medical Center Heart Research Follow-up Program and Isar Heart Center Muenchen Presenter
Mapping and Ablation of Challenging Outflow Tract VTs: Pulmonary Artery, LVOT, Epicardial
 Mapping and Ablation of Challenging Outflow Tract VTs: Pulmonary Artery, LVOT, Epicardial Samuel J. Asirvatham, MD Mayo Clinic Rochester California Heart Rhythm Symposium San Francisco, CA September 8,
Mapping and Ablation of Challenging Outflow Tract VTs: Pulmonary Artery, LVOT, Epicardial Samuel J. Asirvatham, MD Mayo Clinic Rochester California Heart Rhythm Symposium San Francisco, CA September 8,
Focus on the role of Catheter Ablation: Simple cases Intermediate level Difficult cases (and patients) Impossible (almost )
 Impossible (almost )") 22nd SHA Scientific Session 21 24 February 2011, Riyadh, KSA Management of Ventricular Arrhythmias: an Overview Corrado Carbucicchio Ventricular Intensive Care Unit Cardiac Arrhythmias Research Centre
22nd SHA Scientific Session 21 24 February 2011, Riyadh, KSA Management of Ventricular Arrhythmias: an Overview Corrado Carbucicchio Ventricular Intensive Care Unit Cardiac Arrhythmias Research Centre
Catheter Ablation of VT Without Structural Heart Disease 성균관의대 온영근
 Catheter Ablation of VT Without Structural Heart Disease 성균관의대 온영근 Idiopathic Monomorphic Ventricular Tachycardia Adenosine-sensitive Verapamil-sensitive Propranolol-sensitive Mech (Triggered activity)
Catheter Ablation of VT Without Structural Heart Disease 성균관의대 온영근 Idiopathic Monomorphic Ventricular Tachycardia Adenosine-sensitive Verapamil-sensitive Propranolol-sensitive Mech (Triggered activity)
NAAMA s 24 th International Medical Convention Medicine in the Next Decade: Challenges and Opportunities Beirut, Lebanon June 26 July 2, 2010
 NAAMA s 24 th International Medical Convention Medicine in the Next Decade: Challenges and Opportunities Beirut, Lebanon June 26 July 2, 2010 I have a financial interest/arrangement or affiliation with
NAAMA s 24 th International Medical Convention Medicine in the Next Decade: Challenges and Opportunities Beirut, Lebanon June 26 July 2, 2010 I have a financial interest/arrangement or affiliation with
Indications for catheter ablation in 2010: Ventricular Tachycardia
 Indications for catheter ablation in 2010: Ventricular Tachycardia Paolo Della Bella, MD Arrhythmia Department and Clinical Electrophysiology Laboratories Ospedale San Raffaele, IRCCS, Milan, Italy Europace
Indications for catheter ablation in 2010: Ventricular Tachycardia Paolo Della Bella, MD Arrhythmia Department and Clinical Electrophysiology Laboratories Ospedale San Raffaele, IRCCS, Milan, Italy Europace
Πρώτης γραμμή θεραπεία η κατάλυση κοιλιακής ταχυκαρδίας στην ισχαιμική μυοκαρδιοπάθεια
 Πρώτης γραμμή θεραπεία η κατάλυση κοιλιακής ταχυκαρδίας στην ισχαιμική μυοκαρδιοπάθεια Δ. Τσιαχρής Διευθυντής Εργαστηρίου Ηλεκτροφυσιολογίας - Βηματοδότησης, Ιατρικό Κέντρο Αθηνών, Αθήνα Ventricular tachycardia
Πρώτης γραμμή θεραπεία η κατάλυση κοιλιακής ταχυκαρδίας στην ισχαιμική μυοκαρδιοπάθεια Δ. Τσιαχρής Διευθυντής Εργαστηρίου Ηλεκτροφυσιολογίας - Βηματοδότησης, Ιατρικό Κέντρο Αθηνών, Αθήνα Ventricular tachycardia
VENTRICULAR TACHYCARDIA IN THE ABSENCE OF STRUCTURAL HEART DISEASE
 VENTRICULAR TACHYCARDIA IN THE ABSENCE OF STRUCTURAL HEART DISEASE Dimosthenis Avramidis, MD. Consultant Mitera Children s Hospital Athens Greece Scientific Associate 1st Cardiology Dpt Evangelismos Hospital
VENTRICULAR TACHYCARDIA IN THE ABSENCE OF STRUCTURAL HEART DISEASE Dimosthenis Avramidis, MD. Consultant Mitera Children s Hospital Athens Greece Scientific Associate 1st Cardiology Dpt Evangelismos Hospital
Catheter Ablation of Recurrent Ventricular Tachycardia Should Be Done Before Antiarrhythmic Therapy with Amiodarone is Tried CONTRA
 Catheter Ablation of Recurrent Ventricular Tachycardia Should Be Done Before Antiarrhythmic Therapy with Amiodarone is Tried CONTRA Erik Wissner, MD, F.A.C.C. Director - Magnetic Navigation Laboratory
Catheter Ablation of Recurrent Ventricular Tachycardia Should Be Done Before Antiarrhythmic Therapy with Amiodarone is Tried CONTRA Erik Wissner, MD, F.A.C.C. Director - Magnetic Navigation Laboratory
Epicardial Approach to Mapping and Ablation of VT: Clinical and ECG Predictors of Epicardial Location
 Epicardial Approach to Mapping and Ablation of VT: Clinical and ECG Predictors of Epicardial Location Mathew D. Hutchinson, MD, FACC, FHRS Perelman School of Medicine University of Pennsylvania Presenter
Epicardial Approach to Mapping and Ablation of VT: Clinical and ECG Predictors of Epicardial Location Mathew D. Hutchinson, MD, FACC, FHRS Perelman School of Medicine University of Pennsylvania Presenter
that number is extremely high. It s 16 episodes, or in other words, it s 14, one-four, ICD shocks per patient per day.
