Malignant Cerebral Infarction
|
|
|
- Opal Francis
- 6 years ago
- Views:
Transcription

1 Malignant Cerebral Infarction Dr. Ahmed Reshi Neurocritical Care Operations Director Neurocritical Care Fellowship Director University of Minnesota Dr. Christopher Streib Stroke Operations Director Stroke Fellowship Director University of Minnesota
2 Disclosures Dr. Streib is a member of the ICSI Stroke Guidelines Committee (no reimbursement) Dr. Reshi is a member of ENLS marketing committee of Neurocritical Care
3 Disclosures We have no financial relationships or other conflict of interests to disclose, and will not discuss off label use and/or investigational use in my presentation Research grants: Dr. Reshi: Local University grant for a pilot project. Ownership interest in: None No Outside consultancy role
4 Outline 1. Pathophysiology of Malignant Cerebral Infarction (MCI) 2. Treatment Options & Review of Evidence: Medical Surgical 3. Clinical Decision Making 4. Summary
5 Abbreviations mrs = modified Rankin Scale NIHSS = NIH Stroke Scale TLSW = time last seen well DC = decompressive craniectomy Early DC = DC within 48 hours of onset MCI = malignant cerebral infarction LOC = Level of Consciousness
6 Malignant Cerebral Infarction Definition: Large acute ischemic stroke, typically within the MCA territory, complicated by lifethreatening cerebral edema that may lead to brain herniation, coma, respiratory arrest, and death. Natural History of MCI: mortality rate = 80% Hacke W. et al. Malignant middle cerebral atery territory infarction: clinical course and prognostic signs. Arch Neurol Apr;53(4): PMID:
7 Definition
8 Mechanism of Injury Cerebral Edema: What kind of edema is this? Cytotoxic --- Majority Does not respond to hypertonic solution or mannitol. Vasogenic --- very small Responds to hypertonic, mannitol and steroids etc.

9 Cytotoxic Edema

10 Vasogenic Edema

11 Progression 0-24 hours: No major shift Necrotic core.


12 Progression hours: Penumbra progresses to necrosis Progressive edema Midline shift ICP elevation leading to decreased cerebral perfusion, extension of infarction


13 Progression > 72 Hours: Worsening cytotoxic edema Increase in ICP Midline shift leading to prolonged decrease LOC: intubation, aspiration PNA, DVT, etc Lethal herniation
14 Who is likely to develop MCI? Early CT suggesting > 50% of MCA territory Pineal Gland displacement Midline shift > 5mm within first 2 days > 2/3 rd involvement on CT perfusion maps. DWI lesion > 145 cubic cm. Multiple vascular territories T Occlusion of distal ICA Pre Edema Upto 24 Edema 24 on Secondary Injury 48 on
15 What we are treating? - Ischemic infarct - Associated Cerebral Edema - Cytotoxic - Not Treatable with Medical Therapy - Midline shift Decreased LOC - No Evidence that Medical Therapy is effective - Evidence to the contrary - Increased ICP secondary injury - Only thing we can treat with medical Rx. - A Bridge to definite therapy - Already too late
16 Examine the Evidence Head Elevation Schwarz S, Stroke 2002;33: More significant drop in ICP vs CPP (P.0001) No studies with improved benefit, actually recent study showed no benefit. Cooling Mortality in DC vs HT was 12 vs 47% Georgiadis D, et al,. Stroke 2002;33:1584 8
17 Medical Therapy Mannitol Bereczki D, Stroke 2003;34: patients observational study No mortality or functional benefit. Cochrane report Bereczki D, Cochrane Database Syst Rev 2007;(1) 226 pts in three randomized trials No benefit.
18 Medical Therapy Hypertonic solution No RCT No case reports or short series Schwarz S, Stroke 2002;33: ICP dropped and CPP improved. Mortality was 50% in this cohort. Glycerol Righetti E, Cochrane Database Syst Rev 2004;(2) No difference between Glycerol and control
19 Medical Therapy Barbiturates Reduce ICP Debunked in Trauma --- Cochrane Schwab S, Neurology 1997;48: Successfully Rxed ICP in MCI Mortality was 91% Corticosteroids Cochrane Review Slivka AP, Exp Neurol 2001;167: RCT s, 453 patients. No mortality/functional benefit.
20 Summary of Medical Therapy No definitive medical treatment May increase mortality Contrary to belief Increases shift Does not reduce cytotoxic edema Thus
21 NEED FOR MEDICAL THERAPY POINTS TO A FAILURE IN EARLY RECOGNITION AND TREATMENT OF MCI
22 SHOULD ONLY BE USED AS A BRIDGE TO A MORE DEFINITIVE THERAPY IF ONE IS AVAILABLE!!!!!
23 Transition May I say that the medical therapy works for what it is supposed to do i.e. Reduce ICP We should not allow ICP to rise in MCI Already too late --- secondary injury already started. If needed it is only a Bridge and not a definitive therapy.



