Fluids Watch the type and measure the quantity
|
|
|
- Elmer Norton
- 5 years ago
- Views:
Transcription

1 Critical Care Medicine Apollo Hospitals Fluids Watch the type and measure the quantity Ramesh Venkataraman, AB (Int. Med), AB (CCM) Senior Consultant, Critical Care Medicine Apollo Hospitals Chennai

2 My Talk Effect of Fluid therapy Quantitative toxicity Qualitative toxicity
3 Fluid Therapy - Rationale Hypovolemia common in critically ill Fluid administration Reverses shock Restores/sustains perfusion and oxygen delivery Renal benefits Encourages diuresis Contrast and Rhabdomyolysis Dilutes nephrotoxins
4 Does Fluid Therapy Benefit Critically Ill? Hypoperfusion theory alone too simplistic Organ injury from complex interaction of host and disease Excludes inflammatory and microcirculatory alterations Response to fluid therapy unpredictable Critical illness, pre-existing disease and pharmacotherapy Extent and duration of responsiveness unclear Capillary leak Fluids do not correct vasodilatation Prowle, J. R. et al. Nat. Rev. Nephrol. 10, (2014)




5 New EGDT trials ProCESS ARISE ProMISE NO MORTALITY BENEFIT!!! Huang D et al. Intensive Care Med ;Aug 20

6 Neutral balance vs +7 L positive 1/3 rd in shock
 on 60-day mortality")
 2.")

7 1. Fluid balance (per L/day) on 60-day mortality OR 1.61 (95% CI, , p<0.001) 2. Furosemide (per 100mg/d) on 60-d mortality OR 0.48 (95% CI, , p=0.007)


8 Murphy CV et al. CHEST 2009; 136:
9 RRT need lower in restrictive strategy group 10% vs 14% (P = 0.06)
")
10 Can fluid therapy hurt the kidney? Prowle, J. R. et al. Nat. Rev. Nephrol. 10, (2014)
11 Fluid balance in AKI Fluid overload independently associated with poor outcomes Early positive fluid balance predicts AKI after cardiac surgery Fluid overload at RRT initiation associated with increased death and impaired renal recovery Negative balance with RRT associated with increased RRT-free days Prowle, J. R. et al. Nat. Rev. Nephrol. 6, (2010) Schrier RW Clin J Am Soc Nephrol 5: , 2010

12 Under estimation of serum creatinine Delay in diagnosis of AKI Wrong categorization of AKI class

13 Fluid Overload and Organ Dysfunction
14 Fluid Overload and Mortality SOAP study (N=3147 patients) Multicenter observational study (24 European centers) 36% had Sepsis Positive fluid balance (72 hours) predicts mortality Odds ratio (per liter increase) = 1.1 ( ); p = Odds ratio (per liter increase) = 1.21 ( ); p = AKI patients more fluid overloaded than non-aki
15
16 Fluid Overload and Mortality Observational study (N=618) > 10% increase in bodyweight from baseline PICARD study group Mortality Fluid overload at peak serum creatinine Less renal recovery (35 vs. 52%; P = 0.007) days 60 days Hospital DC Fluid Overload No Overload


17 Fluid Dose and Mortality


18 Beyond Starling Hydrostatic pressure Vs. Oncotic pressure Leaky capillaries interstitial edema Manipulation of colloid osmotic pressure ineffective Decreased rate of vascular refilling Potentiation of inflammation Myburgh JA et al. NEJM : 2013 : 369 ;
19 Natrituretic Peptides Shed Endothelial Glycolcalyx Jacob et al. Basic Res Cardiol (2013) 108:347

20 Beyond Starling Model Impaired glycocalyx Disruption of ECM Lymphatic dysfunction Prowle, J. R. et al. Crit. Care Clinics 2015 ( Article in press)


21 Fluids QuantitativeToxicity Dry and Fry Fill and kill Nephrologists Intensivists
: 24-33")
22 Fluid Balance Paradigm Guided fluid resuscitation Even fluid balance Appropriate fluid removal McDermid RC et al. WJCCM 2014; 3(1): 24-33
23 Fluid Measure the Quantity Take Home Optimization of central hemodynamics critical in shock, but. Response to fluids magnitude and duration unpredictable Fluid overload consistently shown to increase AKI and mortality Emerging pathophysiological insights Desire to achieve adequate resuscitation has to be mitigated against the harmful effects of fluid overload Careful volume assessment to avoid hypovolemia and fluid overload imperative throughout critical illness
24 AKI Mortality Quantitative Fluid Toxicity But what fluid to give when needed? Does it matter? Hypovolemia Hypervolemia Euvolemia Fluid Quantity

25 Colloid or Crystalloid? Survival Time Organ dysfunction N = 6933 Duration of MV 4% albumin vs. 0.9% Saline Duration of RRT Albumin: Saline Volume = 1:1.4 NEJM 2004;350: ICU LOS Hospital LOS

26 N = 2857 Colloid HES, Gelatin, Dextrans, 5% or 20% albumin Crystalloid Isotonic/hypertonic saline/buffered solution

27 Are All Colloids The Same? Molecular weight and Number average molecular weight Monodisperse vs polydisperse Mw-Viscosity; Mn Oncotic pressure Osmolality Oncotic pressure Plasma half life Plasma volume expansion Acid-base composition Electrolytes

28 Hydroxyethyl Starch Solutions 1. Concentration High or Low 2. Avg Mol Weight Low, medium or high 3. Molar substitution - Low or high 4. C2/C6 ratio

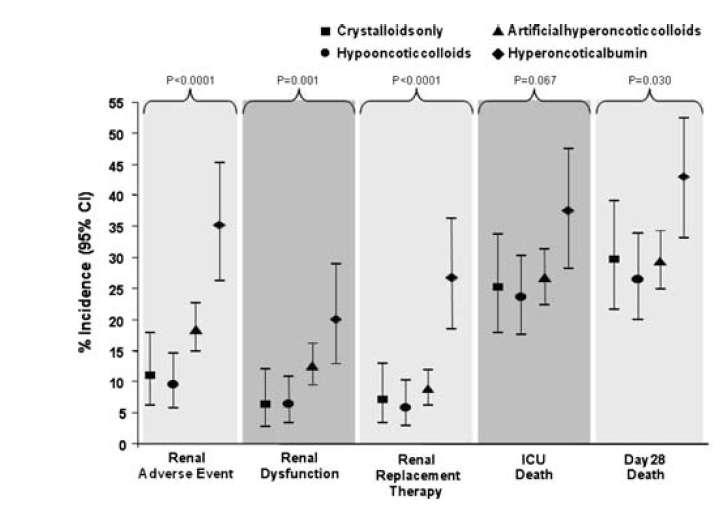
29 Volume Expansion (%) Are All Colloids The Same? Hyperoncotic Colloids
30 (N=1013)