 Doctor Karlsner, Doctor Schumosky, ladies and gentlemen. It s my real pleasure to participate in this session on controversial issues in the management of ventricular tachycardia and I m sure that will
Doctor Karlsner, Doctor Schumosky, ladies and gentlemen. It s my real pleasure to participate in this session on controversial issues in the management of ventricular tachycardia and I m sure that will
Novel Approaches to VT Management Glenn M Polin MD
 Novel Approaches to VT Management Glenn M Polin MD Medical Director, Electrophysiology Laboratory John Ochsner Heart and Vascular Institute New Orleans, LA Disclosures Pfizer Speaker Bureau Bristol Myers
Novel Approaches to VT Management Glenn M Polin MD Medical Director, Electrophysiology Laboratory John Ochsner Heart and Vascular Institute New Orleans, LA Disclosures Pfizer Speaker Bureau Bristol Myers
Epicardial VT Ablation The Cleveland Clinic Experience
 Epicardial VT Ablation The Cleveland Clinic Experience Walid Saliba, MD, FHRS Director, EP Lab Cardiac Electrophysiology Heart and Vascular Institute Epicardial Access in the EP Lab Why Epicardial Special
Epicardial VT Ablation The Cleveland Clinic Experience Walid Saliba, MD, FHRS Director, EP Lab Cardiac Electrophysiology Heart and Vascular Institute Epicardial Access in the EP Lab Why Epicardial Special
Mapping and Ablation of VT in The Operating Room
 Mapping and Ablation of VT in The Operating Room Sanjay Dixit, M.D. Associate Professor, University of Pennsylvania School of Medicine Director, Cardiac Electrophysiology Laboratory, Philadelphia V.A.M.C.
Mapping and Ablation of VT in The Operating Room Sanjay Dixit, M.D. Associate Professor, University of Pennsylvania School of Medicine Director, Cardiac Electrophysiology Laboratory, Philadelphia V.A.M.C.
Ventricular tachycardia and ischemia. Martin Jan Schalij Department of Cardiology Leiden University Medical Center
 Ventricular tachycardia and ischemia Martin Jan Schalij Department of Cardiology Leiden University Medical Center Disclosure: Research grants from: Boston Scientific Medtronic Biotronik Sudden Cardiac
Ventricular tachycardia and ischemia Martin Jan Schalij Department of Cardiology Leiden University Medical Center Disclosure: Research grants from: Boston Scientific Medtronic Biotronik Sudden Cardiac
EHRA EUROPACE How to perform epicardial ventricular tachycardia mapping and ablation
 EHRA EUROPACE 2011 How to perform epicardial ventricular tachycardia mapping and ablation Jacob Atié Director Arrhythmias Department Federal University of Rio de janeiro jacobatie1@gmail.com Presenter
EHRA EUROPACE 2011 How to perform epicardial ventricular tachycardia mapping and ablation Jacob Atié Director Arrhythmias Department Federal University of Rio de janeiro jacobatie1@gmail.com Presenter
ICD Shocks: How to Avoid? Josef Kautzner Department of Cardiology, Institute for Clinical and Experimental Medicine Prague, Czech Republic
 ICD Shocks: How to Avoid? Josef Kautzner Department of Cardiology, Institute for Clinical and Experimental Medicine Prague, Czech Republic joka@medicon.cz www.ikem.cz My Disclosures Advisory Board member
ICD Shocks: How to Avoid? Josef Kautzner Department of Cardiology, Institute for Clinical and Experimental Medicine Prague, Czech Republic joka@medicon.cz www.ikem.cz My Disclosures Advisory Board member
Disclosures 8/29/2016. VT Ablation 2016: Indications and Expected Outcomes. Medtronic: advisory board, review panel. St Jude Medical: speakers bureau
 VT Ablation 2016: Indications and Expected Outcomes California Heart Rhythm Symposium 2016 Henry H. Hsia, MD, FACC, FHRS San Francisco VA Medical Center, University of California, San Francisco Disclosures
VT Ablation 2016: Indications and Expected Outcomes California Heart Rhythm Symposium 2016 Henry H. Hsia, MD, FACC, FHRS San Francisco VA Medical Center, University of California, San Francisco Disclosures
PVCs: Do they cause Cardiomyopathy? Raed Abu Sham a, M.D.
 PVCs: Do they cause Cardiomyopathy? Raed Abu Sham a, M.D. Cardiologist and Electrophysiologist No conflict of interest related to this presentation Objectives 1. PVCs are benign. What is the Evidence?
PVCs: Do they cause Cardiomyopathy? Raed Abu Sham a, M.D. Cardiologist and Electrophysiologist No conflict of interest related to this presentation Objectives 1. PVCs are benign. What is the Evidence?