24 Decompressive Craniectomy 1. Reversed question mark skin incision 2. Craniectomy including frontal, parietal, temporal occipital bones 3. Opening of the dura and insertion of dural patch 4. Fix dura at craniotomy margins 5. Re-approximation of temporal muscle and skin flap 6. Cranioplasty in 6-12 weeks
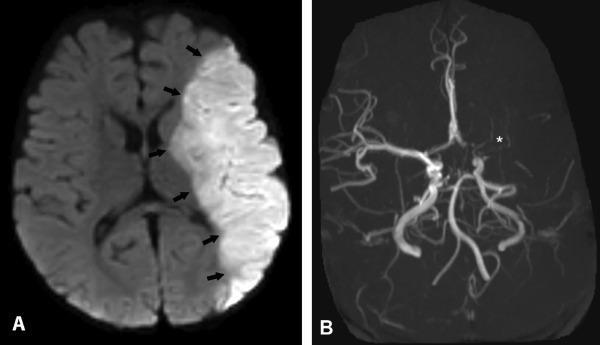
 MRI 5hrs from presentation C.) 28hr Head CT Vahedi K et al. Stroke. 2007;38:2506-2517 Copyright American Heart Association, Inc.")
25 Malignant MCA Infarct 50-year-old female enrolled in DECIMAL, randomized to medical management group. A.) Initial Head CT B.) MRI 5hrs from presentation C.) 28hr Head CT Vahedi K et al. Stroke. 2007;38: Copyright American Heart Association, Inc. All rights reserved.
 12 month MRI (mrs 3) Vahedi K et al. Stroke. 2007;38:2506-2517 Copyright American Heart Association, Inc.")
26 Malignant MCA Infarct treated with DC 22-year-old woman enrolled in DECIMAL A.) Admission MRI. B.) HCT s/p early DC C.) 12 month MRI (mrs 3) Vahedi K et al. Stroke. 2007;38: Copyright American Heart Association, Inc. All rights reserved.

27 Clinical Case 47 yo healthy male with PMHx of HTN TLSW 640PM, arrival at 940PM NIHSS 16, RMCA syndrome 10PM 10PM 11PM
28 Questions 1. Is this patient a good candidate for DC? 2. When is the optimal time to perform DC? A. Now B. Less than 48hrs C. When the patient develops signs of herniation D. Only if he progresses to coma E. This patient will likely not require DC
29 Questions 3. Does early DC increase survival? 4. Does early DC decrease morbidity? 5. What is the approximate likelihood of a favorable outcome, (mrs 0-3) with early DC? A. 0% B. 25% C. 50% D. 75%
30 AHA/ASA Guidelines Decompressive surgery for malignant edema of the cerebral hemisphere is effective and potentially lifesaving (C ass I; Leve of Evide ce B), but Advanced patient age and patient/family valuations of achievable outcome states may affect decisions regarding surgery Jauch et a. AHA/ASA Guide i es for Ma ageme t of Acute Ischemic Stroke 2013
31 Historical Context of DC for MCI s-2000s Early 2000s Present Day Dr. Emil Theodor Kocher first describes DC Advances in neuroimaging and neurocritical care make DC a realistic treatment option Clinical data suggests significant improvement in mortality with DC, long-term outcomes less devastating than expected A landmark interim pooled analysis of 3 ongoing RCTs of DC demonstrates benefit of DC in both mortality and morbidity Upon completion of the three DC RCTs, the results no longer show a benefit for favorable functional outcome DESTINY-II demonstrates decreased mortality for patients > 60 yo and improvement in acceptable functional outcomes Significant debate surrounding DC for MCI persists
32 DC Remains Controversial There is a c ear surviva be efit, but are e i creasi g surviva at the expe se of major disabi ity? 1. No individual RCT or pooled final analysis has shown benefit for excellent or favorable functional outcomes (mrs 0-3) 2. Continued poor understanding of clinical outcomes by many, including treating neurologists and neurosurgeons Impact of age, dominant hemisphere infarction, timing
33 Interim Pooled Analysis: HAMLET, DESTINY, DECIMAL (n=93) Survivors Deceased Survivors Deceased Vahedi. La cet Neuro. 2007; 6:
 Vahedi. La cet Neuro.")
34 Interim Pooled Analysis: HAMLET, DESTINY, DECIMAL (n=93) Vahedi. La cet Neuro. 2007; 6:


