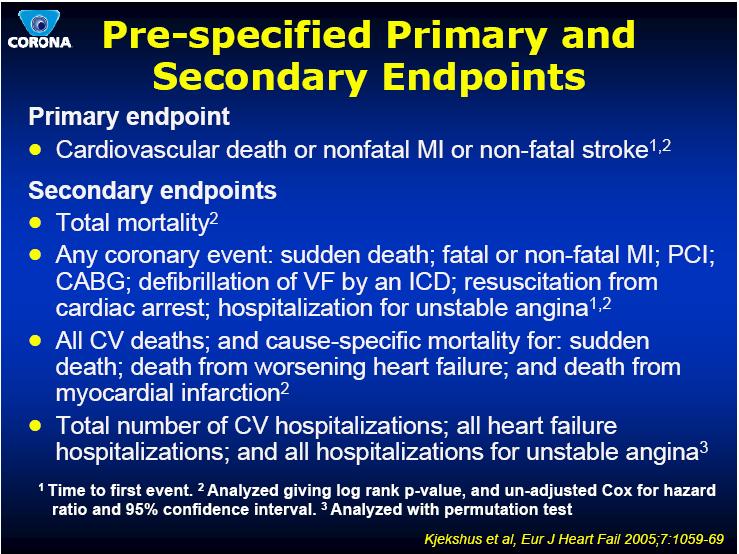
Statins in the Treatment of Heart Failure: Failed Concept?
|
|
|
- Evangeline Lee
- 5 years ago
- Views:
Transcription
1 Statins in the Treatment of Heart Failure: Failed Concept? Tamara Horwich, MD, MS Assistant Professor of Medicine Division of Cardiology March 16, 2012
2 Background: Heart Failure and Statins
3 Heart Failure in the U.S. Prevalence Incidence 5.7 million 670,000 cases/ year Lifetime Risk 1 out of 5 5-year outcomes Est. Expenditures % mortality $37 billion HF due to CAD ~ 50-75% AHA Heart Disease and Stroke Statistics 2009 update. Lloyd-Jones DM et al. Circulation.
4 ACC/AHA Recommendations for Symptomatic, Systolic Heart Failure Class I Diuretics Salt restriction ACEI (or ARB) Beta-blocker Exercise Implantable Cardioverter Defibrillator Biventricular Pacemaker (if QRS>120ms) Aldosterone Antagonist Class IIA Digoxin Hydralazine / Isosorbide Dinitrate Hunt et al. J Am Coll Cardiol 2005;46:
5 CHD and Risk Equivalents in Hospitalized HF Patients: ADHERE Registry n=105,388 from 10/2001 to 12/2003 Coronary Artery Disease (%) Myocardial Infarction (%) Hypertension (%) Stroke of TIA (%) Peripheral Vascular Disease (%) Current Smoker (%) Chronic Renal Insufficiency (%) Chronic Dialysis (%) Diabetes (%) Insulin Treated Diabetes (%) The Nation ADHERE: 267 US Hospitals; 105,388 patients Fonarow Rev Cardiovasc Med 2003;4:S21-30.
6 Use of Medications in Patients Hospitalized with HF ADHERE (N = 187,565) OPTIMIZE-HF (N = 48,612) EVEREST (N = 4,133) Admission Discharge Admission Discharge Admission Discharge Diuretics ACEI ARB Aldost Antagonist β-blockers Digoxin Nitrates CCB?? Aspirin ?? Warfarin ?? Lipid Lowering Agent Adams KF Jr, et al. Am Heart J. 2005;149: Fonarow GC, et al. JAMA 2007;297: Konstam, M. A. et al. JAMA 2007;297:
7 10-year CHD death rate (Deaths/1000) CHD indications per 1000 Relationship Between Cholesterol and CHD Risk: Epidemiologic Trials Multiple Risk Factor Intervention Trial (MRFIT) (n=361,662) Framingham Study (n=5209) Serum cholesterol (mg/dl) 1% reduction in total cholesterol is associated with a 2% decrease in CHD risk Serum cholesterol (mg/100 ml) Each 1% increase in total cholesterol level is associated with a 2% increase in CHD risk Gotto AM Jr, et al. Circulation. 1990;81: Castelli WP. Am J Med. 1984;76:4-12.
8 In Heart Failure, the Reverse is True. Higher Cholesterol Levels are Associated with Reduced Mortality Mortality, % TC< TC> p= p= p= total cohort (n=1134) Ischemic CMY (n=542) Non-ischemic CMY (n=592) Horwich, Fonarow et al. J Card Fail 2002;8:

9 Even if TC and LDL are not Risk Factors in Heart Failure - Potential Benefits of Statins in Heart Failure
10 Impact of HMG CoA Reductase Inhibitor Therapy on Risk of Developing Heart Failure Probability of CHF % Placebo p = % risk reduction Sim vastatin 5 year risk Patients with coronary artery disease and cholesterol > 212 mg/dl Kjekshus J of Cardiac Failure 1997;4:249-54
11 Observational Studies of Statins in Heart Failure show Marked Benefit
12 Survival (%) Survival (%) Observational Study: Statins in Patients with Advanced, Chronic HF Ischemic HF Non-ischemic HF Statin Statin P < No Statin P < No Statin Months Months n = 551 advanced HF patients 51% of patients on statins (79% of CAD and 29% of non-cad) Horwich, MacLellan, and Fonarow. J Am Coll Cardiol; 2004;43:
13 Horwich and Fonarow. J Card Fail 2004; 10:S98. Statins Are Associated with Improved HF Survival Independent of Total Cholesterol Level Univariate Adjusted* TC 162 mg/dl HR = 0.51 ( ) Adjusted HR = 0.52 ( ) TC > 162 mg/dl HR = 0.46 ( ) Adjusted HR = 0.24 ( ) Statin Better No Statin Better
14 Statin Therapy is Associated with Lower Mortality In Severe HF PRAISE study analysis: 1153 patients with severe heart failure, 12% statin use Mozaffarian Am J Cardiol 2004;93:
15 Additional Observational Studies of Statins in Heart Failure Val-HeFT: 1602 of 3408 on statins, 2 year mortality 20.3% vs 17.9%, HR 0.81, P=0.029 CIBIS II: 226 of 2647 on statins, survival 98.3% in statin/bisoprolol vs 87.2% in the no statin/bisoprolol group COMET: 21% of 3029 on statins, statin use adjusted HR 0.75, P<0.001 ICONS Registry: 14% of 4888 pts discharge on statin after HF hospitalizaiton, discharge statin HR 0.65 (95% CI ) P<0.0001
16 Small Prospective Studies of Statins in Heart Failure with Surrogate Endpoints
17 Statins and Inflammation in Humans with Non-Ischemic Heart Failure Baseline 12-month F/U Placebo Atorvastatin Placebo Atorvastatin N=54 N=54 N=54 N=54 hscrp * IL * TNF-a RII * Sola S et al. J Am Coll Cardiol 2006; 47:332-37
