Knowing is not enough; we must apply. Willing is not enough; we must do.
|
|
|
- Johnathan Richardson
- 5 years ago
- Views:
Transcription
1 Cardiovascular Boot Camp Basic Training Day 2: Cardiac Arrhythmias and Emergency Treatment Overview Cardiac Arrhythmias: Physiologic Links to Recognition and Management NTI 2014 Denver 2014 Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN Contact Information: 1 Knowing is not enough; we must apply. Willing is not enough; we must do. Johann Wolfgang von Goethe 2 1

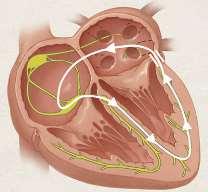
2 Electrical Conduction Pathway SA Node Interatrial pathways AV Node Bundle of His AV Junction Right and Left Bundle Branches Anterior and Posterior Fascicles Purkinge Fibers 3 WAVES and COMPLEXES P QRS P wave: atrial depolarization QRS: ventricular depolarization T wave: ventricular repolarization PR interval: AV conduction time QRS width: intraventricular conduction time ST Segment: sustained ventricular depolarization QT interval: used to reflect ventricular repolarization time QT Interval T PR Interval QRS ST Segment 4 2
3 Overview of Bradyarrhythmias Sinus bradycardia Sinus exist block Sinus Pause or Arrest Junctional Rhythm / Escape Second Degree Type I Second Degree Type II High Grade AV Block Complete Heart Block Idioventricular Rhythm / Ventricular Escape 5 SA Block or SA Exit Block 6 3

4 SA Block or SA Exit Block 7 Sinus Arrest or Sinus Pause 8 4
5 Junctional Escape and Rhythm 9 Wenckebach (2 nd Degree Type I) Note: Progressive lengthening of the PR interval (problem in the AV node) Normal QRS width (no problem in the His Perkinge System) 10 5

6 2 nd Degree Type II Both of these examples: 1. One P wave at a time fails to conduct 2. There is a fixed PR interval 3. There is a wider than normal QRS 11 Heart Blocks - High Grade AV Block Two or more consecutive atrial impulses are blocked. This is not 2 nd degree heart block by definition because more than one P wave in a row fails to conduct. However, this is not complete heart block because there is not complete AV dissociation. 12 6
 or by pacemaker coming from His bundle (narrow QRS less common) 13 Ventricular Escape Beats")
7 Third Degree AV Block Complete No atrial impulses are conducted to the ventricles One form of AV dissociation Ventricular Rate: Maintained by ventricular escape (wide QRS) or by pacemaker coming from His bundle (narrow QRS less common) 13 Ventricular Escape Beats II V


8 Idioventricular Ventricular Rhythm II 15 Classification of SVT Sinus Tachycardia Physiological Inappropriate SANRT Atrial Tachycardia Focal Intra-atrial reentrant Multi-focal AV Nodal Reentrant Tachycardia AV Reentrant Tachycardia Orthodromic Antidromic Atrial Flutter Atrial Fibrillation Junctional Tachycardia Nonparoxysmal JT Junctional ectopic tachycardia 16 8
9 Two Reasons Why a Patient Develops a Tachyarrhythmia Ectopic Foci Focus other than sinus node takes over as pacemaker of heart. Enhanced or abnormal automaticity. Conduction Disturbance An impulse does not travel normally down the conducting pathways but rather finds a way to reenter the conducting pathways Tachycardias with this etiology are called reentrant tachycardias 17 Understanding the Origin of Arrhythmias Disorder of impulse initiation Abnormal automaticity Enhanced Abnormal Triggered mechanism: disturbance in recovery or repolarization (less common) Early or delayed after depolarizations Disorder of impulse conduction Reentrant Circuit (Most common) 18 9
10 Atrial Arrhythmias Organized Atrial tachycardia Atrial Flutter Disorganized Atrial fibrillation 19 Paroxysmal Atrial Tachycardia (PAT) with Block 20 10
11 Multi Focal Paroxysmal Atrial Tachycardia 21 Atrial Flutter 2:1 Conduction 22 11

12 Paroxysmal Atrial Fibrillation Atrial Fibrillation has an irregularly irregular ventricular response. 23 Persistent and Permanent Atrial Fibrillation 24 12


13 AV Nodal Reentrant Tachycardia 25 Arrhythmias of WPW (AVRT or CMT) 26 13

14 27 Antidromic Tachycardia 28 14
15 Example of WPW Atrial Fib (antegrade conduction via accessory pathway) 29 Wide Complex Tachycardias Ventricular Tachycardia SVT with BBB Aberration Torsades de Pointes Atrial Fib with antegrade conduction in WPW AV Reentrant Antidromic Tachycardia in WPW 30 15
16 Acquired Torsade's De Pointes Polymorphic Ventricular Tachycardia preceded by prolonged QT 31 Polymorphic VT with normal QT: Associated with ischemic 32 16


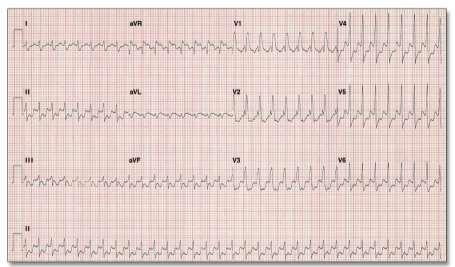
17 Monomorphic VT 33 Ventricular Flutter Spontaneous conversion to NSR (12-lead ECG) 34 17
 35 SVT with")
18 VF with Defibrillation (12-lead ECG) 35 SVT with LBBB 36 18

19 SVT with RBBB 37 Treatments 38 19
20 Treatment: Bradycardias Cessation of drugs slowing conduction through the AV node Beta blockers, calcium channel blockers (diltiazem and verapamil), and digoxin Atropine: For sinus bradycardia and blocks at the level of the AV node Sympathomimetic drugs (i.e. dopamine) to increase rate of impulses from below AV node External pacemaker Temporary transvenous pacemaker Permanent Pacemaker Symptomatic or not? Origin of block or source of escape rhythm? Reversible cause? 39 Fire / Capture Pacing stimulus (fire) results in depolarization of chamber being paced (capture) Pacing spike represent firing Each spike should be followed by a QRS unless it falls in heart s refractory period (capture) Verify Mechanical Pulse! 40 20


