SAHA PCI or CABG for Left Main and Multi-Vessel Disease: when I would definitely/ maybe/never refer my patient for PCI or CABG
|
|
|
- Terence Alexander
- 5 years ago
- Views:
Transcription
1 SAHA 2017 PCI or CABG for Left Main and Multi-Vessel Disease: when I would definitely/ maybe/never refer my patient for PCI or CABG David P Taggart MD PhD FRCS FESC Professor of Cardiovascular Surgery, University of Oxford Conflicts of Interest: (i) Clinical: Cardiac Surgeon (ii) Commercial: Consultant to Medistim, Medtronic, VGS, Somahlution, Stryker) (iii) One of 25 ESC/EACTS Guidelines Writers on Myocardial Revascularization (iv) Chairman of Surgical Committee of the EXCEL trial
2 50 Years Ago: First report of SYSTEMATIC use of SV grafts for CABG ATS [Dec ] 40 Years Ago: Gruentzig reports first PTCA (AHA 1977)
3 PCI or CABG for Left Main and Multi-Vessel Disease: when I would definitely/ maybe/never refer my patient for PCI or CABG (stable or urgent patients but NOT STEMI who should get PCI) UK Most interventions are RECOMMENDED by a HEART TEAM based on 1 ESC/EACTS Guidelines (Evidence Based) 2 Potential contra-indications to the recommended intervention? 3 Patient Preferences ( what is the best treatment for me? )
4 Complex CAD should be discussed by Heart Team IC 79% 66%
5 Mutlivessel Disease (No Left main)

; p < 0.")
6 6054 patients: HR CABG vs PCI 0.73 ( ); p < JAMA 2013
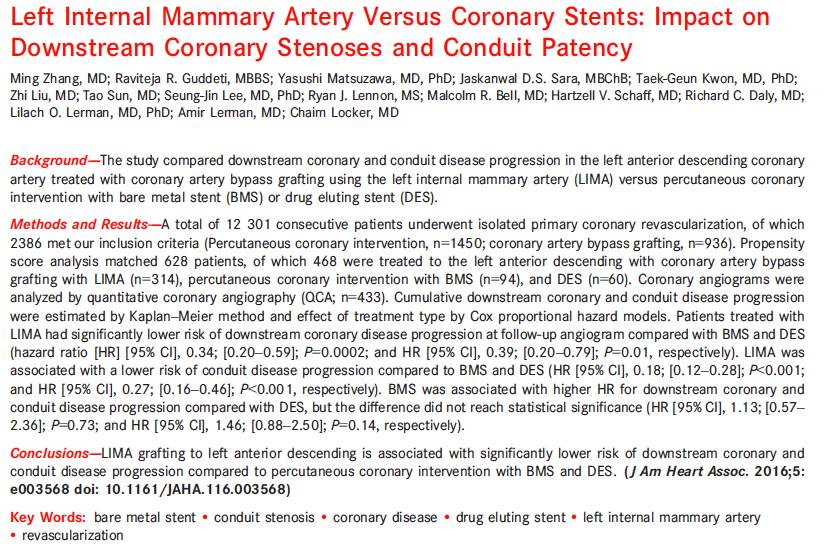
![6054 patients RR CABG vs DES for MI,RR,CVA [Siphai et al JAMA 2013] MI: RR 0.58 (0.](/docs-images/82/85492111/images/7-1.jpg "48-0.72) p<0.001 Revasc: RR 0.29 (0.21-0.41) p<0.001 Stroke: RR 1.36 (0.99-1.86) p=0.")


7 6054 patients RR CABG vs DES for MI,RR,CVA [Siphai et al JAMA 2013] MI: RR 0.58 ( ) p<0.001 Revasc: RR 0.29 ( ) p<0.001 Stroke: RR 1.36 ( ) p=0.06 CONCLUSIONS AND RELEVANCE: In patients with multivessel coronary disease, compared with PCI, CABG leads to an unequivocal reduction in long-term mortality and myocardial infarctions and to reductions in repeat revascularizations, regardless of whether patients are diabetic or not. These findings have implications for management of such patients.
![[IJC 2016] 5 RCTS 4563 patients Survival with CABG continues to increase past 5 years with](/docs-images/82/85492111/images/8-1.jpg "diverging survival curves CABG results could be even better with more arterial grafts and OMT")
8 [IJC 2016] 5 RCTS 4563 patients Survival with CABG continues to increase past 5 years with diverging survival curves CABG results could be even better with more arterial grafts and OMT 0.9%
9 SYNTAX RCT (5 Years): 3 Vessel Disease [EHJ 2013] PCI CABG nos Death (-5.4%).006 Low <23 nos DEATH (0.9%) CVA MI Cardiac Death (-5.2%).001 MI (-7.3%) < % D+C+M Revasc CVA (+0.6%).66 nos D+C+M (-8%) <.001 Revasc (-12.8%) <.001 (i) Consistent with PM registry data > 10 years (ii) Similar rate of stroke in PCI/CABG Int % DEATH (7%) CVA MI D+C+M Revasc nos Survival: Accelerating Divergence at 5 years High >32 DEATH (9%) CVA MI D+C+M Revasc



10 Accelerating Divergence of Survival benefit for CABG [JACC 2016]
11 FREEDOM 1900 patients MVD in DM NEJM % 5.4%

12 Comparison of coronary artery bypass surgery and percutaneous coronary intervention in patients with diabetes: a meta-analysis of randomised controlled trials [Lancet Diabetes Endocrinol 2013] Verma S et al: [LANCET DIABETES and ENDOCRINOLOGY 2013] 8 trials with 3612 patients

13 Patency of RIMA to 20 years [Tatoulis et al Curr Op Cardiol 2011]
14 Left Main
 o<90% have multivessel CAD (CABG already offers")
15 o<90% of LMS are distal/bifurcation (very high risk of restenosis) o<90% have multivessel CAD (CABG already offers survival benefit)
16 Similar outcomes at 3 years for Death, and Composite Death/MI/Stroke but Much Greater Need for Target Vessel Revascularization with Stents MAIN-COMPARE Registry of UPLM disease in 2240 Patients: 1102 stents and 1138 CABG followed for 3 years BMS DES
17 o Competitive flow in CABG if low SYNTAX scores ie less proximal CAD o Accelerating Divergence of Survival Curves in Favour of CABG in >32 o Used to define patients in the EXCEL trial (Syntax Scores <33) SYNTAX LEFT MAIN Left SYNTAX Maintrial 705 RCT patients CIRC 5 years 2014 CIRC 2014
18 CAUTION: ONLY 3 YEARS FOLLOW-UP!!!! LM: SYNTAX < RCT patients 1000 Registry Patients NEJM 2016 At 5 years? No Difference in Stroke
![EXCEL: The Money Shot From randomization to 30 days From 30 days to 3 years PCI (n=948) CABG (n=957) HR [95%CI] P value PCI (n=939) CABG (n=947) HR [95%CI] P value Death, stroke or MI 4.9% 7.9% 0.](/docs-images/82/85492111/images/19-0.jpg "61 [0.42, 0.88] 0.008 11.5% 7.9% 1.44 [1.06, 1.96] 0.02 - Death 1.0% 1.1% 0.90 [0.37, 2.22] 0.82 7.3% 4.9% 1.44 [0.98, 2.13] 0.06 - Stroke 0.6% 1.3% 0.50 [0.19, 1.33] 0.15 1.8% 1.8% 1.00 [0.49, 2.")
19 EXCEL: The Money Shot From randomization to 30 days From 30 days to 3 years PCI (n=948) CABG (n=957) HR [95%CI] P value PCI (n=939) CABG (n=947) HR [95%CI] P value Death, stroke or MI 4.9% 7.9% 0.61 [0.42, 0.88] % 7.9% 1.44 [1.06, 1.96] Death 1.0% 1.1% 0.90 [0.37, 2.22] % 4.9% 1.44 [0.98, 2.13] Stroke 0.6% 1.3% 0.50 [0.19, 1.33] % 1.8% 1.00 [0.49, 2.05] MI 3.9% 6.2% 0.63 [0.42, 0.95] % 2.5% 1.71 [1.00, 2.93] 0.05 By 3 years CABG mortality 2.3% lower (p=0.06) BUT WITH DIVERGING SURVIVAL CURVES and NO increased risk of stroke
20 LM: 1201 RCT patients No Registry Patients Lancet 2016 Mortality 12% 9% MI 7% 2% REVASC 16% 10% STROK E 5% 2%
 Over the long term offers prophylaxis against FUTURE proximal culprit lesions In contrast, PCI only treats SUITABLE localised proximal culprit")
![lesions but has NO PROPHYLACTIC BENEFIT against new proximal disease 2 IMA elutes NO into coronary circulation reducing risk of further disease [CIRC 2007] impairs re-endothelialization, downstream](/docs-images/82/85492111/images/21-3.jpg "endothelial function and creates pro-thrombotic milieu 3 PCI means incomplete revascularization (Hannan Circ 2006) Of 22,000 PCI 69% had incomplete revascularization >2 vessels (+/- CTO) HR for")
21 1 3 REASONS WHY CABG HAS A SURVIVAL BENEFIT OVER PCI Anatomically, atheroma is mainly located in the proximal coronary arteries Placing bypass grafts to the MID CORONARY VESSEL has TWO effects (i) Complexity of proximal CULPRIT lesion is irrelevant (ii) Over the long term offers prophylaxis against FUTURE proximal culprit lesions In contrast, PCI only treats SUITABLE localised proximal culprit lesions but has NO PROPHYLACTIC BENEFIT against new proximal disease 2 IMA elutes NO into coronary circulation reducing risk of further disease [CIRC 2007] impairs re-endothelialization, downstream endothelial function and creates pro-thrombotic milieu 3 PCI means incomplete revascularization (Hannan Circ 2006) Of 22,000 PCI 69% had incomplete revascularization >2 vessels (+/- CTO) HR for mortality 1.4 (95% CI = ) Residual SYNTAX score >8 increases mortality and MACCE (Farooq, Serruys CIRC 2013) PCI will never match the results of CABG for LM/MVD (POBA;BMS;DES)