18 Statins and Cardiac Remodeling in Humans Simvastatin 3 months in subjects with nonischemic HF Node K et al. Circulation 2003
19 Effects of High-Dose HMG CoA Reductase Inhibitor Therapy on Ventricular Remodeling Placebo n=40 Rosuvastatin n=46 P value Reduction in LDL +3% -51% <0.001 LVEF (%) n.s. LVEDD (mm) n.s. LVESD (mm) n.s. 86 subjects with HF were randomized to Placebo or Rosuvastatin 40mg/day 6 months. No change seen in any biomarkers (BNP, ET-1, hscrp, NE, TNF or IL-6) Krum H et al., J Card Fail :1-7
20
21
22
23
24
25 Time out: Composite Endpoints Measurable events that lie on a pathophysiologic spectrum; used to quantify overall treatment effect Frequently used in clinical trials (37%) Reduces sample size requirements, and thus cost of trial WARNING: soft but more frequent clinical endpoints (eg. Re-intervention, biomarker elevation) vs. hard but less frequent endpoints (eg. Death, disabling stroke) can drive the effect of therapy on the composite Kaul and Diamond. JACC 2010; 55:
26 PAMI Stent vs. angioplasty Heterogeneity across clinical endpoints HOPE Ramipril vs. placebo No heterogeneity Supports credibility and validity of compositie endpoint TRITON TIMI 38 Prasugrel vs. clopidogrel Efficacy endpoints combined with safety endpoints masks harmful effect Kaul and Diamond. JACC 2010; 55:
27
28
29
30
31

32
33
34

35
36

37
38
39
40 Recently published subgroup analysis CONCLUSIONS: Patients with heart failure due to ischemic heart disease who have NT-proBNP values <103 pmol/l (868 pg/ml) may benefit from rosuvastatin. Cleland et al. JACC 2009; 54:
41 Time out: Subgroup Analyses Problems Lack of pre-specification Testing of large number of subgroups without the use of statistical adjustment for interactions and multiple comparisons 20 subgroups : 0.64 chance of false positive False negatives can occur because of underpowering Should be considered exploratory and need to be confirmed Kaul and Diamond. JACC 2010; 55:
42
43

44
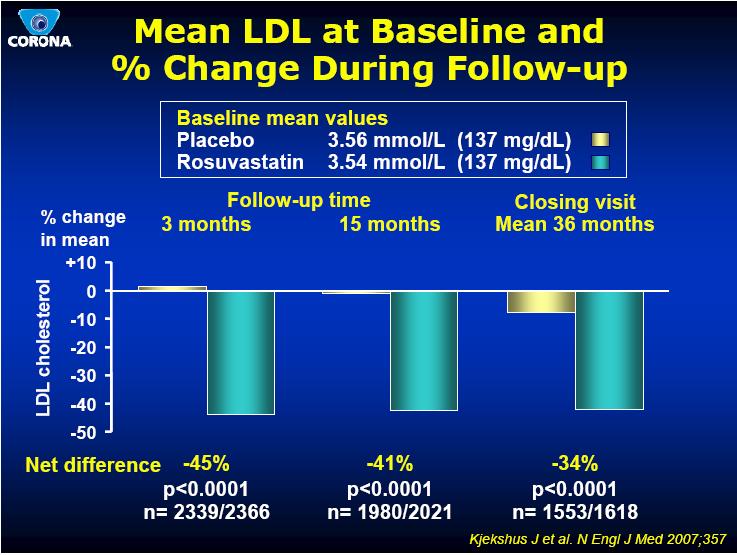
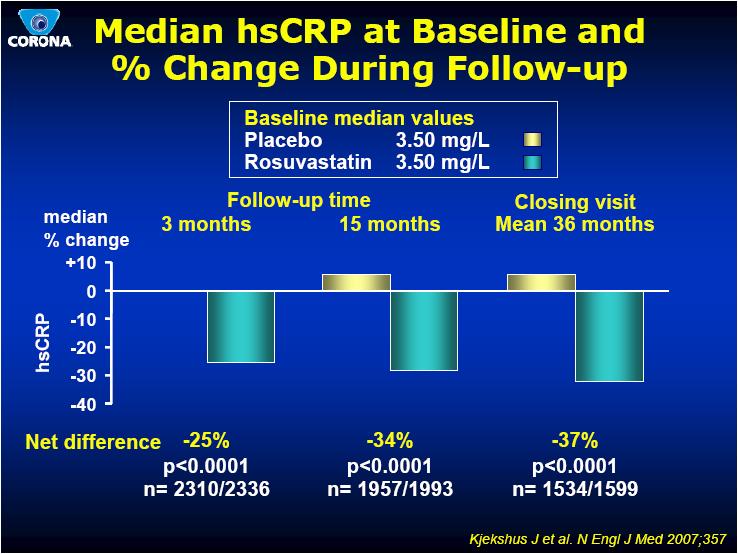
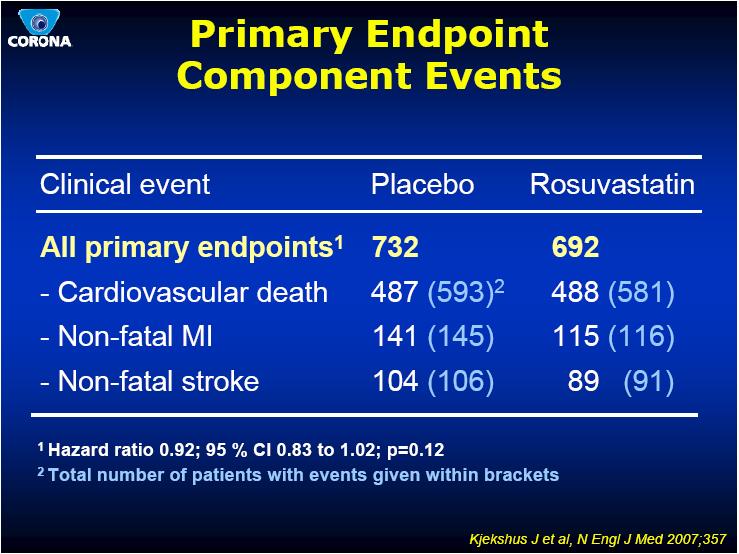
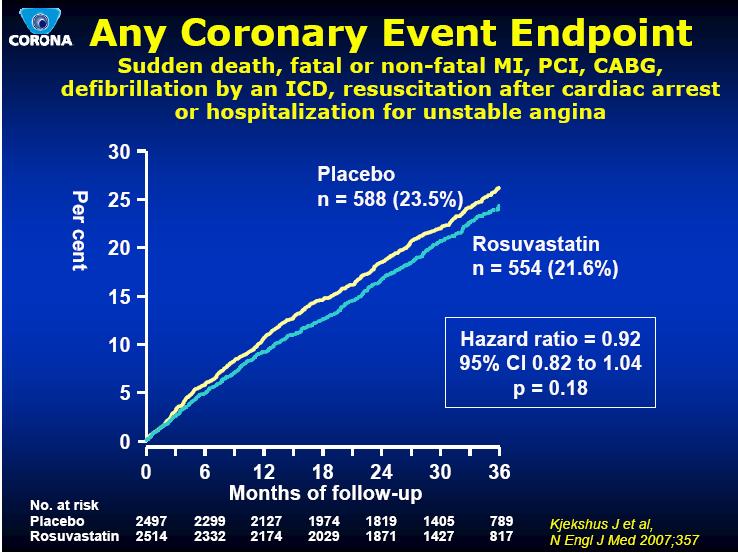
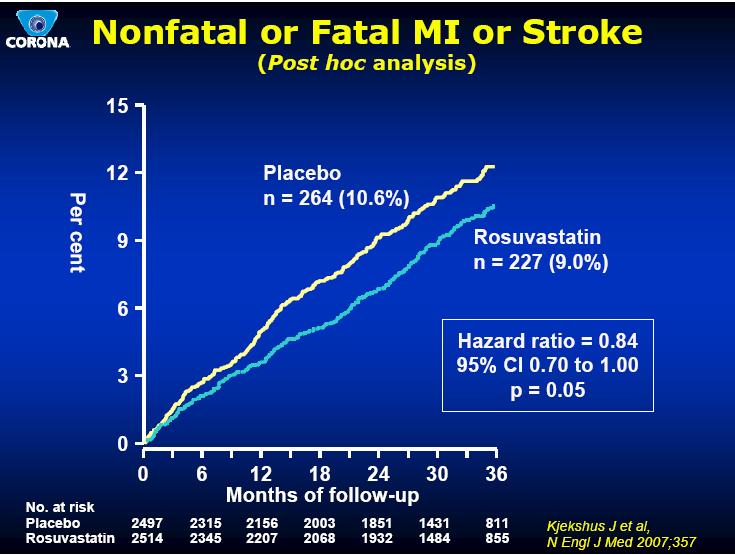
45 Potential Explanations for CORONA Elderly HF patients are less likely to benefit from statin therapy ACS events are an infrequent in cause of fatal events in HF and therefore the wrong primary outcome was chosen No incremental benefit when already treated with ACEI/ARB and beta blockers Dose was too low and higher doses of statin therapy needed Not a class effect and other statins may provide benefit Statins do not benefit patients with HF and the observational data was confounded Kjekshus J et al. N Engl J Med 2007;357.
46 GISSI-HF The Gruppo Italiano per lo Studio della Sopravvivenza nell Insufficienza Cardiaca Heart Failure (GISSI-HF) trial Adapted from: Tavazzi et al. Eur J Heart Fail 2004;6: GISSI-HF Investigators. Lancet 2008;doi: /S (08)
47 GISSI-HF GISSI-HF is a double-blind, placebocontrolled, randomized trial designed to assess the effects of n-3 polyunsaturated fatty acids (PUFAs) and rosuvastatin in symptomatic congestive heart failure patients.
48 GISSI-HF Objectives The primary objective was to investigate whether the long-term administration of n-3 PUFA (1 g q.d.) and rosuvastatin (10 mg q.d.) is more effective than the corresponding placebo in the reduction of two co-primary outcomes: all-cause mortality all-cause mortality or hospitalization for cardiovascular (CV) reasons
49 GISSI-HF Study Design R1 (n=6975) n-3 PUFA 1 g q.d. (n=3494) Placebo (n=3481) R2 (n=4574) Rosuvastatin 10 mg q.d. (n=2285) Placebo (n=2289) R1, R2 Median follow-up 3.9 years Visit: Month: D D At each visit, the following assessments were performed: CV examination, vital signs, 12-lead electrocardiogram, compliance check, serious adverse events assessment and blood chemistry NYHA=New York Heart Association; R1=randomization 1; R2=randomization 2; D=drug distribution D D D D D Adapted from: Tavazzi et al. Eur J Heart Fail 2004;6: GISSI-HF Investigators. Lancet 2008;doi: /S (08)
50 GISSI-HF Study End Points Two Co-primary end points All-cause mortality* All-cause mortality or CV hospitalizations* Secondary end points CV mortality CV mortality or hospitalization for any reason Sudden cardiac death Hospitalization for any reason Hospitalization for CV reasons Hospitalization for heart failure Myocardial infarction (MI) Stroke *assessed as to time to event Adapted from: Tavazzi et al. Eur J Heart Fail 2004;6: GISSI-HF Investigators. Lancet 2008;doi: /S (08)