Ventricular Tachycardia Ablation. Saverio Iacopino, MD, FACC, FESC
 Ventricular Tachycardia Ablation Saverio Iacopino, MD, FACC, FESC ü Ventricular arrhythmias, both symptomatic and asymptomatic, are common, but syncope and SCD are infrequent initial manifestations of
Ventricular Tachycardia Ablation Saverio Iacopino, MD, FACC, FESC ü Ventricular arrhythmias, both symptomatic and asymptomatic, are common, but syncope and SCD are infrequent initial manifestations of
Electrical Storm in Coronary Artery Disease. Saeed Oraii MD, Cardiologist Interventional Electrophysiologist Tehran Arrhythmia Clinic July 2016
 Electrical Storm in Coronary Artery Disease Saeed Oraii MD, Cardiologist Interventional Electrophysiologist Tehran Arrhythmia Clinic July 2016 48 yrs. Old diabetic with ACS 48 yrs. Old diabetic with ACS
Electrical Storm in Coronary Artery Disease Saeed Oraii MD, Cardiologist Interventional Electrophysiologist Tehran Arrhythmia Clinic July 2016 48 yrs. Old diabetic with ACS 48 yrs. Old diabetic with ACS
- Special VT Cases - Idiopathic Dilated Cardiomyopathy. D. Bänsch
 - Special VT Cases - Idiopathic Dilated Cardiomyopathy D. Bänsch Introduction VT Ablation in CAD Strickberger SA, et al. J Am Coll Cardiol 2000 (35: 414-21) Sra J. et al. Pacing Clin Electrophysiol 2001
- Special VT Cases - Idiopathic Dilated Cardiomyopathy D. Bänsch Introduction VT Ablation in CAD Strickberger SA, et al. J Am Coll Cardiol 2000 (35: 414-21) Sra J. et al. Pacing Clin Electrophysiol 2001
Treatment of VT of Purkinje fiber origin: ablation targets and outcome
 Treatment of VT of Purkinje fiber origin: ablation targets and outcome Ch. Piorkowski University Leipzig - Heart Center - Dept. of Electrophysiology Leipzig, Germany Presenter Disclosure Information Gerhard
Treatment of VT of Purkinje fiber origin: ablation targets and outcome Ch. Piorkowski University Leipzig - Heart Center - Dept. of Electrophysiology Leipzig, Germany Presenter Disclosure Information Gerhard
Technique of Epicardial VT Ablation
 CARTO Club Jan 2014 Technique of Epicardial VT Ablation Amir AbdelWahab, MD Electrophysiology and Pacing Service Department of Cardiovascular Medicine, Cairo University Need for Epicardial VT ablation
CARTO Club Jan 2014 Technique of Epicardial VT Ablation Amir AbdelWahab, MD Electrophysiology and Pacing Service Department of Cardiovascular Medicine, Cairo University Need for Epicardial VT ablation
Tachycardia-induced heart failure - Does it exist?
 Tachycardia-induced heart failure - Does it exist? PD Dr Etienne Delacrétaz Clinique Cecil et Hôpital de Fribourg SSC Cardiology meeting 2015 Zürich Rapid atrial fibrillation is a common cause of heart
Tachycardia-induced heart failure - Does it exist? PD Dr Etienne Delacrétaz Clinique Cecil et Hôpital de Fribourg SSC Cardiology meeting 2015 Zürich Rapid atrial fibrillation is a common cause of heart
INNOVATIONS IN DEVICE THERAPY:
 INNOVATIONS IN DEVICE THERAPY: Subcutaneous ICDs, Leadless Pacemakers, CRT Indications David J Wilber MD Loyola University Medical Center Disclosures: ACC Foundation: Consultant; Biosense / Webster: Consultant,
INNOVATIONS IN DEVICE THERAPY: Subcutaneous ICDs, Leadless Pacemakers, CRT Indications David J Wilber MD Loyola University Medical Center Disclosures: ACC Foundation: Consultant; Biosense / Webster: Consultant,
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh
 Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Φαρμακεσηική αγωγή ζηις ιδιοπαθείς κοιλιακές αρρσθμίες. Άννα Κωζηοπούλοσ Επιμελήηρια Α Ωνάζειο Καρδιοτειροσργικό Κένηρο
 Φαρμακεσηική αγωγή ζηις ιδιοπαθείς κοιλιακές αρρσθμίες Άννα Κωζηοπούλοσ Επιμελήηρια Α Ωνάζειο Καρδιοτειροσργικό Κένηρο Όλες οι κοιλιακές αρρσθμίες δεν είναι ίδιες Υπάρτοσν διαθορές ζηον πληθυσμό, ηον μηχανισμό
Φαρμακεσηική αγωγή ζηις ιδιοπαθείς κοιλιακές αρρσθμίες Άννα Κωζηοπούλοσ Επιμελήηρια Α Ωνάζειο Καρδιοτειροσργικό Κένηρο Όλες οι κοιλιακές αρρσθμίες δεν είναι ίδιες Υπάρτοσν διαθορές ζηον πληθυσμό, ηον μηχανισμό
Urgent VT Ablation in a Patient with Presumed ARVC
 Urgent VT Ablation in a Patient with Presumed ARVC Mr Alex Cambridge, Chief Cardiac Physiologist, St. Barts Hospital, London, UK The patient, a 52 year-old male, attended the ICD clinic without an appointment
Urgent VT Ablation in a Patient with Presumed ARVC Mr Alex Cambridge, Chief Cardiac Physiologist, St. Barts Hospital, London, UK The patient, a 52 year-old male, attended the ICD clinic without an appointment
Εκθορηίζεις απινιδωηή και θνηηόηηηα: μέθοδοι μείωζης ηων θεραπειών απινίδωζης
 Εκθορηίζεις απινιδωηή και θνηηόηηηα: μέθοδοι μείωζης ηων θεραπειών απινίδωζης Εμμ. Μ. Κανοσπάκης Καρδιολογική Κλινική Πανεπιζηημίοσ Κρήηης Lessons from large trials Conditioning Rhythm and Electrical Therapy
Εκθορηίζεις απινιδωηή και θνηηόηηηα: μέθοδοι μείωζης ηων θεραπειών απινίδωζης Εμμ. Μ. Κανοσπάκης Καρδιολογική Κλινική Πανεπιζηημίοσ Κρήηης Lessons from large trials Conditioning Rhythm and Electrical Therapy
Case Report Coexistence of Atrioventricular Nodal Reentrant Tachycardia and Idiopathic Left Ventricular Outflow-Tract Tachycardia
 www.ipej.org 149 Case Report Coexistence of Atrioventricular Nodal Reentrant Tachycardia and Idiopathic Left Ventricular Outflow-Tract Tachycardia Majid Haghjoo, M.D, Arash Arya, M.D, Mohammadreza Dehghani,