22 Ratio Elective PCI:CABG per 100,000 population in 24 OECD countries? USA 4 x difference in European states with similar populations and economies
![[CMAJ 2012] 17 cardiac centres in Ontario,CA 5 x difference in PCI:CABG ratio 4% of patients discussed at MDT (96% NOT) INTERPRETATION The physician performing the diagnostic catheterization and the](/docs-images/82/85492111/images/23-1.jpg "treating hospital were strong independent predictors of the mode of revascularization.")
23 [CMAJ 2012] 17 cardiac centres in Ontario,CA 5 x difference in PCI:CABG ratio 4% of patients discussed at MDT (96% NOT) INTERPRETATION The physician performing the diagnostic catheterization and the treating hospital were strong independent predictors of the mode of revascularization. Opportunities exist to improve transparency and consistency around the decision-making process for coronary revascularization, most notably among patients with non-emergent multivessel disease.
![WHY RECOMMENDATIONS for INTERVENTION SHOULD BE BY HEART TEAM [BMJ 2014] Only 1% said](/docs-images/82/85492111/images/24-1.jpg "for symptoms only Only 1% correctly identified that ELECTIVE PCI was for symptoms")
24 WHY RECOMMENDATIONS for INTERVENTION SHOULD BE BY HEART TEAM [BMJ 2014] Only 1% said for symptoms only Only 1% correctly identified that ELECTIVE PCI was for symptoms only
: ESC Guidelines")
25 Multi-Vessel Disease (No Left Main): ESC Guidelines 2013

26 Left Main: ESC Guidelines 2013

27 AR Gruentzig (NEJM 1979) We estimate that only about 10 to 15 per cent of candidates for bypass surgery have lesions suitable for this procedure (PCI). A prospective randomized trial will be necessary to evaluate its usefulness in comparison with surgical and medical management. Opie LH, Commerford PJ, Gersh BJ Lancet 2006; 367:69-78

28 Complex CAD should be discussed by Heart Team IC 66% 79% CABG would be even better with more arterial grafts and greater use of OMT

29 200 patient with stable angina and significant stenoses >80% and FFR <0.7 RCT of PCI vs sham invasive procedure At 6 weeks no difference in exercise test nor frequency or severity of angina
30 Summary and Conclusions: PCI vs CABG % of patients with 3 vessel CAD (SYNTAX >22) and 66% with LM (SYNTAX >32) have strong survival advantage with CABG (reduced MI and repeat revasc) by 3 years and continuing to increase past 5 years CABG is superior to PCI despite inferior OMT and 80% of all grafts being vein grafts (would be even better with widespread use of arterial grafts) In 21% of patients with 3VD (SYNTAX scores <23) and 34% with LM (SYNTAX scores <33), similar 5 year survival between CABG and PCI but less repeat revasc with CABG In contemporary trials CABG causes a non significant increase in stroke with 3VD and LM Consistent unwarranted variation in ratios of PCI:CABG between countries and within countries ABSENCE of Heart Team (using approved guidelines) results both in most elective PCI patients failing to understand its rationale and also a large number of inappropriate or wrong PCI interventions Guidelines are transparent and protect the patients (from receiving wrong interventions) and doctors (from administering wrong interventions) and should be mandatory Professional bodies should persuade statutory bodies/payers that they only reimburse interventions which are approved by the Heart Team based on official guidelines (or clear documentation why guidelines were not followed).
31 Interpreting Efficacy of PCI vs CABG: 3Key Questions 1. Are most trial patients typical of routine practice?: NO (except SYNTAX) 2. What is the duration of follow-up? USUALLY < 5 YEARS (ie Interim Analysis): few exceptions 3. Use of OPTIMAL (Guideline Based) medical therapy? CABG substantially inferior to PCI

32 Ann Thorac Surg 2006;82: [ALL REPORTED PCI EQUAL TO CABG for SURVIVAL]
33 Survival benefit of CABG increases with time (< 5 yr follow-up is interim analyses) SYNTAX 1,095 pts: EHJ 2013 FREEDOM 1,900 pts: NEJM % 5.4% ASCERT 189,793 pts: NEJM % 4.4% NY Registry 16,242 pts: ATS 2013 ACCELERATING DIVERGENCE OF SURVIVAL CURVES BEYOND 5 YEARS!!!
34 [NEJM 2016] N= % of OMT X to CABG 7.2% 8.8%
35 50 Years Ago: First report of SYSTEMATIC use of SV grafts for CABG ATS [Dec ] 1986: Loop et al SYSTEMATIC Use of ITA graft 1999: Lytle et al SYSTEMATIC Use of two ITA grafts 40 Years Ago: Gruentzig reports first PTCA (AHA 1977)

36
 >30 years CABG remains one of the most commonly performed major operations (in")
37 1. Are RCT patients typical of routine patients? CABG first systematically performed in 1967 and PCI in 1977 Trials of coronary revascularization by CABG or stents (PCI) >30 years CABG remains one of the most commonly performed major operations (in 2016 worldwide > 1 million CABG) No other surgical operation has ever been subjected to the same scientific scrutiny as CABG Effect of coronary artery bypass graft surgery on survival: overview of 10-year results from randomised trials by the Coronary Artery Bypass Graft Surgery Trialists Collaboration* [Lancet 1994] 1 2 Summary CABG: BETTER if 2 or 3 vessel CAD involving proximal LAD CABG: NO benefit for 1 or 2 VD NOT involving proximal LAD We carried out a systematic overview using individual patient data from the seven randomised trials that have compared a strategy of initial coronary artery bypass graft (CABG) surgery mortality in patients with stable coronary heart disease (stable angina not severe enough to necessitate surgery on grounds of alone, or infarction). prognostically important clinical and angiographic risk factors were integrated to stratify patients by risk levels and the extension of survival at 10 years was examined (change in survival [SE 3 1] months in low-risk group, 5 0 [4 2] months in moderate-risk group, and 8 8 [5 4] months in high-risk group; p for trend <0 003). A strategy of initial CABG surgery is associated with lower mortality than one of medical management with delayed with Could one of this initial medical information therapy to assess be the used effects onto design a trial to show that PCI is as effective as CABG?
38 CIRC 2015 Substantially inferior OMT in CABG group mortality and MACCE
39 Q: Could industry (who want to sell stents) design an RCT to prove that stents are equal to CABG Original population:100% Angiographic proven multivessel CAD Original population:24 % Angiographic Criteria Original population:6% Cardiologist/Surgeon Agree riginal population:4% Randomized patients (1 or 2 VD + good LV) EXCLUDE 76% (outcome known to be better with CABG: severe 3VD, LM, occluded vessels, poor LV) EXCLUDE 18% (CABG can treat all lesions but stents cannot) EXCLUDE 2% (Patients Refuse Participation) (i) Can now Confidently Predict: No difference in survival (Yusuf 1994) (ii) Generalize results in publications: All patients with coronary disease (iii) Organize Sympathetic Editorials Ignore major flaws/limitations of RCT (iv) Use Trials to Underpin Guidelines
40 Surely this could not REALLY happen: ESPECIALLY in such a prestigious field of medicine dominated by EBM and RCTs (led by distinguished and famous investigators)?
41 [ATS 2006] Society ACC/AHA Circulation 2006 ESC Eur Heart J 2005 BCS Heart 2005 Summary of Guidelines Recommendations for stents vs CABG based on 15 RCTs Patients with 2 or 3 vessel disease who are otherwise eligible for CABG including diabetes NO SURGICAL OPINION RECOMMENDED all patients except diabetics with multivessel disease, unprotected left main, CTO NO SURGICAL OPINION RECOMMENDED patients to be fully informed in decisions, treatment options (GMC Good Medical Practice) NO SURGICAL OPINION RECOMMENDED almost all patients can be treated by PCI NONE RECOMMEND SURGICAL OPINION Written by 23 cardiologists 1 surgeon 46 cardiologists 0 surgeon 8 cardiologists 1 surgeon 77 cardiologists 2 surgeons surgical societies should no longer provide a token surgeon on cardiology guidelines as they are hopelessly outgunned and ineffectual against what are, in effect, exclusive cardiology dictates. If surgical opinion is genuinely to be heard, there must be comparable numbers of surgeons on writing committees
42 Taggart DP. Lancet 2009; 373: Most significantly, the randomized trials only enrolled around 5%-10% of the eligible population, the majority of whom had single or double vessel disease and normal left ventricular function [2], a group in whom it was already well established that there was no prognostic benefit of CABG [3]. By largely excluding patients with a known survival benefit from CABG (left main+/- triple vessel coronary artery disease and especially with impaired ventricular function [3]), the trials ignored the prognostic benefit of surgery in more complex coronary artery disease. Nevertheless, the inappropriate generalization of the trial results from their highly select populations to most patients with multivessel disease has been ubiquitous in the literature and has, at least in part, justified the explosive growth in PCI in developed countries. [2] Taggart DP. Thomas B. Ferguson Lecture. Coronary artery bypass grafting is still the best treatment for multivessel and left main disease, but patients need to know. Ann Thorac Surg 2006;82: [3] Yusuf S, et al. Effect of coronary artery bypass graft surgery on survival: overview of 10-year results from randomised trials by the Coronary Artery Bypass Graft Surgery Trialists Collaboration. Lancet 1994 ;344:
43 [2016] Primary outcome is 10-year survival (in 2018)
44 15,583 patients followed for a mean of >9 years [CIRC 2014]
45 Has the difference in mortality between percutaneous coronary intervention and coronary artery bypass grafting in people with heart disease and diabetes changed over the years? A systematic review and meta-regression Peter Herbison, Cheuk-Kit Wong [BMJ 2015] In DM even with 3 rd generation stents CABG still has strong survival
46 Left Main (+/- Mutlivessel Disease)
47 [JACC Cardiovasc Intervention 2013] 24 studies (3 RCT) with 14,203 patients followed to 5 years DEATH (5 yr): No Difference MI: ( 1-3yrs) TVR: ( 1-5 yr) CVA: ( 1-5yr) 1 yr: 0.8% vs 2.8% 5 yr:1.7% vs 4.7% (Δ 0.9% vs 1.9%):? OMT Different from 3VD where CABG death, MI, RR and NS for CVA
48 LM: CABG BEST ONLY FOR HIGH TERCILES (>32) DEATH MI MACCE TVR

