Noonan Syndrome and twin to twin transfusion
|
|
|
- Harvey Stewart
- 6 years ago
- Views:
Transcription
1 Università degli Studi La Sapienza - Facoltà di Medicina e Chirurgia Roma Master di Terapia Intensiva Pediatrica Direttore Prof. Corrado Moretti Noonan Syndrome and twin to twin transfusion Neonatal outcome in extremely low birth weight premature with severe hypertrophic cardiomyopathy and right ventricular outflow tract obstruction Anno accademico Relatore Dott. Antonino Cutaia
 of monochorionic twin pregnancies 1/4.")
2 Incidence twin to twin transfusion syndrome Twin gestation: 1-2% of all pregnancy Monozygotic twin: 1/3 of all twin pregnancy Monochorionic twin:2/3 of all monozygotic twin TTTS: up to 17,5% (5,5 17,5%) of monochorionic twin pregnancies 1/4.000 pregnancies

3 Type The number, size and type of vascular anastomoses play important roles in the etiologies of various forms of TTTS Chronic TTTS Acute perimortem TTTS Twin anemia polycythemia sequence Acute perinatal TTS Twin reversed arterial perfusion sequence
4 Chronic TTTS Most common form Clinically apparent during the second or early third trimester of pregnancy PROM preterm labor Recipient twin: rapid development of polyhydramnios (hypervolemia >>> polyuria) circulatory volume overload, fetal hydrops Donor twin: severe oligohydramnios (hypovolemia >>> oliguria) stuck twin, fetal hydrops

5 Pathogenesis of chronic TTTS new hypothesis Fetal RAS is reported to be upregulated in donor twins d/t hypovolemia and decreased renal perfusion Transfer of rennin and angiotensin through the vascular anastomoses from the donor into the hypervolemic recipient might increase the BP and aggravate cardiac dysfunction in the recipient

6 Diagnosis Inter twin birth weight discordance >20% Hb difference > 5g/dl
7 Neonatal morbidity Cardiovascular Renal Hematologic GI Neurology Others Donor Renal cortical necrosis/fibrosis Transient renal insufficiency Hematuria Acute renal failure Permanent tubular dysfunction d/t renal tubular dysgenesis Severe anemia - fetal hidrops NEC, intestinal atresia Equally at risk for cerebral injury (HIE, PVL, IVH..) Amniotic band syndrome Recipient Congenital heart disease Neonatal hypertension Hypertrophic cardiomyopathy RVOTO > > > fetal hydrops Cardiac hypertrophy polycythemia idem idem Lower limb necrosis
8 Cardiovascular morbidity 3.8% vs singleton 0.6% Mainly in recipient 1 theory: consequence of increased preload d/t chronic hypervolemia causing cardiac hypertrophy 2 theory: increased afterload induced by elevated levels of vasoconstrictive substances such as endothelin-1 found in recipients Congenital heart disease 12 times more frequent in TTTS than in the general population, mainly found in recipient twins. PPHN, TR, left chamber myocardial infarction, pulmonary artery calcification, RVOTO
9 Cardiovascular morbidity Biventricular hypertrophy with prevalent left ventricular hypertrophic cardiomyopathy may be present in % of the recipient twins. Fetal hypertrophic cardiomyopathy >>> hydrops fetalis Reversible in most cases after delivery. d/t removal of causal factors Cardiac hypertrophy >>>functional RVOTO (4-11%) may be progressive, require urgent treatment