www.ipej.org 149 Case Report Coexistence of Atrioventricular Nodal Reentrant Tachycardia and Idiopathic Left Ventricular Outflow-Tract Tachycardia Majid Haghjoo, M.D, Arash Arya, M.D, Mohammadreza Dehghani,
Ventricular arrhythmias in acute coronary syndromes. Dimitrios Manolatos, MD, PhD, FESC Electrophysiology Lab Evaggelismos General Hospital
 Ventricular arrhythmias in acute coronary syndromes Dimitrios Manolatos, MD, PhD, FESC Electrophysiology Lab Evaggelismos General Hospital introduction myocardial ischaemia and infarction leads to severe
Ventricular arrhythmias in acute coronary syndromes Dimitrios Manolatos, MD, PhD, FESC Electrophysiology Lab Evaggelismos General Hospital introduction myocardial ischaemia and infarction leads to severe
Alcohol Septal Ablation for Hypertrophic Obstructive Cardiomyopathy. CardioVascular Research Foundation
 Alcohol Septal Ablation for Hypertrophic Obstructive Cardiomyopathy Alcohol Septal Ablation (ASA) Nonsurgical technique for septal myocardial reduction Dramatic hemodynamic improvement Technically easy
Alcohol Septal Ablation for Hypertrophic Obstructive Cardiomyopathy Alcohol Septal Ablation (ASA) Nonsurgical technique for septal myocardial reduction Dramatic hemodynamic improvement Technically easy
Theroleofcatheterablationinthemanagement of ventricular tachycardia
 European Heart Journal Advance Access published August 31, 2015 European Heart Journal doi:10.1093/eurheartj/ehv421 REVIEW Novel therapeutic concepts Theroleofcatheterinthemanagement of ventricular tachycardia
European Heart Journal Advance Access published August 31, 2015 European Heart Journal doi:10.1093/eurheartj/ehv421 REVIEW Novel therapeutic concepts Theroleofcatheterinthemanagement of ventricular tachycardia
Medicine. Dynamic Changes of QRS Morphology of Premature Ventricular Contractions During Ablation in the Right Ventricular Outflow Tract
 Medicine CLINICAL CASE REPORT Dynamic Changes of QRS Morphology of Premature Ventricular Contractions During Ablation in the Right Ventricular Outflow Tract A Case Report Li Yue-Chun, MD, Lin Jia-Feng,
Medicine CLINICAL CASE REPORT Dynamic Changes of QRS Morphology of Premature Ventricular Contractions During Ablation in the Right Ventricular Outflow Tract A Case Report Li Yue-Chun, MD, Lin Jia-Feng,
Arrhythmias (II) Ventricular Arrhythmias. Disclosures
 Ventricular Arrhythmias. Disclosures") Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
When to ablate patients with premature ventricular complexes?
 When to ablate patients with premature ventricular complexes? Nikolaos Fragakis Assistant Professor, FESC 3rd University Cardiology Department Hippokration Hospital, Thessaloniki 58 year-old female Case
When to ablate patients with premature ventricular complexes? Nikolaos Fragakis Assistant Professor, FESC 3rd University Cardiology Department Hippokration Hospital, Thessaloniki 58 year-old female Case
Septal ventricular arrhythmias in the presence of structural
 Intramural Idiopathic Ventricular Arrhythmias Originating in the Intraventricular Septum Mapping and Ablation Miki Yokokawa, MD; Eric Good, DO; Aman Chugh, MD; Frank Pelosi, Jr, MD; Thomas Crawford, MD;
Intramural Idiopathic Ventricular Arrhythmias Originating in the Intraventricular Septum Mapping and Ablation Miki Yokokawa, MD; Eric Good, DO; Aman Chugh, MD; Frank Pelosi, Jr, MD; Thomas Crawford, MD;
ICD THERAPIES: are they harmful or just high risk markers?
 ICD THERAPIES: are they harmful or just high risk markers? Konstantinos P. Letsas, MD, PhD, FESC LAB OF CARDIAC ELECTROPHYSIOLOGY EVANGELISMOS GENERAL HOSPITAL ATHENS ICD therapies are common In a meta-analysis
ICD THERAPIES: are they harmful or just high risk markers? Konstantinos P. Letsas, MD, PhD, FESC LAB OF CARDIAC ELECTROPHYSIOLOGY EVANGELISMOS GENERAL HOSPITAL ATHENS ICD therapies are common In a meta-analysis
Idiopathic Ventricular Tachycardia Need for an Update in EHRA/HRS Consensus?
 Idiopathic Ventricular Tachycardia Need for an Update in EHRA/HRS Consensus? Arash Arya, M.D. Department of Interventional Electrophysiology Heart Center University of Leipzig Disclosures: NONE Idiopathic
Idiopathic Ventricular Tachycardia Need for an Update in EHRA/HRS Consensus? Arash Arya, M.D. Department of Interventional Electrophysiology Heart Center University of Leipzig Disclosures: NONE Idiopathic
The Therapeutic Role of the Implantable Cardioverter Defibrillator in Arrhythmogenic Right Ventricular Dysplasia
 The Therapeutic Role of the Implantable Cardioverter Defibrillator in Arrhythmogenic Right Ventricular Dysplasia By Sandeep Joshi, MD and Jonathan S. Steinberg, MD Arrhythmia Service, Division of Cardiology
The Therapeutic Role of the Implantable Cardioverter Defibrillator in Arrhythmogenic Right Ventricular Dysplasia By Sandeep Joshi, MD and Jonathan S. Steinberg, MD Arrhythmia Service, Division of Cardiology
HYPERTROPHIC CARDIOMYOPATHY: Severe Heart Failure. Paolo Spirito, Genoa, Italy
 HYPERTROPHIC CARDIOMYOPATHY: Severe Heart Failure Paolo Spirito, Genoa, Italy Clinical Substrates for Heart Failure Symptoms in HCM Diastolic dysfunction Atrial fibrillation LV outflow obstruction Evolution