49 LEFT MAIN SYNTAX trial 705 RCT patients 5 years CIRC 2014 Different from 3VD!!
50 Politics of PCI vs CABG BMJ 2005 The current tendency of some cardiologists to exclusively investigate and treat patients with severe multivessel disease without a surgical opinion not only belittles the traditional multidisciplinary approach but ensures that the best and most balanced advice is unlikely to be consistently offered. Most importantly, by effectively denying patients the opportunity of making a fully informed choice, it falls far short of best practice.
 for")
51 Current evidence for PCI and CABG in multi-vessel and left main Documented unwarranted variations in ratio of PCI and CABG Documented inappropriate use of investigations and interventions Documented poor patient understanding of the rationale(s) for treatment
52 [EJCTS 2014] 13 x difference for lowest (0.36) and highest (4.74) although only 40 miles apart!!
53 JAMA Int Med ,225,562 angiograms: 25% ASYMPTOMATIC (range 1%-76%)
54 Adherence of Catheterization Laboratory Cardiologists to ACC/AHA Guidelines for PCI and CABG: What happens in Actual Practice? [Hannan et al Circ 2010] o16142 catheter lab patients in New York otreatment decision made by catheter lab cardiologist alone in 64% ACC/AHA Recommendation Numbers % CABG % PCI % Medical None CABG PCI <1 CABG or PCI <1 Neither Total <1 o92% of PCI procedures ad hoc (ie no time for real choice/ genuine consent) ochance of PCI increased in hospitals with PCI facilities
55 JAMA Int Med 2014 In taped interviews benefits of PCI were accurate in 5% BUT overstated in 48% [explicitly (13%) or implicitly (35%)]
56 PCI vs CABG in 2017 THREE KEY AREAS TO ADDRESS 1. EFFICACY of PCI vs CABG: Four important issues (i) Are RCT patients typical of routine practice? (ii) Duration of follow-up? (iii) SYNTAX scores? ie severity of CAD (iv) Use of OPTIMAL (guideline based) medical therapy? 2. EVIDENCE BASIS for PCI and CABG in Multivessel and Left MainDisease 3. POLITICS of PCI vs CABG (Rationale for the Heart Team)
57
58 Relative Efficacy of PCI and CABG: 4 Questions 1.Are patients enrolled in RCTs typical of routine practice? USUALLY NO. With the single exception of the all-comer SYNTAX trial, 19 other RCTs of PCI vs CABG enrolled <10% of the eligible population ie those with low severity CAD (but then generalized the results to the whole population) 2. What is the duration of follow-up? SHOULD BE AT LEAST 5 YEARS. The benefits of CABG (improved survival, reduced MI and repeat revascularization) continue to increase with time (< 5yr follow up is only an interim analyses) 3. What are the SYNTAX scores of the study population? NO SYNTAX SCORE = NO IDEA OF SEVERITY OF CAD Cannot recommend best treatment 4. Did CABG patients in RCTs receive Optimal Medical Therapy? USUALLY NO. In most trials CABG patients received substantially inferior guideline based medical therapy (OMT) leading to increased mortality and MACCE


59

60

61 ojoint Cardiology (ESC) and Cardiac Surgery (EACTS) o25 members from 13 European countries 9 non interventional cardiologists, 8 interventional cardiologists, 8 cardiac surgeons Reflects the Heart Team!!! oextensively reviewed by external referees before publication


62 14 chapters 270 references
63 Increased EDRFs (especially NO) produced by IMA results (i) in superior graft patency (ii) protects native coronary artery circulation % progression of native CAD IMA SVG Kitamura (1987) Loop (1996) Manninen (1998) Hamada (2001) Borges (2010) AVERAGE CIRC 2007 impairs re-endothelialization, creates pro-thrombotic environment impairs distal endothelial function


64 James McGill Glasgow University 1756 Sir William Osler Regius Professor of Medicine Oxford
![[ATS 2009] 1899-1984](/docs-images/82/85492111/images/65-1.jpg "Scottish forefathers!")
65 [ATS 2009] Scottish forefathers!!
66 MAIN-COMPARE Registry of UPLM disease in 1102 stents and 1138 CABG BMS DES there was a trend toward higher rates of death and the composite end point in the group that received DES
67 SYNTAX 5 years 1095 RCT patients EHJ %