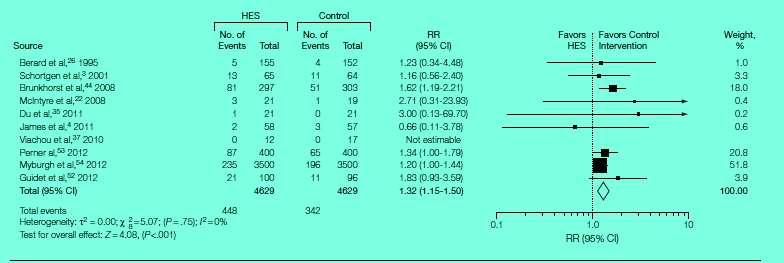
31 What about Starches? N = % Pentastarch (HES 200/0.5) vs. modified RL RL/HES ratio % vs. 22.8% ; P =0.02 Dose of HES independent predictor of both need of RRT and 90 day mortality



32 6S trial- NEJM July 2012 Higher rate of RRT at 90days N = 804 HES 6%/130/0.42 Upto 33ml/kg IBW
33 N = 7000 patients HES 6%/130/0.4-1:1.3 fluid ratio - No short-term hemodynamic benefits NEJM Nov 2012
34 Renal Events
35
36 Colloids Summary Take Home Colloids do not reduce fluid requirement significantly Glycocalyx disruption 5% albumin to be avoided in TBI Hyperoncotic colloids should be avoided HES increases risks of AKI, RRT and mortality Results confounded by fluid overload Should we then use a crystalloid? If so which one?

37 Are all crystalloids the same? Dilutional Acidosis Why doesn t it happen with other bicarbonate poor fluids? Plasma volume expansion Dilution of bicarbonate Renal bicarbonate wasting Grotthus mechanism Excess proton generation Hyperchloremia a mere association!!
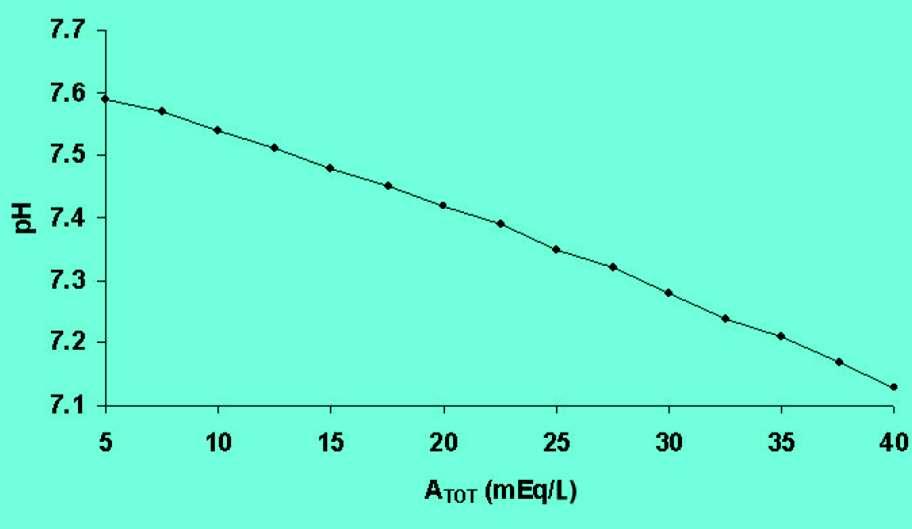
38 Determinants of [H + ] Blood Plasma OH - H + H 2 O Saline induced acidosis is secondary to pco 2 decreased SID caused by excess chloride Aload TOT - Decreased SID: Increased water dissociation and acidosis SID Stewart P. Can J Physiol Pharm 1983;61:1444
39 Saline Induced Acidosis Does it exist clinically? 1. Saline increases Cl- and decreases BE in a dose dependent manner 2. Saline cause moderate acidosis lasting 1-2 days 3. Respiratory compensation attenuates acidosis in an open system 4. Could be significant in patients with another acidemia 1 - Scheingraber S et al Anesthesiol 1999, 90: Boldt J et al. Anesth Analg 2009, 109: O Dell E et al. Crit Care Med 2007, 35:
40 Chloride And The Kidney 1. Hyperchloremia produces 1. Progressive renal vasoconstriction Tubuloglomerular Feedback 2. Fall in GFR that is independent of the renal nerves 3. Changes related to tubular Cl - reabsorption Chloride-induced vasoconstriction appears specific for the renal vessels Wilcox CS. J Clin Invest. 1983;71(3):

41 Does this acidosis pose problems? Renal Renal vasoconstriction and decrease in GFR Delayed time to micturition Decreased urine output and sodium excretion GI function Decreased gastric perfusion Prolonged gastric emptying time and ileus Postoperative nausea and vomiting Pro-inflammatory Cogulation abnormalities May trigger inappropriate therapies Guidet B et al. et al. Critical Care 2010, 14:325
42 Can we prevent Saline-induced acidosis? Large volume of NS Decrease in SID Decrease in A TOT Metabolic Acidemia Metabolic Alkalemia Therefore to prevent Saline induced acidosis, extracellular SID must fall during the infusion ONLY enough to counteract the progressive A TOT dilutional alkalosis (IDEAL SID = 24) 1 1-Morgan T et al. Crit Care Resusc 2003, 5:

43 What is a balanced fluid? The ideal balanced crystalloid is normotonic with a SID of 24 meq/l Achieved by excising chloride from NS and substituting bicarbonate Bicarbonate cannot be included in IVF Instability and precipitation Addition of other anions Acetate, Lactate, or Gluconate