21 Loss of Capture Increase ma until capture achieved then set 2-3 times threshold Reposition patient until pacing wire can be repositioned 41 Sensing Pacemaker sees and responds to intrinsic activity Must be given opportunity to sense Must be in demand mode Must be intrinsic activity to be sensed 42 21
22 Loss of Sensing Increase sensitivity by turning sensitivity dial clockwise (makes the mv number smaller pacemaker can see smaller signals) 43 Supraventricular Tachycardias Goal is to decrease ventricular rate Can occur by converting rhythm or by slowing conduction through AV node Vagal maneuvers IV drugs slowing conduction through AV node Adenosine (rapid acting) Diltiazem (verapamil) Digoxin Cardioversion is the treatment in hemodynamically unstable rhythms regardless of etiology 44 22
23 Supraventricular Treatment Examples AVNRT A rapid acting agent (adenosine) is given to convert the patient A timing problem caused AVNRT Slowing of conduction through AV node breaks reentry circuit and allows sinus node to take back over as pacemaker Atrial Fibrillation Do not want to cardiovert if time in atrial fibrillation is unknown A long acting drug is used to slow conduction through AV node Slowing conduction through AV node does not convert because the atria rather than the sinus node are in control Ablation for ectopic and re-entrant tachycardias. 45 Acute Management of Ventricular Arrhythmias Monomorphic VT Antiarrhythmic infusion if stable Amiodarone Procainamide Lidocaine Adenosine can be considered if regular (can be diagnostic) DC cardioversion with sedation if hemodynamically unstable Defibrillation if pulseless Polymorphic VT Normal QT Beta Blockers Revascularization Prolonged QT Magnesium IV Ablation 46 23

24 Congratulations!!! 47 Cardiovascular Boot Camp Basic Cardiac Arrhythmias: Physiologic Links to Training Day 2: Recognition and Management Cardiac Arrhythmias and Emergency Treatment: Narrow Complex Problems NTI 2014 Denver Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN 48 24

25 Blocks and Bradys 49 Propofol Cardiac disorders and medications Vasovagal CNS injury Hypothyroid Hypothermia Multiple other 50 25
26 51 SA Block (SA Exit Block) Type I and Type II P to P interval progressively shortens Fixed P to P Dropped P waves Typically transient Healthy young people Trained athletes Digitalis toxicity Other antiarrhythmics Infarction / myocarditis Part of SSS Quality of sinus node cells Sinus discharge versus atrial activation 52 26
27 SA Block 53 Sinus Arrest or Sinus Pause Failure of impulse formation Impossible definitive diagnosis on surface ECG Clue: PP intervals of cycle cannot be walked out across the pause and end on P wave 54 27
 Syncope 40% SSS: coronary atherosclerosis 5-10% SSS: idiopathic cardiomyopathy 55 Junctional Escape Rhythm HR 35-60 beats per minute P waves may or may not be")
28 Sick Sinus Syndrome Disorders of impulse generation and conduction Failure of escape pacemakers Susceptibility to atrial tachyarrhythmia s Bradycardia / tachycardia syndrome Long pause after tachycardia (overdrive suppression) Syncope 40% SSS: coronary atherosclerosis 5-10% SSS: idiopathic cardiomyopathy 55 Junctional Escape Rhythm HR beats per minute P waves may or may not be associated with QRS complexes QRS complexes same as sinus beats 56 28
29
30 Heart Blocks: AV Blocks Classification 1 st Degree 2 nd Degree Type I (Wenckebach) Type II High Grade Third Degree When the term heart block is used, clinicians are referring to block within, around, or below the AV node. 59 THE DEFINITION OF 2ND DEGREE AV BLOCK IS. One P Wave at a time fails to conduct to ventricle
31 After you determine it is second degree heart block: THEN YOU CAN ASK IF IT IS TYPE 1 OR TYPE What s the difference between Type 1 and Type 2? Not only is the rhythm strip criteria different. It also has to do with the most common physiological location of the block: Type 1 block is usually within the AV node. Type 2 block is below the AV node and usually involves both bundle branches
32 Remember: PR Interval QRS Interval Reflects atrial depolarization (P wave) and time through the AV node (PR segment) Reflects time through the His Purkinje system (His Bundle, Bundle Branches, and Purkinje Fibers) 63 Most often conduction fails within the AV node Therefore: There will be a problem with the PR interval. The QRS remains narrow (unless there is an existing BBB) because the block is in the AV node and does not involve the His Perkinje system. Conduction fails below the AV node and usually involves both bundles There will be no problem with the PR interval (AV node not involved) QRS complex is usually wide (His Perkinje system involved) Can be narrow if the block only involves the Bundle of His 64 32
33 Wenckebach (2 nd Degree Type I) Sinus node fires regularly Disease is in AV node Group beating is noted First P-R of group of often longer than normal with progressive lengthening of the P-R until a beat is not conducted PR problem because of physiological location of the block In absence of BBB QRS is normal Normal QRS width because of physiological location of the block Conduction ratios may be 2:1, 3:2, 4:3 etc. May develop 2:1 conduction if sinus rate increases Verify the block is still type I P-R longer than normal Absence of prolonged QRS Treatment: Often none Acutely with symptoms: Atropine or TTVP Atropine will work because of physiological location Atropine will only work where there are parasympathetic nervous system fibers. These fibers are present in the AV node. 65 Wenckebach (2 nd Degree Type I) Note: Progressive lengthening of the PR interval (problem in the AV node) Normal QRS width (no problem in the His Perkinge System) 66 33
34 Wenckebach (2 nd Degree Type I) Note: This is a patient with a pre-existing RBBB who develops a 2 nd degree Type I block in the bottom strip. Notice the lengthening PR interval (problem in the AV node) until there is a P wave that is not conducted. The QRS is wide in this patient due to the pre-existing RBBB, not due to the development of the 2 nd degree heart block nd Degree AV Block Type II No progressive lengthening of P-R interval Physiological problem does not involve AV node P-R interval is fixed with normally conducted beats Disease within the Bundle of His or below Bundle of His QRS: wide when below the Bundle of His 68 34

35 Both of these examples: 1. One P wave at a time fails to conduct 2. There is a fixed PR interval 3. There is a wider than normal QRS 69 Heart Blocks - High Grade AV Block Two or more consecutive atrial impulses are blocked. P waves: Regular, but 2 or > in a row fail to conduct to the ventricles. This is not 2 nd degree heart block by definition because more than one P wave in a row fails to conduct. In the strip below every third P wave is conducted. This differentiates High Grade AV Block from Complete Heart block which has no conducted P waves


 Symptomatic")

36 71 Third Degree AV Block Complete No atrial impulses are conducted to the ventricles One form of AV dissociation Ventricular Rate: Maintained by ventricular escape (wide QRS) or by pacemaker coming from His bundle (narrow QRS less common) Symptomatic if develops acutely May be well tolerated if develops overtime Treatment: Permanent Pacemaker 72 36
37 Ventricular Escape Beats II V 1 73 Idioventricular Ventricular Rhythm II Ventricular escape rhythms are like having a ventricular pacemaker