51 GISSI-HF Power Analysis Power calculated on 1 st co-primary endpoint: time to death 90% power Expected mortality rate at 3 years in placebo group of 25% Number of events needed to detect 15% reduction by rosuvastatin n = 1252
52 Statistical Analysis To estimate treatment effect, the main analysis was undertaken by fitting Cox proportional hazards models adjusted for the variables that were unbalanced between the randomized groups (P<0.1) Unconventional, but prespecified because prognostic variables in this type of HF patients unknown Assumption of proportional hazard for the randomized treatments was appropriately checked by means of the log (- log[survival]) plot and time dependent covariate test Kaplan Meier Survival curves with log rank tests To explore effect modification of subjects receiving both treatments, Cox proportional hazards model with model for terms of PUFA, rosuvastatin, and their interaction
53 Statistics Subgroup Analysis The effects of the study drugs will be evaluated in the following predefined subgroups of patients: Age (above vs. below median age; 70 years) Left ventricular (LV) function (LV ejection fraction [LVEF} >40% vs. <40%) Functional capacity (New York Heart Association [NYHA] class II vs. III-IV) Etiology (ischemic vs. non-ischemic) Diabetes (yes vs. no) Baseline total cholesterol levels (above vs. below median value; 4.97 mmol/l) The end point for all the subgroup analyses is the combined outcome measure of all-cause mortality or hospital admission for CV reasons. Adapted from: Tavazzi et al. Eur J Heart Fail 2004;6: GISSI-HF Investigators. Lancet 2008;doi: /S (08)
54 GISSI-HF Entry Criteria Clinical evidence of heart failure of any etiology Classified as NYHA class II IV Treated according to European Society of Cardiology guidelines LVEF measured within three months of enrolment If EF is >40%, at least one hospital admission for heart failure in the previous year is required Age 18 and over Adapted from: Tavazzi et al. Eur J Heart Fail 2004;6: GISSI-HF Investigators. Lancet 2008;doi: /S (08)
55 GISSI-HF Exclusion Criteria Known hypersensitivity to study treatment Presence of any non-cardiac disease (e.g. cancer) that is likely to significantly shorten life expectancy Treatment with any investigational agent within 1 month before randomization Acute coronary syndrome or revascularization procedure within 1 month prior to randomization Planned cardiac surgery expected to be performed within 3 months after randomization Significant liver disease Serum creatinine level >221 µmol/l Alanine and aspartate transaminase levels >1.5 times the upper limit of normal (ULN) Current creatine phosphokinase level above ULN Pregnant or lactating women or women of childbearing potential not protected from pregnancy by an accepted method of contraception Adapted from: Tavazzi et al. Eur J Heart Fail 2004;6: GISSI-HF Investigators. Lancet 2008;doi: /S (08)
56 GISSI-HF Baseline Characteristics Rosuvastatin Placebo n=2285 n=2289 Patient Characteristics Mean age (years) >70 years (%) Female sex (%) Heart disease risk factors Body mass index (kg/m 2 ) Systolic BP (mmhg) Diastolic BP (mmhg) Heart rate (BPM) Current smoker (%) History of hypertension (%) NYHA class (%) II III IV EF(%) EF>40% (%) Adapted from GISSI-HF Investigators. Lancet 2008; doi: /s (08)
57 GISSI-HF Baseline Characteristics Rosuvastatin Placebo n=2285 n=2289 Medical History Hospitalization for HF in previous year (%) Previous MI (%) Previous stroke (%) Diabetes mellitus (%) CABG (%) PCI (%) ICD (%) Pacemaker (%) History of atrial fibrillation (%) PVD (%) 8.1 CABG coronary artery bypass grafting; PCI percutaneous coronary intervention; ICD implantable cardioverter-defibrillator; PVD COPD peripheral vascular (%) disease; COPD chronic obstructive pulmonary disease; HF heart 23.5 failure 22.8 Neoplasia (%) 3.3 Adapted from GISSI-HF Investigators. Lancet 2008; doi: /s (08)
58 GISSI-HF Baseline Characteristics Rosuvastatin Placebo n=2285 n=2289 Heart Failure Cause/Etiology Ischemic (%) Dilatative (%) Hypertensive (%) Other causes (%) Non-detectable/unknown (%) Physical Examinations Pulmonary râles (%) Third heart sound (%) Mitral insufficiency (%) Aortic stenosis (%) ECG Findings *QRS>120 ms (%) Atrial fibrillation (%) Pathological Q waves (%) LV hypertrophy (%) *Assessed with 2257 rosuvastatin patients and 2266 placebo patients Adapted from GISSI-HF Investigators. Lancet 2008; doi: /s (08)