44 What options do we have? Have no conflicts to declare Don t favour any particular product
 5.05 Intervention L per patient period during NS, control 4% albumin period and 4.")
45 Clinical Data Saline Prospective prescription open decreased label sequential (3.2 vs period 0.06 L/patient; study P.001) and 4% Done gelatin during solution entire from ICU (0.7 stay vs 0 L/patient; P.001) 5.05 Intervention L per patient period during NS, control 4% albumin period and % gelatin L per patient avoided during intervention Hartman s, period Plasmalyte- 148 and 20% albumin used Yunos Net al et al. JAMA, October 17, 2012 Vol 308, No. 15
; P = 0.")
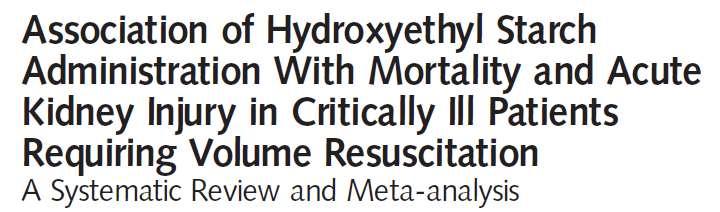
![001] Reduction in the increase of mean creatinine](/docs-images/80/82208500/images/46-1.jpg "level from baseline to peak ICU level Use of RRT (OR-")
46 Chloride rich fluid More AKI and RRT AKI (OR [95% (CI, ); P = 0.001] Reduction in the increase of mean creatinine level from baseline to peak ICU level Use of RRT (OR [95% CI, ]; P=0.004)
47 Annals of Surgery Volume 255, Number 5, May 2012 Retrospective cohort study using a large, US automated hospital claims database Exclusively 0.9% saline or Plasma-Lyte A or Plasma-Lyte 148 on the day of surgery 3:1 propensity match 926:2778 patients analysed


48 Annals of Surgery Volume 255, Number 5, May 2012

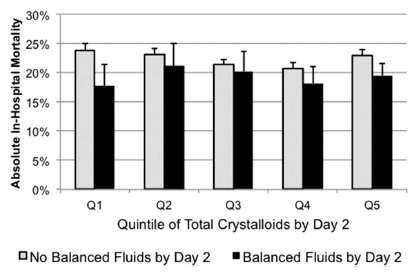
49 N = % balanced crystalloid
50 AKI Mortality Fluid Toxicity Watch the type Fluid type Hypovolemia Hypervolemia Euvolemia Fluid Quantity
51 Fluids Watch the Type and measure the Quantity Take Home Volume and choice of fluid seem to impact renal function and mortality Context of fluid therapy profoundly alters risk/benefit Early aggressive resuscitation of shock followed by a conservative strategy seems prudent Choose your poison carefully Avoid hyperoncotic albumin and HES Avoid hyperchloremia

52
53 HCl loading in a normal 70kg man 10 mmol/l 1N HCl SID [H+] ph HCO pco 2 = 40 ATOT = 15 Na + = 143 Cl - = 110
54 Physico-chemical Approach Both H + and HCO3 - are dependent variables Bicarbonate just a gap filler between strong cations and anions Metabolic component Strong Ion Difference and Atot Respiratory component PCO2 Six acid-base disorders SIDe increase and decrease alkalosis and acidosis A TOT increase and decrease acidosis and alkalosis Respiratory
55 mmol/l Acid Load 3hrs Post-endotoxin Mean acid load 8.7 mmol/l CO2 (3.1%) Lactate (9.6%) SIG (7.7%) Saline (37.4%) Unknown (42.2%) dog # Kellum et al. Shock 1998; 9:
56 SID vs ph & [H + ] ph [H+] nmol/l [SID] meq/l

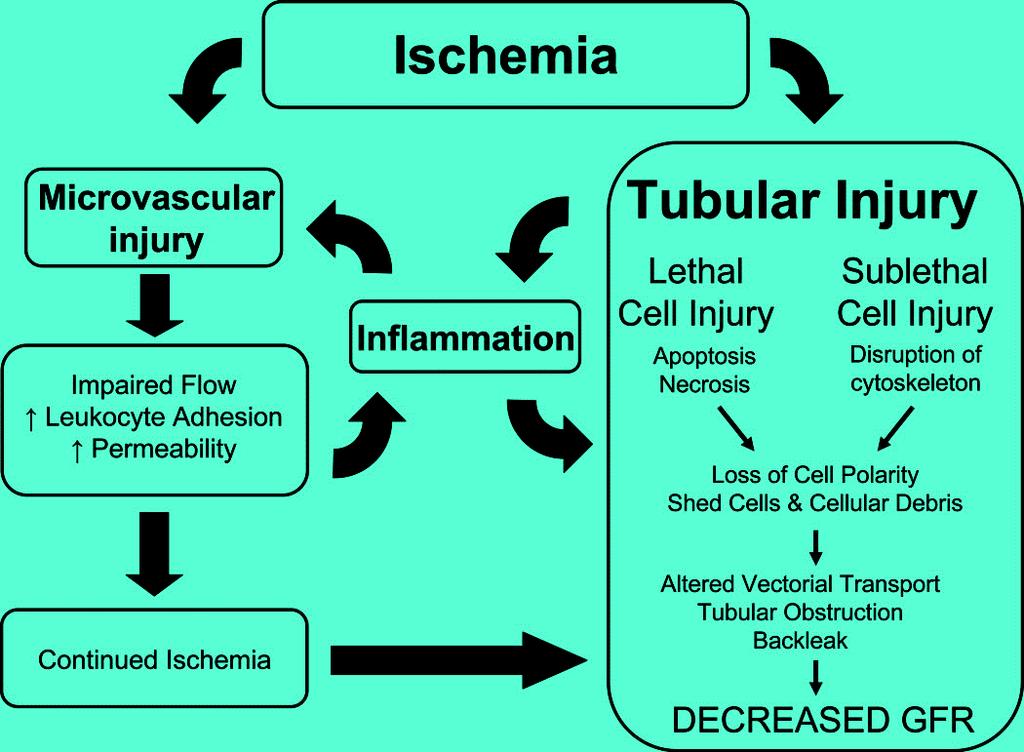
57 Regional Blood Flow Variation
58
59 Fluid balance in AKI Fluid overload independently associated with poor outcomes Early positive fluid balance predicts AKI after cardiac surgery Fluid overload at the commencement of RRT associated with increased death and impaired renal recovery Negative balance with RRT associated with increased RRT-free days
60 Fluid overload - Marker or Mediator? SOAP study definition of AKI Stage 3 only ARDS FACT study Adverse effects of fluid in early AKI group?dilution of serum creatinine Increased fluid overload at dialysis initiation?paradigm shift EGDT study Equal volume at 72 hours (13-14L) Fluid overload Cause vs. effect Direct Indirect marker of severity Intolerance to fluid removal Harm from fluid removal Harm from ineffective fluid removal