38 Two Reasons Why a Patient Develops a Tachyarrhythmia Ectopic Foci Focus other than sinus node takes over as pacemaker of heart. Enhanced or abnormal automaticity. Etiology in atrial tachycardia and often in paroxysmal atrial fibrillation Conduction Disturbance An impulse does not travel normally down the conducting pathways but rather finds a way to re-enter the conducting pathways Tachycardias with this etiology are called re-entrant tachycardias Etiology in atrial flutter, often in atrial fibrillation, and in the two most common forms of PSVT 75 Prerequisites for Re-entrant Tachycardias Available circuit Differing responsiveness in two limbs of circuit Slow Pathway conducts slow; recovers fast Fast Pathway conducts fast; recovers slowly 76 38
39 Supraventricular Arrhythmias (SVA) 77 Supraventricular Tachycardia (SVT) in the broadest sense Covers: All tachycardias originating above the ventricles Supraventricular Arrhythmias (SVA) in ACC/AHA Guidelines excludes Atrial Fibrillation 78 39
40 More on SVT Physiologically based question: If the origin of the tachycardia is above the AV node will the QRS width be narrow or wide? Narrow Why? Because conduction will enter AV node and travel normally through His Perkinje System What two circumstances would result in an exception to the rule? Aberrant conduction due to a refractory BBB Conduction over an accessory pathway 79 Supraventricular Tachycardias Factors determining seriousness of any tachycardia Absolute ventricular rate Size of heart Relationship between atrial and ventricular contraction Presence of additional complications Amount of time in tachycardia Tachycardia mediated cardiomyopathy 80 40

41 Organized Atrial Tachycardias Focal ectopic atrial tachycardia Originate from a point source and activation spreads out from that source. 81 Atrial Tachycardia 1:1 P to QRS P wave different from sinus Rate up 250 minute Regular but may warm up at onset Normal QRS unless aberrant or bundle branch block P wave may be lost in preceding QRS or preceding T wave P not retrograde 82 41


42 Paroxysmal Atrial Tachycardia (PAT) with Block 83 Multi Focal Paroxysmal Atrial Tachycardia Wandering atrial pacemaker with increased rate P waves: three different shapes Absence of one dominant atrial pacemaker Rate > 100 per minute up to 250 P-R interval and R-R interval vary 84 42
43 Multi Focal Paroxysmal Atrial Tachycardia 85 Atrial Flutter Rapid, regular flutter waves at / min Saw tooth II, III, avf (typical) AV conduction is variable 1:1 WPW with conduction over accessory pathway (wider QRS) 2:1 or 3:1 untreated; physiologic block 4:1 Treated Higher degrees of block: AV nodal disease, drugs, increased vagal tone Can use vagal maneuver or drugs for diagnosis QRS usually normal Can have aberration after long - short cycle 86 43


44 87 Atrial Flutter Treatment Difficult to achieve rate and rhythm control with drugs Treatment with ablation Approximately 20% to 25% of all ablations (more common than atrial fibrillation ablation) Excellent short term success of up to 95% At 5 years: Some reports of up to 70% recurrent either atypical atrial flutter or atrial fibrillation Create bidirectional block through isthmus 88 44

45 Saw Tooth Pattern of Typical Atrial Flutter 89 Atrial Flutter 2:1 Conduction 90 45

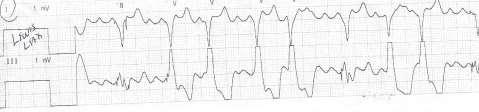
46 91 The Lewis Lead When P waves are not clearly seen in a rhythm strip (see lead 3 above), the Lewis lead can be very helpful in assessing for the presence of atrial activity. As seen in the Lewis lead below, this patient is clearly in an atrial flutter. The atrial flutter is not as obvious in the lead III rhythm strip


47 Lewis Lead 93 V1 MCL6 MCL



48 Lewis Lead Telemetry Pack R A Lead 1 L A 95 Atrial Fibrillation Rapid, irregular fib waves Atrial rate > 350 Fib wave seen best in V1 Irregularly irregular ventricular rate QRS usually normal If QRS is wide and rate > 200 then consider WPW with conduction over accessory pathway 96 48

49 Atrial Fibrillation with Complete Heart Block 97 AV Nodal Reentrant Tachycardia 98 49
50 AV Nodal Re-entrant Tachycardia (AVNRT) Typical A PAC initiates atrial depolarizations which travel via the slow AV nodal pathway the fast pathway is refractory (blocked) due to previous SA node depolarization At the AV node exit depolarizations travel antegrade to depolarize the ventricles and retrograde up the fast pathway to depolarize the atria. This cycle repeats. Slow Fast 99 Typical AV Nodal Re-entrant Tachycardia
51 Typical AV Nodal Re-entrant Tachycardia 101 Typical AV Nodal Re-entrant Tachycardia
52 Typical AV Nodal Re-entrant Tachycardia 103 AV Nodal Reentrant Tachycardia (Typical) Most common supraventricular tachycardia Least likely to be life threatening Narrow QRS has no visible P waves Simultaneous depolarization Or, P waves are so close to QRS they look like part of it (pseudo R waves in V1 and pseudo R waves in inferior leads)
53 Pseudo R Wave V1 105 Pseudo S Wave

54 AVNRT 107 AV Nodal Reentrant Tachycardia
55 II 109 Treatment for AVNRT Vagal (teach patient) Valsalva Carotid massage Facial cold water immersion Adenosine or non-dihydropyridine calcium channel blockers (stable) Adenosine preferred DC Cardioversion (unstable) Ablation : AVNRT is most common reason for cardiac ablation

56 111 Atrioventricular Reciprocating Tachycardias (AVRT) Requires the presence of a bypass tract or accessory pathway Most common: Kent bundles in Wolf Parkinson White Syndrome Pathway can be in several locations: Left lateral free wall, right lateral free wall, and posterior septum


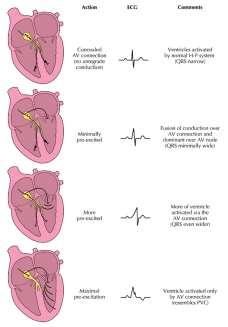
57 Concept of Pre-excitation Termed Pre-excitation because some conduction occurs via the Kent bundles in addition to the normal pathway; because conduction via the Kent bundles is faster than via the AV node the ventricles are pre-excited This produces a delta wave on the EKG Fusion beat Short PR Wider than normal QRS 113 Delta Wave of Pre-excitation Syndrome 60 to 70% of WPW shows evidence in SR Left sided accessory pathway: Positive delta wave in V1 Right sided accessory pathway: Negative delta wave in V


58
 via the accessory pathway. This allows the electrical impulse to re-enter the AV node and stimulate the ventricles once again.")
59 Arrhythmias of WPW (AVRT or CMT) 117 Orthodromic Tachycardia Orthodromic tachycardia occurs when the wave of electrical activation enters the ventricle normally through the AV node and returns to the atrium (retrograde) via the accessory pathway. This allows the electrical impulse to re-enter the AV node and stimulate the ventricles once again. Triggered by PAC conducted down AV node only (no prolonged AV interval), leaves AP non refractory and ready for retrograde conduction