68 JAHA 2013 Death DEATH CARDIAC Cardiac DEATH Death REVASC
CABG vs PCI: What do the Guidelines Say?
 AATS International Cardiovascular Symposium: Sao Paolo 2017 CABG vs PCI: What do the Guidelines Say? David P Taggart MD PhD FRCS FESC Professor of Cardiovascular Surgery, University of Oxford Conflicts
AATS International Cardiovascular Symposium: Sao Paolo 2017 CABG vs PCI: What do the Guidelines Say? David P Taggart MD PhD FRCS FESC Professor of Cardiovascular Surgery, University of Oxford Conflicts
Southern Thoracic Surgical Association CABG in 2012: Implications of the New ESC/EACTS Guidelines
 Southern Thoracic Surgical Association 2011 CABG in 2012: Implications of the New ESC/EACTS Guidelines David P Taggart MD PhD FRCS Professor of Cardiovascular Surgery, University of Oxford Conflicts of
Southern Thoracic Surgical Association 2011 CABG in 2012: Implications of the New ESC/EACTS Guidelines David P Taggart MD PhD FRCS Professor of Cardiovascular Surgery, University of Oxford Conflicts of
Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011
 Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011 Prof. Dr. Volkmar Falk Klinik für Herz- und Gefäßchirurgie, Universitätsspital Zürich, Schweiz In 2004 headlines were
Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011 Prof. Dr. Volkmar Falk Klinik für Herz- und Gefäßchirurgie, Universitätsspital Zürich, Schweiz In 2004 headlines were
What do the guidelines say?
 Percutaneous coronary intervention in 3-vessel disease and main stem What do the guidelines say? Nothing to disclose Dariusz Dudek Institute of Cardiology, Jagiellonian University Krakow, Poland The European
Percutaneous coronary intervention in 3-vessel disease and main stem What do the guidelines say? Nothing to disclose Dariusz Dudek Institute of Cardiology, Jagiellonian University Krakow, Poland The European
Surgery Grand Rounds
 Surgery Grand Rounds Coronary Artery Bypass Grafting versus Coronary Artery Stenting Charles Ted Lord, R1 Coronary Artery Disease Stenosis of epicardial vessels Metabolic & hematologic Statistics 500,000
Surgery Grand Rounds Coronary Artery Bypass Grafting versus Coronary Artery Stenting Charles Ted Lord, R1 Coronary Artery Disease Stenosis of epicardial vessels Metabolic & hematologic Statistics 500,000
Controversies in Cardiac Surgery
 Controversies in Cardiac Surgery 3 years after SYNTAX : Percutaneous Coronary Intervention for Multivessel / Left main stem Coronary artery disease Pro ESC Congress 2010, 28 August 1 September Stockholm
Controversies in Cardiac Surgery 3 years after SYNTAX : Percutaneous Coronary Intervention for Multivessel / Left main stem Coronary artery disease Pro ESC Congress 2010, 28 August 1 September Stockholm
Assessing Myocardium at Risk: Applying SYNTAX
 Assessing Myocardium at Risk: Applying SYNTAX Farouc Jaffer MD PhD FSCAI FACC FAHA Associate Professor of Medicine, Harvard Medical School Director, CAD Program and Chronic Total Occlusion PCI Program
Assessing Myocardium at Risk: Applying SYNTAX Farouc Jaffer MD PhD FSCAI FACC FAHA Associate Professor of Medicine, Harvard Medical School Director, CAD Program and Chronic Total Occlusion PCI Program
Left Main Intervention: Where are we in 2015?
 Left Main Intervention: Where are we in 2015? David A. Cox, MD FSCAI Director, Cardiology Research Associate Director, Cardiac Cath Lab Lehigh Valley Health Network Allentown, PA Fall Fellows Course Laa
Left Main Intervention: Where are we in 2015? David A. Cox, MD FSCAI Director, Cardiology Research Associate Director, Cardiac Cath Lab Lehigh Valley Health Network Allentown, PA Fall Fellows Course Laa
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO!
 Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Management of cardiovascular disease - coronary interventions -
 Master Classes in Preventive Cardiology I Management of diabetes in patients with CVD European Heart House Management of cardiovascular disease - coronary interventions - Francesco Cosentino MD, PhD, FESC
Master Classes in Preventive Cardiology I Management of diabetes in patients with CVD European Heart House Management of cardiovascular disease - coronary interventions - Francesco Cosentino MD, PhD, FESC
Multivessel Coronary Artery Disease : CABG. Zürich, F. Siclari MD
 Multivessel Coronary Artery Disease : CABG Zürich, 10.06.2015 F. Siclari MD Coronary Artery Ruptured Plaque Pathological process with definite subsequent vascular changes most of them irreversible CABG
Multivessel Coronary Artery Disease : CABG Zürich, 10.06.2015 F. Siclari MD Coronary Artery Ruptured Plaque Pathological process with definite subsequent vascular changes most of them irreversible CABG
EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017
 EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017 Igor F. Palacios, MD Director of Interventional Cardiology Professor of Medicine Massachusetts
EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017 Igor F. Palacios, MD Director of Interventional Cardiology Professor of Medicine Massachusetts
ΑΓΓΕΙΟΠΛΑΣΤΙΚΗ ΣΤΟ ΔΙΑΒΗΤΙΚΟ ΑΣΘΕΝΗ
 ΑΓΓΕΙΟΠΛΑΣΤΙΚΗ ΣΤΟ ΔΙΑΒΗΤΙΚΟ ΑΣΘΕΝΗ Νίκος Μεζίλης MD, FESC Κλινική Άγιος Λουκάς Why diabetes is associated with restenosis endothelial dysfunction metabolic alterations accelerated platelet deposition
ΑΓΓΕΙΟΠΛΑΣΤΙΚΗ ΣΤΟ ΔΙΑΒΗΤΙΚΟ ΑΣΘΕΝΗ Νίκος Μεζίλης MD, FESC Κλινική Άγιος Λουκάς Why diabetes is associated with restenosis endothelial dysfunction metabolic alterations accelerated platelet deposition
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital
 VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
PCI vs. CABG From BARI to Syntax, Is The Game Over?
 PCI vs. CABG From BARI to Syntax, Is The Game Over? Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea PCI vs CABG Multi-Vessel Disease
PCI vs. CABG From BARI to Syntax, Is The Game Over? Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea PCI vs CABG Multi-Vessel Disease
When should we indisputably perform CABG? Quand faut-il indiscutablement opérer? Dr Hakim BENAMER
 When should we indisputably perform CABG? Quand faut-il indiscutablement opérer? Dr Hakim BENAMER ICPS, Massy ICV-GVM La Roseraie, Aubervilliers Hôpital FOCH, Suresnes Disclosure Statement of Financial
When should we indisputably perform CABG? Quand faut-il indiscutablement opérer? Dr Hakim BENAMER ICPS, Massy ICV-GVM La Roseraie, Aubervilliers Hôpital FOCH, Suresnes Disclosure Statement of Financial
PCI for Left Main Coronary Artery Stenosis. Jean Fajadet Clinique Pasteur, Toulouse, France
 PCI for Left Main Coronary Artery Stenosis Jean Fajadet Clinique Pasteur, Toulouse, France Athens, October 19, 2018 Left Main Coronary Artery Disease Significant unprotected left main coronary artery disease
PCI for Left Main Coronary Artery Stenosis Jean Fajadet Clinique Pasteur, Toulouse, France Athens, October 19, 2018 Left Main Coronary Artery Disease Significant unprotected left main coronary artery disease
Left Main Intervention: Will it become standard of care?
 Left Main Intervention: Will it become standard of care? David Cox, MD FSCAI, FACC Director, Interventional Cardiology Research Associate Director, Cardiac Cath Lab Lehigh Valley Health Network Allentown,
Left Main Intervention: Will it become standard of care? David Cox, MD FSCAI, FACC Director, Interventional Cardiology Research Associate Director, Cardiac Cath Lab Lehigh Valley Health Network Allentown,
Adecade ago, many cardiac surgeons believed
 CABG for Multivessel CAD Recent studies show that CABG is still preferred over PCI for most patients. BY SUBHASIS CHATTERJEE, MD; JOHN C. ALEXANDER, MD; AND PAUL J. PEARSON, MD, PHD Adecade ago, many cardiac
CABG for Multivessel CAD Recent studies show that CABG is still preferred over PCI for most patients. BY SUBHASIS CHATTERJEE, MD; JOHN C. ALEXANDER, MD; AND PAUL J. PEARSON, MD, PHD Adecade ago, many cardiac
FFR and CABG Emanuele Barbato, MD, PhD, FESC Cardiovascular Center Aalst, Belgium
 FFR and CABG Emanuele Barbato, MD, PhD, FESC Cardiovascular Center Aalst, Belgium Conflict of Interest Institutional research grants and speaker s fee from St. Jude Medical and Boston Scientic to Cardiovascular
FFR and CABG Emanuele Barbato, MD, PhD, FESC Cardiovascular Center Aalst, Belgium Conflict of Interest Institutional research grants and speaker s fee from St. Jude Medical and Boston Scientic to Cardiovascular
Implications of SYNTAX for CABG in 2010: Practice and Politics