10 Must be aware of the risk of RVOTO in recipient twins!!!
11 Neonatal Hypertrophic Cardiomyopathy Familial Idiopathic Hypertrophic Maternal disease Diabetes Myocarditis Infectious endotoxins Drugs /Iatrogenic Dexamathasone (BPD) ECMO Malformation syndromes Beckwith Wiedemann Noonan (case report) Leopard Downs Myocyte hypertrophy & disarray Increased mass & thickness Increased mass/volume ratio Poor diastolic chamber compliance Left ventricle High systolic pressure gradient

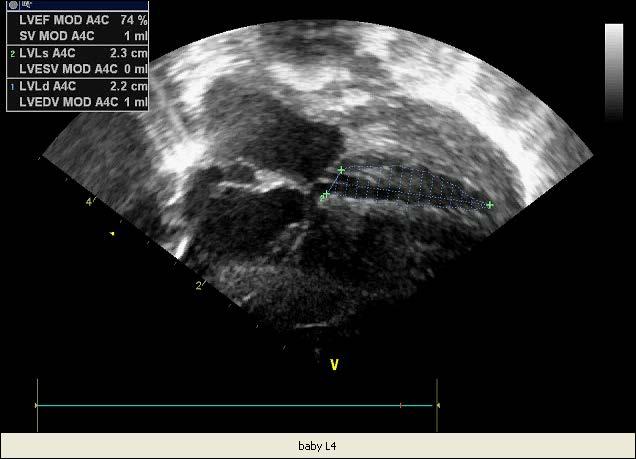
12 Case study Baby L is a 830-g female 1 born, delivered by emergency cesarean section at 27 weeks gestation following an uncomplicated monochorionic twin pregnancy until late in labor, when fetal heart rate decelerations were noted secondary to abruptio placentae. 2 born is a 600-g female, fetal demise ongoing the labor Weight discordance : 230-g 230 : 830 = x : 100 (28%) Parents no consanguineous (mother 43 y. o. gravida para 3, father 45 y.o.) and the other two children were reported to be heathy The week before a fetal echocardiography reported no problems
13 Initial evaluation Apgar scores were 1 at 1 minute and 6 at 5 minutes Phisical examination revealed a weak respiratory effort, therefore, positive pressure ventilation with 60% oxigen was given for approximately 15 seconds, followed by endotracheal intubation delivering sufficient positive pressure ventilation to barely move the infant s chest, because even brief periods of overdistension can cause lung injury and attenuate the benefits of surfactant replacement therapy. Cardiovascular examination was unremarkable
 rate of 40, and an inspired oxigen concentration (FiO2) of 0,40-0,60.")
14 Following care Was transferred to a maximally humidified incubator Placed on a ventilator with an inspiratory pressure (IP) of 18 cm H2O, a positive end-espiratory pressure (PEEP) of 5 cm H2O, a synchronized intermittent mandatory ventilation (SINV) rate of 40, and an inspired oxigen concentration (FiO2) of 0,40-0,60. Surfactant was given UVC was placed The initial blood work demonstrated only high hemoglobin (20mg/dl) and creatinine (1,7 mg/dl) and low calcium (6 mg/dl) Head and abdomen ultrasonography were unremarkable

15 On day 2 Baby L responded poorly to respiratory therapy Despite no heart murmur was heard, a patent ductus arteriosus (PDA) with left-to-right shunting was suspected and then confirmed by color Doppler echocardiography. Since then, evidence of severe biventricular hypertrophy, but no obstruction yet in right and left ventricular outflow tracts A course of ibuprophen was administered, with resolution of the PDA
16 After PDA closure Baby L continued to improve, but she was unable to be estubated because of poor chest wall stability and apnea that was responsive to caffeine therapy Intravenous infusion of catecholamines resulted in a dramatic improvement in peripheral perfusion, acidbase balance, and urine output Dopamine 5 μg/kg/min - Dobutamine 5 μg/kg/min On day 5 ncpap 5 cm H2O FiO2 0.60
17 On day 7 Nadir weight loss Small amounts of breast milk were started On examination, she had a grade 3/6 systolic heart murmur heard best over the left upper chest, and generalized edema most marked in the face, hands, and feet. Echocardiogram indicated : worsenig bi-ventricular hypertrophy Inter Ventricular Septum IVS thickness: 5 mm (> 97 cent.) Left Ventricular Posterior Wall thickness: 8.5 mm (> 97 Cent.) and moderate pulmonic valvular stenosis
18 On day 15 Recovered birth weight At that time the infant was on ncpap and 40% oxigen During feeding or crying events she continued to have 10 to 15 second apnea episodes, accompanied by decrease in heart rate to 70 beats per minute. Echocardiogram showed: Dysplastic pulmonary valve with systolic doming Severe Right ventricular outflow tract obstruction showing increased flow velocity with a predicted maximum instantaneous gradient of approximately 75 mm Hg D/T dynanic compression of hypertrophieed muscle bundles. SIV deviated toward the left ventricle indicative of suprasystemic right ventricular systolic pressure.