60 119 Orthodromic Tachycardia Negative P in lead 1 = left sided accessory pathway Positive P in lead 1 = right sided accessory pathway

61

62

63
64 T Wave Memory Cardiac memory : the phenomenon whereby the T-wave abnormalities that result from altered depolarization persist after the altered depolarization has ceased Tachyarrhythmias Ventricular pacing 127 Orthodromic AVRT or AVNRT AVNRT Simultaneous depolarization P waves buried Initial P -R interval prolonged (.38 second) Orthodromic AVRT Sequential Depolarization Distinct P waves Initial P -R interval normal Faster rate Accessory pathway required

65 Antidromic Tachycardia The less common form of atrioventricular reentrant tachycardia The path of tachycardia passes from the atrium to the ventricle via the accessory pathway (Kent bundles) and returns to the atrium via the AV node The QRS complex is wide because antegrade conduction bypasses the AV node Antidromic tachycardia is very difficult to distinguish from ventricular tachycardia because ventricular depolarization begins where the accessory pathway enters the ventricle Negative concordance will not be antidromic tachycardia 129 Antidromic Tachycardia


66
67 Atrioventricular Reentrant Tachycardia (AVRT) Orthodromic Traveling down the AV junction and up an accessory pathway Sequential depolarization Narrow because travel via the AV node More common than antidromic tachycardia Antidromic Activation of the ventricles is initiated by impulses descending via an accessory pathway Ventricular depolarization begins at an ectopic site in the myocardium and returns via the AV node Presence of pre-excitation on 12 lead and paroxysmal palpitations. 133 Narrow Complex SVT Orthodromic AVRT or AVNRT AVNRT Simultaneous depolarization P waves buried Initial P -R interval prolonged (.38 second) Orthodromic AVRT Sequential Depolarization Distinct P waves Initial P -R interval normal Faster rate Accessory pathway required

 136")
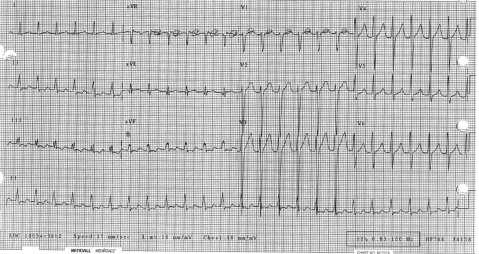
68 AF in WPW Accessory Pathway 135 Example of WPW Atrial Fib (antegrade conduction via accessory pathway)

69 137 Treatment for WPW Tachycardias AV Reentrant (orthodromic) AV Reentrant (antidromic) Atrial Fib with antegrade conduction over accessory pathway Slow conduction over accessory pathway: Amiodarone Procainamide Flecainide Sotalol Propofenone Ibutelide

70

71 Cardiovascular Boot Camp Cardiac Basic Arrhythmias: Training Physiologic Day 2: Links to Recognition and Management Cardiac Arrhythmias and Emergency Treatment: Wide Complex Tachycardias NTI 2014 Denver Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN

72 143 Common Cause of Monomorphic VT
73 Criteria for Differentiating Ectopy from Aberrancy Patient history / assessment QRS Width Concordance AV Dissociation Axis Morphology Note: VT is much more common than supraventricular tachycardia with bundle branch aberration. In wide QRS tachycardias VT is the right answer up to 80% of the time. A wide complex tachycardia is always considered ventricular in origin if the diagnosis is uncertain 145 Patient History Acute ischemia / injury (Abnormal automaticity) Post myocardial infarction / ischemic cardiomyopathy (Reentrant circuit within myocardium) Non ischemic dilated cardiomyopathy (Bundle branch reentrant VT) QRS Width The wider the QRS VT is favored However: SVT with LBBB will have a wider QRS than SVT with RBBB Other causes of SVT with wider than expected QRS: antidromic tachycardia and patients on Class I antiarrhythmics or amiodarone Not all VT is significantly wide VT originating from septum more narrow than VT from free wall If QRS more narrow than sinus rhythm = VT
 is diagnostic for")

74 Negative Concordance 147 AV Dissociation Independent atrial and ventricular activity (AV dissociation) is diagnostic for ventricular ectopy Only seen in 30% VTs Ventricular tachycardia may also have retrograde P waves (retrograde P waves do not confirm VT)
75 AV Dissociation: Fusion or Capture Beats

76 Axis Practice 151 Morphology (Shape) Ventricular Ectopy compared to Aberrancy (BBB) Morphology Challenges: BBB Reentrant VT Idiopathic RVOT Antidromic tachycardia


77 Bedside Cardiac Monitoring LBBB RBBB LVT RVT V1 and V6 are gold standard monitoring leads for ectopy versus aberrancy Bundle branch block patterns and ventricle ectopy can be differentiated by using the morphology of these leads. DON T rely on Lead II!!

78 Right Bundle Branch Block Lead V1 155 Nadir is the distance from the onset of the QRS complex to the lowest point of the S Wave Measure from the beginning of the QRS complex to the bottom valley or peak of the QRS The nadir in V1 should be < 0.06 sec for LBBB (slick down stroke) Left Bundle Branch Lead V
79 RBBB Comparison of Morphology in Lead V1 LBBB VT from Left Ventricle VT from Right Ventricle 157 Physiological Critical Thinking Questions? In a right BBB which ventricle depolarizes first? In a left BBB which ventricle depolarizes first? If VT starts in the left ventricle which ventricle depolarizes first? If VT starts in the right ventricle which ventricle depolarizes first?
80 RBBB Comparison of Morphology in Lead V1 LBBB Left ventricle first Right ventricle first VT from Left Ventricle VT from Right Ventricle Left ventricle first Right ventricle first 159 Left Ventricular Ectopy Lead V1 Right Bundle Branch shaped R wave with an early left peak (Rr ) R wave with a single peak q wave followed by R wave Can also be shape of RBBB
81 Right Ventricular Ectopy Lead V1 LBBB shaped Primarily negative wide rs complex delay to the nadir > 0.06 sec r wave broader than 0.03 sec Slurring on the down stroke Note: LBBB shaped VT can come from RV or septum. VT from RV includes: Idiopathic VT, BB Reentrant VT, Arrhythmogenic right ventricular dysplasia, VT from Brugada Syndrome 161 Comparison of Morphology in Lead V1 RBBB LBBB VT from Left Ventricle VT from Right Ventricle
82 Bundle Branch Block Morphology in Lead V6 RBBB LBBB 163 Ventricular Ectopy Morphology in Lead V6 Left Ventricular VT Right Ventricular VT Morphology in V6 for LVT QS complex r wave followed by S wave with R:S ratio < 1 Morphology in V6 for RVT - Any Q Wave - QS wave
83 Methodology for Differentiation Using ECG / Bedside Monitoring Nice to Knows: AV dissociation, Negative concordance V1-V6, V6 changed from upright to negative, axis changed to right superior YES NO VT V1 positive QRS? V1 negative QRS? SVT with RBBB or VT SVT with LBBB or VT Evaluate QRS Morphology SVT RBBB VT SVT LBBB VT 165 PRACTICE PRACTICE PRACTICE