59 GISSI-HF Current Medications Medication Rosuvastatin Placebo n=2285 n=2289 ACE inhibitors (%) ARBs (%) ACE inhibitors/arbs (%) Beta blockers (%) Spironolactone (%) Diuretics (%) Digitalis (%) Oral anticoagulants (%) ASA (%) Other antiplatelet agents (%) Nitrates (%) Calcium channel blockers (%) Amiodarone (%) ARB =angiotensin receptor blocker Adapted from GISSI-HF Investigators. Lancet 2008; doi: /s (08)
60 Probability of Death (all causes) First co-primary endpoint (death from all causes) Time Since Randomization (mo) GISSI-HF Investigators. Lancet
61 Probability of All-Cause Death or Admission for CV Reason Second co-primary endpoint (death from all causes or CV hospitalization) GISSI-HF Investigators. Lancet Time Since Randomization (mo)
62 GISSI-HF Co-primary End Points (i) All-cause mortality and (ii) all-cause mortality or hospitalizations for CV reasons Rosuvastatin (n=2285) n (%) Placebo (n=2289) n (%) HR* CI P value Primary end points All-cause mortality 657 (29) 644 (28) 1.00 [95.5% CI ] 0.94 All-cause mortality or CV hospitalizations 1305 (57) 1283 (56) 1.01 [99% CI ] 0.90 HR = hazard ratio; CI = confidence interval *adjusted HR Effect modification of rosuvastatin + fish oil excluded for both outcomes Adapted from GISSI-HF Investigators. Lancet 2008; doi: /s (08)
63 GISSI-HF - Secondary Endpoints Rosuvastatin (n=2285) n (%) Placebo (n=2289) n (%) HR* 95% CI P value Secondary end points CV mortality 478 (20.9) 488 (21.3) 0.96 [ ] Sudden cardiac death 220 (9.6) 196 (8.6) 1.12 [ ] Patients hospitalized 1278 (55.9) 1286 (56.2) 0.99 [ ] Hospitalization for CV reason 1033 (45.2) 1060 (46.3) 0.96 [ ] Hospitalization for HF 629 (27.5) 634 (27.7) 0.97 [ ] CV mortality or hospitalization for any reason 1417 (62.0) 1385 (60.5) 1.02 [ ] Fatal/non-fatal MI 61 (2.7) 70 (3.1) 0.89 [ ] Fatal/non-fatal stroke 82 (3.6) 66 (2.9) 1.23 [ ] *adjusted HR Adapted from GISSI-HF Investigators. Lancet 2008; doi: /s (08)
64 GISSI-HF Cause of Death Total mortality CV mortality Acute MI Worsening of heart failure Presumed arrhythmic Stroke Other CV reasons Non-CV mortality Neoplasia Other non-cv reason Not known Rosuvastatin (n=2285) n (%) 657 (28.8) 478 (20.9) 10 (0.4) 203 (8.9) 198 (8.7) 38 (1.7) 29 (1.3) 156 (6.8) 81 (3.5) 75 (3.3) 23 (1.0) Placebo (n=2289) n (%) 644 (28.1) 488 (21.3) 15 (0.7) 231 (10.1) 182 (8.0) 29 (1.3) 31 (1.4) 179 (7.8) 75 (3.3) 55 (2.4) 26 (1.1) Adapted from GISSI-HF Investigators. Lancet 2008; doi: /s (08)
65 GISSI-HF: Causes of CV Mortality No. of CV deaths=478 No. of CV deaths= Other CV Stroke Presumed arrhythmic Worsening HF Acute MI Rosuvastatin (n=2285) Placebo (n=2289) Adapted from GISSI-HF Investigators. Lancet 2008;doi: /S (08)
66 Patients with event (%) GISSI-HF Predefined subgroup analysis All cause mortality or hospitalizations for cardiovascular reasons Rosuvastatin Placebo % ns 48.9% ns ns 63.1% 63.6% 64.7% ns 58.9% 58.7% 56.9% 55.8% ns 63.0% 52.1% ns 51.4% / / / / / 2049 Age <70 yrs Age >70 yrs EF < 40% EF > 40% Ischaemic HF 1151/ / / / / / / 1370 Non-ischaemic HF Adapted from GISSI-HF Investigators. Lancet 2008; doi: /s (08)
67 Patients with event (%) GISSI-HF Predefined Subgroup Analysis All-cause mortality or hospitalizations for CV reasons Rosuvastatin 80 Placebo % ns 51.1% 66.6% ns 64.8% 63.5% ns 63.8% ns ns 60.4% 58.6% 54.7% 53.5% 53.9% ns 53.2% / / / / / 625 NYHA II NYHA III-IV Diabetes No diabetes TC < 4.97 mmol/l 364/ / / / / / / 1118 TC > 4.97 mmol/l Adapted from GISSI-HF Investigators. Lancet 2008; doi: /s (08)
68 GISSI-HF Lipid Data Rosuvastatin (n=2285) Placebo (n=2289) LDL-C Baseline; mmol/l (mg/dl) 3.16 (122) 3.13 (121) One year; mmol/l (mg/dl) 2.15 (83) 3.37 (113) Three years; mmol/l (mg/dl) 2.31 (89) 3.06 (118) Exploratory analysis of treatment effect of how low LDL is lowered shows no effect Adapted from GISSI-HF Investigators. Lancet 2008; doi: /s (08)
69 GISSI-HF Tolerability and Safety Data Permanent discontinuations and adverse drug reactions (ADR) Patients who permanently discontinued study treatment, n (%) Patients who permanently discontinued study treatment due to ADR, n (%) GI disorders Asthenia Allergic reaction Liver dysfunction Lipid abnormality Creatine phosphokinase increase Renal dysfunction Acute renal failure Hepatocellular jaundice Acute dermatitis* Muscle-related symptoms Patients who permanently discontinued study treatment due to serious ADR, n (%) Acute renal failure Acute dermatitis* Rosuvastatin (n=2285) 790 (34.6) 104 (4.6) *Diagnosed as Stevens-Johnson syndrome by the investigator, not confirmed by an expert adjudicator Adapted from GISSI-HF Investigators. Lancet 2008; doi: /s (08) Placebo (n=2289) 831 (36.3) 91 (4.0)