19 Devo aggiungere videoclip Continuous wave Doppler demonstrated a double envelope caused by two velocities; the first is flow across the pulmonary valve and the second represents increased velocity across the subvalvar obstruction.
20 Rule out genetic causes of cardiomyopathy I step Expanded metabolic screening negative II step Chromosomal assessment Normal female chromosomal constitution (46,xx)

21
22 Rule out genetic causes of cardiomyopathy If negative Noonan test IV step Evaluation of mutations in one of a number of genes that encode for one of the sarcomere proteines
23 On day 30 Despite aggressive medical support (dopamine, dobutamine, intravascular volume expansion, sodium bicarbonate) Baby L has gradually developed an increased need for respiratory support, with an oxigen requirement up to 75% Failure to thrive Laboratory studies ruled out infections The chest and abdomen examinations, as well as other exams were unremarkable But
24 A new echocardiogram showed Critical Right ventricular outflow tract obstruction conditioning increased flow velocity with a predicted maximum instantaneous gradient of approximately 135 mm Hg D/T dynanic compression of hypertrophieed muscle bundles. AND Moderate Left ventricular outflow tract obstruction conditioning increased flow velocity with a predicted maximum instantaneous gradient of approximately 55 mm Hg and mitral valve Systolic Anterior Motion (SAM) Therefore
25 Milestone switch-therapy No more Dopa/Dobu Start β-blockers Propanolol 1 mg/kg/die
26 Over the next several days Baby L demonstrated improved activity and vital signs stabilized was weaned from supplemental oxigen was feeding well and had a normal physical examination, except for mild jaundice Sensible improvement to thrive To support tissue oxigenation were infused packed RBCs to keep, as more as possible, a 45% Ht A 21-day tapering course of dexamethasone was instituted
27 Our target is: to gain weight until 1800-g This is the right weight, to performe confidently the pulmonary valvuloplasty by our referral baby heart team of CCPM in Taormina Hospital How small is too small a baby to be operated is their institutional choice
28 On day 84 Baby L was taken to the cath-lab where a pulmonary valvuloplasty was performed Partial success of procedure pulling down trans-valvular gradient from 135 to 40 mmhg but in the next few days increase of gradient to 100 mmhg Therefore it was planned a surgical procedure to relieve right ventricular outflow tract obstruction
29 A week later Enlargement of right ventricular outflow tract by a trans-annulapatch Post-procedure gradient became 40 mmhg, enough, at the moment, to hope a better future for our Baby L
30 On day 105 Baby L was discharged clinically well and thriving (2500-g), without dyspnea or noticeable cardiovascular symptoms, with this supportive Therapy: Reduce afterload Improve cardiac ejection Reduce catecholamine drive prolonging cardiac survival Relieve cholestasis D/T TPN Careful titration necessary ACE inhibitors : Captopril 2 mg per dose PO /Q8 β-blockers : Propanolol 0,5 mg per dose PO /Q8 Diuretics : Furosemide 2 mg per dose PO /Q24 Dihydroxy bile acid : Ursodeoxycholic acid 2 mg per dose PO /Q8
31 The prognosis for Baby L is not good, depending, once its cause is removed, on the desirable regression of her hypertrophic myocardiopathy Approximately a third of these children die during the first 2 years of life, and those that survive need : Implantable defibrillators Hemi-Konno procedure The narrow left ventricular outlet is approached through the right ventricle, the septum is cut open, and filled with a large patch in such a way as to enlarge the LV outflow If failure >>> Cardiac transplant

32

33

34
35
36 Devo aggiungere i video clips
Congenital heart disease in twin-to-twin transfusion syndrome treated with fetoscopic laser surgery
 Chapter 10 Congenital heart disease in twin-to-twin transfusion syndrome treated with fetoscopic laser surgery Enrico Lopriore MD Regina Bökenkamp MD Marry Rijlaarsdam MD Marieke Sueters MD Frank PHA Vandenbussche
Chapter 10 Congenital heart disease in twin-to-twin transfusion syndrome treated with fetoscopic laser surgery Enrico Lopriore MD Regina Bökenkamp MD Marry Rijlaarsdam MD Marieke Sueters MD Frank PHA Vandenbussche
Case Report Right Ventricular Outflow Tract Obstruction in Monochorionic Twins with Selective Intrauterine Growth Restriction
 Case Reports in Pediatrics Volume 2012, Article ID 426825, 4 pages doi:10.1155/2012/426825 Case Report Right Ventricular Outflow Tract Obstruction in Monochorionic Twins with Selective Intrauterine Growth