 AATS 2010 Implications of SYNTAX for CABG in 2010: Practice and Politics David P Taggart MD PhD FRCS Professor Cardiovascular Surgery, University of Oxford Conflicts of Interest: (i) Clinical: Cardiac
AATS 2010 Implications of SYNTAX for CABG in 2010: Practice and Politics David P Taggart MD PhD FRCS Professor Cardiovascular Surgery, University of Oxford Conflicts of Interest: (i) Clinical: Cardiac
Controversies in Coronary Revascularization. Atlanta CCU April 15, 2016
 Controversies in Coronary Revascularization Atlanta CCU April 15, 2016 Habib Samady MD FACC FSCAI Professor of Medicine Director, Interventional Cardiology, Emory University Director, Cardiac Catheterization
Controversies in Coronary Revascularization Atlanta CCU April 15, 2016 Habib Samady MD FACC FSCAI Professor of Medicine Director, Interventional Cardiology, Emory University Director, Cardiac Catheterization
TCTAP When is Surgery the Preferred Therapy? David P Taggart MD PhD FRCS Professor Cardiovascular Surgery, University of Oxford
 TCTAP 2010 When is Surgery the Preferred Therapy? David P Taggart MD PhD FRCS Professor Cardiovascular Surgery, University of Oxford Conflicts of Interest: (i) Clinical: Cardiac Surgeon (ii) Political:
TCTAP 2010 When is Surgery the Preferred Therapy? David P Taggart MD PhD FRCS Professor Cardiovascular Surgery, University of Oxford Conflicts of Interest: (i) Clinical: Cardiac Surgeon (ii) Political:
Δημήτριος Αγγοσράς, FETCS
 ΣΕΜΙΝΑΡΙΟ ΟΜΑΔΩΝ ΕΡΓΑΣΙΑΣ Δημήτριος Αγγοσράς, FETCS Επίκοσρος Καθηγηηής Καρδιοτειροσργικής Ιαηρική Πανεπιζηημίοσ Αθηνών Πανεπιζηημιακό Γενικό Νοζοκομείο Αηηικόν Randomized Controlled Trials (RCTs) Why
ΣΕΜΙΝΑΡΙΟ ΟΜΑΔΩΝ ΕΡΓΑΣΙΑΣ Δημήτριος Αγγοσράς, FETCS Επίκοσρος Καθηγηηής Καρδιοτειροσργικής Ιαηρική Πανεπιζηημίοσ Αθηνών Πανεπιζηημιακό Γενικό Νοζοκομείο Αηηικόν Randomized Controlled Trials (RCTs) Why
Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome
 Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome Chris C. Cook, MD Associate Professor of Surgery Director, CT Residency Program, WVU ACOI 10/17/18 No Disclosures
Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome Chris C. Cook, MD Associate Professor of Surgery Director, CT Residency Program, WVU ACOI 10/17/18 No Disclosures
Optimal Conduit Strategy in 2017
 SAHA 2017 Optimal Conduit Strategy in 2017 David P Taggart MD PhD FRCS Professor of Cardiovascular Surgery, University of Oxford Conflicts of Interest: None Relevant (i) Clinical: Cardiac Surgeon and OPCABG
SAHA 2017 Optimal Conduit Strategy in 2017 David P Taggart MD PhD FRCS Professor of Cardiovascular Surgery, University of Oxford Conflicts of Interest: None Relevant (i) Clinical: Cardiac Surgeon and OPCABG
Chronic Total Occlusion: a case for coronary artery bypass grafting
 Chronic Total Occlusion: a case for coronary artery bypass grafting Rune Haaverstad Professor & Chief Dept. of Cardiothoracic Surgery Haukeland University Hospital Bergen, Norway Disclosure Research cooperation
Chronic Total Occlusion: a case for coronary artery bypass grafting Rune Haaverstad Professor & Chief Dept. of Cardiothoracic Surgery Haukeland University Hospital Bergen, Norway Disclosure Research cooperation
Clinical Seminar. Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective
 Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Important LM bifurcation studies update
 8 th European Bifurcation Club 12-13 October 2012 - Barcelona Important LM bifurcation studies update I Sheiban E-mail: isheiban@yahoo.com Unprotected LM Percutaneous Revascularization What is important
8 th European Bifurcation Club 12-13 October 2012 - Barcelona Important LM bifurcation studies update I Sheiban E-mail: isheiban@yahoo.com Unprotected LM Percutaneous Revascularization What is important
high SYNTAX Score? I Sheiban Division of Cardiology Interventional Card. University of Turin Turin / Italy
 What to do with patients with high SYNTAX Score? I Sheiban Division of Cardiology Interventional Card. University of Turin San Giovanni Battista Hospital Turin / Italy Who are the patients with high SYNTAX
What to do with patients with high SYNTAX Score? I Sheiban Division of Cardiology Interventional Card. University of Turin San Giovanni Battista Hospital Turin / Italy Who are the patients with high SYNTAX
Better CABGs vs Better PCI Devices
 CABG vs PCI 2017 Multivessel Coronary Disease Better CABGs vs Better PCI Devices ACC New York, Dec 8, 2017 No Disclosures CABG vs PCI 2017 Stable Multivessel Coronary Disease 1. Are These The two Critical
CABG vs PCI 2017 Multivessel Coronary Disease Better CABGs vs Better PCI Devices ACC New York, Dec 8, 2017 No Disclosures CABG vs PCI 2017 Stable Multivessel Coronary Disease 1. Are These The two Critical
Diabetic Patients: Current Evidence of Revascularization
 Diabetic Patients: Current Evidence of Revascularization Alexandra J. Lansky, MD Yale University School of Medicine University College of London The Problem with Diabetic Patients Endothelial dysfunction
Diabetic Patients: Current Evidence of Revascularization Alexandra J. Lansky, MD Yale University School of Medicine University College of London The Problem with Diabetic Patients Endothelial dysfunction
Clinical Considerations for CTO
 38 RCTs Clinical Considerations for CTO 18,000 pts Revascularization Whom to treat, Who derives benefit and What can we achieve? David E. Kandzari, MD FACC, FSCAI Director, Interventional Cardiology Research
38 RCTs Clinical Considerations for CTO 18,000 pts Revascularization Whom to treat, Who derives benefit and What can we achieve? David E. Kandzari, MD FACC, FSCAI Director, Interventional Cardiology Research
Patients in whom PCI is preferred over CABG _ Aleksander Ernst Clinical Hospital Center Zagreb University of Zagreb School of Medicine Zagreb, CROATIA
 3rd Dubrovnik Cardiology Highlights An ESC Update Programme in Cardiology 26.09.-29.09.2013, Hotel Excelsior, Dubrovnik, Croatia Patients in whom PCI is preferred over CABG _ Aleksander Ernst Clinical
3rd Dubrovnik Cardiology Highlights An ESC Update Programme in Cardiology 26.09.-29.09.2013, Hotel Excelsior, Dubrovnik, Croatia Patients in whom PCI is preferred over CABG _ Aleksander Ernst Clinical
Reconciling the Results of the Randomized Trials
 Management of Stable Angina in Multivessel Disease: Reconciling the Results of the Randomized Trials Eric A. Cohen MD, FRCPC Schulich Heart Centre Sunnybrook Health Sciences Centre Toronto ON ACC Rockies
Management of Stable Angina in Multivessel Disease: Reconciling the Results of the Randomized Trials Eric A. Cohen MD, FRCPC Schulich Heart Centre Sunnybrook Health Sciences Centre Toronto ON ACC Rockies
Unprotected LM intervention
 Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease
 Impact of Angiographic Complete Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease Young-Hak Kim, Duk-Woo Park, Jong-Young Lee, Won-Jang
Impact of Angiographic Complete Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease Young-Hak Kim, Duk-Woo Park, Jong-Young Lee, Won-Jang
Medical Rx vs PCI vs CABG
 Medical Rx vs PCI vs CABG S. Hinan Ahmed, MD Associate Professor: Cardiology and Cardiothoracic Surgery Program Director: Interventional Fellowship Program Assoc Editor: Cath and Cardiovasc Intervention
Medical Rx vs PCI vs CABG S. Hinan Ahmed, MD Associate Professor: Cardiology and Cardiothoracic Surgery Program Director: Interventional Fellowship Program Assoc Editor: Cath and Cardiovasc Intervention
Benefit of Performing PCI Based on FFR
 Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
Radial Artery Grafting: Why Do It? (Evidence Basis)
") Advanced Techniques for State of the Art CABG Session AATS 2015 Radial Artery Grafting: Why Do It? (Evidence Basis) David P Taggart MD PhD FRCS FESC Professor of Cardiovascular Surgery, University of Oxford
Advanced Techniques for State of the Art CABG Session AATS 2015 Radial Artery Grafting: Why Do It? (Evidence Basis) David P Taggart MD PhD FRCS FESC Professor of Cardiovascular Surgery, University of Oxford
COMMENT DEFINIR UN PLURITRONCULAIRE. Didier Carrié CHU Toulouse Rangueil
 COMMENT DEFINIR UN PLURITRONCULAIRE VISION ANGIOGRAHIQUE DU PLURITRONCULAIRE Didier Carrié CHU Toulouse Rangueil Congrès GRCI 03 Décembre 2010 Pôle Cardiovasculaire et Métabolique Avec quel œil je regarde
COMMENT DEFINIR UN PLURITRONCULAIRE VISION ANGIOGRAHIQUE DU PLURITRONCULAIRE Didier Carrié CHU Toulouse Rangueil Congrès GRCI 03 Décembre 2010 Pôle Cardiovasculaire et Métabolique Avec quel œil je regarde
Most Patients with Elective Left Main Disease. Farrel Hellig