70 GISSI-HF Tolerability and Safety Data Laboratory safety data Rosuvastatin (n=2285) Placebo (n=2289) CK elevations CK > 10 x ULN (n) 1 1 Serum creatinine Doubling of serum creatinine, n (%) 65 (3%) 57 (2.6%) Baseline, µmol/l (mg/dl)* (1.07) (1.08) One year, µmol/l (mg/dl)* (1.09) (1.10) Three years, µmol/l (mg/dl)* (1.10) (1.10) *Median values CK = creatine kinase Adapted from GISSI-HF Investigators. Lancet 2008; doi: /s (08)
71 GISSI-HF Summary and Perspectives GISSI-HF showed no difference between rosuvastatin 10 mg and placebo in the primary end points of death or CV hospitalization in patients with heart failure, with no specific indication for statin treatment, over and above optimized heart failure treatment. GISSI-HF supports the findings from CORONA by showing that adding a statin to optimized heart failure treatment does not significantly improve the prognosis for patients with heart failure because it cannot reverse or prevent the further deterioration of a failing heart. The investigators suggest that there are too few acute ischemic events (heart attacks and strokes) in heart failure patients for a statin to show a benefit. Rosuvastatin10 mg was well tolerated in nearly 2,300 patients during the course of the GISSI-HF study, with a safety profile similar to placebo. Adapted from: GISSI-HF Investigators. Lancet 2008; doi: /s (08) Fonarow GC. Lancet 2008;doi: /S (08) Kjekshus et al. N Engl J Med 2007;357:
72 Limitations GISSI-HF Statin class effect (unlikely), 1 dose tested, only 10% with EF>40%, 24% women, LDL 120 mg/dl Explanations Different HF phenotypes, benefit washed out by ACE/ARB and β-blocker (ie, intensity of treatment) longer duration of treatment may be necessary pleiotrophic effects of statins not clinically relevant Any beneficial effects of statins in this population are off-set by detrimental effect of lowering cholesterol
73 Death or Urgent Transplant, % In Heart Failure, the Reverse is True. Higher Cholesterol Levels are Associated with Reduced Mortality < P= Deciles of Total Cholesterol 1134 Advanced HF patients Horwich. J of Card Failure 2002;8: >250

74 Kaul and Diamond. JACC 2010; 55:

75 Kaul and Diamond. JACC 2010; 55:
76 Cholesterol-Independent Effects of Statins Acetyl-CoA HMG-CoA HMG-CoA Reductase Mevalonate Isopentenyl-PP Geranyl-PP Dolichol, Farnesylated Protein (ie, Ras) Farnesyl-PP + Isopentenyl-PP Squalene Geranylgeranyl-PP Cholesterol Takemoto et al. Arterioscler Thromb Vasc Biol. 2001;21: Geranylgeranylated Proteins (ie, Rho)
New evidences in heart failure: the GISSI-HF trial. Aldo P Maggioni, MD ANMCO Research Center Firenze, Italy
 New evidences in heart failure: the GISSI-HF trial Aldo P Maggioni, MD ANMCO Research Center Firenze, Italy % Improving survival in chronic HF and LV systolic dysfunction: 1 year all-cause mortality 20
New evidences in heart failure: the GISSI-HF trial Aldo P Maggioni, MD ANMCO Research Center Firenze, Italy % Improving survival in chronic HF and LV systolic dysfunction: 1 year all-cause mortality 20
Should I use statins?
 I know the trials in heart failure but how do I manage my patient? Should I use statins? Aldo P Maggioni, MD, FESC ANMCO Research Center Firenze, Italy Disclosures Aldo P Maggioni served as a member of
I know the trials in heart failure but how do I manage my patient? Should I use statins? Aldo P Maggioni, MD, FESC ANMCO Research Center Firenze, Italy Disclosures Aldo P Maggioni served as a member of
Rikshospitalet, University of Oslo
 Rikshospitalet, University of Oslo Preventing heart failure by preventing coronary artery disease progression European Society of Cardiology Dyslipidemia 29.08.2010 Objectives The trends in cardiovascular
Rikshospitalet, University of Oslo Preventing heart failure by preventing coronary artery disease progression European Society of Cardiology Dyslipidemia 29.08.2010 Objectives The trends in cardiovascular
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Performance and Quality Measures 1. NQF Measure Number. Coronary Artery Disease Measure Set
 Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Online Appendix (JACC )
") Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis
Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis
HFpEF, Mito or Realidad?
 HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
Heart Failure: Combination Treatment Strategies
 Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Program Metrics. New Unique ID. Old Unique ID. Metric Set Metric Name Description. Old Metric Name
 Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Is there a mortality risk associated with aspirin use in heart failure? Results from a large community based cohort Margaret Bermingham, Mary-Kate Shanahan, Saki Miwa,
DECLARATION OF CONFLICT OF INTEREST Is there a mortality risk associated with aspirin use in heart failure? Results from a large community based cohort Margaret Bermingham, Mary-Kate Shanahan, Saki Miwa,
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing
 Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Heart Failure Management. Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist
 Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
Protecting the heart and kidney: implications from the SHARP trial
 Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Supplementary Online Content
 Supplementary Online Content Nikolova AP, Hitzeman TC, Baum R, et al. Association of a novel diagnostic biomarker, the plasma cardiac bridging integrator 1 score, with heart failure with preserved ejection
Supplementary Online Content Nikolova AP, Hitzeman TC, Baum R, et al. Association of a novel diagnostic biomarker, the plasma cardiac bridging integrator 1 score, with heart failure with preserved ejection
Polypharmacy - arrhythmic risks in patients with heart failure
 Influencing sudden cardiac death by pharmacotherapy Polypharmacy - arrhythmic risks in patients with heart failure Professor Dan Atar Head, Dept. of Cardiology Oslo University Hospital Ullevål Norway 27.8.2012
Influencing sudden cardiac death by pharmacotherapy Polypharmacy - arrhythmic risks in patients with heart failure Professor Dan Atar Head, Dept. of Cardiology Oslo University Hospital Ullevål Norway 27.8.2012
Pharmacological Treatment for Chronic Heart Failure. Dr Elaine Chau HK Sanatorium & Hospital, Hong Kong 3 August 2014
 Pharmacological Treatment for Chronic Heart Failure Dr Elaine Chau HK Sanatorium & Hospital, Hong Kong 3 August 2014 1 ACC/AHA 2005 guideline update for Diagnosis & management of CHF in the Adult -SA Hunt
Pharmacological Treatment for Chronic Heart Failure Dr Elaine Chau HK Sanatorium & Hospital, Hong Kong 3 August 2014 1 ACC/AHA 2005 guideline update for Diagnosis & management of CHF in the Adult -SA Hunt
Risk Stratification of Sudden Cardiac Death
 Risk Stratification of Sudden Cardiac Death Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC USA Disclosures: None Sudden Cardiac Death A Major Public Health Problem > 1/2 of
Risk Stratification of Sudden Cardiac Death Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC USA Disclosures: None Sudden Cardiac Death A Major Public Health Problem > 1/2 of
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0.
 New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
Role of Clopidogrel in Acute Coronary Syndromes. Hossam Kandil,, MD. Professor of Cardiology Cairo University
 Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials -
 Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials - Clinical trials Evidence-based medicine, clinical practice Impact upon Understanding pathophysiology
Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials - Clinical trials Evidence-based medicine, clinical practice Impact upon Understanding pathophysiology
PROGNOSTIC VALUE OF OSTEOPROTEGERIN IN CHRONIC HEART FAILURE: THE GISSI-HF TRIAL
 PROGNOSTIC VALUE OF OSTEOPROTEGERIN IN CHRONIC HEART FAILURE: THE GISSI-HF TRIAL Ragnhild Røysland MD 1,2, Serge Masson PhD 3, Torbjørn Omland MD, PhD, MPH 1,2, Valentina Milani MS 3, Mette Bjerre PhD
PROGNOSTIC VALUE OF OSTEOPROTEGERIN IN CHRONIC HEART FAILURE: THE GISSI-HF TRIAL Ragnhild Røysland MD 1,2, Serge Masson PhD 3, Torbjørn Omland MD, PhD, MPH 1,2, Valentina Milani MS 3, Mette Bjerre PhD
Decline in CV-Mortality
 Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long. Case Study 2
 HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long Case Study 2 HEART FAILURE WITH MID-RANGE EJECTION FRACTION TREATMENT OPTIONS CLINICAL CASE MEDICAL HISTORY 59-year-old
HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long Case Study 2 HEART FAILURE WITH MID-RANGE EJECTION FRACTION TREATMENT OPTIONS CLINICAL CASE MEDICAL HISTORY 59-year-old
8:30-10:30 WS #4: Cardiology :00-13:00 WS #11: Cardiology 101 (Repeated)
") Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Treating HF Patients with ARNI s Why, When and How?
 Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Cholesterol Treatment Trialists Collaboration.
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Cholesterol Treatment Trialists Collaboration.
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
Quality Payment Program: Cardiology Specialty Measure Set
 Quality Payment Program: Cardiology Specialty Set Title Number CMS Reporting Method(s) Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for
Quality Payment Program: Cardiology Specialty Set Title Number CMS Reporting Method(s) Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
Dialysis-Dependent Cardiomyopathy Patients Demonstrate Poor Survival Despite Reverse Remodeling With Cardiac Resynchronization Therapy
 Dialysis-Dependent Cardiomyopathy Patients Demonstrate Poor Survival Despite Reverse Remodeling With Cardiac Resynchronization Therapy Evan Adelstein, MD, FHRS John Gorcsan III, MD Samir Saba, MD, FHRS
Dialysis-Dependent Cardiomyopathy Patients Demonstrate Poor Survival Despite Reverse Remodeling With Cardiac Resynchronization Therapy Evan Adelstein, MD, FHRS John Gorcsan III, MD Samir Saba, MD, FHRS
New Strategies For Treating Patients With Chronic Heart Failure
 New Strategies For Treating Patients With Chronic Heart Failure Barry Greenberg MD Professor of Medicine Director, Advanced Heart Failure Treatment Program University of California, San Diego Disclosures
New Strategies For Treating Patients With Chronic Heart Failure Barry Greenberg MD Professor of Medicine Director, Advanced Heart Failure Treatment Program University of California, San Diego Disclosures
Cardiovascular Pharmacotherapy
 Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Patient characteristics Intervention Comparison Length of followup
 ISCHAEMIA TESTING CHAPTER TESTING FOR MYCOCARDIAL ISCHAEMIA VERSUS NOT TESTING FOR MYOCARDIAL ISCHAEMIA Ref ID: 4154 Reference Wienbergen H, Kai GA, Schiele R et al. Actual clinical practice exercise ing
ISCHAEMIA TESTING CHAPTER TESTING FOR MYCOCARDIAL ISCHAEMIA VERSUS NOT TESTING FOR MYOCARDIAL ISCHAEMIA Ref ID: 4154 Reference Wienbergen H, Kai GA, Schiele R et al. Actual clinical practice exercise ing
Clinical and Economic Value of Rivaroxaban in Coronary Artery Disease
 CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
The Hearth Rate modulators. How to optimise treatment
 The Hearth Rate modulators How to optimise treatment Munich, ESC Congress 2012 Prof. Luigi Tavazzi GVM Care&Research E.S. Health Science Foundation Cotignola, IT Disclosure Cooperation with: Servier, Medtronic,
The Hearth Rate modulators How to optimise treatment Munich, ESC Congress 2012 Prof. Luigi Tavazzi GVM Care&Research E.S. Health Science Foundation Cotignola, IT Disclosure Cooperation with: Servier, Medtronic,
