Role of radiology and imaging in the daignosis of acute abdominal conditions
|
|
|
- Garry Berry
- 5 years ago
- Views:
Transcription
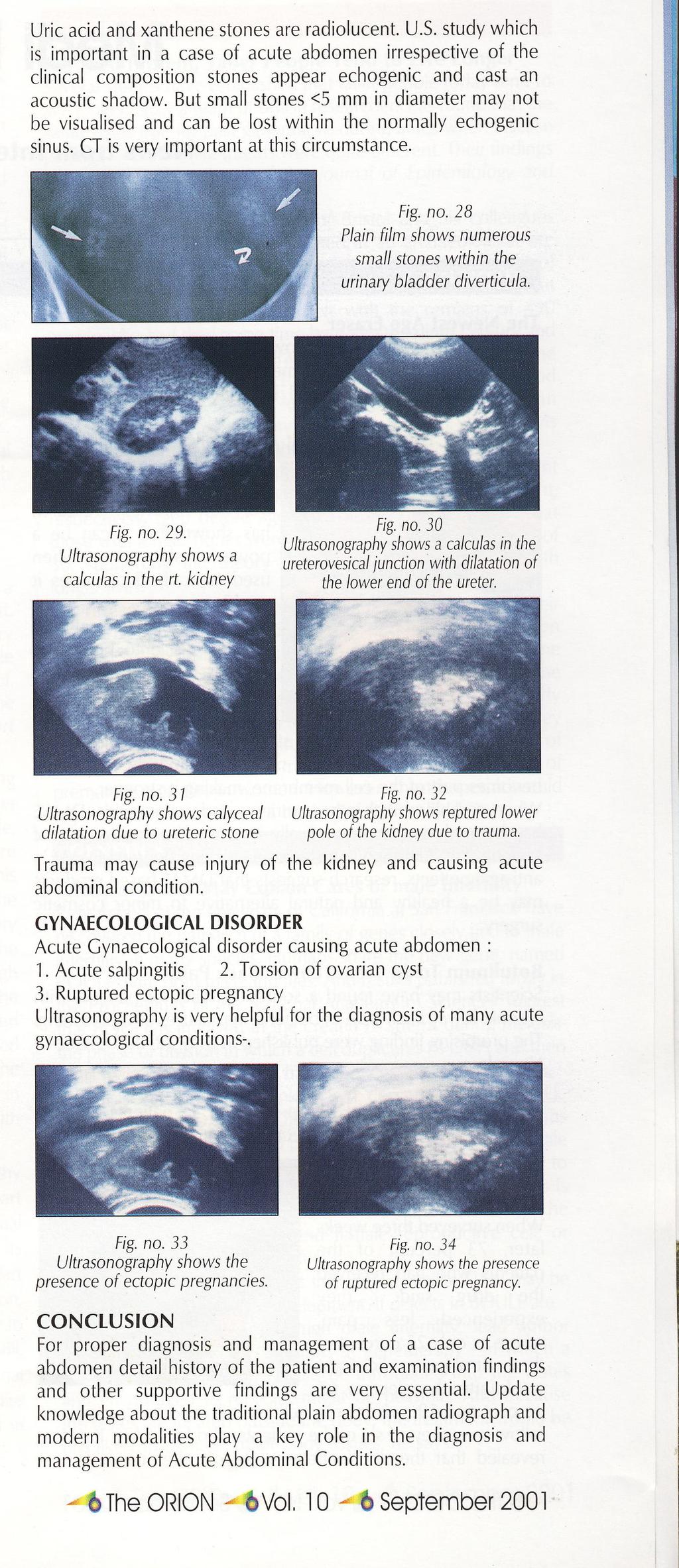
1 Role of radiology and imaging in the daignosis of acute abdominal conditions Miah MAY Introduction In our day to day practice we have to face many of the acute abdominal conditions. As we know acute abdomen means the patient complaints of an acute attack of pain in abdomen which may occur suddenly or for a period of several hours and gradually becoming worse and demands an urgent diagnosis, treatment and even surgical intervention. Early accurate diagnosis is essential for proper management. A careful history and examination findings are very very essential for the radiologists also to give a comment about the cause of the disease. Though not all, many of the cases may be diagnosed without the help of any diagnostic tool. Some cases may be problematic. In those cases Radiology and Imaging can help a lot in determining the proper diagnosis. Usual radiological tools we use are 1. Plain film of abdomen and Chest P.A in erect posture 2. U.S 3. C.T.Scan (Occasionally) 4. MRI (Rarely) What we see in plain radiography (a) In most acute abdominal conditions the radiological diagnosis depends on gas patterns e.g. distribution of gases in dilated & nondilated bowel, presence of gas inside or outside the bowel lumen. (b) Radiopaque shadows (c) Fluid and gas levels. What are the radiographic techniques 1.Supine abdomen: We can see the distribution of gas and calibre of the bowel and may show displacement of bowel gases by a mass. Dr. Md. Abu Yusuf Miah, MBBS,DMRD, Asst. Prof. of Radiology and Imaging, DMCH, Dhaka 2.Erect abdomen:to see fluid levels and free gases. Usually 3 or more small bowel fluid levels longer than 2.5 cm are abnormal. 3.Left lateral decubitus: Patients lying on their left side and the X-ray beam is horizontal. Patients who are unfit to sit or stand for an erect film, it is the projection of choice to show a small pneumoperitonium. In this projection free gas may be trapped between the edge of the liver and the lateral abdominal wall, or sometimes in the pelvis where it is the highest point specially in case of female. 4.Chest X-ray: Why? (a) Erect chest film is the best film to show the presence of a small pneumoperitonium. (b) A number of chest conditions which may mimic acute abdomen: 1. Lower lobar pneumonia 2. Myocardial infarction 3. Pulmonary infarction 4. C.C.F 5. Pericarditis 6. Leaking or dissecting thoracic aortic aneurysm 7. Pneumothorax (c) Acute abdominal conditions may be complicated by chest pathology: e.g. pleural effusion frequently complicate acute pancreatitis, following prolong vomiting in elderly patients in intestinal obstruction, there may be pneumonia or heart failure. Abdomen may be compared with a pandora's magic box. There are many causes of acute abdomen of which some are common which we face at our day to day practice. I want to show some of the radiological findings system wise. Common acute abdominal conditions found in relation with- G.I. Tract (A)Acute appendicitis: Commonest acute surgical condition in the developed world. No role of radiography. But can be done to exclude other causes. Direct visualisation by HRSG Puylaert JB
2 graded compression technique. The fat and the bowel loops are displaced by compression. Inflamed appendix appears to be a thick walled incompressible sausage like tube with concentric layers in transverse plane. Perifocal oedema is also present. Fluid is also seen in the lumen of appendix. It is elongated tube with one end blind. When wall thickness exceeds 6 mm it is suggestive of inflammation. Fig. no.4- -Abdomen supine -A triangular collection of free gas in the sub -hepatic region Fig. no.5--a band of curvilinear pulmonary collapse with a crescent of normal lung beneath it- simulating Pseudo - pneumoperitonium Fig. no.l-shows inflamed appendix in transverse plane. Fig. no.2-shows inflamed appendix in long axis. (B)Pneumoperitonium: Demonstration of small pneumoperitonium is very essential. Most of the cases the cause of the pneumoperitonium will require emergency surgery. Fig. no.3- (a) Erect chest film- Free gas seen under both domes of diaphragm. (b) Abdomen erect, free gas under tile domes 6(diaphragm. (C) Pseudopneumoperitonium: A number of conditions which simulate pneumoperitoneum e.g.- 1. Chilaiditis syndrome -Distended bowel between liver and right. dome of diaphragm 2. Sub diaphragmatic fat-omental fat 3. Curvilinear pulmonary collapse (D)lntestinal obstruction: Dilation of bowel occurs in 1. Mechanical intestinal obstruction 2. Pseudoobstruction 3. Paralytic ileus 4. Air swallowing 5. Several other conditions. Radiological differentiation depends mainly on the size, mucosal appearance and the distribution of loops of bowel. The diagnosis of intestinal obstruction depends on the demonstration of dilated loops of bowel proximally with non-dilated or collapsed bowel distal to the presumed point of obstruction. (A)Acute gastric dilatation: Dilatation of the stomach can be caused by 4 main groups of conditions-- (I)Mechanical gastric outlet obstruction may be a sequel of peptic ulcer or a carcinoma of the antrum. (II)Paralytic ileus- This group of conditions is frequently referred to as acute gastric dilatation. (III)Volvulus and air swallowing are usually uncommon conditions. (B)Small bowel obstruction: Usual causes are the bands,adhesions and strangulations. Complete obstruction of the small bowel usually causes small bowel dilatation with accumulation of both gas and fluid and a reduction in calibre of the large bowel. Plain film changes in small bowel obstruction may appear after 3-5 hours if