HYPERTROPHIC CARDIOMYOPATHY: Severe Heart Failure Paolo Spirito, Genoa, Italy Clinical Substrates for Heart Failure Symptoms in HCM Diastolic dysfunction Atrial fibrillation LV outflow obstruction Evolution
Intramural Reentrant Ventricular Tachycardia in a Patient with Severe Hypertensive Left Ventricular Hypertrophy
 Case Report Print ISSN 1738-5520 On-line ISSN 1738-5555 Korean Circulation Journal Intramural Reentrant Ventricular Tachycardia in a Patient with Severe Hypertensive Left Ventricular Hypertrophy Chin-Yu
Case Report Print ISSN 1738-5520 On-line ISSN 1738-5555 Korean Circulation Journal Intramural Reentrant Ventricular Tachycardia in a Patient with Severe Hypertensive Left Ventricular Hypertrophy Chin-Yu
Ventricular arrhythmias
 Ventricular arrhythmias Assoc.Prof. Lucie Riedlbauchová, MD, PhD Department of Cardiology University HospitalMotol and2nd FacultyofMedicine, Charles University in Prague Definition and classification Ventricular
Ventricular arrhythmias Assoc.Prof. Lucie Riedlbauchová, MD, PhD Department of Cardiology University HospitalMotol and2nd FacultyofMedicine, Charles University in Prague Definition and classification Ventricular
Shock Reduction Strategies Michael Geist E. Wolfson MC
 Shock Reduction Strategies Michael Geist E. Wolfson MC Shock Therapy Thanks, I needed that! Why Do We Need To Reduce Shocks Long-term outcome after ICD and CRT implantation and influence of remote device
Shock Reduction Strategies Michael Geist E. Wolfson MC Shock Therapy Thanks, I needed that! Why Do We Need To Reduce Shocks Long-term outcome after ICD and CRT implantation and influence of remote device
Ablation Update and Case Studies. Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group
 Ablation Update and Case Studies Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group Disclosures No financial relationships to disclose Objectives At the conclusion of this activity,
Ablation Update and Case Studies Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group Disclosures No financial relationships to disclose Objectives At the conclusion of this activity,
Role of Ablation of AF and PVCs in the Management of Heart Failure
 Role of Ablation of AF and PVCs in the Management of Heart Failure Cara Pellegrini, MD, FHRS Acting Chief, Cardiology, SF VA Associate Professor of Medicine, UCSF Disclosures I have nothing to disclose
Role of Ablation of AF and PVCs in the Management of Heart Failure Cara Pellegrini, MD, FHRS Acting Chief, Cardiology, SF VA Associate Professor of Medicine, UCSF Disclosures I have nothing to disclose
Title. CitationJournal of electrocardiology, 46(6): Issue Date Doc URL. Type. File Information
: Issue Date Doc URL. Type. File Information") Title Unique preferential conduction within the isolated s with non-ischemic dilated cardiomyopathy Author(s)Watanabe, Masaya; Yokoshiki, Hisashi; Mitsuyama, Hir CitationJournal of electrocardiology, 46(6):
Title Unique preferential conduction within the isolated s with non-ischemic dilated cardiomyopathy Author(s)Watanabe, Masaya; Yokoshiki, Hisashi; Mitsuyama, Hir CitationJournal of electrocardiology, 46(6):
Tachycardia Devices Indications and Basic Trouble Shooting
 Tachycardia Devices Indications and Basic Trouble Shooting Peter A. Brady, MD., FRCP Cardiology Review Course London, March 6 th, 2014 2011 MFMER 3134946-1 Tachycardia Devices ICD Indications Primary and
Tachycardia Devices Indications and Basic Trouble Shooting Peter A. Brady, MD., FRCP Cardiology Review Course London, March 6 th, 2014 2011 MFMER 3134946-1 Tachycardia Devices ICD Indications Primary and
Ventricular Arrhythmias
 Presenting your most challenging cases Venice Arrhythmias Ventricular Arrhythmias Gioia Turitto, MD Presenter Disclosure Information A questionable indication for CRT-D in a patient with VT after successful
Presenting your most challenging cases Venice Arrhythmias Ventricular Arrhythmias Gioia Turitto, MD Presenter Disclosure Information A questionable indication for CRT-D in a patient with VT after successful
Case Report Substrate Based Ablation of Ventricular Tachycardia Through An Epicardial Approach
 www.ipej.org 364 Case Report Substrate Based Ablation of Ventricular Tachycardia Through An Epicardial Approach Aman Makhija DM 1, Ajit Thachil DM 1, C Sridevi, DNB 2, B Hygriv Rao, DM 2, S Jaishankar
www.ipej.org 364 Case Report Substrate Based Ablation of Ventricular Tachycardia Through An Epicardial Approach Aman Makhija DM 1, Ajit Thachil DM 1, C Sridevi, DNB 2, B Hygriv Rao, DM 2, S Jaishankar
Atrial Fibrillation: Catheter Ablation with New Technologies, Improving Quality of Life and Outcomes in Various Disease States
 Atrial Fibrillation: Catheter Ablation with New Technologies, Improving Quality of Life and Outcomes in Various Disease States Srinivas R. Dukkipati, MD Co-Director, Cardiac Arrhythmia Service The Mount
Atrial Fibrillation: Catheter Ablation with New Technologies, Improving Quality of Life and Outcomes in Various Disease States Srinivas R. Dukkipati, MD Co-Director, Cardiac Arrhythmia Service The Mount
Outflow Tract Ventricular Tachycardia Always Benign?
