Electrocardiogram A valuable diagnostic tool. Jean Vorster Netcare Unitas Hospital STEMI Early Reperfusion Initiative 2015
|
|
|
- Darrell Cooper
- 5 years ago
- Views:
Transcription
1 Electrocardiogram A valuable diagnostic tool Jean Vorster Netcare Unitas Hospital STEMI Early Reperfusion Initiative 2015
2 Overview 1. Arrhythmias 2. Structural heart disease 3. Ischaemia
3 Arrhythmias

4

5
6 Sinus Bradycardia 1. Drugs 2. Well-trained athletes 3. Physiological (Sleep adolescents, young adults) 4. Myxedema 5. Hypothermia 6. Gram negative sepsis 7. Vomiting 8. Vasovagal syncope 9. Sick sinus syndrome 10.Intracranial tumors 11.Increased intracranial pressure

7
8 Conduction System

9
10 Conduction System

11
12 2 nd Degree AV Block 1. Increased vagal tone 2. Athletes 3. Sick sinus syndrome 4. Acute carditis 5. Ischaemic heart disease 6. Hypokalemia 7. Digoxin 8. Beta-blockers 9. Calcium-channel blockers
13
14
15 3 rd Degree AV Block 1. Idiopathic (Conduction tissue fibrosis) 2. Congenital 3. Ischaemic heart disease 4. Associated with aortic valve disease (Stenosis) 5. Cardiac surgery and trauma 6. Digoxin toxicity 7. Bundle branch interruption by tumors, granulomas, injury, etc.

16

17

18

19


20 Atrioventricular Nodal Reentry Pathway (AVNRT)

21

22


23 Atrioventricular Reentry Pathway (AVRT)

24

25 Incidental finding of an irregular pulse

26
27 Atrial Fibrillation 1. Most common arrhythmia 2. Fivefold increase in risk of stroke 3. Twofold increase in all-cause mortality 4. Etiology / Underlying substrate: a. Hypertension b. Ischaemic heart disease c. Mitral valve diseased. d.cardiomyopathy (hypertrophic and dilated) e. Hyperthyroidism f. Open heart / thoracic surgery g. Myocardial infarction h. Pericarditis
28 Atrial Fibrillation - Consequences Heart Failure: Loss of atrial contribution to LV filling: Loss of atrial systole decrease in stroke volume: 15 20% Accelerated ventricular response: Decrease in LV diastolic filling time Myocardial ischaemia Tachycardia-induced Cardiomyopathy
29 Atrial Fibrillation - Consequences Systemic Thrombo-embolisation: Loss of atrial systole (contraction / transport function) Stasis of blood in LA Thrombus formation (90% in left atrial appendage) Fragmentation / Embolisation
30 Atrial Fibrillation - Consequences Syncope: Associated arrhythmias: Sick Sinus Syndrome AV blocks Accelerated ventricular response Structural heart disease e.g. Aortic Stenosis (fixed cardiac output) Underlying: Ischaemia LV dysfunction
31 Indications for Warfarin in Atrial Fibrillation 1. CHA 2 DS 2 -VASc Score: C Congestive Heart Failure / LV dysfunction 1 H Hypertension 1 A Age 75 Years 2 D Diabetes Mellitus 1 S Stroke / Transient Ischaemic Attack 2 V Vascular Disease 1 (prior MI / Peripheral Arterial Disease / Aortic plaque) A Age years 1 Sc Sex Category (Female) 1
32 Indications for Warfarin in Atrial Fibrillation CHA 2 DS 2 -VASc Score Recommended Therapy 2 Oral Anticoagulation 1 Oral Anticoagulation preferred 0 No therapy required

33

34
35
36 Atrial Flutter Less common than atrial fibrillation Can occur as a result of atrial dilation from: Septal defects Pulmonary emboli Mitral or tricuspid valve disease (stenosis / regurgitation) Heart failure Aging Can also occur without underlying heart disease: Thyrotoxicosis Alcoholism Pericarditis
37 Cardioversion: Atrial Flutter - Treatment Electrical ( 50J DCC) Chemical anti-arrhythmic drugs (Class IA, IC or III) Ablation: Highly effective (success rate >90%) Preferred approach because of high relapse rate after cardioversion and difficult to control ventricular response with medical therapy (βblockers, Ca-channel antagonist, digoxin or anti-arrhythmic drugs) Risk of thrombo-embolism: Lower than with atrial fibrillation Indications for anticoagulation similar to atrial fibrillation