61 Natrituretic Peptides Shed Endothelial Glycolcalyx Jacob et al. Basic Res Cardiol (2013) 108:347
62 Fluid Resuscitation Fluid resuscitation is the most frequent intervention in the ICU Normal saline is the commonest fluid used for resuscitation Standard against which other solutions are measured/compared Resuscitation with normal saline causes metabolic acidosis Cardiopulmonary bypass Handy JM et al. British Journal of Anaesthesia 101 (2): (2008) Hayhoe et al. Intensive Care Med. 25: ; 1999
63 Physico - chemical approach H + and HCO3 are only DEPENDENT variables Determinant of H+ is water dissociation Aqueous Solutions Water Dissociation Acids increase water dissociation H 2 O H + + OH -
64 Strong Ion Difference (SID) Mg ++ Ca ++ K + Na + Cl - Others (lactate, etc) These are the Strong Ions, so-called because they do not readily combine with other ions or lose their charge. Conversely, H + and HCO 3 - readily combine, and are called weak ions Normal extracellular fluid SID is 40 Decrease in SID increases water dissociation

65 Stewart Approach


66 Its not the chloride silly!!!! It s the SID of the fluid that matters!!! Story DA et al. Anesth Analg 2006;103:144 8

67 Is all acidosis the same? Gunnerson K et al. et al. Crit Care 2006, 10:R22
Intravenous Fluid Therapy in Critical Illness
 Intravenous Fluid Therapy in Critical Illness GINA HURST, MD DIVISION OF EMERGENCY CRITICAL CARE HENRY FORD HOSPITAL DETROIT, MI Objectives Establish goals of IV fluid therapy Review fluid types and availability
Intravenous Fluid Therapy in Critical Illness GINA HURST, MD DIVISION OF EMERGENCY CRITICAL CARE HENRY FORD HOSPITAL DETROIT, MI Objectives Establish goals of IV fluid therapy Review fluid types and availability
What is the right fluid to use?
 What is the right fluid to use? L McIntyre Associate Professor, University of Ottawa Senior Scientist, Ottawa Hospital Research Institute Centre for Transfusion Research CCCF, November 2, 2016 Disclosures
What is the right fluid to use? L McIntyre Associate Professor, University of Ottawa Senior Scientist, Ottawa Hospital Research Institute Centre for Transfusion Research CCCF, November 2, 2016 Disclosures
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
What is the Role of Albumin in Sepsis? An Evidenced Based Affair. Justin Belsky MD PGY3 2/6/14
 What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
Getting smart with fluids in the critically ill. NOR AZIM MOHD YUNOS Jeffrey Cheah School of Medicine & Health Sciences Monash University Malaysia
 Getting smart with fluids in the critically ill NOR AZIM MOHD YUNOS Jeffrey Cheah School of Medicine & Health Sciences Monash University Malaysia Isotonic Solutions and Major Adverse Renal Events Trial
Getting smart with fluids in the critically ill NOR AZIM MOHD YUNOS Jeffrey Cheah School of Medicine & Health Sciences Monash University Malaysia Isotonic Solutions and Major Adverse Renal Events Trial
Fluids in ICU. JMO teaching 5th July 2016
 Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Fluid Therapy and Outcome: Balance Is Best
 The Journal of ExtraCorporeal Technology Fluid Therapy and Outcome: Balance Is Best Sara J. Allen, FANZCA, FCICM Department of Anaesthesia and the Cardiothoracic and Vascular Intensive Care Unit, Auckland
The Journal of ExtraCorporeal Technology Fluid Therapy and Outcome: Balance Is Best Sara J. Allen, FANZCA, FCICM Department of Anaesthesia and the Cardiothoracic and Vascular Intensive Care Unit, Auckland
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR
 Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
INTRAVENOUS FLUID THERAPY. Tom Heaps Consultant Acute Physician
 INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
Acid-Base balance in the ICU The Stewart Approach. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Acid-Base balance in the ICU The Stewart Approach Intensive Care Training Program Radboud University Medical Centre Nijmegen Relation [H + ] and ph 300 250 [H + ] nmol/l 200 150 100 50 0 6,4 6,6 6,8 7
Acid-Base balance in the ICU The Stewart Approach Intensive Care Training Program Radboud University Medical Centre Nijmegen Relation [H + ] and ph 300 250 [H + ] nmol/l 200 150 100 50 0 6,4 6,6 6,8 7
WHICH FLUIDS SHOULD BE USED IN THE CLINICAL SETTING? My personal strategy : crystalloids + colloids. Why?
 WHICH FLUIDS SHOULD BE USED IN THE CLINICAL SETTING? Big debate: crystalloids colloids crystalloids + colloids My personal strategy : crystalloids + colloids Why? Crystalloids + colloids end of the story?
WHICH FLUIDS SHOULD BE USED IN THE CLINICAL SETTING? Big debate: crystalloids colloids crystalloids + colloids My personal strategy : crystalloids + colloids Why? Crystalloids + colloids end of the story?
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
I Suggest Abnormal Saline
 I Suggest Abnormal Saline Sean M Bagshaw, MD, MSc Division of Critical Care Medicine University of Alberta CCCF Oct 27, 2015 2015 Disclosures Salary support: Canada/Alberta government Grant support: Canada/Alberta
I Suggest Abnormal Saline Sean M Bagshaw, MD, MSc Division of Critical Care Medicine University of Alberta CCCF Oct 27, 2015 2015 Disclosures Salary support: Canada/Alberta government Grant support: Canada/Alberta
Fluid Management in Critically Ill AKI Patients
 Fluid Management in Critically Ill AKI Patients Sang Kyung Jo, MD, PhD Department of Internal Medicine Korea University Medical College KO/MG31/15-0017 Outline Fluid balance in critically ill patients:
Fluid Management in Critically Ill AKI Patients Sang Kyung Jo, MD, PhD Department of Internal Medicine Korea University Medical College KO/MG31/15-0017 Outline Fluid balance in critically ill patients:
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Acid-Base balance in the ICU The Stewart Approach. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Acid-Base balance in the ICU The Stewart Approach Intensive Care Training Program Radboud University Medical Centre Nijmegen Relation [H + ] and ph 300 250 [H + ] nmol/l 200 150 100 50 0 6,4 6,6 6,8 7
Acid-Base balance in the ICU The Stewart Approach Intensive Care Training Program Radboud University Medical Centre Nijmegen Relation [H + ] and ph 300 250 [H + ] nmol/l 200 150 100 50 0 6,4 6,6 6,8 7
Modern fluid therapy. Anders Perner. Dept of Intensive Care, Rigshospitalet, University of Copenhagen
 Modern fluid therapy Anders Perner Dept of Intensive Care, Rigshospitalet, University of Copenhagen Scandinavian Critical Care Trials Group www.ssai.info/research/scctg Intensive Care Medicine www.icmjournal.esicm.org