Efficacy of beta-blockers in heart failure patients with atrial fibrillation: An individual patient data meta-analysis
 Efficacy of beta-blockers in heart failure patients with atrial fibrillation: An individual patient data meta-analysis Dipak Kotecha, MD PhD on behalf of the Selection of slides presented at the European
Efficacy of beta-blockers in heart failure patients with atrial fibrillation: An individual patient data meta-analysis Dipak Kotecha, MD PhD on behalf of the Selection of slides presented at the European
Optimal blockade of the Renin- Angiotensin-Aldosterone. in chronic heart failure
 Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Heart Failure Dr Eric Klug Sunninghill, Sunward Park, CM Johannesburg Academic Hospital
 Heart Failure 2012 Dr Eric Klug Sunninghill, Sunward Park, CM Johannesburg Academic Hospital PRELOAD COWS Reduction in milk production INOTROPY & HEART RATE AFTERLOAD DISTRIBUTION NETWORK THE CLASSIC APPROACH
Heart Failure 2012 Dr Eric Klug Sunninghill, Sunward Park, CM Johannesburg Academic Hospital PRELOAD COWS Reduction in milk production INOTROPY & HEART RATE AFTERLOAD DISTRIBUTION NETWORK THE CLASSIC APPROACH
Trial to Reduce. Aranesp* Therapy. Cardiovascular Events with
 Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
Position Statement on ALDOSTERONE ANTAGONIST THERAPY IN CHRONIC HEART FAILURE
 Position Statement on ALDOSTERONE ANTAGONIST THERAPY IN CHRONIC HEART FAILURE Over 8,000 patients have been studied in two well-designed placebo-controlled outcome-driven clinical trials to evaluate the
Position Statement on ALDOSTERONE ANTAGONIST THERAPY IN CHRONIC HEART FAILURE Over 8,000 patients have been studied in two well-designed placebo-controlled outcome-driven clinical trials to evaluate the
Disclosures. Overview. Goal statement. Advances in Chronic Heart Failure Management 5/22/17
 Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Heart Failure Guidelines For your Daily Practice
 Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
Controversies with regard to 'upstream therapy of atrial fibrillation
 Controversies with regard to 'upstream therapy of atrial fibrillation Barbara Casadei Department of Cardiovascular Medicine John Radcliffe Hospital University of Oxford No conflict of interest to declare
Controversies with regard to 'upstream therapy of atrial fibrillation Barbara Casadei Department of Cardiovascular Medicine John Radcliffe Hospital University of Oxford No conflict of interest to declare
Disclosures. Advances in Chronic Heart Failure Management 6/12/2017. Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017
 Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Diabetes and the Heart
 Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Practice-Level Executive Summary Report
 PINNACLE Registry Metrics 0003, Test Practice_NextGen [Rolling: 1st April 2015 to 31st March 2016 ] Generated on 5/11/2016 11:37:35 AM American College of Cardiology Foundation National Cardiovascular
PINNACLE Registry Metrics 0003, Test Practice_NextGen [Rolling: 1st April 2015 to 31st March 2016 ] Generated on 5/11/2016 11:37:35 AM American College of Cardiology Foundation National Cardiovascular
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
GALECTIN-3 PREDICTS LONG TERM CARDIOVASCULAR DEATH IN HIGH-RISK CORONARY ARTERY DISEASE PATIENTS
 GALECTIN-3 PREDICTS LONG TERM CARDIOVASCULAR DEATH IN HIGH-RISK CORONARY ARTERY DISEASE PATIENTS Table of Contents List of authors pag 2 Supplemental figure I pag 3 Supplemental figure II pag 4 Supplemental
GALECTIN-3 PREDICTS LONG TERM CARDIOVASCULAR DEATH IN HIGH-RISK CORONARY ARTERY DISEASE PATIENTS Table of Contents List of authors pag 2 Supplemental figure I pag 3 Supplemental figure II pag 4 Supplemental
Vitals HR 90 BP 125/58 Tmax 98.7F O2 Sat 97% on NC 2L/min BMP SCr 1.78 K 3.9 Gluc 194 A1c 7.5 Cardiac LVEF 55% NTproBNP 9,200 Troponin 0.
 ALDOSTERONE ANTAGONIST IN HEART FAILURE WITH PRESERVED EJECTION FRACTION ABBREVIATIONS BMP: basic metabolic panel HPI: history of present illness CAD: coronary artery disease HR: heart rate PINHUI (JUDY)
ALDOSTERONE ANTAGONIST IN HEART FAILURE WITH PRESERVED EJECTION FRACTION ABBREVIATIONS BMP: basic metabolic panel HPI: history of present illness CAD: coronary artery disease HR: heart rate PINHUI (JUDY)
Is there a role for Statins in Heart Failure? JC Mohan New Delhi
 Is there a role for Statins in Heart Failure? JC Mohan New Delhi HF/CHF Neuro-humorally mediated inflammatory disorder Demand- Inappropriate Cardiac output ( HRX SV) Elevated filling pressures Both phenotypes
Is there a role for Statins in Heart Failure? JC Mohan New Delhi HF/CHF Neuro-humorally mediated inflammatory disorder Demand- Inappropriate Cardiac output ( HRX SV) Elevated filling pressures Both phenotypes
12 th Annual Biomarkers in Heart Failure and Acute Coronary Syndromes: Diagnosis, Treatment and Devices. Heart Rate as a Cardiovascular Biomarker
 12 th Annual Biomarkers in Heart Failure and Acute Coronary Syndromes: Diagnosis, Treatment and Devices Heart Rate as a Cardiovascular Biomarker Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine,
12 th Annual Biomarkers in Heart Failure and Acute Coronary Syndromes: Diagnosis, Treatment and Devices Heart Rate as a Cardiovascular Biomarker Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine,
Cardiovascular Guideline-Driven Pharmacotherapies: Optimizing Management
 Cardiovascular Guideline-Driven Pharmacotherapies: Optimizing Management David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management
Cardiovascular Guideline-Driven Pharmacotherapies: Optimizing Management David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management
Prevention of Atrial Fibrillation and Heart Failure in the Hypertensive Patient
 Prevention of Atrial Fibrillation and Heart Failure in the Hypertensive Patient The Issue of Primary Prevention of A.Fib. (and Heart Failure) and not the Prevention of Recurrent A.Fib. after Electroconversion
Prevention of Atrial Fibrillation and Heart Failure in the Hypertensive Patient The Issue of Primary Prevention of A.Fib. (and Heart Failure) and not the Prevention of Recurrent A.Fib. after Electroconversion
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM. General Instructions: ID NUMBER: FORM NAME: H F A DATE: 10/13/2017 VERSION: CONTACT YEAR NUMBER:
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study
 Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study Dr. Antonio Magaña M.D. (on behalf I-PREFER investigators group) Stockholm, Sweden, August
Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study Dr. Antonio Magaña M.D. (on behalf I-PREFER investigators group) Stockholm, Sweden, August
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATO trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
Implementing the CardioMEMS HF System into the Management of Heart Failure Patients
 Implementing the CardioMEMS HF System into the Management of Heart Failure Patients Robert W. Hull MD FACC Associate Professor of Medicine WVU Heart Institute Co-director, Arrhythmia Service Director,
Implementing the CardioMEMS HF System into the Management of Heart Failure Patients Robert W. Hull MD FACC Associate Professor of Medicine WVU Heart Institute Co-director, Arrhythmia Service Director,
Checklist for Treating Heart Failure. Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute
 Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