Case Reports in Pediatrics Volume 2012, Article ID 426825, 4 pages doi:10.1155/2012/426825 Case Report Right Ventricular Outflow Tract Obstruction in Monochorionic Twins with Selective Intrauterine Growth
FETAL ECHO IN TWIN PREGNACY: MONOCHORIONIC TWINS DELHI CHILD HEART CENTER & INDRAPRASTHA APOLLO HOSPITAL NEW DELHI
 FETAL ECHO IN TWIN PREGNACY: MONOCHORIONIC TWINS DELHI CHILD HEART CENTER & INDRAPRASTHA APOLLO HOSPITAL NEW DELHI Scope of this talk Twin to Twin Transfusion TRAP Sequence Congenital Heart Defects in
FETAL ECHO IN TWIN PREGNACY: MONOCHORIONIC TWINS DELHI CHILD HEART CENTER & INDRAPRASTHA APOLLO HOSPITAL NEW DELHI Scope of this talk Twin to Twin Transfusion TRAP Sequence Congenital Heart Defects in
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
HISTORY. Question: What category of heart disease is suggested by the fact that a murmur was heard at birth?
 HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
4/19/2018. St. Cloud Hospital Perinatology Kristin Olson, RDMS, RVT
 St. Cloud Hospital Perinatology Kristin Olson, RDMS, RVT Review Fetal Circulation Provide Indications for Umbilical Artery, Middle Cerebral Artery, and Ductus Venosus Doppler studies. Demonstrate normal
St. Cloud Hospital Perinatology Kristin Olson, RDMS, RVT Review Fetal Circulation Provide Indications for Umbilical Artery, Middle Cerebral Artery, and Ductus Venosus Doppler studies. Demonstrate normal
Peripartum Cardiomyopathy. Lavanya Rai Manipal
 Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
2) VSD & PDA - Dr. Aso
 VSD & PDA - Dr. Aso") 2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
Failing right ventricle
 Failing right ventricle U. Herberg 1, U. Gembruch 2 1 Pediatric Cardiology, 2 Prenatal Diagnostics and Fetal Therapy, University of Bonn, Germany Prenatal Physiology Right ventricle dominant ventricle
Failing right ventricle U. Herberg 1, U. Gembruch 2 1 Pediatric Cardiology, 2 Prenatal Diagnostics and Fetal Therapy, University of Bonn, Germany Prenatal Physiology Right ventricle dominant ventricle
Medical Complications of Pregnancy
 Medical Complications of Pregnancy Systems Cardiovascular Pulmonary Endocrine Gastrointestinal Urologic Neurologic Cardiovascular System Physiologic anemia 3:1 increase of plasma volume:rbc mass Treat
Medical Complications of Pregnancy Systems Cardiovascular Pulmonary Endocrine Gastrointestinal Urologic Neurologic Cardiovascular System Physiologic anemia 3:1 increase of plasma volume:rbc mass Treat
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Systematic approach to Fetal Echocardiography. Objectives. Introduction 11/2/2015
 Systematic approach to Fetal Echocardiography. Pediatric Echocardiography Conference, JCMCH November 7, 2015 Rajani Anand Objectives Fetal cardiology pre-test Introduction Embryology and Physiology of
Systematic approach to Fetal Echocardiography. Pediatric Echocardiography Conference, JCMCH November 7, 2015 Rajani Anand Objectives Fetal cardiology pre-test Introduction Embryology and Physiology of
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Hyaline membrane disease. By : Dr. Ch Sarishma Peadiatric Pg
 Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Physiologic Based Management of Circulatory Shock Kuwait 2018
 Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating)
") Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating) Table 1: Appropriate indications (median score 7-9) Indication
Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating) Table 1: Appropriate indications (median score 7-9) Indication
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
PATENT DUCTUS ARTERIOSUS (PDA)
") PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
Topic Page: congestive heart failure
 Topic Page: congestive heart failure Definition: congestive heart f ailure from Merriam-Webster's Collegiate(R) Dictionary (1930) : heart failure in which the heart is unable to maintain an adequate circulation
Topic Page: congestive heart failure Definition: congestive heart f ailure from Merriam-Webster's Collegiate(R) Dictionary (1930) : heart failure in which the heart is unable to maintain an adequate circulation
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM. General Instructions: ID NUMBER: FORM NAME: H F A DATE: 10/13/2017 VERSION: CONTACT YEAR NUMBER:
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction to Fetal Medicine. Lloyd R. Feit M.D. Associate Professor of Pediatrics Warren Alpert Medical School Brown University
 Associate Professor of Pediatrics Warren Alpert Medical School Brown University Fetal Cardiology Important in evaluation of high risk pregnancies. Information obtainable in > 95% of patients attempted.