35 Modified Rankin Scale (mrs) Excellent: Independence preserved Favorable: non-independent, can ambulate Acceptable: cannot ambulate, not bed bound Unacceptable: Totally Dependent/Death

36 Modified Rankin Scale (mrs) Modified Rankin Scale Utility Weights mrs0 mrs1 mrs2 mrs3 mrs4 mrs5 mrs6
37 Meta-Analysis Aims 1. Is there evidence that early DC increases independent outcomes? (mrs 0-2) 2. Is there evidence that early DC increases favorable functional outcomes? (mrs 0-3) 3. Examine the impact of older age on functional outcomes 4. Create a decision algorithm

38 Meta-Analysis of 6 RCTs Streib et a. Ear y DC for Ma ig a t MCA [Meta-a a ysis]. NCP 2016.
39 Meta-Analysis Findings 1. Early DC increased excellent (i.e. independent) functional outcomes (mrs 0-2) 2. Early DC increased favorable outcomes (mrs 0-3)

40 Meta-Analysis Findings 3. Although favorable outcomes for patients > 60 yo increased, older patients had poorer overall functional recovery Streib et a. Ear y DC for Ma ig a t MCA [Meta-a a ysis]. NCP 2016.
41 Number Needed to Treat with DC Patients 60 years old DC vs Control Risk Reduction ~NNT mrs % vs 5% 11% 9 mrs % vs 22% 21% 5 mrs % vs 27% 43% 2 Mortality 21% vs 73% 52% 2
42 Number Needed to Treat with DC Patients > 60 years old DC vs Control Risk Reduction ~NNT mrs 0-2 0% vs 0% NA NA mrs 0-3 8% vs 4% 4% 25 mrs % vs 14% 30% 3 Mortality 39% vs 76% 37% 3

43 Clinical Decision Algorithm Streib et a. Ear y DC for Ma ig a t MCA [Meta-a a ysis]. NCP 2016.
44 Caveats The decision algorithm is only intended to serve as a framework to start discussions with family These results reflect DC performed proactively prior to herniation and <48 hours from TLSW Patients eligible for RCTs had no other major medical comorbidities No role for selecting dominant vs. non-dominant hemisphere patients for functional outcomes Bhatia, R., et a. (2013). "Outcome after decompressive cra iectomy i R versus L hemispheric MCI." Cerebrovascu ar Diseases 35: 114. Su dseth J, et a. Lo g-term Outcome a d Qua ity of Life after Cra iectomy i Speech-domi a t MCA i farctio. J Neuro. Critica Care 2015
45 Randomized Controlled Trials Late DC 1. HeADDFIRST: enrolled patients < 96hrs - No mortality benefit - No morbidity benefit 2. HAMLET: enrolled patients < 99hrs - No morbidity benefit (mrs 0-3 or mrs 0-4) - Mortality benefit alone
 Cerebral edema and increasing mass effect within the")

46 Malignant Cerebral Infarction Large acute ischemic stroke (MCA) Cerebral edema and increasing mass effect within the closed cranial space ICP, CBF, tissue oxygenation New ischemia/brain injury Brain Herniation Coma, Respiratory Failure, Death


47 53 year-old right MCA stroke DC deferred until exam worsened on day #5 What complication of delayed DC do you see? 40 hours Late DC (120hrs)
48 Meta-analysis: Is life worth living? 77% would give retrospective consent for DC, n=209 -responder/survivor bias -reflects clinical outcome Rahme et a. DC for Ma ig a t MCA Territory I farctio : Is ife Worth Livi g. Jour a of NSGY 2012
49 Quality of Life: 3 years after DC 23 of 25 MCI survivors at 1 year were alive 3 years after DC QOL improved from year 1 to year 3 52% lived at home 57% had symptoms of depression Mean Barthel Index: 70 (moderate dependency) Guerts et al. HAMLET at 3 years. Stroke 2013
50 Clinical Case 47 yo male with PMHx of HTN TLSW 640PM, PUH, arrival at 940PM NIHSS 16, RMCA syndrome 10PM 10PM 11PM