The Author(s) This article is published with open access by ASEAN Federation of Cardiology
 This article is published with open access by ASEAN Federation of Cardiology") DOI 10.7603/s40602-014-0011-3 ASEAN Heart Journal http://www.aseanheartjournal.org/ Vol. 22, no. 1, 60 65 (2014) ISSN: 2315-4551 Erratum Erratum to: Impact Of Sex On Clinical Characteristics And In-Hospital
DOI 10.7603/s40602-014-0011-3 ASEAN Heart Journal http://www.aseanheartjournal.org/ Vol. 22, no. 1, 60 65 (2014) ISSN: 2315-4551 Erratum Erratum to: Impact Of Sex On Clinical Characteristics And In-Hospital
Heart Failure Medical and Surgical Treatment
 Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary
 Prior Authorization and Quantity Limit Program Summary") Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
A patient with decompensated HF
 A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
Subclinical AF: Implications of device based episodes
 Subclinical AF: Implications of device based episodes Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Clinical Trials and Consulting: Medtronic, Boston Scientific
Subclinical AF: Implications of device based episodes Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Clinical Trials and Consulting: Medtronic, Boston Scientific
Heart Failure: Guideline-Directed Management and Therapy
 Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Quality Payment Program: Cardiology Specialty Measure Set
 Measure Title * Reportable via PINNACLE α Reportable via Diabetes Collaborative CQMC v1.0 Measure High Priority Measure Cross Cutting Measure Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor
Measure Title * Reportable via PINNACLE α Reportable via Diabetes Collaborative CQMC v1.0 Measure High Priority Measure Cross Cutting Measure Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor
Supplementary Online Content
 Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Update on pharmacological treatment of heart failure. Aldo Pietro Maggioni, MD, FESC ANMCO Research Center Firenze, Italy
 Update on pharmacological treatment of heart failure Aldo Pietro Maggioni, MD, FESC ANMCO Research Center Firenze, Italy Presenter Disclosures Dr. Maggioni : Serving in Committees of studies sponsored
Update on pharmacological treatment of heart failure Aldo Pietro Maggioni, MD, FESC ANMCO Research Center Firenze, Italy Presenter Disclosures Dr. Maggioni : Serving in Committees of studies sponsored
Measurement Name Beta-Blocker Therapy Prior Myocardial Infarction (MI)
") Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for Artery, Atrial Fibrillation, Hypertension
Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for Artery, Atrial Fibrillation, Hypertension
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017
 Clinician Guide SEPTEMBER 2017") Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National Coronary Artery Disease
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National Coronary Artery Disease
I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists
 I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists Alessandro Fucili (Ferrara, IT) Massimo F Piepoli (Piacenza, IT) Clinical Case: 82 year old woman
I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists Alessandro Fucili (Ferrara, IT) Massimo F Piepoli (Piacenza, IT) Clinical Case: 82 year old woman
Treatment to reduce cardiovascular risk: multifactorial management
 Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
An update on the management of UA / NSTEMI. Michael H. Crawford, MD
 An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
Treatment Of Preserved Cardiac Function Heart Failure with an Aldosterone antagonist (TOPCAT) AHA Nov 18, 2014 Update on Randomized Trials
 AHA Nov 18, 2014 Update on Randomized Trials") Treatment Of Preserved Cardiac Function Heart Failure with an Aldosterone antagonist (TOPCAT) AHA Nov 18, 2014 Update on Randomized Trials Marc A. Pfeffer, MD, PhD; Brian Claggett, PhD; Susan F. Assmann,
Treatment Of Preserved Cardiac Function Heart Failure with an Aldosterone antagonist (TOPCAT) AHA Nov 18, 2014 Update on Randomized Trials Marc A. Pfeffer, MD, PhD; Brian Claggett, PhD; Susan F. Assmann,
Catheter-based mitral valve repair MitraClip System
 Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
Objectives. Systolic Heart Failure: Definitions. Heart Failure: Historical Perspective 2/7/2009
 Objectives Diastolic Heart Failure and Indications for Echocardiography in the Asian Population Damon M. Kwan, MD UCSF Asian Heart & Vascular Symposium 02.07.09 Define diastolic heart failure and differentiate
Objectives Diastolic Heart Failure and Indications for Echocardiography in the Asian Population Damon M. Kwan, MD UCSF Asian Heart & Vascular Symposium 02.07.09 Define diastolic heart failure and differentiate
ST2 in Heart Failure. ST2 as a Cardiovascular Biomarker. Competitive Model of ST2/IL-33 Signaling. ST2 and IL-33: Cardioprotective
 ST2 as a Cardiovascular Biomarker Lori B. Daniels, MD, MAS, FACC Professor of Medicine Director, Coronary Care Unit University of California, San Diego ST2 and IL-33: Cardioprotective ST2: member of the
ST2 as a Cardiovascular Biomarker Lori B. Daniels, MD, MAS, FACC Professor of Medicine Director, Coronary Care Unit University of California, San Diego ST2 and IL-33: Cardioprotective ST2: member of the
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
LCZ696 A First-in-Class Angiotensin Receptor Neprilysin Inhibitor
 The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
2017 Summer MAOFP Update
 2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
Cardiac Devices CRT,ICD: Who is and is not a Candidate? Who Decides
 Cardiac Devices CRT,ICD: Who is and is not a Candidate? Who Decides Colette Seifer MB(Hons) FRCP(UK) Associate Professor, University of Manitoba, Cardiologist, Cardiac Sciences Program, St Boniface Hospital
Cardiac Devices CRT,ICD: Who is and is not a Candidate? Who Decides Colette Seifer MB(Hons) FRCP(UK) Associate Professor, University of Manitoba, Cardiologist, Cardiac Sciences Program, St Boniface Hospital
Diagnosis is it really Heart Failure?
 ESC Congress Munich - 25-29 August 2012 Heart Failure with Preserved Ejection Fraction From Bench to Bedside Diagnosis is it really Heart Failure? Prof. Burkert Pieske Department of Cardiology Med.University
ESC Congress Munich - 25-29 August 2012 Heart Failure with Preserved Ejection Fraction From Bench to Bedside Diagnosis is it really Heart Failure? Prof. Burkert Pieske Department of Cardiology Med.University
Digoxin And Mortality in Patients With Atrial Fibrillation With and Without Heart Failure: Does Serum Digoxin Concentration Matter?
 Digoxin And Mortality in Patients With Atrial Fibrillation With and Without Heart Failure: Does Serum Digoxin Concentration Matter? Renato D. Lopes, MD, PhD, FACC on behalf of the ARISTOTLE Investigators
Digoxin And Mortality in Patients With Atrial Fibrillation With and Without Heart Failure: Does Serum Digoxin Concentration Matter? Renato D. Lopes, MD, PhD, FACC on behalf of the ARISTOTLE Investigators
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Known Actions of Digoxin
 Known Actions of Digoxin Hemodynamic effects in heart failure Increases cardiac output, no effect on blood pressure Decreases PCWP Increases LVEF (
Known Actions of Digoxin Hemodynamic effects in heart failure Increases cardiac output, no effect on blood pressure Decreases PCWP Increases LVEF (