 Outflow Tract Ventricular Tachycardia Always Benign? Arash Arya, M.D. Department of Interventional Electrophysiology Heart Center University of Leipzig Disclosures: NONE Outflow Ventricular Tachycardia
Outflow Tract Ventricular Tachycardia Always Benign? Arash Arya, M.D. Department of Interventional Electrophysiology Heart Center University of Leipzig Disclosures: NONE Outflow Ventricular Tachycardia
Ventricular Tachycardia Substrate. For the ablationist. Stanley Tung, MD FRCPC Arrhythmia Service/St Paul Hospital University of British Columbia
 Ventricular Tachycardia Substrate For the ablationist Stanley Tung, MD FRCPC Arrhythmia Service/St Paul Hospital University of British Columbia Two Attitudes of Ventricular Tachycardia Ablation 1 2C:\Documents
Ventricular Tachycardia Substrate For the ablationist Stanley Tung, MD FRCPC Arrhythmia Service/St Paul Hospital University of British Columbia Two Attitudes of Ventricular Tachycardia Ablation 1 2C:\Documents
INTRODUCTION. left ventricular non-compaction is a sporadic or familial cardiomyopathy characterized by
 A Rare Case of Arrhythmogenic Right Ventricular Cardiomyopathy Co-existing with Isolated Left Ventricular Non-compaction NS Yelgeç, AT Alper, Aİ Tekkeşin, C Türkkan INTRODUCTION Arrhythmogenic right ventricular
A Rare Case of Arrhythmogenic Right Ventricular Cardiomyopathy Co-existing with Isolated Left Ventricular Non-compaction NS Yelgeç, AT Alper, Aİ Tekkeşin, C Türkkan INTRODUCTION Arrhythmogenic right ventricular
Do All Patients With An ICD Indication Need A BiV Pacing Device?
 Do All Patients With An ICD Indication Need A BiV Pacing Device? Muhammad A. Hammouda, MD Electrophysiology Laboratory Department of Critical Care Medicine Cairo University Etiology and Pathophysiology
Do All Patients With An ICD Indication Need A BiV Pacing Device? Muhammad A. Hammouda, MD Electrophysiology Laboratory Department of Critical Care Medicine Cairo University Etiology and Pathophysiology
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT JANUARY 24, 2012
 IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
Managing Hypertrophic Cardiomyopathy with Imaging. Gisela C. Mueller University of Michigan Department of Radiology
 Managing Hypertrophic Cardiomyopathy with Imaging Gisela C. Mueller University of Michigan Department of Radiology Disclosures Gadolinium contrast material for cardiac MRI Acronyms Afib CAD Atrial fibrillation
Managing Hypertrophic Cardiomyopathy with Imaging Gisela C. Mueller University of Michigan Department of Radiology Disclosures Gadolinium contrast material for cardiac MRI Acronyms Afib CAD Atrial fibrillation
The Egyptian Journal of Hospital Medicine (Jan. 2016) Vol. 62, Page 51-56
 Vol. 62, Page 51-56") The Egyptian Journal of Hospital Medicine (Jan. 216) Vol. 62, Page 51-56 Radiofrequency Catheter Ablation of Premature Ventricular Beats among Egyptians: Predictors of Success and Recurrence Mustafa Mohamed
The Egyptian Journal of Hospital Medicine (Jan. 216) Vol. 62, Page 51-56 Radiofrequency Catheter Ablation of Premature Ventricular Beats among Egyptians: Predictors of Success and Recurrence Mustafa Mohamed
Ablation of persistent AF Is it different than paroxysmal?
 Ablation of persistent AF Is it different than paroxysmal? Steven J. Kalbfleisch, MD Medical Director Electrophysiology Laboratory Ohio State University Wexner Medical Center Ross Heart Hospital Columbus,
Ablation of persistent AF Is it different than paroxysmal? Steven J. Kalbfleisch, MD Medical Director Electrophysiology Laboratory Ohio State University Wexner Medical Center Ross Heart Hospital Columbus,
Interventional solutions for atrial fibrillation in patients with heart failure
 Interventional solutions for atrial fibrillation in patients with heart failure Advances in Cardiovascular Arrhythmias Great Innovations in Cardiology Matteo Anselmino, MD PhD Division of Cardiology Department
Interventional solutions for atrial fibrillation in patients with heart failure Advances in Cardiovascular Arrhythmias Great Innovations in Cardiology Matteo Anselmino, MD PhD Division of Cardiology Department
Reentrant Ventricular Tachycardia Originating in the Right Ventricular Outflow Tract
 Circ J 2008; 72: 855 860 Reentrant Ventricular Tachycardia Originating in the Right Ventricular Outflow Tract Slow Conduction Identified by Right Coronary Artery Ostium Pacing Emi Nakano, MD; Tomoo Harada,
Circ J 2008; 72: 855 860 Reentrant Ventricular Tachycardia Originating in the Right Ventricular Outflow Tract Slow Conduction Identified by Right Coronary Artery Ostium Pacing Emi Nakano, MD; Tomoo Harada,
Management of Syncope in Heart Failure. University of Iowa
 Management of Syncope in Heart Failure Brian Olshansky University of Iowa 1 Syncope Transient loss of consciousness, with rapid, usually complete, recovery, with or without prodrome A common, non-specific,
Management of Syncope in Heart Failure Brian Olshansky University of Iowa 1 Syncope Transient loss of consciousness, with rapid, usually complete, recovery, with or without prodrome A common, non-specific,
DIAGNOSIS AND MANAGEMENT OF ARRHYTHMOGENIC CARDIOMYOPATHY. David SIU MD ( 蕭頌華醫生 ) Division of Cardiology The University of Hong Kong
 Division of Cardiology The University of Hong Kong") APHRS Summit 2018 in conjunction with HKCC Heart Rhythm Refresher Course DIAGNOSIS AND MANAGEMENT OF ARRHYTHMOGENIC CARDIOMYOPATHY David SIU MD ( 蕭頌華醫生 ) Division of Cardiology The University of Hong Kong
APHRS Summit 2018 in conjunction with HKCC Heart Rhythm Refresher Course DIAGNOSIS AND MANAGEMENT OF ARRHYTHMOGENIC CARDIOMYOPATHY David SIU MD ( 蕭頌華醫生 ) Division of Cardiology The University of Hong Kong
Title. CitationJournal of Electrocardiology, 43(5): Issue Date Doc URL. Type. File Information.