 Gas within the bile duct b)features of small bowel obstruction c)abnormallocation of gallstone d)other previous findings which coincides biliary stone.")
3 there is complete small bowel obstruction and such changes are usually marked after 12 hours. In incomplete obstruction early films may be normal. This slide shows the feature of gall stone ileus. Here you see multiple dilated loops of small bowel with a band of gas within the CBD.Gall stone ileus is a mechanical obstruction caused by the impaction of one or more gall stones in the intestine, usually in the terminal ileum and rarely in the duodenum. Fig, No.9-Gall stone ileus. Slide no.6-shows acute gastric dilatation Slide no. 7-Shows Small bowel obstruction: Multiple dilated loops and air fluid level. A very small amount of gases are noted in the large bowel. Differentiating points between a small and large bowel obstruction: String of beads sign: What is that: In dilated small bowel which is almost completely filled with fluid. Small bubbles of gas may be trapped in rows between the Volvulae connivanties on horizontal ray films- this is known as String of beads sign. This sign if present is virtually diagnostic of small bowel obstruction. Fig. No.8- -Another slide of small bowel obstruction showing String of beads sign. Signs of gallstone ileus a) Gas within the bile duct b)features of small bowel obstruction c)abnormallocation of gallstone d)other previous findings which coincides biliary stone. What are the other causes of gas in the biliary tree: a)physiological if the sphincter is laxed. b)following biliary surgery c)malignant fistula d)perforated peptic ulcer into the bile duct. Its a case of intussusception is seen in children under 2 years of age. In children it usually commences in the ileum as the result of inflammation of the lymphoid tissue and tends to be associated with mesenteric adenitis. The enlarged lymphatic patches are forced into the ileum by peristaltic movement and acting as a tumour. So one part of the ileum is pushed into the other and causing intussusception. In adults intussusception is invariably caused by a tumour of bowel. A barium enema examination is frequently required to establish a definite diagnosis and sometimes also relieves the patient. Fig. no. 10(a)-- Multiple gas filled loops of dilated small bowel there is a soft tissue mass in the right iliac fossa, Contrast enema examination of large gut of a baby shows the intussusception producing a

4 concave defect in the head of the contrast column. Sometimes contrast medium may pass beyond this, causing the well known coiled spring appearance. obstruction, the radiographic appearance may be identical to those of a paralytic ileus. Paralytic ileus causes when intestinal peristalsis ceases and as a result fluid and gas accumulates in the dilated bowel. It is frequently found in cases of peritonitis and in the post operative cases. Along with the radiological findings, history and clinical signs are helpful in differentiating between large bowel obstruction & paralytic ileus. Fig. no.10 (b) (iii) Large bowel obstruction: Usual causes are the a) Carcinoma -60% is situated in the sigmoid colon b) Diverticular disease c)volvulus of the colon. Key to the radiological appearance of the large bowel obstruction depends on the state of the competence of the Ileocaecal valve. The obstructed colon invariably contains large amounts of air and can usually be identified by its location and by the presenc of haustral markings. When both small and large bowel dilatation are present in a case of large bowel Fig. no.10 (c) Fig. no.11. Shows hugely dilated large gut. Its a case of sigmoid volvulus. A haustral loop of sigmoid is seen rising out the pelvis in the shape of an inverted 'U' Dilated haustral colons are present on the two sides of the volvulus. Fig.no.12--Th/s film showsgeneralised dilatat lon of both small and large bowel and its a case of paralytic ileus. Acute pacreatitis: Clinical diagnosis may be difficult in the initial stage.other acute abdominal conditions such as perforation, acute cholecystitis, acute peptic ulcer have to be included in the differential diagnosis. A large number of radiological signs have been described, most of them are non-specific.usg and CT are the diagnostic modality. Fig. no Shows the transverse scan of normal pancreas and its duct. The normal pancreas has about the same echogenecity as that of liver but its echogenecity increase with age. When we scan the pancreas we usually identify the following anatomical landmarks: 1.Aorta 2. Superior mesenteric artery 3. Superior mesenteric vein 4. Liver etc. Average diameter of the head of the pancreas is 2.8 cm. body 2 cm and tail 2.5cm, duct diameter less than 2mm. In acute pancreatitis pancreas is diffusely enlarged and oedematous which is hypoechogenic in comparison with the liver parenchyma. Diffusely enlarged irregularly hypoechogenic pancreas may also seen in



5 acute pancreatitis when it is superimposed on chronic pancreatitis. C. T. is the investigation of choice for such cases. Fig. no Shows diffusely enlarged and oedematous Pancreas

6 Review Article
Introduction and Definitions
 Bowel obstruction Introduction and Definitions Accounts for 5% of all acute surgical admissions Patients are often extremely ill requiring prompt assessment, resuscitation and intensive monitoring Obstruction
Bowel obstruction Introduction and Definitions Accounts for 5% of all acute surgical admissions Patients are often extremely ill requiring prompt assessment, resuscitation and intensive monitoring Obstruction
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients).
.") Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
Abdominal radiology 腹部放射線學
 Abdominal radiology 腹部放射線學 台北醫學大學 - 市立萬芳醫院 留偉順 laowilson@hotmail.com The Normal Abdominal Series Chest Supine abdomen Erect abdomen Left lateral decubitus abdomen Learning objectives Understanding normal
Abdominal radiology 腹部放射線學 台北醫學大學 - 市立萬芳醫院 留偉順 laowilson@hotmail.com The Normal Abdominal Series Chest Supine abdomen Erect abdomen Left lateral decubitus abdomen Learning objectives Understanding normal
Pathology of Intestinal Obstruction. Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College
 Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
Radiology of the abdomen Lecture -1-
 Radiology of the abdomen Lecture -1- Objectives To know radiology modalities used in abdomen imaging mainly GI tract. To know advantages and disadvantages of each modality. To know indications and contraindications
Radiology of the abdomen Lecture -1- Objectives To know radiology modalities used in abdomen imaging mainly GI tract. To know advantages and disadvantages of each modality. To know indications and contraindications
ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O
 ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O Introduction The abdomen (less formally called the belly, stomach, is that part of the body between the thorax (chest) and pelvis,
ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O Introduction The abdomen (less formally called the belly, stomach, is that part of the body between the thorax (chest) and pelvis,
Radiology. Undergraduate Radiology Sample Questions
 Radiology Undergraduate Radiology Sample Questions April 2012 The following examples are offered of questions that might be used to assess undergraduate radiology. There are 3 different styles: An OSCE
Radiology Undergraduate Radiology Sample Questions April 2012 The following examples are offered of questions that might be used to assess undergraduate radiology. There are 3 different styles: An OSCE
INVESTIGATIONS OF GASTROINTESTINAL DISEAS
 INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
Guidelines, Policies and Statements D5 Statement on Abdominal Scanning
 Guidelines, Policies and Statements D5 Statement on Abdominal Scanning Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to ensure that this Guideline/Policy/Statement
Guidelines, Policies and Statements D5 Statement on Abdominal Scanning Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to ensure that this Guideline/Policy/Statement
Role of imaging in the evaluation of the acute abdomen
 Prof. András Palkó MD, PhD Role of imaging in the evaluation of the acute abdomen Faculty of General Medicine University of Szeged Hungary 1 Definition Sudden onset of severe symptoms requiring emergency
Prof. András Palkó MD, PhD Role of imaging in the evaluation of the acute abdomen Faculty of General Medicine University of Szeged Hungary 1 Definition Sudden onset of severe symptoms requiring emergency
Development of pancreas and Small Intestine. ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama
 Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System
 Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Many of the disease processes that acutely affect the abdomen produce
 ABC of Emergency Radiology Radiographic signs oftrauma THE ABDOMEN-II D A Nicholson, P A Driscoll Many of the disease processes that acutely affect the abdomen produce radiographic signs, but most of these
ABC of Emergency Radiology Radiographic signs oftrauma THE ABDOMEN-II D A Nicholson, P A Driscoll Many of the disease processes that acutely affect the abdomen produce radiographic signs, but most of these
Abdominal Pain in Pediatric Patients Image Gently
 Abdominal Pain in Pediatric Patients Image Gently Susan D. John, M.D. Baptist Health Emergency Radiology 2017 Disclosure I have no financial relationships with a commercial entity producing healthcarerelated
Abdominal Pain in Pediatric Patients Image Gently Susan D. John, M.D. Baptist Health Emergency Radiology 2017 Disclosure I have no financial relationships with a commercial entity producing healthcarerelated
Medical application of transabdominal ultrasound in gastrointestinal diseases
 Medical application of transabdominal ultrasound in gastrointestinal diseases Hsiu-Po Wang Department of Emergency Medicine National Taiwan University Hospital Real-time ultrasound has become a standard
Medical application of transabdominal ultrasound in gastrointestinal diseases Hsiu-Po Wang Department of Emergency Medicine National Taiwan University Hospital Real-time ultrasound has become a standard
Nasogastric tube. Stomach. Pylorus. Duodenum 1. Duodenum 2. Duodenum 3. Duodenum 4
 Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Abdominal ultrasound:
 Abdominal ultrasound: Non-traumatic acute abdomen Wittanee Na-ChiangMai, MD Department of Radiology ChiangMai University 26/04/2017 Contents Technique of examination Normal anatomy Emergency conditions
Abdominal ultrasound: Non-traumatic acute abdomen Wittanee Na-ChiangMai, MD Department of Radiology ChiangMai University 26/04/2017 Contents Technique of examination Normal anatomy Emergency conditions
Acute Abdomen 急腹症 钱黎俊. Radiology, Renji Hospital. Shanghai Jiaotong University School of Medicine
 Acute Abdomen 急腹症 Radiology, Renji Hospital Shanghai Jiaotong University School of Medicine 钱黎俊 Learning objectives To understand the normal anatomy of the erect abdominal plain film To understand and
Acute Abdomen 急腹症 Radiology, Renji Hospital Shanghai Jiaotong University School of Medicine 钱黎俊 Learning objectives To understand the normal anatomy of the erect abdominal plain film To understand and
General Data. 王 X 村 78 y/o 男性
 General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
GIT RADIOLOGY. Water-soluble contrast media (e.g. gastrograffin) are the other available agents.which doesn t cause inflammatory peritonitis..