51 36hrs later, > 1cm midline shift Post-DC Post-cranioplasty 2 mths later Clinical Case Continued Exam stable, awake and alert MRI 5 hours, infarct volume = 166.5cc, proactively taken for DC next AM
52 10 months later Found to have Afib on Coumadin Partial seizure with generalization Keppra Deficits: minimal left-sided visual field cut, numbness of left 1 st /2 nd digit, mild changes in cognition, no weakness Returned to work full-time as forklift driver
53 Questions 1. Is this patient a good candidate for DC? 2. When is the optimal time to perform DC? A. Before herniation--less than 48hrs B. When the patient develops signs of herniation C. Only if he progresses to coma D. This patient will likely not require DC
 with early DC? A. 0% B.")
54 Questions 3. Does early DC increase survival? 4. Does early DC decrease morbidity? 5. What is the approximate likelihood of a favorable outcome, (mrs 0-3) with early DC? A. 0% B. 25% C. 50% D. 75%
55 Questions? Chris Streib: Ahmed Reshi:
Malignant Edema and Hemicraniectomy After Stroke
 Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Intensive Medical Therapy with Therapeutic Hypothermia for Malignant Middle Cerebral Artery Infarction
 Intensive Medical Therapy with Therapeutic Hypothermia for Malignant Middle Cerebral Artery Infarction Kyu sun Lee 1, Sung Eun Lee, 1 Jin Soo Lee 1, Ji Man Hong 1 1 Department of Neurology, Ajou University
Intensive Medical Therapy with Therapeutic Hypothermia for Malignant Middle Cerebral Artery Infarction Kyu sun Lee 1, Sung Eun Lee, 1 Jin Soo Lee 1, Ji Man Hong 1 1 Department of Neurology, Ajou University
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Endovascular Therapy: Beyond the Guidelines
 Endovascular Therapy: Beyond the Guidelines Ashutosh P. Jadhav, MD PhD Assistant Professor, Neurology and Neurological Surgery Center for Neuro-endovascular Therapy UPMC Stroke Institute Pittsburgh, PA
Endovascular Therapy: Beyond the Guidelines Ashutosh P. Jadhav, MD PhD Assistant Professor, Neurology and Neurological Surgery Center for Neuro-endovascular Therapy UPMC Stroke Institute Pittsburgh, PA
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
National Collaborating Centre for Chronic Conditions at the Royal College of Physicians
 13. Surgery for acute stroke 13.2 Surgical referral for decompressive hemicraniectomy Reference Gupta R, Connolly ES, Mayer S et al. Hemicraniectomy for massive middle cerebral artery territory infarction:
13. Surgery for acute stroke 13.2 Surgical referral for decompressive hemicraniectomy Reference Gupta R, Connolly ES, Mayer S et al. Hemicraniectomy for massive middle cerebral artery territory infarction:
Stroke: What did we learn in the last year?
 Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS
 CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS Early Management of Patients Considered for Hemicraniectomy Update 2015 Casaubon LK, Boulanger JM (Writing Group Chairs) on Behalf of the Stroke Hyperacute
CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS Early Management of Patients Considered for Hemicraniectomy Update 2015 Casaubon LK, Boulanger JM (Writing Group Chairs) on Behalf of the Stroke Hyperacute
Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare
 Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare Late Time Window Endovascular Trials 48.6% WITH intervention vs
Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare Late Time Window Endovascular Trials 48.6% WITH intervention vs
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
WHITE PAPER: A GUIDE TO UNDERSTANDING LARGE HEMISPHERIC INFARCTION
 WHITE PAPER: A GUIDE TO UNDERSTANDING LARGE HEMISPHERIC INFARCTION Large Hemispheric Infarction (LHI) represents a minority of strokes, yet is responsible for a disproportionately large share of stroke-related
WHITE PAPER: A GUIDE TO UNDERSTANDING LARGE HEMISPHERIC INFARCTION Large Hemispheric Infarction (LHI) represents a minority of strokes, yet is responsible for a disproportionately large share of stroke-related
Stroke Treatment Beyond Traditional Time Windows. Rishi Gupta, MD, MBA
 Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
RBWH ICU Journal Club February 2018 Adam Simpson
 RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
CT Perfusion is Essential for Stroke Triage. Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center
 CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
On Call Guide to CT Perfusion. Updated: March 2011
 On Call Guide to CT Perfusion Updated: March 2011 CT Stroke Protocol 1. Non contrast CT brain 2. CT perfusion: contrast 40cc bolus dynamic imaging at 8 slice levels ~ 60 sec creates perfusion color maps