84 Practice ECG 1 AV Dissociation or Negative Concordance Extreme Axis or V6 Negative SVT RBBB LVT SVT LBBB RVT 167 Practice ECG 2 AV Dissociation or Negative Concordance Extreme Axis or V6 Negative SVT RBBB LVT SVT LBBB RVT

85 Practice ECG 3 AV Dissociation or Negative Concordance Extreme Axis or V6 Negative SVT RBBB LVT SVT LBBB RVT 169 Practice ECG 4 AV Dissociation or Negative Concordance Extreme Axis or V6 Negative SVT RBBB LVT SVT LBBB RVT


86 Practice ECG 5 AV Dissociation or Negative Concordance Extreme Axis or V6 Negative SVT RBBB LVT SVT LBBB RVT 171 Practice ECG 6 AV Dissociation or Negative Concordance Extreme Axis or V6 Negative SVT RBBB LVT SVT LBBB RVT
87 Practice ECG 7 AV Dissociation or Negative Concordance Extreme Axis or V6 Negative SVT RBBB LVT SVT LBBB RVT 173 Practice ECG 8 AV Dissociation or Negative Concordance Extreme Axis or V6 Negative SVT RBBB LVT SVT LBBB RVT


88 Practice ECG 9 AV Dissociation or Negative Concordance Extreme Axis or V6 Negative SVT RBBB LVT SVT LBBB RVT 175 Practice ECG 10 AV Dissociation or Negative Concordance 12 Lead ECG Post Inferior Extreme STEMI on Axis Arrival or V6 to Negative CCU Vital Signs Stable 12 lead ECG Interpretation: Atrial Fibrillation RBBB with Left Anterior Hemiblock SVT RBBB LVT SVT LBBB RVT

89 Practice ECG 11 AV Dissociation or Negative Concordance 12 Lead ECG Post Inferior Extreme STEMI on Axis Arrival or V6 to Negative CCU Vital Signs Stable 12 lead ECG Interpretation: Non Specific Intraventricular Conduction Delay?? SVT RBBB LVT SVT LBBB RVT 177 Linking to the Bedside Monitor Practice ECG 1 SVT RBBB LVT SVT LBBB RVT
90 Linking to the Bedside Monitor Practice ECG 2 SVT RBBB LVT SVT LBBB RVT 179 Linking to the Bedside Monitor Practice ECG 3 SVT RBBB LVT SVT LBBB RVT

91 Linking to the Bedside Monitor Practice ECG 4 SVT RBBB LVT SVT LBBB RVT 181 Linking to the Bedside Monitor Practice ECG 5 SVT RBBB LVT SVT LBBB RVT

92 Linking to the Bedside Monitor Practice ECG 6 SVT RBBB LVT SVT LBBB RVT 183 Case Study SVT RBBB LVT SVT LBBB RVT


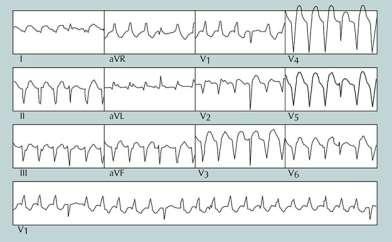
93 Case Study 185 Case Study I avr V1 V4 II avl V2 V5 III avf V3 V
94 The Electronics Action Potential of Cardiac Cells Phase 0: Rapid depolarization Sodium Influx (beginning of QRS complex) Phase 1: Brief, rapid initiation of repolarization 187 The Electronics Phase 2: Slowing of the repolarization Calcium Influx correlates with ST segment Phase 3: Sudden acceleration in the rate of repolarization - Potassium Efflux Correlates with T wave Phase 4: Resting membrane potential
95 189 Dangers of Abnormal Repolarization Places of unequal repolarization can set up for reentrant tachyarrhythmias There can be the development of early after depolarizations
 and ventricular repolarization (T wave) Used most specifically to reflect ventricular")
96 191 QT Interval Measured from beginning of QRS complex to the end of the T wave Reflects both ventricular depolarization (QRS) and ventricular repolarization (T wave) Used most specifically to reflect ventricular repolarization
97 Technical Issues for Consideration Role of QRS width in QT interval Manual versus computer generated measurement U waves End of T wave in biphasic T wave Which lead for measurement RR interval in irregular rhythms Calculated measurement via 12 Lead ECG Bedside monitor calculation via e-calipers Continuous QT interval monitoring software Qtip Study 193 Which Lead for Measurement QT usually measures longest V2 or V3 T wave is often clearest V5 or V6 For repetitive QT interval monitoring in an inpatient setting: Pick a lead with a well defined T wave Use the same lead consistently
98 U Waves and Biphasic T waves. 195 Heart Rate Adjustment QT interval needs to be adjusted for HR QT does not adjust to HR on a beat to beat basis Dynamic changes are most important Abnormal findings are uncovered during abrupt changes in the R to R Irregular heart rhythms (i.e. atrial fibrillation) remain a clinical challenge
99 Assessing for Risk of Torsades de Pointes in Atrial Fibrillation Print a long rhythm strip to assess over the course of the strip if the interval from the R wave to the peak of the following T wave is more than 50% of the proceeding RR interval. If so this is considered too long a QT interval and the risk for Torsades de Pointes is increased. Source: Sommargren & Drew, Measurements are using seconds. Bazett Formula Formula not reliable at slow rates (under estimates); over estimates QT interval at fast HRs QT Dynamics Linear regression analysis
100 Expected QTc Intervals 1 to 15 Years Adult Males Adult Females Normal <.44 seconds <.43 seconds <.45 seconds Borderline.44 to.46 seconds.43 to.45 seconds.45 to.47 seconds Prolonged >.46 seconds >.45 seconds >.47 seconds Source: Moss AJ, Robinson JL. Long QT Syndromes. Heart Dis Stroke. 1992; QTc.50 sec (500 msec or more is dangerous and should be considered an ominous sign of impending Torsade's de Pointes. 199 Torsade's De Pointes Recognition of this life-threatening arrhythmia is important because it is not treated like other VTs Two groups: Acquired and congenital Acquired Drugs prolonging repolarization Most often as a result of blocking the potassium channel Electrolyte abnormalities Low potassium Low magnesium Severe bradycardias / pauses