Associate Professor of Pediatrics Warren Alpert Medical School Brown University Fetal Cardiology Important in evaluation of high risk pregnancies. Information obtainable in > 95% of patients attempted.
Pathophysiology: Heart Failure
 Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
INTRAVENOUS FLUID THERAPY
 INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
Outline. Pathophysiology: Heart Failure. Heart Failure. Heart Failure: Definitions. Etiologies. Etiologies
 Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Maternal and Fetal Physiology
 Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS Pediatric Cardiology
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Cor pulmonale. Dr hamid reza javadi
 1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
SESSION D5. The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
 37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION D5 Session Description: The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION D5 Session Description: The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Valve Disease in the Pregnant Patient
 Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
INTRAVENOUS FLUIDS PRINCIPLES
 INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
Absent Pulmonary Valve Syndrome
 Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009
 www.ivis.org Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009 São Paulo, Brazil - 2009 Next WSAVA Congress : Reprinted in IVIS with the permission of the Congress Organizers MANAGEMENT
www.ivis.org Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009 São Paulo, Brazil - 2009 Next WSAVA Congress : Reprinted in IVIS with the permission of the Congress Organizers MANAGEMENT
Valutazione del neonato con sospetta ipertensione polmonare
 Valutazione del neonato con sospetta ipertensione polmonare Cardiologia Pediatrica Seconda Università degli Studi di Napoli A.O. R.N. dei Colli-Monaldi Napoli Hypoxiemic infant Full or near-term neonate
Valutazione del neonato con sospetta ipertensione polmonare Cardiologia Pediatrica Seconda Università degli Studi di Napoli A.O. R.N. dei Colli-Monaldi Napoli Hypoxiemic infant Full or near-term neonate
Treatment of Hypertrophic Cardiomyopathy in Bruce B. Reid, MD
 Treatment of Hypertrophic Cardiomyopathy in 2017 Bruce B. Reid, MD Disclosures I have no conflicts of interest to disclose I will not be discussing any off label medications and/or devices Objectives 1)
Treatment of Hypertrophic Cardiomyopathy in 2017 Bruce B. Reid, MD Disclosures I have no conflicts of interest to disclose I will not be discussing any off label medications and/or devices Objectives 1)
How to Recognize a Suspected Cardiac Defect in the Neonate
 Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
HEART CONDITIONS IN SPORT
 HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
State of Florida Systemic Supportive Care Guidelines. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
SWISS SOCIETY OF NEONATOLOGY. Prenatal closure of the ductus arteriosus
 SWISS SOCIETY OF NEONATOLOGY Prenatal closure of the ductus arteriosus March 2007 Leone A, Fasnacht M, Beinder E, Arlettaz R, Neonatal Intensive Care Unit (LA, AR), University Hospital Zurich, Cardiology
SWISS SOCIETY OF NEONATOLOGY Prenatal closure of the ductus arteriosus March 2007 Leone A, Fasnacht M, Beinder E, Arlettaz R, Neonatal Intensive Care Unit (LA, AR), University Hospital Zurich, Cardiology
Stabilization and Transportation guidelines for Neonates and infants with Heart disease:
 Stabilization and Transportation guidelines for Neonates and infants with Heart disease: Background: Referral Pediatric Cardiac Units, frequently receive neonates and infants referred and transported from
Stabilization and Transportation guidelines for Neonates and infants with Heart disease: Background: Referral Pediatric Cardiac Units, frequently receive neonates and infants referred and transported from
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Bits and Bobs secondary causes of heart problems. Dr Angela McBrien 9 th September 2017
 Bits and Bobs secondary causes of heart problems Dr Angela McBrien 9 th September 2017 Not the heart Dextroposition Heart in the right chest with the apex to the left Often caused by left sided chest mass
Bits and Bobs secondary causes of heart problems Dr Angela McBrien 9 th September 2017 Not the heart Dextroposition Heart in the right chest with the apex to the left Often caused by left sided chest mass
Cardiomyopathy: The Good, the Bad.and the Insurable?