38 Atrial Flutter

39
40 Ventricular Premature Complexes Occur in association with: Aging Excessive use of Tobacco Caffeine Alcohol Various medications Electrolyte imbalances (e.g. hypokalemia) Ischemic or inflamed myocardium Infections Hypoxia Autonomic stimulation Anesthesia Surgery Importance depends on clinical setting: In the absence of underlying heart disease: No impact on longevity or limitation of activity Anti-arrhythmic drugs are not indicated
41 Ventricular Premature Complexes In the setting of an acute myocardial infarction: Occur in the early phase Seldom cause ventricular fibrillation (VF) Frequent VPC s Multiform configuration Early coupling ( R-on-T ) Repetitive patterns (couplets / salvos) Check for: Recurrent ischemia Electrolyte or metabolic disturbances Maintain S-K + > 4.5mmol/l and S-Mg 2+ > 2mmol/l Β-blocker if sinus tachycardia Low sensitivity and specificity for identifying patients at risk for VF Anti-arrhythmic drugs not indicated, may increase risk for fatal bradycardic and asystolic events


42 82 year old man Smoking history:140 to 150 pack years Severe COPD Severe pulmonary hypertension Dilated right ventricle
43 Chaotic (Multifocal) Atrial Tachycardia Characteristics: Atrial rates between 100 and 130 beats/min Marked variation in P-wave morphology (at least 3 P-wave contours) Irregular P-P intervals Variable PR-intervals Etiology / Associations: COPD Congestive heart failure (elderly patients) Digitalis (unusual cause) Theophylline May develop into atrial fibrillation Treatment: Avoid β-blockers (COPD) Verapamil / Amioderone K- / Mg supplementation


44 46-year old male Mitral valve prolapse Infective endocarditis in 2012 managed medically Rupture of chord with severe mitral regurgitation Underwent mitral valve repair in April 2014 This arrhythmia documented during routine follow up (asymptomatic)
45 Focal Atrial Tachycardia Characteristics: Atrial rates between 150 and 200 beats/min P-wave contour different from sinus P-wave At the onset there may be some warming up of the rate that results in an increase in heart rate over the initial several complexes Frequently occur in short, recurrent burst with spontaneous terminations; may also be incessant Etiology / Associations: Coronary artery disease (with or without myocardial infarction) Heart failure Digitalis intoxication Potassium depletion May develop tachycardia-induced cardiomyopathy if incessant Treatment: β-blockers / Calcium channel blocker Discontinue digitalis K-supplementation

46
47 Accelerated Idioventricular Rhythm Characteristics: Rate: 55 to 110 beats / min Broad QRS complex AV dissociation Setting: Seen in 20% of STEMI patients Frequently occurs in first 2 days Most episodes are of short duration Occurs with about equal frequency in both anterior and inferior infarctions Often seen after successful reperfusion Not a reliable marker of reperfusion Not thought to affect prognosis No treatment required
 Previous inferior")

48 Ischemic Cardiomyopathy (LV ejection fraction = 39%) Previous inferior myocardial infarction CABG graft to right coronary artery Recurrent palpitations (no syncope)
49
50 Etiology: Ventricular Tachycardia (VT) Most patients with symptomatic recurrent VT have ischemic heart disease Sustained VT displays a circadian variation peak frequency in the morning Next largest group has cardiomyopathy (congestive and hypertrophic) Lesser percentages: Inherited ion channel abnormalities Idiopathic VT Congenital heart disease Patients with sustained VT are more likely to have: Reduced ejection fraction ECG abnormalities (e.g., wide QRS) Previous myocardial infarction

51 Polymorphic VT from hypokalemia
52 Ventricular Tachycardia (VT) - Management Acute (Termination): No hemodynamic decompensation: Anti-arrhythmic drug (e.g., Amioderone) Hemodynamic compromise / decompensation: Synchronized DC cardioversion (10 to 50 J) Search for reversible cause: Ischemia Hypotension Hypokalemia Prevention of recurrences or sudden death: Implantable Cardioverter / Defibrillator (ICD): LV ejection fraction < 35% Survivors of cardiac arrest Structural heart disease Sustained VT with hemodynamic decompensation

53

54 ECG and hemodynamic tracing during angiography
55 Ventricular Fibrillation Clinical scenario s: Most commonly in association with coronary artery disease As such a terminal event Most frequently in the morning Anti-arrhythmic drug administration Hypoxia Ischaemia Electrical cardioversion (non-synchronized, faulty) Accidental electrical shock (improperly grounded) AF with pre-excitation (WPW) Severe derangement of cardiac contractility: Terminate fatally or produce significant brain damage within 3 to 5 minutes unless corrective measures are undertaken promptly Management: CPR and non-synchronized DC shock (200 to 400J)
56 Structural
57