101 Torsade's De Pointes Poly Morphic VT preceded by prolonged QT 201 More on Drugs that Prolong Repolarization (blocking of potassium channel efflux) Class Ia and Class III antiarrhythmics Antihistamines Antibiotics Antipsychotics Antidepressants Sedatives Gastric motility agents Anticancer agents Opiate agonists Risk Possible Risk Conditional
102 Other Risk Factors for Torsade's de Pointes Rapid (IV) administration of QT prolonging agent Renal or hepatic dysfunction Female gender (particularly for drug induced) Advanced age Anorexia Heart disease Poly pharmacy 203 Warning signs for Torsades de Pointes Increase QTc from predrug baseline of 60 ms, Marked QTc interval prolongation.500 ms T-U wave distortion that becomes more exaggerated in the beat after a pause Visible (macroscopic) T-wave alternans New-onset ventricular ectopy, couplets Nonsustained polymorphic ventricular tachycardia initiated in the beat after a pause
103 Torsade's de Pointes Class I Discontinue offending drugs Note: Class IA drug induced TdP usually appears soon after the initial administration of the drug Correct electrolytes Magnesium Potassium Increase HR Isoproteronol 2 mcg/min then titrate to HR of 100 beats per minute Temporary pacing at rate of 100 to 110 Magnesium is considered treatment of choice. Permanent pacing if bradycardia or CHB cannot be resolved. Defibrillation if sustained However, continue to assess for and treat cause 205 More on Magnesium in Torsade's de Pointes 2 Gm IV bolus over 1-2 minutes Followed in 15 minutes by another bolus if necessary May start continuous infusion at rate of 3-20 mg/min Benefit occurs without shortening of QT interval and in presence of normal Magnesium level

104 207 Case Example

105 Case Example 209 Case Example
 for several years. Recent chemotherapy for breast CA resulting in a reduction of EF.")
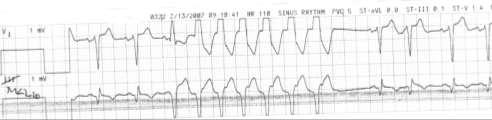
106 QT Interval Monitoring Case Example Patient admitted for syncope after having motor vehicle crash while driving. Long standing history of paroxysmal atrial fibrillation on dofetilide (Tykosin) for several years. Recent chemotherapy for breast CA resulting in a reduction of EF. Recent increase in carvedilol and lisinopril per general cardiology to improve EF. Next slide is admission ECG. Note the QTc interval
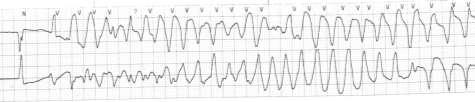
107 1. Strip 1: QTc consistent with admission ECG. 2. Strip 2: Marked QTc prolongation when patient asleep. 3. Initial run of ventricular tachycardia initiated by PVC firing at end of T wave, 213 Same patient with sustained Torsades de Pointes. Treated effectively with 2 grams IV Magnesium (magnesium level was normal at baseline). Magnesium is the drug of choice to stabilize the cardiac membrane. Dofetilide (Tikosyn) was also discontinued. Note: Although the patient had been on dofetilide (Tikosyn) for several years, the recent change in ejection fraction and increase in beta blocker therapy increased her risk for Torsades de Pointes