On Call Guide to CT Perfusion Updated: March 2011 CT Stroke Protocol 1. Non contrast CT brain 2. CT perfusion: contrast 40cc bolus dynamic imaging at 8 slice levels ~ 60 sec creates perfusion color maps
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016
 Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
5/31/2018. Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment. Disclosures. Impact of clot burden
 Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Building a Stroke Portfolio. June 28, 2018
 Building a Stroke Portfolio June 28, 2018 1 Forward-Looking Statements This presentation contains forward-looking statements, including statements relating to: the potential benefits, safety and efficacy
Building a Stroke Portfolio June 28, 2018 1 Forward-Looking Statements This presentation contains forward-looking statements, including statements relating to: the potential benefits, safety and efficacy
Decompressive Hemicraniectomy in Acute Neurological Diseases
 Decompressive Hemicraniectomy in Acute Neurological Diseases Angela Crudele, MD 1 ; Syed Omar Shah, MD 1 ; Barak Bar, MD 1,2 Department of Neurology, Thomas Jefferson University, Philadelphia, PA, Department
Decompressive Hemicraniectomy in Acute Neurological Diseases Angela Crudele, MD 1 ; Syed Omar Shah, MD 1 ; Barak Bar, MD 1,2 Department of Neurology, Thomas Jefferson University, Philadelphia, PA, Department
Feeling the Pressure
 Feeling the Pressure (as in Intracranial Pressure.) Liz Kim, MSN, ACNS-BC, FAHA Advanced Practice Provider Neurocritical Care Stanford Health Care May 15, 2017 World Live Neurovascular Conference Disclosures
Feeling the Pressure (as in Intracranial Pressure.) Liz Kim, MSN, ACNS-BC, FAHA Advanced Practice Provider Neurocritical Care Stanford Health Care May 15, 2017 World Live Neurovascular Conference Disclosures
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
The DAWN of a New Era for Wake-up Stroke
 The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
framework for flow Objectives Acute Stroke Treatment Collaterals in Acute Ischemic Stroke framework & basis for flow
 Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Broadening the Stroke Window in Light of the DAWN Trial
 Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
Byung Rhae Yoo, Chan Jong Yoo, Myeong Jin Kim, Woo-Kyung Kim, Dae Han Choi
 Journal of Cerebrovascular and Endovascular Neurosurgery pissn 2234-8565, eissn 2287-3139, http://dx.doi.org/10.7461/jcen.2016.18.3.175 Original Article Analysis of the Outcome and Prognostic Factors of
Journal of Cerebrovascular and Endovascular Neurosurgery pissn 2234-8565, eissn 2287-3139, http://dx.doi.org/10.7461/jcen.2016.18.3.175 Original Article Analysis of the Outcome and Prognostic Factors of
WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer
 WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer Dr. Jim Kyle, FACSM, FAAFP Regional Medical Director WVOEMS Executive Director, The Kyle Group
WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer Dr. Jim Kyle, FACSM, FAAFP Regional Medical Director WVOEMS Executive Director, The Kyle Group
7/22/2016. Navaz Karanjia, MD. FINANCIAL DISCLOSURE: none. UNLABELED/UNAPPROVED USE DISCLOSURE: none
 Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Interventional Treatment of Stroke
 Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Ongoing Acute Stroke Studies 10/5/2015
 Ongoing Acute Stroke Studies 10/5/2015 Wade S. Smith, MD, PhD Director UCSF Neurovascular Service Daryl R. Gress Professor of Neurocritical Care and Stroke Disclosures NIH U10 NS 086494 (PI) NorCal RCC
Ongoing Acute Stroke Studies 10/5/2015 Wade S. Smith, MD, PhD Director UCSF Neurovascular Service Daryl R. Gress Professor of Neurocritical Care and Stroke Disclosures NIH U10 NS 086494 (PI) NorCal RCC
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Disclosure. + Outline. What is a stroke? Role of imaging in stroke Ischemic stroke Venous infarct Current topics
 + Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 + Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Thank you
+ Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 + Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Thank you
Case Series. Abstract. Introduction. Patients and Methods
 Case Series Salvage decompressive craniectomy in malignant MCA infarcts results of local experience at Shifa International Hospital, Islamabad, Pakistan Ismail A. Khatri, Maimoona Siddiqui, Inayatullah
Case Series Salvage decompressive craniectomy in malignant MCA infarcts results of local experience at Shifa International Hospital, Islamabad, Pakistan Ismail A. Khatri, Maimoona Siddiqui, Inayatullah