58
")
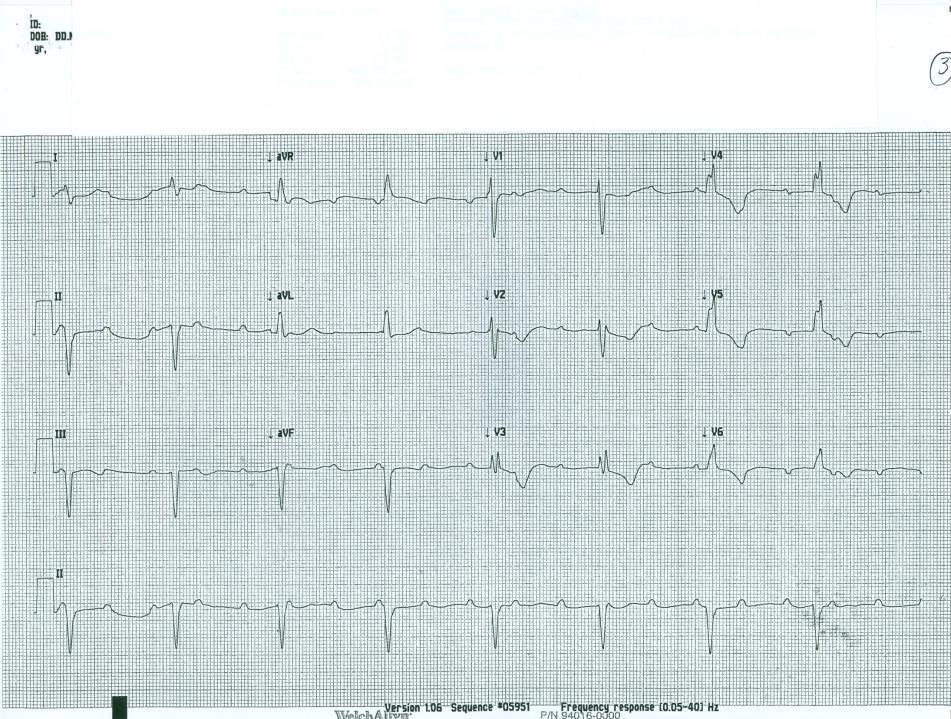
59 67 year old man Presented with unstable angina due to left main stem disease (underwent CABG)

60 Right Bundle Branch Block - Significance 1. Common finding in general population: a. Many people with RBBB have no structural heart disease b. Fragility of RBBB 2. New onset RBBB predicts a higher rate of: a. Coronary artery disease b. Heart failure c. Cardiovascular mortality 3. In the presence of cardiac disease, coexistence of RBBB suggests: a. Advanced disease b. Extensive multi-vessel disease c. Reduced long-term survival in ischaemic heart disease

61

62

63
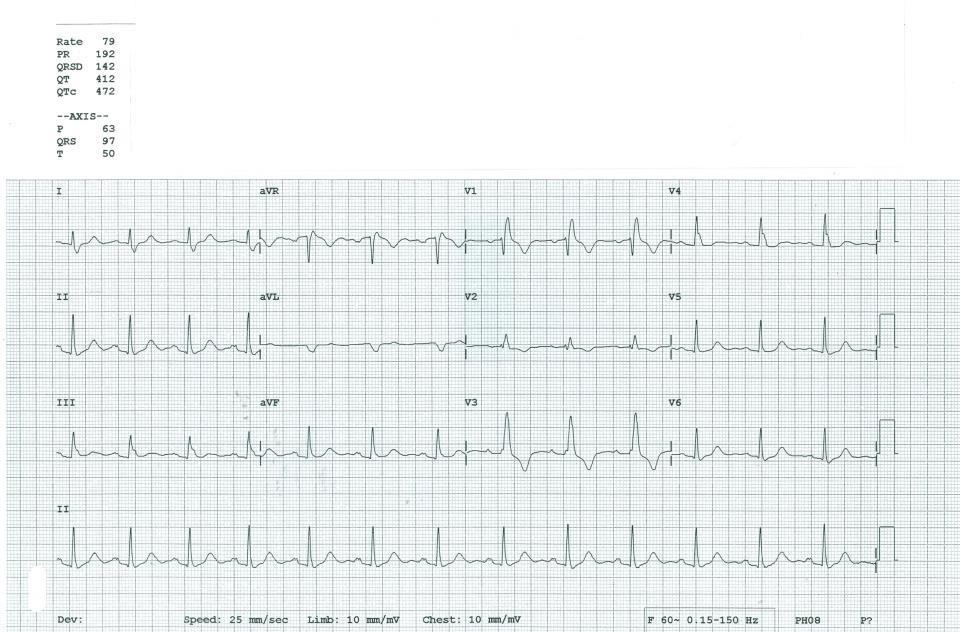
64 Left Bundle Branch Block 1. Criteria: QRS duration >120ms Broad, notched, or slurred R waves in leads I, avl, V 5 and V 6 Prolonged time to peak R wave (>60msec) in V 5 and V 6 2. ST-T wave changes ST-segment and T-wave discordant with QRS complex
65 Left Bundle Branch Block - Significance Usually in patients with underlying heart disease: a. 30% of patients with CCF have LBBB b. 70% of people developing LBBB have preceding LVH (Only 12% of patients with LBBB have no demonstrable disease) Prognostic implications: a. Higher risk of CV mortality from infarction and heart failure b. Higher risk of AV block and cardiac death c. CAD: more extensive disease and LV dysfunction and reduced survival rates Obscuring other ECG patterns: a. Myocardial infarction (ST-segment elevation equivalent) / ischaemia b. LV hypertrophy
")
66 Left Anterior Fascicular (Hemi) Block
67
68 Left Posterior Fascicular (Hemi) Block
69