 Most Patients with Elective Left Main Disease Should be Treated with PCI! Farrel Hellig Sunnnghill and Sunward Park Hospitals Johannesburg South Africa Everything that can be invented has been invented
Most Patients with Elective Left Main Disease Should be Treated with PCI! Farrel Hellig Sunnnghill and Sunward Park Hospitals Johannesburg South Africa Everything that can be invented has been invented
The SYNTAX-LE MANS Study
 The SYNTAX-LE MANS Study Synergy Between PCI with TAXUS Express and Cardiac Surgery: Late (15-month) Left Main Angiographic Substudy A. Pieter Kappetein, MD, PhD Erasmus MC, Rotterdam, NL SYNTAX-LE MANS
The SYNTAX-LE MANS Study Synergy Between PCI with TAXUS Express and Cardiac Surgery: Late (15-month) Left Main Angiographic Substudy A. Pieter Kappetein, MD, PhD Erasmus MC, Rotterdam, NL SYNTAX-LE MANS
LEFT MAIN PERCUTANEOUS CORONARY INTERVENTION. A/Prof Koh Tian Hai Medical Director National Heart Centre, Singapore
 LEFT MAIN PERCUTANEOUS CORONARY INTERVENTION A/Prof Koh Tian Hai Medical Director National Heart Centre, Singapore Disclosures Advisory Panel, Asian Medical Board Medtronics, Abbott Vascular. Speaker-honoraria,
LEFT MAIN PERCUTANEOUS CORONARY INTERVENTION A/Prof Koh Tian Hai Medical Director National Heart Centre, Singapore Disclosures Advisory Panel, Asian Medical Board Medtronics, Abbott Vascular. Speaker-honoraria,
Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction
 Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction Dipti Itchhaporia, MD, FACC, FESC Trustee, American College of Cardiology Director of Disease Management, Hoag Hospital Robert and Georgia
Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction Dipti Itchhaporia, MD, FACC, FESC Trustee, American College of Cardiology Director of Disease Management, Hoag Hospital Robert and Georgia
Left Main Disease: what is left to surgery? Prof. Jacques Monségu CardioVascular Institute Grenoble, France
 Left Main Disease: what is left to surgery? Prof. Jacques Monségu CardioVascular Institute Grenoble, France Background on LM stenosis 5% of patients undergoing angiography Of the myocardium 80% Bifurcation
Left Main Disease: what is left to surgery? Prof. Jacques Monségu CardioVascular Institute Grenoble, France Background on LM stenosis 5% of patients undergoing angiography Of the myocardium 80% Bifurcation
STEMI AND MULTIVESSEL CORONARY DISEASE
 STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
PTCA 1979: : I
 The SYNTAX Message is Clear: CABG is Preferred in Complex MVD Angioplasty Summit TCTAP 2012 Seoul, Korea April 2012 David R. Holmes, MD Mayo Clinic Rochester, MN Presenter Disclosure Information David
The SYNTAX Message is Clear: CABG is Preferred in Complex MVD Angioplasty Summit TCTAP 2012 Seoul, Korea April 2012 David R. Holmes, MD Mayo Clinic Rochester, MN Presenter Disclosure Information David
The Case for PCI as the Preferred Therapy in Most Patients with Chronic Stable Angina
 The Case for PCI as the Preferred Therapy in Most Patients with Chronic Stable Angina Ajay J. Kirtane,, MD Columbia University Medical Center The Cardiovascular Research Foundation Conflict of Interest
The Case for PCI as the Preferred Therapy in Most Patients with Chronic Stable Angina Ajay J. Kirtane,, MD Columbia University Medical Center The Cardiovascular Research Foundation Conflict of Interest
Approach to Multi Vessel disease with STEMI
 Approach to Multi Vessel disease with STEMI MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION Dr. Thomas Alexander, M.D; D.M; F.A.C.C. Senior Consultant and Interventional Cardiologist Kovai Medical Centre
Approach to Multi Vessel disease with STEMI MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION Dr. Thomas Alexander, M.D; D.M; F.A.C.C. Senior Consultant and Interventional Cardiologist Kovai Medical Centre
FFR in Multivessel Disease
 FFR in Multivessel Disease April, 26 2013 Coronary Physiology in the Catheterization Laboratory Location: European Heart House, Nice, France Pim A.L. Tonino, MD, PhD Hartcentrum, Eindhoven, the Netherlands
FFR in Multivessel Disease April, 26 2013 Coronary Physiology in the Catheterization Laboratory Location: European Heart House, Nice, France Pim A.L. Tonino, MD, PhD Hartcentrum, Eindhoven, the Netherlands
RADIATION HEART DISEASE: MANAGEMENT STRATEGIES
 RADIATION HEART DISEASE: MANAGEMENT STRATEGIES AMMAR CHAUDHARY MBChB, ABIM, FRCPC ASSOCIATE CONSULTANT CARDIOLOGIST KING FAISAL SPECIALIST HOSPITAL & RESEARCH CENTER - JEDDAH Scope of the Problem ~ 50
RADIATION HEART DISEASE: MANAGEMENT STRATEGIES AMMAR CHAUDHARY MBChB, ABIM, FRCPC ASSOCIATE CONSULTANT CARDIOLOGIST KING FAISAL SPECIALIST HOSPITAL & RESEARCH CENTER - JEDDAH Scope of the Problem ~ 50
Case Report Left Main Stenosis. Percutaneous Coronary Intervention (PCI) or Coronary Artery Bypass Graft Surgery (CABG)?
 or Coronary Artery Bypass Graft Surgery (CABG)?") Cronicon OPEN ACCESS CARDIOLOGY Case Report Left Main Stenosis. Percutaneous Coronary Intervention (PCI) or Coronary Artery Bypass Graft Surgery (CABG)? Valentin Hristov* Department of Cardiology, Specialized
Cronicon OPEN ACCESS CARDIOLOGY Case Report Left Main Stenosis. Percutaneous Coronary Intervention (PCI) or Coronary Artery Bypass Graft Surgery (CABG)? Valentin Hristov* Department of Cardiology, Specialized
Fractional Flow Reserve: Review of the latest data
 Fractional Flow Reserve: Review of the latest data Michalis Hamilos, MD, PhD, FESC University Hospital of Heraklion Fractional Flow Reserve (FFR) Coronary angiography does not always tell the truth Most
Fractional Flow Reserve: Review of the latest data Michalis Hamilos, MD, PhD, FESC University Hospital of Heraklion Fractional Flow Reserve (FFR) Coronary angiography does not always tell the truth Most
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Multivessel disease and cardiogenic shock: CABG is the optimal revascularization therapy. Contra Prof. Christian JM Vrints Cardiogenic Shock Spiral Acute Myocardial
DECLARATION OF CONFLICT OF INTEREST Multivessel disease and cardiogenic shock: CABG is the optimal revascularization therapy. Contra Prof. Christian JM Vrints Cardiogenic Shock Spiral Acute Myocardial
Advances in Cardiovascular Diagnosis and Therapy. No disclosure or conflicts. Outline
 Advances in Cardiovascular Diagnosis and Therapy Firas Zahr, MD Assistant Professor of Medicine Interventional Cardiology University Of Iowa No disclosure or conflicts Outline What is new with revascularization?
Advances in Cardiovascular Diagnosis and Therapy Firas Zahr, MD Assistant Professor of Medicine Interventional Cardiology University Of Iowa No disclosure or conflicts Outline What is new with revascularization?
Chronic Total Occlusions. Stephen Cook, MD Medical Director, Cardiac Catheterization Laboratory Oregon Heart & Vascular Institute
 Chronic Total Occlusions Stephen Cook, MD Medical Director, Cardiac Catheterization Laboratory Oregon Heart & Vascular Institute Financial Disclosures /see -tee-oh / abbr. Med. Chronic Total Occlusion,
Chronic Total Occlusions Stephen Cook, MD Medical Director, Cardiac Catheterization Laboratory Oregon Heart & Vascular Institute Financial Disclosures /see -tee-oh / abbr. Med. Chronic Total Occlusion,
Rationale for Percutaneous Revascularization ESC 2011
 Rationale for Percutaneous Revascularization Marie Claude Morice, Massy FR MD, FESC, FACC ESC 2011 Paris Villepinte - 27-31 August, 2011 Massy, France Potential conflicts of interest I have the following
Rationale for Percutaneous Revascularization Marie Claude Morice, Massy FR MD, FESC, FACC ESC 2011 Paris Villepinte - 27-31 August, 2011 Massy, France Potential conflicts of interest I have the following
CONTEMPORARY USE OF ARTERIAL GRAFTS DURING CORONARY ARTERY BYPASS SURGERY: PARADIGM SHIFT? OR A LITTLE (MORE) TALK THAT NEEDS A LOT MORE ACTION
 TALK THAT NEEDS A LOT MORE ACTION") CONTEMPORARY USE OF ARTERIAL GRAFTS DURING CORONARY ARTERY BYPASS SURGERY: PARADIGM SHIFT? OR A LITTLE (MORE) TALK THAT NEEDS A LOT MORE ACTION JAMES L ZELLNER MD I have no financial disclosures. 1897
CONTEMPORARY USE OF ARTERIAL GRAFTS DURING CORONARY ARTERY BYPASS SURGERY: PARADIGM SHIFT? OR A LITTLE (MORE) TALK THAT NEEDS A LOT MORE ACTION JAMES L ZELLNER MD I have no financial disclosures. 1897
Coronary stenting: the appropriate use of FFR
 Coronary stenting: the appropriate use of FFR Morton J. Kern, MD Professor of Medicine Chief of Cardiology LBVA Associate Chief Cardiology University California Irvine Orange, California To treat or not