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
12/4/2017. Disclosure. Educational Objectives. Has been consultant for Bard, Chiesi
 Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Advanced Neuroimaging for Acute Stroke
 Advanced Neuroimaging for Acute Stroke E. Bradshaw Bunney, MD, FACEP Professor Department Of Emergency Medicine University of Illinois at Chicago Swedish American Belvidere Hospital Disclosures FERNE Board
Advanced Neuroimaging for Acute Stroke E. Bradshaw Bunney, MD, FACEP Professor Department Of Emergency Medicine University of Illinois at Chicago Swedish American Belvidere Hospital Disclosures FERNE Board
12/4/2017. Disclosures. Study organization. Stryker Medtronic Penumbra Viz Route 92. Data safety monitoring board Tudor G.
 12/4/2017 Update on Stroke Trials:Extending the Window DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo NP001713
12/4/2017 Update on Stroke Trials:Extending the Window DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo NP001713
Endovascular Treatment of Ischemic Stroke
 Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Decompressive Surgery for the Treatment of Malignant Infarction of the Middle Cerebral Artery (DESTINY) A Randomized, Controlled Trial
 A Randomized, Controlled Trial") Decompressive Surgery for the Treatment of Malignant Infarction of the Middle Cerebral Artery (DESTINY) A Randomized, Controlled Trial Eric Jüttler, MD; Stefan Schwab, MD, PhD; Peter Schmiedek, MD, PhD;
Decompressive Surgery for the Treatment of Malignant Infarction of the Middle Cerebral Artery (DESTINY) A Randomized, Controlled Trial Eric Jüttler, MD; Stefan Schwab, MD, PhD; Peter Schmiedek, MD, PhD;
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Changing Demographics in Death After Devastating Brain Injury
 Changing Demographics in Death After Devastating Brain Injury Andreas H. Kramer MD MSc FRCPC Departments of Critical Care Medicine & Clinical Neurosciences Foothills Medical Center, University of Calgary
Changing Demographics in Death After Devastating Brain Injury Andreas H. Kramer MD MSc FRCPC Departments of Critical Care Medicine & Clinical Neurosciences Foothills Medical Center, University of Calgary
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
Mechanical thrombectomy beyond the 6 hours. Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital
 Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke
 Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Update sulle lesioni emorragiche posttraumatiche
 Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
Significant Relationships
 Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
ACUTE STROKE IMAGING
 ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Large ischemic strokes presenting as malignant cerebral
 Neurosurg Focus 30 (6):E18, 2011 Decompressive hemicraniectomy after malignant middle cerebral artery infarction: rationale and controversies Omar M. Arnaout, M.D., Salah G. Aoun, M.D., H. Hunt Batjer,
Neurosurg Focus 30 (6):E18, 2011 Decompressive hemicraniectomy after malignant middle cerebral artery infarction: rationale and controversies Omar M. Arnaout, M.D., Salah G. Aoun, M.D., H. Hunt Batjer,
Chapter 8. HAMLET protocol
 HAMLET protocol Chapter 8 Hemicraniectomy After Middle cerebral artery infarction with Life-threatening Edema Trial (HAMLET). Protocol of a randomized controlled trial of decompressive surgery in space-occupying
HAMLET protocol Chapter 8 Hemicraniectomy After Middle cerebral artery infarction with Life-threatening Edema Trial (HAMLET). Protocol of a randomized controlled trial of decompressive surgery in space-occupying
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Decompressive Hemicraniectomy for Malignant Middle Cerebral Artery Infarct
 DOI: 10.5137/1019-5149.JTN.13241-14.1 Received: 27.10.2014 / Accepted: 08.01.2015 Published Online: 24.02.2016 Original Investigation Decompressive Hemicraniectomy for Malignant Middle Cerebral Artery
DOI: 10.5137/1019-5149.JTN.13241-14.1 Received: 27.10.2014 / Accepted: 08.01.2015 Published Online: 24.02.2016 Original Investigation Decompressive Hemicraniectomy for Malignant Middle Cerebral Artery
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand
 Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
9/18/16. Management of Ischemic Stroke in the Intensive Care Unit. Outline. Introduction. Kyle B Walsh MD. Phases of Stroke Diagnosis and Treatment
 Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
Acute Stroke Care: the Nuts and Bolts of it. ECASS I and II ATLANTIS. Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center