70

71

72
73 Left Ventricular Hypertrophy 1. Criteria: a. Sokolow Lyon: SV 1 + RV 5/6 > 35mV b. Cornell voltage: SV 3 + RaVL 28mV (men) SV 3 + RaVL 20mV (women) 2. Etiology: a. Hypertension b. Aortic stenosis c. LV outflow tract obstruction
74 Left Ventricular Hypertrophy 1. Other QRS changes in LVH: a. Widening of the QRS complex beyond 110ms b. Delay in the intrinsicoid deflection (ventricular activation) c. Notching of the QRS complex 2. ST-T wave patterns: a. Normal b. Somewhat elevated in leads with tall R-waves c. ST-segment slopes downward from depressed J-point and T-wave is asymmetrically inverted 3. Additional abnormalities: a. Prolongation of QT-interval b. Left atrial abnormality
75 Left Ventricular Hypertrophy - Significance Increased risk for cardiovascular morbidity & mortality: LIFE study Losartan antihypertensive therapy: A 1 SD decrease in Cornell product associated with: 25% decrease in cardiovascular death 17% lower rate of myocardial infarction Repolarization abnormalities: More severe degrees of anatomic LV hypertrophy Greater risk of future cardiovascular events: LIFE study: Significant increases: Risk of cardiovascular death (HR, 2.42) Myocardial infarction (HR, 1.95)

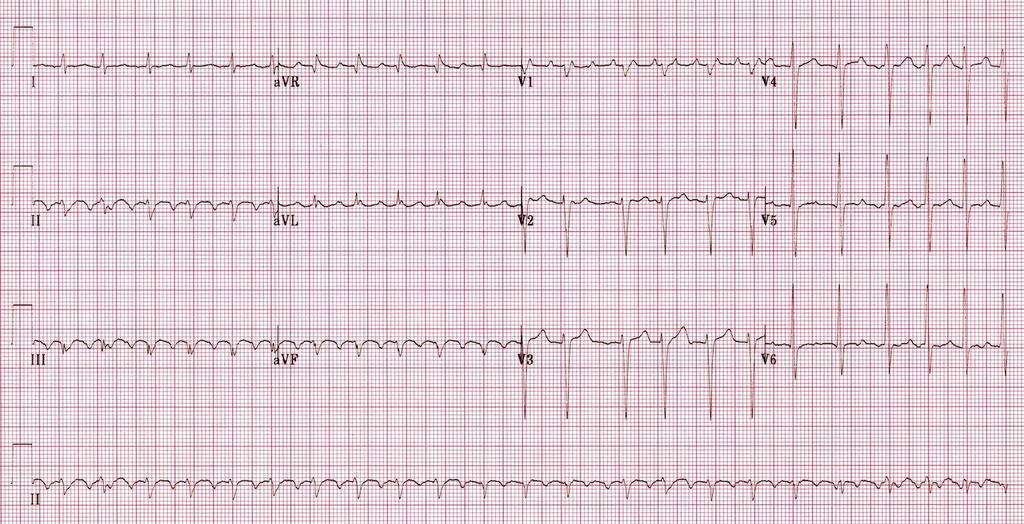
76 74 year old lady Cor Pulmonale with severe pulmonary hypertension secondary to chronic and multiple pulmonary emboli


77 48-year old female Cor Pulmonale Severe Pulmonary hypertension PAP = 75 to 95mmHg Dilated RV and main pulmonary artery, paradoxical septal motion Spontaneous pulmonary embolism in 2007
78 Criteria: Right Ventricular Hypertrophy R in V 1 0.7mV R vs. S ratio in V 1 >1 with R > 0.5mV Right axis deviation (>90 ) P-pulmonale Etiology: Pulmonary hypertension Respiratory disease COPD, Interstitial lung disease Pulmonary emboli Left to right shunting - ASD Idiopathic
79 Ischaemia

80


81 54 year old man with 3 hour duration central chest discomfort Risk factors: Smoking Dyslipidemia Total occlusion of mid LAD