Coronary stenting: the appropriate use of FFR Morton J. Kern, MD Professor of Medicine Chief of Cardiology LBVA Associate Chief Cardiology University California Irvine Orange, California To treat or not
Le# Main Interven-on: When Is It Appropriate. Femi Philip, MD Assistant Professor Of Medicine UC Davis
 Le# Main Interven-on: When Is It Appropriate Femi Philip, MD Assistant Professor Of Medicine UC Davis Nil Disclosures Outline What is the LMCA? Should we revascularize severe LMCA disease? What revascularizacon
Le# Main Interven-on: When Is It Appropriate Femi Philip, MD Assistant Professor Of Medicine UC Davis Nil Disclosures Outline What is the LMCA? Should we revascularize severe LMCA disease? What revascularizacon
Coronary Artery Disease: Revascularization (Teacher s Guide)
") Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
FFR Incorporating & Expanding it s use in Clinical Practice
 FFR Incorporating & Expanding it s use in Clinical Practice Suleiman Kharabsheh, MD Consultant Invasive Cardiology Assistant professor, Alfaisal Univ. KFHI - KFSHRC Concept of FFR Maximum flow down a vessel
FFR Incorporating & Expanding it s use in Clinical Practice Suleiman Kharabsheh, MD Consultant Invasive Cardiology Assistant professor, Alfaisal Univ. KFHI - KFSHRC Concept of FFR Maximum flow down a vessel
Mise à Jour sur le traitement du Pluritronculaire Philippe Généreux, MD
 Mise à Jour sur le traitement du Pluritronculaire Philippe Généreux, MD Columbia University Medical Center and The Cardiovascular Research Foundation, New York, USA Hôpital du Sacré-Coeur de Montréal,
Mise à Jour sur le traitement du Pluritronculaire Philippe Généreux, MD Columbia University Medical Center and The Cardiovascular Research Foundation, New York, USA Hôpital du Sacré-Coeur de Montréal,
How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting
 How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting Ahmed A A Suliman, MBBS, FACP, FESC Associate Professor, University of Khartoum Interventional Cardiologist,
How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting Ahmed A A Suliman, MBBS, FACP, FESC Associate Professor, University of Khartoum Interventional Cardiologist,
Komplexe Koronarintervention heute: Von Syntax zu bioresorbierbaren Stents
 Komplexe Koronarintervention heute: Von Syntax zu bioresorbierbaren Stents Prof. Dr. med. Julinda Mehilli Medizinische Klinik und Poliklinik I Klinikum der Universität München Campus Großhadern Key Factors
Komplexe Koronarintervention heute: Von Syntax zu bioresorbierbaren Stents Prof. Dr. med. Julinda Mehilli Medizinische Klinik und Poliklinik I Klinikum der Universität München Campus Großhadern Key Factors
Lésions du tronc commun: Reste t il une place pour la chirugie? Pierre Deharo, CHU TIMONE, Marseille
 Lésions du tronc commun: Reste t il une place pour la chirugie? Pierre Deharo, CHU TIMONE, Marseille Disclosure Statement of Financial Interest I currently have, or have had over the last two years, an
Lésions du tronc commun: Reste t il une place pour la chirugie? Pierre Deharo, CHU TIMONE, Marseille Disclosure Statement of Financial Interest I currently have, or have had over the last two years, an
New Generation Drug- Eluting Stent in Korea
 New Generation Drug- Eluting Stent in Korea Young-Hak Kim, MD, PhD Department of Cardiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea Purpose To briefly introduce the
New Generation Drug- Eluting Stent in Korea Young-Hak Kim, MD, PhD Department of Cardiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea Purpose To briefly introduce the
PCI for Stable Ischemic Heart Disease: What Happened in the Last Week?
 PCI for Stable Ischemic Heart Disease: What Happened in the Last Week? Ajay J. Kirtane, MD, SM Center for Interventional Vascular Therapy Columbia University Medical Center / NewYork Presbyterian Hospital
PCI for Stable Ischemic Heart Disease: What Happened in the Last Week? Ajay J. Kirtane, MD, SM Center for Interventional Vascular Therapy Columbia University Medical Center / NewYork Presbyterian Hospital
Management of High-Risk Coronary Artery Disease
 Management of High-Risk Coronary Artery Disease Jeffrey J. Popma, MD Director, Interventional Cardiology Clinical Services Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard Medical
Management of High-Risk Coronary Artery Disease Jeffrey J. Popma, MD Director, Interventional Cardiology Clinical Services Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard Medical
CLINICAL CONSEQUENCES OF THE
 CLINICAL CONSEQUENCES OF THE FAME STUDY TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands GUIDELINES ESC SEPTEMBER 2010 FFR UPGRADED TO LEVEL
CLINICAL CONSEQUENCES OF THE FAME STUDY TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands GUIDELINES ESC SEPTEMBER 2010 FFR UPGRADED TO LEVEL
Update 2012 Herzchirurgie
 Update 2012 Herzchirurgie Prof. Dr. Jürg Grünenfelder Klinik für Herz- und Gefässchirurgie UniversitätsSpital Zürich Themenübersicht - update Koronarchirurgie - Syntax 5 Jahre - Freedom 5 Jahre - update
Update 2012 Herzchirurgie Prof. Dr. Jürg Grünenfelder Klinik für Herz- und Gefässchirurgie UniversitätsSpital Zürich Themenübersicht - update Koronarchirurgie - Syntax 5 Jahre - Freedom 5 Jahre - update
Treatment Options for Angina
 Treatment Options for Angina Interventional Cardiology Perspective Michael A. Robertson, M.D. 10/30/10 Prevalence of CAD in USA 15 million Americans with CAD 2 million diagnostic catheterizations 1 million
Treatment Options for Angina Interventional Cardiology Perspective Michael A. Robertson, M.D. 10/30/10 Prevalence of CAD in USA 15 million Americans with CAD 2 million diagnostic catheterizations 1 million
Coronary Revascularization for Patients with Severe Coronary Artery Disease: An Overview of Current Evidence and Treatment Strategies
 Review J Jpn Coron Assoc 2015; 21: 267-271 Coronary Revascularization for Patients with Severe Coronary Artery Disease: An Overview of Current Evidence and Treatment Strategies Hiroki Shiomi, Takeshi Kimura
Review J Jpn Coron Assoc 2015; 21: 267-271 Coronary Revascularization for Patients with Severe Coronary Artery Disease: An Overview of Current Evidence and Treatment Strategies Hiroki Shiomi, Takeshi Kimura
Asian AMI Registry Session The 17 th Joint Meeting of Coronary Revascularization (JCR 2017) Busan, Korea Dec 8 th 2017
 Busan, Korea Dec 8 th 2017") Asian AMI Registry Session The 17 th Joint Meeting of Coronary Revascularization (JCR 2017) Busan, Korea Dec 8 th 2017 Trends of acute myocardial infarction in Korea from the experience of Korea Acute
Asian AMI Registry Session The 17 th Joint Meeting of Coronary Revascularization (JCR 2017) Busan, Korea Dec 8 th 2017 Trends of acute myocardial infarction in Korea from the experience of Korea Acute
Guidelines/Appropriateness ARCH 2015 St Louis, Missouri April 9-11, 2015 Manish A. Parikh, MD, FACC,FSCAI
 Guidelines/Appropriateness ARCH 2015 St Louis, Missouri April 9-11, 2015 Manish A. Parikh, MD, FACC,FSCAI Center for Interventional Vascular Therapy Columbia University Medical Center / New York Presbyterian
Guidelines/Appropriateness ARCH 2015 St Louis, Missouri April 9-11, 2015 Manish A. Parikh, MD, FACC,FSCAI Center for Interventional Vascular Therapy Columbia University Medical Center / New York Presbyterian
Σεμινάριο Ομάδων Εργασίας Fractional Flow Reserve (FFR) Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική
 Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική") ΕΛΛΗΝΙΚΗΚΑΡΔΙΟΛΟΓΙΚΗΕΤΑΙΡΕΙΑ Σεμινάριο Ομάδων Εργασίας 2011 Fractional Flow Reserve (FFR) Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική GUIDELINES ON MYOCARDIAL
ΕΛΛΗΝΙΚΗΚΑΡΔΙΟΛΟΓΙΚΗΕΤΑΙΡΕΙΑ Σεμινάριο Ομάδων Εργασίας 2011 Fractional Flow Reserve (FFR) Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική GUIDELINES ON MYOCARDIAL
Perspective of LM stenting with Current registry and Randomized Clinical Data
 Asian Pacific TCT Perspective of LM stenting with Current registry and Randomized Clinical Data Patrick W. Serruys MD PhD Yoshinobu Onuma MD Seung-Jung Park MD, PhD 14:48-15:00, 2009 Symposium Arena, Level
Asian Pacific TCT Perspective of LM stenting with Current registry and Randomized Clinical Data Patrick W. Serruys MD PhD Yoshinobu Onuma MD Seung-Jung Park MD, PhD 14:48-15:00, 2009 Symposium Arena, Level
Declaration of conflict of interest NONE
 Declaration of conflict of interest NONE Claudio Muneretto MD, PhD Director of Division of Cardiac Surgery University of Brescia Medical School Italy Hybrid Chymera Different features and potential advantages