 Cardiomyopathy: The Good, the Bad.and the Insurable? WAHLU Spring Seminar 2014 Joy Geiger, RN, BSN, ALMI Medical Consultant The Northwestern Mutual Life Insurance Company Milwaukee, WI Objectives Overview
Cardiomyopathy: The Good, the Bad.and the Insurable? WAHLU Spring Seminar 2014 Joy Geiger, RN, BSN, ALMI Medical Consultant The Northwestern Mutual Life Insurance Company Milwaukee, WI Objectives Overview
Index of subjects. effect on ventricular tachycardia 30 treatment with 101, 116 boosterpump 80 Brockenbrough phenomenon 55, 125
 145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
On Referral to our Unit
 Case Presentation By Samah Ibrahim Abdel Meguid Idris, MD Internal Medicine & Nephrology Consultant Head of Hemodialysis Unit Ahmed Maher Hospital, Alexandria Patient Data MEA 27-year-old male patient
Case Presentation By Samah Ibrahim Abdel Meguid Idris, MD Internal Medicine & Nephrology Consultant Head of Hemodialysis Unit Ahmed Maher Hospital, Alexandria Patient Data MEA 27-year-old male patient
Assessment of fetal heart function and rhythm
 Assessment of fetal heart function and rhythm The fetal myocardium Early Gestation Myofibrils 30% of myocytes Less sarcoplasmic reticula Late Gestation Myofibrils 60% of myocytes Increased force per unit
Assessment of fetal heart function and rhythm The fetal myocardium Early Gestation Myofibrils 30% of myocytes Less sarcoplasmic reticula Late Gestation Myofibrils 60% of myocytes Increased force per unit
Neonatal Resuscitation. Dustin Coyle, M.D. Anesthesiology
 Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
2
 1 2 Although the term "cardiomyopathy" could theoretically apply to almost any disease affecting the heart, it is usually reserved for "severe myocardial disease leading to heart failure".cardiomyopathy
1 2 Although the term "cardiomyopathy" could theoretically apply to almost any disease affecting the heart, it is usually reserved for "severe myocardial disease leading to heart failure".cardiomyopathy
Two Cardiology Zebras ERIC MARTIN MD
 Two Cardiology Zebras ERIC MARTIN MD Disclosures Bayer Gilead Sciences NIH Vascular Dynamics, In. Employer Iowa Heart Center/Mercy Des Moines Zebra # 1 History CC: 52-year-old man seen in consultation
Two Cardiology Zebras ERIC MARTIN MD Disclosures Bayer Gilead Sciences NIH Vascular Dynamics, In. Employer Iowa Heart Center/Mercy Des Moines Zebra # 1 History CC: 52-year-old man seen in consultation
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM
 MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM Are Particular Anti-hypertensives More Effective or Harmful Than Others in Hypertension in Pregnancy? Existing data is inadequate Methyldopa and
MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM Are Particular Anti-hypertensives More Effective or Harmful Than Others in Hypertension in Pregnancy? Existing data is inadequate Methyldopa and
CHAPTER 12 HYPERTENSION IN SPECIAL GROUPS HYPERTENSION IN PREGNANCY
 CHAPTER 12 HYPERTENSION IN SPECIAL GROUPS HYPERTENSION IN PREGNANCY v Mild preeclampsia is managed by close observation of the mother and fetus preferably in hospital. If the diastolic blood pressure remains
CHAPTER 12 HYPERTENSION IN SPECIAL GROUPS HYPERTENSION IN PREGNANCY v Mild preeclampsia is managed by close observation of the mother and fetus preferably in hospital. If the diastolic blood pressure remains
Hypotension in the Neonate
 Neonatal Nursing Education Brief: Hypotension in the Neonate http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/ Neonatal
Neonatal Nursing Education Brief: Hypotension in the Neonate http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/ Neonatal
2019 Qualified Clinical Data Registry (QCDR) Performance Measures
 Performance Measures") 2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
CongHeartDis.doc. Андрій Миколайович Лобода
 CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
Maternal And Fetal Outcome In Pregnancies Complicated With Maternal Cardiac Diseases: Experience At A Tertiary Care Hospital
 ISPUB.COM The Internet Journal of Gynecology and Obstetrics Volume 19 Number 1 Maternal And Fetal Outcome In Pregnancies Complicated With Maternal Cardiac Diseases: Experience At A Tertiary Care Hospital
ISPUB.COM The Internet Journal of Gynecology and Obstetrics Volume 19 Number 1 Maternal And Fetal Outcome In Pregnancies Complicated With Maternal Cardiac Diseases: Experience At A Tertiary Care Hospital
Diagnosis & Management of Heart Failure. Abena A. Osei-Wusu, M.D. Medical Fiesta
 Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year
![Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year](/thumbs/76/74263761.jpg "Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year") PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
Influence of RAAS inhibition on outflow tract obstruction in hypertrophic cardiomyopathy
 ORIGINAL ARTICLE 5 RAAS inhibitors should be avoided if possible in patients with obstructive HCM Influence of RAAS inhibition on outflow tract obstruction in hypertrophic cardiomyopathy Katrin Witzel,
ORIGINAL ARTICLE 5 RAAS inhibitors should be avoided if possible in patients with obstructive HCM Influence of RAAS inhibition on outflow tract obstruction in hypertrophic cardiomyopathy Katrin Witzel,
Heart Failure. Dr. William Vosik. January, 2012
 Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Case # 1. Page: 8. DUKE: Adams
 Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Pediatric Neurointervention: Vein of Galen Malformations
 Pediatric Neurointervention: Vein of Galen Malformations Johanna T. Fifi, M.D. Assistant Professor of Neurology, Neurosurgery, and Radiology Icahn School of Medicine at Mount Sinai November 9 th, 2014
Pediatric Neurointervention: Vein of Galen Malformations Johanna T. Fifi, M.D. Assistant Professor of Neurology, Neurosurgery, and Radiology Icahn School of Medicine at Mount Sinai November 9 th, 2014
HISTORY. Question: What type of heart disease is suggested by this history? CHIEF COMPLAINT: Decreasing exercise tolerance.
 HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
Management of Heart Failure and Cardiomyopathies in Pregnancy
 Management of Heart Failure and Cardiomyopathies in Pregnancy Professor Sanjay Sharma Disclosures: None Epidemiology of Cardiac Disease In Pregnancy Cardiovascular disease in pregnancy is increasing in
Management of Heart Failure and Cardiomyopathies in Pregnancy Professor Sanjay Sharma Disclosures: None Epidemiology of Cardiac Disease In Pregnancy Cardiovascular disease in pregnancy is increasing in
Fetal Tetralogy of Fallot
 36 Fetal Tetralogy of Fallot E.D. Bespalova, R.M. Gasanova, O.A.Pitirimova National Scientific and Practical Center of Cardiovascular Surgery, Moscow Elena D. Bespalova, MD Professor, Director Rena M,
36 Fetal Tetralogy of Fallot E.D. Bespalova, R.M. Gasanova, O.A.Pitirimova National Scientific and Practical Center of Cardiovascular Surgery, Moscow Elena D. Bespalova, MD Professor, Director Rena M,
Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016
 1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
Leitlinien. Hypoplastisches Linksherzsyndrom. Hypoplastic left heart syndrome (HLHS)
") 1.Title Hypoplastic left heart syndrome (HLHS) N.A. Haas, Bad Oeynhausen Ch. Jux, Giessen J. Photiadis, Berlin H.-H. Kramer, Kiel Typical forms: Mitral atresia/aortic atresia (MA/AoA) Mitral stenosis/aortic
1.Title Hypoplastic left heart syndrome (HLHS) N.A. Haas, Bad Oeynhausen Ch. Jux, Giessen J. Photiadis, Berlin H.-H. Kramer, Kiel Typical forms: Mitral atresia/aortic atresia (MA/AoA) Mitral stenosis/aortic
CASE DISCUSSION. Dr JAYASREE VEERABOINA 2nd yr PG MS OBG
 CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
What is Your Diagnosis?