 are the other available agents.which doesn t cause inflammatory peritonitis..") GIT RADIOLOGY Imaging techniques-general principles: Contrast examinations: Barium sulphate is the best contrast for GIT (with good mucosal coating & excellent opacification & being inert); but is contraindicated
GIT RADIOLOGY Imaging techniques-general principles: Contrast examinations: Barium sulphate is the best contrast for GIT (with good mucosal coating & excellent opacification & being inert); but is contraindicated
Evidence Process for Abdominal Pain Guideline Research 11/16/2017. Guideline Review using ADAPTE method and AGREE II instrument 11/16/2017
 Evidence Process for Abdominal Pain Guideline Research Guideline Review using ADAPTE method and AGREE II instrument Approximately 139 Potentially relevant guidelines identified in various resources* 59
Evidence Process for Abdominal Pain Guideline Research Guideline Review using ADAPTE method and AGREE II instrument Approximately 139 Potentially relevant guidelines identified in various resources* 59
Sonographic Appearances of Common Gut Pathology in Paediatric Patients: Comparison with Plain Abdominal Radiography
 3668 Radiographer Text 1/4/04 2:57 PM Page 11 The Radiographer vol. 51: 11-17 Sonographic Appearances of Common Gut Pathology in Paediatric Patients: Comparison with Plain Abdominal Radiography Lino Piotto
3668 Radiographer Text 1/4/04 2:57 PM Page 11 The Radiographer vol. 51: 11-17 Sonographic Appearances of Common Gut Pathology in Paediatric Patients: Comparison with Plain Abdominal Radiography Lino Piotto
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
Spleen indications of splenectomy complications OPSI
 Intestinal obstruction Differences between adynamic ileus and mechanical obstruction Aetiology Pathophysiology (Cluster contractions- bowel proximal to the obstruction dilate- wall of obstructed gut is
Intestinal obstruction Differences between adynamic ileus and mechanical obstruction Aetiology Pathophysiology (Cluster contractions- bowel proximal to the obstruction dilate- wall of obstructed gut is
Radiological Anatomy of Thorax. Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem
 Radiological Anatomy of Thorax Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem Indications for Chest x - A chest x-ray may be used to diagnose and plan treatment for various conditions, including: Diseases/Fractures
Radiological Anatomy of Thorax Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem Indications for Chest x - A chest x-ray may be used to diagnose and plan treatment for various conditions, including: Diseases/Fractures
Perforation of a Duodenal Diverticulum. Elective Student S. C.
 Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
GASTROINTESTINAL SYSTEM
 GASTROINTESTINAL SYSTEM Topographic Anatomy of the Abdomen Surface Landmarks Xiphoid process T9/T10 Inferior costal margin L2/L3 Iliac Crest L4 level ASIS L5/S1 level Pubic symphysis level of greater trochanter
GASTROINTESTINAL SYSTEM Topographic Anatomy of the Abdomen Surface Landmarks Xiphoid process T9/T10 Inferior costal margin L2/L3 Iliac Crest L4 level ASIS L5/S1 level Pubic symphysis level of greater trochanter
Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code
 Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code Herring, W ISBN-13: 9780323074445 Table of Contents 1. Recognizing Anything The "colorful" world of radiology A
Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code Herring, W ISBN-13: 9780323074445 Table of Contents 1. Recognizing Anything The "colorful" world of radiology A
Gastrointestinal Tract Imaging. Objectives. Reference. VMB 960 April 6, Stomach Small Intestine Colon. Radiography & Ultrasound
 Gastrointestinal Tract Imaging VMB 960 April 6, 2009 Stomach Small Intestine Colon Objectives Radiography & Ultrasound Contrast Examination of the Small Intestine Reference Chapters 45 47 Pages 750 805
Gastrointestinal Tract Imaging VMB 960 April 6, 2009 Stomach Small Intestine Colon Objectives Radiography & Ultrasound Contrast Examination of the Small Intestine Reference Chapters 45 47 Pages 750 805
Intestinal Obstruction Clinical Presentation & Causes
 Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Gastrointestinal Pathology. August 2007
 Gastrointestinal Pathology August 2007 Case 1 Dysphagia and halitosis Case 1 Dilatation of the oesophagus with a smooth narrowing of its lower end. The large volume of contained fluid indicates delayed
Gastrointestinal Pathology August 2007 Case 1 Dysphagia and halitosis Case 1 Dilatation of the oesophagus with a smooth narrowing of its lower end. The large volume of contained fluid indicates delayed
DR JAIKISHOR JOTHIRAJ MD POST GRADUATE DEPT OF RADIODIAGNOSIS
 DR JAIKISHOR JOTHIRAJ MD POST GRADUATE DEPT OF RADIODIAGNOSIS YASHODAMMAL 70 YRS OD LADY had C/o diffuse lower abdominal pain 20 days h/o blood in stools 4 days h/o vomiting 2 days h/o burning micturation
DR JAIKISHOR JOTHIRAJ MD POST GRADUATE DEPT OF RADIODIAGNOSIS YASHODAMMAL 70 YRS OD LADY had C/o diffuse lower abdominal pain 20 days h/o blood in stools 4 days h/o vomiting 2 days h/o burning micturation
CT abdomen and pelvis
 CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
Duodenum retroperitoneal
 Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
Policies, Standards, and Guidelines. Guidelines for Abdominal Ultrasound Examination
 Policies, Standards, and Guidelines Guidelines for Abdominal Ultrasound Examination Approved by Council Feb 2018 Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to
Policies, Standards, and Guidelines Guidelines for Abdominal Ultrasound Examination Approved by Council Feb 2018 Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to
No Disclosures. Approach to Abdominal Radiographs
 Approach to Abdominal Radiographs Tapas K. Tejura, M.D. Assistant Professor of Clinical Radiology Keck Medical Center of USC tapas.tejura@med.usc.edu No Disclosures 34-year-old male with acute abdominal
Approach to Abdominal Radiographs Tapas K. Tejura, M.D. Assistant Professor of Clinical Radiology Keck Medical Center of USC tapas.tejura@med.usc.edu No Disclosures 34-year-old male with acute abdominal