 Acute Stroke Care: the Nuts and Bolts of it Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center ECASS I and II tpa for patients presenting
Acute Stroke Care: the Nuts and Bolts of it Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center ECASS I and II tpa for patients presenting
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
Spontaneous Recanalization after Complete Occlusion of the Common Carotid Artery with Subsequent Embolic Ischemic Stroke
 Original Contribution Spontaneous Recanalization after Complete Occlusion of the Common Carotid Artery with Subsequent Embolic Ischemic Stroke Abstract Introduction: Acute carotid artery occlusion carries
Original Contribution Spontaneous Recanalization after Complete Occlusion of the Common Carotid Artery with Subsequent Embolic Ischemic Stroke Abstract Introduction: Acute carotid artery occlusion carries
ELVO update. Michael Wilder, MD Director, Neurointerventional Program PeaceHealth Sacred Heart Springfield, Oregon
 ELVO update Michael Wilder, MD Director, Neurointerventional Program PeaceHealth Sacred Heart Springfield, Oregon Riverbend 24/7 thrombectomy ELVO alert Access PH PACU Anesthesia Goyal et al. Lancet. 2016
ELVO update Michael Wilder, MD Director, Neurointerventional Program PeaceHealth Sacred Heart Springfield, Oregon Riverbend 24/7 thrombectomy ELVO alert Access PH PACU Anesthesia Goyal et al. Lancet. 2016
THE EFFICACY OF DECOMPRESSIVE CRANIECTOMY IN TREATMENT OF PATIENTS WITH MASSIVE HEMISPHERIC CEREBRAL INFARCTION
 Medical Journal of the Islamic Republic of Iran A. Ebrahiminejad, et al. Volume 18 Number 1 Spring 1383 May 2004 THE EFFICACY OF DECOMPRESSIVE CRANIECTOMY IN TREATMENT OF PATIENTS WITH MASSIVE HEMISPHERIC
Medical Journal of the Islamic Republic of Iran A. Ebrahiminejad, et al. Volume 18 Number 1 Spring 1383 May 2004 THE EFFICACY OF DECOMPRESSIVE CRANIECTOMY IN TREATMENT OF PATIENTS WITH MASSIVE HEMISPHERIC
DISCLOSURES OBJECTIVES 11/18/2014. Stroke Network Update. None. Discuss
 Stroke Network Update MOUHAMMAD A. JUMAA MD ASSISTANT PROFESSOR VASCULAR & INTERVENTIONAL NEUROLOGY UNIVERSITY OF TOLEDO DISCLOSURES None OBJECTIVES Discuss Regional stroke systems of care in NW OHIO Evolution
Stroke Network Update MOUHAMMAD A. JUMAA MD ASSISTANT PROFESSOR VASCULAR & INTERVENTIONAL NEUROLOGY UNIVERSITY OF TOLEDO DISCLOSURES None OBJECTIVES Discuss Regional stroke systems of care in NW OHIO Evolution
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
AMSER Case of the Month: March 2019
 AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew
AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew
Acute Stroke Treatment KPNC Stroke EXPRESS
 Acute Stroke Treatment 2018 KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke 1 Jeffrey G. Klingman, MD The Permanente Medical Group Stroke Treatment in the old days Prior to 1996:
Acute Stroke Treatment 2018 KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke 1 Jeffrey G. Klingman, MD The Permanente Medical Group Stroke Treatment in the old days Prior to 1996:
9/16/2018. Recognizing & Managing Seizures in Pediatric TBI. Objectives. Definitions and Epidemiology
 Recognizing & Managing Seizures in Pediatric TBI UW Medicine EMS & Trauma 2018 Conference September 17 and 18, 2018 Mark Wainwright MD PhD Herman and Faye Sarkowsky Professor of Neurology Division Head,
Recognizing & Managing Seizures in Pediatric TBI UW Medicine EMS & Trauma 2018 Conference September 17 and 18, 2018 Mark Wainwright MD PhD Herman and Faye Sarkowsky Professor of Neurology Division Head,
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015
 UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Outcome and Prognostic Factors of Decompressive Hemicraniectomy in Malignant Middle Cerebral Artery Infarction
 ORIGINAL ARTICLE Outcome and Prognostic Factors of Decompressive Hemicraniectomy in Malignant Middle Cerebral Artery Infarction Chun-Chung Chen, Der-Yang Cho*, Shu-Chiu Tsai Department of Neurosurgery,
ORIGINAL ARTICLE Outcome and Prognostic Factors of Decompressive Hemicraniectomy in Malignant Middle Cerebral Artery Infarction Chun-Chung Chen, Der-Yang Cho*, Shu-Chiu Tsai Department of Neurosurgery,
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO
 TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN
 Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN Background 30% of patients have history of hypertension prior to stroke 80% will present with
Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN Background 30% of patients have history of hypertension prior to stroke 80% will present with
Do Prognostic Models Matter in Neurocritical Care?