82 After restoring flow to LAD with percutaneous coronary intervention

83
84 47 year old man with an occluded LAD

85

86

87

88

89

90

91

92

93

94


95 38 year old man Ischaemic chestpain

96

97

98

99

100

101

102

103

104

105

106

107 Thank you! Don t be caught between a rock and a hard place!

108

109

110

111

112

113
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Electrical System Overview Electrocardiograms Action Potentials 12-Lead Positioning Values To Memorize Calculating Rates
 Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Ventricular tachycardia Ventricular fibrillation and ICD
 EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
12-Lead ECG Interpretation. Kathy Kuznar, RN, ANP
 12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
Rhythm ECG Characteristics Example. Normal Sinus Rhythm (NSR)
") Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
ECG Interpretation Made Easy
 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
402 Index. B β-blockers, 4, 5 Bradyarrhythmias, 76 77
 Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
Sudden cardiac death: Primary and secondary prevention
 Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
Arrhythmia 341. Ahmad Hersi Professor of Cardiology KSU
 Arrhythmia 341 Ahmad Hersi Professor of Cardiology KSU Objectives Epidemiology and Mechanisms of AF Evaluation of AF patients Classification of AF Treatment and Risk stratification of AF Identify other
Arrhythmia 341 Ahmad Hersi Professor of Cardiology KSU Objectives Epidemiology and Mechanisms of AF Evaluation of AF patients Classification of AF Treatment and Risk stratification of AF Identify other
Acute Coronary Syndromes Unstable Angina Non ST segment Elevation MI (NSTEMI) ST segment Elevation MI (STEMI)
 ST segment Elevation MI (STEMI)") Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
Cardiology/Cardiothoracic
 Cardiology/Cardiothoracic ICD-9-CM to ICD-10-CM Code Mapper 800-334-5724 www.contexomedia.com 2013 ICD-9-CM 272.0 Pure hypercholesterolemia 272.2 Mixed hyperlipidemia 272.4 Other and hyperlipidemia 278.00
Cardiology/Cardiothoracic ICD-9-CM to ICD-10-CM Code Mapper 800-334-5724 www.contexomedia.com 2013 ICD-9-CM 272.0 Pure hypercholesterolemia 272.2 Mixed hyperlipidemia 272.4 Other and hyperlipidemia 278.00
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Cardiac Arrhythmias. Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company
 Cardiac Arrhythmias Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company The Cardiovascular System Three primary functions Transport of oxygen, nutrients, and hormones to
Cardiac Arrhythmias Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company The Cardiovascular System Three primary functions Transport of oxygen, nutrients, and hormones to
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Common Codes for ICD-10
 Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
APPROACH TO TACHYARRYTHMIAS
 APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
Cardiac arrhythmias. Janusz Witowski. Department of Pathophysiology Poznan University of Medical Sciences. J. Witowski
 Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Chapter 16: Arrhythmias and Conduction Disturbances
 Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Cardiology Flash Cards
 Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Ablative Therapy for Ventricular Tachycardia
 Ablative Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS 2 nd Annual UC Davis Heart and Vascular Center Cardiovascular Nurse / Technologist Symposium May 5, 2012 Disclosures Research
Ablative Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS 2 nd Annual UC Davis Heart and Vascular Center Cardiovascular Nurse / Technologist Symposium May 5, 2012 Disclosures Research
December 2018 Tracings
 Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
Basic electrocardiography reading. R3 lee wei-chieh
 Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด
 Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
Skin supplied by T1-4 (medial upper arm and neck) T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio
 T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio") Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
12 Lead ECG Workshop. Virginia Hass, DNP, FNP-C, PA-C Kim Newlin, CNS, ANP-C, FPCNA. California Association of Nurse Practitioners March 18, 2016
 12 Lead ECG Workshop Virginia Hass, DNP, FNP-C, PA-C Kim Newlin, CNS, ANP-C, FPCNA California Association of Nurse Practitioners March 18, 2016 Learning Objectives Identify key changes on the ECG which
12 Lead ECG Workshop Virginia Hass, DNP, FNP-C, PA-C Kim Newlin, CNS, ANP-C, FPCNA California Association of Nurse Practitioners March 18, 2016 Learning Objectives Identify key changes on the ECG which
4/14/15 HTEC 91. Topics for Today. Guess That Rhythm. Premature Ventricular Contractions (PVCs) Ventricular Rhythms
 Ventricular Rhythms") 4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