108 Polymorphic VT with normal QT: Seen frequently in ischemic conditions Think revascularization Think beta blockers


109 217 BE THE BEST THAT YOU CAN BE EVERY DAY. YOUR PATIENTS ARE COUNTING ON IT! Final slides will be available at next week
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Chapter 16: Arrhythmias and Conduction Disturbances
 Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material
 1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
Course Objectives. Proper Lead Placements. Review the ECG print paper. Review the mechanics of the Myocardium. Review basics of ECG Rhythms
 ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
Paramedic Rounds. Tachyarrhythmia's. Sean Sutton Dallas Wood
 Paramedic Rounds Tachyarrhythmia's Sean Sutton Dallas Wood Objectives At the end of this session, the paramedic will be able to: State the key components of the cardiac conduction pathway, along with the
Paramedic Rounds Tachyarrhythmia's Sean Sutton Dallas Wood Objectives At the end of this session, the paramedic will be able to: State the key components of the cardiac conduction pathway, along with the
CORONARY ARTERIES. LAD Anterior wall of the left vent Lateral wall of left vent Anterior 2/3 of interventricluar septum R & L bundle branches
 CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
Case-Based Practical ECG Interpretation for the Generalist
 Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
The most common. hospitalized patients. hypotension due to. filling time Rate control in ICU patients may be difficult as many drugs cause hypotension
 Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT
 ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
ARRHYTHMIAS IN THE ICU
 ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
ECG Interpretation Made Easy
 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University. OBHG Education Subcommittee
 -RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Pediatrics ECG Monitoring. Pediatric Intensive Care Unit Emergency Division
 Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD
 Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
CRC 431 ECG Basics. Bill Pruitt, MBA, RRT, CPFT, AE-C
 CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
Case #1. 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136
 Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT
 Link download full: http://testbankair.com/download/test-bank-for-ecgs-made-easy-5thedition-by-aehlert/ TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT Chapter 5 TRUE/FALSE 1. The AV junction consists
Link download full: http://testbankair.com/download/test-bank-for-ecgs-made-easy-5thedition-by-aehlert/ TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT Chapter 5 TRUE/FALSE 1. The AV junction consists
ECGs on the acute admission ward. - Cardiology Update -
 ECGs on the acute admission ward - Cardiology Update - Dr Simon Fynn Consultant Cardiologist Papworth Hospital, Cambridge RCP London Oct 2017 ECG 1 1. AF with BBB 2. Pre-excited AF 3. SVT with BBB 4.
ECGs on the acute admission ward - Cardiology Update - Dr Simon Fynn Consultant Cardiologist Papworth Hospital, Cambridge RCP London Oct 2017 ECG 1 1. AF with BBB 2. Pre-excited AF 3. SVT with BBB 4.
Paroxysmal Supraventricular Tachycardia PSVT.
 Atrial Tachycardia; is the name for an arrhythmia caused by a disorder of the impulse generation in the atrium or the AV node. An area in the atrium sends out rapid signals, which are faster than those
Atrial Tachycardia; is the name for an arrhythmia caused by a disorder of the impulse generation in the atrium or the AV node. An area in the atrium sends out rapid signals, which are faster than those
ABCs of ECGs. Shelby L. Durler
 ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด
 Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
Presented By: Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN 1
 Presented By: Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN 1 1 st CCU in the world opened in March 1962 was in Toronto, Canada In May of 1962 the 1 st CCU in
Presented By: Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN 1 1 st CCU in the world opened in March 1962 was in Toronto, Canada In May of 1962 the 1 st CCU in
Conduction Problems / Arrhythmias. Conduction
 Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
Fast & Slow Tachy & Brady Arrhythmias DAVID STULTZ, MD, FACC KPN HEART & VASCULAR AUGUST 7, 2017
 Fast & Slow Tachy & Brady Arrhythmias DAVID STULTZ, MD, FACC KPN HEART & VASCULAR AUGUST 7, 2017 Normal EKG EKG boxes Heart Rate 1 big box = 200ms 1 small box = 40ms Big Boxes Between QRS complexes Heart
Fast & Slow Tachy & Brady Arrhythmias DAVID STULTZ, MD, FACC KPN HEART & VASCULAR AUGUST 7, 2017 Normal EKG EKG boxes Heart Rate 1 big box = 200ms 1 small box = 40ms Big Boxes Between QRS complexes Heart
Dr.Binoy Skaria 13/07/15
 Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
BEDSIDE ECG INTERPRETATION
 BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
Supraventricular Tachycardia (SVT)
") Supraventricular Tachycardia (SVT) Daniel Frisch, MD Cardiology Division, Electrophysiology Section Thomas Jefferson University Hospital daniel.frisch@jefferson.edu Short RP Are these the Mid same RP tachycardias?
Supraventricular Tachycardia (SVT) Daniel Frisch, MD Cardiology Division, Electrophysiology Section Thomas Jefferson University Hospital daniel.frisch@jefferson.edu Short RP Are these the Mid same RP tachycardias?
Antiarrhythmic Drugs
 Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
Core Content In Urgent Care Medicine
 Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
Lecture outline. Electrical properties of the heart. Automaticity. Excitability. Refractoriness. The ABCs of ECGs Back to Basics Part I
 Lecture outline The ABCs of ECGs Back to Basics Part I Meg Sleeper VMD, DACVIM (cardiology) University of Florida Veterinary School Electrical properties of the heart Action potentials Normal intracardiac
Lecture outline The ABCs of ECGs Back to Basics Part I Meg Sleeper VMD, DACVIM (cardiology) University of Florida Veterinary School Electrical properties of the heart Action potentials Normal intracardiac
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology)
") ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient September 25, 2009
 Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Supraventricular Tachycardia: From Fetus to Adult. Mohamed Hamdan, MD
 Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Presented By: Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN
 Presented By: Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN 1 1 st CCU in the world opened in March 1962 was in Toronto, Canada In May of 1962 the 1 st CCU in
Presented By: Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN 1 1 st CCU in the world opened in March 1962 was in Toronto, Canada In May of 1962 the 1 st CCU in
TACHYARRHYTHMIAs. Pawel Balsam, MD, PhD
 TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
Relax and Learn At the Farm 2012
 Relax and Learn At the Farm 2012 Session 2: 12 Lead ECG Fundamentals 101 Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Though for Today Mastery is not something that strikes in an instant, like a thunderbolt,
Relax and Learn At the Farm 2012 Session 2: 12 Lead ECG Fundamentals 101 Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Though for Today Mastery is not something that strikes in an instant, like a thunderbolt,
3. AV Block 1. First-degree AV block 1. Delay in AV node 2. Long PR interval 3. QRS complex follows each P wave 4. Benign, no tx
 1. Rhythms & arrhythmias SA nodal rhythms Sinus rhythm Sinus tachycardia Sinus bradycardia Sinus arrhythmia Sick sinus syndrome SA block Sinus arrest AV blocks First-degree Second-degree Mobitz Type I
1. Rhythms & arrhythmias SA nodal rhythms Sinus rhythm Sinus tachycardia Sinus bradycardia Sinus arrhythmia Sick sinus syndrome SA block Sinus arrest AV blocks First-degree Second-degree Mobitz Type I
Ventricular arrhythmias
 Ventricular arrhythmias Assoc.Prof. Lucie Riedlbauchová, MD, PhD Department of Cardiology University HospitalMotol and2nd FacultyofMedicine, Charles University in Prague Definition and classification Ventricular
Ventricular arrhythmias Assoc.Prof. Lucie Riedlbauchová, MD, PhD Department of Cardiology University HospitalMotol and2nd FacultyofMedicine, Charles University in Prague Definition and classification Ventricular
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient October 4, 2007
 Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Cardiology Flash Cards
 Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
FLB s What Are Those Funny-Looking Beats?
 FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
Return to Basics. Normal Intervals & Axes. ECG Rate and Rhythm
 Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Cardiac arrhythmias. Janusz Witowski. Department of Pathophysiology Poznan University of Medical Sciences. J. Witowski
 Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천
 The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천 Differentiation Supraventricular Origin from Ventricular Origin on ECG. QRS-Complex Width. 1. Narrow QRS-Complex Tachycardia (
The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천 Differentiation Supraventricular Origin from Ventricular Origin on ECG. QRS-Complex Width. 1. Narrow QRS-Complex Tachycardia (
ECG Interactive Session
 SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE. Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology
 PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
Study methodology for screening candidates to athletes risk
 1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
The ECG Course. Boone County Fire Protection District EMS Education