 Do Prognostic Models Matter in Neurocritical Care? Alexis F. Turgeon MD MSc FRCPC Associate Professor and Director of Research Department of Anesthesiology and Critical Care Medicine Division of Critical
Do Prognostic Models Matter in Neurocritical Care? Alexis F. Turgeon MD MSc FRCPC Associate Professor and Director of Research Department of Anesthesiology and Critical Care Medicine Division of Critical
Surgical Management of an Unusual Case of Malignant Middle Cerebral Artery Infarction
 Elmer Press Case Report Surgical Management of an Unusual Case of Malignant Middle Cerebral Artery Infarction Jon Durrani a, c, Mohammed Rahman b, Phillip Porcelli a, Keith Kattner a Abstract Decompressive
Elmer Press Case Report Surgical Management of an Unusual Case of Malignant Middle Cerebral Artery Infarction Jon Durrani a, c, Mohammed Rahman b, Phillip Porcelli a, Keith Kattner a Abstract Decompressive
ACUTE STROKE MANAGEMENT
 ACUTE STROKE MANAGEMENT. Before the Specialist Arrives C A R L O S L C H U A, M D, F P N A UP- P H I L I P P I N E G E N E R A L H O S P I T A L P R E S I D E N T, S T R O K E S O C I E T Y O F T H E P
ACUTE STROKE MANAGEMENT. Before the Specialist Arrives C A R L O S L C H U A, M D, F P N A UP- P H I L I P P I N E G E N E R A L H O S P I T A L P R E S I D E N T, S T R O K E S O C I E T Y O F T H E P
Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Hemicraniectomy and Durotomy Upon Deterioration From Infarction-Related Swelling Trial Randomized Pilot Clinical Trial
 Hemicraniectomy and Durotomy Upon Deterioration From Infarction-Related Swelling Trial Randomized Pilot Clinical Trial Jeffrey I. Frank, MD; L. Philip Schumm, MA; Kristen Wroblewski, MS; Douglas Chyatte,
Hemicraniectomy and Durotomy Upon Deterioration From Infarction-Related Swelling Trial Randomized Pilot Clinical Trial Jeffrey I. Frank, MD; L. Philip Schumm, MA; Kristen Wroblewski, MS; Douglas Chyatte,
Acute Ischemic Stroke Imaging. Ronald L. Wolf, MD, PhD Associate Professor of Radiology
 Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Update on Early Acute Ischemic Stroke Interventions
 Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Acute Stroke Rescue and Recovery
 Acute Stroke Rescue and Recovery Qaisar A. Shah, MD Director, Neurointerventional and Neurocritical care Nancy Arena Gogal,, RN Manager Cath/EPS/Neuro lab AMH Stroke Program Evolution 1997: Stroke Program
Acute Stroke Rescue and Recovery Qaisar A. Shah, MD Director, Neurointerventional and Neurocritical care Nancy Arena Gogal,, RN Manager Cath/EPS/Neuro lab AMH Stroke Program Evolution 1997: Stroke Program
Disclosures. Anesthesia for Endovascular Treatment of Acute Ischemic Stroke. Acute Ischemic Stroke. Acute Stroke = Medical Emergency!
 Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
occlusions. Cerebral perfusion is driven fundamentally by regional cerebral
 Appendix Figures Figure A1. Hemodynamic changes that may occur in major anterior circulation occlusions. Cerebral perfusion is driven fundamentally by regional cerebral perfusion pressure (CPP). In response
Appendix Figures Figure A1. Hemodynamic changes that may occur in major anterior circulation occlusions. Cerebral perfusion is driven fundamentally by regional cerebral perfusion pressure (CPP). In response
Perioperative Management of Traumatic Brain Injury. C. Werner
 Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion
 Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion Aman B. Patel, MD Robert & Jean Ojemann Associate Professor Director, Cerebrovascular Surgery Director, Neuroendovascular
Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion Aman B. Patel, MD Robert & Jean Ojemann Associate Professor Director, Cerebrovascular Surgery Director, Neuroendovascular
Advanced Stroke Care in the context of the Cardiovascular Patient
 EASTERN MAINE MEDICAL CENTER Advanced Stroke Care in the context of the Cardiovascular Patient Advancing Science in Cardiovascular Care Samoset Conference NOV 8, 2018 Dr. Gillian Gordon Perue Conflict
EASTERN MAINE MEDICAL CENTER Advanced Stroke Care in the context of the Cardiovascular Patient Advancing Science in Cardiovascular Care Samoset Conference NOV 8, 2018 Dr. Gillian Gordon Perue Conflict
Interventional therapies in stroke management: anaesthetic and critical care implications
 BJA Education, 17 (2): 43 47 (2017) doi: 10.1093/bjaed/mkw039 Advance Access Publication Date: 24 May 2016 Matrix reference 2A12, 3F00 Interventional therapies in stroke management: anaesthetic and critical
BJA Education, 17 (2): 43 47 (2017) doi: 10.1093/bjaed/mkw039 Advance Access Publication Date: 24 May 2016 Matrix reference 2A12, 3F00 Interventional therapies in stroke management: anaesthetic and critical