Declaration of conflict of interest NONE Claudio Muneretto MD, PhD Director of Division of Cardiac Surgery University of Brescia Medical School Italy Hybrid Chymera Different features and potential advantages
Lessons learned From The National PCI Registry
 Lessons learned From The National PCI Registry w a v e On Behalf of The Publication Committee of the National PCI Registry Objectives & Anticipated Achievements To determine the epidemiology of patients
Lessons learned From The National PCI Registry w a v e On Behalf of The Publication Committee of the National PCI Registry Objectives & Anticipated Achievements To determine the epidemiology of patients
Application of Appropriate Use Criteria in Clinical Care of CAD. Peter K. Smith, MD Professor and Chief Thoracic Surgery Duke University 4/29/2012
 Application of Appropriate Use Criteria in Clinical Care of CAD Peter K. Smith, MD Professor and Chief Thoracic Surgery Duke University 4/29/2012 Influence of Severity and Location of Stenosis on Cardiac
Application of Appropriate Use Criteria in Clinical Care of CAD Peter K. Smith, MD Professor and Chief Thoracic Surgery Duke University 4/29/2012 Influence of Severity and Location of Stenosis on Cardiac
Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX
 Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX Boston Scientific, Inc.- Syntax Trial Steering Committee Member- travel expenses paid by trial sponsor Maquet, Inc.- unpaid
Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX Boston Scientific, Inc.- Syntax Trial Steering Committee Member- travel expenses paid by trial sponsor Maquet, Inc.- unpaid
Coronary interventions
 Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
SYNTAX score before decision making! Corrado Tamburino, MD, PhD
 SYNTAX score in left main - Tamburino TCT Asia Pacific Seoul, 27 April 2011 Slide 1 SYNTAX score before decision making! Corrado Tamburino, MD, PhD Full Professor of Cardiology, Director of Postgraduate
SYNTAX score in left main - Tamburino TCT Asia Pacific Seoul, 27 April 2011 Slide 1 SYNTAX score before decision making! Corrado Tamburino, MD, PhD Full Professor of Cardiology, Director of Postgraduate
Management of Multivessel CAD: Stenting or CABG?
 Management of Multivessel CAD: Stenting or CABG? Filippos Triposkiadis, MD, FESC, FACC Department of Cardiology, University of Thessaly Long-term Outcome of Patients With 3VD Undergoing CABG A Report from
Management of Multivessel CAD: Stenting or CABG? Filippos Triposkiadis, MD, FESC, FACC Department of Cardiology, University of Thessaly Long-term Outcome of Patients With 3VD Undergoing CABG A Report from
Rationale for Left Ventricular Support During Percutaneous Coronary Intervention
 Rationale for Left Ventricular Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Associate Professor, Division of Cardiology Director, Acute Circulatory Support Program
Rationale for Left Ventricular Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Associate Professor, Division of Cardiology Director, Acute Circulatory Support Program
SURGICAL MYOCARDIAL REVASCULARIZATION: ARTERIAL VS VENOUS GRAFTS, SINGLE VS MULTIPLE GRAFTS?
 SURGICAL MYOCARDIAL REVASCULARIZATION: ARTERIAL VS VENOUS GRAFTS, SINGLE VS MULTIPLE GRAFTS? Luigi Martinelli Chief, Dept. of Surgery Istituto Clinico Ligure di Alta Specialità RAPALLO During 1987 2006,
SURGICAL MYOCARDIAL REVASCULARIZATION: ARTERIAL VS VENOUS GRAFTS, SINGLE VS MULTIPLE GRAFTS? Luigi Martinelli Chief, Dept. of Surgery Istituto Clinico Ligure di Alta Specialità RAPALLO During 1987 2006,
COMPARE Trial Elvin Kedhi Maasstad Ziekenhuis Rotterdam The Netherlands
 COMPARE Trial Elvin Kedhi Maasstad Ziekenhuis Rotterdam The Netherlands TCTAP 2010 Seoul, Korea Disclosures Research Foundation of the Cardiology Department has received unrestricted research grants from:
COMPARE Trial Elvin Kedhi Maasstad Ziekenhuis Rotterdam The Netherlands TCTAP 2010 Seoul, Korea Disclosures Research Foundation of the Cardiology Department has received unrestricted research grants from:
Adults With Diagnosed Diabetes
 Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Fractional Flow Reserve: Basics, FAME 1, FAME 2. William F. Fearon, MD Associate Professor Stanford University Medical Center
 Fractional Flow Reserve: Basics, FAME 1, FAME 2 William F. Fearon, MD Associate Professor Stanford University Medical Center Conflict of Interest Advisory Board for HeartFlow Research grant from St. Jude
Fractional Flow Reserve: Basics, FAME 1, FAME 2 William F. Fearon, MD Associate Professor Stanford University Medical Center Conflict of Interest Advisory Board for HeartFlow Research grant from St. Jude
Cindy L. Grines MD FACC FSCAI
 Cindy L. Grines MD FACC FSCAI Hofstra Northwell School of Medicine Chair, Cardiology Academic Chief of Cardiology, Northwell Health North Shore University Hospital, Manhasset NY Multivessel Disease in
Cindy L. Grines MD FACC FSCAI Hofstra Northwell School of Medicine Chair, Cardiology Academic Chief of Cardiology, Northwell Health North Shore University Hospital, Manhasset NY Multivessel Disease in
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
FAME STUDY: 2-year Follow-Up & CLINICAL SUBGROUP ANALYSIS
 Coronary Physiology In The Cathlab FAME STUDY: 2-year Follow-Up & CLINICAL SUBGROUP ANALYSIS Educational Training Program ESC European Heart House april 7th 9th 2011 Nico H.J.Pijls, MD, PhD Catharina Hospital,
Coronary Physiology In The Cathlab FAME STUDY: 2-year Follow-Up & CLINICAL SUBGROUP ANALYSIS Educational Training Program ESC European Heart House april 7th 9th 2011 Nico H.J.Pijls, MD, PhD Catharina Hospital,
ROLE OF CORONARY PRESSURE & FFR IN MULTIVESSEL DISEASE
 ROLE OF CORONARY PRESSURE & FFR IN MULTIVESSEL DISEASE Angioplasty Summit TCT ASIA Seoul, Korea, april 24th, 2008 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands A rather common
ROLE OF CORONARY PRESSURE & FFR IN MULTIVESSEL DISEASE Angioplasty Summit TCT ASIA Seoul, Korea, april 24th, 2008 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands A rather common
Quality of Life After Everolimus- Eluting Stents or Bypass Surgery for Treatment of Left Main Coronary Artery Disease:
 Quality of Life After Everolimus- Eluting Stents or Bypass Surgery for Treatment of Left Main Coronary Artery Disease: Results from the EXCEL Trial Suzanne J. Baron MD MSC on behalf of the EXCEL Investigators
Quality of Life After Everolimus- Eluting Stents or Bypass Surgery for Treatment of Left Main Coronary Artery Disease: Results from the EXCEL Trial Suzanne J. Baron MD MSC on behalf of the EXCEL Investigators
The MAIN-COMPARE Study
 Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
Percutaneous Coronary Interventions Without On-site Cardiac Surgery
 Percutaneous Coronary Interventions Without On-site Cardiac Surgery Hassan Al Zammar, MD,FESC Consultant & Interventional Cardiologist Head of Cardiology Department European Gaza Hospital Palestine European
Percutaneous Coronary Interventions Without On-site Cardiac Surgery Hassan Al Zammar, MD,FESC Consultant & Interventional Cardiologist Head of Cardiology Department European Gaza Hospital Palestine European
Incremental Value of Multiple Arterial conduits in CABG
 Incremental Value of Multiple Arterial conduits in CABG Nirav C Patel MD FRCS CTh Professor Zucker School of Medicine at Hofstra Northwell Director of Robotic Cardiac Surgery Northwell Health Vice Chairman
Incremental Value of Multiple Arterial conduits in CABG Nirav C Patel MD FRCS CTh Professor Zucker School of Medicine at Hofstra Northwell Director of Robotic Cardiac Surgery Northwell Health Vice Chairman
Left Main PCI vs. CABG: Real World
 Management of Patients with Stable CAD Left Main PCI vs. CABG: Real World Marco Roffi, MD, FESC University Hospital Geneva, Switzerland SYNTAX-LMT The SYNTAX trial included a pre-specified subgroup of
Management of Patients with Stable CAD Left Main PCI vs. CABG: Real World Marco Roffi, MD, FESC University Hospital Geneva, Switzerland SYNTAX-LMT The SYNTAX trial included a pre-specified subgroup of
Primary Percutaneous Coronary Intervention
 The big 5 in PCI Primary Percutaneous Coronary Intervention W. Wijns (Aalst, BE) Disclosures Consulting Fees: on my behalf go to the Cardiovascular Research Center Aalst Contracted Research between the
The big 5 in PCI Primary Percutaneous Coronary Intervention W. Wijns (Aalst, BE) Disclosures Consulting Fees: on my behalf go to the Cardiovascular Research Center Aalst Contracted Research between the