Modern fluid therapy Anders Perner Dept of Intensive Care, Rigshospitalet, University of Copenhagen Scandinavian Critical Care Trials Group www.ssai.info/research/scctg Intensive Care Medicine www.icmjournal.esicm.org
Comment on infusion solutions containing HES
 Comment on infusion solutions containing HES The European Medicines Agency (EMA) published on 14 June 2013 Pharmacovigilance Risk Assessment Committee (PRAC) recommends suspending marketing authorisations
Comment on infusion solutions containing HES The European Medicines Agency (EMA) published on 14 June 2013 Pharmacovigilance Risk Assessment Committee (PRAC) recommends suspending marketing authorisations
Fluid assessment, monitoring and therapy for the acute nurse
 Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Bicarbonate in the NICU
 OMG Bicarbonate in the NICU A Useless Therapy? At first I thought I was going to have to refute the paper Then I got into it and thought: I m so confused Then I learned a lot HOPEFULLY I CAN LEARN YOU
OMG Bicarbonate in the NICU A Useless Therapy? At first I thought I was going to have to refute the paper Then I got into it and thought: I m so confused Then I learned a lot HOPEFULLY I CAN LEARN YOU
Principles of Fluid Balance
 Principles of Fluid Balance I. The Cellular Environment: Fluids and Electrolytes A. Water 1. Total body water (TBW) = 60% of total body weight 2. Fluid Compartments in the Body a. Intracellular Compartment
Principles of Fluid Balance I. The Cellular Environment: Fluids and Electrolytes A. Water 1. Total body water (TBW) = 60% of total body weight 2. Fluid Compartments in the Body a. Intracellular Compartment
Managing Acid Base and Electrolyte Disturbances with RRT
 Managing Acid Base and Electrolyte Disturbances with RRT John R Prowle MA MSc MD MRCP FFICM Consultant in Intensive Care & Renal Medicine RRT for Regulation of Acid-base and Electrolyte Acid base load
Managing Acid Base and Electrolyte Disturbances with RRT John R Prowle MA MSc MD MRCP FFICM Consultant in Intensive Care & Renal Medicine RRT for Regulation of Acid-base and Electrolyte Acid base load
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Fluids in Sepsis Less is more. Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth,
 Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
Resuscitation fluids in critical care
 Resuscitation fluids in critical care John A Myburgh MBBCh PhD FCICM UNSW Professor of Critical Care Medicine The George Institute for Global Health University of New South Wales St George Hospitals, Sydney
Resuscitation fluids in critical care John A Myburgh MBBCh PhD FCICM UNSW Professor of Critical Care Medicine The George Institute for Global Health University of New South Wales St George Hospitals, Sydney
Actualités sur le remplissage peropératoire. Philippe Van der Linden MD, PhD
 Actualités sur le remplissage peropératoire Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Perioperative Fluid Volume Administration
Actualités sur le remplissage peropératoire Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Perioperative Fluid Volume Administration
Biochemistry of acid-base disorders. Alice Skoumalová
 Biochemistry of acid-base disorders Alice Skoumalová Main topics of the lecture: Measurement of acid-base dysbalance Classification of the acid-base disorders 4 basic acid-base disorders and their compensaiton
Biochemistry of acid-base disorders Alice Skoumalová Main topics of the lecture: Measurement of acid-base dysbalance Classification of the acid-base disorders 4 basic acid-base disorders and their compensaiton
Fencl Stewart analysis of acid base changes immediately after liver transplantation
 Fencl Stewart analysis of acid base changes immediately after liver transplantation David A Story, Rakesh Vaja, Stephanie J Poustie and Larry McNicol The acid base changes associated with liver transplantation
Fencl Stewart analysis of acid base changes immediately after liver transplantation David A Story, Rakesh Vaja, Stephanie J Poustie and Larry McNicol The acid base changes associated with liver transplantation
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Salty Solutions or Salty Problems? Outline. Outline 29/04/2013
 Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Acute Kidney Injury for the General Surgeon
 Acute Kidney Injury for the General Surgeon UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Epidemiology & Definition Pathophysiology Clinical Studies Management Summary Hobart W. Harris,
Acute Kidney Injury for the General Surgeon UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Epidemiology & Definition Pathophysiology Clinical Studies Management Summary Hobart W. Harris,
JOURNAL CLUB: THE FLUIDS DEBATE. Veronica Ueckermann
 JOURNAL CLUB: THE FLUIDS DEBATE Veronica Ueckermann INTRODUCTION The selection and use of resuscitation fluids should be based on physiological principles. However, historically, clinical practice has
JOURNAL CLUB: THE FLUIDS DEBATE Veronica Ueckermann INTRODUCTION The selection and use of resuscitation fluids should be based on physiological principles. However, historically, clinical practice has
LETTER TO THE EDITOR
 LETTER TO THE EDITOR A PHYSICOCHEMICAL ACID-BASE APPROACH FOR MANAGING DIABETIC KETOACIDOSIS doi: 10.1590/S1807-59322009000700018 Alexandre Toledo Maciel, Marcelo Park INTRODUCTION Diabetic ketoacidosis
LETTER TO THE EDITOR A PHYSICOCHEMICAL ACID-BASE APPROACH FOR MANAGING DIABETIC KETOACIDOSIS doi: 10.1590/S1807-59322009000700018 Alexandre Toledo Maciel, Marcelo Park INTRODUCTION Diabetic ketoacidosis
Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED. Surgical Grand Rounds
 Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED Surgical Grand Rounds ALBUMIN Most abundant plasma protein 1/3 intravascular 50% of interstitial SKIN Synthesized in hepatocytes Transcapillary escape rate COP
Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED Surgical Grand Rounds ALBUMIN Most abundant plasma protein 1/3 intravascular 50% of interstitial SKIN Synthesized in hepatocytes Transcapillary escape rate COP
Fluid management. Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center
 Fluid management Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center Disclosure Consultant and research funding Edwards Lifesciences Goals of fluid therapy 1. Maintain
Fluid management Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center Disclosure Consultant and research funding Edwards Lifesciences Goals of fluid therapy 1. Maintain