Basic Abdominal and Pelvic Imaging Concepts. David L. Smith, MD Assistant Professor of Radiology
 Basic Abdominal and Pelvic Imaging Concepts David L. Smith, MD Assistant Professor of Radiology Basic Imaging Concepts Contrast Resolution vs Spacial Resolution Spacial Resolution......refers to the ability
Basic Abdominal and Pelvic Imaging Concepts David L. Smith, MD Assistant Professor of Radiology Basic Imaging Concepts Contrast Resolution vs Spacial Resolution Spacial Resolution......refers to the ability
Pitfalls in the CT diagnosis of appendicitis
 The British Journal of Radiology, 77 (2004), 792 799 DOI: 10.1259/bjr/95663370 E 2004 The British Institute of Radiology Pictorial review Pitfalls in the CT diagnosis of appendicitis 1 C D LEVINE, 2 O
The British Journal of Radiology, 77 (2004), 792 799 DOI: 10.1259/bjr/95663370 E 2004 The British Institute of Radiology Pictorial review Pitfalls in the CT diagnosis of appendicitis 1 C D LEVINE, 2 O
Request Card Task ANSWERS
 Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
Original Article INTRODUCTION MATERIALS AND METHODS ABSTRACT
 Original Article Diagnostic value of Plain Abdominal Radiograph, Ultrasonography and Clinical impression of the surgeon in acute peritonitis. Ankit Shukla 1, Ramesh Bharti 2, Rajesh Chaudhary 1, Manjeet
Original Article Diagnostic value of Plain Abdominal Radiograph, Ultrasonography and Clinical impression of the surgeon in acute peritonitis. Ankit Shukla 1, Ramesh Bharti 2, Rajesh Chaudhary 1, Manjeet
Gastrointestinal Tract. Anatomy of GI Tract. Anatomy of GI Tract. (Effective February 2007) (1%-5%)
 (1%-5%)") Gastrointestinal Tract (Effective February 2007) (1%-5%) Anatomy of GI Tract Esophagus bulls-eye or target EG junction seen on sagittal scan posterior to left lobe of liver and anterior to aorta Anatomy
Gastrointestinal Tract (Effective February 2007) (1%-5%) Anatomy of GI Tract Esophagus bulls-eye or target EG junction seen on sagittal scan posterior to left lobe of liver and anterior to aorta Anatomy
Volvulus of the Gastrointestinal Tract: x-ray and CT imaging
 Volvulus of the Gastrointestinal Tract: x-ray and CT imaging Poster No.: C-0076 Congress: ECR 2013 Type: Educational Exhibit Authors: E. Papadaki, S. Paschalidou, S. GIANNOU ; Rethymno, CR/ 1 2 2 3 1 3
Volvulus of the Gastrointestinal Tract: x-ray and CT imaging Poster No.: C-0076 Congress: ECR 2013 Type: Educational Exhibit Authors: E. Papadaki, S. Paschalidou, S. GIANNOU ; Rethymno, CR/ 1 2 2 3 1 3
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University.
 Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
The Role of Ultrasound in the Assessment of Inflammatory Bowel Disease
 The Role of Ultrasound in the Assessment of Inflammatory Bowel Disease Dr. Richard A. Beable Consultant Gastrointestinal Radiologist Queen Alexandra Hospital Portsmouth Hospitals NHS Trust Topics for Discussion
The Role of Ultrasound in the Assessment of Inflammatory Bowel Disease Dr. Richard A. Beable Consultant Gastrointestinal Radiologist Queen Alexandra Hospital Portsmouth Hospitals NHS Trust Topics for Discussion
My Patient Has Abdominal Pain PoCUS of the Biliary Tract and the Urinary Tract
 My Patient Has Abdominal Pain PoCUS of the Biliary Tract and the Urinary Tract Objectives PoCUS for Biliary Disease PoCUS for Renal Colic PoCUS for Urinary Retention Biliary Disease A patient presents
My Patient Has Abdominal Pain PoCUS of the Biliary Tract and the Urinary Tract Objectives PoCUS for Biliary Disease PoCUS for Renal Colic PoCUS for Urinary Retention Biliary Disease A patient presents
LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL
 SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
TIPS AND PITFALLS IN PLAIN FILM INTERPRETATION
 TIPS AND PITFALLS IN PLAIN FILM INTERPRETATION Dr Philip Touska MBBS, BMedSci(Hons), MRCS, DO-HNS, FRCR Radiology Fellow Guy s & St Thomas Hospitals LEARNING OBJECTIVES Where do we go wrong? Common pitfalls
TIPS AND PITFALLS IN PLAIN FILM INTERPRETATION Dr Philip Touska MBBS, BMedSci(Hons), MRCS, DO-HNS, FRCR Radiology Fellow Guy s & St Thomas Hospitals LEARNING OBJECTIVES Where do we go wrong? Common pitfalls
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
Radiology of hepatobiliary diseases
 GI cycle - Lecture 14 436 Teams Radiology of hepatobiliary diseases Objectives 1. To Interpret plan x-ray radiograph of abdomen with common pathologies. 2. To know the common pathologies presentation.
GI cycle - Lecture 14 436 Teams Radiology of hepatobiliary diseases Objectives 1. To Interpret plan x-ray radiograph of abdomen with common pathologies. 2. To know the common pathologies presentation.
Suspected Foreign Body Ingestion
 Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
US in non-traumatic acute abdomen. Lalita, M.D. Radiologist Department of radiology Faculty of Medicine ChiangMai university
 US in non-traumatic acute abdomen Lalita, M.D. Radiologist Department of radiology Faculty of Medicine ChiangMai university Sagittal Orientation Transverse (Axial) Orientation Coronal Orientation Intercostal
US in non-traumatic acute abdomen Lalita, M.D. Radiologist Department of radiology Faculty of Medicine ChiangMai university Sagittal Orientation Transverse (Axial) Orientation Coronal Orientation Intercostal
Acquired pediatric esophageal diseases Imaging approaches and findings. M. Mearadji International Foundation for Pediatric Imaging Aid
 Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
SWISS SOCIETY OF NEONATOLOGY. Prenatal diagnosis and postnatal management of meconium pseudocysts
 SWISS SOCIETY OF NEONATOLOGY Prenatal diagnosis and postnatal management of meconium pseudocysts September 2007 2 Burch E, Caduff JH, Hodel M, Berger TM, Neonatal and Pediatric Intensive Care Unit (BE,
SWISS SOCIETY OF NEONATOLOGY Prenatal diagnosis and postnatal management of meconium pseudocysts September 2007 2 Burch E, Caduff JH, Hodel M, Berger TM, Neonatal and Pediatric Intensive Care Unit (BE,
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina
 Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 09/17/2011 Radiology Quiz of the Week # 38 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 09/17/2011 Radiology Quiz of the Week # 38 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Anatomy of the Large Intestine