 What is Your Diagnosis? A STORM R Dulgheru, Liege, Belgium Faculty disclosure Raluca Dulgheru I have no financial relationships to disclose. Case presentation 52 years old male Ongoing oppressive chest
What is Your Diagnosis? A STORM R Dulgheru, Liege, Belgium Faculty disclosure Raluca Dulgheru I have no financial relationships to disclose. Case presentation 52 years old male Ongoing oppressive chest
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014
 USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014 ino for Late Preterm and Term Infants with Severe PPHN Background:
USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014 ino for Late Preterm and Term Infants with Severe PPHN Background:
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Debate in Management of native COA; Balloon Versus Surgery
 Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
More History. Organization. Maternal Cardiac Disease: a historical perspective. The Parturient with Cardiac Disease 9/21/2012
 The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
Dr. Md. Rajibul Alam Prof. of Medicine Dinajpur Medical college
 Dr. Md. Rajibul Alam Prof. of Medicine Dinajpur Medical college PULMONARY HYPERTENSION Difficult to diagnose early Because Not detected during routine physical examination and Even in advanced cases symptoms
Dr. Md. Rajibul Alam Prof. of Medicine Dinajpur Medical college PULMONARY HYPERTENSION Difficult to diagnose early Because Not detected during routine physical examination and Even in advanced cases symptoms
Neonatal and Pediatric Pulmonary Vascular Disease
 Neonatal and Pediatric Pulmonary Vascular Disease Emma Olson, MS, ARNP Pediatric Cardiology Nurse Practitioner Canadian Respiratory Conference April 14, 2018 Financial Interest Disclosure (over the past
Neonatal and Pediatric Pulmonary Vascular Disease Emma Olson, MS, ARNP Pediatric Cardiology Nurse Practitioner Canadian Respiratory Conference April 14, 2018 Financial Interest Disclosure (over the past
TRAINING NEONATOLOGY SILVANA PARIS
 TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
How to Assess and Treat Obstructive Lesions
 How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Adults with Congenital Heart Disease. Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP
 Adults with Congenital Heart Disease Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP Outline History of CHD Statistics Specific lesions (TOF, TGA, Single ventricle) Erythrocytosis Pregnancy History
Adults with Congenital Heart Disease Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP Outline History of CHD Statistics Specific lesions (TOF, TGA, Single ventricle) Erythrocytosis Pregnancy History
Neonatal/Pediatric Cardiopulmonary Care. Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN. Other. Other Diseases
 PPHN. Other. Other Diseases") Neonatal/Pediatric Cardiopulmonary Care Other Diseases Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN 3 Also known as Persistent Fetal Circulation (PFC) Seen most frequently in term, post-term
Neonatal/Pediatric Cardiopulmonary Care Other Diseases Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN 3 Also known as Persistent Fetal Circulation (PFC) Seen most frequently in term, post-term
MITRAL STENOSIS. Joanne Cusack
 MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
3/14/2011 MANAGEMENT OF NEWBORNS CARDIAC INTENSIVE CARE CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 WITH HEART DEFECTS
 CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept
 Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
HISTORY. Question: How do you interpret the patient s history? CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: 45-year-old man.
 HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
TOPIC : Cardiogenic Shock
 University of Ferrara Department of Morphology, Surgery and Experimental Medicine. Section of Anaesthesia and Intensive Care Medicine TOPIC : Cardiogenic Shock What is shock? Shock is a condition of inadequate
University of Ferrara Department of Morphology, Surgery and Experimental Medicine. Section of Anaesthesia and Intensive Care Medicine TOPIC : Cardiogenic Shock What is shock? Shock is a condition of inadequate
Patent ductus arteriosus (PDA)
") Patent ductus arteriosus (PDA) Information for families Great Ormond Street Hospital for Children NHS Foundation Trust 2 This information sheet explains about the congenital (present at birth) heart condition
Patent ductus arteriosus (PDA) Information for families Great Ormond Street Hospital for Children NHS Foundation Trust 2 This information sheet explains about the congenital (present at birth) heart condition