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
Les solutés de remplissage. Philippe Van der Linden MD, PhD
 Les solutés de remplissage Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Fluid Resuscitation Morbidity Procedure Co-morbidities
Les solutés de remplissage Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Fluid Resuscitation Morbidity Procedure Co-morbidities
Change in Serum Chloride Level after Loading Dose of Sterofundin Solution Compared with Normal Saline Solution
 Original Article Change in Serum Chloride Level after Loading Dose of Sterofundin Solution Compared with Normal Saline Solution Sunthiti Morakul MD 1, Cherdkiat Karnjanarachata MD 1, Thanist Pravitharangul
Original Article Change in Serum Chloride Level after Loading Dose of Sterofundin Solution Compared with Normal Saline Solution Sunthiti Morakul MD 1, Cherdkiat Karnjanarachata MD 1, Thanist Pravitharangul
Acid and Base Balance
 Acid and Base Balance 1 2 The Body and ph Homeostasis of ph is tightly controlled Extracellular fluid = 7.4 Blood = 7.35 7.45 < 7.35: Acidosis (acidemia) > 7.45: Alkalosis (alkalemia) < 6.8 or > 8.0: death
Acid and Base Balance 1 2 The Body and ph Homeostasis of ph is tightly controlled Extracellular fluid = 7.4 Blood = 7.35 7.45 < 7.35: Acidosis (acidemia) > 7.45: Alkalosis (alkalemia) < 6.8 or > 8.0: death
[Chapter 25] The Liver and the Gut. John A Kellum
![[Chapter 25] The Liver and the Gut. John A Kellum](/thumbs/85/92127350.jpg "[Chapter 25] The Liver and the Gut. John A Kellum") [Chapter 25] The Liver and the Gut John A Kellum 25.1 Introduction Throughout this book we have seen that the Stewart formulation can be used to help understand the mechanisms of acid-base equilibrium
[Chapter 25] The Liver and the Gut John A Kellum 25.1 Introduction Throughout this book we have seen that the Stewart formulation can be used to help understand the mechanisms of acid-base equilibrium
Dialyzing challenging patients: Patients with hepato-renal conditions
 Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Fluids and Lactate. A/Prof Peter Morley
 Fluids and Lactate A/Prof Peter Morley RCTs Other evidence 5 6 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid Plan Background
Fluids and Lactate A/Prof Peter Morley RCTs Other evidence 5 6 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid Plan Background
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
METHODS RESULTS. Int. J. Med. Sci. 2012, 9. Methods of measurement. Outcome measures. Primary data analysis. Study design and setting
 59 Research Paper Ivyspring International Publisher International Journal of Medical Sciences 2012; 9(1):59-64 A Randomized Clinical Trial Comparing the Effect of Rapidly Infused Crystalloids on Acid-Base
59 Research Paper Ivyspring International Publisher International Journal of Medical Sciences 2012; 9(1):59-64 A Randomized Clinical Trial Comparing the Effect of Rapidly Infused Crystalloids on Acid-Base
Fluid Management in the Critically-Ill
 Fluid Management in the Critically-Ill Dan Schuller, M.D. Professor and Chair Department of Internal Medicine - Transmountain Texas Tech University Health Sciences Center El Paso Paul L. Foster School
Fluid Management in the Critically-Ill Dan Schuller, M.D. Professor and Chair Department of Internal Medicine - Transmountain Texas Tech University Health Sciences Center El Paso Paul L. Foster School
Principles of Infusion Therapy: Fluids
 Principles of Infusion Therapy: Fluids Christie Heinzman, MSN, APRN-CNP Acute Care Pediatric Nurse Practitioner Cincinnati Children s Hospital Medical Center May 22, 2018 Conflict of Interest Disclosure
Principles of Infusion Therapy: Fluids Christie Heinzman, MSN, APRN-CNP Acute Care Pediatric Nurse Practitioner Cincinnati Children s Hospital Medical Center May 22, 2018 Conflict of Interest Disclosure
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Approach to Severe Sepsis. Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore
 Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
FLUID RESUSCITATION SUMMARY
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Albumina nel paziente critico. Savona 18 aprile 2007
 Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Is there a role for Sodium Bicarbonate in NICU? Stephen Wardle Consultant Neonatologist Nottingham University Hospitals
 Is there a role for Sodium Bicarbonate in NICU? Stephen Wardle Consultant Neonatologist Nottingham University Hospitals Aim / Objectives To persuade you:- there is no evidence in favour of using bicarbonate
Is there a role for Sodium Bicarbonate in NICU? Stephen Wardle Consultant Neonatologist Nottingham University Hospitals Aim / Objectives To persuade you:- there is no evidence in favour of using bicarbonate
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Fluid Treatments in Sepsis: Meta-Analyses
 Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
Inter Inter Pretation of Acid Base Disturbance in Critically ill Patients. By :-: Dr. Vinay Bhomia M.D.
 Inter Inter Pretation of Acid Base Disturbance in Critically ill Patients. By :-: Dr. Vinay Bhomia M.D. Normal Blood PH 7.35 to 7.45 Crucial importance to maintain homeostatic function of Body. Any Significant
Inter Inter Pretation of Acid Base Disturbance in Critically ill Patients. By :-: Dr. Vinay Bhomia M.D. Normal Blood PH 7.35 to 7.45 Crucial importance to maintain homeostatic function of Body. Any Significant
Acid-Base disturbances Physiological approach
 AcidBase disturbances Physiological approach Pieter Roel Tuinman, M.D., PhD, intensivist Department of Intensive Care, VU Medical Center, Amsterdam, The Netherlands p.tuinman@vumc.nl Content Introduction
AcidBase disturbances Physiological approach Pieter Roel Tuinman, M.D., PhD, intensivist Department of Intensive Care, VU Medical Center, Amsterdam, The Netherlands p.tuinman@vumc.nl Content Introduction
Fluid therapy using a balanced crystalloid solution and acid base stability after cardiac surgery
 Fluid therapy using a balanced crystalloid solution and acid base stability after cardiac surgery Roger J Smith, David A Reid, Elizabeth F Delaney and John D Santamaria There is increasing interest in
Fluid therapy using a balanced crystalloid solution and acid base stability after cardiac surgery Roger J Smith, David A Reid, Elizabeth F Delaney and John D Santamaria There is increasing interest in
ROBERT SÜMPELMANN MD, PhD*, LARS WITT MD*, MEIKE BRÜTT MD*, DIRK OSTERKORN MD, WOLFGANG KOPPERT MD, PhD* AND WILHELM A.