: Issue Date Doc URL. Type. File Information.") Title Pleomorphic ventricular tachycardia originating from Author(s)Yokoshiki, Hisashi; Mitsuyama, Hirofumi; Watanabe, M CitationJournal of Electrocardiology, 43(5): 452-458 Issue Date 2010-09 Doc URL
Title Pleomorphic ventricular tachycardia originating from Author(s)Yokoshiki, Hisashi; Mitsuyama, Hirofumi; Watanabe, M CitationJournal of Electrocardiology, 43(5): 452-458 Issue Date 2010-09 Doc URL
Electroanatomic Substrate and Outcome of Catheter Ablative Therapy for Ventricular Tachycardia in Setting of Right Ventricular Cardiomyopathy
 Electroanatomic Substrate and Outcome of Catheter Ablative Therapy for Ventricular Tachycardia in Setting of Right Ventricular Cardiomyopathy Francis E. Marchlinski, MD; Erica Zado, PA-C; Sanjay Dixit,
Electroanatomic Substrate and Outcome of Catheter Ablative Therapy for Ventricular Tachycardia in Setting of Right Ventricular Cardiomyopathy Francis E. Marchlinski, MD; Erica Zado, PA-C; Sanjay Dixit,
Use of Catheter Ablation in the Treatment of Ventricular Tachycardia Triggered by Premature Ventricular Contraction
 J Arrhythmia Vol 22 No 3 2006 Case Report Use of Catheter Ablation in the Treatment of Ventricular Tachycardia Triggered by Premature Ventricular Contraction sao Kato MD, Toru wa MD, Yasushi Suzuki MD,
J Arrhythmia Vol 22 No 3 2006 Case Report Use of Catheter Ablation in the Treatment of Ventricular Tachycardia Triggered by Premature Ventricular Contraction sao Kato MD, Toru wa MD, Yasushi Suzuki MD,
Long-Term Outcome and Risks of Catheter Ablation for Atrial Fibrillation
 Long-Term Outcome and Risks of Catheter Ablation for Atrial Fibrillation Carlo Pappone, MD, PhD, FACC EP Director, Villa Maria Hospital Group How many times AF can increase mortality DO MORTALITY REALLY
Long-Term Outcome and Risks of Catheter Ablation for Atrial Fibrillation Carlo Pappone, MD, PhD, FACC EP Director, Villa Maria Hospital Group How many times AF can increase mortality DO MORTALITY REALLY
Prevention of Sudden Death in ARVC
 ESC Munich, August 29, 2012 Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC): Prevention of Sudden Death in ARVC Thomas Wichter, MD, FESC Professor of Medicine - Cardiology Marienhospital Osnabrück
ESC Munich, August 29, 2012 Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC): Prevention of Sudden Death in ARVC Thomas Wichter, MD, FESC Professor of Medicine - Cardiology Marienhospital Osnabrück
How to Distinguish Focal Atrial Tachycardia from Small Circuits and Reentry
 How to Distinguish Focal Atrial Tachycardia from Small Circuits and Reentry Pierre Jaïs; Bordeaux, France IHU LIRYC ANR-10-IAHU-04 Equipex MUSIC imaging platform ANR-11-EQPX-0030 Eutraf HEALTH-F2-2010-261057
How to Distinguish Focal Atrial Tachycardia from Small Circuits and Reentry Pierre Jaïs; Bordeaux, France IHU LIRYC ANR-10-IAHU-04 Equipex MUSIC imaging platform ANR-11-EQPX-0030 Eutraf HEALTH-F2-2010-261057
Rate and Rhythm Control of Atrial Fibrillation
 Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Implantable cardioverter defibrillators for the treatment of arrhythmias and cardiac resynchronisation therapy for the treatment of heart failure (review
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Implantable cardioverter defibrillators for the treatment of arrhythmias and cardiac resynchronisation therapy for the treatment of heart failure (review
Recurrent refractory ventricular tachycardia in a patient with LVAD
 Monster Cases Recurrent refractory ventricular tachycardia in a patient with LVAD Maurizio Lunati MD Director SC Cardiologia 3 Elettrofisiologia Chairman De Gasperis Cardio Center Department ASST G.O.M.
Monster Cases Recurrent refractory ventricular tachycardia in a patient with LVAD Maurizio Lunati MD Director SC Cardiologia 3 Elettrofisiologia Chairman De Gasperis Cardio Center Department ASST G.O.M.
Ruolo della ablazione della fibrillazione atriale nello scompenso cardiaco
 Ruolo della ablazione della fibrillazione atriale nello scompenso cardiaco Matteo Anselmino Division of Cardiology Città della Salute e della Scienza Hospital University of Turin, Italy Disclosure: Honoraria
Ruolo della ablazione della fibrillazione atriale nello scompenso cardiaco Matteo Anselmino Division of Cardiology Città della Salute e della Scienza Hospital University of Turin, Italy Disclosure: Honoraria
Silvia G Priori MD PhD
 The approach to the cardiac arrest survivor Silvia G Priori MD PhD Molecular Cardiology, IRCCS Fondazione Salvatore Maugeri Pavia, Italy AND Leon Charney Division of Cardiology, Cardiovascular Genetics
The approach to the cardiac arrest survivor Silvia G Priori MD PhD Molecular Cardiology, IRCCS Fondazione Salvatore Maugeri Pavia, Italy AND Leon Charney Division of Cardiology, Cardiovascular Genetics
Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know
 Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know Steven J. Kalbfleisch, M.D. Medical Director Electrophysiology Laboratory Ross Heart Hospital Wexner Medical Center Sudden
Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know Steven J. Kalbfleisch, M.D. Medical Director Electrophysiology Laboratory Ross Heart Hospital Wexner Medical Center Sudden
Conventional Mapping. Introduction
 Conventional Mapping Haitham Badran Ain Shams University it Introduction The mapping approach used to guide ablation depends on the type of arrhythmia being assessed. Simple fluoroscopic anatomy is essential
Conventional Mapping Haitham Badran Ain Shams University it Introduction The mapping approach used to guide ablation depends on the type of arrhythmia being assessed. Simple fluoroscopic anatomy is essential
Tachy. Induction tachycardia lead ECG during Tachy /25/2009. Sinus Rhythm Single His