Pediatrics. Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment. Overview
 Pediatrics Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment See online here The most common form of cardiac arrhythmia in children is sinus tachycardia which can be caused by
Pediatrics Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment See online here The most common form of cardiac arrhythmia in children is sinus tachycardia which can be caused by
Tachycardias II. Štěpán Havránek
 Tachycardias II Štěpán Havránek Summary 1) Supraventricular (supraventricular rhythms) Atrial fibrillation and flutter Atrial ectopic tachycardia / extrabeats AV nodal reentrant a AV reentrant tachycardia
Tachycardias II Štěpán Havránek Summary 1) Supraventricular (supraventricular rhythms) Atrial fibrillation and flutter Atrial ectopic tachycardia / extrabeats AV nodal reentrant a AV reentrant tachycardia
ECGs: Everything a finalist needs to know. Dr Amy Coulden As part of the Simply Finals series
 ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
Myocardial Infarction. Reading Assignment (p66-78 in Outline )
") Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Chapter 2 Practical Approach
 Chapter 2 Practical Approach There are beginners in electrocardiogram (ECG) analysis who are fascinated by a special pattern (e.g., a bundle-branch block or a striking Q wave) and thereby overlook other
Chapter 2 Practical Approach There are beginners in electrocardiogram (ECG) analysis who are fascinated by a special pattern (e.g., a bundle-branch block or a striking Q wave) and thereby overlook other
Advances in Ablation Therapy for Ventricular Tachycardia
 Advances in Ablation Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS Director, Cardiac Electrophysiology Training Program University of California, San Francisco For those of you who
Advances in Ablation Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS Director, Cardiac Electrophysiology Training Program University of California, San Francisco For those of you who
Anti arrhythmic drugs. Hilal Al Saffar College of medicine Baghdad University
 Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Section V. Objectives
 Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Implantable cardioverter defibrillators for the treatment of arrhythmias and cardiac resynchronisation therapy for the treatment of heart failure (review
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Implantable cardioverter defibrillators for the treatment of arrhythmias and cardiac resynchronisation therapy for the treatment of heart failure (review
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
MICS OF MYOCARDIAL ISCHEMIA AND INFARCTION REVISED FOR LAS VEGAS
 ECG MIMICS OF MYOCARDIAL ISCHEMIA AND INFARCTION 102.06.05 Tzong-Luen Wang MD, PhD, JM, FESC, FACC Professor. Medical School, Fu-Jen Catholic University Chief, Emergency Department, Shin-Kong Wu Ho-Su
ECG MIMICS OF MYOCARDIAL ISCHEMIA AND INFARCTION 102.06.05 Tzong-Luen Wang MD, PhD, JM, FESC, FACC Professor. Medical School, Fu-Jen Catholic University Chief, Emergency Department, Shin-Kong Wu Ho-Su
Ventricular arrhythmias
 Ventricular arrhythmias Assoc.Prof. Lucie Riedlbauchová, MD, PhD Department of Cardiology University HospitalMotol and2nd FacultyofMedicine, Charles University in Prague Definition and classification Ventricular
Ventricular arrhythmias Assoc.Prof. Lucie Riedlbauchová, MD, PhD Department of Cardiology University HospitalMotol and2nd FacultyofMedicine, Charles University in Prague Definition and classification Ventricular
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1
 usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1") If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1 mm depth and 3 mm width( most specific) Since Mitral
If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1 mm depth and 3 mm width( most specific) Since Mitral
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders
 C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology)
") ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
Cardiovascular Disorders. Heart Disorders. Diagnostic Tests for CV Function. Bio 375. Pathophysiology
 Cardiovascular Disorders Bio 375 Pathophysiology Heart Disorders Heart disease is ranked as a major cause of death in the U.S. Common heart diseases include: Congenital heart defects Hypertensive heart
Cardiovascular Disorders Bio 375 Pathophysiology Heart Disorders Heart disease is ranked as a major cause of death in the U.S. Common heart diseases include: Congenital heart defects Hypertensive heart
ECG Cases and Questions. Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology
 ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
Electrocardiography Abnormalities (Arrhythmias) 7. Faisal I. Mohammed, MD, PhD
 7. Faisal I. Mohammed, MD, PhD") Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
Management of ATRIAL FIBRILLATION. in general practice. 22 BPJ Issue 39
 Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
ECG Workshop. Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care
 ECG Workshop Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care ECG workshop case study1 44 Year old male. Reports SOB, Lethargy, tiredness. PMH: Hypertension, nil else. What tests? What treatment?
ECG Workshop Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care ECG workshop case study1 44 Year old male. Reports SOB, Lethargy, tiredness. PMH: Hypertension, nil else. What tests? What treatment?
Office ECG Interpretation
 Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
HTEC 91. Performing ECGs: Procedure. Normal Sinus Rhythm (NSR) Topic for Today: Sinus Rhythms. Characteristics of NSR. Conduction Pathway
 Topic for Today: Sinus Rhythms. Characteristics of NSR. Conduction Pathway") HTEC 91 Medical Office Diagnostic Tests Week 3 Performing ECGs: Procedure o ECG protocol: you may NOT do ECG if you have not signed up! If you are signed up and the room is occupied with people who did
HTEC 91 Medical Office Diagnostic Tests Week 3 Performing ECGs: Procedure o ECG protocol: you may NOT do ECG if you have not signed up! If you are signed up and the room is occupied with people who did
Cardiovascular Disease
 Cardiovascular Disease Session Guidelines This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars on the 3 rd Wednesday of each month to address topics related to risk adjustment
Cardiovascular Disease Session Guidelines This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars on the 3 rd Wednesday of each month to address topics related to risk adjustment
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient September 25, 2009
 Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Conduction Problems / Arrhythmias. Conduction
 Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
Diploma in Electrocardiography
 The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
Dos and Don t in Cardiac Arrhythmia. Case 1 -ECG. Case 1. Management. Emergency Admissions. Reduction of TE risk -CHADS 2 score. Hospital Admissions
 Emergency Admissions Dos and Don t in Cardiac Arrhythmia Tom Wong, MD, FESC Consultant Cardiologist, Honorary Senior Lecturer Royal Brompton & Harefield Hospitals National Heart and Lung Institute, Imperial
Emergency Admissions Dos and Don t in Cardiac Arrhythmia Tom Wong, MD, FESC Consultant Cardiologist, Honorary Senior Lecturer Royal Brompton & Harefield Hospitals National Heart and Lung Institute, Imperial
MAT vs AFIB. Henry Clemo. Fast & Easy ECGs, 2E 2013 The McGraw-Hill Companies, Inc. All rights reserved.
 MAT vs AFIB Henry Clemo 1 Multifocal Atrial Tachycardia (MAT) > 3 P wave morphologies HR > 100 HR < 100 wandering pacemaker I 2 Multifocal Atrial Tachycardia 3 Multifocal Atrial Tachycardia 4 Multifocal
MAT vs AFIB Henry Clemo 1 Multifocal Atrial Tachycardia (MAT) > 3 P wave morphologies HR > 100 HR < 100 wandering pacemaker I 2 Multifocal Atrial Tachycardia 3 Multifocal Atrial Tachycardia 4 Multifocal
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT JANUARY 24, 2012
 IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Congestive Heart Failure or Heart Failure
 Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Atrial fibrillation (AF) is a disorder seen
 is a disorder seen") This Just In... An Update on Arrhythmia What do recent studies reveal about arrhythmia? In this article, the authors provide an update on atrial fibrillation and ventricular arrhythmia. Beth L. Abramson,
This Just In... An Update on Arrhythmia What do recent studies reveal about arrhythmia? In this article, the authors provide an update on atrial fibrillation and ventricular arrhythmia. Beth L. Abramson,
Appendix D Output Code and Interpretation of Analysis
 Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
Index of subjects. effect on ventricular tachycardia 30 treatment with 101, 116 boosterpump 80 Brockenbrough phenomenon 55, 125
 145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT
 ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
Dysrhythmias 11/7/2017. Disclosures. 3 reasons to evaluate and treat dysrhythmias. None. Eliminate symptoms and improve hemodynamics
 Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
BUSINESS. Articles? Grades Midterm Review session
 BUSINESS Articles? Grades Midterm Review session REVIEW Cardiac cells Myogenic cells Properties of contractile cells CONDUCTION SYSTEM OF THE HEART Conduction pathway SA node (pacemaker) atrial depolarization
BUSINESS Articles? Grades Midterm Review session REVIEW Cardiac cells Myogenic cells Properties of contractile cells CONDUCTION SYSTEM OF THE HEART Conduction pathway SA node (pacemaker) atrial depolarization
TACHYARRHYTHMIAs. Pawel Balsam, MD, PhD
 TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
A Review of Cardiac Pathophysiology and EKG. Jamie Dyson PT, DPT Kathy Swanick PT, DPT, OCS