 Large intestine Anatomy of the Large Intestine 2 Large Intestine Extends from ileocecal valve to anus Length = 1.5-2.5m = 5 feet Regions Cecum = 2.5-3 inch Appendix= 3-5 inch Colon Ascending= 5 inch Transverse=
Large intestine Anatomy of the Large Intestine 2 Large Intestine Extends from ileocecal valve to anus Length = 1.5-2.5m = 5 feet Regions Cecum = 2.5-3 inch Appendix= 3-5 inch Colon Ascending= 5 inch Transverse=
National Museum of Health and Medicine
 National Museum of Health and Medicine Otis Historical Archives Bower Photograph Collection Date of Records: 1910s-1920s Size: 1 box Finding Aid: by Eric W. Boyle (2012) Biographical Note: Col. Morris
National Museum of Health and Medicine Otis Historical Archives Bower Photograph Collection Date of Records: 1910s-1920s Size: 1 box Finding Aid: by Eric W. Boyle (2012) Biographical Note: Col. Morris
Vomiting in children: The good coordination between radiologists and pediatricians is the key to success
 Vomiting in children: The good coordination between radiologists and pediatricians is the key to success C. Santos Montón 1, M. T. Garzon Guiteria 2, A. Hortal Benito-Sendín 1, K. El Karzazi 1, P. Sanchez
Vomiting in children: The good coordination between radiologists and pediatricians is the key to success C. Santos Montón 1, M. T. Garzon Guiteria 2, A. Hortal Benito-Sendín 1, K. El Karzazi 1, P. Sanchez
GENERAL ABDOMINAL IMAGING PERITONEAL SPACE, PANCREAS, & SPLEEN. VMB 960 March 25, 2013
 GENERAL ABDOMINAL IMAGING PERITONEAL SPACE, PANCREAS, & SPLEEN VMB 960 March 25, 2013 REFERENCE Chapters 35-36 Pages 650-678 Chapter 37 Pages 694-701 Chapter 3 Pages 38-49 OBJECTIVES Radiography and Ultrasound
GENERAL ABDOMINAL IMAGING PERITONEAL SPACE, PANCREAS, & SPLEEN VMB 960 March 25, 2013 REFERENCE Chapters 35-36 Pages 650-678 Chapter 37 Pages 694-701 Chapter 3 Pages 38-49 OBJECTIVES Radiography and Ultrasound
Comparative Study between Plain Radiography and Ultrasound Abdomen in Non Traumatic Surgical Acute Abdominal Conditions
 ORIGINAL ARTICLE Comparative Study between Plain Radiography and Ultrasound Abdomen in Non Traumatic Surgical Acute Sharma P 1, Sidharth 2, Singh BP 3, Singh D 3, Gupta A 4 1 Department of Radiology and
ORIGINAL ARTICLE Comparative Study between Plain Radiography and Ultrasound Abdomen in Non Traumatic Surgical Acute Sharma P 1, Sidharth 2, Singh BP 3, Singh D 3, Gupta A 4 1 Department of Radiology and
د. عصام طارق. Objectives:
 GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
Summary and conclusions
 Summary and conclusions 7 Chapter 7 68 Summary and conclusions Chapter 1 provides a general introduction to this thesis focused on the use of ultrasound (US) in children with abdominal problems. The literature
Summary and conclusions 7 Chapter 7 68 Summary and conclusions Chapter 1 provides a general introduction to this thesis focused on the use of ultrasound (US) in children with abdominal problems. The literature
Abdomen and Pelvis CT (1) By the end of the lecture students should be able to:
 By the end of the lecture students should be able to:") RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
Chest X-ray Interpretation
 Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Original Research Article
 Original Research Article Role of (Non Gynaecological Causes) Kaleem Ahmad 1, Rishav Kumar Jain 2, Ashok Yadav 3, Shilpa Vahikar 4 1 Associate Professor, Department of Radiodiagnosis, 2 Professor, Department
Original Research Article Role of (Non Gynaecological Causes) Kaleem Ahmad 1, Rishav Kumar Jain 2, Ashok Yadav 3, Shilpa Vahikar 4 1 Associate Professor, Department of Radiodiagnosis, 2 Professor, Department
Abdominal Assessment
 Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
The peritoneum. Prof. Oluwadiya KS, MBBS, FMCS(Orthop) Website:
 Website:") The peritoneum Prof. Oluwadiya KS, MBBS, FMCS(Orthop) Website: http://oluwadiya.com The peritoneum Serous membrane that lines the abdominopelvic cavity and invests the viscera The largest serous membrane
The peritoneum Prof. Oluwadiya KS, MBBS, FMCS(Orthop) Website: http://oluwadiya.com The peritoneum Serous membrane that lines the abdominopelvic cavity and invests the viscera The largest serous membrane
Nordic Forum - Trauma & Emergency Radiology. Bowel Obstruction: Imaging Update
 Nordic Forum - Trauma & Emergency Radiology Bowel Obstruction: Imaging Update Borut Marincek Institute of Diagnostic Radiology University Hospital Zurich, Switzerland Acute Abdomen Bowel Obstruction Bowel
Nordic Forum - Trauma & Emergency Radiology Bowel Obstruction: Imaging Update Borut Marincek Institute of Diagnostic Radiology University Hospital Zurich, Switzerland Acute Abdomen Bowel Obstruction Bowel
The Alimentary System
 The Alimentary System Contrast Medium: 1. Barium Examinations of different parts of the GI tract require different densities of Barium suspension. The escape of Barium into the peritoneal cavity is extremely
The Alimentary System Contrast Medium: 1. Barium Examinations of different parts of the GI tract require different densities of Barium suspension. The escape of Barium into the peritoneal cavity is extremely
Question 1 History. Likely Diagnosis Differential. Further Investigation or Management. Requires Paediatric Surgical referral for laparotomy
 Question 1 Male newborn spilling green tinged vomit day 1 of life Imaging Abdominal X-Rays performed on 03/05/2012 Upper and lower gastrointestinal contrast studies performed on 03/05/2012 Abdominal X-Rays
Question 1 Male newborn spilling green tinged vomit day 1 of life Imaging Abdominal X-Rays performed on 03/05/2012 Upper and lower gastrointestinal contrast studies performed on 03/05/2012 Abdominal X-Rays
ABDOMEN - GI. Duodenum
 TALA SALEH ABDOMEN - GI Duodenum - Notice the shape of the duodenum, it looks like capital G shape tube which extends from the pyloroduodenal junction to the duodenojejunal junction. - It is 10 inches
TALA SALEH ABDOMEN - GI Duodenum - Notice the shape of the duodenum, it looks like capital G shape tube which extends from the pyloroduodenal junction to the duodenojejunal junction. - It is 10 inches
To describe the liver. To list main structures in porta hepatis.
 GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
Abdomen and Retroperitoneum Ultrasound Protocols
 Abdomen and Retroperitoneum Ultrasound Protocols Reviewed By: Anna Ellermeier, MD Last Reviewed: March 2018 Contact: (866) 761-4200, Option 1 **NOTE for all examinations: 1. If documenting possible flow
Abdomen and Retroperitoneum Ultrasound Protocols Reviewed By: Anna Ellermeier, MD Last Reviewed: March 2018 Contact: (866) 761-4200, Option 1 **NOTE for all examinations: 1. If documenting possible flow
The abdominal Esophagus, Stomach and the Duodenum. Prof. Oluwadiya KS
 The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
ACUTE ABDOMEN IN OLDER CHILDREN. Carlos J. Sivit M.D.
 ACUTE ABDOMEN IN OLDER CHILDREN Carlos J. Sivit M.D. ACUTE ABDOMEN Clinical condition characterized by severe abdominal pain developing over several hours ACUTE ABDOMINAL PAIN Common childhood complaint
ACUTE ABDOMEN IN OLDER CHILDREN Carlos J. Sivit M.D. ACUTE ABDOMEN Clinical condition characterized by severe abdominal pain developing over several hours ACUTE ABDOMINAL PAIN Common childhood complaint
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations
 Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
CHEST & ABDOMINAL X-RAYS MALIKA IBRAHIM CORE MEDICAL TRAINEE BLACKPOOL VICTORIA HOSPITAL DATA INTERPRETATION COURSE FEB 20, 2017
 CHEST & ABDOMINAL X-RAYS MALIKA IBRAHIM CORE MEDICAL TRAINEE BLACKPOOL VICTORIA HOSPITAL DATA INTERPRETATION COURSE FEB 20, 2017 1. Sample x-rays 2. Basic chest x-ray interpretation skills 3. Chest x-ray
CHEST & ABDOMINAL X-RAYS MALIKA IBRAHIM CORE MEDICAL TRAINEE BLACKPOOL VICTORIA HOSPITAL DATA INTERPRETATION COURSE FEB 20, 2017 1. Sample x-rays 2. Basic chest x-ray interpretation skills 3. Chest x-ray
Jhia Anjela D. Rivera 1 1. BS Biology, Department of Biology, College of Science, Polytechnic University of the Philippines
 DIGESTIVE SYSTEM Jhia Anjela D. Rivera 1 1 BS Biology, Department of Biology, College of Science, Polytechnic University of the Philippines DIGESTIVE SYSTEM Consists of the digestive tract (gastrointestinal
DIGESTIVE SYSTEM Jhia Anjela D. Rivera 1 1 BS Biology, Department of Biology, College of Science, Polytechnic University of the Philippines DIGESTIVE SYSTEM Consists of the digestive tract (gastrointestinal
RADIOLOGY (SURGERY) BY MARYAM MALIK Rawalpindi Medical College
 BY MARYAM MALIK Rawalpindi Medical College") RADIOLOGY (SURGERY) BY MARYAM MALIK Rawalpindi Medical College NORMAL BOWEL GAS PATTERN Any part of the bowel may be visible if it contains gas/air within the lumen. Gas/air is of low density and forms
RADIOLOGY (SURGERY) BY MARYAM MALIK Rawalpindi Medical College NORMAL BOWEL GAS PATTERN Any part of the bowel may be visible if it contains gas/air within the lumen. Gas/air is of low density and forms
OUTLINE ANATOMY, RADIOGRAPHY,
 16 ABDOMEN R OUTLINE SUMMARY OF PROJECTIONS, 84 ANATOMY, 85 Abdominopelvic cavity, 85 SUMMARY OF ANATOMY, 86 SUMMARY OF PATHOLOGY, 86 EXPOSURE TECHNIQUE CHART, 87 ABBREVIATIONS, 87 RADIOGRAPHY, 88 Abdominal
16 ABDOMEN R OUTLINE SUMMARY OF PROJECTIONS, 84 ANATOMY, 85 Abdominopelvic cavity, 85 SUMMARY OF ANATOMY, 86 SUMMARY OF PATHOLOGY, 86 EXPOSURE TECHNIQUE CHART, 87 ABBREVIATIONS, 87 RADIOGRAPHY, 88 Abdominal
Interesting Pediatric ultrasound cases. Presented by: Falguni Patel (RDMS, RVT)
") Interesting Pediatric ultrasound cases Presented by: Falguni Patel (RDMS, RVT) Role of ultrasound to rule out Appendicitis Overview: Ultrasound is relatively inexpensive, safe and quick solution to rule
Interesting Pediatric ultrasound cases Presented by: Falguni Patel (RDMS, RVT) Role of ultrasound to rule out Appendicitis Overview: Ultrasound is relatively inexpensive, safe and quick solution to rule
Preview from Notesale.co.uk Page 1 of 34
 Abdominal viscera and digestive tract Digestive tract Abdominal viscera comprise majority of the alimentary system o Terminal oesophagus, stomach, pancreas, spleen, liver, gallbladder, kidneys, suprarenal
Abdominal viscera and digestive tract Digestive tract Abdominal viscera comprise majority of the alimentary system o Terminal oesophagus, stomach, pancreas, spleen, liver, gallbladder, kidneys, suprarenal
DIAGNOSTIC VALUE OF PLAIN ABDOMINAL RADIOGRAPH IN NON TRAUMATIC CAUSES OF ACUTE ABDOMEN
 30 Original article DIAGNOSTIC VALUE OF PLAIN ABDOMINAL RADIOGRAPH IN NON TRAUMATIC CAUSES OF ACUTE ABDOMEN Dr Deepak Rajput ( Associate Professor ) Dr Aashaka Patel ( Resident ) Radio diagnosis Department,
30 Original article DIAGNOSTIC VALUE OF PLAIN ABDOMINAL RADIOGRAPH IN NON TRAUMATIC CAUSES OF ACUTE ABDOMEN Dr Deepak Rajput ( Associate Professor ) Dr Aashaka Patel ( Resident ) Radio diagnosis Department,
FHS Appendicitis US Protocol
 FHS Appendicitis US Protocol Reviewed By: Shireen Khan, MD; Sarah Farley, MD; Anna Ellermeier, MD Last Reviewed: May 2018 Contact: (866) 761-4200 **NOTE for all examinations: 1. If documenting possible
FHS Appendicitis US Protocol Reviewed By: Shireen Khan, MD; Sarah Farley, MD; Anna Ellermeier, MD Last Reviewed: May 2018 Contact: (866) 761-4200 **NOTE for all examinations: 1. If documenting possible
Appropriate Imaging Tests Lead to Meaningful Results. Dr. Richard Wasley May 2011
 Appropriate Imaging Tests Lead to Meaningful Results Dr. Richard Wasley May 2011 Summarize the advantages and limitations of specific imaging tests and why clinical information is so important to radiologists
Appropriate Imaging Tests Lead to Meaningful Results Dr. Richard Wasley May 2011 Summarize the advantages and limitations of specific imaging tests and why clinical information is so important to radiologists
In any operation. Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications.