 Pediatric Anesthesia 21 2: 1 14 doi:1.1111/j.146-9592.29.3197.x Changes in acid-base, electrolyte and hemoglobin concentrations during infusion of hydroxyethyl starch 13.42 6 : 1 in normal saline or in
Pediatric Anesthesia 21 2: 1 14 doi:1.1111/j.146-9592.29.3197.x Changes in acid-base, electrolyte and hemoglobin concentrations during infusion of hydroxyethyl starch 13.42 6 : 1 in normal saline or in
KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS
 KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS INTRODUCTION Formulating a fluid therapy plan for the critical small animal patient requires careful determination of the current volume
KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS INTRODUCTION Formulating a fluid therapy plan for the critical small animal patient requires careful determination of the current volume
Burn Resuscitation Formulas. John P. Sabra, MD Seton Surgical Group Department of Surgery Dell Medical School Austin, TX
 Burn Resuscitation Formulas John P. Sabra, MD Seton Surgical Group Department of Surgery Dell Medical School Austin, TX BURN INJURY % Physiologic Change % TBSA burn Stasis BURN VASCULAR PERMEABILITY
Burn Resuscitation Formulas John P. Sabra, MD Seton Surgical Group Department of Surgery Dell Medical School Austin, TX BURN INJURY % Physiologic Change % TBSA burn Stasis BURN VASCULAR PERMEABILITY
Acute Kidney Injury in the ED
 + Acute Kidney Injury in the ED + Dr Eric Clark, MD FRCPC University of Ottawa Canada Canadian Association of Emergency Physicians + Outline 1. Diagnostic challenges 2. ED treatment 3. Contrast induced
+ Acute Kidney Injury in the ED + Dr Eric Clark, MD FRCPC University of Ottawa Canada Canadian Association of Emergency Physicians + Outline 1. Diagnostic challenges 2. ED treatment 3. Contrast induced
Septic AKI in ICU patients
 Septic AKI in ICU patients Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany achim.joerres@charite.de Agenda Epidemiology
Septic AKI in ICU patients Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany achim.joerres@charite.de Agenda Epidemiology
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
1. 09/07/16 Ch 1: Intro to Human A & P 1
 Table of Contents # Date Title Page # 1. 09/07/16 Ch 1: Intro to Human A & P 1 2. 09/19/16 Ch 18: Water, Electrolyte, and Acid-Base Balance 5 i 1 09/19/16 Chapter 18: Water, Electrolyte, and Acid-Base
Table of Contents # Date Title Page # 1. 09/07/16 Ch 1: Intro to Human A & P 1 2. 09/19/16 Ch 18: Water, Electrolyte, and Acid-Base Balance 5 i 1 09/19/16 Chapter 18: Water, Electrolyte, and Acid-Base
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua
 & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua") Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
Nurse Driven Fluid Optimization Using Dynamic Assessments
 Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
The equilibrium between basis and acid can be calculated and termed as the equilibrium constant = Ka. (sometimes referred as the dissociation constant
 Acid base balance Dobroslav Hájek dhajek@med.muni.cz May 2004 The equilibrium between basis and acid can be calculated and termed as the equilibrium constant = Ka. (sometimes referred as the dissociation
Acid base balance Dobroslav Hájek dhajek@med.muni.cz May 2004 The equilibrium between basis and acid can be calculated and termed as the equilibrium constant = Ka. (sometimes referred as the dissociation
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
The incidence and prognostic value of hypochloremia in critically ill patients
 1 The incidence and prognostic value of hypochloremia in critically ill patients Makiko Tani 1, Hiroshi Morimatsu 2#, FumiakiTakatsu 3, Kiyoshi Morita 1 1. Department of Anesthesiology and Resuscitology,
1 The incidence and prognostic value of hypochloremia in critically ill patients Makiko Tani 1, Hiroshi Morimatsu 2#, FumiakiTakatsu 3, Kiyoshi Morita 1 1. Department of Anesthesiology and Resuscitology,
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Acid Base Balance. Professor Dr. Raid M. H. Al-Salih. Clinical Chemistry Professor Dr. Raid M. H. Al-Salih
 Acid Base Balance 1 HYDROGEN ION CONCENTRATION and CONCEPT OF ph Blood hydrogen ion concentration (abbreviated [H + ]) is maintained within tight limits in health, with the normal concentration being between
Acid Base Balance 1 HYDROGEN ION CONCENTRATION and CONCEPT OF ph Blood hydrogen ion concentration (abbreviated [H + ]) is maintained within tight limits in health, with the normal concentration being between
INTRAVENOUS FLUIDS. Ahmad AL-zu bi
 INTRAVENOUS FLUIDS Ahmad AL-zu bi Types of IV fluids Crystalloids colloids Crystalloids Crystalloids are aqueous solutions of low molecular weight ions,with or without glucose. Isotonic, Hypotonic, & Hypertonic
INTRAVENOUS FLUIDS Ahmad AL-zu bi Types of IV fluids Crystalloids colloids Crystalloids Crystalloids are aqueous solutions of low molecular weight ions,with or without glucose. Isotonic, Hypotonic, & Hypertonic
Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia (Spain) Pulsion MAB
 Pulsion MAB") State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
SHOCK. Pathophysiology
 SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
The kidney. (Pseudo) Practical questions. The kidneys are all about keeping the body s homeostasis. for questions Ella
 Practical questions. The kidneys are all about keeping the body s homeostasis. for questions Ella") The kidney (Pseudo) Practical questions for questions Ella (striemit@gmail.com) The kidneys are all about keeping the body s homeostasis Ingestion Product of metabolism H 2 O Ca ++ Cl - K + Na + H 2 O
The kidney (Pseudo) Practical questions for questions Ella (striemit@gmail.com) The kidneys are all about keeping the body s homeostasis Ingestion Product of metabolism H 2 O Ca ++ Cl - K + Na + H 2 O
Acids and Bases their definitions and meanings
 Acids and Bases their definitions and meanings Molecules containing hydrogen atoms that can release hydrogen ions in solutions are referred to as acids. (HCl H + Cl ) (H 2 CO 3 H + HCO 3 ) A base is an
Acids and Bases their definitions and meanings Molecules containing hydrogen atoms that can release hydrogen ions in solutions are referred to as acids. (HCl H + Cl ) (H 2 CO 3 H + HCO 3 ) A base is an
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Keywords acid base disorder, hyperchloremia, metabolic acidosis, strong ion difference, strong ion gap