 A Review of Cardiac Pathophysiology and EKG Jamie Dyson PT, DPT Kathy Swanick PT, DPT, OCS Cardiac Pathophysiology Coronary Artery Disease Congestive Heart Failure Valvular Heart Disease Athletic Heart
A Review of Cardiac Pathophysiology and EKG Jamie Dyson PT, DPT Kathy Swanick PT, DPT, OCS Cardiac Pathophysiology Coronary Artery Disease Congestive Heart Failure Valvular Heart Disease Athletic Heart
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient October 4, 2007
 Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
The ABCs of EKGs/ECGs for HCPs. Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions
 The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
My Patient Needs a Stress Test
 My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
Management of Arrhythmias The General Practitioners role
 Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
The ECG in healthy people
 The ECG in healthy people The normal cardiac rhythm 3 The heart rate 3 Extrasystoles 7 The P wave 7 The PR interval The QRS complex 3 The ST segment 29 The T wave 33 The QT interval 42 The ECG in athletes
The ECG in healthy people The normal cardiac rhythm 3 The heart rate 3 Extrasystoles 7 The P wave 7 The PR interval The QRS complex 3 The ST segment 29 The T wave 33 The QT interval 42 The ECG in athletes
Return to Basics. Normal Intervals & Axes. ECG Rate and Rhythm
 Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Masqueraders of STEMI
 Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
ARRHYTHMIAS IN THE ICU
 ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
Understanding the 12-lead ECG, part II
 Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Blocks & Dissociations. Reading Assignment (p47-52 in Outline )
") Blocks & Dissociations Reading Assignment (p47-52 in Outline ) Objectives Who are Wenckebach and Mobitz? Review SA and AV Blocks AV Dissociations: learning who s the boss and why 2 nd degree SA Block:
Blocks & Dissociations Reading Assignment (p47-52 in Outline ) Objectives Who are Wenckebach and Mobitz? Review SA and AV Blocks AV Dissociations: learning who s the boss and why 2 nd degree SA Block:
ACLS Study Guide for Precourse Self-Assessment
 20 rhythm strips on Precourse Self-Assessment with the following matching choices: Agonal Rhythm/Asystole Atrial Fibrillation Flutter Ventricular Fibrillation Monomorphic Ventricular Normal Sinus Rhythm
20 rhythm strips on Precourse Self-Assessment with the following matching choices: Agonal Rhythm/Asystole Atrial Fibrillation Flutter Ventricular Fibrillation Monomorphic Ventricular Normal Sinus Rhythm
Chapter 03: Sinus Mechanisms Test Bank MULTIPLE CHOICE
 Instant download and all chapters Tesst Bank ECGs Made Easy 5th Edition Barbara J Aehlert https://testbanklab.com/download/tesst-bank-ecgs-made-easy-5th-edition-barbara-jaehlert/ Chapter 03: Sinus Mechanisms
Instant download and all chapters Tesst Bank ECGs Made Easy 5th Edition Barbara J Aehlert https://testbanklab.com/download/tesst-bank-ecgs-made-easy-5th-edition-barbara-jaehlert/ Chapter 03: Sinus Mechanisms
Supraventricular Arrhythmias. Reading Assignment. Chapter 5 (p17-30)
") Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
DR QAZI IMTIAZ RASOOL OBJECTIVES
 PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
Revisions to the BC Guide for Physicians in Determining Fitness to Drive a Motor Vehicle
 Revisions to the BC Guide for Physicians in Determining Fitness to Drive a Motor Vehicle Thank you for taking the time to review the draft Cardiovascular Diseases and Disorders chapter. Please provide
Revisions to the BC Guide for Physicians in Determining Fitness to Drive a Motor Vehicle Thank you for taking the time to review the draft Cardiovascular Diseases and Disorders chapter. Please provide
InterQual Care Planning SIM plus Criteria 2014 Clinical Revisions
 InterQual Care Planning SIM plus Criteria 2014 Clinical Revisions The Clinical Revisions provide details of changes to InterQual Clinical Criteria. They do not provide information on changes made to CareEnhance
InterQual Care Planning SIM plus Criteria 2014 Clinical Revisions The Clinical Revisions provide details of changes to InterQual Clinical Criteria. They do not provide information on changes made to CareEnhance
CORONARY ARTERIES. LAD Anterior wall of the left vent Lateral wall of left vent Anterior 2/3 of interventricluar septum R & L bundle branches
 CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
ΔΙΑΤΑΡΑΧΕΣ ΕΝΔΟΚΟΙΛΙΑΚΗΣ ΑΓΩΓΙΜΟΤΗΤΑΣ ΔΗΜΗΤΡΙΟΣ Δ. ΜΑΝΩΛΑΤΟΣ Β ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΕΡΓΑΣΤΗΡΙΟ ΗΛΕΚΤΡΟΦΥΣΙΟΛΟΓΙΑΣ Γ.Ν.Α.
 ΔΙΑΤΑΡΑΧΕΣ ΕΝΔΟΚΟΙΛΙΑΚΗΣ ΑΓΩΓΙΜΟΤΗΤΑΣ ΔΗΜΗΤΡΙΟΣ Δ. ΜΑΝΩΛΑΤΟΣ Β ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΕΡΓΑΣΤΗΡΙΟ ΗΛΕΚΤΡΟΦΥΣΙΟΛΟΓΙΑΣ Γ.Ν.Α. «ΕΥΑΓΓΕΛΙΣΜΟΣ» Intraventricular conduction delay and Blocks Right Bundle Branch
ΔΙΑΤΑΡΑΧΕΣ ΕΝΔΟΚΟΙΛΙΑΚΗΣ ΑΓΩΓΙΜΟΤΗΤΑΣ ΔΗΜΗΤΡΙΟΣ Δ. ΜΑΝΩΛΑΤΟΣ Β ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΕΡΓΑΣΤΗΡΙΟ ΗΛΕΚΤΡΟΦΥΣΙΟΛΟΓΙΑΣ Γ.Ν.Α. «ΕΥΑΓΓΕΛΙΣΜΟΣ» Intraventricular conduction delay and Blocks Right Bundle Branch