 The ECG Course Level I G rated material AV Blocks What Causes AV Block? Long list of bad things that includes ischemia and.. Old age / disease Medications or drugs Electrolyte imbalances Physiologic Blocks
The ECG Course Level I G rated material AV Blocks What Causes AV Block? Long list of bad things that includes ischemia and.. Old age / disease Medications or drugs Electrolyte imbalances Physiologic Blocks
ECG QUIZ Luc DE ROY Brussels Belgium Disclosure in relation to this topic: none
 ECG QUIZ Luc DE ROY Brussels Belgium Disclosure in relation to this topic: none TEST EXAMPLE What is the colour of this rectangle? 1. Blue? 2. Red? 3. Purple? 4. Green? 5. Yellow? 6. 1 and 3? 7. Any of
ECG QUIZ Luc DE ROY Brussels Belgium Disclosure in relation to this topic: none TEST EXAMPLE What is the colour of this rectangle? 1. Blue? 2. Red? 3. Purple? 4. Green? 5. Yellow? 6. 1 and 3? 7. Any of
ECGs: Everything a finalist needs to know. Dr Amy Coulden As part of the Simply Finals series
 ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
Supraventricular Arrhythmias. Reading Assignment. Chapter 5 (p17-30)
") Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
Ventricular tachycardia Ventricular fibrillation and ICD
 EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
Relax and Learn at the FARM 2012: Session 8: 12 Lead ECG 401: ECG Variants
 Relax and Learn at the FARM 2012: Session 8: 12 Lead ECG 401: ECG Variants A Ship in the Harbor is Safe But that is not what ships are built for. Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN Cardiovascular
Relax and Learn at the FARM 2012: Session 8: 12 Lead ECG 401: ECG Variants A Ship in the Harbor is Safe But that is not what ships are built for. Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN Cardiovascular
Atrial Fibrillation 10/2/2018. Depolarization & ECG. Atrial Fibrillation. Hemodynamic Consequences
 Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
PACEMAKER INTERPRETATION AND DEVICE MANAGEMENT PART I
 1 PACEMAKER INTERPRETATION AND DEVICE MANAGEMENT PART I Cynthia Webner DNP, RN, CCNS, CCRN-CMC Karen Marzlin DNP, RN, CCNS, CCRN-CMC 2 PROFESSIONAL NURSING PRACTICE CAN ONLY ADVANCE AS MUCH AS INDIVIDUAL
1 PACEMAKER INTERPRETATION AND DEVICE MANAGEMENT PART I Cynthia Webner DNP, RN, CCNS, CCRN-CMC Karen Marzlin DNP, RN, CCNS, CCRN-CMC 2 PROFESSIONAL NURSING PRACTICE CAN ONLY ADVANCE AS MUCH AS INDIVIDUAL
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
Anti arrhythmic drugs. Hilal Al Saffar College of medicine Baghdad University
 Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Miscellaneous Stuff Keep reading the Outline
 Miscellaneous Stuff Keep reading the Outline Welcome to the 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic measurements:
Miscellaneous Stuff Keep reading the Outline Welcome to the 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic measurements:
EKG Rhythm Interpretation Exam
 as EKG Rhythm Interpretation Exam Name: Date: ID# Unit Assume each strip is a 6 second strip. Passing is 80%. 1. Identify the following rhythm: a. Asystole b. Ventricular fibrillation c. Atrial fibrillation
as EKG Rhythm Interpretation Exam Name: Date: ID# Unit Assume each strip is a 6 second strip. Passing is 80%. 1. Identify the following rhythm: a. Asystole b. Ventricular fibrillation c. Atrial fibrillation
2017 EKG Workshop Advanced. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs
 EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important step for
EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important step for
12 Lead ECG Skills: Building Confidence for Clinical Practice. Presented By: Cynthia Webner, BSN, RN, CCRN-CMC. Karen Marzlin, BSN, RN,CCRN-CMC
 12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
Dr. Schroeder has no financial relationships to disclose
 Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)
 PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)") 1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
Lake EMS Basic EKG Review: Atrial Rhythms. The Lake EMS Quality Development Team
 Lake EMS Basic EKG Review: Atrial Rhythms The Lake EMS Quality Development Team This program is the Intellectual Property of Lake Emergency Medical Services Use of this program is limited to training and
Lake EMS Basic EKG Review: Atrial Rhythms The Lake EMS Quality Development Team This program is the Intellectual Property of Lake Emergency Medical Services Use of this program is limited to training and
Rhythm ECG Characteristics Example. Normal Sinus Rhythm (NSR)
") Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/AV Blocks Connie J. Mattera, M.S., R.N., EMT-P
 Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/ Connie J. Mattera, M.S., R.N., EMT-P Reading assignments: Bledsoe Vol. 3: pp. 88-93; 120-121 (atropine, norepinephrine,
Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/ Connie J. Mattera, M.S., R.N., EMT-P Reading assignments: Bledsoe Vol. 3: pp. 88-93; 120-121 (atropine, norepinephrine,
You Don t Want to Miss This One! Focus on can t miss EKG tracings
 You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013 Wolff-Parkinson-White syndrome (WPW) is a syndrome of pre-excitation of the
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013 Wolff-Parkinson-White syndrome (WPW) is a syndrome of pre-excitation of the
WPW syndrome and AVRT
 WPW syndrome and AVRT Myung-Yong Lee, MD, PhD Division of Cardiology Department of Internal Medicine School of Medicine Dankook University, Cheonan, Korea Supraventricular tachycardia (SVT) Paroxysmal
WPW syndrome and AVRT Myung-Yong Lee, MD, PhD Division of Cardiology Department of Internal Medicine School of Medicine Dankook University, Cheonan, Korea Supraventricular tachycardia (SVT) Paroxysmal
Sustained tachycardia with wide QRS
 Sustained tachycardia with wide QRS Courtesy from Prof. Antonio Américo Friedmann. Electrocardiology Service of University of Faculty of São Paulo. Opinions from colleagues Greetings to everyone, In a
Sustained tachycardia with wide QRS Courtesy from Prof. Antonio Américo Friedmann. Electrocardiology Service of University of Faculty of São Paulo. Opinions from colleagues Greetings to everyone, In a
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
a lecture series by SWESEMJR
 Electrolyte disturbances Hypokalaemia Decreased extracellular potassium increases excitability in the myocardial cells and consequently the effect of very severe hypokalaemia is ventricular arrhythmia.
Electrolyte disturbances Hypokalaemia Decreased extracellular potassium increases excitability in the myocardial cells and consequently the effect of very severe hypokalaemia is ventricular arrhythmia.
ECG CONVENTIONS AND INTERVALS
 1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
ECG Interpretation. Introduction to Cardiac Telemetry. Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services
 ECG Interpretation Introduction to Cardiac Telemetry Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services Disclosures Nothing to disclose Objectives Describe the electrical conduction pathway in
ECG Interpretation Introduction to Cardiac Telemetry Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services Disclosures Nothing to disclose Objectives Describe the electrical conduction pathway in
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
Diploma in Electrocardiography
 The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
Cardiovascular Nursing Education Associates Carol Jacobson RN, MN
 CMC Certification Review Arrhythmias and Arrhythmia Therapy Cardiovascular Nursing Education Associates Carol Jacobson RN, MN www.cardionursing.com Bradycardias & Blocks www.cardionursing.com 1 Sinus Node:
CMC Certification Review Arrhythmias and Arrhythmia Therapy Cardiovascular Nursing Education Associates Carol Jacobson RN, MN www.cardionursing.com Bradycardias & Blocks www.cardionursing.com 1 Sinus Node:
Dysrhythmias. Dysrythmias & Anti-Dysrhythmics. EKG Parameters. Dysrhythmias. Components of an ECG Wave. Dysrhythmias
 Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
Intermediate ECG Course - Part 4. Joe M. Moody, Jr, MD UTHSCSA and STVAHCS
 Intermediate ECG Course - Part 4 Joe M. Moody, Jr, MD UTHSCSA and STVAHCS Topics in Intermediate ECG Consolidation of prior information with additional details Not advanced, but feel free to ask advanced
Intermediate ECG Course - Part 4 Joe M. Moody, Jr, MD UTHSCSA and STVAHCS Topics in Intermediate ECG Consolidation of prior information with additional details Not advanced, but feel free to ask advanced
Arrhythmias. Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center
 Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Electrocardiography Abnormalities (Arrhythmias) 7. Faisal I. Mohammed, MD, PhD
 7. Faisal I. Mohammed, MD, PhD") Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
ELECTROCARDIOGRAPHY KEVIN REBECK PA-C. For more presentations
 ELECTROCARDIOGRAPHY KEVIN REBECK PA-C For more presentations www.medicalppt.blogspot.com Objectives ECG History Pathophysiology Basics Case Historys Electrical activation of the heart In the heart
ELECTROCARDIOGRAPHY KEVIN REBECK PA-C For more presentations www.medicalppt.blogspot.com Objectives ECG History Pathophysiology Basics Case Historys Electrical activation of the heart In the heart
Pathologic ECG. Adelina Vlad, MD PhD
 Pathologic ECG Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze the morphology and
Pathologic ECG Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze the morphology and
Basic electrocardiography reading. R3 lee wei-chieh
 Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Clinical Cardiac Electrophysiology
 Clinical Cardiac Electrophysiology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of
Clinical Cardiac Electrophysiology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of