 12-lead ECG during Tachy 10.30.31 Sinus Rhythm Single His 11.20.02 Induction tachycardia 11.23.23 Tachy 11.25.23 1 I This finding excludes: (a) AVNRT (either typical or atypical) Tachy: Alternating cycle
12-lead ECG during Tachy 10.30.31 Sinus Rhythm Single His 11.20.02 Induction tachycardia 11.23.23 Tachy 11.25.23 1 I This finding excludes: (a) AVNRT (either typical or atypical) Tachy: Alternating cycle
Interesting EP Cases Catheter ablation to treat congestive heart failure (CHF)
") Interesting EP Cases Catheter ablation to treat congestive heart failure (CHF) Yiming WU, MD, PhD. Alaska heart and vascular institute. ywu@alaskaheart.com 907-561-3211 19 yo man transferred for out side
Interesting EP Cases Catheter ablation to treat congestive heart failure (CHF) Yiming WU, MD, PhD. Alaska heart and vascular institute. ywu@alaskaheart.com 907-561-3211 19 yo man transferred for out side
Declaration of conflict of interest
 Declaration of conflict of interest Electrical activation pattern in Left Bundle Branch Block Patients Angelo Auricchio, MD FESC Director, Cardiac Electrophysiology Programme, Fondazione Cardiocentro Ticino,
Declaration of conflict of interest Electrical activation pattern in Left Bundle Branch Block Patients Angelo Auricchio, MD FESC Director, Cardiac Electrophysiology Programme, Fondazione Cardiocentro Ticino,
The patient with (without) an ICD and heart failure: Management of electrical storm
 an ICD and heart failure: Management of electrical storm") ISHNE Heart Failure Virtual Symposium April 2008 The patient with (without) an ICD and heart failure: Management of electrical storm Westfälische Wilhelms-Universität Münster Günter Breithardt, MD, FESC,
ISHNE Heart Failure Virtual Symposium April 2008 The patient with (without) an ICD and heart failure: Management of electrical storm Westfälische Wilhelms-Universität Münster Günter Breithardt, MD, FESC,
Jean François Leclercq Department of Rythmology Private Hospital of Parly 2 - Le Chesnay F
 SECONDARY PREVENTION of Sudden Death: in which patients? Jean François Leclercq Department of Rythmology Private Hospital of Parly 2 - Le Chesnay F Why an AID is effective? Because it stoppes a VT very
SECONDARY PREVENTION of Sudden Death: in which patients? Jean François Leclercq Department of Rythmology Private Hospital of Parly 2 - Le Chesnay F Why an AID is effective? Because it stoppes a VT very
Ventricular tachycardia ablation
 Ventricular tachycardia ablation Paolo Della Bella, Corrado Carbucicchio, Nicola Trevisi Arrhythmia Department, Institute of Cardiology, University of Milan, Centro Cardiologico Monzino, Milan, Italy Key
Ventricular tachycardia ablation Paolo Della Bella, Corrado Carbucicchio, Nicola Trevisi Arrhythmia Department, Institute of Cardiology, University of Milan, Centro Cardiologico Monzino, Milan, Italy Key
Imaging and heart failure
 Imaging and heart failure Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston, St Jude, BMS imaging, GE Healthcare,
Imaging and heart failure Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston, St Jude, BMS imaging, GE Healthcare,
Cardiac Devices CRT,ICD: Who is and is not a Candidate? Who Decides
 Cardiac Devices CRT,ICD: Who is and is not a Candidate? Who Decides Colette Seifer MB(Hons) FRCP(UK) Associate Professor, University of Manitoba, Cardiologist, Cardiac Sciences Program, St Boniface Hospital
Cardiac Devices CRT,ICD: Who is and is not a Candidate? Who Decides Colette Seifer MB(Hons) FRCP(UK) Associate Professor, University of Manitoba, Cardiologist, Cardiac Sciences Program, St Boniface Hospital
Catheter Ablation of Ventricular Arrhythmias via the Radial Artery in a Patient With Prior Myocardial Infarction and Peripheral Vascular Disease
 Case Report Print ISSN 1738-5520 On-line ISSN 1738-5555 Korean Circulation Journal Catheter Ablation of Ventricular Arrhythmias via the Radial Artery in a Patient With Prior Myocardial Infarction and Peripheral
Case Report Print ISSN 1738-5520 On-line ISSN 1738-5555 Korean Circulation Journal Catheter Ablation of Ventricular Arrhythmias via the Radial Artery in a Patient With Prior Myocardial Infarction and Peripheral
Atrial Fibrillation Ablation in Patients with Heart Failure
 Atrial Fibrillation Ablation in Patients with Heart Failure Eleftherios M. Kallergis, MD, PhD, FESC Cardiology Department, Heraklion University Hospital Since auricular fibrillation so often complicates
Atrial Fibrillation Ablation in Patients with Heart Failure Eleftherios M. Kallergis, MD, PhD, FESC Cardiology Department, Heraklion University Hospital Since auricular fibrillation so often complicates
Preventing Sudden Death Current & Future Role of ICD Therapy
 Preventing Sudden Death Current & Future Role of ICD Therapy Derek V Exner, MD, MPH, FRCPC, FACC, FAHA, FHRS Professor, Libin Cardiovascular Institute of Alberta Canada Research Chair, Cardiovascular Clinical
Preventing Sudden Death Current & Future Role of ICD Therapy Derek V Exner, MD, MPH, FRCPC, FACC, FAHA, FHRS Professor, Libin Cardiovascular Institute of Alberta Canada Research Chair, Cardiovascular Clinical
Ventricular tachycardia Ventricular fibrillation and ICD
 EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
What s new in my specialty?
 What s new in my specialty? Jon Melman, MD Heart Rhythm Specialists McKay-Dee Hospital some would say some would say my specialty 1 some would say my specialty First pacemaker 1958 some would say my specialty
What s new in my specialty? Jon Melman, MD Heart Rhythm Specialists McKay-Dee Hospital some would say some would say my specialty 1 some would say my specialty First pacemaker 1958 some would say my specialty