 Research Conventional or physicochemical approach in intensive care unit patients with metabolic acidosis Mirjam Moviat 1, Frank van Haren 2 and Hans van der Hoeven 3 Open Access 1 Research Fellow, Department
Research Conventional or physicochemical approach in intensive care unit patients with metabolic acidosis Mirjam Moviat 1, Frank van Haren 2 and Hans van der Hoeven 3 Open Access 1 Research Fellow, Department
Clinical Study The Incidence and Prognostic Value of Hypochloremia in Critically Ill Patients
 The Scientific World Journal Volume 2012, Article ID 474185, 7 pages doi:10.1100/2012/474185 The cientificworldjournal Clinical Study The Incidence and Prognostic Value of Hypochloremia in Critically Ill
The Scientific World Journal Volume 2012, Article ID 474185, 7 pages doi:10.1100/2012/474185 The cientificworldjournal Clinical Study The Incidence and Prognostic Value of Hypochloremia in Critically Ill
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
University of Groningen. Acute kidney injury after cardiac surgery Loef, Berthus Gerard
 University of Groningen Acute kidney injury after cardiac surgery Loef, Berthus Gerard IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it.
University of Groningen Acute kidney injury after cardiac surgery Loef, Berthus Gerard IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it.
mmol.l -1 H+ Ca++ K+ Na+
 Disorders of acid-base equilibrium Pathobiochemistry and diagnostics of acid-base and mineral metabolism Physiologic ph Plasma and most extracellular fluids ph = 7.40 ± 0.02 Significance of constant ph
Disorders of acid-base equilibrium Pathobiochemistry and diagnostics of acid-base and mineral metabolism Physiologic ph Plasma and most extracellular fluids ph = 7.40 ± 0.02 Significance of constant ph
9/13/2015. Laboratory. HPI and PE
 Critical Care HPI and PE 74 yo male confused SBP 90/20 MAP50, P 122, RR 34 Ox1 w/o nuchal rigidity S1S2 wo m RLL reduced breath sounds Skin warm dry Laboratory» WBC 15,600 Hgb 8.4 HCt 23%, Plts 95000,
Critical Care HPI and PE 74 yo male confused SBP 90/20 MAP50, P 122, RR 34 Ox1 w/o nuchal rigidity S1S2 wo m RLL reduced breath sounds Skin warm dry Laboratory» WBC 15,600 Hgb 8.4 HCt 23%, Plts 95000,
Purist? or Pragmatist? Assessment & Management of ICU Volume Status
 Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis
 How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis") Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Renal physiology D.HAMMOUDI.MD
 Renal physiology D.HAMMOUDI.MD Functions Regulating blood ionic composition Regulating blood ph Regulating blood volume Regulating blood pressure Produce calcitrol and erythropoietin Regulating blood glucose
Renal physiology D.HAMMOUDI.MD Functions Regulating blood ionic composition Regulating blood ph Regulating blood volume Regulating blood pressure Produce calcitrol and erythropoietin Regulating blood glucose
The History & Practice of IV Fluid Therapy have we advanced in 185 years?
 The History & Practice of IV Fluid Therapy have we advanced in 185 years? Liam Plant Clinical Professor of Renal Medicine University College Cork Consultant Renal Physician Cork University Hospital National
The History & Practice of IV Fluid Therapy have we advanced in 185 years? Liam Plant Clinical Professor of Renal Medicine University College Cork Consultant Renal Physician Cork University Hospital National
When and how to start RRT in critically ill patients? Intensive Care Training Program Radboud University Medical Centre Nijmegen
 When and how to start RRT in critically ill patients? Intensive Care Training Program Radboud University Medical Centre Nijmegen Case history (1) 64 Hypertension 2004 AVR 2009 Paravalvular leak - dilated
When and how to start RRT in critically ill patients? Intensive Care Training Program Radboud University Medical Centre Nijmegen Case history (1) 64 Hypertension 2004 AVR 2009 Paravalvular leak - dilated
Fluids: occult effects. S Magder Department of Critical Care, McGill University Health Centre
 Fluids: occult effects S Magder Department of Critical Care, McGill University Health Centre Why is volume important? 1. Water is essential to dissolve substances and allow them to diffuse 2. Necessary
Fluids: occult effects S Magder Department of Critical Care, McGill University Health Centre Why is volume important? 1. Water is essential to dissolve substances and allow them to diffuse 2. Necessary
Fluid and electrolyte therapies including nutritional support are markedly developing in medicine
 J Korean Med Assoc 2010 December; 53(12): 1103-1112 DOI: 10.5124/jkma.2010.53.12.1103 pissn: 1975-8456 eissn: 2093-5951 http://jkma.org Continuing Education Column Fluid therapy: classification and characteristics
J Korean Med Assoc 2010 December; 53(12): 1103-1112 DOI: 10.5124/jkma.2010.53.12.1103 pissn: 1975-8456 eissn: 2093-5951 http://jkma.org Continuing Education Column Fluid therapy: classification and characteristics
Introduction to the kidney: regulation of sodium & glucose. Dr Nick Ashton Senior Lecturer in Renal Physiology Faculty of Biology, Medicine & Health
 Introduction to the kidney: regulation of sodium & glucose Dr Nick Ashton Senior Lecturer in Renal Physiology Faculty of Biology, Medicine & Health Objectives Overview of kidney structure & function Glomerular
Introduction to the kidney: regulation of sodium & glucose Dr Nick Ashton Senior Lecturer in Renal Physiology Faculty of Biology, Medicine & Health Objectives Overview of kidney structure & function Glomerular
Dr. Carlos Fernando Estrada Garzona. Departamento de Farmacología Universidad de Costa Rica
 Dr. Carlos Fernando Estrada Garzona Departamento de Farmacología Universidad de Costa Rica OBJETIVOS FISIOLOGIA LIQUIDOS CORPORALES SOLUCIONES PARENTERALES PRINCIPIOS DE FLUIDOTERAPIA CRISTALOIDE VS COLOIDE
Dr. Carlos Fernando Estrada Garzona Departamento de Farmacología Universidad de Costa Rica OBJETIVOS FISIOLOGIA LIQUIDOS CORPORALES SOLUCIONES PARENTERALES PRINCIPIOS DE FLUIDOTERAPIA CRISTALOIDE VS COLOIDE
Fluids and electrolytes
 Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
1. What is the acid-base disturbance in this patient?
 /ABG QUIZ QUIZ 1. What is the acid-base disturbance in this patient? Presenting complaint: pneumonia 1 point Uncompensated metabolic alkalosis Partially compensated respiratory alkalosis Mixed alkalosis
/ABG QUIZ QUIZ 1. What is the acid-base disturbance in this patient? Presenting complaint: pneumonia 1 point Uncompensated metabolic alkalosis Partially compensated respiratory alkalosis Mixed alkalosis