 In any operation Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications. Abdominal operation I position for operation Supine Abdominal operation I position for
In any operation Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications. Abdominal operation I position for operation Supine Abdominal operation I position for
L o o k L i s t e n F e e l S c a n. Your Pocus Cards For Your Every Day Scanning.
 L o o k L i s t e n F e e l S c a n Your Pocus Cards For Your Every Day Scanning E-FAST Extended Focused Assessment by Sonography in Trauma Subcostal Heart View Pleural Sliding on M-mode (Sea-shore sign)
L o o k L i s t e n F e e l S c a n Your Pocus Cards For Your Every Day Scanning E-FAST Extended Focused Assessment by Sonography in Trauma Subcostal Heart View Pleural Sliding on M-mode (Sea-shore sign)
Computed tomography (CT) imaging review of small bowel obstruction
 imaging review of small bowel obstruction") Computed tomography (CT) imaging review of small bowel obstruction Poster No.: C-1602 Congress: ECR 2010 Type: Educational Exhibit Topic: GI Tract - Small Bowel Authors: A. Vousough, D. S. Prasad ; Aberdeen/UK,
Computed tomography (CT) imaging review of small bowel obstruction Poster No.: C-1602 Congress: ECR 2010 Type: Educational Exhibit Topic: GI Tract - Small Bowel Authors: A. Vousough, D. S. Prasad ; Aberdeen/UK,
Objectives. Pediatric Mortality. Another belly pain. Gastroenteritis. Spewing & Pooing Child 4/18/16
 Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
Exploring Anatomy: the Human Abdomen
 Exploring Anatomy: the Human Abdomen PERITONEUM AND PERITONEAL CAVITY PERITONEUM The peritoneum is a thin serous membrane that lines the abdominal cavity and covers, in variable amounts, the viscera within
Exploring Anatomy: the Human Abdomen PERITONEUM AND PERITONEAL CAVITY PERITONEUM The peritoneum is a thin serous membrane that lines the abdominal cavity and covers, in variable amounts, the viscera within
A novel plain abdominal radiograph sign to diagnose malrotation with volvulus
 A novel plain abdominal radiograph sign to diagnose malrotation with volvulus Nataraja RM 1, Mahomed AA 1* 1. Department of Paediatric Surgery, Royal Alexandra Hospital for Sick Children, Brighton,UK *
A novel plain abdominal radiograph sign to diagnose malrotation with volvulus Nataraja RM 1, Mahomed AA 1* 1. Department of Paediatric Surgery, Royal Alexandra Hospital for Sick Children, Brighton,UK *
Intestinal Obstruction
 By the Name of ALLAH the Most Gracious the Most Merciful Intestinal Obstruction د. أحمد اسامة حسن Specialist in General Surgery and Laparoscopic Surgery To be read in Bailey & Love s Short Practice of
By the Name of ALLAH the Most Gracious the Most Merciful Intestinal Obstruction د. أحمد اسامة حسن Specialist in General Surgery and Laparoscopic Surgery To be read in Bailey & Love s Short Practice of
INTRA-THORACIC AND INTRA-ABDO-MINAL PERFORATION OF THE COLON IN TRAUMATIC DIAPHRAGMATIC
 INTRA-THORACIC AND INTRA-ABDO-MINAL PERFORATION OF THE COLON IN TRAUMATIC DIAPHRAGMATIC Pages with reference to book, From 14 To 16 S. Amjad Hussain, Chinda Suriyapa, Karl Grubaugh ( Depts. of Surger and
INTRA-THORACIC AND INTRA-ABDO-MINAL PERFORATION OF THE COLON IN TRAUMATIC DIAPHRAGMATIC Pages with reference to book, From 14 To 16 S. Amjad Hussain, Chinda Suriyapa, Karl Grubaugh ( Depts. of Surger and
4/16/2017. Learning Objectives. Interpretation of the Chest Radiograph. Components. Production of the Radiograph. Density & Appearance
 Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
Diagnostic Imaging
 www.fisiokinesiterapia.biz Diagnostic Imaging Diagnostic Imaging is no longer limited to radiography. Major technological advancements have lead to the use of new and improved imaging technologies. The
www.fisiokinesiterapia.biz Diagnostic Imaging Diagnostic Imaging is no longer limited to radiography. Major technological advancements have lead to the use of new and improved imaging technologies. The
What can you expect after your ERCP?
 ERCP Explained and respond to bed rest, pain relief and fasting to rest the gut with the patient needing to stay in hospital for only a few days. Some patients develop severe pancreatitis and may require
ERCP Explained and respond to bed rest, pain relief and fasting to rest the gut with the patient needing to stay in hospital for only a few days. Some patients develop severe pancreatitis and may require
Gastroschisis Sequelae and Management
 Gastroschisis Sequelae and Management Mary Finn Gillian Lieberman, MD Primary Care Radiology Beth Israel Deaconess Medical Center Harvard Medical School April 2014 Outline I. Definition and Epidemiology
Gastroschisis Sequelae and Management Mary Finn Gillian Lieberman, MD Primary Care Radiology Beth Israel Deaconess Medical Center Harvard Medical School April 2014 Outline I. Definition and Epidemiology
Case Cholecystoduodenal fistula with migrated gallstone leading to gastric outlet obstruction: Bouveret's syndrome
 Case 14613 Cholecystoduodenal fistula with migrated gallstone leading to gastric outlet obstruction: Bouveret's syndrome Eva De Backer 1, Filip Vanhoenacker 2, 3, 4, Adelard De Backer5 1: Ghent University,
Case 14613 Cholecystoduodenal fistula with migrated gallstone leading to gastric outlet obstruction: Bouveret's syndrome Eva De Backer 1, Filip Vanhoenacker 2, 3, 4, Adelard De Backer5 1: Ghent University,
Midgut. Over its entire length the midgut is supplied by the superior mesenteric artery
 Gi Embryology 3 Midgut the midgut is suspended from the dorsal abdominal wall by a short mesentery and communicates with the yolk sac by way of the vitelline duct or yolk stalk Over its entire length the
Gi Embryology 3 Midgut the midgut is suspended from the dorsal abdominal wall by a short mesentery and communicates with the yolk sac by way of the vitelline duct or yolk stalk Over its entire length the